
Current Status of Lymphatic Filariasis in Three Selected Communities in Sagbama Local Government Area of Bayelsa State, Nigeria.
- Eze, Chinwe Nwadiuto
- Yenagoa, Bebe.Edwin
- 85-92
- Mar 30, 2024
- Environmental Impact
Current Status of Lymphatic Filariasis in Three Selected Communities in Sagbama Local Government Area of Bayelsa State, Nigeria.
Eze, Chinwe Nwadiuto and Yenagoa, Bebe.Edwin
Department of Animal and Environmental Biology, University of Port Harcourt, Choba, Rivers State, Nigeria
DOI: https://doi.org/10.51584/IJRIAS.2024.90309
Received: 01 February 2024; Revised: 04 March 2024; Accepted: 09 March 2024; Published: 29 March 2024
ABSTRACT
Current status of lymphatic filariasis in three selected communities in Sagbama LGA Bayelsa State, Nigeria was conducted between July and October, 2019. Descriptive Cross-Sectional study was carried out to determine LF prevalence, microfilaria density and W. bancrofti in mosquitoes. Blood samples were collected at night through vein puncture and examined using Giesma staining and Knott concentration techniques. Indoor resting mosquitoes were collected using pyrethrum spray technique and dissected for filarial worms. Out of 274 participants 37(13.5%) were infected of LF, Adagbabiri had the highest prevalence of 21(21.4%) followed by Sagbama 11(12.6%) and 5(5.6%) in Tungbabiri. The females were more infected than males, 22(59.5%) and 15(40.5%) respectively, there was no significant difference (P>0.05) between sex. The highest prevalence of 19.4% were recorded in ages 40-49yrs and least prevalence of 5.3% in 10-19yrs. Low microfilaria density 0.08,0.04 and 0.08 were observed among age groups, 0.10 and 0.20 between sex across 3 communities. There was no significant difference (P>0.05) of mean filarial density among age groups and sex. Participants knowledge on LF was very low but a good perception on socio economic consequences of LF was recorded across the three communities. No filaria larvae was discovered in mosquitoes of Anopheles gambiae and Culex quniquifasciatus dissected. In conclusion, although low prevalence was observed. Therefore, there is need for control programs and surveillance of LF in Sagbama Local Government Area.
INTRODUCTION
Lymphatic Filariasis (LF) is one of the Neglected Tropical Diseases (NTD) that poses major public health causing considerable morbidity as well as numerous Disability Adjusted Life Years (DALYs) among sufferers all around the world (WHO, 2010; WHO, 2013). LF remains a major cause of permanent disability in tropical and subtropical countries (WHO 2016). In Africa, with over 120 million people at risk (Brant et al., 2018). LF is a vector borne parasitic disease transmitted by the several mosquito species which include Anopheles gambiae, Anopheles funestus and Culex quenquifasciatus (Nwoke et al., 2010; James et al., 2017; Kelly-Hope et al., 2011). Human activities which include deforestation, afforestation, dam construction, agriculture and irrigation has resulted to provision of suitable breeding sites and increase of mosquitos’ populations both in the Rural and Urban area of Nigeria. Urbanization and overcrowding among humans also resulted into closeness of human settlement to breeding sites of these vectors which had resulted in better transmission of LF among humans (Nwoke et al., 2010). James et al., (2017) in a study showed that chronic clinical manifestation of LF leads to body disfigurement such as legs or arm enlargement known as elephantiasis, genital