
Multiple Compound Odontomas in A 13 -Year-Old- Child: A Case Report
- Jazi Imen
- Awled brahim Faten
- Kachti Soumaya
- Zaroui Jihene
- Khouja Samia
- Chemli Mohamed Ali
- 62-67
- Jan 1, 2024
- Health
Multiple Compound Odontomas in A 13 -Year-Old- Child: A Case Report
*Jazi Imen1,2,3, *Awled brahim Faten1,2,3, Kachti Soumaya1,2,3 Zaroui Jihene1,2,3, Khouja Samia1,2,3, Chemli Mohamed Ali 1,2,3
1Pediatric dentistry department, Rabta hospital, Tunis, Tunisia
2Laboratory of research abcdf,
3Faculty of dental medicine of monastir, Tunisia
DOI: https://doi.org/10.51584/IJRIAS.2023.81207
Received: 20 November 2023; Revised: 28 November 2023; Accepted: 02 December 2023; Published: 31 December 2023
ABSTRACT
Many developmental anomalies of the jaw are accidentally diagnosed during radiographic investigations for other symptoms. Odontomas are benign odontogenic tumors formed from epithelial and mesenchymal cells. They are mostly associated with disorders of tooth eruption, causing impaction and/or delayed tooth eruption.
This article describes a case of a 13-year-old boy consulted for the delayed eruption of tooth #21, and discusses the fortuitous discovery of multiple odontomas on a radiographic examination.
The treatment consisted on the surgical extraction of the multiple compound odontoma with preservation of the impacted tooth, monitoring clinically and radiologically its eruption followed by ultimate orthodontic positioning. Routine follow-up was carried out for more than 3 years.
Early diagnosis of odontomas allowed adoption of less expensive treatment and ensured a better prognosis.
Keywords: Delayed eruption, multiple Odontomas, pediatric dentistry, surgical extraction, fortuitous discovery
INTRODUCTION
The term ‘odontoma’ was first introduced by Paul Broca in 1867 and was originally used for any tumor and tumor-like lesion of odontogenic origin (1). Over years, as a consequence of new insights, the term odontoma has changed its meaning, and since 2017 it has been classified according to the World Health Organization (WHO) in a group of benign mixed epithelial and mesenchymal odontogenic tumors (2).
They are considered the most common type of odontogenic tumors, accounting for up to 70% of all clinical cases (3). These tumors are usually asymptomatic and are frequently discovered during routine radiographic examinations.
They are commonly found in the maxillary incisor and molar regions. The discovery of the odontoma is typically associated with a delay in the eruption of the permanent tooth, which becomes impacted, and they are typically diagnosed in children and young adults (4). Odontomas commonly occur in the permanent dentition and are rarely reported in association with primary teeth (5, 6, 7).
In this paper, we present a rare case of odontomas in a child with a long period of follow-up, highlighting the clinical and radiographic features and discussing the management strategies.
Consequently, providing insight into the diagnosis and management of odontomas in children as well as increasing awareness of this condition among pediatric dentists.
CASE PRESENTATION
A 13-year-old boy consulted the department of Pediatric and Preventive Dentistry. The chief complaint was the delay of the eruption of the #21, #22, and #12 teeth, while having temporary teeth on the #61, #52, and #62 (Figure1).
Patient’s medical history excluded trauma or infection, with no family history of odontoma.
Extraoral examination showed no facial asymmetry. Intraoral clinical examination revealed a stage of mixed dentition with delayed eruption of the left central maxillar permanent incisor #21, the second right mandibular permanent premolar #45 and the second left mandibular permanent premolar #35. (Figure 2)
On the Panoramic radiograph, a tumor was observed above the crown of the left central maxillar permanent incisor #11, second right mandibular permanent premolar 45 and the second left mandibular permanent premolar #35 of similar intensity of calcified dental tissues, surrounded by a radiolucent zone that separated it from the surrounding bone. (figure4)
Additionally, there were two odontomas presented behind teeth #18 and #28, which were not causing any discomfort. Hence, we choosed the abstention option (figure7)
Cone Beam was deemed necessary to determine the extent of the odontomas and their impact on the surrounding teeth. (Figure 5)
Treatment options were discussed with the patient and his family, taking into account the age of the patient and the potential impact on oral health.
Based on radiographic and clinical features, a provisional diagnosis of multiple compound odontomas was determined. In agreement with the parodontist, surgical procedure was planned to remove odontomas under local anesthesia (figure9), after which spontaneous eruption of the impacted tooth followed. Then we controlled the spontaneous eruption of impacted tooth.
A maxillary removable partial prosthesis replacing #21 was placed to maintain space until its eruption after removal of the obstacle (figure 10)
After 3 years of monitoring and programming for the extraction of the remaining odontomas, a control panoramic X-ray revealed that the impacted tooth #11 is still in a high position, not favorable for spontaneous eruption. The patient was referred to the orthodontist for an eventual orthodontic traction of tooth #11 (figure 11).
DISCUSSION
Odontomas are generally asymptomatic and are usually discovered incidentally on radiographs or during routine dental examinations (12). Radiographic examination is the most common method for diagnosis, which may show a tumor (a radiopaque lesion with a distinct and recognizable appearance on radiological images. This radiopacity is due to the dense nature of the dental tissues (enamel, dentin, cementum) within the odontoma, and it stands out as a bright, white area on X-ray images). Cone-beam computed tomography may be used to obtain a more detailed image of the odontoma (13).
