
Molecular Characterization and Antibiotic Susceptibility Pattern of Commonly Encountered Bacteria from Wound Infection in Diabetic Patients Attending Specialist Hospital, Bauchi, Bauchi State
- Nasiru Sani Gital
- Ahmed Faruk Umar
- Aliyu Sani Ado
- Zakari Nuhu Lambu
- Yasir Abdulhadi Muhammad
- 264-275
- Jun 12, 2024
- Microbiology
Molecular Characterization and Antibiotic Susceptibility Pattern of Commonly Encountered Bacteria from Wound Infection in Diabetic Patients Attending Specialist Hospital, Bauchi, Bauchi State
Nasiru Sani Gital1*, Ahmed Faruk Umar2, Aliyu Sani Ado3 Zakari Nuhu Lambu3, Yasir Abdulhadi Muhammad4
1Department of Biological Sciences, Federal University Kashere, Gombe State, Nigeria
2Department of Biological Sciences, Abubakar Tafawa Balewa University Bauchi, Bauchi State, Nigeria
3Department of Science Laboratory Technology, Aliko Dangote University of Science and Technology Wudil, Kano State, Nigeria
4Department of Microbiology, Aliko Dangote University of Science and Technology Wudil, Kano State, Nigeria
*Corresponding Author
DOI: https://doi.org/10.51584/IJRIAS.2024.905023
Received: 22 April 2024; Accepted: 01 May 2024; Published: 12 June 2024
ABSTRACT
Diabetic wounds are significantly more susceptible to wound infection by bacteria as well as external contamination than non-diabetic wounds. This study characterized and determined the antibiotic susceptibility pattern of commonly encountered bacteria from wound infection in diabetic patients attending Specialist Hospital, Bauchi, involving 120 diabetic and 120 non-diabetic patients from February to May, 2023. Socio demographic data was collected using structured questionnaire, and sterile swab stick was used in sample collection the subjects and immediately processed for characterization of bacterial isolates according to the standard district microbiological laboratory techniques while Kirby Bauer disk diffusion technique was adopted for susceptibility testing of the isolates. Among diabetic and non-diabetic cases, majority of patients were in the age group 51-60 and the least were in the age group 11-20. The predominant organism isolated was Staphylococcus aureus (41.7%) in both diabetic and non-diabetic wounds. In diabetic wounds, the predominant Gramnegative bacteria were Pseudomonas aeruginosa (20.8%) followed by Klebsiella pneumoniae (17.5%) and Escherichia coli (3.3%) and in non-diabetic wounds, the predominant organism was K. pneumoniae (21.7%) followed by Pseudomonas aeruginosa (17.5%) and E. coli (13.3%). A total of five (5) antibiotics from Gram negative and five (5) from Gram positive disks, which represent the most commonly prescribed antibiotics for treatment of wound infections in the study area, were used in the study. In this study Levofloxacin (71.25%), Chloramphenicol (81.25%) and Gentamicin (69.6%) were effective for S. aureus from all patients, Erythromycin (52.65%) has intermediate effect. From the other hand, Gentamicin (73.7%), Streptomycin (72.4%) and Ampicillin (80.7%) were effective for P. aeruginosa, K. pneumoniae and E. coli. Treatment of wound infections has to be made based on the culture and susceptibility test results for the choice of appropriate antibiotics with maximum efficacy.
INTRODUCTION
Chronic wounds, like arterial or leg ulcers, take a longer time to heal and they are caused by internal factors that can be associated with diseases like diabetes or immune deficiency diseases (Negut et. al., 2018). The major innate barrier to the establishment of infections in internal tissues is the skin, the disruption of which leads to wound formation. Such wounds can be contaminated by bacterial pathogens thereby hampering the healing process and its management becomes resource demanding (Tom et al., 2019). According to 2017 statistics, 425 million people worldwide have diabetes. Compared to 2013 and 1980, in which reported 382 million and 108 million, respectively, it can be seen that this progressive chronic metabolic disease is developing rapidly worldwide (Arman et. al., 2020). In Nigeria, Based on a report by the International Diabetes Federation in 2013, there were 3.9 million cases of diabetes in Nigeria, the highest prevalence rate in Africa (Afolalu et al., 2020) with All regions of the country been affected (Balogun et al., 2018). The diagnosis of infection requires a long time, adequate instrumentation and qualified professionals and it is usually based on wound examination, infection biomarker detection, and microbiological analysis. Antibiotic treatment and wound care represent two critical factors for the management of the infection (Jeschke et al., 2020).
Wounds can be contaminated by bacterial pathogens thereby preventing the healing process and its management becomes too expensive (Tom et al., 2019). Wound infection can be due to variety of microorganisms ranging from bacteria, fungi, parasites and virus. The common responsible bacterial pathogens are Staphylococcus aureus, Pseudomonas aeruginosa, Acinetobacter spp. and bacteria belonging to the family Enterobacteriaceae. Wound infections may be caused by only one pathogen known as mono-microbial or by more than one pathogen known as poly-microbial. The control of wound infection has become more challenging due to widespread bacterial resistance to antibiotics. Hospital acquired wounds are among the leading nosocomial cause of morbidity and increasing medical expense (Balchandra et al., 2018).
