
Evaluation of Non-Adrenergic – Non-Cholinergic Mediators in Response to Thermal Balance in Lifestyle Clients at Risk of Heat Illness.
- Emmanuel Kairania
- 9-55
- Mar 25, 2025
- Health
Evaluation of Non-Adrenergic – Non-Cholinergic Mediators in Response to Thermal Balance in Lifestyle Clients at Risk of Heat Illness.
Emmanuel Kairania
Busitema University, Faculty of Health Sciences
DOI: https://doi.org/10.51584/IJRIAS.2025.10030002
Received: 12 February 2025; Accepted: 18 February 2025; Published: 25 March 2025
ABSTRACT
The study examined how non-adrenergic-non- cholinergic (NANC) mediators affect the body’s temperature balance and heart rate responses in people prone to heat-related illnesses because of their lifestyle. The study aimed to investigate the influence of prostaglandins and histamines on core body temperature, skin temperature, sweat rate, heart rate, and blood pressure dynamics during exercise and heat stress, providing insights into the physiological mechanisms underlying heat regulation in at-risk populations.
The research methodology involved systematically examining core body temperature, skin temperature, sweat rate, heart rate, and blood pressure changes during control, as well as prostaglandin and histamine blockade in lifestyle clients deemed vulnerable to heat illness. These disruptions in non-adrenergic and non-cholinergic pathways led to changes in cardiovascular responses. This could affect thermal balance and make people more likely to have heat-related problems.
Changes in NANC mediators led to changes in core body temperature, skin temperature, sweat rate, heart rate, and blood pressure. This shows the relationship between these mediators and how the heart and lungs react to heat stress. The observed trends provide valuable implications for managing thermal balance and preventing heat-related issues in at-risk lifestyle clients.
Finally, looking at the role of NANC mediators in controlling temperature gives us a better idea of how the body reacts to heat in people who are more likely to get sick. We propose personalized interventions that focus on hydration and cooling strategies, and further research into other pathways that influence thermal balance and cardiovascular responses in high-risk individuals.
By integrating these findings into clinical practice, healthcare providers can enhance preventive measures and interventions for lifestyle clients at risk of heat illness, contributing to improved outcomes and well-being in heat-exposed environments. This study offers valuable insights into the interplay between NANC mediators and thermal balance, advancing our understanding of heat-related physiology and promoting optimal health in at-risk populations.
Keywords: NANC, lifestyle clients, skin temperature, cardiovascular response.
INTRODUCTION
When humans need to lose more heat to keep their body temperature stable, their skin blood flow goes up through cutaneous vasodilation and sweating. This is made easier by lower vascular resistance in the skin, an integral part of thermoregulation (Charkoudian, 2016; Lenasi & Šijanec, 2023; Nazari et al., 2020). When you work out or are in a warm place, your body’s thermoregulatory responses prioritise getting rid of heat. This causes more blood to flow through your skin through convective heat transfer and evaporative heat loss (Charkoudian, 2016; Lenasi & Šijanec, 202). Skin blood flow adjustments are crucial for maintaining thermal homeostasis. Vasodilation of the skin’s vessels helps move heat from the core to the skin’s edges, and sweating increases evaporative heat loss, both of which help keep the body’s core temperature in a narrow optimal range (Charkoudian, 2016; Nazari et al., 2020).
Thermal balance, critical for normal physiological function, entails maintaining core temperature despite external temperature changes caused by sweating, vasodilation, and vasoconstriction. Traditionally, thermoregulation emphasises adrenergic and cholinergic pathways (2022 Conference Poster Collection: Thermoregulation,” 2022). However, recent research highlights the significant involvement of non-adrenergic and non-cholinergic pathways in thermal balance (Lenasi & Šijanec, 2023). During physical exercise, the body’s response to heat stress involves adjustments in cutaneous vascular conductance, skin blood flow, and sweating rate to achieve thermal homeostasis (Lenasi & Šijanec, 2023). Due to high temperatures, central and peripheral thermoreceptors set off reflex neural pathways for heat loss, such as vasodilation and sweating of the skin (Charkoudian, 2016). Understanding these many systems is critical for comprehending the intricate processes that regulate thermal homeostasis in the human body.
I Bon (2023) says that NANC mediators like nitric oxide, vasoactive intestinal peptide, and substance P change how the body works without the help of adrenergic or cholinergic systems. These mediators control blood vessel tone and sweating responses, critical for thermal balance (Yahiro et al., 2023). Understanding the unique contributions of NANC mediators to thermoregulation is critical for people susceptible to heart disease, such as athletes, outdoor labourers, and those living in hot areas (Yahiro et al., 2023). According to Yahiro et al. (2023), dehydration and long-term exposure to heat may make heat-related disorders more common. This shows the need to study NANC mediators in thermal balance to create personalized therapies for prevention and treatment. We can evaluate NANC mediators by measuring blood or sweat sample levels, examining their effect on blood vessel dilation and sweating response, and comparing these findings to thermal balance markers like core body temperature (Osei et al., 2022).
Understanding the role of non-adrenergic and non-cholinergic (NANC) mediators in maintaining thermal homeostasis is critical for people at risk of heart disease (Mündel, 2023). Environmental heat stress provides severe health hazards, with heatstroke being a significant cause of morbidity and mortality (Mündel, 2023). The human heat stress response (HSR) is critical in defending against heat-induced damage, yet its inability to prevent heatstroke demonstrates the intricacy of thermoregulation processes (Mündel, 2023). Insects have sophisticated thermoregulatory strategies to adapt to changing ambient temperatures, underscoring the necessity of understanding these mechanisms in climate change and pathogen development (Lahondère, 2023). By investigating the roles of NANC mediators, researchers can improve heart disease prevention and management measures, perhaps leading to better results for people who face thermal problems.
MATERIALS AND METHODS
Equipment and Drugs
The Wash and Wills Hotel gym and physiology laboratory at Busitema University used an exercise bike of high medical quality and standard. We obtained ibuprofen and cetirizine (internal standard) from the Regional Referral Hospital pharmacy.
Subjects and Intervention
In treatment groups, we randomly assigned subjects to oral ibuprofen or cetirizine per evaluation day, starting when they reported heat exposure and exercise.
This would continue for a week in both groups (Du & Zhou, 2016; Matterne et al., 2019; Zhou et al., 2022).
We determined the possibility of effectiveness and heat illness using the binomial distribution and compared changes in p-value using the paired t-test (Douglas, 2022; Satoh et al., 2021; Wooditch et al., 2021).
This study enrolled twenty-four healthy volunteers. After carefully evaluating their health status, the pharmacist prescribed ibuprofen (two 200 mg tablets taken three times a day before the experiment) and cetirizine (10 mg once a day daily) to each of the three groups.
We recorded the mean values for test parameters at the beginning and during heat exposure and exercise. We determined the heart rate, blood pressure, core body temperature, skin temperature, and sweat rate daily before and during heat exposure and exercise. However, we also recorded any possible change in the health status as a matter of importance. We assessed changes in physiological parameters for case studies in the groups.
Table 1: Enrollment and grouping of participants.
| Control group | Treatment groups | ||
| Prostaglandins blockade | Histamines blockade | Either prostaglandin blockade or histamine blockade | |
| (Ibuprofen) | (Cetirizine) | (Ibuprofen or Cetirizine) | |
| n=6 | n=6 | n=6 | n=6 |
| Total, N=24 | |||
This study enrolled 24 healthy male and female adult volunteers at Busitema University, the Faculty of Health Sciences Physiology Laboratory, and the Wash and Wills Hotel Health Club in Mbale. The age range of the subjects was 18–40 years, with a weight range of 53–101 kg and a height range of 164–187 cm. The investigators instructed the subjects to refrain from using any medication for at least 2 weeks prior to and during the study period. The investigators informed all eligible subjects about the purpose and potential risks of this study and requested that they confirm their informed consent in writing prior to their participation. The investigators informed the subjects that they could withdraw from the study at any time (Agaba et al., 2020; Andrade et al., 2018; Cook, 2022; Puiguriguer-Ferrando & Caballero-Bermejo, 2023; Sidana et al., 2019).
Clinical protocol
We conducted the study using an open-label, randomized, nonreplicated, single-period design with a seven-day treatment period. Study Before the study started, the Institutional Review Board of the Selinus University of Science and Literature Research Ethics Committee approved the study protocol and informed consent form. We conducted the study using Good Clinical Practice guidelines and the Revised Declaration of Helsinki. The study began with a screening that included a physical examination, a medical history, laboratory safety tests, an electrocardiogram, and vital signs. The investigators also assessed safety parameters during treatment days and follow-up. All subjects had to meet carefully selected exclusion and inclusion criteria determined by the investigators, accounting for their current medical status and life expectancy. The case report forms documented any changes in the concomitant disorder and medication, for disorders not included in the exclusion criteria. The Mbale Regional Referral Hospital performed all clinical laboratory tests (Cox et al., 2022; Golubovskaya et al., 2023; Ngaage et al., 2023; Pastena et al., 2023; Sun et al., 2023).
Study subjects
Subjects arrived at the hospital two hours prior to the start of study. We used a computer-generated table to select and randomly assign the volunteers to the study groups. The investigators supervised the subjects as they administered a single oral dose of one of the drugs (test) at 9 a.m. in each period, following a 12-hour overnight fast. Each group received an equal number of subjects. We prohibited alcohol consumption 24 hours before each study period and until we measured the last parameter in each period, we measured the parameter. Volunteers were ambulatory during the study, but were prohibited from strenuous activity and were under direct medical supervision at the study site (Atkinson et al., 2023; Gerth et al., 2023; Oxley et al., 2022; Pereira et al., 2022).
Administering drugs and measuring various parameters
All experiments followed the same basic double-masked design: baseline heart rate, blood pressure, body temperature, and sweat rate recording, followed by heat and exercise challenge recordings 5, 10, and 15 minutes later. For each experiment, subjects received all treatments randomly, with only one treatment allowed daily. We administered oral histamine antagonists, cetirizine and prostaglandin antagonists, ibuprofen, and drinking water 2 hours before the heat and exercise challenge. Cetirizine and ibuprofen doses and time courses were based on previously published reports (McNeil et al., 1981; Dubuske, 1995).
We administered the drugs orally with 240 mL of water. The investigator supervised the administration of the study medication to ensure its swallowing and conducted a mouth check to verify the volunteers’ compliance. The study design concluded with further monitoring and a seven-day washout period for the subjects after seven days of the study (Gerth et al., 2023; Xiang et al., 2023).
Body temperature monitoring
Using a patient’s body temperature to screen for infectious diseases, making diagnoses, track treatment, and making management decisions is routine practice.
People commonly use axillary digital thermometers (ADTs) and non-contact (infrared) forehead thermometers (NCIFTs) (Bright et al., 2023; Lin et al., 2023).
We recorded and quantified the body temperature at both the skin and core levels.
