The Status of Health Professionals’ Knowledge of Complications of Impaired Deglutition among Acute-Care Inpatients in a Kenyan Referral Hospital
- Ndiema Dalphine C.
- Abuom T., Karia M.
- 195-205
- Jun 7, 2024
- Health
The Status of Health Professionals’ Knowledge of Complications of Impaired Deglutition among Acute-Care Inpatients in a Kenyan Referral Hospital
Ndiema Dalphine C., Abuom T., Karia M.
Department of Early Childhood Studies and Special Needs Education (Speech-Language Pathology), Kenyatta University, Nairobi City County, Kenya
DOI: https://doi.org/10.51584/IJRIAS.2024.905017
Received: 20 April 2024; Revised: 05 May 2024; Accepted: 11 May 2024; Published: 07 June 2024
ABSTRACT
Early dysphagia screening and identification are vital for improved clinical outcomes for patients with impaired deglutition. The Interprofessional Collaboration model advocates for a collective approach to dysphagia management to facilitate early dysphagia screening and identification. Such collaboration requires all health professionals involved in management of impaired deglutition to have a high awareness of its symptoms and signs, risk factors, and associated complications. However, there is limited research on dysphagia awareness among health professionals in Kenya. This paper reports on a study to establish health professionals’ awareness levels of oropharyngeal dysphagia-associated complications among adult inpatients in the medical and surgical wards (Acute Care Facility-ACF) of a National referral hospital in Kenya. The study employed a descriptive, cross-sectional design. Questionnaires were administered to an initial sample of 19 health professionals attending to adult inpatients in the ACF. Sixteen (16) of the sampled professionals completed and returned the questionnaires and were included in the final analyses. Awareness levels were assessed using a ten-item questionnaire and analyzed using frequencies, percentages, and means. The independent samples t-test and one-way ANOVA were used to compare the scores across selected individual characteristics. The mean proportion of correct responses to the questionnaire items was 73.0% (SD = 17.49), indicating that, on average, participants had moderate awareness of oropharyngeal dysphagia-associated complications. There were no significant differences in awareness levels due to gender, age, educational attainment, experience, specialization, or training. The findings show that health professionals attending to adult inpatients in the hospital’s medical and surgical units have, on average, moderate awareness of oropharyngeal dysphagia-associated complications.
Keyword: Awareness, complications, interprofessional collaboration, oropharyngeal dysphagia, swallowing/deglutition
INTRODUCTION
Dysphagia (impaired deglutition) screening and identification are recurring topics in healthcare discussions, especially about stroke and other acute or chronic conditions affecting the swallowing process, and for good reasons. According to some estimates, between 40% and 70% of stroke patients experience dysphagia symptoms within three days following stroke (Donovan et al., 2013). Dysphagia is a prevalent condition, particularly among older adults, and is associated with several complications that may inhibit the swallowing process (McHutchion et al., 2022; Rajati et al., 2022). The deglutition pathway plays a vital role in human nutrition while also preventing food from entering the respiratory tract (Nishino, 2013). Given that dysphagia inhibits the deglutition process, it can have adverse effects on nutrition, respiration, and overall health (Adkins et al., 2019; Altman et al., 2010; Bolinger and Dembowski, 2022; Bonilha, 2014).
The specific complications resulting from dysphagia may vary depending on patient characteristics, underlying conditions, and its presentation. Generally, dysphagia symptoms involve the various swallowing stages, including oral, pharyngeal, and esophageal phases (Cook, 2009). This paper focuses on oropharyngeal dysphagia (OPD), which affects the oral transit-pharyngeal stage (Rofes et al., 2011). In their review, Rofes et al. (2011) noted that OPD causes two types of complications in elderly patients. The first type entails decreased deglutition efficacy, leading to dehydration and malnutrition. In the second form, OPD compromises deglutition safety, causing tracheobronchial aspiration and, subsequently, aspiration pneumonia. Dysphagia has also been linked to depression, compromised life quality, and, in extreme cases, death (Verdonschot et al., 2013).