In the present situation, an increase in antibiotic-resistant microorganisms has become one of the most vital threats to the healthcare sector. Multidrug-resistant bacteria (MDR) that are deadly pathogenic are rising day by day and pose a very serious threat to human health. Earlier, these types of antibiotic-resistant bacterial strains were rare and limited to only nosocomial-acquired infections, but nowadays, they have become very common. This issue is more prevalent among both Gram-positive and Gram-negative bacterial species, which include A. baumannii, E. coli, P. aeruginosa, and K. pneumonia (Gram-negative), along with S. aureus, S. pneumoniae, E. faecium, and E. faecalis (Gram-positive). It has been found that this antibiotic resistance occurred among these bacterial species due to the attainment of plasmids through the transfer of resistance genes (Jubeh et al., 2020).
The extensive and, in most cases, inappropriate uses of antimicrobials, at both human and veterinary levels, contribute to the selective pressure at the basis of MDRO diffusion. Different factors contribute to the spread of resistant bacteria to humans and animals, including poorly prepared food, proximity, and inadequate hygiene. Resistant bacteria can be spread in the environment and food through contaminated wastewater or through wildlife. The best strategy to contrast the spread of MDRO is the implementation of a One Health approach, which involves the collaboration of multiple sectors to improve public health outcomes as defined by the World Health Organization (McEwen and Collignon, 2018).
Bacterial infections and complications associated with the diabetic mellitus are on the increase due to multiple effects of this disease on the host immune system (Ajayi et al., 2019). It has been documented in literature that diabetic persons are more likely to get infections and more susceptible to certain organisms than non-diabetic patients. The most appropriate mode and duration of therapy for foot infection had not been well defined (Venkata et al., 2020).
Studies have revealed that diabetic wounds showed significantly higher bacterial counts compared with non-diabetic wounds. It is a fact that diabetic patients are not only more susceptible to infection but also when infection occurs they are more severe as the diabetic is a compromised host while certain types of infection do have predilection for the diabetic. (Bisore et al., 2020).
The World Health Organization (WHO) has considered the antimicrobial resistance as top ten threats to global health and is working to increase the knowledge in this field, in order to decrease the rate of microbial infections and to provide a more awareness and appropriate use of antimicrobial drugs (WHO, 2019).
Generally, the medical practitioners advice antibiotics when the classical symptoms of infection are evident. However, inappropriate and excessive use of antibiotics was followed by a rapid emergence of resistant strains of pathogens to various traditionally administered antibiotics. Resistance to conventional antibiotics can be deterrent to usual wound treatment procedures especially threatening the lives of elderly and patients with comorbidities such as diabetes or obesity. Furthermore, compromised vasculature around the wound site can prevent efficient delivery of systemically administered antibiotics. Under such circumstances, topical application of antimicrobials that are effective only in the vicinity of the compromised area is recommended (Öhnstedt et al., 2019).
The control of wound infections has become more challenging due to widespread bacterial resistance to antibiotics and to a greater incidence of infections caused by bacteria, polymicrobial flora, and fungi (Ali, et. al., 2019). It’s currently appreciated that about 20% of the patients with such foot ulcers continue to need associate amputation. Nearly 85% of foot amputations are due to diabetic foot ulcers (Benjamin et al., 2017). To address the current challenges in the field, significant research efforts from both academia and industries are directed towards deeper understanding of wound pathology and treatment optimization to enhance the healing process (Sim et al., 2018).
The detection of microbial species, pathogens distribution and antimicrobial susceptibility patterns are important aspects, often underestimated, in order to limit the spread of antibiotic-resistant isolates. In particular, the detection of the different microbial species colonizing a wound, as well as their susceptibility to the antimicrobials, can provide an indication for a more appropriate therapy to be administered to patients, significantly reducing the health care costs (Moghadam el al., 2020).
MATERIALS AND METHODS
The study was carried out at Specialist Hospital Bauchi between the month of February and May, 2023. A total of 240 samples were collected from diabetic and non-diabetic patients with wound infections.
Ethical Clearance
Ethical approval for this study with number (MOH/GEN/S/1409/II) was obtained from Research and Ethic Committee of Bauchi State Ministry of health, and the signed consent – letter was obtained from all participants, after explaining the purpose of the study and the benefit intended for the patients based on the consent of the Hospitals Ethical committees.
Collection of Sample and Processing
The wound swab samples were obtained before cleaning of the wounds and processed for characterization and identification of bacterial isolates according to the standard microbiological methods including cultural, Gram staining, morphological characteristics (Khan et al., 2018; Muhammad et al., 2020).
