Brachytherapy in Cervical Cancer: Accuracy in Point Dose Demarcation
- V. Ramanathan
- M.S. Gulawita
- M.P.O.T Kumari
- S. Malaviarachchi
- 284-293
- Jun 14, 2024
- Health
Brachytherapy in Cervical Cancer: Accuracy in Point Dose Demarcation
V. Ramanathan1, M.S. Gulawita1, M.P.O.T Kumari1 and S. Malaviarachchi2
1Department of Radiography and Radiotherapy, Faculty of Allied Health Sciences, General Sir John Kotelawala Defence University, Ratmalana, Sri Lanka
2Department of Clinical Sciences, Faculty of Medicine, General Sir John Kotelawala Defence University, Ratmalana, Sri Lanka
DOI: https://doi.org/10.51584/IJRIAS.2024.905025
Received: 27 April 2024; Revised: 09 May 2024; Accepted: 13 May 2024; Published: 14 June 2024
ABSTRACT
Cervical cancer is one of the commonest gynecological cancers in Sri Lanka. Due to very limited high dose rate (HDR) after loader facility, conventional brachytherapy is practiced in government sectors in our country. The dose specification point A in brachytherapy is a geometrical concept which represents the anatomical position of uterine artery crosses the ureter. This study aimed to assess how the Manchester point A represents the true anatomical point A (APA). A total of 48 diagnostic contrast enhanced CT scans of carcinoma of the cervix/endometrium were reviewed retrospectively for this descriptive quantitative study. Manchester point A was established. The APA and high-risk clinical target volume (HRCTV) were marked and contoured on the CT data.The dimensions of HRCTV on AP projection and coordinates of APA were recorded. The relationship between the dimensions of HRCTV and the position of APA also was assessed to discuss the possibilities of individualizing the point-based brachytherapy. The mean APA of the sample was at a vertical level of 1.18±0.35 cm from the external-orifice along the uterine axis and 3.63±0.52 cm laterally to either side. A significant moderate positive correlation exists between HRCTV dimensions and APA position. An approximate individualized Point A is defined using this correlation as a function of HRCTV dimensions, which can easily be measured from radiotherapy planning CT scans. The geometric point A does not provide an accurate estimate of the APA that indicates there is a need for patient-based model. The developed model is useful in a 3D brachytherapy setup for individualized dose recording and can be used in a 2D brachytherapy setup to individualize dose prescription if the applicability is proven.
Keywords: Brachytherapy, Cervical cancer, Intracavitary brachytherapy, Manchester point A, Point A
INTRODUCTION
Cancer of uterine cervix (Ca Cervix) is the fourth most common cancer and fourth most common cause of cancer death in women worldwide and about 70% of cervical cancer incidence and 90% of deaths occur in developing countries.1 In Sri Lanka, it is the second commonest female cancer with an incidence of 1407 in 2020.2 A combination of external radiation therapy (EBRT) and intracavitary brachytherapy contributes to the total therapeutic radiation dose to tumor volume in locally advanced cervical cancer, and several studies have shown a reduced rate of local recurrence and an improved survival rate.3,4
The conventional 2D brachytherapy planning is commonly based on the Manchester method (a dosimetric system) which prescribes the dose to a point A; a representative of the dose throughout a considerable zone of tumor bearing tissue.3,5 Tod and Meredith defined the point A as the dose limiting and specification point in the treatment of Ca-Cervix because it represented the average dose to the paracervical region, where over-dosage is especially dangerous and which often is the site of early infiltration by cancer.5 It is regarded the point where the ureter crosses the uterine artery and is considered here as the anatomical point A.6,7
In order to relate the anatomical position to simple geometrical conceptions, Tod and Meredith defined the point A as 2 cm lateral to the central canal of the uterus and 2 cm from the mucous membrane of the lateral fornix in the axis of the uterus. This definition was later altered by the same authors as a point located 2 cm superior to the external cervical os and 2 cm lateral to the cervical canal.5 Dose specification based on this geometrical point A was proposed at a time with limited availability of imaging technology where the planning was done based on 2 orthogonal x-ray radiographs. Since the first defined point A could not be visualized on radiograph, it was redefined in relation to the visible brachytherapy applicators, to be the point 2 cm up from the lower end of the last intrauterine tube and 2 cm laterally in the plane of the uterus. 5,7
Manchester system was designed for low dose rate brachytherapy, but however the same specification point A was used for dose prescription in high dose rate (HDR) brachytherapy as well. Applicator types, isotopes, source strength and distribution have all altered in HDR gynecologic brachytherapy. To address these concerns, Madison system was developed in 1990s to describe a set of dose schedules and dose specification points for treatment of Ca-cervix with HDR brachytherapy and external beam radiation. Instead of “A”, this system uses a central reference point, “M” which is defined in relation to the applicator and patient’s anatomy, to be the point that lies “2 cm lateral to the center of the uterine canal and 2 cm cephalad from a line joining the center dwell position of the vaginal colpostat sources”.8 Brachytherapy has evolved much from the point based brachytherapy to individualized 3D-image based brachytherapy where the treatment is planned using contoured structures, the target (HR-CTV) and other critical structures. 9,10
