Contribution of Hepatitis D Virus in Liver Cancer Among Hepatitis B Virus Infected Populations of Central Africa: A Systematic Review and Meta-Analysis
- Mbia Job Henri
- Lebomo Etogo Eugene Liliane
- Njandja Seuyip Darryl Duriannie
- 360-373
- Apr 16, 2024
- Public Health
Contribution of Hepatitis D Virus in Liver Cancer Among Hepatitis B Virus Infected Populations of Central Africa: A Systematic Review and Meta-Analysis
Mbia Job Henri, Lebomo Etogo Eugene Liliane, Njandja Seuyip Darryl Duriannie
Douala Gynéco-Obstetric and Pediatric Hospital
DOI: https://doi.org/10.51584/IJRIAS.2024.90333
Received: 03 March 2024; Accepted: 09 March 2024; Published: 13 April 2024
ABSTRACT
Background and aims: Hepatocellular carcinoma (HCC) is a rampant disease in sub-Saharan Africa. Viral hepatitis is currently the most common factor in the occurrence of HCC in sub-Saharan Africa. Hepatitis B virus (HBV) causes liver disease which may or may not progress to HCC. In a dual infection with Hepatitis D virus (HDV), HCC tends to have a faster turn out. Our aim is to evaluate the influence of HDV on the risk of HCC and elaborate on factors favouring HDV infection.
Methods: A review of available literature in English or French was conducted in major data bases with the search terms “liver disease”, “hepatocellular carcinoma”, “hepatitis delta and liver disease”, “hepatitis D virus infection”, “prevalence of HDV”, and “hepatitis D in Central Africa”, and each term was associated to a central African country. A meta-analysis of included publications was then performed.
Results: The prevalence of HDV was 28% (95% CI). There was a higher risk of HCC in HBV-HDV dual infection (OR: 0.82 [95% CI: -0.01 to 1.65]) compared to that in HBV mono-infection. HDV genotype 1 was found to be the most prominent in central Africa, with HDV subgenotypes 1a and 1b dominating. Hepatitis delta was more prevalent in rural areas than in urban areas.
Conclusion: Hepatitis D is highly prevalent in the HBV population of central Africa. The presence of HDV increases the risk of HCC. More research has to be carried out to understand how HDV speeds up liver disease and hence how to prevent it.
Keywords: Hepatocellular carcinoma; Hepatitis delta; Hepatitis B; Dual infection; Superinfection; Sub-Saharan Africa
INTRODUCTION
Background
Hepatocellular carcinoma (HCC) is a disease with the highest yearly fatality ratio worldwide as concerns human cancers (1). According to the National Cancer Institute, chronic liver disease which is due to a hepatitis virus infection commonly results in HCC (2). report is in accordance with the fact that hepatitis B virus (HBV), hepatitis D virus (HDV), and hepatitis C virus (HCV) have been considered the greatest etiological risk factors for HCC for some years now (3). The WHO declared that 70% of the world’s HBV infections occur in Africa (4). HBV has high endemicity in sub-Saharan Africa, with approximately 60 million people having chronic hepatitis B (5), which is a very conducive environment for HDV. Chronic hepatitis D is considered the most severe form of viral hepatitis. Hepatitis D virus is dependent on HBV for key aspects of its life cycle (6), and from this fact we can extrapolate that HDV is very prominent in central Africa because of the high endemicity of HBV. It has been noticed that when HDV infects people with hepatitis B, progression to HCC is faster (7). Despite the lack of knowledge about the role of HDV in the occurrence of HCC in an HBV-HDV dual infection, it has been postulated in recent studies that the prevalence of HCC increases in populations with chronic hepatitis D as compared with people chronically infected only with HBV (8).HDV heavily contributes to the global burden of liver disease. It is capable of causing about 1 in 6 cirrhosis cases and about 1 in 5 liver cancer cases in people with hepatitis B (9). Not very long ago, it was discovered that the prevalence of HDV in hepatitis B surface antigen (HBsAg) positive populations of west and central Africa exceeded the estimated global prevalence (10).
In order to infect and be transmitted, HDV requires the HBV envelope glycoproteins (11). The hepatitis D virus includes a circular single-stranded RNA genome of 1.7 kb (which encodes a single 214-amino acid peptide), a bivariant hepatitis delta antigen (HDAg); one large (L-HDAg) and one small (S-HDAg) with 19 additional C-terminal amino acids (12). According to recent studies, HDV is probably specifically attracted to hepatocytes due to HBsAg distinctive interaction with sodium taurocholate co-transporting polypeptide (NTCP), the receptor for HBV and HDV on the hepatocyte surface. The virions of HDV then interact with heparan sulfate proteoglycans (HSPG) including GPC5, on the hepatocyte surface and binds precisely to the NTCP receptor prior to cell entry through endocytosis (13). Upon entry in hepatocytes, an L-HDAg signal localises the nucleus and launches the translocation of HDV nucleocapsid to the nucleus in which viral genome is replicated. No replication enzyme is coded for by HDV to replicate its genome, rather it uses RNA polymerase II from hepatocytes to synthesize its RNAs (14). Each virion contains close to two hundred of these molecules assembled as nucleosome-like ribonucleoproteins which consist of the HDAgs and viral RNA, essential for viral replication (15). The type of HDV and HBV dual infection gives rise to two possibilities of HDV pathogenesis; an HDV and HBV simultaneous infection leads to an acute hepatitis which may spontaneously resolve in most patients, but HDV superinfection of chronic hepatitis B patients ends in chronic HDV infection that leads to cirrhosis, liver decompensation and HCC in most cases (11). It has been elucidated in recent studies that HCC caused by HDV has a molecular profile that is unique and distinct from that of HBV despite its dependence on HBV. HDV carcinogenesis is characterised by an upset of genes involved in the cell cycle/DNA replication, and DNA damage and repair (7).
Due to its mode of replication and more importantly its genetic diversity, HDV is a difficult-to-treat virus (16). For many years now, isolates of HDV from several areas around the world have been sequenced. Studies of these isolates led to the overall recognition of eight different genotypes. Each genotype’s nucleotide sequence can vary by as much as 35% from others (17). A study carried out in sub-Saharan Africa from 1998 to 2010 showed that HDV-1 is the most prevalent across sub-Saharan Africa, distantly followed by HDV-5 and HDV-6 (18). Another, more recent study confirms that HDV-1 predominates in sub-Saharan Africa, and also shows that HDV-5 to HDV-8 are present in Africa as a whole (19). From then, it has been documented that sub-Saharan Africa is a potent host to all the above mentioned HDV subtypes (20).
