
3D Ultrasound using 3D Phantom Models for Oculofacial Injuries in Emergencies
- Hadi Khazaei
- Danesh Khazaei
- Binita Bhattarai
- G Prasad Seethapathy
- 10-18
- Oct 30, 2023
- Microbiology
3D Ultrasound using 3D Phantom Models for Oculofacial Injuries in Emergencies
Hadi Khazaei[1],2*, Danesh Khazaei3, Nashrah Junejo4, Binita Bhattarai5, G Seethapathy6, John Lipor7, Faryar Etesami8, John Ng9
1Research Scholar and Visiting Professor, Division of Oculofacial Plastic, Orbital, and Reconstructive Surgery, Oregon Health and Science 1University, Portland, Oregon
2Department of Mechanical Engineering/Portland State University
3Student, Portland State University
4Student/Washington State University
5MD, CEI Observer/Clinical Fellow ,OHSU, Portland, Oregon
6MD, FRCS Manipal Hospital Salem INDIA)
7Associate Professor Electrical & Computer Engineering/Portland State University
8Emeritus Professor- Department of Mechanical Engineering/Portland State University
9Professor and Head, of Plastic, Orbital, and Reconstructive Surgery, OHSU, Portland, Oregon
*Corresponding Author
DOI: https://doi.org/10.51584/IJRIAS.2023.81002
Received: 15 July 2023; Accepted: 07 September 2023; Published: 30 October 2023
ABSTRACTS
The incidence of ocular trauma has been on the rise for the past few years, which urges the medical community to be more apt at diagnosing and treating this condition. An effective way to diagnose different etiologies of ocular trauma involve the use of ultrasound to visualize the anatomical layers of the eye and orbit, which is vital for deciding the best management plan. In this review article, the focus of discussion will be the accuracy of 3D ultrasound in diagnosing oculofacial injury, the function of ultrasound in stabilization and triage of visual emergencies in austere environments and prolonged field care settings. The gathered data and information will assist physicians in managing ocular trauma more effectively.
Objectives: To assess the suitability of Ultrasound as a first-line investigation for ocular trauma resulting from blast injury in a deployed military setting.
Keywords: Ocular Ultrasonography, Phantom tissue /Ocular trauma, Ocular Triage, Ocular emergencies
INTRODUCTION
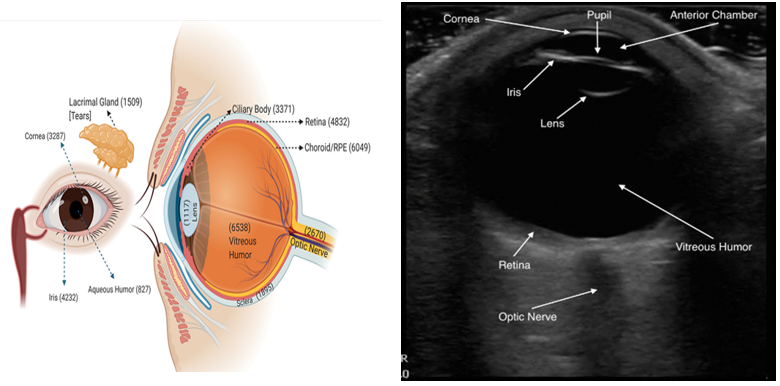
3D ultrasonography in the ambulatory and critical care setting has become an invaluable diagnostic tool for patients presenting with traumatic or atraumatic vision and ocular complaints. Sonographic bedside evaluation is intuitive and easy to perform and can accurately diagnose a variety of pathologies. These include detachment or hemorrhage of the retina or vitreous, lens dislocation, retrobulbar hematoma or air, as well as ocular foreign bodies, infections, tumors, and increased optic nerve sheath diameter that can be assessed in the setting of suspected increased intracranial pressure. The ocular anatomy is easy to visualize with sonography, as the eye is a superficial structure filled with fluid. Over the last two decades, a large number of scientific publications have documented that 3D ultrasound in emergent or critical care settings is an accurate diagnostic tool and expands and improves emergency diagnosis and management.