Radiotherapy treatment workload is significantly high11 in Sri Lanka due to the lack of radiotherapy treatment facilities.12 Therefore, conventional (2D) radiotherapy treatment is still practiced in some treatment centers in Sri Lanka.13 Moreover, the conventional point-based brachytherapy is still used in many institutes for its simplicity and affordability. In Sri Lanka, only three HDR after loader are available in government and private sectors for about 22 million people.2 Therefore, 2D-based conventional brachytherapy is practiced mostly. Moreover, Point A is still important in 3D brachytherapy as well. The Groupe Européen de Curiethérapie–European Society for Radiotherapy and Oncology (GEC–ESTRO), in their published recommendations for the practice of 3-D image-based brachytherapy, recommends to start with the standard method of dose prescription either the point A or the 60 Gy reference volume, and then doing adjustments to ensure target coverage in regions of under-dosage.14
If the prescription point A could not accurately represent the actual anatomical point A or on average the paracervical region, that might result in under dosage or inadequate coverage of the target leading to recurrences or over dosage of surrounding sensitive normal tissue leading to radiation toxicities. It motivates to identify the variations between the anatomical and Manchester point A. To address this issue, position of the two points; anatomical and Manchester point A were compared using CT data and a means to individualize point-based prescription with the use of available resources is investigated.
MATERIALS AND METHODS
The study was designed to assess how the brachytherapy dose prescription point (Manchester point A) represents the true anatomical point A and to evaluate whether the HRCTV is adequately covered in point-based brachytherapy. This study also aims to explore the possibility to individualize the point-based brachytherapy. The contrast enhanced CT scans performed for the patients with carcinoma cervix or endometrium at Radiology Unit of Apeksha Hospital, Maharagama, Sri Lanka from September 2020 to January 2021 were selected for this descriptive quantitative study. The selected patients had pathologically proven squamous cell carcinoma or adenocarcinoma of the uterine cervix or uterus. In addition, the patients were either treated with external beam radiotherapy or were waiting for radiotherapy/surgery.
The routine radiological assessment is performed for the patients who diagnosed with cervical carcinoma to assess the operability and further confirmation of staging. In order to assess the radiotherapy treatment response and recurrence disease, radiological assessment is again performed during their follow-up. Generally, staging MRI is performed as the standard test but contrast enhanced CT is performed at Apeksha hospital due to the unavailability of MRI facility. Apeksha hospital was selected as the study setting since it is the main cancer treatment center in Sri Lanka. In addition, it is the largest government institute provides high dose rate brachytherapy facility. Hence, a large cohort of patient population can be observed during the set period of time. In the inclusion criteria, diagnostic contrast enhanced CT scans of patients with biopsy proven carcinoma of uterine cervix or uterus, intra-venous contrast enhanced CT scans with slice thickness less than or equal to 5 mm, CT scans of patients who were in the age range of 18 to 80 years were included in this study.
A total of 73 samples were collected retrospectively. Out of 73 sample, 25 scans were rejected because of not clearly seen anatomical data of para-cervical tissue. Finally, 48 CT scans were selected for this study. APA was marked on all selected CT scans. The HR-CTV was only marked on the CT scans of patients of whom uterus was surgically excised since it is not possible to differentiate cervix from the uterus on CT scan, and for patients who haven’t had radiotherapy. In this research work, we did not specifically select patients who have the indication for radiotherapy as it was not a requirement to achieve the aims of the study. However, the selected sample contained CT data who were treated with radiotherapy as well.
The CT scans were obtained from a Siemens Emotion 6 slice CT scanner. According to the pelvic protocol, intravenous injection of iodinated contrast material based on patient’s weight (1.2 ml/kg) was administrated with angiographic injector at 2 ml per second, and superior to inferior image with 2 mm section thickness from the diaphragm to the anus level was obtained after 70 second waiting time. The scanned data were extracted from the system and imported to 3D slicer (version 4) software which is an open source platform for medical image informatics, image processing and 3D visualization. Contouring and measurements were performed using 3D slicer and data were recorded into Microsoft Excel data sheet.