These participants were chosen at random. An axillary thermometer (Medisafe digital thermometer, Model: PT-01A; range is 32oC–42oC, +0.2oC) and a noncontact infrared forehead thermometer (Model: FI01; Range is 32oC–42oC, +0.2oC) were used to monitor body temperature. We simultaneously compared the readings from the digital thermometer with a probe in the axilla and the infrared frontal thermometer (Chen et al., 2022).
All study participants had their body temperatures taken simultaneously at the axillary and mid-forehead sites by qualified nurses who had completed a particular one-hour training program to guarantee measurement accuracy by manufacturer guidelines.
In addition to being told it was complete, the study’s participation was voluntary and anonymous, and, subjects were also informed about its aim. In all groups, not a single individual declined to participate. It took about two minutes to complete the measurement process. The triage nurse concurrently recorded vital signs and took the body temperature (BT) using two separate devices. Prior to viewing the BT value on the display for ADT measurements, the nurse positioned the device under the armpit and waited for the beep. Before taking the patient’s forehead temperature, the nurse waited for two beeps, or if the BT was more excellent and more significant than 37.5°C, a long beep followed by three short beeps. Before taking the temperature readings, nurses waited for the acoustic alarm to ring, and they calibrated all equipment prior to use (Lin et al., 2023; Patel et al., 2023).
Monitor your heart rate and blood pressure.
There is less “white-coat effect” when using an automated blood pressure recorder than when using a mercury sphygmomanometer. These devices provide stable, reproducible, cost-effective, and prognostic data for cardiovascular (CV) risk. They are simple to incorporate into daily routines, accurately assess hypertensive therapy responses, and enable remote consultations (Muniyandi et al., 2022; Stopa et al., 2022).
The study used an arm type, an oscilloscope test method, and a Smart Angel automatic blood pressure monitor to record blood pressure and heart rate.
These automatic blood pressure monitors measures blood pressure: 0-280 mmHg (0.37.3 kPa), heart rate: 40 to 199 beats/min, with accuracy of pressure: ±3 mmHg (0.4 kPa), pulse rate: within ±5% of reading, and diagnostic flags on a digital panel. Users could record readings and keep track of them in an electronic personal health record. Proper cuff size, tight wrapping, patient restraint, and consistent heart level achieved accuracy. Users were aware of potential instrument malfunctions and repeated readings if necessary (Niu et al., 2022).
During the trial, all participants permitted the automated arm blood pressure monitor to take their blood pressure. The researchers calibrated the monitoring gadget. The investigators allowed five minutes between each measurement, all taken from the left arm. We used the instruction manual and identical monitors. We strictly followed the manufacturer’s guidelines for each monitor, including those regarding patient preparation. During testing, investigators were unaware of other investigators’ readings (Araujo-Moura et al., 2022; Muniyandi et al., 2022).
Sweat rate estimation
Baker (2016) used the whole-body washdown technique to measure sweat rate by analyzing body weight before and after exercise and heat stress, accounting for fluid intake and urine output.
Before exercise and heat stress, subjects voided their bladders and then had body mass measured on a digital scale. We weighed the subjects with minimal clothing (e.g., compression shorts for males, shorts and sports-bras for females) to avoid the confounding effect of sweat trapped in clothing or uniforms. We determined the fluid intake during exercise by weighing the drinking bottles before and after consumption. The investigators made water available in bottles labelled explicitly for each subject throughout the exercise and heat stress. The investigators instructed the subjects to refrain from spitting, spilling, or pouring fluid from the labelled bottles used for testing. We gave them an additional water bottle, marked for this purpose, if they wanted to pour water over themselves. We determined their food intake during exercise by weighing the product in its wrapper before and after consumption. During exercise and heat stress, the investigators provided them with a pre-weighed container and instructed them to collect all urine for subsequent weighing. The investigators instructed the subjects to inform them if they needed a bowel movement during the test, so they could measure their body mass before and after going to the bathroom, thereby determining stool mass loss. After completing the exercise and heat stress sessions, the subjects had to towel-dry themselves and then measure their body mass on the same scale while wearing the same clothes as the pre-exercise and heat stress body mass assessments. Study investigators and training staff carefully observed the subjects during exercise and heat stress to record any protocol deviations (Baker, 2016; Dautta et al., 2023).
We estimated the total whole-body sweat loss and the whole-body sweating rate using the following equations:
Equation 1: WBSL (L) = [Body MassPRE-EX – (Body MassPOST-EX – Fluid IntakeEX + Urine OutputEX)]
Equation 2: WBSR (L/h) = WBSL/EExercise Duration
The acronym EX stands for exercise, PRE-EX for pre-exercise, POST-EX for post-exercise, WBSL for whole-body sweat loss, and WBSR for whole-body sweating rate (Baker, 2016).
The Skin Blood Flow (SkBF)
Four component factors, AVD, CVCM, CVCL, and CVCE, determine the perfusion rate at a reference state. These factors are defined based on experimental data, highlighting the impact of temperature, skin temperature, and exercise intensity on cutaneous vasoconstriction (Wissler, 2008).
Model, the model defines the rate of cutaneous blood flow (q s)
as q s = q s, r AVD × CVCM × CVCL × CVCE.
The four components combine multiplicatively rather than additively, and it offers a logical explanation for the non-thermal effect of exercise on active cutaneous vasodilation.
The coefficient q s,r represents the perfusion rate in a reference state. The four component factors are defined as follows: They say that AVD is active vasodilation that is influenced by central temperature (T c), mean skin temperature (T s), and the amount of exercise (VO2); CVCM is cutaneous vasoconstriction that is influenced by T s; CVCL is cutaneous vasoconstriction that is influenced by local skin temperature (T s); and CVCE is the relationship between exercise and cutaneous vasoconstriction and mean arterial pressure (Wang et al., 2022; Webb et al., 2015; Wissler, 2008).
Study population
During the study period, both men and women attended health club clinics.
This indicates that the study population consisted of individuals who regularly visits and regular visits to health club clinics.
Inclusion and Exclusion Criteria
Inclusion criteria
Young adult men and women between 18 and 40 make up this demographic.
Willing to participate
The individual has no history of cardiovascular risk.
Exclusion criteria
I am unwilling to participate in the study.
The age range is below 18 years and above 40 years.
Has a history of cardiovascular risk
Sample size determination
The study’s sample size estimate was based on the idea that 40% of the people who took part would positively respond to NANC mediators in thermoregulation and 10% would have a delay with ibuprofen and histamine blockade compared to control cycles.
A one-sample test of proportions revealed the need for 11 subjects to reach a power of 80% at a two-sided alpha level of 0.05.
We calculated the sample size using Kish’s formula, which considers the desired power, alpha level, and the estimated proportion of subjects experiencing a positive increase in skin blood flow.
The formula used for sample size determination is N = (Z^2 (p(1-p)))/ε^2, where N is the required sample size, Z is the Z-score corresponding to the desired power and alpha level, p is the estimated proportion, and ε is the desired margin of error.
Sampling technique
The study employed consecutive sampling, enrolling each man and woman who met the inclusion criteria.
Data collection methods
We collected the data for the study using a pretested, structured questionnaire during an exit interview with clients using sauna, steam bath, and gym services.
We asked participants to sign written informed consent after explaining the study and answering their questions.
We designed the questionnaire to gather information on socio-demographic characteristics, health history, utilization of modern health lifestyle methods, and factors affecting these methods.
We prepared the questionnaire in English and translated it into the local language during data collection for participants who do not understand English well.
Data representation and interpretation
Tables, line graphs, bar charts, scatter plots, correlation plots, and heat maps all represent categorical variables.
We computed hypothesis tests using ANOVA, independent t-tests, correlation, multivariate analysis, and time series analysis to test the effectiveness of non-adrenergic and non-cholinergic mediators in response to thermal balance in lifestyle clients at risk of heat illness.
We used the binomial distribution to determine the probability of reduced skin blood flow for ibuprofen and cetirizine compared to control.
Statistical data analysis
We recorded all measurements in Microsoft Excel® worksheets (Microsoft Office 2010; Microsoft, Redmond, Washington, USA), and used measures of central tendency, dispersion, and frequencies to analyze differences between the control and test groups. We correlated differences in average core body temperature, skin temperature, sweat rate, heart rate, and blood pressure using the Pearson coefficient, and compared mediators’ response P-values between ibuprofen, cetirizine, and control experiments using ANOVA and a paired t-test. The point of statistical significance was a p-value of <0.05.
Quality control
The questionnaire for data collection was pre-tested to ensure clarity and gather the necessary information for the study. We revisited and modified any ambiguous questions during pre-testing as needed. This process of pre-testing and modification helped to improve the quality and effectiveness of the questionnaire. By addressing any issues identified during pre-testing, the researchers ensured that the questions were clear and allowed for the gathering of accurate and relevant information. This quality control measure helped to enhance the reliability and validity of the data collected through the questionnaire.
Ethical considerations
The Selinus University of Science and Literature research ethics committee provided ethical approval, demonstrating the researchers’ dedication to conducting the study ethically.
Written and verbal consent was obtained from the respondents before their participation in the study, ensuring that they were fully informed about the study’s purpose, procedures, and potential risks or benefits.
Seeking ethical approval and obtaining informed consent were important ethical considerations in research, as they protected the rights and well-being of the participants and ensured that the study adhered to ethical guidelines and principles.
These measures demonstrated the researchers’ commitment to conducting the study in an ethical manner and respecting the autonomy and privacy of the participants.
By obtaining ethical approval and informed consent, the researcher upheld the principles of beneficence, respect for autonomy, and justice in the study.
RESULTS
Tabular presentation of physiological measurements
We used tabular representation to summarize and compare measurements of core body temperature, skin temperature, sweat rate, heart rate, blood pressure, and mediators’ responses at various time points or conditions.
Table 2: Summary of Physiological Measurements for the Control Group at Different Time Points for the Exercise Protocol Participant Time Point Core Body Temperature (°C) Skin Temperature (°C) Sweat Rate (ml/min) Heart Rate (bpm) Blood Pressure (mmHg).
| Participant | Time Point | Core Body Temperature (°C) | Skin Temperature (°C) | Sweat Rate (ml/min) | Heart Rate (bpm) | Blood Pressure (mmHg) |
| 1 | Pre-exercise | 37.2 | 33.1 | 10 | 80 | 120/80 |
| During Exercise | 37.5 | 34.0 | 25 | 120 | 140/90 | |
| Post-exercise | 36.8 | 33.2 | 15 | 100 | 130/85 | |
| 2 | Pre-exercise | 36.6 | 33.5 | 8 | 75 | 118/78 |
| During Exercise | 37.2 | 33.8 | 20 | 110 | 135/88 | |
| Post-exercise | 37.5 | 33.7 | 12 | 85 | 125/82 | |
| 3 | Pre-exercise | 36.3 | 33.2 | 11 | 65 | 131/87 |
| During Exercise | 36.5 | 33.7 | 16 | 70 | 120/75 | |
| Post-exercise | 36.1 | 33.5 | 13 | 83 | 123/81 | |
| 4 | Pre-exercise | 36.2 | 33.4 | 9 | 140 | 136/86 |
| During Exercise | 36.3 | 33.8 | 15 | 106 | 136/69 | |
| Post-exercise | 36.7 | 33.7 | 12 | 98 | 132/66 | |