Isolation and Identification of Isolates
The wound swab samples were inoculated onto Chocolate agar, MacConkey agar and Nutrient agar. Plates were incubated aerobically at 37oC for 24 hours. After incubation, bacterial growth were observed for colony appearance and morphology. Each colony was re-inoculated into freshly prepared agar plates until a pure colony was obtained. For identification, each pure colony was Gram stained and subjected to further biochemical tests (Muhammad et al., 2020). Results were interpreted according to the guidelines of the Clinical and Laboratory Standards Institute (APHA, 2018).
Molecular Identification of the Isolates
Four bacterial species were further identified at Advanced Biomedical and Public health initiatives limited, Bayero University, Kano using molecular technique by amplification and sequencing of 16S rRNA.
DNA Extraction
Extraction of genomic DNA using commercial kit (Zymos research) according to the manufacturer’s information as follows: Isolated colonies were obtained from the overnight growth bacteria. The colonies were put in a test tube containing 1ml of distilled water and boiled for 10 minutes in a water bath and centrifuged for 5 minutes at 1000 rpm. Five microliters of the supernatant were used for PCR (Agueta et al., 2021).
Amplification of 16S rRNA
Amplification of 16S rRNA genes were performed with the following cycling profile: initial denaturation at 95oC for 30 seconds, annealing temperature at 55oC for 30 seconds, extension at 72oC for 30 seconds, followed by final extension at 72oC for 10 minutes (MoniacaC et al., 2020).
Gel Electrophoresis
The amplified DNA fragments were analyzed and visualized on 1% agarose gel which facilitates the quantification of the DNA according to the ultraviolet (uv)-absorbance at 260 and 280 nm. The PCR product was recovered using the QIA quick gel extraction kit and the amplified product was then purified and used for sequencing (Mukh, 2021).
Genome Sequencing
The DNA eluted from agarose gel was sequenced using the forward (5′ AGA GTT TGA TCC TGG CTC AGT 3′) and reverse (5′ TAC GGY TAC CTT GTT ACG ACT 3′) primers for all the bacteria used in this study. The comparison of the nucleotide sequences of the unique fragment with the sequences available in the Genbank database was carried out using the NCBI blast program (Gillbert, 2020).
Susceptibility Test
Preparation of Bacterial Inoculum
Pure isolates of bacteria were inoculated into Nutrient broth and incubated at 37˚C for 5 hours until turbidity equals to 0.5 Mcfarland standard on the turbidity scale. This turbidity scale was adjusted by adding 9.6 ml of 1% aqueous solution of barium chloride in 0.4 ml of 1% sulphuric acid to give an approximate bacterial density of 1.2 × 109 CFU/ml (Ali and Asmaa, 2017).
Antimicrobial Susceptibility Testing
Pure bacterial isolates were tested against selected antibiotics using Gram-negative and Gram-positive multidiscs. Gram-negative multidisc consist of the following antibiotics: Gentamicin (10μg/ml), Augmentin (30 μg/ml), Streptomycin (30μg/ml), Ampicillin (30μg/ml), and Ciprofloxacin (10μg/ml); whereas the Gram-positive multidisc consist of the following antimicrobial drugs: Levofloxacin (20μg/ml), Chloramphenicol (30μg/ml), Erythromycin (30μg/ml), Gentamicin (10μg/ml), Streptomycin (30μg/ml). Prepared bacterial inoculum (1.2 × 109 CFU/ml) was seeded onto prepared Mueller Hinton agar (MHA) plate under aseptic condition and the surface was allowed to absorb. Gram-negative and Gram-positive multidisc were then carefully placed onto the surface of the seeded plate with the aid of sterile forceps and incubated at 37˚C for 24 hours. After 24 hours, the zones of inhibition were measured in millimetres. Results were interpreted in accordance with CLSI interpretation chart for antimicrobials susceptibility testing. The percentage frequencies of sensitivity and resistance were recorded (Syal, et al., 2017).
Statistical Analysis
The data obtained was analyzed using the statistical package of SPSS (Statistical package for social Science –Version 22) in which tables, charts, percentages, figures and graphs for visualization were presented. The relationships between organisms isolated from wounds and socio-demographic factors were analyzed using Chi Square test (X2 test). Values were considered statistically significant when P value was less than 0.01.