Effective OPD identification and screening strategies are vital to enhance the health outcomes of patients diagnosed with impaired deglutition. Early dysphagia and aspiration risk identification, help avoid the adverse complications that may result from deglutition difficulties (Donovan et al., 2013, Head et al., 2007). Disturbances in saliva management, swallowing, drinking, sucking, chewing, medication intake, and airway protection may cause severe medical manifestations, such as choking, dehydration, malnutrition, aspiration pneumonia, silent aspiration, and mortality risks when these are not easily detected and managed (Matar et al., 2021; Takizawa et al., 2016). Health professionals (HPs) who are familiar with deglutition impairment can promptly identify its symptoms and recommend appropriate interventions. Early dysphagia symptom recognition and appropriate referrals, in turn, minimize the risk of aspiration pneumonia and other complications, like death (Anderle et al., 2018; Matar et al., 2021)
Traditionally, OPD diagnosis and treatment are primarily the role of speech-language pathologists or therapists (SLTs). They assume an essential role in swallowing mechanics by providing services that mostly involve compensatory rehabilitation, muscle strengthening, swallowing maneuvers, and adaptation (Gupta et al., 2022). However, there are growing calls for a collaborative approach to dysphagia management. Logemann (1994), for example, stressed that multidisciplinary dysphagia management facilitates an in-depth appreciation of its underlying etiology and ensures that patients diagnosed with this condition receive optimal assessment and treatment. The need for a collaborative approach is necessitated by the complexity of dysphagia symptoms and the specificity of underlying conditions. On this note, Alagiakrishnan et al. (2013) point out that an interdisciplinary approach is vital for efficient treatment of dysphagia pathology, symptom reduction, nutrition improvement, and aspiration risk reduction. A dysphagia management team could include SLTs, radiologists, gastroenterologists, otolaryngologists, neurologists, occupational therapists, physical therapists, dietitians, nurses, and respiratory specialists (Alagiakrishnan et al., 2013; Logemann, 1994). Fig. 1 summarizes the various roles needed for collaborative OPD management.
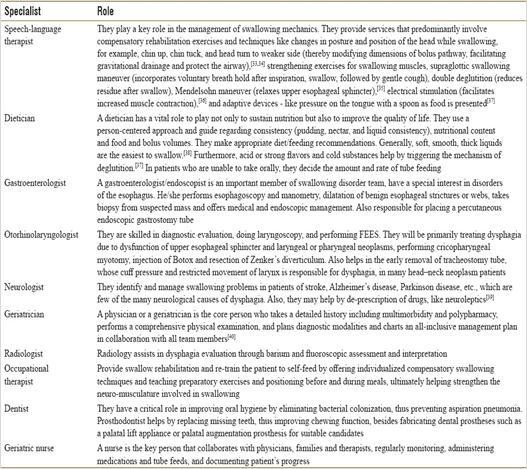
Fig. 1: Health Professionals Involved in Dysphagia Management (Logemann, 1994)
A multi-disciplinary approach to OPD management is consistent with the World Health Organization (WHO)’s Interprofessional Collaboration (IPC) framework. The IPC also advocates for inter-disciplinary cooperation to facilitate knowledge sharing between practitioners in varied specialties (WHO, 2010). The mode stresses the importance of collaboration between HPs to deliver effective and comprehensive care to patients (WHO, 2010). This model is relevant to the current study because of the growing recognition of the need for HPs to collaborate when addressing complex, multifaceted issues, such as OPD (Reeves et al., 2017). By promoting collaboration and communication among diverse healthcare professionals, this model can facilitate effective dysphagia management and ultimately improve patient outcomes. To neutralize the hierarchical interdisciplinary approach, IPC advocates for equitable role-sharing and inclusion of families. Therefore, incorporating this model in OPD management could facilitate holistic care for individuals diagnosed with impaired swallowing.
Effective collaboration in OPD management requires all HPs to be aware of its manifestations, risk factors (Ndiema et al., 2024) and associated complications (Bakhtiyari et al., 2019). Generally, HPs in most healthcare facilities come from different specialties and have varied educational, occupational training, and experience levels. Hence, they may have varied levels of OPD awareness. Indeed, studies from different parts of the globe show that many medical practitioners have either low or moderate dysphagia awareness levels (Anderle et al., 2018; Matar et al., 2021; Takizawa et al., 2016). For example, Anderle et al. (2018) revealed that many nurses in South Brazil were not ready to administer medication to OPD inpatients due to the absence of sufficient guidance on how to care for them. Similarly, Knight et al. (2020) conducted a study in Eastern Cape, South Africa, to clarify how nurses should identify and care for patients with stroke-related OPD. In their sample of 130 nurses, the average OPD complication awareness was estimated to be only 47.3% (low).
In Kenya, there are suggestions that many HPs have low awareness of swallowing disorders due to their low interaction with dysphagia patients (Martino, 2005; Oduor et al., 2015; Omondi et al., 2019). Nevertheless, there is limited research on HPs’ awareness of various OPD parameters, including its associated complications. Addressing this knowledge gap could be an important step toward developing strategies to provide holistic care to OPD patients. To this end, this descriptive, cross-sectional quantitative study aimed to establish HPs’ awareness of OPD among adult inpatients in the medical and surgical wards (acute-care facility) of a level-six (national) hospital in Kenya. Specifically, it assessed HPs’ awareness levels of OPD-associated complications among adult inpatients in the hospital’s acute-care facility (ACF).