Ultrasound has found limited acceptance in the emergency department (ED), despite studies showing its value for the diagnosis of globe rupture, vitreous hemorrhages, retinal detachments, retrobulbar hemorrhages (9) and raised intracranial pressure. (10) In penetrating injury, in particular, this may be due to concerns about pressure on an open globe causing further damage. It is very easy to learn if one has a basic grounding in ultrasonography, (11) and if the technique is carried out with care, one should demonstrate at all times that no pressure is being applied. Expertise to deal with eye injuries on deployment is limited—ophthalmologists are available at some referral hospitals. Many smaller health care units undertaking the initial management of casualties have no CT facility. Injured civilians are transferred to local health care providers whenever the infrastructure can manage them, but these have similarly limited access to ophthalmology. It is therefore essential that potential eye injuries are identified early so that appropriate transfers can be arranged. Transfer must be reserved for those most likely to benefit from ophthalmology review. Although the prognosis for visual recovery in penetrating eye trauma is poor, there is some evidence that vision can sometimes be improved if the fragment is extracted. (12–14)
A subgroup of patients cannot comply with visual assessment (e.g., intubated in intensive care) and have injuries associated with ocular blast injury (e.g., penetrating eyelid injury) but no overt globe injury on careful inspection. These patients need to be triaged for transfer to facilities capable of managing them. 3D ultrasonography may provide a tool for this triage. (15)
A recent study of board-certified residents and attending physicians in an emergency department showed that ultrasound examinations had 100% sensitivity and 97.2% specificity for detecting globe rupture, retinal detachment, and vitreous hemorrhage. (16) Simulation training in ultrasound has been shown to improve patient safety in procedures. (17,18) and early diagnosis in a variety of areas
DISCUSSION
Ocular ultrasonography is still a novel technique in emergency medicine. Ultrasound is generally thought to be sensitive for intraocular penetrating foreign bodies but is often considered a specialist investigation. (1) CT or plain orbital views are often employed instead, especially if craniofacial or brain injuries are also suspected. (2) There is concern about the ability of non- radiologists to perform and interpret Ultrasound. (3-7) These are sensitive for metallic foreign bodies, but in the context of an IED injury, they may be less so. (4) Non-metallic penetrating foreign body is relatively uncommon outside this arena but does still occur; therefore, the findings are relevant wherever access to an ophthalmologist is difficult. (5) Also, there is concern that probe pressure on an open globe could extrude the ocular contents. We require an ultrasonically visible layer of gel between the probe and the eyelid proving that no pressure is applied. (8) Despite these limitations, there can be no doubt that Ultrasound shows promise in the assessment of the blast-injured globe. In the military context, where transfer for gold standard assessment may be difficult and dangerous, it may prove to be a useful triage tool. (9)
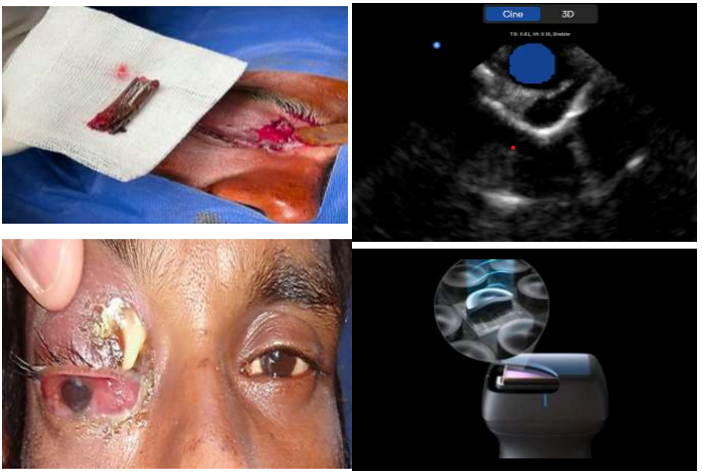
“Image courtesy of Professor G. Seethapathy MD, FRCS Manipal Hospital Salem INDIA”.
