
Assessment and Analysis of Incidence of Urinary Schistosomiasis and Socio-Economic Status Among Secondary Schools Students in Kano State Metropolis
- Zubaida Hamza Muhammad
- Yahya Sabo
- Abubakar Balarabe Isah
- 35-44
- Mar 28, 2024
- Education
Assessment and Analysis of Incidence of Urinary Schistosomiasis and Socio-Economic Status Among Secondary Schools Students in Kano State Metropolis
Zubaida Hamza Muhammad1, Yahya Sabo2, Abubakar Balarabe Isah3
1Department of Biology Sa’adatu Rimi College of Education Kumbotso, Kano State, Nigeria
2Department of Psychology Sa’adatu Rimi College of Education Kumbotso, Kano State, Nigeria
3Department of Computer Science Sa’adatu Rimi College of Education Kumbotso, Kano State, Nigeria
DOI: https://doi.org/10.51584/IJRIAS.2024.90304
Received: 05 March 2024; Accepted: 19 March 2024; Published: 28 March 2024
ABSTRACT
The objective of this study was to determine the incidence of urogenital schistosomiasis in relation to the socio-economic status of senior secondary school students in urban areas of Kano State. A cross-sectional research design was used. Three hundred and eight (308) students were randomly selected, of which one hundred and thirty-six (136) were male and one hundred and seventy-two (172) were female. A self-developed questionnaire and a standard urine filtration technique were used to collect data. The questionnaire was validated by experts from public health, Murtala Muhammad Specialist Hospital and Aminu Kano Teaching Hospital with a validity index of 0.89. Urine samples from 308 randomly selected students aged 12->20 years were collected and examined for the presence of Schistosoma haematobium egg(s) in the urine using standard filtration techniques. 126 (40.90%) students were found to be Schistosoma haematobium positive with a mean egg intensity (S.D) of 50.69 (44.57) eggs per 10 milliliter of the urine. Students infected with S. haematobium were found to be from both poor and well socio-economic background. It is recommended that government and all stake holders concern should ensure appropriate measures of preventing incidence of Schistosoma haematobium.
Keywords—secondary school students; socioeconomic status; urban areas; urinary schistosomiasis;
INTRODUCTION
Schistosomiasis, a neglected tropical disease caused by the parasitic genus Schistosoma, ranks as the second most economically devastating parasitic ailment following malaria. This water-borne sickness, also known as bilharziasis, is prevalent among rural residents and remains a significant health concern in developing countries. According to [1], it affects rural populations most frequently, posing a substantial health risk. Approximately 200–300 million individuals in Africa, South America, the Caribbean, the Middle East, China, and Southeast Asia suffer from this illness [3,4]. Urinary schistosomiasis, caused by Schistosoma haematobium, a flatworm belonging to the widely observed group of digenetic blood trematodes, has been documented in various regions of the country with varying degrees of intensity and prevalence rates. There is a growing belief that the incidence of urinary schistosomiasis is on the rise [5,6]. Ranking as the second most impactful human parasitic disease in terms of socioeconomic consequences and public health concerns in tropical and subtropical regions, it follows closely behind malaria [7]. Despite being among the most disliked tropical diseases, this ailment stands as the most prevalent water-borne disease and a significant health menace in underdeveloped nations. Numerous studies indicate the presence of this parasitic illness in Nigeria, with prevalence varying across different areas [8].
Schistosomiasis stands out as a highly prevalent and significant neglected tropical disease in sub-Saharan Africa, with the primary disease burden attributed to Schistosoma mansoni and S. haematobium [9,10]. Transmission of S. haematobium occurs through freshwater snail species belonging to the genus Bulinus, which comprises about 36 species distributed across four species groups [11]. The outcomes for individuals infected with S. haematobium vary widely, ranging from mild to severe damage to the kidneys and/or bladder [12]. The distinctive clinical manifestation involves terminal hematuria, often accompanied by an increased frequency of urination and dysuria [13]. The pathology of urinary schistosomiasis is primarily instigated by the eggs laid by female S. haematobium adult worms residing in the venous plexus of the bladder and other pelvic organs. As these eggs traverse the bladder mucosal tissue on their way out through the urinary stream, they cause significant damage and initiate granulomatous inflammation. This inflammatory process can progress over many years, leading to complications such as fibrosis and bladder cancer [14-16].