Since the year 2016, the WHO global health sector strategy on viral hepatitis was created in order to significantly reduce new chronic hepatitis cases, and mortality due to viral hepatitis by 2030 (21). Key strategies needed to effectively accomplish these goals include; identification of all infected people, full vaccination of the non-infected population, prevention of mother to child transmission, and most importantly, the implementation of strategies with the support of adequate investment and funding (22).
Objectives
The main aim of this study is to investigate the contribution of hepatitis D virus in liver cancer among hepatitis B virus infected populations of central Africa. In order to attain this objective, we shall seek the prevalence of hepatitis D in hepatitis B patients and analyse the risk of HCC in patients with a dual infection compared to those with a mono-infection. Additionally, we shall assess the various HDV genotypes present in central Africa, elaborate on HDV persistence and population factors the favour the endemicity of HDV, and finally, elaborate on treatment options currently available, and prevention strategies suitable for central African populations.
METHODS
Search Strategy and Study Selection
A search for available literature was performed following the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) checklist (23). We searched Google Scholar, PubMed and Embase for articles published in English and French between January 2009 and March 2023. The search for articles was done by a group of three; the main author and two of his colleagues from the Douala Gyneco-obstetric and Pediatric Hospital. During the search, we used the terms “liver disease”, “hepatocellular carcinoma”, “hepatitis delta and liver disease”, “hepatitis D virus infection”, “prevalence of HDV”, and “hepatitis D in Central Africa”, and each search term was also associated to each central African country. On the basis of titles and abstracts, all articles were screened in order to proceed to full text review. The references of selected articles were used to obtain additional articles. The main author assessed each paper prior to inclusion in the present study. Each qualified paper was critically appraised by the main author using a critical appraisal checklist.
Inclusion and Exclusion Criteria
In this meta-analysis, we included cross-sectional studies, case control studies and cohort studies. We had as inclusion criteria: (1) Full length articles, (2) Inclusion of HDV-HBV dual infection and HBV mono-infection, (3) Inclusion of information about HDV seroprevalence and (4) Information on the incidence of hepatocellular carcinoma (HCC) in patients with HDV-HBV dual infection and HBV mono-infection. HDV infection was confirmed by a positive result for hepatitis D virus antibody (anti-HDV Ab) and/or detection of RNA and HBV infection was confirmed by a positive result for hepatitis B surface antigen (HBsAg)and/or detection of its DNA.
The exclusion criteria were as follows; (1) Lack or incomplete information about the number of cases (dual infection) and controls (mono-infection), (2) Incomplete data on the percentage of positive anti-HDV and/or HDV RNA, (3) Non availability of HBV mono-infected control group, and (4) Review articles. The Newcastle-Ottawa Scale (NOS) was used to assess risk of bias by the main author. The NOS was used in evaluating the quality of studies through; (1) the selection of study individuals, (2) Study group comparability, (3) Outcome ascertainment, and (4) Adequacy of follow up.
Statistical Analysis
All statistical analyses were performed using Jamovi version 2.3.21.0. The main investigator extracted data relevant to this study. Pooled seroprevalence was calculated using the DerSimonian-Laird random effects model with raw proportions. It was evident that heterogeneity would arise due to variations in study geography and populations, reason why we chose to use a random-effects model. We decided not to consider any study in which fewer than 50 people were tested so as to avoid small sample bias in the random-effects model. In order to determine the association between HCC incidence and HBV-HDV dual infection, odds ratios (ORs) and confidence intervals (CIs) were calculated. Heterogeneity between studies was evaluated with the Q-test for heterogeneity and the I2 statistic. Funnel plots will be used to detect the presence of publication bias amongst the selected studies.
RESULTS
Search Results
At the end of our search through the data bases, we identified 198 citations. Upon reviewing abstracts and titles, non-compliant and duplicate articles were removed, and 21 articles were left. After performing full text review 4 articles were excluded according to the exclusion criteria (Figure 1). In the end, 17 articles from 6out of the 9 central African countries were included in the meta-analysis. Amongst these, only 5 could be included in the risk for HCC meta-analysis, while all were included in the prevalence meta-analysis. The 17 articles were unevenly distributed across the 6 countries; 8 from Cameroon, 3 from Gabon, 2 from Republic of Congo and Central African Republic respectively, and 1 each from the Democratic Republic of Congo and the Republic of Chad (Table 1).
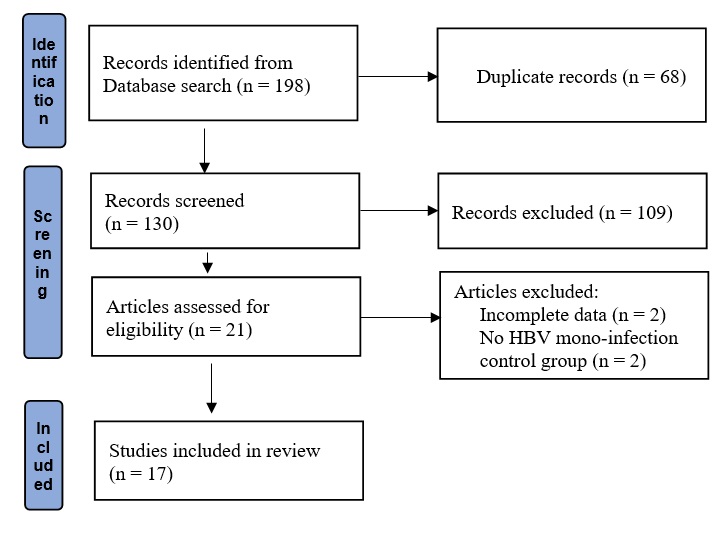
Fig. 1. Flow diagram of the selection of studies.
| Country | Authors | Year |
| Cameroon | Foupouapouognigni et al. | 2011 |
| Torimiro et al. | 2014 | |
| Amougou et al. | 2016 | |
| Luma et al. | 2017 | |
| Butler et al. | 2018 | |
| Bessombes et al. | 2019 | |
| Noubissi-Jouegouo et al. | 2019 | |
| Foupouapouognigni et al. | 2022 | |
| Gabon | Makuwa et al. | 2009 |
| Francois-Souquiere et al. | 2015 | |
| Groc et al. | 2019 | |
| Republic of Congo | Mongo-Onkouo et al. | 2018 |
| Mokono et al. | 2021 | |
| Central African Republic | Bekondi et al. | 2009 |
| Basimane-Bisimwa et al. | 2022 | |
| Democratic Republic of Congo | Kabamba et al. | 2020 |
| Republic of Chad | Mousa et al. | 2022 |
Table 1. Selected studies according to country and year of publication.