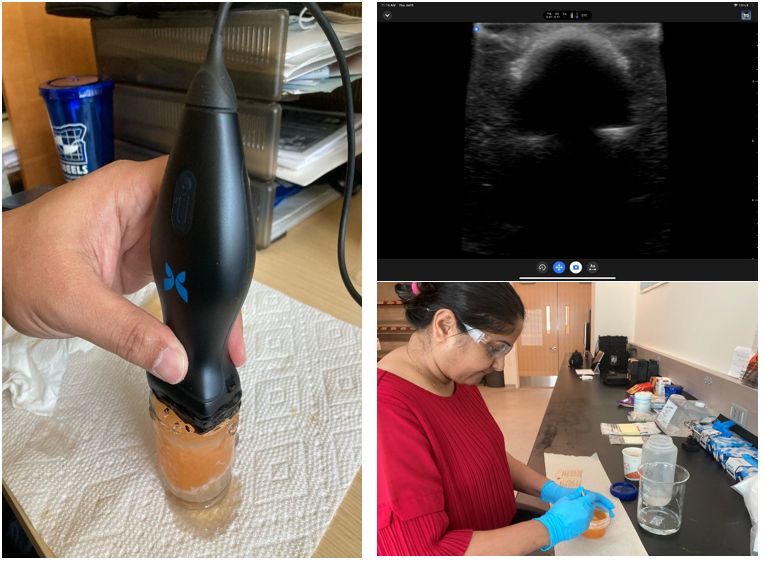
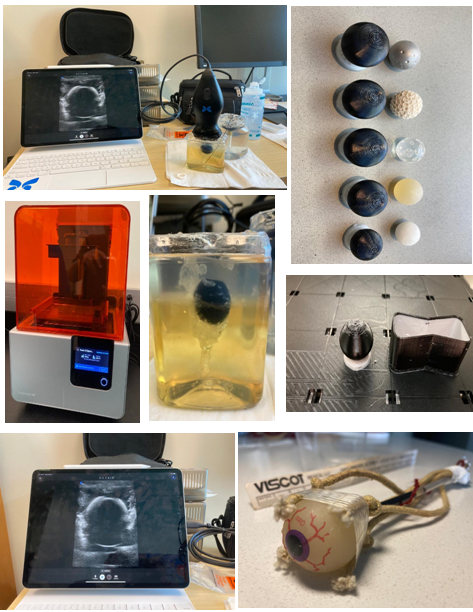
The biometric parameters of the eye can also be measured/learned using an ultrasound of the phantom eye at the appropriate positions or the correct diagnostic planes. We use the Butterfly IQ plus, which is interfaced with 3D facilities to collect and process the data and generate the final ultrasound image. The Anatomically Intelligent Ultrasound (AIUS) imaging technology deploys an Ultrasound Phantom Dataset with DNN Evaluations advanced organ modeling and imaging technique to generate a three-dimensional image of the ocular phantom using the default settings for the “Ophthalmology” imaging option. The imaging depth was set to 5cm and captured at a 10Hz frame rate. Sufficient ultrasound gel is applied on the phantom model to ensure acoustic coupling with the probe, thereby reducing acoustic impedance, and enabling clear imaging. We executed two protocols to collect the images used in this dataset:
(1) Protocol-I: The probe is placed on the phantom surface and navigated to the correct diagnostic planes that can be used for the measurement of the three primary biometric parameters of the eye, namely the horizontal plane, which is used to obtain the transverse diameter, the vertical standard plane, which is used to estimate the eye circumference , and the sagittal standard plane, which is used to estimate the optic nerve diameter. The correct diagnostic planes were identified using the proposed research protocol. To further enrich the dataset, after the acquisition of several frames at the correct diagnostic plane, we tilt, rotate, or traverse the ultrasound probe in random directions to collect more information.
(2) Protocol-II: The focus of this protocol is to obtain images capturing the anatomies of the phantom eye in the generated images. We do this by navigating the probe to obtain the lacrimal gland, optic nerve, muscles and orbital fats, individually or combined, in the picture and move the probe in different directions to obtain a heterogeneous set of images capturing the orbital anatomies. Furthermore, the phantom tissue model was also rotated and placed in the four possible orientations [head up or down, view front or back, when collecting the ultrasound data, to potentially mimic the real-life behavior of anatomical orientation and presentation. Additionally, the probe orientation was also changed between horizontal and vertical, with respect to the midline, when the data was collected to enhance the dataset with more information. Here we present some examples of eye ultrasound comparing real eye vs phantom eye tissue.