While Schistosomiasis control programs have achieved notable progress, the disease burden remains substantial in Africa, with the sub-Saharan region accounting for approximately 90% of infections [17]. In South Africa, S. haematobium infection is endemic, particularly in the province of KwaZulu-Natal, where the prevalence in the Mkha-nyakude District was reported to be 37.5% in 2015 [20]. Individuals contract the infection during various activities, including domestic, occupational, and recreational pursuits that expose them to water containing cercariae from intermediate host snails.
Several factors contribute to the spread of Schistosomiasis in endemic areas, including climate change, proximity to water bodies, irrigation practices, dam construction, and socio-demographic factors [9,21,20]. The development of irrigation schemes and dam construction, driven by insufficient rainfall due to seasonal variations and community needs, influences migration from both endemic and non-endemic areas into project areas, introducing Schistosomiasis [23,26]. School children are particularly vulnerable to infection due to their frequent contact with infested water, with the risk decreasing progressively in adulthood [27].
The disease is associated with various factors that significantly correlate with its spread in different regions of the country. These factors encompass low socioeconomic status, lack of access to clean water, inadequate basic infrastructure, relatively poor housing quality, and insufficient environmental sanitation [28].
In light of what is examined from the literature and the gap identified, there is need to investigate the incidence of Urinary Schistosomiasis and its associated risks factors in urban areas whether the disease affect students’ students from well socio-economic background with the believe that urban areas are said to have been provided with clean and safe water, good environment sanitation etc. Most of the study on Schistosomiasis was conducted in rural areas and disease incidence has been reported to be affecting people from poor socio-economic background. Recent studies on Urinary Schistosomiasis reported its prevalence in urban areas [29-30]. This research study was design to be conducted in urban areas as findings shows prevalence of Schistosomiasis in urban areas that are not here in Kano State Metropolis.
Objective(s) of the Study
- To investigate the occurrence and severity of Urinary Schistosomiasis among secondary school students in urban areas within the Kano State Metropolis.
- To determine Influence of Urinary Schistosomiasis in relation to Socio-Economic status among Secondary School Students in Urban Areas of Kano Metropolis.
Research Questions
- What are the Incidence and Intensity of Urinary Schistosomiasis among Secondary School Students in Urban Areas of Kano Metropolis?
- Is there relationship among Urinary Schistosomiasis incidence and Socio-Economic status of Secondary School Students in Urban Areas of Kano Metropolis?
Problem Statement
The parasitic disease “Schistosomiasis” is one of the 20 ailments identified as neglected tropical infections by World Health Organization. It frequently has adverse environmental effects and seriously affects rural networks. It significantly affects cognitive development impairment and handicap, which have an adverse effect on students’ academic performance [31]. Studies shows that socio-economic status is one of the risks factor associated with incidence of Urinary Schistosomiasis and has been found to be affecting people from poor socio-economic background. Numerous studies may have indicated the prevalence of urinary Schistosomiasis in urban and peri urban settings, but none have been discovered to have been carried out in Kano state’s urban districts. Because most studies on Schistosomiasis were conducted in rural regions, the incidence of urinary Schistosomiasis in urban settings has to be investigated in light of the aforementioned findings.
MATERIALS AND METHOD
Study Sites
The study sites comprised eight urban areas in Kano metropolis among which include; Municipal, Gwale, Fagge, Tarauni, Dala Nassarawa, Kumbotso and Ungoggo local government area.