Characteristics of the Selected Studies
Most articles were cross-sectional studies while five were case control studies and two were cohort studies. Four studies were conducted in rural settings, three in both rural and urban settings and the rest in urban settings. Patients co-infected with human immunodeficiency virus (HIV) and/or HCV were excluded in two studies while five studies included them in their analysis as a tool for comparing their impact on liver disease to that of HBV and HDV, hence there was a clear distinction between them and HBV-HDV infected patients. The remaining studies did not mention anything about HIV and/or HCV co-infected patients. In addition, most articles also took into consideration confounding factors for the risk of developing HCC such as age, gender, alcohol, smoking, chemicals and other comorbidities to confirm results.
Every selected study included patients with HBV mono-infection and HBV-HDV dual infection, and almost all estimated the prevalence of HDV. Two of the studies included information on the stage of liver disease in mono-infection and dual infection respectively, six included information about the level of liver enzymes in both mono-infected and dual infected sera while three reported both. Fourteen studies used both serologic (antibody and antigen detection) and molecular (DNA and RNA detection) methods to determine infection while three used only serologic methods. Eight studies included the molecular characterization of HDV and the viral loads while two included viral loads but not molecular characterisation, but none mentioned the rate of HBsAg clearance nor indicated if the patients were on any treatment.
Estimating the Prevalence of Hepatitis Delta
The 17studies included in this analysis enrolled 7805 HBsAg positive patients amongst which 2223 were HBV-HDV dual infected and 5582 were HBV mono-infected [24]– [40]. From our analysis, the prevalence of hepatitis D was 0.28(95% CI: 0.20 to 0.36), hence a prevalence of 28%. Most studies provided large sample sizes, making most confidence intervals less stretched. As predicted, there was high heterogeneity (I2= 98.89%, P< 0.001) amidst the studies due to variation in population, population sizes and geographical location (Figure 2).
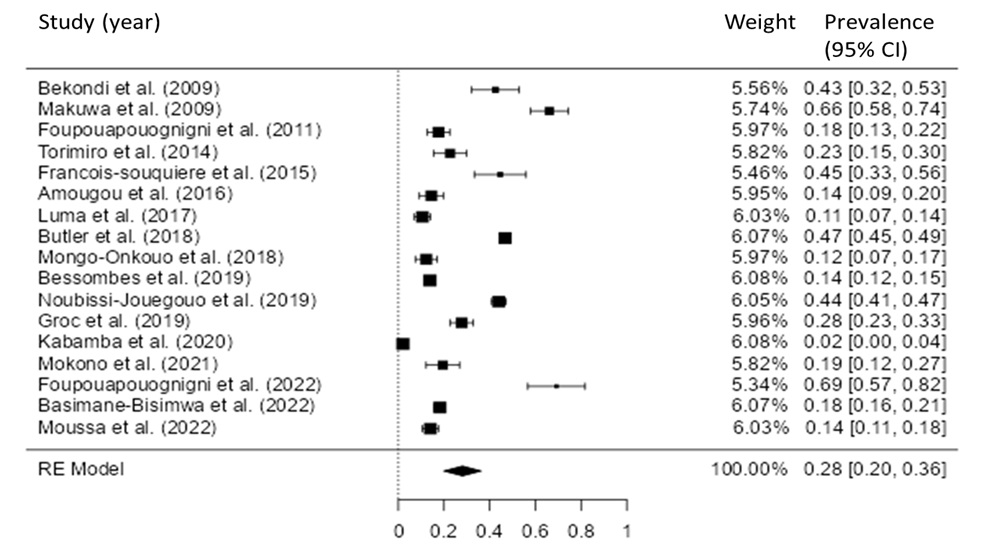
Figure 2. Forest plot for the prevalence of HDV.
Comparing the Risk of HCC Between HBV-HDV Dual Infection and HBV Mono-infection
There were five studies in which the stage of liver disease (fibrosis, cirrhosis or HCC) in both dual and mono-infected patients was included, comprising 1060 patients; 175 people with HBV-HDV dual infection amongst which 67 had liver disease and 108 did not; 761 people with HBV mono-infection amongst which 140 had liver disease and 621 did not; 124 people who could not be included as cases in this analysis due to the influence of other infections such as HIV and HCV(24,27,29,30,40). The HBV-HDV dual infection group had a higher risk of HCC (OR: 0.82 [95% CI: -0.01 to 1.65]). The Q-test for heterogeneity was not significant, but some heterogeneity may still be present in the true outcomes (Q [4] = 7.8765, p = 0.0962, tau² = 0.4531, I² = 55.5452%). An examination of the studentized residuals revealed that none of the studies had a value larger than ± 2.5758 and hence there was no indication of outliers in the context of this model (Figure 3A). According to the Cook’s distances, none of the studies could be considered to be overly influential. Neither the rank correlation nor the regression test indicated any funnel plot asymmetry (p = 0.2333 and p = 0.0904, respectively) as shown in figure 3B.