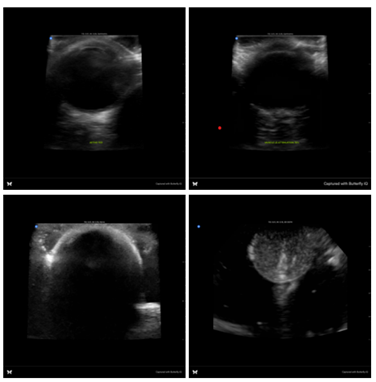
“Image taken by Butterfly IQ plus ultrasound Comparing phantom tissue vs normal eye “ www.Butterflynetwork.com
Keep in mind that creating a realistic eye phantom tissue can be challenging, as the eye has complex structures with varying acoustic properties. Advanced simulations may involve the use of different materials and techniques, such as incorporating materials with different densities or using layered phantoms to simulate the different layers of the eye. It’s important to note that creating a high-fidelity 3D model of the eye and orbit structure for ultrasound systems require specialized skills, software, and access to appropriate medical imaging data. Collaboration with medical professionals and experts in medical imaging and 3D modeling may be beneficial for a more accurate and realistic representation.
“Image Courtesy of Dr. Binita Bhattarai MD Ophthalmology, Ex-Fellow CEI , Nepal”
Creating a phantom tissue for ultrasound systems typically involves using a combination of materials that mimic the acoustic properties of human tissues. While it’s not possible to precisely replicate all the characteristics of real tissue, you can create a phantom that simulates some of the key features.
Use the ultrasound system to scan the eye phantom, like how you would scan a real eye. Adjust the settings, such as frequency and gain, to obtain optimal ultrasound images. Evaluate the phantom’s performance in terms of simulating the eye structures and their acoustic properties. Additional materials to mimic specific eye structures (e.g., acrylic balls for lens simulation). Convert imaging data into a 3D model: Use specialized medical imaging software, such as Mimics to convert the acquired imaging data into a digital 3D model. This involves segmenting the relevant structures of the eye and orbit from the imaging data to create a detailed representation. Validate the model: Use the 3D printed eye and orbit structure model with ultrasound systems to verify its accuracy and functionality. Perform ultrasound scans on the model and compare the results to real-world ultrasound images to assess its fidelity and usefulness as a training or simulation tool.
How to make a phantom tissue for ultrasound:
Creating a phantom tissue for ultrasound systems typically involves using a combination of materials that mimic the acoustic properties of human tissues. While it’s not possible to precisely replicate all the characteristics of real tissue, you can create a phantom that simulates some of the key features. Here’s a general procedure to make a basic phantom tissue for ultrasound:
MATERIALS AND METHODS
Gelatin or agar powder, Water, Containers (such as molds or trays), Ultrasonic coupling gel
Optional: Additional materials to simulate specific tissue properties (e.g., additives for echogenicity or scattering)
Procedure:
Prepare the gelatin/agar mixture: Follow the instructions on the gelatin or agar powder package to create a gelatin solution. Generally, this involves dissolving the powder in hot water and allowing it to cool. Use the recommended ratio for a firm, yet flexible, gelatin. Pour the gelatin mixture into the containers or molds, filling them to the desired thickness. You can use rectangular or cylindrical containers depending on your needs. Set the gelatin: Allow the gelatin to cool and solidify completely. This may take several hours or overnight, depending on the size and depth of the containers.
Optional: Add additional materials: If you want to simulate specific tissue properties, you can mix additives into the gelatin mixture before pouring it into the containers. For example, you can add materials that provide echogenicity (reflecting sound waves) or scattering (diffusing sound waves) to mimic certain tissue characteristics. These additives can be in the form of small particles, such as glass beads, ground rubber, or titanium dioxide.
Prepare the phantom for scanning: Once the gelatin has set, remove it from the containers or molds and place it on a suitable surface. Ensure the surface is smooth and flat to facilitate ultrasound scanning.
Apply coupling gel: Before scanning, apply a layer of ultrasonic coupling gel on the surface of the phantom. This gel helps transmit the sound waves between the ultrasound probe and the phantom, simulating the coupling between the probe and human skin.
Perform ultrasound scanning: Use the ultrasound system as you would with human subjects, placing the probe on the gel layer and scanning the phantom tissue. You can evaluate the ultrasound images and assess the phantom’s performance in terms of tissue-like characteristics.