By using 3D slicer software, right and left anatomical point A (the crossing of uterine artery and the ureter in para-cervical tissue, located by the uterine artery arc sign around the pelvic ureter on either side), external cervical orifice, axis of the uterine cervical canal were located and marked for each patient. Moreover, HR-CTV was contoured, for the patients who did not get radiotherapy and of whom the uterus was excised, as shown in figure 1.
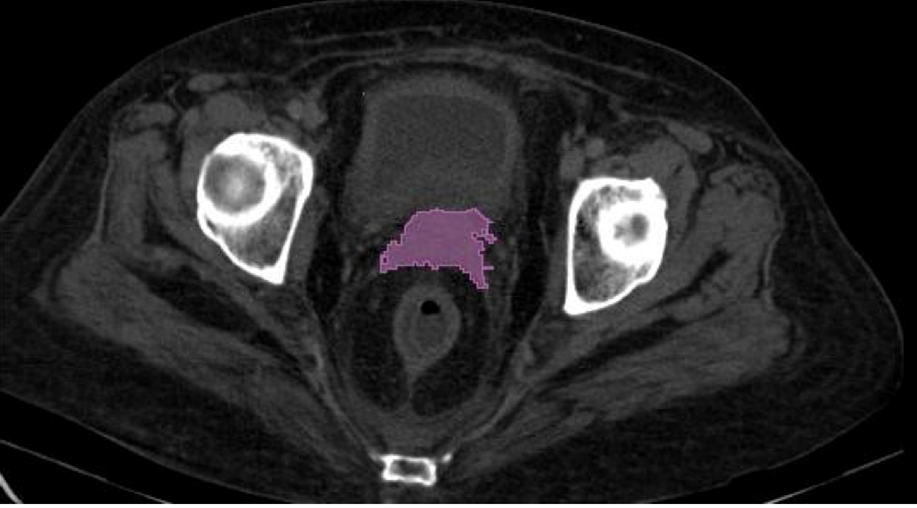
Figure 1: HR-CTV marked on axial slice.
For the measurements, the same geometrical basis as defined in the Manchester report was established; the external os is taken as the geometrical origin and the axis of the uterus as the general axis of reference (or x-axis). The z-axis is designated as the axis of the vagina at right angle to the axis of the uterus while y-axis is the horizontal lateral axis through the cervix (see figure 2). The Manchester point A is thus the point (2 cm, 2 cm) in the xy plane. Distance along each axis (x and y) is taken from the origin to each APA.
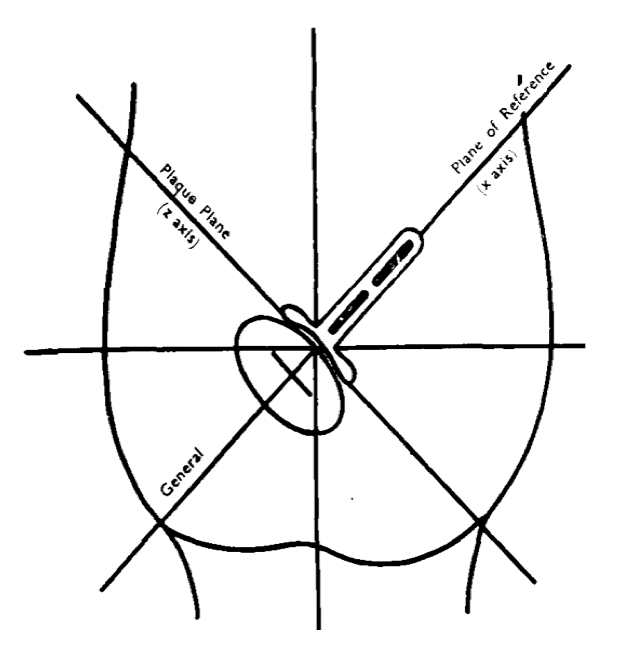
Figure 2: Geometric coordinates used by the Manchester system to define the position of point A (left) and the geometric coordinates used for the study (right), where the x-axis is the axis of the uterine canal and y is the horizontal lateral axis through the cervix.
For consistent contouring, preset pelvis window leveling and level tracing were used to aid for all CT data. The maximum width of HR-CTV in left and right directions, the distance between the femoral heads at the level of the mid femoral head, and maximum width of the pelvic cavity at mid-pelvis, vertical distance from the level of iliac crest level to femoral head level were measured for each patient on their CT data. AP orthogonal view of scan data with segmented structures was used to determine whether the APA and Manchester point A lies within or outer to the HR-CTV.