enlargement in men as well as breast enlargement in women. Inflammation of the inguinal node, fever, local warmth and chill are the acute symptoms of LF as reported by Omudu et al., (2011). Lymphatic filariasis has been documented in rural communities in the lower Cross River Basin (Udoidung et al., 2008, Okon et al., 2010), Ezza people of Ebonyi State (Anosike et al., 2005), Igwun basin of Rivers State and parts of the Niger Delta (Udonsi, 1988, Agi and Ebenezer, 2009) as well as parts of central Nigeria including rural communities in Plateau and Nasarawa States (Eigege et al., 2003). Despite the increase in health care, interventions and enlightenment towards LF by the Nigeria Nation Lymphatic Filariasis Elimination Program (NNLFEP) as well as the Federal Ministry of Health, infection and transmission was still on the increase on the daily basis with proportionate threat to human health and life (Agi and Ebenizer, 2009; Brant, et al, 2018)
MATERIAL AND METHOD
Study Area
A community based cross sectional study was conducted in Bayelsa State in three villages Sagbama, Tungbabiri and Adagbabiri from June-October 2019. Sagbama L.G.A is 5 Km from the State capital, Bayelsa and is located between latitude 50.10N-60.121 Longitude 5.670 N – 6.20E, total area of 945km2. The area is water logged with annual rainfall of about 3,000 mm3 which last for nine months; the vegetation is fresh water swampy forest (Agi and Ebenezer, 2009). The major occupation of the three communities includes subsistent farming, fishing and trading. Sagbama Community is the head quarter and the most populated community in the LGA while Adagbabiri and Tungbabiri are the only two neighboring communities to Sagbama community.
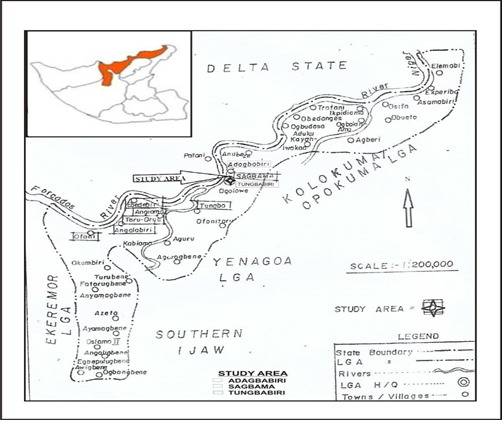
Map of the studied area
Collection of blood samples
Informed consent was obtained from participants through the community heads after sensitization and pre-notice period with the help of Community leaders, primary healthcare workers, community health mobilizers and family heads. Bio-data of each participant was obtained through a questionnaire which elicited responses for name, sex, age, occupation as well as their perception of filarial infection. Two milliliters (2ml) of blood were collected from 274 volunteers intravenously into a heparinized tube containing 0.5ml acetic acid during night hours of 10pm-2am (this is due to the nocturnal periodicity of the microfilaria worm) with the aid of a professional Laboratory Scientists. All the samples were taken to laboratory for examination.
Examination of blood samples
A modified Knott’s concentration technique described by Chessbrough (2006) was used to detect the presence of microfilariae in the blood. Species of microfilariae in positive blood samples were identified by smearing the sediments of the concentration on a slide and allowing it, to dry. The slide was stained with 8% phosphate buffer (pH 7.2) Giemsa stain. This was rinsed in buffered water and finally in distilled water and kept to dry. Microfilariae were identified and counted under the microscope using the nature of the sheath and the position of the nuclei. The microfilaria density was determined by the use of hand-count and expressed as mf/µL (Cleide et al., 1999; Cletus et al., 2012). Trained medical personnel was recruited to examine the volunteers for clinical manifestation of Lf. Both male and females were examined for signs of the limb, breast and scrotal (hydrocele) elephantiasis.