| 5 | Pre-exercise | 36.9 | 33.1 | 7 | 109 | 148/72 |
| During Exercise | 36.4 | 33.9 | 18 | 124 | 148/62 | |
| Post-exercise | 36.6 | 33.1 | 14 | 112 | 141/64 | |
| 6 | Pre-exercise | 36.4 | 33.3 | 11 | 75 | 170/116 |
| During Exercise | 36.9 | 33.8 | 23 | 71 | 146/86 | |
| Post-exercise | 36.3 | 33.9 | 16 | 74 | 135/72 |
Note: There was an increase in core body temperature, skin temperature, sweat rate, heart rate, and blood pressure with variations in participants 3,4,5, and 6.
Table 3: Summary of Physiological Measurements for Histamine Blockade at Different Time Points for the Exercise Protocol Participant Time Point Core Body Temperature (°C) Skin Temperature (°C) Sweat Rate (ml/min) Heart Rate (bpm) Blood Pressure (mmHg).
| Participant | Time Point | Core Body Temperature (°C) | Skin Temperature (°C) | Sweat Rate (ml/min) | Heart Rate (bpm) | Blood Pressure (mmHg) |
| 1 | Pre-exercise | 36.1 | 34.0 | 6 | 99 | 122/80 |
| During Exercise | 36.5 | 35.4 | 24 | 146 | 131/76 | |
| Post-exercise | 36.0 | 33.4 | 14 | 153 | 142/76 | |
| 2 | Pre-exercise | 35.9 | 33.8 | 7 | 81 | 108/73 |
| During Exercise | 36.4 | 34.9 | 19 | 98 | 125/65 | |
| Post-exercise | 36.1 | 32.5 | 11 | 101 | 115/61 | |
| 3 | Pre-exercise | 36.8 | 33.7 | 10 | 105 | 126/81 |
| During Exercise | 36.2 | 35.5 | 15 | 141 | 144/83 | |
| Post-exercise | 36.1 | 34.0 | 12 | 138 | 135/91 | |
| 4 | Pre-exercise | 36.4 | 33.9 | 8 | 73 | 137/90 |
| During Exercise | 36.5 | 35.4 | 14 | 151 | 160/84 | |
| Post-exercise | 36.4 | 33.8 | 11 | 155 | 149/81 | |
| 5 | Pre-exercise | 36.8 | 34.7 | 6 | 72 | 107/80 |
| During Exercise | 36.2 | 35.2 | 17 | 115 | 145/92 | |
| Post-exercise | 36.3 | 33.7 | 13 | 126 | 156/82 | |
| 6 | Pre-exercise | 36.5 | 33.9 | 10 | 79 | 118/80 |
| During Exercise | 36.2 | 35.1 | 22 | 118 | 142/91 | |
| Post-exercise | 36.0 | 33.5 | 15 | 133 | 160/86 |
Note: There was an increase in core body temperature, skin temperature, sweat rate, heart rate, and blood pressure with variations in participants 3, and 6.
Table 4: Summary of Physiological Measurements for Prostaglandin Blockade at Different Time Points for Exercise Protocol Participant Time Point Core Body Temperature (°C) Skin Temperature (°C) Sweat Rate (ml/min) Heart Rate (bpm) Blood Pressure (mmHg).
| Participant | Time Point | Core Body Temperature (°C) | Skin Temperature (°C) | Sweat Rate (ml/min) | Heart Rate (bpm) | Blood Pressure (mmHg) |
| 1 | Pre-exercise | 36.7 | 33.6 | 7 | 63 | 105/64 |
| During Exercise | 36.9 | 35.4 | 22 | 110 | 150/90 | |
| Post-exercise | 36.8 | 34.2 | 12 | 124 | 138/80 | |
| 2 | Pre-exercise | 36.0 | 33.9 | 5 | 70 | 110/76 |
| During Exercise | 36.1 | 35.6 | 17 | 119 | 116/80 | |
| Post-exercise | 36.5 | 34.9 | 9 | 114 | 105/73 | |
| 3 | Pre-exercise | 36.2 | 33.6 | 8 | 71 | 115/75 |
| During Exercise | 36.5 | 36.0 | 16 | 122 | 149/82 | |
| Post-exercise | 36.3 | 35.7 | 10 | 125 | 143/80 | |
| 4 | Pre-exercise | 36.2 | 33.5 | 6 | 85 | 113/67 |
| During Exercise | 36.5 | 35.0 | 12 | 93 | 114/69 | |
| Post-exercise | 36.7 | 34.1 | 9 | 97 | 117/70 | |
| 5 | Pre-exercise | 36.6 | 33.5 | 4 | 83 | 127/77 |
| During Exercise | 36.2 | 34.7 | 15 | 133 | 156/74 | |
| Post-exercise | 36.3 | 33.7 | 11 | 133 | 150/84 | |
| 6 | Pre-exercise | 36.6 | 33.5 | 7 | 67 | 105/64 |
| During Exercise | 36.9 | 35.4 | 20 | 102 | 116/82 | |
| Post-exercise | 36.2 | 33.6 | 13 | 105 | 119/67 |
Note: There was an increase in core body temperature, skin temperature, sweat rate, heart rate, and blood pressure with variations in participants 2, and 5.
Table 5: Summary of Physiological Measurements for Control at Different Time Points for Sauna Protocol Participant Time Point Core Body Temperature (°C) Skin Temperature (°C) Sweat Rate (ml/min) Heart Rate (bpm) Blood Pressure (mmHg).
| Participant | Time Point | Core Body Temperature (°C) | Skin Temperature (°C) | Sweat Rate (ml/min) | Heart Rate (bpm) | Blood Pressure (mmHg) |
| 1 | Pre-sauna | 36.6 | 35.5 | 16 | 89 | 109/62 |
| During sauna | 37.7 | 36.4 | 24 | 79 | 115/69 | |
| Post-sauna | 37.4 | 35.8 | 20 | 74 | 111/65 | |
| 2 | Pre-sauna | 36.6 | 35.5 | 13 | 64 | 104/63 |
| During sauna | 37.3 | 36.0 | 23 | 83 | 113/63 | |
| Post-sauna | 37.4 | 35.7 | 21 | 100 | 114/83 | |
| 3 | Pre-sauna | 36.5 | 35.3 | 17 | 65 | 122/72 |
| During sauna | 36.4 | 35.1 | 22 | 89 | 122/76 | |
| Post-sauna | 36.9 | 35.2 | 18 | 83 | 121/75 | |
| 4 | Pre-sauna | 36.5 | 35.4 | 20 | 76 | 115/69 |
| During sauna | 37.4 | 36.1 | 24 | 89 | 119/71 | |
| Post-sauna | 37.5 | 35.9 | 19 | 83 | 130/81 | |
| 5 | Pre-sauna | 36.5 | 35.4 | 23 | 83 | 154/90 |
| During sauna | 37.6 | 36.2 | 27 | 92 | 131/86 | |
| Post-sauna | 37.5 | 36.2 | 21 | 86 | 130/66 | |
| 6 | Pre-sauna | 36.7 | 35.6 | 15 | 76 | 112/72 |
| During sauna | 37.4 | 36.1 | 20 | 88 | 128/82 | |
| Post-sauna | 36.5 | 35.7 | 18 | 84 | 121/75 |
Note: There was an increase in core body temperature, skin temperature, sweat rate, heart rate, and blood pressure with variations in participants 1,2,3, and 5.
Table 6: Summary of Physiological Measurements for Histamine Blockade at Different Time Points for Sauna Protocol Participant Time Point Core Body Temperature (°C) Skin Temperature (°C) Sweat Rate (ml/min) Heart Rate (bpm) Blood Pressure (mmHg).
| Participant | Time Point | Core Body Temperature (°C) | Skin Temperature (°C) | Sweat Rate (ml/min) | Heart Rate (bpm) | Blood Pressure (mmHg) |
| 1 | Pre-sauna | 36.7 | 35.6 | 14 | 106 | 120/75 |
| During sauna | 37.5 | 36.2 | 22 | 105 | 119/75 | |
| Post-sauna | 37.3 | 35.7 | 18 | 107 | 118/76 | |
| 2 | Pre-sauna | 36.5 | 35.4 | 11 | 125 | 129/82 |
| During sauna | 36.7 | 35.4 | 21 | 107 | 102/71 | |
| Post-sauna | 36.8 | 35.2 | 19 | 110 | 131/67 | |
| 3 | Pre-sauna | 37.0 | 35.9 | 15 | 78 | 146/82 |
| During sauna | 37.5 | 36.2 | 20 | 87 | 120/77 | |
| Post-sauna | 37.4 | 35.8 | 16 | 87 | 128/77 | |
| 4 | Pre-sauna | 36.6 | 35.5 | 18 | 73 | 145/80 |
| During sauna | 37.2 | 35.9 | 22 | 107 | 135/82 | |
| Post-sauna | 37.1 | 35.7 | 17 | 89 | 125/80 | |
| 5 | Pre-sauna | 36.5 | 35.4 | 21 | 74 | 146/96 |
| During sauna | 37.8 | 36.3 | 25 | 99 | 142/88 | |
| Post-sauna | 37.6 | 36.0 | 19 | 93 | 137/93 | |
| 6 | Pre-exercise | 36.7 | 35.6 | 13 | 72 | 126/78 |
| During sauna | 37.8 | 36.5 | 18 | 88 | 134/83 | |
| Post-sauna | 37.2 | 35.6 | 16 | 75 | 125/76 |
Note: There was an increase in core body temperature, skin temperature, sweat rate, heart rate, and a decrease in blood pressure with variations in participants 1,2, and 6.
Table 7: Summary of Physiological Measurements for Prostaglandin Blockade at Different Time Points for Sauna Protocol Participant Time Point Core Body Temperature (°C) Skin Temperature (°C) Sweat Rate (ml/min) Heart Rate (bpm) Blood Pressure (mmHg).
| Participant | Time Point | Core Body Temperature (°C) | Skin Temperature (°C) | Sweat Rate (ml/min) | Heart Rate (bpm) | Blood Pressure (mmHg) |
| 1 | Pre-sauna | 36.5 | 35.4 | 13 | 82 | 136/82 |
| During sauna | 37.4 | 36.1 | 21 | 75 | 144/82 | |
| Post-sauna | 38.2 | 36.6 | 17 | 78 | 130/86 | |
| 2 | Pre-sauna | 36.4 | 35.3 | 10 | 62 | 94/62 |
| During sauna | 37.2 | 35.9 | 20 | 83 | 111/77 | |
| Post-sauna | 37.1 | 35.5 | 18 | 83 | 111/64 | |
| 3 | Pre-sauna | 37.0 | 35.9 | 14 | 71 | 128/71 |
| During sauna | 37.8 | 36.5 | 23 | 84 | 133/82 | |
| Post-sauna | 37.1 | 35.5 | 15 | 96 | 125/75 | |
| 4 | Pre-sauna | 36.7 | 35.6 | 17 | 62 | 114/62 |
| During sauna | 37.1 | 36.0 | 21 | 85 | 105/60 | |
| Post-sauna | 37.0 | 35.4 | 16 | 103 | 101/68 | |
| 5 | Pre-sauna | 36.6 | 35.5 | 20 | 77 | 123/77 |
| During sauna | 37.4 | 36.1 | 24 | 87 | 101/61 | |
| Post-sauna | 37.7 | 36.1 | 18 | 98 | 112/61 | |
| 6 | Pre-sauna | 36.7 | 35.6 | 12 | 63 | 104/63 |
| During sauna | 37.3 | 36.0 | 17 | 78 | 123/72 | |
| Post-sauna | 36.8 | 35.2 | 15 | 82 | 121/68 |
Note: There was an increase in core body temperature, skin temperature, sweat rate, heart rate, and blood pressure with variations in participants 1,4 and 5.
Table 8: Summary of Physiological Measurements for Control at Different Time Points for the Steam Bath Protocol Participant Time Point Core Body Temperature (°C) Skin Temperature (°C) Sweat Rate (ml/min) Heart Rate (bpm) Blood Pressure (mmHg).
| Participant | Time Point | Core Body Temperature (°C) | Skin Temperature (°C) | Sweat Rate (ml/min) | Heart Rate (bpm) | Blood Pressure (mmHg) |
| 1 | Pre-steam bath | 36.6 | 35.5 | 15 | 89 | 109/62 |
| During steam bath | 37.1 | 35.8 | 23 | 77 | 103/66 | |
| Post-steam bath | 37.6 | 36.0 | 19 | 86 | 125/72 | |
| 2 | Pre-steam bath | 36.6 | 35.5 | 12 | 64 | 104/63 |
| During steam bath | 37.2 | 35.9 | 22 | 84 | 129/78 | |
| Post-steam bath | 38.5 | 36.9 | 20 | 82 | 131/77 | |
| 3 | Pre-steam bath | 36.5 | 35.4 | 16 | 65 | 122/72 |
| During steam bath | 37.1 | 35.8 | 21 | 97 | 117/71 | |
| Post-steam bath | 37.9 | 36.3 | 17 | 102 | 133/80 | |
| 4 | Pre-steam bath | 36.5 | 35.4 | 19 | 76 | 115/69 |
| During steam bath | 37.0 | 35.7 | 23 | 87 | 132/90 | |
| Post-steam bath | 37.1 | 35.5 | 18 | 85 | 130/92 | |
| 5 | Pre-steam bath | 36.5 | 35.4 | 22 | 83 | 154/90 |
| During steam bath | 37.8 | 36.5 | 26 | 98 | 121/73 | |
| Post-steam bath | 36.9 | 35.3 | 20 | 84 | 132/84 | |
| 6 | Pre-steam bath | 36.3 | 35.2 | 14 | 76 | 126/72 |
| During steam bath | 37.6 | 36.3 | 19 | 83 | 134/85 | |
| Post-steam bath | 36.7 | 35.1 | 17 | 79 | 128/78 |
Note: There was an increase in core body temperature, skin temperature, sweat rate, heart rate, and blood pressure with variations in participant1.
Table 9: Summary of Physiological Measurements for Histamine Blockade at Different Time Points for the Steam Bath Protocol Participant Time Point Core Body Temperature (°C) Skin Temperature (°C) Sweat Rate (ml/min) Heart Rate (bpm) Blood Pressure (mmHg).
| Participant | Time Point | Core Body Temperature (°C) | Skin Temperature (°C) | Sweat Rate (ml/min) | Heart Rate (bpm) | Blood Pressure (mmHg) |
| 1 | Pre-steam bath | 36.7 | 35.6 | 13 | 106 | 120/75 |
| During steam bath | 37.5 | 36.2 | 21 | 83 | 126/79 | |
| Post-steam bath | 36.9 | 35.3 | 17 | 105 | 117/72 | |
| 2 | Pre-steam bath | 36.5 | 35.4 | 10 | 125 | 129/82 |
| During steam bath | 37.5 | 36.2 | 20 | 91 | 125/75 | |
| Post-steam bath | 37.5 | 36.2 | 18 | 103 | 111/67 | |
| 3 | Pre-steam bath | 37.0 | 35.9 | 14 | 78 | 146/82 |
| During steam bath | 37.9 | 36.6 | 19 | 102 | 139/74 | |
| Post-steam bath | 36.7 | 35.1 | 15 | 84 | 119/76 | |
| 4 | Pre-steam bath | 36.6 | 35.5 | 17 | 73 | 145/80 |
| During steam bath | 37.9 | 36.6 | 21 | 92 | 126/75 | |
| Post-steam bath | 37.6 | 36.0 | 16 | 97 | 136/79 | |
| 5 | Pre-steam bath | 36.5 | 35.4 | 20 | 74 | 146/96 |
| During steam bath | 38.0 | 36.7 | 24 | 91 | 140/93 | |
| Post-steam bath | 37.2 | 36.1 | 18 | 88 | 138/86 | |
| 6 | Pre-steam bath | 36.6 | 35.5 | 12 | 82 | 128/83 |
| During steam bath | 37.5 | 36.2 | 17 | 93 | 125/78 | |
| Post-steam bath | 37.1 | 35.5 | 15 | 87 | 121/72 |
Note: There was an increase in core body temperature, skin temperature, sweat rate, heart rate, and a decrease in blood pressure with variations in participants 1, and 2.
Table 10: Summary of Physiological Measurements for Prostaglandin Blockade at Different Time Points for the Steam Bath Protocol Participant Time Point Core Body Temperature (°C) Skin Temperature (°C) Sweat Rate (ml/min) Heart Rate (bpm) Blood Pressure (mmHg).
| Participant | Time Point | Core Body Temperature (°C) | Skin Temperature (°C) | Sweat Rate (ml/min) | Heart Rate (bpm) | Blood Pressure (mmHg) |
| 1 | Pre-steam bath | 36.5 | 35.4 | 11 | 65 | 136/82 |
| During steam bath | 37.5 | 36.2 | 19 | 70 | 139/75 | |
| Post-steam bath | 38.2 | 36.6 | 15 | 89 | 126/78 | |
| 2 | Pre-steam bath | 36.4 | 35.3 | 8 | 74 | 94/62 |
| During steam bath | 37.4 | 36.1 | 18 | 91 | 109/71 | |
| Post-steam bath | 37.8 | 36.2 | 16 | 88 | 142/75 | |
| 3 | Pre-steam bath | 37.0 | 35.9 | 12 | 74 | 128/71 |
| During steam bath | 37.2 | 35.9 | 17 | 95 | 106/66 | |
| Post-steam bath | 36.5 | 34.9 | 13 | 97 | 107/68 | |
| 4 | Pre-steam bath | 36.7 | 35.6 | 15 | 101 | 114/62 |
| During steam bath | 37.1 | 35.8 | 19 | 97 | 121/71 | |
| Post-steam bath | 37.6 | 36.0 | 14 | 99 | 110/69 | |
| 5 | Pre-steam bath | 36.7 | 35.6 | 18 | 83 | 123/77 |
| During steam bath | 37.5 | 36.2 | 22 | 85 | 107/67 | |
| Post-steam bath | 37.8 | 36.2 | 17 | 92 | 104/74 | |
| 6 | Pre-steam bath | 36.6 | 35.5 | 16 | 82 | 123/83 |
| During steam bath | 37.5 | 36.2 | 21 | 93 | 120/75 | |
| Post-steam bath | 37.6 | 36.0 | 18 | 91 | 121/72 |
Note: There was an increase in core body temperature, skin temperature, sweat rate, heart rate, and a decrease in blood pressure with variations in participants 1,2, and 4.
Line Graphs
Line graphs were an effective tool for visualizing trends over time. To illustrate their variations during heat stress and exercise protocols, we plotted core body temperature, skin temperature, heart rate, and blood pressure as line graphs.