An IBM SPSS Statistics 23.0 software was used for the data analysis. Descriptive statistics were applied to include frequencies, means, dispersion and distribution to describe the analyzed variables in this sample of study. Each of the variables of entire sample and their subsets were separately assessed to determine their distribution using normality tests and plots. For all inferences, the statistical significance was defined as p value of less than 0.05. The independent samples t-test was used to compare the mean APAs of the patients who were treated with radiotherapy and of those who were not treated with radiotherapy. Two-tailed one sample t-test was used to assess whether the mean APA(μ) represent the Manchester point A along x and y axes.
Pearson correlation coefficient and least square-best fit regression lines were used to assess the correlation of APA distance to both HR-CTV dimensions and to multiple skeletal dimensions. The plots of APA (along y axis) versus maximum HR-CTV width, and APA (along x axis) versus HR-CTV height were assessed to find any significant correlation of APA with HR-CTV dimensions. The plots of APA (along y axis) versus distance between femoral heads, APA (along y axis) versus maximum cavity dimensions and APA (along x axis) versus distance from the level of iliac crest level to femoral head level were assessed to find any significant correlation of APA with skeletal dimensions.
RESULTS
Among a total of 39 patients who had records of their radiotherapy treatment, 16 patients were given radiotherapy and 23 patients were not given radiotherapy yet. Independent sample t-test was performed for APA measures of radiotherapy treated and untreated patients, it failed to reject the null hypothesis which assumes equal means. Therefore, there was no statistically significant difference between mean APA of the patients who had radiotherapy and mean APA of the patients who did not have radiotherapy, for right APA (vertical p=0.981, lateral p=0.625), left APA (vertical p=0.879, lateral p=0.504) and mean APA of each patient (vertical p=0.930, lateral p=0.799).
The position of Manchester point A is the point (2 cm ,2 cm) in the XY plane of the geometrical coordinate system defined in Manchester report 1938. Table 1 shows the measured distance to the anatomical point A. Sample means are greater than 2 cm in y axis and less than 2 cm along x axis. One sample t test (2 tailed) performed on APA measurements to check with the Manchester point A which is the accepted population mean, was strongly significant (p<0.001) at 95% confidence interval to reject the null hypothesis. Therefore, there is strong evidence to prove that the mean APAs (Right, left and the mean of right and left of each patient) of the two populations do not match. In addition, HR-CTV was contoured for 24 patients. The HR-CTV dimensions are shown in Table 2. The lateral coverage of HR-CTV by point A in AP projection is shown in Table 3.
Table 1: Distance to the Anatomical point A along XY-axes
| Axis of measurement | Mean (cm) | Standard Deviation (cm) | Maximum (cm) | Minimum (cm) | |
| Vertical (along x axis) | Right | 1.18 | 0.36 | 2.22 | 0.27 |
| Left | 1.19 | 0.35 | 2.22 | 0.27 | |
| Meana | 1.18 | 0.35 | 2.22 | 0.27 | |
| Lateral (along y axis) | Right | 3.61 | 1.00 | 6.00 | 1.50 |
| Left | 3.65 | 1.22 | 6.15 | 1.50 | |
| Meana | 3.63 | 0.52 | 4.57 | 2.45 | |
Origin of the coordinate system is the external os where axis of uterine canal is the general axis of reference (x axis), perpendicularly axis of vagina is z axis, horizontal axis through the cervix is y axis a = (Right + Left)/2.
Vertical mean APA and lateral mean APA for each patient is the mean value of right and left APAs, along vertical (x) and lateral (y) axes respectively.
Table 2: HR-CTV dimensions.
| Mean | Standard Deviation | Maximum | Minimum | ||
| Width* | Maximum (cm) | 6.02 | 1.00 | 8.14 | 4.23 |
| Half of the maximum (cm) | 3.01 | 0.50 | 4.07 | 2.12 | |
| Height from ex-os | Maximum (cm) | 2.49 | 0.76 | 3.79 | 1.49 |
*HR-CTV dimensions in an AP projection
Table 3: HR-CTV lateral coverage by point A in AP projection
| Count | ||
| ½ of maximum HRCTV with coverage by mean lateral APA | Not covered | 1 |
| Covered | 23 | |
| ½ of maximum HRCTV width coverage by Manchester point A | Not covered | 24 |
| Covered | 0 |
The correlation is significant at the 0.05 level (2-tailed) and there is a moderately positive correlation between mean lateral APA distance and maximum HR-CTV width with Pearson correlation coefficient of 0.472. Simple linear regression analysis shows that 18.7% of the variance in mean lateral distance of an APA is due to the maximum HR-CTV width (F(1,22) = 6.293,p=0.02). The correlation can be explained by the equation; y= 0.192x + 2.537, where y is the mean lateral distance to APA and x is the maximum HRCTV width. The same correlation can be explained by y= 0.384x + 2.537, when x is taken as half of the maximum HRCTV width. (see figure 3).