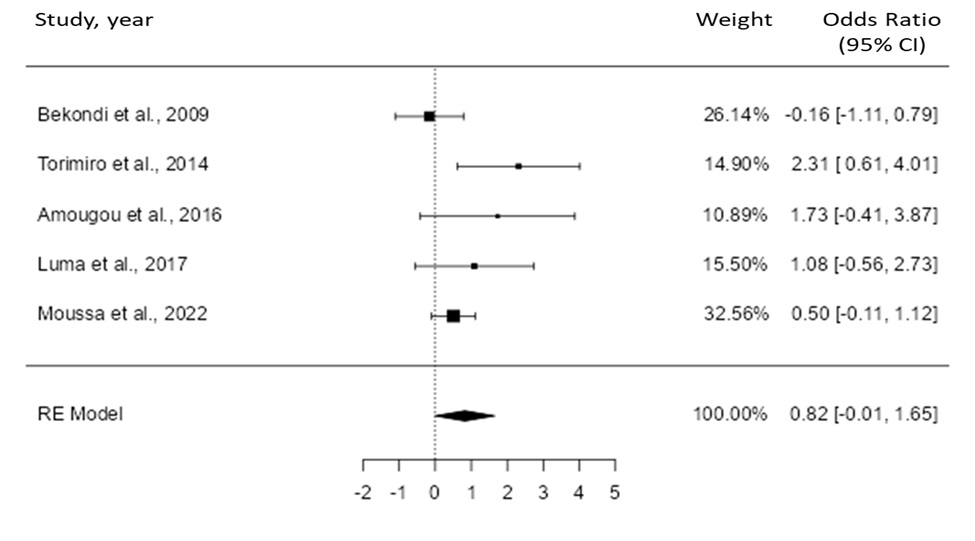
Figure 3A. Comparison of the risk of HCC between HBV-HDV dual infection and HBV mono-infection.
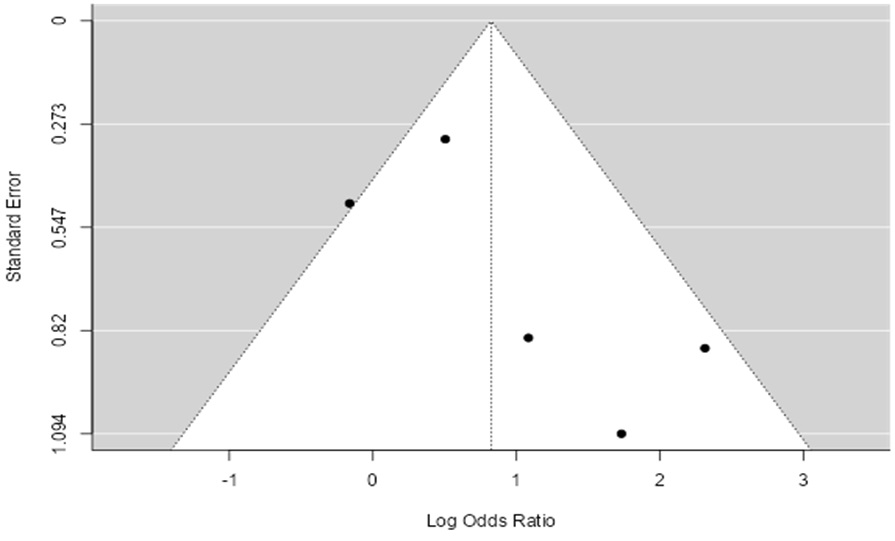
Figure 3B. Funnel plot for assessment of publication bias.
Liver Disease (Fibrosis, Cirrhosis, HCC) Detection Method
The five studies involved in the diagnosis of liver disease used various methods in order to reach their conclusion. The most used method was the Fibro Test/Acti Test which has four levels of detection; F1 (portal and periportal fibrosis without septa), F2 (portal and periportal fibrosis with rare septa), F3 (numerous septa without cirrhosis) and F4 (cirrhosis). One study did histologic analyses of liver biopsies, another used soft tissue aspirated through cytopuncture for cytopathologic analyses, and the final study did liver mass ultrasound followed by liver biopsy. Every method used was explicitly described by the authors using them. In the situation in which an adaptation or modification of the original operating procedure was deemed necessary, the authors gave adequate explanations.
HDV Genotype Distribution
Hepatitis D virus RNA was tested in 10 studies, among which 8 performed genetic analyses. Genetic profiling was done in 4 out of the 9 central African countries; 3 studies in Cameroon, 1 in Central African Republic, 1 in the Republic of Congo, and 3 in Gabon. HDV-1 was prominent in all 4 countries, HDV-5 in Cameroon and Republic of Congo, HDV-6 only in Cameroon, HDV-7 in Cameroon and Gabon, and HDV-8 in all 4 countries (Table 2A). A total of 395 samples were included in the HDV genotype analysis. Hepatitis D virus genotype 1 (HDV-1) was the most prominent (66.84%; 264/395) of all genotypes, distantly followed by HDV-7 (19.24%; 76/395) and HDV-8 (8.86%; 35/395). HDV-6 had a very low outcome (3.03%; 12/395) and HDV-5 was the least represented (0.51%; 2/395). Some samples (1.52%; 6/395) showed undetectable levels of HDV RNA and so the HDV genotypes of these could not identified (Table 2B).
DISCUSSION
Prevalence of HDV
We obtained a prevalence of 28% for hepatitis D in HBV infected populations of central Africa. In 2017, Stockdale et al. (10) obtained a prevalence of 26% for Hepatitis D among hepatitis B patients in central Africa. In their review, data was extracted from a total of 7 studies obtained from just two central African countries. More to that, the studies they used were performed between 2007 and 2015. On the other hand, our study extracted data from a total of 17 studies representing six central African countries, and the studies were performed between 2009 and 2022. Our results may be more representative of central Africa and possibly an update to what Stockdale et al. obtained. Miao et al. (41) also obtained a HDV prevalence of 26% in the HBsAg positive population of central Africa. Their findings also included the fact that Africa is the world’s second most endemic area for HDV after Asia.
Hepatitis D is continuously spreading in sub-Saharan Africa in part due to the high endemicity of HBV (4), which is in part as a result of non-adherence to or unfinished birth dose immunization, inadequate follow-up care, and difficult access to antiviral therapy. These can only build an environment where HDV can thrive and put the prevalence of hepatitis D on the rise. The prevalence of hepatitis D among hepatitis B patients in central Africa has the tendency to exceed by far the worldwide prevalence as raised up by Stockdale et al. in 2017. Chen et al. (20) obtained a worldwide prevalence for hepatitis D among hepatitis B patients of 15% and Miao et al. (41) obtained a worldwide prevalence of 13%. From these results we can confidently say that the prevalence of HDV in central Africa contributes quite substantially to the global prevalence.