RESULTS
Of the two hundred and fourty (240) wound samples analysed, only 193(80.4%) were found culture positive. In this study, diabetic patients, 42.02% of the total specimens yielded significant bacterial growth than non-diabetic patients 38.3%. Biochemical characteristics and molecular analysis of the bacterial isolates confirmed the presence of S. aureus, P. aeruginosa, K. pneumoniae and E. coli from the sample wound (Figure 1). In this study, among 120 diabetic wound infection cases, 69.2% were men, 30.8% were women while in the case of non- diabetic wound 56.7% were men, 43.3% were women as shown in table 1. In this study, total organisms isolated in 120 diabetic wounds were about 100 giving an average of 0.8 organisms per case and total organisms isolated in 120 non-diabetic wounds were about 92 giving an average of 0.7 organisms per case and among diabetic wound infection cases, the predominant organism isolated was S. aureus (41.7%) followed by P. aeruginosa (20.8%), K. pneumoniae (17.5%) and E. coli (3.3%). Among non-diabetic wound infection cases, the predominant organism isolated was S. aureus (25.0%) followed by K. pneumoniae (21.7%), P. aeruginosa (17.5%) and E. coli (13.3%) (Table 2). In this study among diabetic and non-diabetic cases, majority of patients were in the age group 51-60 and the least were in the age group 11-20 (Table 3).
However the Gram positive bacteria account for 62.5% and 37.5% of the isolated bacteria among diabetic and non-diabetic wound respectively, meanwhile Gram negative account for 44.2% and 55.8% among diabetic and non-diabetic wound samples as shown in table 4.4 and 4.5 respectively.
In this study Levofloxacin (71.25%), Chloramphenicol (81.25%) and Gentamicin (69.6%) were effective for S. aureus from Diabetic and non-diabetic patients, Erythromycin (52.65%) has intermediate effect. From the other hand, Gentamicin (73.7%), Streptomycin (72.4%) and Ampicillin (80.7%) were effective for against P. aeruginosa, K. pneumoniae and E. coli. as shown in table 6 and 7 respectively.
PCR amplicons were produced successfully in all DNA samples of the wounds. Similarly, 16S rRNA genes were amplified in all the bacteria and the closest homologs were identified. Agarose Gel Lane of 16S rRNA of the Isolates Lane 1=ladder, Lanes 2,3,4, and 5 of the Amplified PCR product of D1, D2, D3 and D4, Lane 6 is positive control. mecA was amplified in D3 but mecC was not amplified. SHV was only detected in D1 and D4, TEM was present in D2 and D4 but absent in D1.
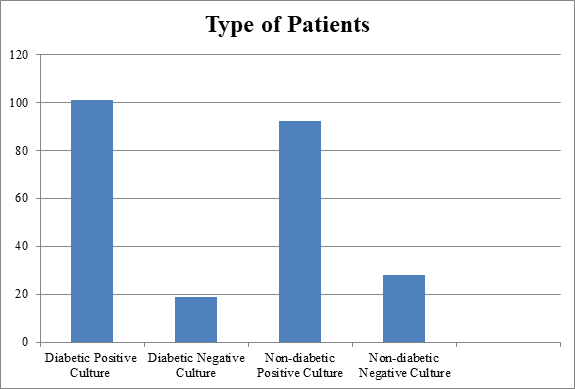
Fig 1: Bacterial Culture in Diabetic and Non-Diabetic patients in the study population
Table 1: Bacterial Infection Distribution according to patients’ Gender in the study population
| Type of Patients | Male No. of cases (%) | Female No. of cases (%) | Ratio | X2 | P Value |
| Diabetic | 83 (69.2) | 37 (30.8) | 2.25 | 4.018 | 0.134 |
| Non-Diabetic | 68 (56.7) | 52 (43.3) | 1.3 |
*Figures in parenthesis indicate percentages
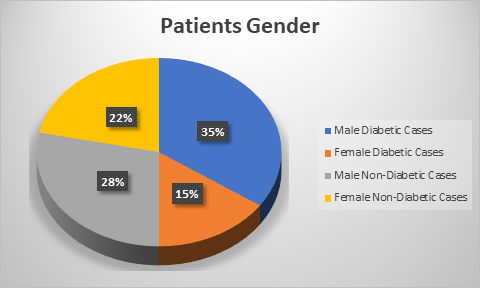
Figure 2: Bacterial Infection Distribution according to patients’ Gender in the study population
Table 2: Proportion of Bacterial isolates in specific Age Groups from Diabetic and Non-Diabetic patients in the study population
| Age in years | Diabetic (%) | Non-Diabetic (%) | Total |
| 11-20 | 01 | 09 | 10 |
| 21-30 | 16 | 15 | 31 |
| 31-40 | 19 | 14 | 33 |
| 41-50 | 18 | 16 | 34 |
| 41-50 | 31 | 28 | 59 |
| 61-70 | 16 | 10 | 26 |
| 101 | 92 | 193 | |
| (52.3) | (47.7) |
*Figures in parenthesis indicate percentages
Table 3: Microorganisms isolated in Diabetic and Non-Diabetic patients attending Specialist Hospital Bauchi
| Organism | Gram reaction | Diabetic (%) | Non-Diabetic (%) | Total |