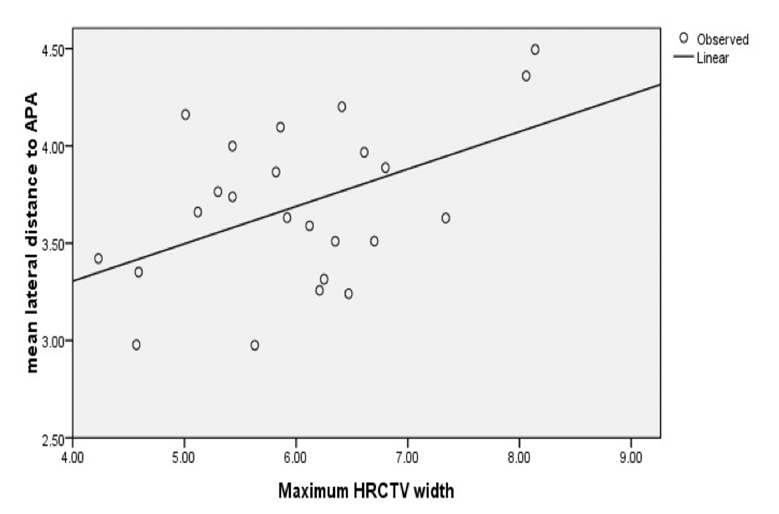
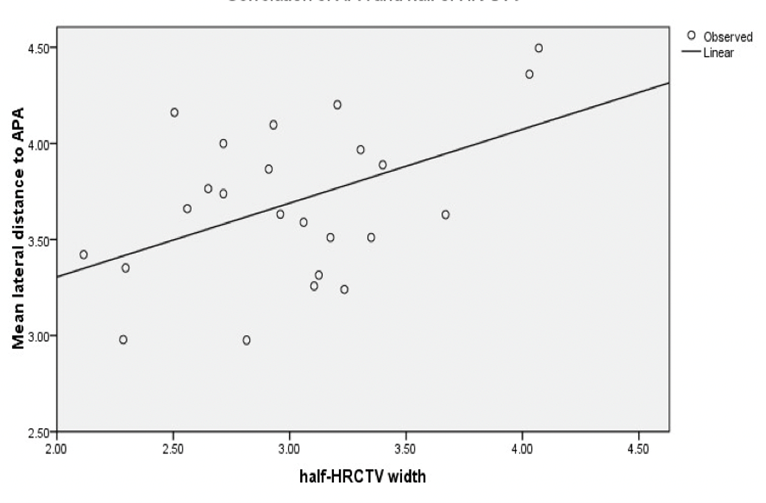
Figure 3: The left figure shows the correlation of APA and HR-CTV (laterally) and the right figure shows the correlation of APA and half of HR-CTV width.
The correlation is statistically significant at the 0.05 level and there is a moderate positive correlation between mean vertical APA distance and HR-CTV height with a Pearson correlation coefficient of 0.430. Simple linear regression analysis shows that 14.8% of the variance in mean vertical distance of APA is due to the HR-CTV height. (F(1,22) = 5.004, p=0.036.) The correlation can be explained by the equation; y= 0.219x + 0.633, where y is the mean vertical distance to APA and x is the HRCTV height from ex-os. (see figure 4)
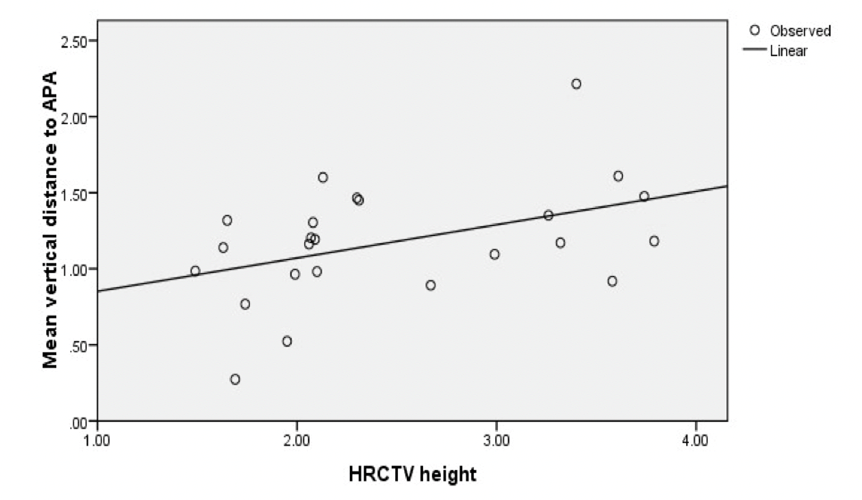
Figure 4: The correlation of APA and HR-CTV along x-axis.