The Kano metropolis study area is situated between the latitude 11°05′ N to 12°07′ N and longitude 8°23′ E to 8°47′ E, with an altitude of 472 meters above sea level. It shares borders with Minjibir LGA to the North East, Gezawa LGA to the East, Dawakin Kudu LGA to the South East, and Madobi and Tofa LGAs to the South West. As the second-largest industrial and commercial center in Nigeria after Lagos, Kano Metropolis has undergone rapid population growth. In 2006, the population stood at 2.828,861 million, according to the National Population Commission of Nigeria (NPC) and National Bureau of Statistics (NBS) 2006 Report. By 2022, the population had increased to 4.648,400 million (NPC and NBS, 2022), covering an area of approximately 499 square kilometers.
The population density within the Kano closed-settled zone is around 1000 inhabitants per km², significantly higher than the national average of 267 inhabitants per km². Kano Metropolis has become one of the most densely populated cities, with a substantial migrant worker population growing at a rate of 30 to 40 percent per annum (UNDP 2004). Over time, it has evolved into a cosmopolitan city, representing various ethnic groups.
The metropolis includes six core urban local governments (Dala, Fagge, Gwale, Kano Municipal, Nassarawa, and Tarauni) and two peri-urban local governments (Kumbotso and Ungogo). While residential areas dominate the study area, commercial, institutional, and educational land uses are also distributed throughout. Industrial layouts such as Dakata, Sharada, and Bompai host industries like steel rolling, packaging, and beverage processing.
Commercial activities in the area have witnessed rapid growth, with prominent markets such as Sabon Gari, Kantin Kwari, Singer market, Dawanau, and Yankaba contributing to the bustling economic landscape.
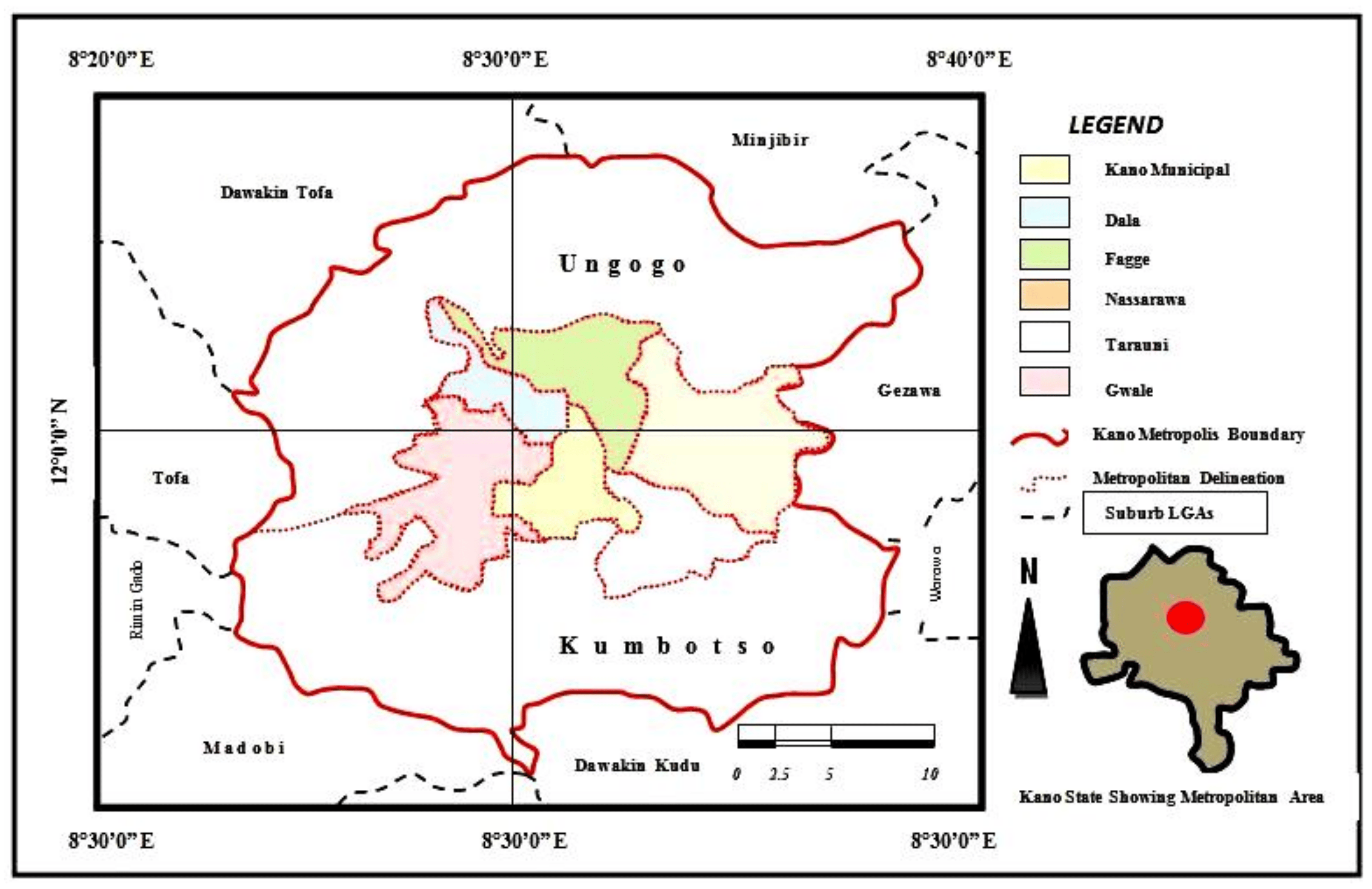
Figure 1. Map of Kano State indicating Urban Areas
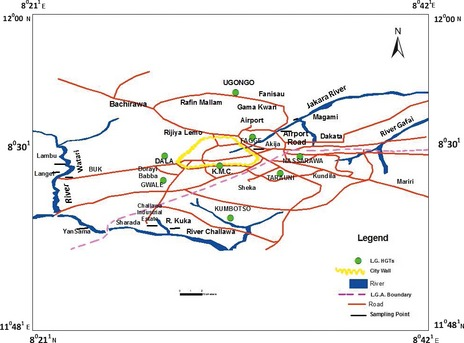
Figure 2 Map showing Kano State Metropolis