| S. aureus | Gram positive | 50 (41.7) | 30 (25.0) | 80 (41.5) |
| P. aeruginosa | Gram negative | 25 (20.8) | 21 (17.5) | 46 (23.8) |
| E. coli | Gram negative | 4 (3.3) | 16 (13.3) | 20 (10.4) |
| K. pneumonia | Gram negative | 21 (17.5) | 26 (21.7) | 47 (24.4) |
| Total | 100 (51.8) | 93 (48.2) | 193 (100) |
*Figures in parenthesis indicate percentage
Table 4: Data based on Gram negative isolates in Diabetic and Non-Diabetic patients attending Specialist Hospital Bauchi
| Gram negative Organisms | Diabetic (%) | Non-Diabetic (%) | Total |
| P. aeruginosa | 25 (54.3) | 21 (45.7) | 46 |
| E. coli | 4 (20) | 16 (80) | 20 |
| K. pneumoniae | 21 (44.7) | 26 (55.3) | 47 |
| Total | 50 (44.2) | 63 (55.8) | 113 |
*Figures in parenthesis indicate percentage
Table 5: Data based on Gram positive isolates in Diabetic and Non-Diabetic patients attending Specialist Bauchi
| Gram positive Organism | Diabetic (%) | Non-Diabetic (%) | Total |
| S. aureus | 50 (62.5) | 30 (37.5) | 80 |
*Figures in parenthesis indicate percentage
Table 6: Percentage Susceptibility Profile of Gram positive Bacteria isolated from Diabetic and Non-Diabetic wound infection in patients attending Specialist Hospital Bauchi
| Antibiotic | Susceptibility profile | |||
| S. aureus (Diabetic%) | S. aureus (Non-Diabetic%) | |||
| S | R | S | R | |
| Levofloxacin | 76.2 | 23.8 | 66.3 | 34.7 |
| Chloramphenicol | 83.7 | 16.3 | 78.8 | 20.2 |
| Erythromycin | 50.0 | 50.0 | 55.3 | 44.7 |
| Gentamicin | 73.4 | 26.6 | 65.8 | 34.2 |
| Streptomycin | 33.6 | 66.4 | 40.1 | 59.9 |
CLSI, 2020
Key: S: Sensitivity, R: Resistance
Table 7: Percentage Susceptibility Profile of Gram negative Bacteria isolated from Diabetic and Non-Diabetic wound infection in patients attending Specialist Hospital Bauchi
| Antibiotic | P. aeruginosa | E.coli | K. pneumoniae | |||||||||
| Non-Diabetic (%) | Diabetic (%) | Non-Diabetic (%) | Diabetic (%) | Non-Diabetic (%) | Diabetic (%) | |||||||
| S | R | S | R | S | R | S | R | S | R | S | R | |
| Gentamicin | 95.0 | 5.0 | 65.7 | 34.3 | 62.0 | 38.0 | 60.6 | 39.4 | 87.8 | 12.2 | 71.1 | 29.9 |
| Augmentin | 39.1 | 60.9 | 19.5 | 80.5 | 20.5 | 79.5 | 41.2 | 59.8 | 33.6 | 66.4 | 11.9 | 88.1 |
| Streptomycin | 76.0 | 24.0 | 68.6 | 31.4 | 73.8 | 26.2 | 70.0 | 30.0 | 80.2 | 19.8 | 65.8 | 34.2 |
| Ampicillin | 85.4 | 14.6 | 89.9 | 10.1 | 69.8 | 30.2 | 65.4 | 35.6 | 100 | 00 | 73.7 | 36.3 |
| Ciprofloxacin | 22.8 | 77.2 | 29.4 | 70.6 | 35.1 | 64.9 | 68.5 | 32.5 | 33.3 | 66.7 | 34.9 | 65.1 |
CLSI, 2020; Key: S: Sensitivity, R: Resistance.
Table 8: 16S rRNA sequencing results of the isolates to identify the closest homologs
| Sample ID | Identity of the Closet Homologs of the sequence | Identify % | Accession No. of the closet homolog |
| D1 | Escherichia coli | 90.57 | NR-024570.1 |
| D2 | K. pneumoniae | 90.77 | NR_117683.1 |
| D3 | S. aureus | 100 | NR_113956.1 |
| D4 | P. aeruginosa | 83.6 | NR_041042.1 |
Key: D1 = Escherichia coli, D2 = K. pneumoniae,
D3 = Staphylococcus aureus D4 = Pseudomonas aeruginosa
Table 9: Specific oligonucleotide primers and conditions in multiplex PCR
| Sample ID | Genes | Primers Sequence | Amplicon (bp) | Reference |
| D1 | SHV | F:5′-CTTTATCGGCCCTCCACTCAA-3′ | 237 | El-masy et al., 2019 |
| R:5′-AGGTGCTCATCATGGGAAAG-3′ | ||||
| D2 | SHV | F:5′-CTTTATCGGCCCTCCACTCAA-3′ | 1080 | Teklu et al., 2019 |
| TEM | R:5′-AGGTGCTCATCATGGGAAAG-3′ | |||
| D3 | mecA | F:5′-CTTTATCGGCCCTCCACTCAA-3′ | 108 | Ibtihaji et al., 2021 |
| R:5′-AGGTGCTCATCATGGGAAAG-3′ | ||||
| D4 | SHV | F:5′-CTTTATCGGCCCTCCACTCAA-3′ | 1080 | Teklu et al., 2019 |
| TEM | R:5′-AGGTGCTCATCATGGGAAAG-3′ |
PCR conditions: denature at 94oC for 30s, annealing at 47oC for 60s and extension at 72oC for 90s for 25 cycles.