The hospital chosen for the study is a referral institution equipped to offer various specialized services, including rehabilitation medicine and acute care. A post practicum clinical-files review conducted in the facility in 2022 revealed that over 60% of initial adult SLT consultations in its ACF presented an OPD diagnosis (Ndiema et al., 2023). Therefore, it was an ideal target for the present research. The study was motivated by the need to establish whether HPs in the facility were prepared to handle patients with swallowing disorders, considering the high presentation of this condition in the hospital’s medical and surgical wards. Using a previously validated ten-item questionnaire and a purposive sample of 16 HPs working in the facility, the study showed that their awareness level of OPD-associated complications was, on average, moderate.
DATA AND METHODS
The study adopted a cross-sectional, descriptive design to assess HPs’ awareness of OPD-associated complications as a basis for developing interventions to improve dysphagia management in Kenya. The setting was a level-six (national) hospital in Nairobi City County, Kenya. The hospital offers specialized rehabilitation medicine, oncology, trauma and orthopaedics, renal, accident and emergency, and other acute care services to a wide range of patients.
Health professionals attending to adult inpatients in the hospital’s medical and surgical wards (acute-care facility) constituted the target population. The HPs involved in dysphagia management in government ACFs in Kenya are from three specific professional groups: medical (medical officers, including specialists like in oncology, radiology, gastroenterology, and neurology), allied health professionals (speech therapists, physiotherapists and nutritionists), and nursing (Rhoda and Pickel-Voight, 2015). There were 63 such HPs at the ACF at the time of the study. For populations less than 10,000, Mugenda and Mugenda (2013) recommend that a sample size 10-30% of the population is sufficient for quantitative surveys. For this study, 30% or 19 of the 63 HPs were sampled. Purposive sampling was used to ensure that only HPs who should be involved in swallowing disorder management were recruited (Ary et al., 2014). Sixteen (16) of the 19 HPs completed and returned the questionnaires and were included in the final sample.
Quantitative methods were used to generate and analyze data. For data collection, a close-ended, multiple-choice questionnaire was administered to the sample. The questionnaire assessed participants’ awareness levels using ten (10) possible complication items. They were to indicate whether or not a complication in the list applied to OPD. The number of correctly identified items was used as a proxy for their awareness levels. The questionnaire also obtained data on participants’ relevant demographic and general information, including gender, age, education attainment, work experience, area of specialization (work units), and whether they had been trained in OPD management. The questionnaires were delivered online through Google Forms following approvals and formal consent from the Kenya National Commission for Science Technology and Innovation (NACOSTI), Ethics Review Committee- Kenyatta University, and the hospital’s individual participants.
The adapted questionnaire used in this study has been validated previously (Rhoda and Pickel-Voight, 2015). A pilot study was conducted in a national referral hospital in Nairobi City County to assess the questionnaire’s validity and reliability. Two experts were constantly consulted to judge the instruments’ relevance, clarity, and adequacy. The instrument was probed, and individual items reviewed to ensure the tools measured the variables under examination. The stability of the questionnaire was established by employing the test-retest procedure within a 15-day window to assess the consistency of the test results (Streiner et al., 2014). Pearson’s product-moment correlation coefficient showed high test-retest reliability (r = 83.4).
The collected data were entered into the Statistical Package for Social Sciences (SPSS) and coded appropriately. Two statistics experts entered and coded the data independently. Their datasets were then compared for inconsistencies, and adjustments were made as appropriate. Raw frequencies, percentages, means, and standard deviations were used to summarize the data and identify key patterns in variables of interest. Independent samples t-test and one-way ANOVA were then used to compare participants’ awareness levels across categories of selected demographic and general characteristic variables. Tests of significance were performed at the 95% confidence level. The findings are presented in the next section.
RESULTS
A. Participant Characteristics
Of the 19 sampled HPs, sixteen (16) completed and returned the questionnaires, translating into an 84.2% return rate. The high return rate was due to persistent follow-up. Their characteristics were as shown in TABLE I.