Examination of mosquitoes for infection
Mosquito vectors were trapped using residual spray inside the houses of participants across the 3 communities at hours 10pm -3am. Knock downed mosquitoes collected were transferred to a glass container with cotton wool-soaked chloroform and sent to the laboratory for identification and examination of infection. The identification of mosquitoes was done using the key prepared by Gordon and Lavopierre (Gordon & Lavoipiere, 1978). This was examined under the microscope for filarial parasite after dissection of the mosquito vectors as described by Agi and Ebenezer (2009). The head, thorax and abdomen were separated using dissecting needles. Each section of the body was teased and examined under a dissecting microscope for the presence of micro filariae
RESULT
Of the 274 persons examined for lymphatic filariasis, 37(13.5%) were infected, Adagbabiri community had the highest prevalence 21(21.4%), followed by Sagbama 11(12.6%) and Tungbabiri 5(5.6%). Prevalence of infection was higher in the females 22(15.9%) than in males 15(11.0%). Highest infection rates of 8(15.7%) and 13(27.7) were recorded in males and females in Adagbabiri respectively. Although more females were infected, the differences were not significant (P>0.05).This result also showed that 4(2.0%) of the entire sampled respondents had elephantiasis and 1(1.9%) experience swollen breast/scrotum (Table 1), just as only 1(0.5%), 0(0.0%) and 4(2.0%) of the entire sample respondents had swollen breast/scrotum, skin ruptures and crawling sensation respectively as shown in (Table 1).The age group 40-49years had the highest prevalence 6(19.4%) followed by 20-29 age group with an infection rate of 15(18.3%) and least prevalence of 5.3% among 10-19yrs (Table 2). A mean microfilarial density of 0.08, 0.04 and 0.08 was observed for Adagbabiri, Tungbabiri and Sagbama respectively, there was no significant difference (P>0.05) in mean microfilarial density across the communities Table 2. The male had a mean microfilarial density of 0.10 with 0.23, 0.03 and 0.03 for Adagbabiri, Tungbabiri and Sagbama respectively while the female had a mean microfilarial density of 0.20 with 0.35, 0.10 and 0.18 for Adagbabiri, Tungbabiri and Sagbama respectively (Table 3). Knowledge and perception on LF revealed that 16(7.8%) of the total (205) respondents knew that mosquito is the causative vector of LF, 65(27.3%) attributed ‘stepping on charm’ as the cause of LF. Also, 12(5.9%) of respondents attributed LF mode of transmission to mosquito bite, while 66(32.3%) attributed actions and inactions to witchcraft, 64(31.2%) indicated both sexual intercourse and body contact while the least 43(21.0%) attributed the mode of transmission to hereditary (Table 4). It was observed that, only 7(11.1%) of the total participant were aware of Lf prevention was to avoid Mosquitoes bite, 2(2.2%) in Adagbabiri, 3(5.0%) Tungbabiri and 2(3.9%) Sagbama (Table 5). However, 194(94.6%) believed that LF causes some level of discomfort in the public, 198(96.6%) believed that LF affect the work and income of the affected persons, while 194(94.6%) and 181(88.3%) believed that LF affects sexual relationship as well as ‘spouse desertion and divorce’ respectively (Table 5).
Table 1: Prevalence of Lymphatic filariasis and clinical signs across the three communities