The researcher selected four local government areas which are Dala, Kumbotso, Municipal and Nassarawa to represent the case study area. The choice of the areas is being an urban area in Kano State and the need to find out Incidence of Schistosomiasis in urban areas. Multistage sampling technique was employed where cluster sampling technique was used to select the four local government areas, which are Dala, Kumbotso, Municpal and Nassarawa. Stratified sampling technique was used to select three males and three females’ secondary schools in each local government making a total of six 6 schools in each local government and a grand total of twenty-four 24 schools sampled for the study.
Study Design, Population and Sampling Size
The study employed cross sectional research design. The population comprises of all secondary schools’ students in Kano metropolis. They are thirty eight thousand four hundred and ninety seven (38,497). A sample size of three hundred and seven one (371) participants were sampled according to Research Advisor table of determining sample size. Out of these three hundred and seven one (371) participants sampled, only three hundred and eight (308) students responded to participate in the research.
Method of Data Collection
Before the commencement of the study, informed consent letter was presented to the local head of the selected local government, the executive secretary Kano State Senior Secondary Schools Management Board and also the executive secretary Kano State Hospital Management Board to explain to them the objectives and plan of the study in order to get their cooperation and permission to conduct the study. The selected schools were visited few days before the collection of urine sample and administering the questionnaire and the interview to brief the schools’ authorities, teachers, and students on the study purpose and outlined. Thereafter, students were randomly selected and provided with information leaflets and consent forms, which was written in Hausa language to take to their parents or guardians. On the next day, the research study team collected the data from the students with signed consent forms.