Figure 1: Core body temperature generally increases with exercise intensity and gradually decreases to its resting state.

Figure 2: Potential variability raises core body temperature, sustains it, and gradually decreases it to the resting state.

Figure 3: Core body temperature decreases with variability but may show little change with rise and stabilization.

Figure 4: Skin temperature initially increases, fluctuates, and gradually decreases as the body cools down.

Figure 5: Skin temperature increases with exercise and ambient temperature, then decreases with variability and minimal changes to the resting state.

Figure 6: Skin temperature increases with exercise and ambient temperature, then gradually decreases to a resting state.

Figure 7: The sweat rate increases with exercise, intensity, and sustained elevation, but gradually decreases as the body cools down.

Figure 8: As exercise and ambient temperature increase, the sweat rate decreases with variability, then gradually decreases as the body cools down.

Figure 9: As exercise and ambient temperature increase, the sweat rate decreases with variability, then gradually decreases as the body cools down.

Figure 10: With exercise and an increase in ambient temperature, the heart rate increases, then gradually decreases to a resting state with individual variations.

Figure 11: Exercise intensity and an increase in ambient temperature support an increase in heart rate, which then gradually decreases to a resting state with individual variations.

Figure 12: shows a sustained increase in heart rate with exercise intensity and a rise in ambient temperature, followed by a gradual decrease to a resting state with individual variations.

Figure 13: Blood pressure rises quickly with exercise and a rise in ambient temperature, sustained by potential variability, and may have a slight decrease.

Figure 14: Blood pressure increases with exercise and heat stress, reaches stability with individual variation, and may show a slight decrease.

Figure 15: Blood pressure increases with exercise and heat stress, reaches stability with individual variation, and may show a slight decrease.
Bar Charts
We used bar charts to compare the mean sweat rate values and mediators’ responses across various conditions or groups.

Figure 16: There were individual variations; participant 1 recorded the highest for exercise, and participant 5 recorded the highest for sauna and steam bath.