| Community | Number examined | Total | Number Infected (%) | Total (%) | Number Examined
(%) |
Number with swollen legs (%) | Number with swollen breast/Scrotum
(%) |
Skin rupture
(%) |
Crawling sensation on legs (%) | ||
| Male | Female | Male | Female | Clinical Cases | |||||||
| Adagbabiri | 51 | 47 | 98 | 8(15.7) | 13(27.7) | 21(21.4) | 94 | 2(2.1)a | 0(0.0)b | 0(0.0) | 2(2.1)d |
| Tungbabiri | 40 | 49 | 89 | 2(5.0) | 3(6.1) | 5(5.6) | 60 | 0(0.0)a | 0(0.0)b | 0(0.0) | 1(1.7)d |
| Sagbama | 45 | 42 | 87 | 5(11.1) | 6(14.3) | 11(12.6) | 51 | 2(3.9)a | 1(1.9)b | 0(0.0) | 1(2.0)d |
| Total | 136 | 138 | 274 | 15(11.0) | 22(15.9) | 37(13.5) | 205 | 4(2.0) | 1(0.5) | 0(0.0) | 4(2.0)
|
Numbers with the same letter superscript on same row shows that there is no significant difference (p>0.05)
Table 2: Evaluation of microfilaria density based on age across the three communities
| Age group (years) | No of individual Examined (%) | Adagbabiri | Mean microfilarial density | Tungbabiri | Mean microfilarial density | Sagbama | Mean microfilarial density | Overall Infected (%) | P-Value |
| Infected (%) | MF/40µL | Infected (%) | MF/40µL | Infected (%) | MF/40µL | Infected (%) | |||
| 10-19 | 57(20.8) | 3(14.3) | 0.03 | 0(0) | – | 0(0) | – | 3(5.3) | 0.52 |
| 20-29 | 82(29.9) | 7(33.3) | 0.20 | 2(40.0) | 0.03 | 6(54.6) | 0.18 | 15(18.3) | |
| 30-39 | 64(23.4) | 3(14.3) | 0.03 | 2(40.0) | 0.03 | 4(36.4) | 0.03 | 9(14.1) | |
| 40-49 | 31(11.3) | 6(28.6) | 0.18 | 0(0) | – | 0(0) | – | 6(19.4) | |
| 50-59 | 21(7.7) | 0(0) | – | 1(10) | 0.05 | 1(9.1) | 0.03 | 2(9.5) | |
| 60-69 | 12(4.4) | 1(4.8) | 0.03 | 0(0) | – | 0(0) | – | 1(8.3) | |
| 70+ | 7(2.6) | 1(4.8) | 0.03 | 0(0) | – | 0(0) | – | 1(14.3) | |
| Total | 274(100) | 21(7.7) | 0.08 | 5(1.8) | 0 04 | 11(4.0) | 0.08 | 37(13.5) |
Table 3: Mean Microfilarial density across Sex and communities
| Male | Female | |||
| Communities | No infected | Mean microfilarial density | No infected | Mean microfilarial density |
| Adagbabiri | 8 | 0.23 | 13 | 0.35 |
| Tungbabiri | 2 | 0.03 | 3 | 0.10 |
| Sagbama | 5 | 0.03 | 6 | 0.18 |
| Mean Microfilarial Density | 15 | 0.10 | 22 | 0.20 |
Table 4. Respondents Knowledge on Causes and Mode of Transmission on L. filariasis
| Causes | Mode of Transmission | ||||||||
| Adagba. N= 94 | Tungba. N=60 | Sagba. N=51 | Total N= 205 | Adagba. N= 94 | Tungba. N=60 | Sagba. N=51 | Total N = 205 | ||
| Walking long distance | 35(37.2) | 11(18.3) | 6(11.8) | 47(67.3) | Sexual Intercourse | 24(25.5) | 15(25.0) | 5(9.8) | 44(60.3) |
| Sexual intercourse | 23(24.5) | 11(18.3) | 3(5.9) | 37(48.7) | Body Contact | 33(35.1) | 8(13.3) | 3(5.9) | 44(54.3) |
| Stepping on charm | 26(27.7) | 26(43.3) | 13(25.5) | 62(95.15) | Witchcraft | 24(25.5) | 27(45.0) | 15(29.4) | 66(99.9) |
| Contaminated food | 34(36.2) | 15(25.0) | 7(13.7) | 56(74.9) | Steppingon charm | 23(24.5) | 27(45.0) | 14(27.5) | 64(94.0) |
| Personal hygiene | 17(18.1) | 25(41.7) | 10(19.6) | 52(79.4) | Food poisoning | 22(23.4) | 21(35.0) | 10(19.6) | 53(78.0) |
| Mosquito bite | 3(3.2) | 6(10.0) | 7(13.7) | 16(26.9) | Inheritance | 11(11.7) | 20(33.3) | 12(23.5) | 43(68.5) |
| Mosquito Bite | 3(3.2) | 4(6.7) | 5(9.8) | 12(19.7) |
N.B: Adagba- Adagbabiri, Tungba- Tungbabiri, Sagba- Sagbama .