Elevated Risk of Developing HCC in Dual Infection
There is still considerable debate on whether and how HDV increases the risk of developing HCC in patients with HBV infection. However, the results of this meta-analysis are in favour of the fact that HBV-HDV dual infection brings about a higher risk of developing HCC. This risk is not as apparent where the comparison is among patients confirmed with liver disease (fibrosis, cirrhosis or HCC). It should be noted that the gold standard for the diagnosis of HCC is histology, specifically using magnetic resonance imaging (MRI) (42). In the African context, access to HCC diagnosis is very limited. This could be the reason why only a few studies ventured in diagnosing liver disease. Nevertheless, the results we obtained matches those obtained in other studies.
Chang et al. (43) successfully demonstrated that there is higher risk for HCC in HBV-HDV dual infected patients. The difference between our meta-analysis and theirs resides in the search strategy and selection criteria. The contrariety in the number of studies included can definitely produce different results in the analysis, as our analysis included five studies while theirs included 21. In our study we focused solely on the consequence of an HBV-HDV dual infection on the progression of liver disease, be it a co-infection or a superinfection, and we made sure that other essential liver disease enhancers such as HIV and HCV do not derail us from that focus. While in their study, the also specified how an HDV superinfection causes faster damage to the liver than an HBV-HDV co-infection. They went further into subgroup analyses of different aspects such as fibrosis stage and various ethnic groups. Kamal et al. (44) found a similar result as they found a 2-fold increase in the risk of developing HCC with HBV-HDV dual infection as compared to HBV mono-infection. Despite the fact that the aim was the same, their study was quite different from ours as they considered only longitudinal studies that granted them the possibility to include temporality when assessing the risk of HCC development with HDV. Their review and analyses show that people with HBV-HDV dual infection develop severe liver complications in a shorter time and more aggressively than people with HBV mono-infection.
Distribution of HDV Across Central African Populations
Recruitment of participants was generally done at regional or district hospitals and in research laboratories in urban areas, and was done in health centres, homes and during health campaigns in rural areas. Of the 7805 patients recruited, 3523 were from urban areas within which 23.9% (841/3523) had HBV-HDV dual infection, 609 were from rural areas with 28.7% (175/609) having dual infection and 3673 were recruited at random from both urban and rural areas with 32.9% (1207/3673) having dual infection. Following these, we can conclude that HDV is more common in rural settings. Stockdale et al. (10) also arrived the same conclusion in which HDV was significantly higher in rural areas than in urban areas. There are a number of recurring explanations for this across the studies we used. Besombes et al. (33) noted an intra-household clustering of HDV infection. In their study, in households where there were three to four HBV-infected members, introducing HDV led to co-infection with HDV in almost all HBV-infected household members. They performed logistic regression analyses and were able to discover a ninefold increased risk of HDV in HBV carriers in a household where at least one HDV seropositive individual was present. Other meaningful explanations equally noted across the studies included in this review include; inadequately equipped health facilities in most rural areas, non-availability of screening centres ad of qualified medical personnel, inadequate follow up of cases when detected. These are mostly due to the difficulties in implementing strategies such as difficult access to many areas, especially by land, and the stoicity of governments concerned.
Hepatitis D Genotypes Present in Central Africa
Human HDV genomes have a large biodiversity and quite rapid evolution. This is very much linked to the highly operational HDV recombination. The presence of HDV-1 and HDV-5 to 8 in Central Africa as our results reveal is in accordance with what Netter et al. (45) had as result concerning Africa in general. Another study also revealed similar results to ours, showing that genotypes 1, 5, 6, 7 and 8 are endemic in Africa with HDV-1 being the most common (46).Central Africa is said to be the principal zone of diversification of HDV. The most pathogenic known form of hepatitis delta virus genotypes (HDV-3) is not prevalent in Africa. Whereas the next most pathogenic genotype (HDV-1) is most prevalent in Africa, especially central Africa (47). It is already known that HDV-1a and HDV-1b are the most common HDV-1 subgenotypes in Africa, hence are most likely what predominate in central Africa.HDV-1 has been shown to have greater efficiencies in assembly and replication as compared to the other genotypes present in central Africa, and this ability leads to a faster and more aggressive HDV virion assembly and propagation (48,49). Alongside the lack of proper detection and care, this ability is definitely a key reason why HDV-1 is the most common hepatitis D genotype in central Africa.
HDV Persistence
Chronic hepatitis has been considered a silent killer due to its nature and course, and a neglected killer due to the slothfulness of stakeholders and policy makers. Several years ago it was forecasted that the burden of liver disease in Africa would increase, principally due to inappropriate disease surveillance, lack of tools to assess liver disease, and underestimated needs for human and financial resources (50). In order to achieve effective eradication of viral hepatitis, especially that caused by HDV, regional prevalence and epidemiology of HBV and HDV must be known such that prevention and treatment strategies can be implemented (51). It has been estimated that 5% of people with hepatitis B virus also have hepatitis D. Most of these people end up with chronic HBV-HDV co-infection and develop liver cirrhosis, liver failure and quite expectedly, hepatocellular carcinoma. This disease course most often takes 5–10 years (52). Although there exist therapies that can control HBV and possibly eradicate it, treatments with efficacy in HDV treatment are still under active investigation.
Current and Potential Treatments Options for Hepatitis D
For a good number of years interferon-alpha (IFN-α [subtype 2a and 2b]) was the sole drug used in treating patients with chronic hepatitis D. Unfortunately, most patients did not remain RNA negative six months after treatment, and more to that, relapse occurred 39 months later (53). Years after, several pilot studies were conducted for the evaluation of interferon (IFN) and pegylated-IFN (Peg-IFN) efficiency in HDV-infected patients. Peg-IFN-α was more effective than standard IFN-α even though it still was not able to eliminate HDV in most patients (54). Certain studies pointed out the fact that treatment extension for, let’s say a period of 2 years with standard IFN-α or even 5 years with Peg-IFN-α produced no significant improvement on response rates. Meanwhile other studies demonstrated that prolongation of IFN treatment increased efficacy. Nonetheless, long-term follow up showed high relapse rates (55). Soriano et al. (56) in their study, focused entirely on bulevirtide (BLV) as a treatment for hepatitis D. According to their results, identifying NTCP as cell surface receptor for both HDV and HBV entry in hepatocytes led to the discovery of BLV which inhibits HDV and HBV binding by inhibitory competition. In combination with Peg-INF or as a monotherapy, BLV shows evident antiviral activity and is well tolerated. In their randomized trial, Wedemeyer et al. (57) demonstrated that BLV successfully reduced HDV RNA and ALT levels by 48 weeks of treatment in patients with chronic hepatitis D. Their results also showed that HBsAg levels were not affected after 48 weeks of treatment with BLV. Both studies show that BLV effectively prevents HDV and HBV from penetrating hepatocytes, thus clearing HDV and leaving HBsAg at the disposal of the immune system. It is very important for the fight against HDV to access new molecular insights into key determinants of HDV persistence and accelerated the development of antivirals that are capable of interfering with the replication cycle of HDV.