Questionnaire survey
Questionnaire was administered to the students who are to participate in the study. The questionnaire contains information on students demographic data (age, gender and family size), socioeconomic background (educational level and occupation), behavioural risks (personal hygiene such as types of water supply and water contact activities), and health conditions (symptoms of haematuria infection,). The participants were also interviewed by the researchers and the research assistants who received a specific training on how to apply the questionnaire and conduct the interview on participants’ socio-economic status.
Parasitology
After administering the questionnaire, participants were provided with wide-mouth 100 mL screw-capped containers, pre-labelled with their names and codes, for the collection of urine samples. Within 5 hours of collection, the samples were transported in suitable cool boxes, maintaining temperatures between 4 and 6 °C, to Murtala Muhammad Specialist Hospital in Kano, Nigeria, for subsequent examination. All urine samples underwent scrutiny for haematuria using a standard urine filtration technique. S. haematobium egg counts were conducted and recorded as eggs per 10 millilitres of urine (EP10 mL). Additionally, 20% of the samples underwent re-examination for Schistosoma egg presence by another parasitologist to ensure data quality. The collected data were analyzed by two independent statistical experts using the Statistical Package for Social Science (SPSS) Software. The researchers crosschecked the two datasets for accuracy and created a unified dataset for further analysis. Demographic, socioeconomic, environmental, and behavioral characteristics were treated as categorical variables and presented as frequencies and percentages. Egg counts were analyzed using mean and standard deviation to provide a summary of Schistosoma haematobium egg counts in the examined urine samples.
Ethical statement
This research study adhered to the guidelines outlined by the Medical Ethics Committee of the Ministry of Health in Kano State, Nigeria. Approvals were also secured from various entities, including Kano State’s Ministry of Health, the Kano State Hospitals Management Board, local government authorities, and the district heads of communities. Consent from research participants in each school was sought, and the study’s objectives and procedures were clearly explained in the local Hausa language. Participants were assured of their right to withdraw from the study without facing consequences. Consequently, written and signed informed consents were obtained from the guardians/parents of all participants before commencing the survey, with approval from the ethics committees.
The Medical Ethics Committee of the Ministry of Health in Kano State, Nigeria provided guidelines for the conduct of the study, and approvals were obtained from district heads of communities, local government officials, the Kano State Hospitals Management Board, and the Ministry of Health. The study’s objectives and methods were thoroughly communicated to research participants in each school in the local Hausa language during the consent process, emphasizing their right to withdraw at any time. As a result, written and signed informed consents were obtained from the guardians/parents of all participants before initiating the survey, with approval from the ethics committees. All individuals affected by the condition were treated with a single dose of 40 mg/kg body weight of praziquantel under the supervision of a researcher, a medical officer, and the guidance and counseling focal person of each selected school (Direct Observed Therapy).
RESULTS
Table 1 shows demographic characteristics of the participants, out of three hundred and eight (308) participants (44.1% were males and 55.9% were females). Out of these, 87(28.2%) were from Dala, 75(24.3%) reside in Kumbotso, 76(24.6%) in Municipal, and 70 (22.7%) in Nassarawa local government area respectively.
Table 2 shows Incidence of Urinary Schistosomiasis among secondary schools in the study area in which out of three hundred and eight (308) urine sample of the participants examined, one hundred and twenty six (126) were found to be Schistosoma haematobium positive with mean egg intensity of (S.D) of 50.69 (44.57) egg/10 mL of urine. S
Table 3 shows the influence of Urinary Schistosomiasis on socio- economic status of the participants where majority of the respondents infected were found to be from a well socio-economic background.