Table 5. Respondents Knowledge on Prevention and Perception on L. filariasis
| Prevention | Psychological Consequensis. | ||||||||
| Adagba N= 94 | Tungba. N=60 | Sagba. N=51 | Total N= 205 | Adagba. N= 94 | Tungba. N=60 | Sagba. N=51 | Total N = 205 | ||
| Avoid Sex. Intercourse | 23(24.5) | 11(18.3) | 3(5.9) | 37(48.7) | Personally Uncomfortable | 88(93.6) | 56(93.3) | 50(98.0) | 196(284.9) |
| Avoid body contact | 17(18.1) | 25(41.7) | 10(19.6) | 52(79.4) | Affect work and Income | 91(96.8) | 57(95.0) | 50(98.0) | 198(289.8) |
| Sacrifice to the gods | 26(27.7) | 26(43.3) | 13(25.5) | 62(95.1) | Affect Sexual Relationship | 92(97.9) | 55(91.7) | 47(92.2) | 194(281.8) |
| Avoid mosquito bite | 2(2.2) | 3(5.0) | 2(3.9) | 7(11.1) | Spouse Desertion | 84(89.4) | 52(86.7) | 45(88.2) | 181(264.3) |
| Food poisoning | 34(36.2) | 15(25.0) | 7(13.7) | 56(74.9) | |||||
| Avoid eating with infected | 35(37.2) | 11(18.3) | 5(11.8) | 46(66.3) |
N.B: Adagba- Adagbabiri, Tungba- Tungbabiri, Sagba- Sagbama
DISCUSSION
The cross-sectional study revealed a prevalence of 13.5% which is comparatively lower than that of Agi and Ebenezer (2009) who recorded 28.9% in Amassoma, Bayelsa State and 37.8% observed by Muawiyya et al., (2019) in Zafara State. This finding is similar to the observation of Ojurongbe et al., (2010) in Osun State who reported 15.45% and Cletus et al., (2012) in Cross River State who observed, 17.2% prevalence among Yakurr people. It is interesting to note that several factors are responsible for the various prevalence rates of lymphatic filariasis observed herein. This could be due to their occupational dispositions such as fishing, hunting and farming, poor housing, poor environmental conditions, unhygienic practices and destruction of mosquito’s habitats due to construction of building projects. The existence of LF in the study areas is probably related to the ecological nature of the area which favours the breeding of the arthropod vectors. Highest prevalence was observed in Adagbabiri followed by Sagbama and Tungbabiri. This trend of prevalence variation between communities were also reported by other works on human filariasis (Elkanah et al., 2017; Okon et al., 2010; Muawiyya et al., 2019; kelly-Hope et al., 2018; Oluwabiyi et al., 2017). However, high prevalence in Adagbabiri could be attributed to occupation, poor medical facilities and poor housing. In Adagbabiri, people live in mud/zinc houses, with no ceiling and net windows exposing them to bites of mosquitoes while lower prevalence in Sagbama and Tungbabiri were due to good housing in these communities, high socio-economic status, access to medical facilities and improved environmental conditions. Low clinical manifestation of L.F across the three communities observed: elephantiasis, hydrocele and crawling sensation were consistent with the study of Patricia et al., (2015) and Elkanah et al., (2017). Studies on LF had revealed that, clinical features of LF were slow to develop coupled with filarial density proportion in the infected persons (Elkanah et al., 2011). Sex-related prevalence of L.F infection was observed and no significant variation of prevalence among the sexes was reported. Females had more infections than males across the three communities, this observation agrees with Elkanah et al., (2017). This is related to exposure of the females to disease vectors while fishing and selling alcohol in the night, their behavioral pattern predisposes them easily to insect bite. However, this contradicts the report of Agi and Ebenezer (2009), Brant and Kelly-Hope (2018) and Muawiyya et al., (2019); who recorded high prevalence in male. High infection rates were observed in 20-49years across the three communities and these groups are known to be the most productive age between the phases of life (Cletus et al., 2012). This prevalence was similar to the observations of Agi and Ebenezer (2009), Ekanem et al (2011), this could be attributed to occupational and immunity to the infection developed over time. However, this is in contracts to Mu’awiyya et al., (2019), who reported a higher prevalence among 51-60yrs age group. Filarial density estimation is very important for intervention/control programs. The mean micro filarial density recorded in this study was low among age groups and sex across the three communities. Most participants across the three communities believed that stepping on charm, sexual intercourse, witchcraft and food poison etc was the cause of LF, only few of the subjects acknowledged that mosquitoes’ bites were the cause of LF. However, very high perceptions on socioeconomic and psychological consequences were observed across the communities. Almost all the participants believed that LF can cause personal discomfort in public, affects work and income, affects sexual relation and spouse desertion. Similar results were obtained among the residents of Port Harcourt metropolis in a survey done by Nzeako, et al., (2016). Finally, Ignorance and sensitization of LF are poor among the residents of Sagbama, Tungbabiri and Ebedebiri in Bayelsa State.