Figure 17: There were individual variations; participant 1 recorded the highest for control, histamine, prostaglandin, and reduction in both histamines, with prostaglandin having the lowest.

Figure 18: There was variation in experimental protocols, with the highest recorded in the sauna in the control group, followed by a steam bath in the prostaglandin group, a sauna for histamine, and then exercise.

Figure 19: There was variation in the experimental groups; control recorded the highest for exercise, sauna, and steam bath, followed by histamine in exercise and sauna, and prostaglandin recorded higher than histamine in steam bath.
Scatter Plots
We utilized scatter plots to investigate potential correlations between sweat rate and core body temperature.

Figure 20: There is a steady positive correlation between sweat rate and core body temperature.

Figure 21: There is a gradual positive correlation between sweat rate and core body temperature.

Figure 22: There is a slight positive correlation between sweat rate and core body temperature.
Heat Maps
We have used heat maps to visualize changes in skin temperature across various body regions during heat stress or exercise, providing a spatial understanding of temperature distribution.
A heat map provides a spatial depiction of the distribution of skin temperature prior to, during, and following physical activity.
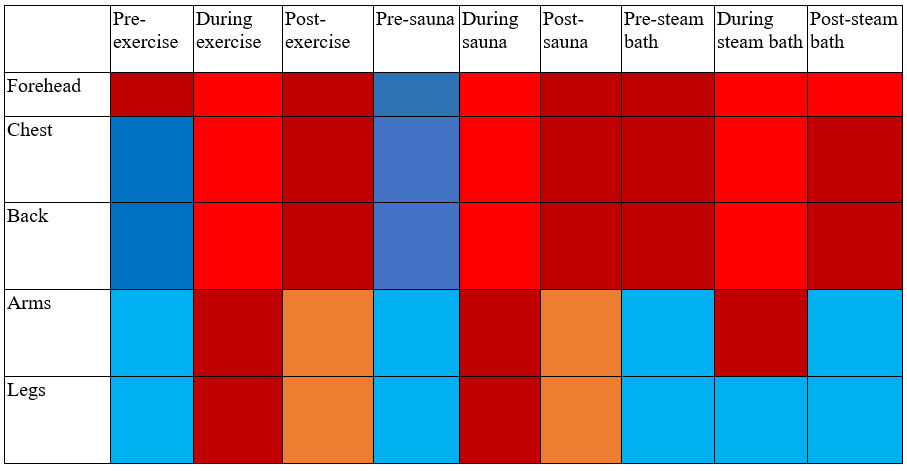
Figure 23: Color coding: Cooler temperatures (lower values)- Blue and Warmer temperatures (higher temperatures)- Red. The intensity of the color indicates the intensity of the temperature change. Darker hues indicate higher temperatures, while lighter hues indicate lower temperatures, providing insights into the spatial distribution, patterns, and trends in skin temperature across various body regions over time.
The forehead recorded the highest temperature, followed by the chest and back, which showed similar patterns and trends. The arms and legs, on the other hand, recorded the lowest average temperature and the most variation between them during the steam bath.
Hypothesis Testing and Comparison
Independent t-tests or ANOVA
We used independent t-tests (for binary comparisons) or ANOVA (for multiple group comparisons) to look at how differences in core body temperature, sweat rate, and heart rate affected mediator responses in different situations.
(a) The study compared the heart rates for control against histamine blockade in the sauna.
| t-Test: Two-Sample Assuming Equal Variances | |||
| Pre-sauna | During sauna | ||
| Mean | 36.5833333 | 37.3 | |
| Variance | 0.00566667 | 0.216 | |
| Observations | 6 | 6 | |
| Pooled Variance | 0.11083333 | ||
| Hypothesized Mean Difference | 0 | ||
| df | 10 | ||
| t Stat | -3.7285729 | ||
| P(T<=t) one-tail | 0.00195978 | ||
| t Critical one-tail | 1.81246112 | ||
| P(T<=t) two-tail | 0.00391955 | ||
| t Critical two-tail | 2.22813885 | ||
Figure 24: Independent t-test for control against histamine with a positive significance of p -value. When histamine blocks prostaglandin in a sauna, the heart rate increases.
Core body temperature for Pre-steam bath against During steam bath.
| t-Test: Two-Sample Assuming Equal Variances | ||||
| Pre-steam bath | During steam bath | |||
| Mean | 36.5 | 37.3 | ||
| Variance | 0.012 | 0.104 | ||
| Observations | 6 | 6 | ||
| Pooled Variance | 0.058 | |||
| Hypothesized Mean Difference | 0 | |||
| df | 10 | |||
| t Stat | -5.7535596 | |||
| P(T<=t) one-tail | 9.2134E-05 | |||
| t Critical one-tail | 1.81246112 | |||
| P(T<=t) two-tail | 0.00018427 | |||
| t Critical two-tail | 2.22813885 | |||
Figure 25: Independent t-test for histamine against prostaglandin with a positive significance of p -value.
Core body temperature comparison for three protocols: exercise, sauna and steam bath.
The study conducted an ANOVA on the single factor sweat rate during a steam bath.
| ANOVA: Single Factor | |||||||
| SUMMARY | |||||||
| Groups | Count | Sum | Average | Variance | |||
| During exercise | 6 | 221.2 | 36.8666667 | 0.17866667 | |||
| During sauna | 6 | 223.8 | 37.3 | 0.216 | |||
| During steam bath | 6 | 223.8 | 37.3 | 0.104 | |||
| ANOVA | |||||||
| Source of Variation | SS | df | MS | F | P-value | F crit | |
| Between Groups | 0.75111111 | 2 | 0.37555556 | 2.25935829 | 0.13877141 | 3.68232034 | |
| Within Groups | 2.49333333 | 15 | 0.16622222 | ||||
| Total | 3.24444444 | 17 | |||||
Figure 26: ANOVA with no significance for P-value across exercise, sauna, and steam bath.
Sweat rate comparison for three experiments.
Sweat rate for control against prostaglandin blockade during steam bath.
| t-Test: Two-Sample Assuming Equal Variances | |||
| Control | Prostaglandin | ||
| Mean | 22.3333333 | 19.3333333 | |
| Variance | 5.46666667 | 3.46666667 | |
| Observations | 6 | 6 | |
| Pooled Variance | 4.46666667 | ||
| Hypothesized Mean Difference | 0 | ||
| df | 10 | ||
| t Stat | 2.45861264 | ||
| P(T<=t) one-tail | 0.01687826 | ||
| t Critical one-tail | 1.81246112 | ||
| P(T<=t) two-tail | 0.03375653 | ||
| t Critical two-tail | 2.22813885 | ||
Figure 27: Independent t-test for control against prostaglandin with a positive significance of p -value.
| ANOVA: Single Factor | Sweat rate during steam bath | |||||
| SUMMARY | ||||||
| Groups | Count | Sum | Average | Variance | ||
| Control | 6 | 134 | 22.3333333 | 5.46666667 | ||
| Histamine | 6 | 122 | 20.3333333 | 5.46666667 | ||
| Prostaglandin | 6 | 116 | 19.3333333 | 3.46666667 | ||
| ANOVA | ||||||
| Source of Variation | SS | df | MS | F | P-value | F crit |
| Between Groups | 28 | 2 | 14 | 2.91666667 | 0.08511257 | 3.68232034 |
| Within Groups | 72 | 15 | 4.8 | |||
| Total | 100 | 17 | ||||
Figure 28: ANOVA with no significance for P-value across exercise, sauna, and steam bath.
Heart rate comparison for three experiments.
Heart rate for control against histamine blockade for sauna.
| t-Test: Two-Sample Assuming Equal Variances | |||
| Control | Histamine | ||
| Mean | 86.6666667 | 98.8333333 | |
| Variance | 22.6666667 | 85.7666667 | |
| Observations | 6 | 6 | |
| Pooled Variance | 54.2166667 | ||
| Hypothesized Mean Difference | 0 | ||
| df | 10 | ||
| t Stat | -2.861975 | ||
| P(T<=t) one-tail | 0.0084498 | ||
| t Critical one-tail | 1.81246112 | ||
| P(T<=t) two-tail | 0.01689959 | ||
| t Critical two-tail | 2.22813885 | ||
Figure 29: Independent t-test for control against histamine with a positive significance of p -value.
Heart rate for histamine against prostaglandin blockade for sauna.
| t-Test: Two-Sample Assuming Equal Variances | |||
| Histamine | Prostaglandin | ||
| Mean | 98.8333333 | 82 | |
| Variance | 85.7666667 | 20.8 | |
| Observations | 6 | 6 | |
| Pooled Variance | 53.2833333 | ||
| Hypothesized Mean Difference | 0 | ||
| df | 10 | ||
| t Stat | 3.99424829 | ||
| P(T<=t) one-tail | 0.00127091 | ||
| t Critical one-tail | 1.81246112 | ||
| P(T<=t) two-tail | 0.00254181 | ||
| t Critical two-tail | 2.22813885 | ||
Figure 30: Independent t-test for histamine against prostaglandin with a positive significance of p -value.
Heart rate comparison for three experiments during sauna.
| ANOVA: Single Factor | ||||||||||||
| SUMMARY | ||||||||||||
| Groups | Count | Sum | Average | Variance | ||||||||
| Control | 6 | 520 | 86.6666667 | 22.6666667 | ||||||||
| Histamine | 6 | 593 | 98.8333333 | 85.7666667 | ||||||||
| Prostaglandin | 6 | 492 | 82 | 20.8 | ||||||||
| ANOVA | ||||||||||||
| Source of Variation | SS | df | MS | F | P-value | F crit | ||||||
| Between Groups | 906.333333 | 2 | 453.166667 | 10.5197318 | 0.00139588 | 3.68232034 | ||||||
| Within Groups | 646.166667 | 15 | 43.0777778 | |||||||||
| Total | 1552.5 | 17 | ||||||||||
Figure 31: ANOVA with significance for P-value across control, histamine, and prostaglandin.
CORRELATION ANALYSIS
We conducted a correlation analysis to determine the strength and direction of the relationships between core body temperature and sweat rate, as well as investigate the potential correlation between heart rate and blood pressure under exercise and heat stress conditions.
Core body temperature with sweat rate in sauna.
| Histamine | ||
| Core body temperature | Sweat rate | |
| Core body temperature | 1 | |
| Sweat rate | 0.03421048 | 1 |
Figure 32: We found a positive and significant correlation between core body temperature and sweat rate in a sauna.
Heart rate with blood pressure in sauna
| Histamine | |||
| Heart rate | Systolic blood pressure | ||
| Heart rate | 1 | ||
| Systolic blood pressure | -0.2650837 | 1 |
Figure 33: We observed a correlation between heart rate and blood pressure.
| Prostaglandin | |||
| Heart rate | Systolic blood pressure | ||
| Heart rate | 1 | ||
| Systolic blood pressure | -0.7886027 | 1 | |
Figure 34: shows a positive, non-significant correlation between heart rate and systolic blood pressure.
Heart rate with blood pressure in steam bath
| Prostaglandin | |||
| Heart rate | Systolic blood pressure | ||
| Heart rate | 1 | ||
| Systolic blood pressure | -0.6632256 | 1 | |
Figure 35: illustrates a positive, nonsignificant correlation between heart rate and systolic blood pressure.
Multivariate Analysis
To evaluate the combined influence of multiple variables on mediator responses, we used multivariate regression models.
This could help to understand how core body temperature, skin temperature, heart rate, and blood pressure collectively influence the response of non-adrenergic and non-cholinergic mediators.
Multivariate analysis for exercise protocol
| Control during exercise. | |||||
| Core body temperature | Skin temperature | Sweat rate | Heart rate | Diastolic blood pressure | |
| Core body temperature | 0.19333333 | ||||
| Skin temperature | 0.02166667 | 0.00888889 | |||
| Sweat rate | 1.38333333 | 0.21666667 | 12.9166667 | ||
| Heart rate | 1.91666667 | 1.56111111 | 9.25 | 475.472222 | |
| Diastolic blood pressure | 3.73333333 | 0.06111111 | 25 | -62.277778 | 96.2222222 |
Figure 36: All metric variables had positive impact on mediator responses.
| Histamine during exercise. | ||||||
| Core body temperature | Skin temperature | Sweat rate | Heart rate | Diastolic blood pressure | ||
| Core body temperature | 0.01888889 | |||||
| Skin temperature | 0.00333333 | 0.0425 | ||||
| Sweat rate | 0.15555556 | -0.1916667 | 17.1388889 | |||
| Heart rate | 0.78333333 | 3.58333333 | -13.5 | 333.666667 | ||
| Diastolic blood pressure | -0.5222222 | 0.70833333 | -4.9722222 | 65.5 | 65.1388889 | |
Figure 37: All metric variables had positive impact on mediator responses except sweat rate and blood pressure.
| Prostaglandin during exercise. | |||||
| Core body temperature | Skin temperature | Sweat rate | Heart rate | Diastolic blood pressure | |
| Core body temperature | 0.09472222 | ||||
| Skin temperature | 0.0225 | 0.1725 | |||
| Sweat rate | 0.63333333 | 0.46666667 | 10.6666667 | ||
| Heart rate | -2.3361111 | 0.10833333 | 0.5 | 174.472222 | |
| Diastolic blood pressure | 1.10833333 | 1.60833333 | 20.1666667 | 11.0833333 | 43.9166667 |
Figure 38: All metric variables had positive impact on mediator responses except heart rate.
Multivariate analysis for Sauna protocol
| Control during sauna. | |||||
| Core body temperature | Skin temperature | Sweat rate | Heart rate | Diastolic blood pressure | |
| Core body temperature | 0.17138889 | ||||
| Skin temperature | 0.17138889 | 0.17138889 | |||
| Sweat rate | 0.10555556 | 0.10555556 | 2.22222222 | ||
| Heart rate | -0.8388889 | -0.8388889 | -2.3888889 | 13.2222222 | |
| Diastolic blood pressure | -0.8638889 | -0.8638889 | -4.8888889 | 12.5555556 | 39.8055556 |
Figure 39: All metric variables had positive impact on mediator responses except heart rate and blood pressure.
| Histamine during sauna. | |||||
| Core body temperature | Skin temperature | Sweat rate | Heart rate | Diastolic blood pressure | |
| Core body temperature | 0.14472222 | ||||
| Skin temperature | 0.13194444 | 0.12472222 | |||
| Sweat rate | 0.02777778 | -0.0944444 | 4.55555556 | ||
| Heart rate | -2.0305556 | -2.0361111 | 9.88888889 | 71.4722222 | |
| Diastolic blood pressure | 1.59444444 | 1.30555556 | 4.05555556 | -13.944444 | 31.5555556 |
Figure 40: All metric variables had positive impact on mediator responses except heart rate, sweat rate, and blood pressure.
| Prostaglandin during sauna. | |||||
| Core body temperature | Skin temperature | Sweat rate | Heart rate | Diastolic blood pressure | |
| Core body temperature | 0.04888889 | ||||
| Skin temperature | 0.04 | 0.03666667 | |||
| Sweat rate | 0.2 | 0.23333333 | 4 | ||
| Heart rate | 0.07777778 | 0.11666667 | -3 | 52.4722222 | |
| Diastolic blood pressure | 1.11111111 | 0.7 | 8.33333333 | -43.444444 | 81.5555556 |
Figure 41: All metric variables had positive impact on mediator responses except heart rate and blood pressure.
Multivariate analysis for steam bath protocol
| Control during steam bath. | |||||
| Core body temperature | Skin temperature | Sweat rate | Heart rate | Diastolic blood pressure | |
| Core body temperature | 0.08666667 | ||||
| Skin temperature | 0.08666667 | 0.08666667 | |||
| Sweat rate | 0.13333333 | 0.13333333 | 4.55555556 | ||
| Heart rate | 0.76666667 | 0.76666667 | 5.77777778 | 57.2222222 | |
| Diastolic blood pressure | -0.0333333 | -0.0333333 | -5.3888889 | -4.9444444 | 67.8055556 |
Figure 42: All metric variables had positive impact on mediator responses except blood pressure.
| Histamine during steam bath. | |||||
| Core body temperature | Skin temperature | Sweat rate | Heart rate | Diastolic blood pressure | |
| Core body temperature | 0.04805556 | ||||
| Skin temperature | 0.02444444 | 0.03555556 | |||
| Sweat rate | 0.26111111 | -0.0444444 | 4.55555556 | ||
| Heart rate | 0.58333333 | 0.66666667 | -4.3333333 | 30.6666667 | |
| Diastolic blood pressure | 0.60277778 | -0.5777778 | 9.88888889 | -8.6666667 | 42.4722222 |
Figure 43: All metric variables had positive impact on mediator responses except sweat rate, heart rate, and blood pressure.
| Prostaglandin during steam bath. | |||||
| Core body temperature | Skin temperature | Sweat rate | Heart rate | Diastolic blood pressure | |
| Core body temperature | 0.02555556 | ||||
| Skin temperature | 0.02555556 | 0.02555556 | |||
| Sweat rate | 0.16111111 | 0.16111111 | 2.88888889 | ||
| Heart rate | -0.9333333 | -0.9333333 | -2.8333333 | 82.5833333 | |
| Diastolic blood pressure | 0.22777778 | 0.22777778 | 1.05555556 | -12.416667 | 12.1388889 |
Figure 44: All metric variables had positive impact on mediator responses except heart rate and blood pressure.
Time Series Analysis
Because data was collected over time, time series analysis techniques were applied to detect patterns, trends, and periodic variations in variables during exercise and heat stress. This involved analyzing fluctuations in core body temperature, sweat rate, and heart rate over the duration of the study. Identifying any cyclic patterns in mediator responses in response to changing thermal conditions.
Core body temperature across the three experimental groups; control, histamine, and prostaglandin blockade.
Core body temperature for exercise protocol.