Table 1 Demographic Characteristics of the Participants and Areas Studied (n = 308)
| Items | Male | Female | Total Participants (%) |
| Gender | |||
| Male | 136(44.2%) | ||
| Female | 172(55.8%) | ||
| Total | 308(100%) | ||
| Study Areas | |||
| Dala | 49 | 38 | 87(28.2%) |
| Kumbotso | 28 | 47 | 75(24.3%) |
| Municipal | 40 | 36 | 76(24.6%) |
| Nassarawa | 36 | 34 | 70(22.7%) |
| Total | 153 | 155 | 308(100%) |
Table 2 Urinary Schistosomiasis Incidence among participants Responded (n = 308)
| Number of Participants | Participants infected % | Mean egg count /10ml of urine |
| 308 | 126 (40.90) | 44.58 |
Table 3. Students’ Socio-Economic Status Responses (n = 308)
| Socio-Economic Status | Total Number | Percentage% |
| Father educational level | ||
| Tertiary | 131 | 42.3 |
| Secondary | 116 | 37.7 |
| Primary | 38 | 12.3 |
| None | 23 | 7.5 |
| Mother educational level | ||
| Tertiary | 86 | 27.9 |
| Secondary | 128 | 41.6 |
| Primary | 78 | 25.3 |
| None | 16 | 5.9 |
| Father occupation | ||
| Salary earner | 69 | 22.4 |
| Business | 159 | 51.6 |
| Farming | 26 | 8.5 |
| Trading | 54 | 17.5 |
| Mother occupation | ||
| Salary earner | 25 | 8.1 |
| Business | 179 | 58.1 |
| Trading | 86 | 27.9 |
| None | 18 | 5.8 |
| Main source of water | ||
| Tap | 35 | 11.4 |
| Well/Borehole | 136 | 44.2 |
| Water vendors | 117 | 37.9 |
| Streams | 14 | 4.6 |
| Water contact activity | ||
| Bathing | 135 | 43.8 |
| Washing | 148 | 48.1 |
| Farming | 25 | 8.1 |
DISCUSSION OF THE RESULT
The result obtained from demographic data of the respondents’ shows that majority of the participants responded were female. Out of 308 participants examined, 126 participants were infected with incidence rate of 40.9%. This finding confirmed the findings obtained from Akpet-1 community in Cross River State with 19% incidence of Urogenital Schistosomiasis.
With regards to Urinary Schistosomiasis influence on participants’ socio-economic status, this study revealed that majority of the respondents was from well socio-economic background and were also found positive with Schistosome egg. Urinary Schistosomiasis does not only affect people from poor socio- economic background as revealed from finding of other studies but also affect people from well socio-economic background. This could be resulted due to urbanization which leads to high population densities as a result of rural-urban migration , poor sanitation conditions in most of the urban areas, lack of provision of clean and safe water as findings shows that the major source of water in urban areas studied was well/borehole water with (44.2%) which mostly are constructed nearby soak ways, drainages and always open for anybody to fetch water and that somebody could be a Schistosome infected person that migrated from rural to urban for business purposes or settlement. It is also common to see some kinds of small snails habited nearby well/borehole because of the moist environment. These have been found to be contaminating the well/borehole water thereby resulting to Schistosome endemic in that particular area. Water vendors with (37.9%) are the next providing water to the urban areas studied. Most of these water vendors are from rural areas and some are even migrants and some of them poorly present themselves with dirty looks, not regularly cleaning the water can, the type of water they are providing in most cases in not clean and safe and they usually fetch the water from any source of water canal and even the water provided after some days some kind of larval stage could be observed physically inside the water and which could be a Schistosome larvae. Only (11.4%) were reported to source water from Tap water which is not on regular basis and the water distributed is poorly unclean and unsafe and sometimes with even odour indicating that the water might have been contaminated and some of the pipes have been for long not being treated. This could also lead to incidence of the disease.