REFERENCE
- Anosike JC, Nwoke BE, Ajayi EG, Onwuliri CO, Okoro OU, Oku EE, Asor JE, Amajuoyi OU, Ikpeama CA, Ogbusu FI, Meribe CO. (2005). Lymphatic filariasis among the Ezza people of Ebonyi State, Eastern Nigeria. Ann Agric Environ Med. 2005;12(2):181-6. PMID: 16457471.
- Agi, P. I. and Ebenezer, A. (2009). Observations on filarial infection in Amassoma community in the Niger Delta, Nigeria. Journal of Applied Sciences and Environmental Management, 13(1): 15-19.
- Brant, A.T. and Kelly-Hope, A.C. (2018). Integrated risk Mapping and land scape characterization of lymphatic filariasis and loiasis in South west Nigeria, Parasite Epidemiology and Control. 3(1): 21-35.
- Brant, A.T, Okorie, P.N., Ogunmola, O., Ojeyode, B.N., Davies, E., Saka, S., Stanton, C.M., Molyneux, D.H., Stothand, R.J. and Kelly-Hope, A.C. (2018). Integrated risk mapping and landscape characterization of lymphatic filariasis and loiasis in south west Nigeria. Parasitology epidemiology and control, 3:21-35
- Chessbrough, M. (2006). District Laboratory Practice in Tropical Countries, Volume (2) Cambridge, England: Cambridge University Press. 313-319
- Cleide, M.R.A., Vania, M.S., Maria, A.V., Leda, N.R.& Hilary, H. (1999). Blood meal microfilaria density and the uptake and Establishment of Wucheria bancrofti infection in Culex quniquefasciatus and Aedes aegypt. SciELO. 91(5):591-596.
- Cletus, I.1, Okpoki, E.O., Kenneth, N.O., Joseph, E.A. and Susan E.E. (2012). Lymphatic filariasis among the Yakurr people of Cross River State, Nigeria. Parasite and vectors. 5(1):203.
- Eigege, A., Evans, D. S., Noland, G. S., Davies, E., Umaru, J., Adelamo, S. E. and Griswold, E. P. (2017). Criteria to stop mass drug administration for lymphatic filariasis have been achieved throughout plateau and Nasarawa States, Nigeria. The American journal of tropical medicine and hygiene, 97 (3): 677-680.
- Elkanah, O. S., Elkanah, D. S., Wahedi, J. A., Samaila S. L.& Anyanwu, G. I. (2017). Lymphatic Filariasis in Muri Emirate: Clinical and Parasitological Studies in Jalingo L. G. A, Taraba state, Nigeria. Asian Journal of medicine and Health.6 (1): 1-7.