Strategies for Preventing Hepatitis D in Central Africa
Upcoming research on viral hepatitis will have to include the evaluation of innovative testing strategies, the validation of simplified methods to diagnose liver cirrhosis and hepatocellular carcinoma, and the monitoring of long-term treatment outcomes and toxicity. Added to these, there is an urgent need to conceive national plans for the elimination of HBV mother-to-child transmission. This includes effective ways of testing pregnant women, treating those who are eligible, and ensuring birth dose vaccination is received by all new-borns. It’s a shame that current proposals on how to manage and monitor chronic viral hepatitis rely mainly on data obtained outside low and middle income settings. Elimination of viral hepatitis at the global level will only be accomplished provided prevention, testing, and treatment strategies specific to low and middle-income countries are implemented. There is high need for scalable and cost-effective interventions, but these can only be obtained if dedicated research initiatives are undertaken (58).
The problems faced in central Africa in the fight against viral hepatitis are quite similar across the whole of sub-Saharan Africa. Given that HDV can only infect in the presence of HBV, working towards the complete eradication of HBV will eventually mean eradication of HDV. Greenhalgh and Klug (59) demonstrated that complete vaccination against HBV at a certain rate will lead to both HBV and HDV elimination. Vaccination strategies have been put in place in many sub-Saharan African countries for a good number of years now. Apart from vaccination, treatments (antiviral therapies) for HDV and HBV also form part of the overall strategy. The next step following the putting in place of strategies is monitoring of the said strategies, a very important and crucial step. This step has proven to be the most difficult step in the African context.
SUMMARY AND LIMITATIONS
Our analysis provides an estimate of the epidemiology of hepatitis D virus infection in central Africa and an evaluation of the risk of HCC in an HDV-HBV dual infection. These are accompanied by an examination and explanation for the continuously increasing presence of HDV. All these highlight several gaps in knowledge and points to consider in future research. There is high need for systematic epidemiological data collection across central Africa. The true incidence of HCC due to HDV is currently underestimated, and to overcome this, imaging diagnostic modalities and population-based cancer registries are required so as to provide suitable data. The result of this is will enable medical personnel and policy makers will take appropriate public health decisions, allocate resources properly and formulate management guidelines specific for HDV-HBV patients of central Africa or sub-Saharan Africa as a whole.
There were a number of limitations to our meta-analysis; (1) Most of the studies did not mention the status of HIV and HCV infection, (2) Hepatitis B and D viral loads were not assessed in most of the studies. This could have permitted us to have more accurate numbers of inactive HDV carriers, (3) The HBsAg clearance rate was not mentioned in the selected studies meaning we could not determine whether the risk of HCC remains high in an HBV suppressed environment or not.
CONCLUSION
There are several postulates for the mechanism through which HDV increases the risk for HCC in HBV infected patients, but there is still a lot to understand about it. Nonetheless HDV does increase the risk of HCC as compared to HBV mono-infection. The prevalence of HDV is very high amongst HBV patients of central Africa and will probably increase with time primarily due to the fact that hepatitis B remains endemic. There is need for improvement in the implementation of preventive measures against HBV such as Vaccination and expansion of medical facilities for the diagnosis and treatment of HBV. These will help a great deal in preventing both HDV and HBV.
REFERENCES
- Mak D, Kramvis A. Epidemiology and aetiology of hepatocellular carcinoma in sub-saharan africa. Hepatoma Res. 2021;7.
- NIH N cancer institute. Liver Cancer Causes, Risk Factors, and Prevention. NIH – Natl cancer Inst [Internet]. 2022;1–12. Available from: https://www.cancer.gov/types/liver/what-is-liver-cancer/causes-risk-factors#:~:text=Chronic alcoholism and chronic hepatitis, risk factor for liver cancer.
- D’souza S, Lau KCK, Coffin CS, Patel TR. Molecular mechanisms of viral hepatitis induced hepatocellular carcinoma. World J Gastroenterol. 2020;26(38):5759–83.
- WHO AFRO. 91 million Africans infected with Hepatitis B or C | WHO | Regional Office for Africa. 2022;1–5. Available from: https://www.afro.who.int/news/91-million-africans-infected-hepatitis-b-or-c
- Sonderup MW, Dusheiko G, Desalegn H, Lemoine M, Tzeuton C, Spearman CW. Hepatitis B in sub-Saharan Africa — How many patients need therapy? 2020;(November 2019):560–7.
- Muhammad H, Tehreem A, Hammami MB, Ting PS, Gurakar A, Idilman R. Hepatitis D virus and liver transplantation: Indications and outcomes. World J Hepatol. 2021;13(3):291–9.
- Farci P, Niro GA, Zamboni F, Diaz G. Hepatitis d virus and hepatocellular carcinoma. Viruses. 2021;13(5).
- Costante F, Stella L, Santopaolo F, Gasbarrini A, Pompili M, Asselah T, et al. Molecular and Clinical Features of Hepatocellular Carcinoma in Patients with HBV-HDV Infection. J Hepatocell Carcinoma. 2023; Volume 10:713–24.