This finding aligns with the results reported by [32] concerning the prevalence of urinary Schistosomiasis among primary school children in Ikwo and Ohaukwu Communities of Ebonyi State, Nigeria. The research establishes a significant correlation between Schistosomiasis infection and the socio-economic status of participants, emphasizing that reliance on contaminated water sources constitutes a crucial modifiable risk factor. Similarly, individuals with uneducated parents are more prone to urinary Schistosomiasis. The primary source of water supply and engagement in water-related activities play a substantial role in the transmission of urinary Schistosomiasis. Evidently, those who predominantly rely on river or stream water and engage in agricultural activities tend to harbor higher infection rates than others. A bivariate logistic regression analysis of factors associated with urinary Schistosomiasis within the study population reveals a close association with age, primary water source, and engagement in water-related activities.
CONCLUSION
Incidence of Urinary Schistosomiasis has been found to be a serious endemic disease in urban areas of Kano State which has been found to be of a public health importance and a serious concern as it affects both individual from either of poor or well socio-economic background.
RECOMMENDATION
- It is recommended that government and all stake holders concern should ensure appropriate measures of controlling the incidence of the disease.
- Parent should also ensure proper utilization of clean and safe water for all domestic purposes.
- It is recommended that further studies should be conducted among students in private schools
REFERENCES
- Atalabi, T.E., Adoh, S.D., Eze, K.M. (2018). The current epidemiological status of urogenital schistosomiasis among primary school pupils in Katsina State, Nigeria: An imperative for a scale up of water and sanitation initiative and mass administration of medicines with Praziquantel. PLoS Negl. Trop. Dis. 12 (7), 1–19. https:// doi.org/10.1371/journal.pntd.0006636.
- Oniya, M.O. (2007). Socio-cultural practices promoting the transmission of urinary Schistosomiasis among school aged pupils in a South Western Village in Nigeria. Research Journal of Biological Sciences; 2: 1-4.
- W.H.O 2004. Schistosomiasis division of control of Tropical Diseases, pp 5-7.
- Igumbor EO., Ojo SKS., Olateru-Olagbebi A. (2010). Detection of Urinary Schistosomiasis among School-aged Children in Ukwani LGA of Delta State Nigeria. The South Pacific Journal of Natural and Applied Sciences; 28: 48-51.
- Igumbor EO., Ojo SKS., Olateru-Olagbebi A. (2010). Detection of Urinary Schistosomiasis among School-aged Children in Ukwani LGA of Delta State Nigeria. The South Pacific Journal of Natural and Applied Sciences; 28: 48-51.
- Okon, O.E., Oduotu, M.F., Oku, E.E., Nta, A.I., Etim, S.E., Abraham, J.T & Akpan P.A. (2007). Urinary Schistosomiasis in Abini Community Biase Local Government Area, Cross River State, Nigeria. Nigeria Journal of Parasitology 2007; 28: 28-31.
- World Health Organization (2003). Manual of basic techniques for a health laboratory, 2nd Edition. World Health Organization, Geneva.
- Jimeta, B. H. & Abba, J.A. (2013). Survey of Urinary Schistosomiasis among school-aged children in the rural communities of Mayo-belwa Local Government Area, Adamawa State, Nigeria. Journal of Natural Sciences Research; Vol.3, No.4, 73
- Adenowo, A.F., Oyinloye, B.E., Ogunyinka, B.I., Kappo, A.P. (2015). Impact of human schistosomiasis in sub Saharan Africa. Braz J Infect Dis;19:196-205.
- LoVerde, P.T. (2019). Schistosomiasis. Adv Exp Med Biol; 1154:45-70.
- Rollinson, D. A. (2009). Wake up call for urinary schistosomiasis: reconciling research effort with public health importance. Parasitolog; 136:1593-1610.
- Brouwer, K.C., Ndhlovu, P.D., Wagatsuma, Y., Munatsi, A., Shiff, C.J. (2003). Urinary tract pathology attributed to schistosoma haematobium: does parasite genetics play a role? Am J Trop Med Hyg; 68:456-462.
- Barsoum, R.S. (2013).Urinary schistosomiasis: review. J Adv Res; 4:453-459.
- Honeycutt, J., Hammam, O., Fu C.L., Hsieh M.H. (2014). Controversies and challenges in research on urogenital schistosomiasis-associated bladder cancer. Trends Parasitol ;30:324-332.