The correlation for mean lateral APA and femoral head distance is not statistically significant (2-tailed p= 0.385). The correlation for mean lateral APA and maximum pelvic cavity dimension is not statistically significant (2-tailed p =0.404). The correlation for mean vertical APA and mean vertical distance from level of iliac crest to level of femoral head is also not statistically significant (2-tailed p= 0.957).
DISCUSSION
The study aimed to compare the position of brachytherapy dose prescription point of Manchester A (geometrical) and the anatomical point A, and to assess the possibilities of individualizing point-based brachytherapy. The mean position of APA of the patients who had radiotherapy and who did not have radiotherapy was not significantly different from each other implying that there is no significant change in APA due to the effects of radiotherapy such as tumour shrinkage. This implication fit well with the outcomes of the Wang et.al., (2007)6 which reports that the right APA varied only by a mean of 0.3±0.2 cm and the left by a mean of 0.2±0.2 cm where the mean change in tumour size was 0.9± 0.5 cm over the treatment period. It concludes that the tumour itself was not responsible for the marked difference in location between geometrical point A and the APA.
Further, the results of the present study indicate that the mean distance to the APA from the origin was less than 2 cm vertically (x axis) and greater than 2 cm laterally (y axis) for both right and left APAs and mean APA (Table 1). The results do not fit well with the findings of Wang et.al., 20076, however it supports the mismatch of anatomical point A. It has to be noted that the present study measured the APA position in XY plane based on the original Manchester geometric coordinates and Wang et.al., 2007 measured the position of APA in relation to geometric point A defined based on applicator geometry. Therefore, the results of the two studies cannot be compared by their magnitude.
The study population failed to represent the mean of population from which the Manchester point A was derived (p<0.01, one sample t-test (2 tailed)). It is a limitation of the study that we cannot assess the possible effect that the rigid applicators (uterine tandem) used in HDR treatments may have on the position of APA in relation to the uterine axis, as all CT scans were of diagnostic purpose, taken without HDR applicators. However, the Manchester point A was originally defined for low dose rate (LDR) brachytherapy which used small radium tubes that do not displace the uterine axis significantly. Therefore, the methodology used for assessment is not faulty since the same geometric coordinate plane was used for the study but the practicability of clinical application in HDR setting may be affected. It has to be noted that the same point A that was defined for LDR brachytherapy was used for the HDR setting despite the fact that it might displace the uterine axis in relation to the APA.
The half of maximum HR-CTV width in AP projection is compared to Manchester point A to assess whether the half of HRCTV width is enclosed by Manchester point A bilaterally. The sample results indicate that Manchester point A failed to enclose half of HRCTV in any of the patients when the maximum dimension of the HRCTV width is considered. But as expected this is suboptimal in assessing the HRCTV coverage as it is not the position of one point but the planned iso-dose distribution that determines HRCTV coverage. However, as the half of HRCTV width (which ranges from 4.07 cm – 2.12 cm with a mean of 3±0.5 cm) is greater than 2 cm, there is a high chance of HRCTV being under-dosed. This can be only confirmed by assessing the 3D dose distribution when the treatment is planned in a 3D brachytherapy setting.
Goyal et al., (2016)3 in their study reported the correlation between HR-CTV width and ND90 (normalized D90) as a negative correlation which implies poor target coverage as the HRCTV width increases (Pearson coefficient of 0.84, linear regression equation y = (0.282) x + 2.299 which has to be y=0*x +1 in the ideal case (i.e. ND90=1).The proposed goal for 3D image-guided conformal brachytherapy treatment is for 90% of the high-risk clinical target volume (HR-CTV D90) to receive the prescribed dose. If applied our mean HRCTV width to the above regression formula of Goyal et al., (2016), the ND90 would approximately be 0.60 (ranging from 0.33 to 0.80 to when accounted the standard deviation) implying inadequate coverage. Although the HR CTV was enclosed by the bilateral APAs all the time, half of the HRCTV width was not always less than the lateral mean APA for each patient but for most (95.8% of the sample), it was. However, no predictions can be done on the HRCTV coverage by APA, unless the dose distribution is assessed in a 3D setting by prescribing dose to the APA.