Figure 45: There was a decrease and a gradual increase up to sustainability.
Core body temperature for sauna protocol.

Figure 46: There was a steady increase up to sustainability.
Core body temperature for steam bath protocol.

Figure 47: There was a gradual increase up to sustainability with variations.
Sweat rate across the three experimental groups; control, histamine, and prostaglandin blockade.
Sweat rate for exercise protocol

Figure 48: There was a gradual decrease up to rest state.
Sweat rate for sauna protocol

Figure 49: There was a steady decrease up to rest state.
Sweat rate for steam bath protocol

Figure 50: There was a steady decrease up to rest state.
Heart rate across the three experimental groups: control, histamine, and prostaglandin blockade.
Heart rate for exercise protocol.

Figure 51: There was a steady increase in sustainability and decrease up to rest state.
Heart rate for sauna protocol.

Figure 52: There was a gradual increase in sustainability and decrease up to rest state.
Heart rate for steam bath protocol

Figure 53: There was a steady increase in sustainability and decrease up to rest state.
By utilizing these statistical analysis methods, we evaluated the significance of differences between conditions, explored relationships between variables, assessed the impact of multiple factors on outcomes, and understand temporal patterns in physiological responses during heat stress and exercise protocols.
DISCUSSION, CONCLUSIONS, AND RECOMMENDATIONS
Core body temperature and skin temperature change during exercise.
Regular exercise often elevates the body’s internal temperature due to the metabolic heat produced by working muscles. Martin et al. (2019) discovered that high-intensity exercise causes a greater increase in body temperature. Sweating is necessary for heat dispersal and body temperature regulation during physical activity (Martin et al., 2019). After physical activity, the core body temperature progressively falls as the body goes back to its normal state of rest (Martin et al., 2019). The skin temperature increases during the beginning of exercise due to an increase in blood flow near the surface, which helps to release heat. Ambient temperature, clothing type, and degree of physical activity all influence temperature rise (Travers et al., 2022). Sweat evaporation from the skin is a thermoregulatory process that helps the body maintain a steady temperature during physical exercise (Travers et al., 2022). Following physical exertion, the skin temperature typically decreases as the body gradually returns to a cooler state (Travers et al., 2022). Temperature fluctuations are influenced by variances in individuals, their level of physical fitness, the surrounding environment, and their hydration status. To efficiently regulate your body’s temperature, it is crucial to be attentive to the signs it provides and provide adequate hydration.
Core body temperature and skin temperature change during a sauna or steam bath.
Heat-stress settings, such as saunas and steam baths, cause major alterations in temperature regulation. Core body temperature rises as the body absorbs heat from the environment, causing mechanisms such as perspiration and increased blood circulation to disperse heat (Adiele et al., 2022; Siquier-Coll et al., 2023). This increases heart rate as the body works harder to cool itself (Siquier-Coll et al., 2023). Skin temperature rises in response to rising ambient temperatures, while vasodilation and perspiration contribute to heat loss (Adiele et al., 2022; Sasai et al., 2023). Following heat exposure, the temperature of the skin may stay elevated while the body is in the process of cooling down (Nur Siddiq and Mulyono, 2020). Sufficient hydration is essential for mitigating the risk of dehydration caused by excessive sweating in hot conditions (Fehling et al., 2015). Individuals should pay close attention to their body’s signals, ensure adequate hydration, and avoid prolonged exposure to extreme temperatures, especially if they have pre-existing medical conditions. Before engaging in such activities, consult a healthcare practitioner for guidance.
The role of prostaglandins and histamines in regulating body temperature
Inhibiting prostaglandins and histamines can have a substantial effect on the body’s thermoregulation mechanisms. Prostaglandins modulate body temperature by acting on the hypothalamus. Blocking them may interfere with the body’s ability to regulate temperature, perhaps leading to a decrease in core body temperature (Gerstberger et al., 1994; Tymoshchuk et al., 2018). Conversely, when histamines are inhibited, they can hinder the expansion of blood vessels and enhance the circulation of blood to the skin, so preventing the emission of heat. This has the potential to lead to an increased core body temperature (Gerstberger et al., 1994). Prostaglandins and histamines affect skin temperature by widening blood vessels and improving blood flow to the skin. Blocking these chemicals could change how the skin responds to changes in its environment and its blood flow (Branco et al., 2018; Gerstberger et al., 1994). It’s important to understand how prostaglandins and histamines affect temperature regulation, especially when thinking about medicines that target these pathways for certain medical conditions. A healthcare professional must closely monitor body and skin temperature responses for safe and effective management of related conditions.
The sweat rate responds to exercise intensity
Research findings indicate that the rate at which perspiration is produced during exercise is controlled by multiple factors. The level of exercise intensity has a significant impact on sweat rates. Increased degrees of intensity result in heightened perspiration as the body generates a greater amount of thermal energy. Conversely, lesser levels of intensity may initially lead to reduced rates of sweating, which gradually increase as the body becomes warmer (Foster et al., 2023). The duration of exercise affects sweat rate, with a progressive rise reported as the body temperature increases, until reaching a stable level to regulate core temperature (Ravanelli et al., 2020). Temperature and humidity exert a notable influence on sweat rates, since elevated environmental conditions prompt heightened sweating in an effort by the body to enhance cooling efficiency (Smith et al., 2021). The rates at which individuals sweat are noticeably influenced by their degree of physical fitness and hydration. Individuals who participate in more intense physical activity and maintain proper hydration tend to report higher rates of perspiration. Perspiration is crucial for regulating body temperature and enhancing physical performance (Klous et al., 2021; Prada et al., 2020). Individual variations, such as hereditary factors and differences between genders, also have a role in the variability in sweat rates during exercise. This highlights the significance of monitoring sweat production to regulate hydration and performance effectively.
The initial sweat rate response to heat stress
Under heat-stress conditions, like those experienced in saunas and steam baths, the body’s sweat rate undergoes substantial alterations in response to elevated temperatures. First, there is a sudden surge in the rate of sweat production as the body tries to release heat (Fujii et al., 2023). High temperature is known to be a stress-inducing element that stimulates the activation of sweat glands to improve the process of evaporative cooling (Fujii et al., 2023). The production of sweat is increased to facilitate the process of cooling, and ongoing sweating helps in the regulation of body temperature (Fujii et al., 2023). Nevertheless, the increased rate of perspiration can lead to a substantial depletion of fluids, highlighting the danger of dehydration if sufficient fluid consumption is not upheld (Akerman et al., 2016). Genetic characteristics, fitness levels, and acclimatization to heat can independently influence sweat rates during heat stress (Foster et al., 2020). Comprehending these reactions is essential for effectively controlling fluid consumption and maximizing temperature regulation in difficult situations, emphasizing the significance of maintaining proper hydration and being vigilant for indications of dehydration during periods of heat strain.
The sweat rate has an impact on both prostaglandin and histamine blockade
Suppressing prostaglandins and histamines can indeed affect the rate of perspiration and the mechanism of thermoregulation. Prostaglandins have a vital role in promoting heat responses and triggering sweat production. Blocking prostaglandins can reduce the amount of sweating and hinder the body’s ability to regulate temperature (Fujii et al., 2015). Blocking histamines might potentially lower sweat rates and change skin blood flow responses by inhibiting the activation of sweat glands and reducing skin blood flow (Metzler-Wilson & Wilson, 2013).
These blockades may disrupt heat dissipation mechanisms, increasing the risk of overheating and heat-related issues, highlighting the importance of efficient sweating for cooling during thermal stress (Fujii et al., 2015). Genetics, overall health, and medication dosages can all affect how different people respond to these blockades. This highlights the need for personalized monitoring and healthcare provider guidance when undergoing treatments that affect these pathways (Metzler-Wilson & Wilson, 2013).
Heart rate and blood pressure respond to exercise intensity
During physical activity, the heart rate and blood pressure change rapidly to meet the body’s increased demand for oxygen and energy. The heart rate rises quickly initially to enhance the supply of oxygen to the working muscles, with higher-intensity physical activity resulting in a greater increase (Wazir Ali et al., 2022). During exercise of moderate intensity, the heart rate enters a constant state to fulfil the oxygen demands. After physical activity, it gradually diminishes when the body returns to a state of rest (Wazir Ali et al., 2022). During muscular oxygen demand, systolic blood pressure generally rises initially, and it continues to increase during intensive activity. Nevertheless, it stabilizes when there is a modest level of activity (Ikhsani et al., 2023). During exercise, the diastolic blood pressure may vary or slightly decrease as a result of vasodilation in the active muscles. The heart’s increased blood pumping leads to an elevation in pulse pressure (Ikhsani et al., 2023). Various factors, including cardiovascular fitness, exercise style, and mental state, can impact these changes (Abderrahmen et al., 2024; ŠTURSOVÁ et al., 2023). It is critical to monitor heart rate and blood pressure when exercising to assess cardiovascular health and exercise intensity. This emphasises the importance of staying hydrated, exercising at an appropriate fitness level, and seeking medical attention if you experience unusual symptoms (Sathiyabama et al., 2023).
Heart Rate and Blood Pressure: Initial Response to Heat Stress
When exposed to elevated temperatures in saunas and steam baths, individuals generally have an initial rise in heart rate as their body endeavors to maintain blood flow and cardiac output (Cottle et al., 2023; Ikhsani et al., 2023). Extended heat exposure can lead to a sustained elevation in heart rate as the body attempts to dissipate heat (Leach et al., 2024). At first, the systolic blood pressure may rise to enhance blood flow to the skin for the specific goal of cooling. Nevertheless, over an extended time, the body may adapt to heat stress, resulting in the stabilization or minor reduction of its effects (Ikhsani et al., 2023). Vasodilation and enhanced cutaneous blood flow may lead to a modest or minor decrease in diastolic blood pressure (Ikhsani et al., 2023; Leach et al., 2024). Heat stress causes extensive vasodilation, which affects the reactions of heart rate and blood pressure (Ikhsani et al., 2023). In instances of high temperature, the loss of bodily fluids through perspiration can impact the regulation of blood volume and pressure. This highlights the importance of keeping adequate water to effectively control cardiovascular responses in situations of heat stress (Ikhsani et al., 2023).
Prostaglandins and histamine blockade have an impact on heart rate and blood pressure regulation
The regulation of heart rate and blood pressure can be significantly influenced by the inhibition of prostaglandins and histamines, as these chemicals play vital roles in modulating vascular tone and inflammation (Kalafutova et al., 2014; Rivasi et al., 2022). Inhibiting prostaglandins can alter the heart’s rhythm and its reaction to stress by affecting the autonomic nervous system, which they regulate. Conversely, inhibiting histamine could alter the heart’s reaction to stresses and its overall functionality (Kalafutova et al., 2014; Rivasi et al., 2022). In addition, prostaglandins modify the tone of blood vessels, so it affects the regulation of blood pressure. Blocking them may alter systemic vascular resistance and blood pressure levels. Conversely, histamines affect blood arteries by modifying blood pressure and vascular permeability. This has the potential to alter the responsiveness of blood vessels and the level of resistance within the entire blood vessel system (Kalafutova et al., 2014; Rivasi et al., 2022). It is essential to monitor cardiovascular reactions when suppressing prostaglandin and histamine, as changes in these responses can affect autonomic function. Consulting your physician is imperative when dealing with any negative impacts on blood pressure and heart rate management (Kalafutova et al., 2014; Rivasi et al., 2022).
Conclusion
The study of the reactivity of non-adrenergic-non-cholinergic (NANC) mediators to thermal balance in physically active people who are prone to heat illness can provide insight into the complex physiological systems that regulate body temperature. A detailed understanding of how prostaglandins and histamines regulate body temperature is essential for analyzing the body’s response to heat stress and minimizing the risk of heat-related diseases.
This study examines the effects of blocking prostaglandin and histamine on heart rate and blood pressure. This study investigates the potential consequences of interrupting these pathways during thermal stress on the cardiovascular system. The observed changes in heart rate and blood pressure highlight the complex interplay between these mediators and cardiovascular regulation, underscoring the importance of managing thermal balance in at-risk populations.
Recommendations
Clinical Implications, healthcare professionals who work with individuals at risk of heart disease due to their lifestyle should take into account the influence of prostaglandin and histamine regulation on cardiovascular function. Assessing heart rate and blood pressure reactions during thermal stress can aid in identifying individuals prone to heat-related problems.
Personalized therapies, consist of adjusting treatments according to individual variations in reactivity to non-adrenergic, non-cholinergic (NANC) mediators. It is essential for enhancing thermal equilibrium in people who are susceptible to temperature variations. Personalized approaches to reducing heat disease can be developed by taking into account genetic traits, levels of physical fitness, and interactions with medications.
To properly address heat stress, it is crucial to prioritise sufficient hydration and employ appropriate cooling methods. Efficiently controlling body temperature and reducing the occurrence of heat-related illnesses in vulnerable populations can be achieved by ensuring sufficient hydration and implementing suitable cooling methods.
Further investigation is required to explore other routes that are independent of adrenaline or acetylcholine and their associations with the regulation of body temperature. This could improve our understanding of the physiological mechanisms associated with heat. Subsequent investigations should explore the impact of supplementary mediators on the cardiovascular responses to heat stress in different populations.
By implementing these recommendations into medical practice and conducting additional research, healthcare professionals can effectively regulate thermal balance in individuals who are susceptible to heat-related conditions, thus improving outcomes and promoting overall well-being in environments with increased heat exposure.
Abbreviations
NANC (non-adrenergic non- Cholinergic)
HSR (Heat Stress Response)
TST (thermoregulatory sweat test)
Core body temperature (CT)
ST: Skin temperature
NO: Nitric oxide
VIP (vasoactive intestinal peptide).
cGMP: cyclic guanosine monophosphate
ADTs: axillary digital thermometers
Non-contact (infrared) forehead thermometers (NCIFTs)
BT: body temperature
CV: Cardiovascular