- Zaghloul, M.S., Zaghloul, T.M., Bishr, M.K., Baumann, B.C. (2020). Urinary schistosomiasis and the associated bladder cancer: update. J Egypt Natl Canc Inst.; 32:44.
- Zaghloul, M.S. (2012). Bladder cancer and schistosomiasis. J Egypt Natl Canc Inst; 24:151-159.
- World Health Organization (WHO). Schistosomiasis (2015). https://www.who.int/news-room/fact-sheets/detail/schistosomiasis
- World Health Organization (WHO). Schistosomiasis (2015). https://www.who.int/news-room/fact-sheets/detail/schistosomiasis
- Kabuyaya M, Chimbari MJ, Manyangadze T, Mukaratirwa S. (2017a). Schistosomiasis risk factors based on the infection status among school-going children in the Ndumo area, uMkhanyakude district, South Africa. SAJID; 32:67–72.
- Adenowo, A.F., Oyinloye, B.E., Ogunyinka, B.I., Kappo, A.P. (2015). Impact of human schistosomiasis in sub Saharan Africa. Braz J Infect Dis;19:196-205.
- Adenowo, A.F., Oyinloye, B.E., Ogunyinka, B.I., Kappo, A.P. (2015). Impact of human schistosomiasis in sub Saharan Africa. Braz J Infect Dis;19:196-205.
- Kabuyaya M, Chimbari MJ, Manyangadze T, Mukaratirwa S. (2017a). Schistosomiasis risk factors based on the infection status among school-going children in the Ndumo area, uMkhanyakude district, South Africa. SAJID; 32:67–72.
- Adenowo, A.F., Oyinloye, B.E., Ogunyinka, B.I., Kappo, A.P. (2015). Impact of human schistosomiasis in sub Saharan Africa. Braz J Infect Dis;19:196-205.
- Chimbari M, Chirebvu E, Ndlela B.(2004). Malaria and schistosomiasis risks associated with surface and sprinkler irrigation systems in Zimbabwe. Acta Trop; 89:205– 13.
- Colley DG, Bustinduy AL, Secor WE, King CH (2014) Human schistosomiasis. Lancet 383(9936):2253–2264
- Hajissa, K.; Abd Elhafiz M. A. Muhajir, Hamza Adam Eshag, Alnzer Alfadel, Elkhatieb Nahied,
- M’Bra, R.K., B. Kone, Y.G. Yapi, K.D. Silué, I. Sy, D. Vienneau, N. Soro, G. Cissé, and J. Utzinger. 2018. Risk factors for schistosomiasis in an urban area in northern Côte d′Ivoire. Infectious Diseases of Poverty 7: 47. https://doi.org/10.1186/s40249-018-0431- 6.
- Dabo, ; Adama Z Diarra, Vanessa Machault, Ousmane Touré, Diarra Sira Niambélé, Abdoulaye Kanté, Abdoulaye Ongoiba and Ogobara Doumbo (2015). Urban schistosomiasis and associated determinant factors among school children in Bamako, Mali, West Africa http://www.idpjournal.com/content/4/1/4
- Inyang-Etoh, P. C., Akpan F.B., Opara-Osuoha, U. “Effects of Urogenital Schistosomiasis on Academic Performance and Anthropometric Parameters of School-aged Children” JMID/ 2018; 8 (2):49-54 Journal of Microbiology and Infectious Diseases doi: 10.5799/jmid. 434592
- Umoh, N.O., Nwamini, C.F., Inyang, N.J., Umo, A. N., Usanga, V. U., Nworie, A., Elom, M.O. & Ukwah, B. N. (2020). Prevalence of urinary schistosomiasis amongst primary school children in Ikwo and Ohaukwu Communities of Ebonyi State, Nigeria. Afr J Lab Med. ;9(1), a812. https://doi. org/10.4102/ajlm.v9i1.812