Key: D1 = Escherichia coli, D2 = K. pneumoniae,
D3 = Staphylococcus aureus D4 = Pseudomonas aeruginosa
DISCUSSION
The prevalence of bacterial infections among diabetic and non-diabetic patients, the most predominant bacterial types and the most common isolates and sensitivity pattern were carried out in this study. The results were in agreement with the work done by Vidhaya and Nithyalakshi (2014), in his study showed that diabetic wounds were significantly more susceptible to wound infections by endogenous bacterial challenge as well as external contamination than non-diabetic wounds as presented in figure 1.
In this study, among 120 diabetic wound infection cases, 69.2% were men, 30.8% were women and male to female ratio was 2.25%. In 120 non- diabetic wound infection cases, 56.7% were men, 43.3% were women and male to female ratio was 1.3% which is similar to the work done by (Tom et al., 2019). Male influence in the present study was due to more exposure to injuries during their occupational and recreational activities and to a possible wound and/or trauma is greater as they represent the majority of the workforce responsible for hard/risky labour. It was further indicated that the diabetic and non diabetic cases, majority of patients were in the age group 51-60 (Table 2). Venkata et al. (2020) had also made similar observation that majority of diabetic and non-diabetic wound infection patients (64%) were in the age group 51 to 60 years and the least were in the age group 11-20. This may be because people within this age group have more participants and at the time people within this range are at higher risk because they are involved in so many risk factors activities such as accidents during transportation and sporting practices and farming which may expose them more to injuries and infections.
Moreover, a total organisms isolated in 120 diabetic wounds were about 100 giving an average of 0.8 organisms per case and total organisms isolated in 120 non-diabetic wounds were about 92 giving an average of 0.7 organisms per case and among diabetic wound infection cases, the predominant organism isolated was S. aureus (41.7%) followed by P. aeruginosa (20.8%), K. pneumonia (17.5%) and E. coli (3.3%). Among non-diabetic wound infection cases, the predominant organism isolated was S. aureus (25.0%) followed by K. pneumonia (21.7%), P. aeruginosa (17.5%) and E. coli (13.3%). Similar results were obtained by Venkata et al. (2020) as their study reported highest positivity of S. aureus (60%) followed by P. aeruginosa (16%), E. coli (12%) and K. pneumoniae (8%). The possible reason for the high frequency of S. aureus and P. aeruginosa might be these bacteria commonly found in the hospital environment.
Meanwhile the study shows that the bacterial isolates in diabetic wounds, Gram positive organisms accounted for 62.5% and Gram negative organisms accounted for 44.2%. Mardaneh et al., 2015 had a similar observation in their study from diabetic foot infections that 122 aerobic microorganisms were isolated from the patients. Among them, 78 (63.9%) were Gram positive, 7 (5.7%) were fungi, and others (30.3%) were Gram negative. Among bacterial isolates in non-diabetic wounds, Gram positive organisms accounted for 37.5% and Gram negative organisms accounted for 55.8%. Shemekaw et al., (2020) had a similar observation in their study that 162 microorganisms from wound infections were isolated, 59.3% (96/162) were Gram negative bacteria while the rest, 40.7% (66/162), were Gram positive bacteria.
Furthermore, the study reveals the pattern of the antibiotics susceptibility of bacteria isolated from Diabetic and non-diabetic wound infections in patients attending Specialist Hospital Bauchi. A total of five (5) antibiotics from Gram negative and five (5) from Gram positive disks, which represent the most commonly prescribed antibiotics for treatment of wound infections in the study area, were used in the study. Levofloxacin, Chloramphenicol and Gentamicin were effective for S. aureus from Diabetic and non-diabetic patients, Erythromycin has intermediate effect from diabetic and non-diabetic patients. Gentamicin, Ampicillin and Streptomycin were effective for P. aeruginosa, E. coli and K. pneumonia from diabetic and non-diabetic patients.
CONCLUSION
It was concluded that, the diabetic wound specimens yielded significant bacterial growth than non-diabetic wound specimens which shows that diabetic wounds were significantly more susceptible to wound infection by bacterial challenge as well as external contamination than non-diabetic wounds.