Table I: Participant Demographic and General Characteristics
| Characteristic | Category | n | % |
| Gender | Male | 8 | 50.0 |
| Female | 8 | 50.0 | |
| Age group | 25-30 years | 6 | 37.5 |
| 31-35 years | 5 | 31.3 | |
| 36-40 years | 5 | 31.3 | |
| Educational attainment | Diploma | 4 | 25.0 |
| Bachelor | 8 | 50.0 | |
| Post-graduate | 4 | 25.0 | |
| Experience | 4-6 years | 5 | 31.3 |
| 7-9 years | 5 | 31.3 | |
| > 9 years | 6 | 37.5 | |
| Specialization | Nurse | 5 | 31.3 |
| Physiotherapist | 7 | 43.8 | |
| Other | 4 | 25.0 | |
| Speech Pathologist present in work unit | No | 1 | 6.3 |
| Yes | 15 | 93.8 | |
| Swallowing disorder training | No | 10 | 62.5 |
| Yes | 6 | 37.5 |
There was an equal number of males and females in the sample. All were aged between 25 and 40 years, with almost equal distribution across 25-30, 31-35, and 36-40 years. Overall, the sample was well-educated and highly experienced. The majority (75%, n = 12) had either a bachelor’s or post-graduate degree, while all had been practicing for at least four (4) years, with over a third having been in their profession for over nine (9) years. Regarding their specialization, the majority were either physiotherapists (43.8%, n = 7) or nurses (31.3%, n = 5). The remaining four included a neurologist, an oncologist, a physiotherapist, an SLT, and a nutritionist. They are represented in the table under the “other” category. All but one mentioned that an SLT was present in their unit. Only a slight majority (62.5%, n = 10) had attended a training program in swallowing disorder management, and 93.8% shared interest in further training in swallowing disorders management.
B. Health Professionals’ Awareness Levels on Oropharyngeal Dysphagia-Associated Complications
The study’s objective was to establish the level of OPD-associated complications awareness among HPs attending to adult inpatients in the hospital’s ACF. Participants were presented with ten (10) possible health complications and asked to select those that applied to OPD during their experience. It was assumed that participants with high awareness levels would identify most or all OPD complications correctly. TABLE II summarizes their responses. For each item, the table displays both raw frequencies (n) and corresponding percentages (in brackets). The last column “N” shows the total number of participants who responded to each item. The maximum possible total is 16.
From the “N” column of TABLE II, seven (7) of the items had less than 16 (the maximum) responses. All participants identified aspiration pneumonia as a complication resulting from OPD. The other items most identified as OPD-associated complications were aspiration (93.8%, n = 15), dehydration (86.7%, n = 13), malnutrition (81.3%, n = 13), and general weakness (80%, n = 12). At the other extreme, sudden heart attack (23.1%, n = 3) was the least selected item. The highest unable-to-decide responses were reported for sudden heart attack (23.1%, n = 3), haematemesis (18.8%, n = 3), and anaphylactic shock (14.3%, n = 2). Overall, the diverse responses may imply that participants had varied awareness levels of OPD-associated complications.
Table II: Responses to the Complication Awareness Items
| Sign or Symptom | Agree,
n (%) |
Undecided,
n (%) |
Disagree,
n (%) |
N |
| Aspiration pneumonia | 14 (100) | 0 (0.0) | 0 (0.0) | 14 |
| General weakness | 12 (80.0) | 1 (6.7) | 2 (13.3) | 15 |
| Digestion problems | 9 (60.0) | 2 (13.3) | 4 (26.7) | 15 |
| Aspiration | 15 (93.8) | 1 (6.3) | 0 (0.0) | 16 |
| Dehydration | 13 (86.7) | 0 (0.0) | 2 (12.5) | 15 |
| Anaphylactic shock (narrow airway, blocking breathing) | 8 (57.1) | 2 (14.3) | 4 (28.6) | 14 |
| Sudden heart attack | 3 (23.1) | 3 (23.1) | 7 (53.8) | 13 |
| Malnutrition | 13 (81.3) | 1 (6.3) | 2 (12.5) | 16 |
| Haematemesis (vomiting blood) | 7 (43.8) | 3 (18.8) | 6 (37.5) | 16 |
| Increased mortality (death of a patient) | 11 (73.3) | 1 (6.7) | 3 (20.0) | 15 |
Participants’ awareness levels were then assessed by isolating correct responses. For each participant, an awareness level was computed based on the number of correct as a percentage of the total number of items (10). One participant responded to only two items. Hence, their record was removed in this analysis, leaving only 15 participants. The mean score after deleting this participant’s record was 64.7% (SD = 21.00). In other words, on average, each participant responded correctly to 64.7% of the questions. The study used the following scheme to categorize awareness levels: 0–25% = very low, 26-50% = low, 51-75% = moderate, and > 75% = high awareness. Based on this scheme, the sample had, on average, moderate awareness of OPD-associated complications. Fig. 2 depicts their distribution according to the computed awareness levels.