Whole-body sweat loss (WBSL)
WBSR (whole-body sweating rate)
X is during exercise.
PRE-EX is pre-exercise.
POST-EX is post-exercise.
Skin blood flow (SkBF)
In a reference state, the formula qs,r represents the perfusion rate.
AVD defines centrally mediated active vasodilation.
The central temperature (Tc)
mean skin temperature (Ts)
Exercise intensity (VO2)
CVCM defines reflexly mediated cutaneous vasoconstriction.
CVCL defines locally mediated cutaneous vasoconstriction.
CVCE defines exercise’s effect on cutaneous vasoconstriction and mean arterial pressure.
USA: United States of America
ANOVA (analysis of variance)
Ethical consideration
The Selinus University of Science and Literature research ethics committee provided ethical approval, demonstrating the researchers’ dedication to conducting the study ethically.
Written and verbal consent was obtained from the respondents before their participation in the study, ensuring that they were fully informed about the study’s purpose, procedures, and potential risks or benefits.
Seeking ethical approval and obtaining informed consent were important ethical considerations in research, as they protected the rights and well-being of the participants and ensured that the study adhered to ethical guidelines and principles.
These measures demonstrated the researchers’ commitment to conducting the study in an ethical manner and respecting the autonomy and privacy of the participants.
By obtaining ethical approval and informed consent, the researcher upheld the principles of beneficence, respect for autonomy, and justice in the study.
REFERENCES
- 2022 Conference Poster Collection: Thermoregulation. (2022). AORN Journal, 116(5). https://doi.org/10.1002/aorn.13812
- Abderrahmen, T., Chaouki, H. A., Mehamed, G., Khaled, K. A., & Rachid, B. (2024). Impact of exercise modalities on blood pressure control in hypertensive patients. International Journal of Health Sciences, 8(S1). https://doi.org/10.53730/ijhs.v8ns1.14701
- Adiele, D., Chantell, G., & Breukelman, G. J. (2022). Exercise-Heat Stress, Hyperthermia, Dehydration and Fatigue Effects on Cognitive Performance among SemiProfessional Male Athletes. Physical Activity Review, 10(1). https://doi.org/10.16926/PAR.2022.10.02
- Agaba, D. C., Migisha, R., Lugobe, H. M., Katamba, G., & Ashaba, S. (2020). A 10-Year Risk of Cardiovascular Disease among Patients with Severe Mental Illness at Mbarara Regional Referral Hospital, Southwestern Uganda. BioMed Research International, 2020. https://doi.org/10.1155/2020/2508751
- Akerman, A. P., Tipton, M., Minson, C. T., & Cotter, J. D. (2016). Heat stress and dehydration in adapting for performance: Good, bad, both, or neither? In Temperature (Vol. 3, Issue 3). https://doi.org/10.1080/23328940.2016.1216255
- Alele, F. O., Malau-Aduli, B. S., Malau-Aduli, A. E. O., & Crowe, M. J. (2020). Epidemiology of exertional heat illness in the military: A systematic review of observational studies. In International Journal of Environmental Research and Public Health (Vol. 17, Issue 19). https://doi.org/10.3390/ijerph17197037
- Andrade, A. D. N., Vale, M. E. G., Melo, M. L. V., Isidório, U. D. A., Sousa, M. N. A. de, Araujo, W. A. de, Custódio, P. P., & Assis, E. V. de. (2018). Fatores de risco cardiovasculares e qualidade de vida em universitários. Revista de Enfermagem UFPE on Line, 12(10). https://doi.org/10.5205/1981-8963-v12i10a237491p2743-2752-2018
- Araujo-Moura, K., Souza, L. G., Mello, G. L., & De Moraes, A. C. F. (2022). Blood pressure measurement in pediatric population: comparison between automated oscillometric devices and mercury sphygmomanometers—a systematic review and meta-analysis. In European Journal of Pediatrics (Vol. 181, Issue 1). https://doi.org/10.1007/s00431-021-04171-3
- Atkins, W., McKenna, Z., Foster, J., Belval, L., Orth, B., Johnson, E., Benning, M., Watso, J., Hakes, C., Jay, O., & Crandall, C. (2023). Core temperature responses in well-healed burn survivors during exercise heat stress: effect of cooling modalities. Physiology, 38(S1). https://doi.org/10.1152/physiol.2023.38.s1.5733355
- Atkinson, D. J., Romeiser, J. L., Almasry, I. O., Tannous, H. J., Parikh, P. B., & Bennett-Guerrero, E. (2023). Randomized controlled trial of liberal vs. standard fasting instructions in percutaneous cardiac procedures. Perioperative Medicine, 12(1). https://doi.org/10.1186/s13741-023-00333-z
- Baker, L. (2016). Sweat testing methodology in the field: Challenges and best practices. Sports Science Exchange, 28(161).
- Bali, A., & Jaggi, A. S. (2015). Clinical experimental stress studies: Methods and assessment. Reviews in the Neurosciences, 26(5). https://doi.org/10.1515/revneuro-2015-0004
- Branco, A. C. C. C., Yoshikawa, F. S. Y., Pietrobon, A. J., & Sato, M. N. (2018). Role of Histamine in Modulating the Immune Response and Inflammation. In Mediators of Inflammation (Vol. 2018). https://doi.org/10.1155/2018/9524075
- Brasier, N., Widmer, A. F., Osthoff, M., & Eckstein, J. (2021). Digital biomarkers from sweat analysis for therapeutic drug monitoring in soft tissue infections. DigiBiom 2021 – Proceedings of the 2021 Future of Digital Biomarkers. https://doi.org/10.1145/3469266.3471179
- Braun, K., Oeckl, J., Westermeier, J., Li, Y., & Klingenspor, M. (2018). Non-adrenergic control of lipolysis and thermogenesis in adipose tissues. In Journal of Experimental Biology (Vol. 121). https://doi.org/10.1242/jeb.165381
- Bright, B., PS, A., & Kumar KP, G. (2023). Diagnostic Accuracy of Non-Contact Infrared Thermometer in Comparison with Mercury Thermometer and Digital Thermometers. International Journal of Health Sciences and Research, 13(3). https://doi.org/10.52403/ijhsr.20230318
- Chakalian, P. M., Kurtz, L., Harlan, S. L., White, D., Gronlund, C. J., & Hondula, D. M. (2019). Exploring the Social, Psychological, and Behavioral Mechanisms of Heat Vulnerability in the City of Phoenix, AZ. Journal of Extreme Events, 06(03n04). https://doi.org/10.1142/s2345737620500062
- Charkoudian, N. (2016). Human thermoregulation from the autonomic perspective. In Autonomic Neuroscience: Basic and Clinical (Vol. 196). https://doi.org/10.1016/j.autneu.2016.02.007
- Charkoudian, N., & Morrison, S. F. (2022). Physiology of thermoregulation: central and peripheral mechanisms. In Primer on the Autonomic Nervous System, Fourth Edition. https://doi.org/10.1016/B978-0-323-85492-4.00104-6
- Chen, A., Zhu, J., Lin, Q., & Liu, W. (2022). A Comparative Study of Forehead Temperature and Core Body Temperature under Varying Ambient Temperature Conditions. International Journal of Environmental Research and Public Health, 19(23). https://doi.org/10.3390/ijerph192315883
- Cook, I. (2022). Objectively-measured step cadence and walking patterns in a rural African setting: a cross-sectional analysis. BMC Research Notes, 15(1). https://doi.org/10.1186/s13104-022-06045-9
- Cottle, R., Fisher, K., Wolf, S. T., & Kenney, W. L. (2023). Heart rate responses during progressive heat stress in young, healthy adults (PSU HEAT Project). Physiology, 38(S1). https://doi.org/10.1152/physiol.2023.38.s1.5731315
- Cox, Z., Zalawadiya, S., Simonato, M., Redfors, B., Zhou, Z., Kotinkaduwa, L., Zile, M., Udelson, J., Lim, D. S., Grayburn, P. A., Mack, M. J., Abraham, W. T., Stone, G. W., & Lindenfeld, J. (2022). Maximally tolerated guideline-directed medical therapy and barriers to optimization in patients with heart failure with reduced ejection fraction: the COAPT trial. European Heart Journal, 43(Supplement_2). https://doi.org/10.1093/eurheartj/ehac544.975
- Dautta, M., Ayala-Cardona, L. F., Davis, N., Aggarwal, A., Park, J., Wang, S., Gillan, L., Jansson, E., Hietala, M., Ko, H., Hiltunen, J., & Javey, A. (2023). Tape-Free, Digital Wearable Band for Exercise Sweat Rate Monitoring. Advanced Materials Technologies, 8(6). https://doi.org/10.1002/admt.202201187
- DeHan, P. J., Warren, K. C., Buchanan, B. K., & DeGroot, D. W. (2023). Gastrointestinal Associated Exertional Heat Stroke. Current Sports Medicine Reports, 22(4). https://doi.org/10.1249/JSR.0000000000001054
- Douglas, P. (2022). Re-thinking lactation-related nipple pain and damage. In Women’s Health (Vol. 18). https://doi.org/10.1177/17455057221087865
- Du, Q., & Zhou, Y. (2016). Placebo-controlled assessment of somnolence effect of cetirizine: a meta-analysis. International Forum of Allergy and Rhinology, 6(8). https://doi.org/10.1002/alr.21746
- Dwyer, I. J., Barry, S. J. E., Megiddo, I., & White, C. J. (2022). Evaluations of heat action plans for reducing the health impacts of extreme heat: methodological developments (2012–2021) and remaining challenges. In International Journal of Biometeorology (Vol. 66, Issue 9). https://doi.org/10.1007/s00484-022-02326-x
- Fealey, R. D. (2018). Thermoregulation in neuropathies. In Handbook of Clinical Neurology (Vol. 157). https://doi.org/10.1016/B978-0-444-64074-1.00048-3
- Fehling, P. C., Haller, J. M., Lefferts, W. K., Hultquist, E. M., Wharton, M., Rowland, T. W., & Smith, D. L. (2015). Effect of exercise, heat stress and dehydration on myocardial performance. Occupational Medicine, 65(4). https://doi.org/10.1093/occmed/kqv015
- Foster, J., Balmain, B. N., Wilhite, D. P., Watso, J. C., Babb, T. G., Cramer, M. N., BelvaL, L. N., & Crandall, C. G. (2023). Inhibiting regional sweat evaporation modifies the ventilatory response to exercise: interactions between core and skin temperature. Journal of Applied Physiology (Bethesda, Md. : 1985), 134(4). https://doi.org/10.1152/japplphysiol.00597.2022
- Foster, J., Hodder, S. G., Lloyd, A. B., & Havenith, G. (2020). Individual Responses to Heat Stress: Implications for Hyperthermia and Physical Work Capacity. In Frontiers in Physiology (Vol. 11). https://doi.org/10.3389/fphys.2020.541483
- Fujii, N., McGinn, R., Halili, L., Singh, M. S., Kondo, N., & Kenny, G. P. (2015). Cutaneous vascular and sweating responses to intradermal administration of ATP: A role for nitric oxide synthase and cyclooxygenase? Journal of Physiology, 593(11). https://doi.org/10.1113/JP270147
- Fujii, N., Tanabe, Y., Amano, T., Watanabe, K., Kondo, N., Nishiyasu, T., & Kenny, G. P. (2023). Serum, interstitial and sweat ATP in humans exposed to heat stress: Insights into roles of ATP in the heat loss responses. Clinical Physiology and Functional Imaging, 43(5). https://doi.org/10.1111/cpf.12825
- Gamboa, L., Lafuente, A. S., Morera-Herreras, T., Garcia, M., Aguirre, C., & Lertxundi, U. (2023). Analysis of heat stroke and heat exhaustion cases in EudraVigilance pharmacovigilance database. European Journal of Clinical Pharmacology, 79(5). https://doi.org/10.1007/s00228-023-03487-3
- Gerstberger, R., Hjelmqvist, H., & Keil, R. (1994). Nitric Oxide Modulates Thermoregulatory Effector Mechanisms in the Conscious Rabbit. In Thermal Balance in Health and Disease. https://doi.org/10.1007/978-3-0348-7429-8_69
- Gerth, M. A., Mußmann, Y. M., Büchler, B., Hartmann, E. K., & Wittenmeier, E. (2023). Preoperative fasting in children—Experiences with implementing a liberal fasting policy. Anaesthesiologie, 72(8). https://doi.org/10.1007/s00101-023-01303-2
- Gifford, R. M., Todisco, T., Stacey, M., Fujisawa, T., Allerhand, M., Woods, D. R., & Reynolds, R. M. (2019). Risk of heat illness in men and women: A systematic review and meta-analysis. Environmental Research, 171. https://doi.org/10.1016/j.envres.2018.10.020
- Golubovskaya, D. P., Karetnikova, V. N., Osokina, A. V., Oleinik, I. R., & Barbarash, O. L. (2023). Clinical Efficacy and Safety of Empagliflozin in Patients with Acute Heart Failure from the First Day of Hospitalization. Rational Pharmacotherapy in Cardiology, 19(2). https://doi.org/10.20996/1819-6446-2023-03-02
- Guy, J. H., Edwards, A. M., Miller, C. M., Deakin, G. B., & Pyne, D. B. (2017). Short-term reliability of inflammatory mediators and response to exercise in the heat. Journal of Sports Sciences, 35(16). https://doi.org/10.1080/02640414.2016.1227464
- Guzman-Echavarria, G., Middel, A., & Vanos, J. (2023). Beyond heat exposure — new methods to quantify and link personal heat exposure, stress, and strain in diverse populations and climates: The journal Temperature toolbox. Temperature, 10(3). https://doi.org/10.1080/23328940.2022.2149024
- Hanna, N., & Riad, K. (2020). Mechanisms of thermal dysregulation in primary hyperhidrosis and hypohidrosis. In Journal of Physiology (Vol. 598, Issue 21). https://doi.org/10.1113/JP280322
- Hata, F., Takeuchi, T., Nishio, H., & Fujita, A. (2000). Mediators and intracellular mechanisms of NANC relaxation of smooth muscle in the gastrointestinal tract. In Journal of Smooth Muscle Research (Vol. 36, Issue 6). https://doi.org/10.1540/jsmr.36.181
- I Bon, E. (2023). Mediators of the Nervous System Kinds Characteristic. Biomedical Journal of Scientific & Technical Research, 48(4). https://doi.org/10.26717/bjstr.2023.48.007692
- Ibrahim, A. A., Khan, M., Nnaji, C., & Koh, A. S. (2023). Assessing Non-Intrusive Wearable Devices for Tracking Core Body Temperature in Hot Working Conditions. Applied Sciences (Switzerland), 13(11). https://doi.org/10.3390/app13116803
- Ikhsani, R., Tiksnadi, B. B., & Putra, A. P. (2023). 52. The Association of Cardiovascular Risk Factors and Blood Pressure Changes after Exercise in Coronary Artery Disease Patients. Journal of Hypertension, 41(Suppl 2). https://doi.org/10.1097/01.hjh.0000935588.24607.a0
- Johnson, J. M., & Kellogg, D. L. (2010). Thermoregulatory and thermal control in the human cutaneous circulation. Frontiers in Bioscience – Scholar, 2 S(3). https://doi.org/10.2741/s105
- Kalafutova, S., Juraskova, B., & Vlcek, J. (2014). The impact of combinations of non-steroidal anti-inflammatory drugs and anti-hypertensive agents on blood pressure. In Advances in Clinical and Experimental Medicine (Vol. 23, Issue 6). https://doi.org/10.17219/acem/37357
- Kiatkitroj, K., Arphorn, S., Tangtong, C., Maruo, S. J., & Ishimaru, T. (2022). Risk factors associated with heat-related illness among sugarcane farmers in Thailand. Industrial Health, 60(5). https://doi.org/10.2486/indhealth.2021-0161
- Klous, L., de Ruiter, C. J., Scherrer, S., Gerrett, N., & Daanen, H. A. M. (2021). The (in)dependency of blood and sweat sodium, chloride, potassium, ammonia, lactate and glucose concentrations during submaximal exercise. European Journal of Applied Physiology, 121(3). https://doi.org/10.1007/s00421-020-04562-8
- Lahondère, C. (2023). Recent advances in insect thermoregulation. In Journal of Experimental Biology (Vol. 226, Issue 18). https://doi.org/10.1242/jeb.245751
- Laxminarayan, S., Hornby, S., Belval, L. N., Giersch, G. E. W., Morrissey, M. C., Casa, D. J., & Reifman, J. (2023). Prospective Validation of 2B-Cool: Integrating Wearables and Individualized Predictive Analytics to Reduce Heat Injuries. Medicine and Science in Sports and Exercise, 55(4). https://doi.org/10.1249/MSS.0000000000003093
- Leach, O. K., Strong, K., Mack, G. W., & Gifford, J. R. (2024). The vascular response to acute sauna heating is similar in young and middleaged adults. Journal of Applied Physiology, 136(3). https://doi.org/10.1152/japplphysiol.00287.2023
- Lenasi, H., & Šijanec, J. (2023). (1) J. The Physiology of Thermoregulation in Exercise: A Brief Review. In European Medical Journal (Vol. 7, Issue 1).
- Li, F., Yigitcanlar, T., Nepal, M., Thanh, K. N., & Dur, F. (2022). Understanding Urban Heat Vulnerability Assessment Methods: A PRISMA Review. In Energies (Vol. 15, Issue 19). https://doi.org/10.3390/en15196998
- Lin, J., Fu, Y., Lin, Y., Yang, H., Zhang, X., & Zhan, Y. (2023). The Value of Non-Contact Infrared Thermometer in Measuring Temperatures of Different Body Surfaces: A Clinical Diagnostic Study. Journal of Health and Environmental Research. https://doi.org/10.11648/j.jher.20230902.11
- López Dávila, A. J. (2014). Actualidad en termorregulación. Pensar En Movimiento: Revista de Ciencias Del Ejercicio y La Salud, 12(2). https://doi.org/10.15517/pensarmov.v12i2.14918
- Machado-Moreira, C. A., McLennan, P. L., Lillioja, S., Van Dijk, W., Caldwell, J. N., & Taylor, N. A. S. (2012). The cholinergic blockade of both thermally and non-thermally induced human eccrine sweating. Experimental Physiology, 97(8). https://doi.org/10.1113/expphysiol.2012.065037
- Martin, T., Dauvilliers, Y., Koumar, O. C., Besnard, S., Dauphin, F., & Bessot, N. (2019). Dual orexin receptor antagonist induces changes in core body temperature in rats after exercise. Scientific Reports, 9(1). https://doi.org/10.1038/s41598-019-54826-3
- Matsuda, N. M., & Miller, S. M. (2010). Non-adrenergic non-cholinergic inhibition of gastrointestinal smooth muscle and its intracellular mechanism(s). In Fundamental and Clinical Pharmacology (Vol. 24, Issue 3). https://doi.org/10.1111/j.1472-8206.2009.00761.x
- Matterne, U., Böhmer, M. M., Weisshaar, E., Jupiter, A., Carter, B., & Apfelbacher, C. J. (2019). Oral H1 antihistamines as “add-on” therapy to topical treatment for eczema. In Cochrane Database of Systematic Reviews (Vol. 2019, Issue 1). https://doi.org/10.1002/14651858.CD012167.pub2