Remember, this is a basic method to create a phantom tissue for ultrasound systems. For more advanced and accurate simulations, additional techniques and materials may be required.
Creating an eye phantom tissue for ultrasound systems involves simulating the acoustic properties of the different structures within the eye. Additional materials to mimic specific eye structures (e.g., acrylic balls for lens simulation). Familiarize yourself with the anatomy and acoustic properties of the eye structures you want to simulate, such as the cornea, lens, and vitreous humor. This will help guide your phantom creation process.
Choose an appropriate 3D printing method: Select a 3D printing method that suits your needs and available resources. Common options include stereolithography (SLA), selective laser sintering (SLS), or fused deposition modeling (FDM). Consider the resolution, material properties, and printing capabilities of the chosen method.
3D prints the model: Send the prepared 3D model file to the chosen 3D printer and initiate the printing process. Follow the manufacturer’s guidelines for your specific printer to ensure successful printing. This step may take several hours or longer, depending on the size and complexity of the model.
Post-processing: Once the 3D printing is complete, perform any necessary post-processing steps to refine the printed model. This may involve removing support structures, sanding or polishing the surfaces, or applying a coating for a smooth finish.
Validate the model: Use the 3D printed eye and orbit structure model with ultrasound systems to verify its accuracy and functionality. Perform ultrasound scans on the model and compare the results to real-world ultrasound images to assess its fidelity and usefulness as a training or simulation tool.
Keep in mind that creating a realistic phantom eye tissue can be challenging, as the eye has complex structures with varying acoustic properties. Advanced simulations may involve the use of different materials and techniques, such as incorporating materials with different densities or using layered phantoms to simulate the different layers of the eye.
FUTURE PLANNING
Medical imaging is important in clinical diagnosis and individualized treatment of eye diseases. Ultrasound imaging is one of the most prominent technologies to evaluate the orientations, anomalies and anatomical features of the eye and orbit. However, the interpretation of the data obtained from such studies is best left to expert physicians and technicians who are trained and well-versed in analyzing such images. This technology can provide high-resolution information regarding anatomic and functional changes. In recent years, imaging techniques have developed rapidly, together with Therapeutic advances. However, with the increasing sophistication of imaging technology, comprehension and management of eye disease has become more complex due to the large numbers of images and findings that can be recorded for individual patients, as well as the hypotheses supported by these data. Thus, each patient has become a “big data” challenge. Conventional diagnostic methods greatly depend on physicians’ professional experience and knowledge, which can lead to a high rate of misdiagnosis and wastage of medical data. The new era of clinical diagnostics and therapeutics urgently requires intelligent tools to manage medical data safely and efficiently.
Ultrasound imaging, widely employed in various medical fields, offers several advantages for evaluating optic nerve neuropathy. It provides real-time, dynamic imaging of tissues, is non-invasive, cost-effective, and can be conducted at the bedside. (31) These features make ultrasound an attractive option for detecting optic nerve abnormalities. Phantom tissue models, designed to mimic the acoustic properties of human ocular tissues, are invaluable for preliminary investigations and method development. They provide a controlled and reproducible environment for refining ultrasound techniques and assessing their diagnostic potential. (32) Real tissue, on the other hand, represents the complexity of human anatomy and physiology, acting as a crucial bridge between controlled experimental settings and clinical application.
CONCLUSIONS
3D Ultrasound offers a sensitive screening tool for penetrating foreign bodies or blast injury to the globe. It may even be more sensitive than CT scan. Ultrasound is portable, cheap, and easy to interpret. Careful assessment by an appropriately trained practitioner in selected cases allows a high-yield, low-risk examination. We recommend that patients with suspected eye injuries should undergo careful 3D ultrasound examination by appropriately trained personnel as part of a process of triage for ophthalmological assessment.