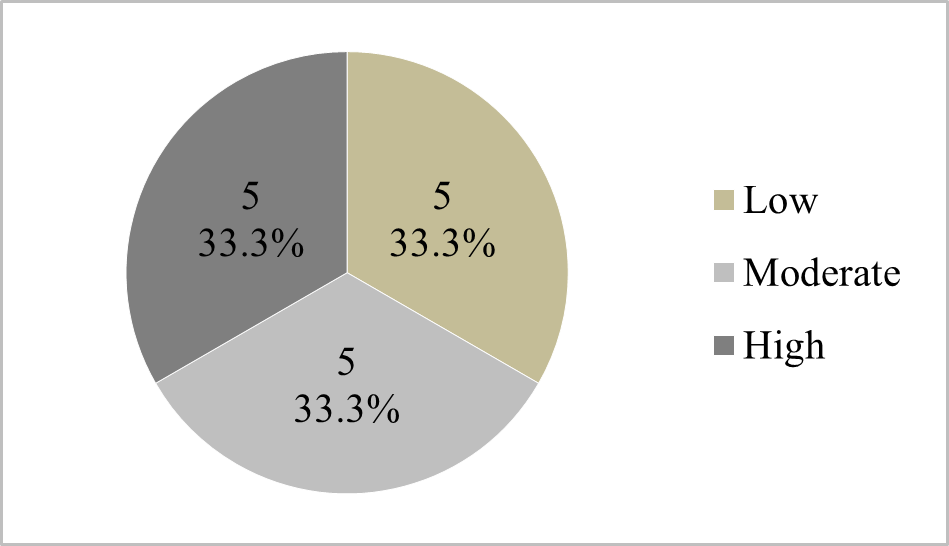
Fig. 2: Complication Awareness Levels Grouped as Low, Moderate, or High
From Fig. 2, only 33.3% (n = 5) of the participants had high OPD complication awareness scores. The other 66.7% (n = 10) had either low or moderate awareness. For further analyses, the study computed the aggregate awareness of specific OPD complications. TABLE III displays the number of participants who responded correctly to each of the OPD complication awareness items.
Table III: Number (%) of Correct Responses to the Complication Awareness Items
| Complication | n | % | Interpretation |
| Aspiration pneumonia | 14 | 93.33 | High |
| General weakness | 12 | 80.00 | High |
| Digestion problems | 4 | 26.67 | Low |
| Aspiration | 14 | 93.33 | High |
| Dehydration | 13 | 86.67 | High |
| Anaphylactic shock (narrow airway, blocking breathing) | 4 | 26.67 | Low |
| Sudden heart attack | 7 | 46.67 | Low |
| Malnutrition | 12 | 80.00 | High |
| Haematemesis (vomiting blood) | 6 | 40.00 | Low |
| Increased mortality (death of a patient) | 11 | 73.33 | Moderate |
High awareness levels were recorded for aspiration pneumonia, aspiration, dehydration, general weakness, and malnutrition. Over 80% of the participants matched these items correctly. Participants had the lowest awareness levels concerning anaphylactic shock and digestion problems. Although these two are not OPD-associated complications, 73.3% (n = 11) considered them complications arising from the condition. The other most misidentified items were haematemesis and sudden hard attack. Only 40.0% (n = 6) and 46.7% (n = 7) matched haematemesis and sudden hard attack, respectively, correctly.
C. Differences in Oropharyngeal Dysphagia Complications Awareness Levels due to Individual Characteristics
The study also assessed whether HPs’ individual characteristics influenced their awareness of OPD-associated complications. For this objective, mean complication awareness score were then compared across participant selected categories, including their gender, age, educational attainment, experience, specialization, and OPD training. The Shapiro-Wilk test showed that the scores were normally distributed, allowing for the use of parametric tests (SW = .925, p = .229). Specifically, independent samples t-tests were used to compare mean awareness scores across gender and training categories, while one-way ANOVA was used for the other characteristics. The results were as depicted in TABLE IV. The mean scores for each category and their corresponding standard deviations are in the “M” and “SD” columns, respectively. The last column shows the test statistics (t or F) and the corresponding p-values (in brackets). Levene’s test showed that the assumption of homogeneity in variance was met for all the variables (p > 0.05).