- Stockdale AJ, Kreuels B, Henrion MYR, Giorgi E, Kyomuhangi I, de Martel C, et al. The global prevalence of hepatitis D virus infection: Systematic review and meta-analysis. J Hepatol [Internet]. 2020;73(3):523–32. Available from: https://doi.org/10.1016/j.jhep.2020.04.008
- Stockdale AJ, Chaponda M, Beloukas A, Phillips RO, Matthews PC, Papadimitropoulos A, et al. Prevalence of hepatitis D virus infection in sub-Saharan Africa: a systematic review and meta-analysis. Lancet Glob Heal [Internet]. 2017;5(10): e992–1003. Available from: http://dx.doi.org/10.1016/S2214-109X(17)30298-X
- Tseligka ED, Clément S, Negro F. Hdv pathogenesis: Unravelling ariadne’s thread. Viruses. 2021;13(5).
- Zhang Z, Urban S. Review New insights into HDV persistence: The role of interferon response and implications for upcoming novel therapies. J Hepatol [Internet]. 2021;74(3):686–99. Available from: https://doi.org/10.1016/j.jhep.2020.11.032
- Turon-lagot V, Saviano A, Schuster C, Baumert TF, Verrier ER. Targeting the Host for New Therapeutic Perspectives in Hepatitis D. 2020;
- Romeo R, Petruzziello A, Pecheur EI, Facchetti F, Perbellini R, Galmozzi E, et al. Hepatitis delta virus and hepatocellular carcinoma: an update. 2018;
- Kohsar M, Landahl J, Neumann-Haefelin C, Schulze zur Wiesch J. Human hepatitis D virus-specific T cell epitopes. JHEP Reports [Internet]. 2021;3(4):100294. Available from: https://doi.org/10.1016/j.jhepr.2021.100294
- Urban S, Neumann- C, Lampertico P. Hepatitis D virus in 2021: virology, immunology and new treatment approaches for a difficult- treat disease. 2021;1782–94.
- Taylor JM. Hepatitis D Virus Replication. 2015;1–13.
- Iris E. Andernacha, Lukas V. Leissa, Zekiba S. Tarnagdab, Marc C.Tahitab, Jesse A. Otegbayoc, Joseph C. Forbid, Sunday Omilabue, Ionela Gouandjika-Vasilachef, Narcisse P. Komasf, Okwen P. Mbahg and CPM. Characterization of Hepatitis Delta Virus in Sub-Saharan Africa. J Clin Microbiol. 2014;(March).
- Le Gal F, Brichler S, Drugan T, Alloui C, Roulot D, Pawlotsky JM, et al. Genetic diversity and worldwide distribution of the deltavirus genus: A study of 2,152 clinical strains. Hepatology. 2017;66(6):1826–41.
- Chen H, Shen D, Ji D, Han P, Zhang W, Ma J, et al. Prevalence and burden of hepatitis D virus infection in the global population : a systematic review and meta-analysis. 2019;512–21.
- Spearman CW, Afihene M, Ally R, Apica B, Awuku Y, Cunha L, et al. Hepatitis B in sub-Saharan Africa: strategies to achieve the 2030 elimination targets. Lancet Gastroenterol Hepatol. 2017;2(12):900.
- Sonderup MW, Spearman CW. Global Disparities in Hepatitis B Elimination—A Focus on Africa. Viruses. 2022;14(1).
- Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Hoffmann C, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews Systematic reviews and Meta-Analyses. 2021;
- Bekondi C, Mobima T, Ouavènè JO, Koffi B, Konamna X, Béré A, et al. Étiopathologie du carcinome hépatocellulaire à Bangui, République centrafricaine: Caractéristiques cliniques, biologiques et aspects virologiques des patients. Pathol Biol. 2010;58(2):152–5.
- Makuwa M, Mintsa-ndong A, Souquie S, Leroy EM, Kazanji M. Prevalence and Molecular Diversity of Hepatitis B Virus and Hepatitis Delta Virus in Urban and Rural Populations in Northern Gabon in Central Africa ᰔ. 2009;47(7):2265–8.
- Foupouapouognigni Y, Noah DN, Sartre T, Njouom R. High Prevalence and Predominance of Hepatitis Delta Virus Genotype 1 Infection in Cameroon ᰔ. 2011;49(3):1162–4.
- Torimiro J, Monamele G, Kowo M, Takou D, Pouokam G-B, Fokam J, et al. Co-Infection of Hepatitis B Virus and Hepatitis Delta Virus in Yaounde-Cameroon. Br Microbiol Res J. 2014;4(12):1381–91.
- François-souquière S, Makuwa M, Bisvigou U, Kazanji M. Epidemiological and molecular features of hepatitis B and hepatitis delta virus transmission in a remote rural community in central Africa. MEEGID [Internet]. 2015; Available from: http://dx.doi.org/10.1016/j.meegid.2015.12.021
- Amougou MA, Noah DN, Moundipa PF, Pineau P, Njouom R. A prominent role of Hepatitis D Virus in liver cancers documented in Central Africa. BMC Infect Dis [Internet]. 2016;16(1):1–8. Available from: http://dx.doi.org/10.1186/s12879-016-1992-2
- Luma HN, Eloumou SAFB, Okalla C, Donfack-Sontsa O, Koumitana R, Malongue A, et al. Prevalence and Characteristics of Hepatitis Delta Virus Infection in a Tertiary Hospital Setting in Cameroon. J Clin Exp Hepatol. 2017;7(4):334–9.
- Butler EK, Rodgers MA, Coller KE, Barnaby D, Krilich E, Olivo A, et al. High prevalence of hepatitis delta virus in Cameroon. Sci Rep [Internet]. 2018;(June):1–9. Available from: http://dx.doi.org/10.1038/s41598-018-30078-5
- Mongo-Onkouo A, Okombi RI, Boumba A, Niama FR. Seroprevalence and Molecular Biodiversity of Hepatitis B and Delta Virus Infections in the Republic of Congo. 2018;448–54.
- Besombes C, Njouom R, Paireau J, Lachenal G, Texier G, Tejiokem M, et al. The epidemiology of hepatitis delta virus infection in Cameroon. 2020;1–7.
- Jouegouo LN, Atsama MA, Alain P, Ngoupo T, Monamele CG, Ngono L, et al. Evolutionary trends in the prevalence of anti ‑ HDV antibodies among patients positive for HBsAg referred to a national laboratory in Cameroon from 2012 to 2017. BMC Res Notes [Internet]. 2019;1–6. Available from: https://doi.org/10.1186/s13104-019-4460-4
- Groc S, Abbate JL, LeGal F, Gerber A, Tuaillon E, Albert J-L, et al. High Prevalence and Diversity of Hepatitis B and Hepatitis Delta Virus in Gabon. J Viral Hepat. 2019;26(1):33.