Relevant ocular ultrasound experience to obtain information regarding the (1) diagnostic plane, (2) eye orientation, (3) ocular anatomy, and (4) their anomalies, using box annotations. The generated dataset is used to train a variety of deep learning models to illustrate the model’s ability to extract vital information, which can be used to accurately distinguish among an Ultrasound Phantom Dataset with DNN Evaluations the classes in different categories and detect the anomalies. Furthermore, to evaluate their deployability in portable resource-constrained devices, we evaluated the capability of a smaller DNN compressed using pruning and quantization to illustrate that smaller DNNs are equally competent at extracting relevant information from the dataset and are capable of execution on resource-constrained devices and embedded platforms.
DECLARATION OF HELSINKI
This review is adhered to the ethical principles outlined in the Declaration of Helsinki as amended in 2013. (https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/).
Funding: NIH training grant: OT20D032644
Conflict of interest: The corresponding author(H.KH) is Research scholar and visiting professor, Division of Oculofacial Plastic, Orbital, and Reconstructive Surgery, Oregon Health and Science University, Portland, Oregon and Department of Mechanical Engineering/Portland State University. AI-READI NIH funded training program intern, UCSD.
AUTHORS’ CONTRIBUTION ACKNOWLEDGEMENT
All the concerned authors jointly edited and approved the final manuscript. The authors thank Dr. Kaneez Abbas for her critical feedback and assistance in developing the search strategy and for proof reading.
With special thanks to the Department of Mechanical Engineering/Portland State University staff and students for helping us set up the phantom laboratory and imaging departments.
REFERENCES
- Khazaei H, Khazaei D, Ashraf D, Mikkilineni S, Ng JD. Overview of Orbital Ultrasonography. Ann Ophthalmol Vis Sci. 2022; 5(1): 1028.
- Joseph DP, Pieramici DJ, Beauchamp NJ: Computed tomography in the diagnosis and prognosis of open globe injuries. Ophthalmology 2000;107: 1899–906.
- Arey ML, Mootha VV, Whittemore AR, Chason DP, Blomquist PH: Computed tomography in the diagnosis of occult open globe injuries. Ophthalmology 2007; 114: 1448–52.
- Turkcuer I, Atilla R, Topacoglu H, et al: Do we really need plain and soft-tissue radiographies to detect radiolucent foreign bodies in the IED. Am J Emerg Med 2006; 24(7): 763–8.
- Bray PW, Mahoney JL, Campbell JP: Sensitivity and specificity of ultrasound in the diagnosis of foreign bodies in the hand. J Hand Surg Am 1995; 20(4): 661–6.
- Oikarinen KS, Nieminen TM, Makkarainen H, Pyhtinen J: Visibility of foreign bodies in soft tissue in plain radiographs, computed tomography, magnetic resonance imaging and ultrasound. An in vitro study. Int J Oral Maxillofac Surg 1993; 22(2): 119–24.
- Aras MH, Miloglu O, Barutcugil C, Kantarci M, Ozcan E, Harorli A:Comparison of the sensitivity for detecting foreign bodies among conventional plain radiography, computed tomography and ultrasonography. Dentomaxillofacradiol 2010; 39(2): 72–8.
- Blaivas M, Theodoro D, Sierzenski P: A study of bedside ocular ultrasonography in the emergency department. Acad Emerg Med 2002; 9:791–9.
- Blaivas M: Bedside emergency department ultrasonography in the evaluation of ocular pathology. Acad Emerg Med 2000; 7(8): 947–50.
- Soldatos T, Chatzimichail K, Papathanasiou M, Gouliamos A: Opticnerve sonography: a new window for the non-invasive evaluation of intracranial pressure in brain injury. Emerg Med J 2009; 26:630–4.
- Sargsyan AE, Dulchavsky AG, Adams J, Melton S, Hamilton DR,Dulchavsky, SA: Detection of simulated intra-ocular foreign bodiesby minimally trained personnel. Avait Space Environ Med 2008; 79(1):58–61.
- Weichel ED, Colver MH: Combat ocular trauma and systemic injury. Curr Opin Opthalmol 2008; 19(6): 519–25.
- Colyer MH, Chun DW, Bower KS, Dick JS, Weichel ED: Perforating globe injuries during operation Iraqi Freedom. Ophthalmology 2008;115(11): 2087–93.
- Colyer MH, Weber ED, Weichel ED, et al: Delayed intraocular foreignbody removal without endophthalmitis during operations Iraqi Freedom and Enduring freedom. Ophthalmology 2007; 114: 1439–47.