Table IV: Complication Awareness Levels by Participant Characteristics
| Characteristic | Category | n | M | SD | t/F (p) |
| Gender | Male | 8 | 62.50 | 19.086 | 0.414 (.865) |
| Female | 8 | 67.14 | 24.300 | ||
| Age group | 25-30 years | 6 | 60.00 | 12.247 | 1.72 (.221) |
| 31-35 years | 5 | 78.00 | 17.889 | ||
| 36-40 years | 5 | 56.00 | 27.019 | ||
| Education | Diploma | 4 | 63.33 | 15.275 | 0.043 (.958) |
| Bachelor | 8 | 63.75 | 24.458 | ||
| Post-graduate | 4 | 67.50 | 22.174 | ||
| Experience | 4-6 years | 5 | 60.00 | 14.142 | 1.119 (.359) |
| 7-9 years | 5 | 76.00 | 9.274 | ||
| > 9 years | 6 | 58.33 | 9.804 | ||
| Specialization | Nurse | 5 | 67.50 | 15.000 | 0.137 (.873) |
| Physiotherapist | 7 | 61.43 | 25.448 | ||
| Other | 4 | 67.50 | 22.174 | ||
| Training | No | 9 | 67.78 | 17.873 | 0.689 (.503) |
| Yes | 6 | 60.00 | 26.077 |
Table IV shows that none of the factors produced a significant difference in the mean complication awareness levels. Thus, keeping other variables constant, neither gender, age group, educational attainment, work experience, specialization, nor training had a significant influence on this sample’s average awareness of OPD-associated complications.
DISCUSSION
Interprofessional collaboration continues to assume a leading role in efforts to improve patient outcomes in all clinical settings (WHO, 2010; Reeves et al., 2017). These strategies aim to promote a holistic view of health in which the contributions of specialists from various disciplines are valued. Such an interdisciplinary-like approach promotes structural learning, knowledge sharing, and teamwork vital for quality care of OPD patients. To increase the effectiveness of their collaborative efforts, all HPs involved in OPD management should have adequate awareness levels of its signs and symptoms, risk factors, and associated complications (Anderle et al., 2018; Knight et al., 2023). On this basis, the present study sought to establish the level of OPD-associated complications awareness among HPs attending to adult inpatients in the ACF of a level-six hospital in Kenya. A previously validated questionnaire was administered to a sample of HPs in the facility to generate data on their awareness levels. From TABLE II, seven of the ten items had less than the maximum possible response, while eight had at least one “undecided” response. Although not directly implied, the high number of missing or “undecided” responses could suggest that many participants were either unaware or uncertain of OPD-associated complications.
Further analyses of their responses to the questionnaire items seemed to support the above observation that many participants were either unaware or uncertain of OPD-associated complications. From Fig. 2, two-thirds of the sample had either low or moderate awareness of OPD-related complications. Only a third had high awareness. This finding is consistent with those of (Knight et al., 2023), who reported an OPD complication awareness level of 47.3% among nurses in a South African hospital. They also support those of Hady et al. (2023), who observed low awareness of OPD complications in an Egyptian hospital. In Hady et al. (2023), while HPs identified aspiration, pneumonia, and malnutrition as OPD complications, there was low awareness regarding weight loss, general weakness, dehydration, and increased mortality.
Notably, archival records showed a high number of initial intakes in a Kenyan National hospital’s surgical and medical wards diagnosed with OPD (Ndiema et al., 2023). Hence, it was anticipated that the majority of HPs in these facilities would have high OPD management awareness. Contrary to this expectation, average awareness of OPD-associated complications among the sampled HPs was only moderate. A possible implication is that many HPs in the hospital’s ACF may not have the capacity to identify factors that could expose OPD patients to additional complications. Low awareness in this area may make it challenging for professionals to identify and minimize patients’ exposure to OPD-associated complications (Hady et al., 2023). There is a need for the facility’s management to implement OPD complication awareness training for the hospital’s HPs.
Aside from the average moderate awareness, individually, participants exhibited varied levels regarding specific OPD-related complications. Further, their awareness of OPD-related complications was independent of their gender, age, educational attainment, experience, or specialty. Thus, any intervention to improve complication awareness within the facility should target all HPs, irrespective of their characteristics.
SUMMARY AND CONCLUSION
The study’s objective was to establish the levels of awareness of OPD-associated complications among HPs attending to adult inpatients in the ACF of a level-six hospital in Kenya. A previously validated questionnaire with ten awareness items was administered to a sample of HPs in the facility. On average, the sample had moderate awareness levels of the assessed items. Individually, participants had varied awareness levels, ranging from low (< 50%) to high (> 75%). None of the assessed characteristics (gender, age, educational attainment, experience, specialty, and training) seemed to have a significant influence on the awareness levels. Based on the above findings, it can be concluded that HPs attending to adult inpatients in the hospital’s ACF have, on average, only moderate awareness of health complications resulting from OPD in adult inpatients. Their awareness of OPD complications is independent of their demographic and general characteristics.