- Ekanem, I.A., Alaribe, A. A.A.& Ekanem, A.P. (2011). Prevalence of Bancroftian filariasis among EdimOtop Sub-Urban dwellers in Calaber Municipality of Cross River state Nigeria. Journal of applied Pharmaceutical Science. 01(09): 63-67.
- Gordon, R. M.,and Lavoipierre, M. M. J., Lavoipierre, (1962). Entomology for Students of Medicine, By R.M. Gordon and M.M.J. Lavoipierre. Illustrated by Margaret A. Johnson.
- Kelly-Hope, L. A., Hemingway, J., Taylor, M. J. & Molyneux, D. H. (2018). Increasing evidence of low lymphatic filariasis prevalence in high-risk Loa loa areas in Central and West Africa: a literature review. Parasites & vectors. 11(1): 349.
- Kelly-Hope, L.A., Thomos, B.C., Molyneux D.H. (2011) Lymphatic filariasis in Democratic Republic of Congo; Micro Stratification overlap mapping (MOM) as a prerequisite for control and surveillance. Parasites and vectors 4:178.
- Mu’awiyya, U. L., Tukur, A., Aminu, Y. B.& Muhtari J. L. (2019). Sero-Prevalence of lymphatic Filariasis in six Communities of Talata mafara Local Government Area, Zamfara State, Nigeria. Research Journal of Parasitology 14(1):1-6.
- Nwoke, B.E.B., Nwoke, E.A., Ukaga, C.N. & Nwachukwu, M.I. (2010). Epidemiological charateristics of Bancroftian filariasis and the Nigerian environment. Journal of public Health and Epidemiology. 2(6):113-117.
- Nzeako, S.O., Okunnug, O.H., Nduka, F.O. and Ezenwaka, C.O. (2016). Lymphatic Filariasis and Malaria Awareness amongst Residents of Port Harcourt Metropolis. International Journal of Applied Science. 3:6.
- Okon, O. E., Iboh, C.I. & Opara, K. N. (2010). Bancroftian filariasis among the Mbembe people of Cross River State, Nigeria.” Journal of vector borne diseases, 47(2): 91.
- Oluwabiyi, B., Oyeyemi, O.T., Olurunlana, A., Omiyemiye, A, and Koleosho, A. (2017) Lymphatic Filariasis in Southwestern Nigerian Rural Communities: A Cross Sectional Survey of the knowledge, Awareness and Predisposing factors. Annals of Global Health. 82 (5): 806-812.
- Omudu, E.A. and Ochoga J.O. (2011). Clinical Epidemiology of lymphatic filariasis and community practices and perceptions amongst the Ado people of Benue State, Nigeria. Afr. J. Infection. 5 (2): 47-52.
- Ojurongbe, O., Akinbo, J.A., Ogiogwa, I.J. & Bolaji. O. A. (2010). Lymphatic Filariasis in a rural community in Nigeria: challenge ahead. Afri J med med sci. 179-183
- Udoidung NI, Braide IE, Opara KN, Atting IA, Adie H. Current status of Bancroftian filariasis in rural communities of the Lower Cross River Basin, Nigeria. Parasitological and Clinical aspects. (2008). J Public Health; 16:383–388. doi: 10.1007/s10389-008-0189-6. [CrossRef] [Google Scholar]
- Udonsi J. Filariasis in the Igwun River Basin, Nigeria: an epidemiological and clinical study with a note on the vectors. Ann Trop Med Parasitol. 1988;82(1):75–82. [PubMed] [Google Scholar
- WHO, (2010). Global programmes to eliminate Lymphatic filariasis: progress report 2000-2009 and strategic plan 2010-2020. World health organization.
- WHO, (2013). Morbidity management and Disability prevention in Lymphatic Filariasis; an aide-memorre for national program managers
- World Health Organization. Global programme to eliminate lymphatic filariasis: progress report, 2015. Weekly Epidemiological Record. 2016; 91(39):441–60. [PubMed] [Google Scholar]