The conventional dose calculation and prescription for 2D point based brachytherapy rely solely on applicator geometry and information from orthogonal radiographs. In this study we located the APA using contrast enhanced CT scans and assessed its relation to the HRCTV to find possible effect of HR-CTV size on the position of APA. There was a statistically significant correlation between APA and maximum HRCTV width, and between APA and HRCTV height (Pearson correlation coefficient of 0.472 and 0.43 respectively). Therefore, the regression equations can be used to approximately define the APA position using HRCTV measures.
According to the correlations provided, the lateral APA (y axis) distance based on maximum HR CTV width can be defined approximately as A (cm) = 0.192 × (maximum HR CTV width) +2.537. The vertical APA (x axis) distance based on HR CTV height can be defined approximately as A (cm) = 0.219 × (HRCTV height) + 0.633. Thus the point (x,y) gives an approximate estimate of position of true anatomical point. These relations give fairly appropriate location of APA which provides adequate coverage to the target tissue volume (Para-cervical tissue where ureter and uterine arteries cross) where the dose really matters. Hence this point can be used in point-based brachytherapy to specify the dose instead of the geometric point A to individualize point base brachytherapy if and only if the target coverage and critical organ sparing is achievable. Also, in 3D volume-based brachytherapy this individualized point A can be used to report instead of the Manchester point A as it represents the true dose limiting point. Strictly, the applicability of this point for dose specification should be verified before using clinically on a 3D image-based treatment planning setting, by comparing the HRCTV coverage, Organ at risk doses (bladder, rectum) when the dose is prescribed to the Manchester point A versus, to the individualized point A.
Although it is not possible to detect APA on planning CT scans, the individualized APA approximation based on above equations can be calculated simply by measuring the HRCTV dimensions. In a 3D brachytherapy setup, this can be done using Brachytherapy planning CT data and on a limited setup, EBRT planning CT scans can be used to measure HRCTV dimensions. As discussed earlier, there is no statistically significant change in APA position due to the radiotherapy treatment, which justifies the use of EBRT planning CT data for APA calculation.
The present study only formulated a model to approximately locate the position of the point A (individualized) to guide modification but did not prove the clinical applicability with regard to dose distribution. The study also assessed the correlation between APA and Multiple anatomic dimensions; however, we failed to find a significant correlation between APA and any of the measured anatomical structures (Femoral head distance, maximum pelvic cavity dimensions in AP projection and vertical distance from the level of iliac crest to the level of femoral heads).
A limitation of the study which may probably affect the reliability of the study is that the sample data was taken when the patient had a comfortably full bladder which is not practiced the same during the brachytherapy treatments (bladder catheterized). Bladder filling may have an impact on the shape of the HRCTV and hence the HRCTV dimensions. But since we used the CT data of patients whose uterus is surgically excised, the effect of bladder filling on the HRCTV dimensions is ignored.
As accuracy of the study would increase with increased sample size, the proposed model should be verified with a greater sample size and a tighter significant level to determine the best fitting linear regression values. Accuracy of locating APA would increase if a tailored contrast protocol is used for CT scanning or if a fiducial-marker is placed during the laparotomy procedures, if followed, as explained in the literature. Reliability of sample data would increase if the original CT data is used without extracting data into secondary software. The clinical applicability of the proposed model must be tested in a 3D brachytherapy planning setting for that HRCTV volume and critical structures be contoured on the CT data, the dose coverage of HRCTV and doses to critical structures be determined when the dose is prescribed to the Manchester point A, and to the individualized point A separately. The comparison can be done by assessing dose volume histograms (DVHs) of each plan and regression patterns of normalized D90 and HRCTV measures when the dose is prescribed to point A versus to the approximated individualized point A. verification of the appropriateness of the model can be performed as a second phase of the study. If proved appropriate, this individualized point A can be used in clinical setting for limited resource institutes for individualized dose prescription simply by taking the HRCTV measures using the staging CT scan or from CT simulation scan (EBRT planning).
CONCLUSION
The results of the present study provide a hybrid approach, where the outcome is useful in 3D brachytherapy setup for individualized dose recording, and can be useful in a 2D Brachytherapy setup with limited resources to individualize dose prescription if the applicability is proved. A simple mathematical formalism is derived to calculate an individualized point A, based on HRCTV measurements which can easily be recorded from planning CT data (either EBRT or Brachytherapy) and consequently can be used in point-based dose prescription or recording as it represents the dose limiting tissue. Results of this study reveal that the dose prescription to classically defined point A may under-dose the tumor due to variable size of the tumor probably resulting in treatment failure. The study only formulated a geometric relationship which has to be further tested prior to clinical utilization and we strictly caution not to use the proposed model unless the tumor coverage and doses to critical structures are evaluated.