- Metzler-Wilson, K., & Wilson, T. E. (2013). Topical anaesthesia does not affect cutaneous vasomotor or sudomotor responses in human skin. Autonomic and Autacoid Pharmacology, 33(3–4). https://doi.org/10.1111/aap.12007
- Morrissey, M. C., Langan, S. P., Brewer, G. J., Struder, J. F., Navarro, J. S., Nye, M. N., & Casa, D. J. (2023). Limitations associated with thermoregulation and cardiovascular research assessing laborers performing work in the heat. In American Journal of Industrial Medicine (Vol. 66, Issue 4). https://doi.org/10.1002/ajim.23462
- Mündel, T. (2023). Human thermal resilience and vulnerability to environmental heat: Does a molecular signature underlie pathophysiology? In Journal of Physiology (Vol. 601, Issue 12). https://doi.org/10.1113/JP284704
- Muniyandi, M., Sellappan, S., Chellaswamy, V., Ravi, K., Karthikeyan, S., Thiruvengadam, K., Selvam, J. M., & Karikalan, N. (2022). Diagnostic accuracy of mercurial versus digital blood pressure measurement devices: a systematic review and meta-analysis. Scientific Reports, 12(1). https://doi.org/10.1038/s41598-022-07315-z
- Nazari, S., Kourosh-Arami, M., Komaki, A., & Hajizadeh, S. (2020). Relative contribution of central and peripheral factors in superficial blood flow regulation following cold exposure. In Physiology and Pharmacology (Iran) (Vol. 24, Issue 2). https://doi.org/10.32598/ppj.24.2.50
- Nazarian, N., Liu, S., Kohler, M., Lee, J. K. W., Miller, C., Chow, W. T. L., Alhadad, S. B., Martilli, A., Quintana, M., Sunden, L., & Norford, L. K. (2021). Project Coolbit: Can your watch predict heat stress and thermal comfort sensation? Environmental Research Letters, 16(3). https://doi.org/10.1088/1748-9326/abd130
- Ngaage, D. L., Mitchell, N., Dean, A., Mitchell, A., Hinde, S., Akowuah, E., Doherty, P., Nichols, S., Fairhurst, C., Flemming, K., Hewitt, C., Ingle, L., & Watson, J. (2023). A randomised controlled, feasibility study to establish the acceptability of early outpatient review and early cardiac rehabilitation compared to standard practice after cardiac surgery and viability of a future large-scale trial (FARSTER). Pilot and Feasibility Studies, 9(1). https://doi.org/10.1186/s40814-023-01304-3
- Niu, H. D., Yuan, S. N., Zhu, Z. F., Ye, J. L., Zhang, X., & Yu, H. (2022). Miniature Non-invasive Blood Pressure Measurement and Verification System. Zhongguo Yi Liao Qi Xie Za Zhi = Chinese Journal of Medical Instrumentation, 46(3). https://doi.org/10.3969/j.issn.1671-7104.2022.03.009
- Notley, S. R., Akerman, A. P., D’Souza, A. W., Meade, R. D., McCourt, E. R., McCormick, J. J., & Kenny, G. P. (2024). Dose-dependent nonthermal modulation of whole body heat exchange during dynamic exercise in humans. American Journal of Physiology – Regulatory Integrative and Comparative Physiology, 326(1). https://doi.org/10.1152/ajpregu.00203.2023
- Nunes, M. J., Moura, J. J. G., Noronha, J. P., Branco, L. C., Samhan-Arias, A., Sousa, J. P., Rouco, C., & Cordas, C. M. (2022). Evaluation of Sweat-Sampling Procedures for Human Stress-Biomarker Detection. Analytica, 3(2). https://doi.org/10.3390/analytica3020013
- Nur Siddiq, M. C., & Mulyono. (2020). The relationship between heat stress and dehydration in the continous casting machine section of pt x. Indian Journal of Forensic Medicine and Toxicology, 14(2). https://doi.org/10.37506/ijfmt.v14i2.3098
- Osborne, T. F., Veigulis, Z. P., Vaidyanathan, A., Arreola, D. M., & Schramm, P. J. (2023). Trends in heat related illness: Nationwide observational cohort at the US department of veteran affairs. Journal of Climate Change and Health, 12. https://doi.org/10.1016/j.joclim.2023.100256
- Osei, F., Block, A., & Wippert, P. M. (2022). Association of primary allostatic load mediators and metabolic syndrome (MetS): A systematic review. In Frontiers in Endocrinology (Vol. 13). https://doi.org/10.3389/fendo.2022.946740
- Oxley, C., Lingam, G., & Metcalfe, M. (2022). TH6.1 Fasting times and medication administration in ‘nil by mouth’ emergency surgery patients. British Journal of Surgery, 109(Supplement_5). https://doi.org/10.1093/bjs/znac248.241
- Pastena, G., Bocchino, M., Paraggio, L., Ferranti, F., Scardala, R., Sorrentino, C., Romano, M., & Ammirati, F. (2023). P158 REMOTE FOLLOW–UP OF ISCHEMIC HEART DISEASE AFTER MYOCARDIAL INFARCTION: PRELIMINARY RESULTS OF A TELEVISIT PROJECT IN THE CARDIOLOGY OF G.B. GRASSI HOSPITAL IN ROME. European Heart Journal Supplements, 25(Supplement_D). https://doi.org/10.1093/eurheartjsupp/suad111.238
- Patel, D. V., Barot, R. B., Cecil, R., Phatak, A. G., Shinde, M. K., Patel, A. J., & Nimbalkar, S. M. (2023). Temperature Monitoring in Children: An Agreement Study. Journal of Neonatology, 37(2). https://doi.org/10.1177/09732179231164527
- Pereira, C. P. B., Gouvêa, N. W. da C., Toniatti, C. B., Pinto, T. A., Kihara, K. de A., Forquesato, A. E. A. de O., Pierozzi, C. V., & Mendes, A. C. de S. (2022). Motivos do jejum superior a 24 horas em um hospital privado de nível terciário/ Reasons for fasting longer than 24 hours in a tertiary-level private hospital. Brazilian Journal of Health Review, 5(2). https://doi.org/10.34119/bjhrv5n2-235
- Prada, J., Vivaldi, F., Bonini, A., Lanata, A., Franchi, E., & Di Francesco, F. (2020). Multiphysics Modeling of a Wearable Sensor for Sweat Rate Measurements. 2020 IEEE International Workshop on Metrology for Industry 4.0 and IoT, MetroInd 4.0 and IoT 2020 – Proceedings. https://doi.org/10.1109/MetroInd4.0IoT48571.2020.9138185
- Puiguriguer-Ferrando, J., & Caballero-Bermejo, A. F. (2023). Réplica a la carta sobre las intoxicaciones en la tercera edad durante la pandemia. Revista Clínica Española, 223(4). https://doi.org/10.1016/j.rce.2023.01.005
- Rabost-Garcia, G., Colmena, V., Aguilar-Torán, J., Vieyra Galí, J., Punter-Villagrasa, J., Casals-Terré, J., Miribel-Catala, P., Muñoz, X., Cadefau, J., Padullés, J., & Brotons Cuixart, D. (2023). Non-Invasive Multiparametric Approach To Determine Sweat-Blood Lactate Bioequivalence. ACS Sensors, 8(4). https://doi.org/10.1021/acssensors.2c02614
- Ravanelli, N., Imbeault, P., & Jay, O. (2020). Steady-state sweating during exercise is determined by the evaporative requirement for heat balance independently of absolute core and skin temperatures. Journal of Physiology, 598(13). https://doi.org/10.1113/JP279447
- Rivasi, G., Menale, S., Turrin, G., Coscarelli, A., Giordano, A., & Ungar, A. (2022). The Effects of Pain and Analgesic Medications on Blood Pressure. In Current Hypertension Reports (Vol. 24, Issue 10). https://doi.org/10.1007/s11906-022-01205-5
- S, : Scheffers Carola, Sarah, : Armstrong, EP, : Cantineau Astrid, Cindy, : Farquhar, & Vanessa, : Jordan. (2015). : Dehydroepiandrosterone for women in the peri- or postmenopausal phase SO-: Cochrane Database of Systematic Reviews YR-: 2015 NO-: 1. Cochrane Database of Systematic Reviews, 1.
- Sasai, F., Roncal-Jimenez, C., Rogers, K., Sato, Y., Brown, J. M., Glaser, J., Garcia, G., Sanchez-Lozada, L. G., Rodriguez-Iturbe, B., Dawson, J. B., Sorensen, C., Hernando, A. A., Gonzalez-Quiroz, M., Lanaspa, M., Newman, L. S., & Johnson, R. J. (2023). Climate change and nephrology. In Nephrology Dialysis Transplantation (Vol. 38, Issue 1). https://doi.org/10.1093/ndt/gfab258
- Sathiyabama, G., Kalabarathi, Dr. S. ., & Nidhisharma, Dr. (2023). Yoga and Exercise for Fetal Heart Rate, Body Mass Index, And Blood Pressure of Antenatal Mothers. International Journal of Life Science and Pharma Research. https://doi.org/10.22376/ijlpr.2023.13.6.l584-l594
- Satoh, T., Yokozeki, H., Murota, H., Tokura, Y., Kabashima, K., Takamori, K., Shiohara, T., Morita, E., Aiba, S., Aoyama, Y., Hashimoto, T., & Katayama, I. (2021). 2020 guidelines for the diagnosis and treatment of cutaneous pruritus. Journal of Dermatology, 48(9). https://doi.org/10.1111/1346-8138.16066
- Savioli, G., Zanza, C., Longhitano, Y., Nardone, A., Varesi, A., Ceresa, I. F., Manetti, A. C., Volonnino, G., Maiese, A., & La Russa, R. (2022). Heat-Related Illness in Emergency and Critical Care: Recommendations for Recognition and Management with Medico-Legal Considerations. In Biomedicines (Vol. 10, Issue 10). https://doi.org/10.3390/biomedicines10102542
- Scheffers, C. S., Armstrong, S., Cantineau, A. E. P., Farquhar, C., & Jordan, V. (2015). Dehydroepiandrosterone for women in the peri- or postmenopausal phase. In Cochrane Database of Systematic Reviews (Vol. 2017, Issue 6). https://doi.org/10.1002/14651858.CD011066.pub2
- Schoessow, F. S., Li, Y., Marlon, J. R., Leiserowitz, A., & Howe, P. D. (2022). Sociodemographic Factors Associated with Heatwave Risk Perception in the United States. Weather, Climate, and Society, 14(4). https://doi.org/10.1175/WCAS-D-21-0104.1
- Sedilla, K. B., & Maeda, T. (2022). Autonomic thermoregulatory responses and subjective thermal perceptions upon the initiation of thermal behavior among resting humans in hot and humid environment. Journal of Physiological Anthropology, 41(1). https://doi.org/10.1186/s40101-022-00308-x
- Shanks, J., Thomson, S., & Ramchandra, R. (2023). Neural control of coronary artery blood flow by non-adrenergic and non-cholinergic mechanisms. Experimental Physiology. https://doi.org/10.1113/EP090917
- Sidana, A., Singh, A., & Singh, G. (2019). Socio-demographic and clinical factors associated with drop out from walk in-clinic in patients with psychoactive substance use. Telangana Journal of Psychiatry, 5(1). https://doi.org/10.18231/j.tjp.2019.017
- Siquier-Coll, J., Bartolomé, I., Pérez-Quintero, M., Toro-Román, V., Grijota, F. J., & Maynar-Mariño, M. (2023). Heart Rate and Body Temperature Evolution in an Interval Program of Passive Heat Acclimation at High Temperatures (100 ± 2 °C) in a Sauna. International Journal of Environmental Research and Public Health, 20(3). https://doi.org/10.3390/ijerph20032082
- Smith, J. W., Bello, M. L., & Price, F. G. (2021). A case-series observation of sweat rate variability in endurance-trained athletes. Nutrients, 13(6). https://doi.org/10.3390/nu13061807
- Snape, D., Wainwright, B., Woods, D. R., & O’hara, J. P. (2023). Reliability of Biomarkers of Physiological Stress at Rest and Post-exertional Heat Stress. International Journal of Sports Medicine, 44(3). https://doi.org/10.1055/a-1890-0993
- Sorensen, C., Howard, C., Prabhakaran, P., Horton, G., & Basu, R. (2022). Heat illnesses in clinical practice. The BMJ. https://doi.org/10.1136/bmj-2022-070762
- Stopa, M., Zieba, K., Tofilska, A., Korpala, B. B., Rajzer, M., & Olszanecka, A. (2022). THE SIZE OF BLOOD PRESSURE MEASUREMENT REDUCTION IN THE UNATTENDED AUTOMATED BLOOD PRESSURE MEASUREMENTS IS CORRELATED WITH THE LEVEL OF ANXIETY. Journal of Hypertension, 40(Suppl 1). https://doi.org/10.1097/01.hjh.0000836104.04656.84
- ŠTURSOVÁ, P., BUDINSKÁ, X., NOVÁKOVÁ, Z., DOBŠÁK, P., & BABULA, P. (2023). Sports Activities and Cardiovascular System Change. Physiological Research, 72. https://doi.org/10.33549/physiolres.935238
- Sun, B., Wang, C. Y., & Chen, R. R. (2023). Clinical Efficacy and Safety of Early Intravenous Administration of Beta-Blockers in Patients Suffering from Acute ST-Segment Elevation Myocardial Infarction Without Heart Failure Undergoing Primary Percutaneous Coronary Intervention: A Study-Level Meta-Analysis of Randomized Clinical Trials. In Cardiovascular Drugs and Therapy. https://doi.org/10.1007/s10557-023-07448-x
- Syah Arsad, F., Hod, R., Ahmad, N., & Baharom, M. (2022). Heatwave Impact on Mortality and Morbidity and Associated Vulnerable Factors: A Systematic Review Protocol. International Journal of Public Health Research, 12(01). https://doi.org/10.17576/ijphr.1201.2022.12
- Takada, A., Kodera, S., Suzuki, K., Nemoto, M., Egawa, R., Takizawa, H., & Hirata, A. (2023). Estimation of the number of heat illness patients in eight metropolitan prefectures of Japan: Correlation with ambient temperature and computed thermophysiological responses. Frontiers in Public Health, 11. https://doi.org/10.3389/fpubh.2023.1061135
- Tan, C. C. S., Chin, L. K. K., & Low, I. C. C. (2020). Thermoregulation in the Aging Population and Practical Strategies to Overcome a Warmer Tomorrow. In Proteomics (Vol. 20, Issues 5–6). https://doi.org/10.1002/pmic.201800468
- Tanner, R. L., & Dowd, W. W. (2019). Inter-individual physiological variation in responses to environmental variation and environmental change: Integrating across traits and time. Comparative Biochemistry and Physiology -Part A : Molecular and Integrative Physiology, 238. https://doi.org/10.1016/j.cbpa.2019.110577
- Tonello, S., Abate, G., Borghetti, M., Lopomo, N. F., Serpelloni, M., & Sardini, E. (2022). How to Assess the Measurement Performance of Mobile/Wearable Point-of-Care Testing Devices? A Systematic Review Addressing Sweat Analysis. In Electronics (Switzerland) (Vol. 11, Issue 5). https://doi.org/10.3390/electronics11050761
- Travers, G., Kippelen, P., Trangmar, S. J., & González-Alonso, J. (2022). Physiological Function during Exercise and Environmental Stress in Humans—An Integrative View of Body Systems and Homeostasis. Cells, 11(3). https://doi.org/10.3390/cells11030383
- Tymoshchuk, О. V., Lembryk, І. S., & Кocherga, Z. R. (2018). Prostaglandins – universal biological regulators in the human body (literature review). Zaporozhye Medical Journal, 0(1). https://doi.org/10.14739/2310-1210.2018.1.122129
- Unnikrishnan, G., Hatwar, R., Hornby, S., Laxminarayan, S., Gulati, T., Belval, L. N., Giersch, G. E. W., Kazman, J. B., Casa, D. J., & Reifman, J. (2021). A 3-D virtual human thermoregulatory model to predict whole-body and organ-specific heat-stress responses. European Journal of Applied Physiology, 121(9). https://doi.org/10.1007/s00421-021-04698-1
- Update: Heat Illness, Active Component, U.S. Armed Forces, 2019. (2020). Medical Surveillance Monthly Report, 27(4).
- Update: Heat Illness, Active Component, U.S. Armed Forces, 2021. (2022). Medical Surveillance Monthly Report, 29(4).
- Wang, L., Yu, C. C., Li, J., Tian, Q., & Du, Y. J. (2021). Mechanism of Action of Acupuncture in Obesity: A Perspective From the Hypothalamus. In Frontiers in Endocrinology (Vol. 12). https://doi.org/10.3389/fendo.2021.632324
- Wang, Y. P., Cheng, R. H., He, Y., & Mu, L. Z. (2022). Thermal Analysis of Blood Flow Alterations in Human Hand and Foot Based on Vascular-Porous Media Model. Frontiers in Bioengineering and Biotechnology, 9. https://doi.org/10.3389/fbioe.2021.786615
- Wazir Ali, H., Aslam, M., Aziz, S., & Hussain, M. M. (2022). Secretion of Atrial Natriuretic Peptide (ANP), Heart Reconditioning and Remolding in Elite Endurance Trained Athletes. Pakistan Journal of Medical and Health Sciences, 16(2). https://doi.org/10.53350/pjmhs22162627
- Webb, R. C., Ma, Y., Krishnan, S., Li, Y., Yoon, S., Guo, X., Feng, X., Shi, Y., Seidel, M., Cho, N. H., Kurniawan, J., Ahad, J., Sheth, N., Kim, J., TaylorVI, J. G., Darlington, T., Chang, K., Huang, W., Ayers, J., … Rogers, J. A. (2015). Materials Science/Clinical Medi Cine: Epidermal devices for noninvasive, precise, and continuous mapping of macrovascular and microvascular blood flow. Science Advances, 1(9). https://doi.org/10.1126/sciadv.1500701
- Westwood, C. S., Fallowfield, J. L., Delves, S. K., Nunns, M., Ogden, H. B., & Layden, J. D. (2021). Individual risk factors associated with exertional heat illness: A systematic review. In Experimental Physiology (Vol. 106, Issue 1). https://doi.org/10.1113/EP088458
- Wissler, E. H. (2008). A quantitative assessment of skin blood flow in humans. European Journal of Applied Physiology, 104(2). https://doi.org/10.1007/s00421-008-0697-7
- Wooditch, A., Johnson, N. J., Solymosi, R., Medina Ariza, J., & Langton, S. (2021). Hypothesis Testing Using the Binomial Distribution. In A Beginner’s Guide to Statistics for Criminology and Criminal Justice Using R. https://doi.org/10.1007/978-3-030-50625-4_8
- Xiang, H., Yang, G., & Tan, H. (2023). Bioequivalence of Levocetirizine Hydrochloride Granules (Kangzhitai) in Healthy Subjects. Alternative Therapies in Health and Medicine, 29(4).
- Yahiro, T., Kataoka, N., & Nakamura, K. (2023). Exploration of thermosensory central neural pathways that drive thermoregulatory behavior. Physiology, 38(S1). https://doi.org/10.1152/physiol.2023.38.s1.5730524
- Yermakova, I. I., Potter, A. W., Raimundo, A. M., Xu, X., Hancock, J. W., & Oliveira, A. V. M. (2022). Use of Thermoregulatory Models to Evaluate Heat Stress in Industrial Environments. International Journal of Environmental Research and Public Health, 19(13). https://doi.org/10.3390/ijerph19137950
- Zhou, P., Jia, Q., Wang, Z., Zhao, R., & Zhou, W. (2022). Cetirizine for the treatment of allergic diseases in children: A systematic review and meta-analysis. In Frontiers in Pediatrics (Vol. 10). https://doi.org/10.3389/fped.2022.940213
- Смолянинова, О. Г., & Иванов, Н. А. (2022). Review of the practice of professional training of mediators: context of humanitarianism. Management of Education, 2(48). https://doi.org/10.25726/e7691-3585-1354-e