- Sawyer N: Ultrasound imaging of penetrating ocular trauma. J EmergMed 2009; 36(2): 181–2.
- Blaivas M. Bedside emergency department ultrasonography in the evaluation of ocular pathology. Acad Emerg Med 2000; 7:947–950.
- Evans LV, Dodge KL, Shah TD, et al. Simulation training in central venous catheter insertion: improved performance in clinical practice. Acad Med 2010; 85:1462–1469.
- Keenan SP. Use of ultrasound to place central lines. J Crit Care 2002; 17:126–137
- Sharma R, Brunette DD. Ophthalmology. In: Marx J, HockbergerR,Walls R (eds). Rosen’s Emergency Medicine. 7th ed. Philadelphia, PA: Elsevier Mosby; 2010:226–239.
- Blaivas M. Bedside emergency department ultrasonography in the evaluation of ocular pathology. Acad Emerg Med 2000; 7:947–950.
- Evans LV, Dodge KL, Shah TD, et al. Simulation training in central venous catheter insertion: improved performance in clinical practice. Acad Med 2010; 85:1462–1469
- Keenan SP. Use of ultrasound to place central lines. J Crit Care 2002; 17:126–137.
- Yan H, Ahmed AS, Han J, Cui J, Yu J. A vitreous hemorrhage animal model in rabbits using force percussion injury. Curr Eye Res 2009; 34:717–726.
- Glickman RD, Maswadi SM, Dodd SJ, Gao J. Mapping 3-dimensional temperature gradients using magnetic resonance thermography in an ocular phantom during laser-induced hyperthermia. Invest Ophthalmol Vis Sci 2003; 44: e-abstract 3631.
- Kendall JL Faragher, JP. Ultrasound-guided central venous access: a homemade phantom for simulation. CJEM2007; 9:371–373.
- Madsen EL, Frank GR, Dong F. Liquid or solid ultrasonically tissue-mimiicking materials with very low scJun Shi, Shichong Zhou, Xiao Liu, Qi Zhang, Minhua Lu, and Tianfu Wang. Stacked.deep polynomial network-based representation learning for tumor classification with small ultrasound image dataset. Neurocomputing, 194:87–94, 2016.
- Zahra Sobhaninia, Shima Rafiei, Ali Emami, Nader Karimi, Kayvan Najarian, ShadrokhSamavi, and SM Reza Soroushmehr. Fetal ultrasound image segmentation for measuring biometric parameters using multi-task deep learning. In 2019 41st annual international conference of the IEEE engineering in medicine and biology society (EMBC), pages 6545– 6548. IEEE, 2019.
- 28- Vivienne Sze, Yu-Hsin Chen, Tien-Ju Yang, and Joel S Emer. Efficient processing of deep neural networks: A tutorial and survey. Proceedings of the IEEE, 105(12):2295–2329, 2017.
- Jeya Maria Jose Valanarasu, Rajeev Yasarla, Puyang Wang, Ilker Hacihaliloglu, and Vishal M Patel. Learning to segment brain anatomy from 2d ultrasound with less data. IEEE Journal of Selected Topics in Signal Processing, 14(6):1221–1234, 2020.
- Thomas LA van den Heuvel, Dagmar de Bruijn, Chris L de Korte, and Bram van Ginneken. Automated measurement of fetal head circumference using 2d ultrasound images. PloS one, 13(8): e0200412, 2018.
- Bergès O, Koskas P, Lafitte F, Piekarski JD. Echographie de l' oeil et de l' orbite avec unéchographe polyvalent [Sonography of the eye and orbit with a multipurpose ultrasound unit]. J Radiol. 2006;87(4 Pt 1):345-353. doi:10.1016/s0221-0363(06)74012-4
- Silverman RH. Focused ultrasound in ophthalmology. Clin Ophthalmol. 2016; 10:1865- 1875. Published 2016 Sep 27. doi:10.2147/OPTH.S99535
FOOT NOTES
[1]Research scholar andvisiting professor, Division of Oculofacial Plastic, Orbital, and Reconstructive Surgery, Oregon Health and Science University, Portland, Oregon and Department of Mechanical Engineering/Portland State University.AI-READI NIH funded training program intern, UCSD.