The findings are subject to various limitations, notably the small sample size and the over-reliance on the descriptive design. The small sample size increased the study’s exposure to biases, while the descriptive design did not allow for controlling other factors that could influence awareness. Additionally, some participants may have not been truthful or accurate in their responses. The drawbacks notwithstanding, the study, for the first time, reports on awareness levels of oropharyngeal dysphagia complications among HPs attending to patients in the hospital’s medical and surgical wards. More training should be encouraged in that facility to increase dysphagia awareness levels among its HPs. The institution’s management could rely on the findings to develop evidence-based interventions to increase the dysphagia awareness levels of its medical staff.
ACKNOWLEDGEMENT
Humble gratitude to the willing participants for the timely and honest responses to accomplish this study.
REFERENCES
- Adkins, W. Takakura, B. M. Spiegel, Et Al., “Prevalence And Characteristics of Dysphagia Based On A Population-Based Survey,” Clinical Gastroenterology And Hepatology, Vol. 18, No. 9, Pp. 1970-79, Oct. 2019.
- Alagiakrishnan, R. A. Bhanji And M. Kurian, “Evaluation And Management Of Oropharyngeal Dysphagia In Different Types Of Dementia: A Systematic Review,” Archives Of Gerontology And Geriatrics, Vol. 56, No. 1, Pp. 1-9, Jan-Feb. 2013.
- W. Altman, G. P. Yu And S. D. Schaefer, “Consequence Of Dysphagia In The Hospitalized Patient: Impact On Prognosis And Hospital Resources,” Archives Of Otolaryngology, Vol. 136, No. 8, Pp. 784-789, Aug. 2010.
- Anderle, R. S., Rech, V. M. Pasqualeto And B. N. de Goulart, “Knowledge Of The Medical And Nursing Teams About The Management Of Oral Medications In Hospitalized Adult Dysphagic Patients,” Audiology Communication Research, Vol. 23, No. 1, P. e1933, Jan. 2018.
- Ary, L. C. Jacobs, C. K. Sorensen And A. Walker, Introduction To Research In Education, Wadsworth: Cengage Learning, 2014.
- Bakhtiyari, R. Ghorbani, M. Salmani Et Al. “Physicians’ Perspective On a Multidisciplinary Approach To Dysphagia Management,” Iranian Journal Of Otorhinolaryngoly, Vol. 31, No. 104, Pp. 141-146, May 2019.
- S. Bonilha, “The One-Year Attributable Cost Of Post-Stroke Dysphagia,” Dysphagia, Vol. 29, No. 5, Pp. 545–552, Oct. 2014.
- Bolinger And J. Dembowski, “Speech Language Pathology Consultations And Medical Outcomes For Patients With Aspiration Pneumonia,” Journal Of Medical And Health Studies, Vol. 3, No. 3, Pp. 45-58, Aug. 2022.
- J. Cook, “Oropharyngeal Dysphagia,” Gastroenterology Clin, Vol. 38, No. 3, Pp. 411-431, Sep. 2009.
- J. Donovan, S. K. Daniels, J. Edmiaston, et al., “Dysphagia screening: State of the art – Invitational conference proceeding from the State-of-the-Art Nursing Symposium, International Stroke Conference 2012,” Stroke, vol. 44, no. 4, pp. e24-e3, Feb. 2013.
- Gupta, M. Gupta And A. Gupta, “Dysphagia In The Elderly: A Multidisciplinary Approach,” Journal Of Datta Meghe Institute Of Medical Sciences University, Vol. 17, No. 3, Pp 779-785, Jul–Sep 2022.
- F. Hady, H. M. Farag And A. R. Sheikhany, “The Awareness And Knowledge Of Dysphagia Among Health Care Practitioners In Egypt,” Egyptian Journal of Otolaryngology, Vol. 39, No. 25, Pp. 1-16, Jan. 2023.
- Head, K. Weeks, A. Stroud And A. M. Coll, “A Survey Of Dysphagia Screening Practices Across England And Wales,” International Journal Of Therapy And Rehabilitation, Vol. 14, No. 9, 409-417, Sep. 2007.
- J. Logemann, “Multidisciplinary Management Of Dysphagia,” Acta oto-Rhino-Laryngologica Belgica, 48(2), 235-238, Jan. 1994.
- Knight, B. Pillay, J. van der Linde And E. Krüger, “Nurses’ Knowledge Of Stroke-Related Oropharyngeal Dysphagia In The Eastern Cape, South Africa,” South African Journal Of Communication Disorders, Vol. 67, No. 1, Pp. 703-713, Sep. 2020.
- Martino, N. Foley And S. Bhogal, “Dysphagia After Stoke: Incidence, Diagnosis, And Pulmonary Complications,” Stroke, Vol. 36, No. 12, Pp. 2756-63, Nov. 2005.