- Kabamba AT, Mwamba CM, Nyembo CM, Kabamba BM. Séroprévalence de l’ hépatite D chez les personnes atteintes d’ hépatite B chronique à Lubumbashi (RDC ) Hepatitis D Seroprevalence in people with chronic hepatitis B in Lubumbashi (DRC ). 2020;14(December):3110–6.
- Mokono SO, Mbani CJ, Angounda BM, Bakoua BS, Mbao-bongo SR, Nanitelamio EPL, et al. Prevalence and Risk Factors for Hepatitis Delta Virus Transmission among HBsAg Positive Blood Donors in Brazzaville, Congo. 2021;43–50.
- Foupouapouognigni Y, Delors J, Mfonkou T, Boyomo O, Gessain A, Njouom R. Endemicity and genetic diversity of Hepatitis delta virus among Pygmies in Cameroon, Central Africa. BMC Res Notes [Internet]. 2022;1–5. Available from: https://doi.org/10.1186/s13104-022-05976-7
- Basimane-bisimwa P, Demi-sibiro OA, Zemingui-bambete PII, Gal F Le. Molecular characterization of hepatitis delta virus strains isolated from patients at the Institut Pasteur de Bangui, Central African Republic, 2014 – 2017. 2022;2014–7.
- Moussa AM, Saleh TM, Habkreo M, Nadlaou B, Ngare AA, Stanislas DA, et al. Prevalence and Predictors of Viral Hepatitis D Co-Infection in Chronic HbsAg Carriers. 2022;213–20.
- Miao Z, Zhang S, Ou X, Li S, Ma Z, Wang W, et al. Estimating the Global Prevalence, Disease Progression, and Clinical Outcome of Hepatitis Delta Virus Infection. 2020; 221:1677–87.
- Parra NS, Ross HM, Khan A, Wu M, Goldberg R, Shah L, et al. Advancements in the Diagnosis of Hepatocellular Carcinoma. Int J Transl Med. 2023;3(1):51–65.
- Chang T, Su C, Huang Y, Huang Y, Hou M. Hepatitis D virus dual infection increased the risk of hepatocellular carcinoma compared with hepatitis B virus mono infection : A meta-analysis. J Chinese Med Assoc. 2022; 85:30–41.
- Kamal H, Fornes R, Simin J, Stål P, Duberg AS, Brusselaers N, et al. Risk of hepatocellular carcinoma in hepatitis B and D virus co-infected patients: A systematic review and meta-analysis of longitudinal studies. J Viral Hepat. 2021;28(10):1431–42.
- Netter HJ, Barrios MH, Littlejohn M, Yuen LKW. Hepatitis Delta Virus (HDV) and Delta-Like Agents: Insights Into Their Origin. Front Microbiol. 2021;12(June):1–12.
- Sharafi H, Rezaee-Zavareh MS, Miri SM, Alavian SM. Global distribution of hepatitis d virus genotypes: A systematic review. Hepat Mon. 2020;20(2).
- Da BL, Heller T, Koh C. Hepatitis D infection: From initial discovery to current investigational therapies. Gastroenterol Rep. 2019;7(4):231–45.
- Ahn J, Gish RG. Hepatitis D virus: A call to screening. Gastroenterol Hepatol. 2014;10(10):647–86.
- Chiou WC, Lu HF, Chen JC, Lai YH, Chang MF, Huang YL, et al. Identification of a novel interaction site between the large hepatitis delta antigen and clathrin that regulates the assembly of genotype III hepatitis delta virus. Virol J [Internet]. 2022;19(1):1–9. Available from: https://doi.org/10.1186/s12985-022-01866-3
- Lemoine M, Eholié S, Lacombe K. Review Reducing the neglected burden of viral hepatitis in Africa: Strategies for a global approach. 2014;xxx:4–11.
- Ceesay A, Bouherrou K, Tan BK, Lemoine M, Ndow G, Testoni B, et al. Viral Diagnosis of Hepatitis B and Delta: What We Know and What Is Still Required? Specific Focus on Low- and Middle-Income Countries. Microorganisms. 2022;10(11).
- Urban S, Neumann-Haefelin C, Lampertico P. Hepatitis D virus in 2021: Virology, immunology and new treatment approaches for a difficult-to-treat disease. Gut. 2021;70(9):1782–94.
- Farci P, Roskams T, Chessa L, Peddis G, Mazzoleni AP, Scioscia R, et al. Long-term benefit of interferon α therapy of chronic hepatitis D: Regression of advanced hepatic fibrosis. Gastroenterology. 2004;126(7):1740–9.
- Alavian SM, Tabatabaei SV, Behnava B, Rizzetto M. Standard and pegylated interferon therapy of HDV infection: A systematic review and meta- analysis. J Res Med Sci. 2012;17(10):967–74.
- Wu F, Wang Y, Cui D, Tian Y, Lu R, Liu C, et al. Short-Term Peg-IFN α-2b Re-Treatment Induced a High Functional Cure Rate in Patients with HBsAg Recurrence after Stopping Peg-IFN α-Based Regimens. J Clin Med. 2023;12(1):0–13.
- Soriano V, Moreno-Torres V, Treviño A, Corral O, de Mendoza C. Bulevirtide in the Treatment of Hepatitis Delta: Drug Discovery, Clinical Development and Place in Therapy. Drug Des Devel Ther. 2023; Volume 17(January):155–66.
- Lampertico P, Degasperi E, Sandmann L, Wedemeyer H, Yurdaydin C, Roulot D, et al. Hepatitis D Virus Infection: Pathophysiology, Epidemiology and Treatment. Report from the first International Delta Cure Meeting 2022. JHEP Reports. 2023;100818.
- Jaquet A, Muula G, Ekouevi DK, Wandeler G. Elimination of Viral Hepatitis in Low and Middle-Income Countries: Epidemiological Research Gaps. Curr Epidemiol Reports. 2021;8(3):89–96.
- Greenhalgh S, Klug A. Hepatitis B and D: A Forecast on Actions Needed to Reduce Incidence and Achieve Elimination. SPORA A J Biomath. 2022;1–25.