REFERENCES
- S. Pimple, G. Mishra. Cancer cervix: Epidemiology and disease burden. Cytojournal. 2022 Mar 29;19:21. doi: 10.25259/CMAS_03_02_2021. PMID: 35510109; PMCID: PMC9063649.
- V. Ramanathan, J. Balawardane, A.H. Dilip Kumara and S.Sarasanandarajah, 2022. Current status and future prospects of radiation oncology in Sri Lanka, Physica Medica, Volume 100, pp. 6-11.
- M. Goyal, D. Raj, T. Kehwar, J. Manjhi, B. Heintz, K. Shide and J. Barker. 2016. Anatomy-based definition of point A utilizing three-dimensional volumetric imaging approach for high-dose-rate (HDR) intracavitary brachytherapy dose prescription when treating cervical cancer using limited resources. Journal of Applied Clinical Medical Physics, 17(6), pp.69-77.
- P.M. Devlin, R.A. Cormack, C.L. Holloway and A.J. Stewart, 2016. Brachytherapy-Applications and Techniques. Demos Medical Publishing.
- M. Tod and W. Meredith, 1953. Treatment of cancer of the cervix uteri-A revised “Manchester Method”, The British Journal of Radiology, 26(305), pp.252-257.
- K. Wang, Y. Yang, K. Chao, M. Wu, H. Tai, T. Chen, M. Huang, J. Chen, T. Su and Y. Chen, 2007. Correlation of traditional point A with anatomic location of uterine artery and ureter in cancer of the uterine cervix. International Journa of Radiation Oncology, Biology, Physics, 69(2), pp.498-503.
- A. Srivastava and N.R. Datta, 2014. Brachytherapy in cancer cervix: Time to move ahead from point A?, World Journal of Clinical Oncology, 5(4), pp. 764-774.
- J.A. Stitt, J.F. Fowler, B.R.Thomadsen, D.A. Buchler, B.P. Paliwal and T.J. Kinsella, 1992. High dose rate intracavitary brachytherapy for carcinoma of the cervix: The Madison system:I.Clinical and radiological considerations. Int J Radiat Oncol Biol Phys 24(2):335-48
- K. Derks, J.L.G. Steenhuijsen, H.A. Van den Berg, S. Houterman, J. Cnossen, Paul van Haaren and Katrien De Jaeger, Impact of brachytherapy technique (2D versus 3D) on outcome following radiotherapy of cervical cancer. J Contemp Brachytherapy, 10(1):17-25.
- R. Madan, S. Pathy, V. Subramani, S Sharma, B.K.Mohanti, S. Chander, S. Thulkar, L Kumar and V Dadhwal, 2014. Comparative evaluation of two-dimensional radiography and three dimensional computed tomography based dose-volume parameters for high-dose-rate intracavitary brachytherapy of cervical cancer: a prospective study. Asian Pac J Cancer Prev. 15(11):4717-21.
- V. Ramanathan, S.C.S.M. Gamage and L.W.M.N. Jayarathna ,A study on workload of a medical linear accelerator at a high throughput cancer treatment centre in Sri Lanka, 2023. KDU Journal of Multidisciplinary Studies. 5(2): 119-124, DOI: 10.4038/kjms.v5i2.82
- V. Ramanathan, K. Gunarathne, D.C. Sampath, M.M. Rizwy, 2022. Evaluation of set-up errors and set-up margin in three-dimensional conformal radiotherapy for pelvic tumours by using electronic portal imaging device. KDU Journal of Multidisciplinary Studies. 4(2): 77-85.DOI: 10.4038/kjms.v4i2.53
- V. Ramanathan, W.A.I.U. Kumara, L.P.M. Sawandi, W.M.A.K.B. Weerakoon, N. Jeyakumaran and R. Tudugala, 2023. Evaluation of scatter dose received by the thyroid region in patients with breast cancer receiving adjuvant chest wall irradiation using 2-D radiotherapy. KDU Journal of Multidisciplinary Studies. 5(1):77- 85. DOI: 10.4038/kjms.v5i1.65
- IAEA Human Health Reports No-12, 2015. The Transition from 2-D Brachytherapy to 3-D High Dose Rate Brachytherapy.