- Matar, H. Smaily, P. Cherfane And C. Hanna, “Profiling Of Oropharyngeal Dysphagia In An Acute Care Hospital Setting,” Ear, Nose, & Throat Journal, Vol. 100, No. 8, Pp. 357-361, Apr. 2021
- D., McHutchion, J. M. Pringle, M. N. Tran, et al. “A Survey Of Public Awareness Of Dysphagia,” International Journal Of Speech-Language Pathology, Vol. 23, No. 6, Pp. 614–621, May 2022.
- Mugenda And O. Mugenda, Research Methods: Quantitative And Qualitative Approaches, Nairobi: ACTS Press, 2013.
- Ndiema, D. C., Abuom, T., & Karia, M. (2024). Health Professionals’ Awareness of Signs and Symptoms of Oropharyngeal Dysphagia among inpatients at a Level – Six Referral Hospital in Kenya. International journal of research and scientific innovation (IJRSI), Vol. 11, No. 3, Pp. 369-380, Apr. 2024. https://doi.org/10.51244/IJRSI.2024.1103026
- Ndiema, D. C., Abuom, T., & Karia, M. “Health Professionals’ Identification Levels of Risk Factors: In View of the Management of In-Patients Admitted with Upper Gastrointestinal Tract Swallowing Disorders in a Kenyan National Hospital,” International journal of research and scientific innovation (IJRSI), Vol. 11, No. 3, Pp. 740-751, Apr. 2024. https://doi.org/10.51244/IJRSI.2024.1103052
- Ndiema, D. C., Abuom T., And Karia M. “A Descriptive Retrospective Review On The Epidemiology Of Oropharyngeal Dysphagia In The Acute-Care Facility Of A Kenyan (Level-Six) National Hospital,” IOSR Journal of Nursing and Health Science, Vol. 12, No. 6, pp. 20-28, Dec. 2023. https://doi.org/10.9790/1959- 1206062028
- Nishino, “The Swallowing Reflex And Its Significance As An Airway Defensive Reflex,” Frontiers In Physiology, Vol. 3, No. 489, Pp. 1-15, Jan. 2013.
- O. Oduor, A. Keter, L. O. Diero et al. “Stroke Types, Risk Factors, Quality Of Care And Outcomes At a Referral Hospital In Western Kenya,” East Africa Medical Journal, Vol. 92, No. 7, Pp. 324-332, Oct. 2015.
- G. Omondi, A Quality Audit on the management of acute ischaemic stroke at Kenyatta National Hospital (Unpublished Thesis). Nairobi: University of Nairobi, 2019.
- Rajati, N. Ahmadi, Z. Naghibzadeh And M. Kazeminia, “The Global Prevalence Of Oropharyngeal Dysphagia In Different Populations: A Systematic Review And Meta-Analysis,” Journal Of Translational Medicine, Vol. 20, No. 1, Pp. 175-187, Apr. 2022.
- Reeves, F. Pelone, R. Harrison et al., “Interprofessional Collaboration To Improve Professional Practice And Healthcare Outcomes,” The Cochrane Database Of Systematic Reviews, Vol. 6, No. 6, P. Cd000072, Jun. 2017.
- Rhoda and A. Pickel-Voight, “Knowledge Of Nurses Regarding Dysphagia In Patients Post Stroke In Namibia,” Curationis,Vol. 38, No. 2, Pp. 1564-1571, Nov. 2015.
- Rofes, V. Arreola, J. Almirall Et Al., “Diagnosis And Management Of Oropharyngeal Dysphagia And Its Nutritional And Respiratory Complications In The Elderly,” Gastroenterology Research And Practice, Vol. 1, No. 1., Pp. 1-13, Aug. 2011.
- L. Streiner, G. R. Norman And J. Cairney, Health Measurement Scales: A Practical Guide To Their Development And Use, New York: Oxford University Press, 2014.
- Takizawa, E. Gemmell, J. Kenworthy And R. Speyer, “A Systematic Review Of The Prevalence Of Oropharyngeal Dysphagia In Stroke, Parkinson’s Disease, Alzheimer’s Disease, Head Injury, And Pneumonia,” Dysphagia, Vol. 31, No. 3, Pp. 434-441, Mar. 2016.
- J. Verdonschot, L. W. Baijens, J. L. Serroyen, et al. “Symptoms Of Anxiety And Depression Assessed With The Hospital Anxiety And Depression Scale In Patients With Oropharyngeal Dysphagia,” Journal Of Psychosomatic Research, Vol. 75, No. 5, Pp. 451-455, Nov. 2013.
- World Health Organization. Framework For Action On Interprofessional Education and Collaborative Practice. Available at: https://interprofessional.global/wp-content/uploads/2019/11/WHO-2010-Framework-for-Action-on-Interprofessional-Education-and-Collaborative-Practice.pdf