The most common isolate in diabetic wound infection was Staphylococcus aureus while E. coli has the least occurrence and the most common isolate in non-diabetic wound infection was Staphylococcus aureus, with the high occurrence while E. coli has the least occurrence. Furthermore, the study shown that Staphylococcus aureus was the most prevalent most and susceptible to Levofloxacin, Chloramphenicol and Gentamicin while Erythromycin has intermediate effect. From the other hand, Gentamicin, Streptomycin and Ampicillin were effective against P. aeruginosa, K. pneumoniae and E. coli. Antibiogram becomes very important in clinical cases to block possible recurrence of infection. However, there is need for routine antibiotic sensitivity check.
The variety of microorganisms observed in this study support the need to obtain culture specimen from infected wounds for microbiological evaluation and antibiotic susceptibility determination, so that adapted chemotherapy can be prescribed. The presence and multiplication of the mentioned bacteria in the wound may delay the healing process of the wound. Therefore, routine bacterial culture and its susceptibility to various antibiotics should be carried out whenever there is a wound to choice the appropriate antibiotic for treatment.
ACKNOWLEDGEMENTS
I wish to acknowledge the staff of Specialist Hospital Bauchi for their cooperation and samples provision. Sincere thanks to Bauchi State Government through Ministry of health for granting me with ethical clearance for the conduct of the research.
Conflict of Interest
No conflict of interest.
REFERENCES
- Afolalu, T. D., Wada, O. Z., Olawade, D. B. and Suntai, A. D. (2020). Prevalence of diabetes mellitus among adult residents of Tinda rural community, Nigeria. Journal of Biosciences and Medicines, 8(11), 107-116.
- Agueta, A., Bengt, K., Andersson, F. A. and Sonia, B. (2021). DNA extraction Protocol for DNA metaborcoding of marine phytoplankton, using Zymobiomics DNA minprep kit (Zymo research; D4300) V1.
- Ajayi, E. I. O., Modo, E. U., Kiakubu, O. T. and Molehin, O. R. (2019). Diabetes Care and Wound Healing Using Nauclea latifolia, Manihot esculenta, and Other Natural Products. In Bioactive Food as Dietary Interventions for Diabetes (pp. 545-558). Academic Press.
- Ali, S.A. and Asmaa, A. H. (2017). Isolation and Identification of Escherichia coli Producing Cytosine Deaminase from Iraqi patients. International Journal of Advanced Research in Biological Sciences, 4 (11): 1-6.
- Ali, M., Abdullahi, S.I. and Jido, B.A. (2019). Characterization and Determination of Antibiotic Susceptibility Pattern of Bacteria Associated with Untreated Infected Wound. Clin Res Dermatol 2(2):1-6.
- Al-joda, B. M. and Aziz, H. J. (2021). Biochemical Testing Revision for Identification Several kinds of Bacteria . Journal of University of Babylon for Pure and Applied Science. Vol. 29; No. 2; page: 168-176.
- American Public Health Association – APHA (2018). Compendium of Methods for
- Microbiological Examination of Clinical Samples. 5th Edition.
- Arman, A., Pavivash, D., Saeed, S., Bita, A., Habib, D., Hosein, H. and Reza, S. (2020). Frequency and Antimicrobial Susceptibility Patterns of Diabetic Foot infection. Hindawi Journal of pathogens. p. 10.
- Balchandra, M.H., Naik, S.D. and Verma, P.K. (2018). Aerobic Bacterial profile of wound infections and its sensitivity pattern at Tertiary care hospital. International Journal of Current Microbiology and Applied Sciences; 7(6):1668-79.
- Balogun, W. O., Uloko, A. E., Ipadeola, A., Enang, O., Adamu, A. N., Mubi, B. M., Okafor, C.I, Odeniyi, I., Lawal, I.U, Adeleye, J.O. and Fasanmade, O. A. (2018). Prevalence of obesity and ethno-geographic variation in body sizes of Nigerians with type 2 diabetes mellitus-A multi-centre study. Nigerian Journal of Medicine, 27(1), 69-77.
- Benjamin, A., Michael, H.L. and Joseph, S.W.S. (2017). A Proposed New Classification of Skin and Soft Tissue Infections Modeled on the Subset of Diabetic Foot Infection. Open Forum Infectious Diseases 4(1):255.
- Bisore, O., Kailasia, Y., Sharma, P., Evne, S., Garg, M. (2020). Comparative Study of Bacteriological Profile of Cellulitis in Diabetic and Non Diabetic patients. Int. J. Sci Stud. 8(2):27-31.
- Clinical and Laboratory Standards Institute (2020). Performance Standards for Antimicrobial Susceptibility Testing. 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087 USA.
- El-masy, E. A., Melake, N. A. and Taher, I. A. (2019). Phenotypic and Molecular Characterization of Extended-spectrum ß-lactamase producing Klebsiella spp. From nosocomial infections in Egypt Int Med J; 26:376-80.
- Gillbert, G. L. and Kerridge, I. (2020). Hospital infection, prevention and control (IPC) and Antimicrobial stewardship (AMS): Dual strategies to Reduce Antibiotic Resistance (ABR) in Hospitals; 89-108.
- Ibtihaji, K., Dadah, A. and Abdulfatai, K. (2021). Prevalence of extended spectrum beta-lactamase producing Klebsiella pneumoniae and Pseudomonas aeruginosa among women with urinary tract infections attending antenatal care in Kaduna, Nigeria, Sci World J.; 16: 312-8.
- Jeschke, M.G., Phelan, H. A., Wolf, S., Romanowski, K., Rehou, S., Saetamal, A., Weber, J., Schulz, J., New, C. and Wiktor, A. (2020). State of the Science Burn Research: Burns in the Elderly. J. Burn Care Res; 41, 65–83.
- Jubeh, B., Breijyeh, Z. and Karaman, R. (2020). “Resistance of Gram positive bacteria to current antibacterial agents and overcoming approaches,” Molecules, vol. 25, no. 12, p. 2888.
- Khan, A., Isfahan, T., Bibi, A., Muhammad, A. K., Sadia, A., Nighat, S. and Kashif, S. H. (2018). Age-related variation in the in vitro bactericidal activity of human sera against Pseudomonas aeruginosa. Central European Journal of Immunology; 43(1).
- Mardaneh, J., Anvarinejab, M., Pouladfar, G., Japoni, A., Bolandparvaz, S., Satiary, Z. and Abbasi, P. (2015). Isolation and Antibiotic Susceptibility of the Microorganisms isolated from Diabetic foot infections in Nemazee Hospital, Southern Iran. Journal of Pathogens.
- McEwen, S.A., Collignon, P.J. (2018). Antimicrobial Resistance: A One Health Perspective. Microbiol. Spectr.
- Moghadam, M., Khoshbayan, A., Chegini, Z., Farahani, I., Shariati, A. (2020). Bacteriophages, a New Therapeutic Solution for Inhibiting Multidrug-Resistant Bacteria CausingWound Infection: Lesson from Animal Models and Clinical Trials.
- MonicaC, W., Alexis, G., Peggy, Y., Nathan, J. B. (2020). Influence of PCR cycle number on 16S rRNA gene amplicon sequencing of low biomass samples. Journal of Microbiological Methods.
- Muhammad, S., Iqra, M., and Muhammad, H. (2020). “A Mini-Review on Commonly used Biochemical Tests for Identification of Bacteria,” International Journal of Research Publications, 54(1), pp. 2708-3578.
- Mukh, S. (2021). Gel Electrophoresis: The Applications and its improvement with Nuclear Technology. Transforming Research and Education of Science and Mathematics in the Digital Age.
- Negut, I., Grumezescu, V., Grumezescu, A. M. (2018). Treatment Strategies for Infected Wounds. Molecules; 9, 2392.
- Öhnstedt, E., Tomenius, H., Vågesjö, E. and Phillipson, M. (2019). The discovery and development of topical medicines for wound healing. Expert Opinion on Drug Discovery;14 (5), 485-497.
- Shimekaw, M., Tagabu, M. and Tessema, B. (2020). Bacterial profile,Antimicrobial Susceptibility pattern and Associated Risk Factors Among Patients with Wound infections at Debre Markos Referral Hospital, Northwest, Ethiopia. International Journal of Lower Extremity Wounds.
- Sim, W., Barnard, R. T., Blaskovich, M. A. and Ziora, Z. M. (2018). Antimicrobial Silver in Medicinal and Consumer Applications: A Patent Review of the Past Decade (2007–2017). Antibiotics; 7 (4), 93.
- Teklu, D. S., Negeri, A. A., Legese, M. H., Bedada, T. L., Woldemariam, H. k., Tullu, k. D. (2019). Extended-spectrum beta-lactamase production and multi-drug resistance among Enterobacteriaceae isolated in Addis Ababa, Ethiopia, Antimicrob Resist Infect Control; 8:39.
- Tom, I. M., Ibrahim, M. M., Umoru, A. M., Umar, J. B., Bukar, M. A., Haruna, A. B. and Aliyu, A. (2019). Infection of Wounds by potential Bacterial pathogens and their Resistogram. Open Access Library Journal, 6: e5528.
- Venkata R. M., Varun D. K. and Inamdar, P. (2020). A Comparative Study of foot infections in diabetic and non diabetic patients with Reference to Etiopathogenesis, Clinical features and Outcome. International Surgery Journal; 7 (5): 1496-1502.
- Vidhaya, R., and Nithyalakshi, J. (2014). A Comparative Study of Diabetic and non Diabetic Wound infections with Special Reference to MSRA and ESBL. International Journal of Current Microbiology and Applied Sciences; 3(12): 546-554.
- World Heath Organitazion (2019). Ten Threats to Global Health.