The treatment of odontomas typically involves surgical excision, although in cases where the odontoma is asymptomatic and does not require treatment, it should be monitored with regular radiographs to ensure it does not cause any issues. The prognosis for odontomas is excellent, with a low recurrence rate. (13)
This article reviewed the current literature on odontomas in children, with a focus on the clinical presentation, diagnosis, and treatment of the condition.
Accurate diagnosis and appropriate treatment can help to prevent further dental problems and improve the quality of life of affected children. (10) Pediatric dentist should be aware of the potential for odontomas in these patients, particularly those with delayed eruption of anterior teeth.
However, there are still limitations in the current understanding of odontomas in children, including the lack of standardized diagnostic criteria and variability in treatment approaches.
Odontomas, as in this case, are most commonly diagnosed on radiography examination taken to determine the cause of missing or malposition of an individual tooth, more frequently in permanent dentition than in deciduous dentition. For the same reason, it is recommended for them to be removed early in order to allow proper spontaneous eruption of teeth in dental arch. The treatment of odontoma is surgical and may be associated with orthodontic therapy, malocclusion correction or orthodontic traction of an impacted tooth caused by the presence of odontoma . In the case presented, surgical removal of the odontoma was indicated, as well as monitoring of spontaneous eruption of the affected tooth. (14)
Further research is needed to address these issues and to develop effective management strategies for odontomas in children.
It will also explore the potential impact of these tumors on the development of teeth and the overall oral health of young patients.
Presenting this case study, it will provide a real-life example of the challenges faced by pediatric dentists in diagnosing and treating multiple odontomas in children.
CONCLUSION
Odontomas in children are a common dental anomaly that can have significant consequences if left untreated. The management of this tumor may require a multidisciplinary approach involving surgery, pediatric dentistry by interception, and orthodontic treatment in some cases. Early diagnosis and management of odontomas in children are important to prevent potential complications such as tooth eruption disturbances, malocclusion, or facial asymmetry (8).
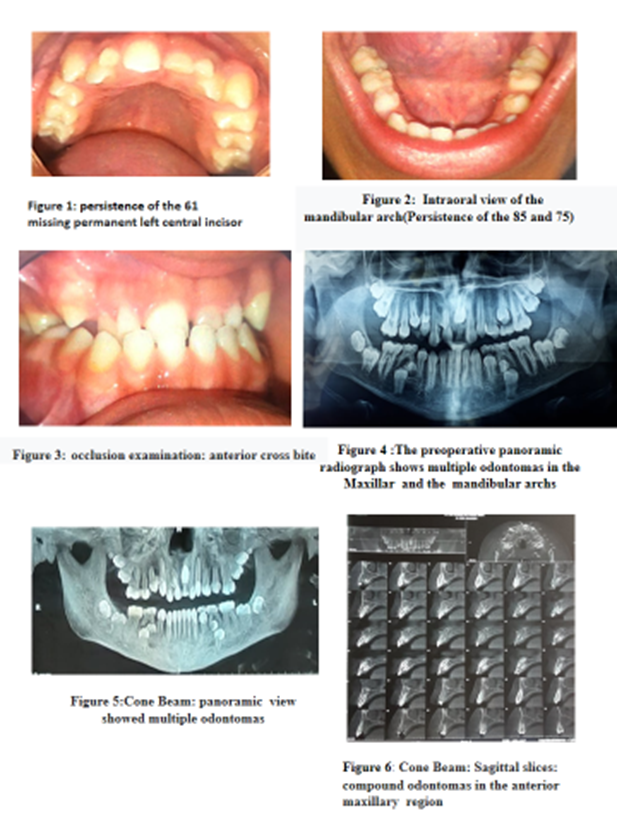

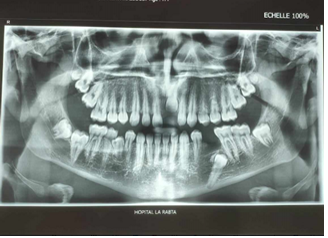
Figure 11 : a panoramic dental radiograph shows the 11 in the high position not favorable for spontaneous eruption
REFERENCES
- Satish V, Prabhadevi MC, Sharma R. Odontome: a brief over-view. Int J Clin Pediatr Dent. 2011;4(3):177-85. doi: 10.5005/jp-journals-10005-1106
- EI-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ.WHO Classification of Head and Neck Tumours: Odonto-genic and Maxillofacial Bone Tumours. IARC: Lyon, 2017; p.224-6.
- Philipsen HP, Reichart PA. Odontogenic tumors and allied lesions. London: Quintessence Publishing; 2004.
- Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology. 4th ed. Philadelphia: Saunders Elsevier; 2016.
- Regezi JA, Kerr DA, Courtney RM. Odontogenic tumors:Analysis of 706 cases. Journal of Oral Surgery 1978; 36:771–778.
- de Oliveira BH, Campos V, Marcal S. Compound odontoma– diagnosis and treatment: three case reports. Pediatric Dentistry 2001; 23 (2): 151–157.
- Stajcic ZZ. Odontoma associated with a primary tooth. Journal of Pedodontics 1988; 12 (4): 415–420.
- Shafer WG, Hine MK, Levy BM. A Textbook of Oral Pathology. 4th ed. Philadelphia: Saunders Elsevier; 1993.
- Barnes L, Eveson JW, Reichart P, Sidransky D. Pathology and genetics of head and neck tumors. World Health Organization Classification of Tumors. 2005.
- Neville BW, Damm DD, Allen CM, Chi AC. Oral and maxillofacial pathology. Elsevier Health Sciences. 2015.
- Scully C, Bagan JV, Hopper C. Oral cancer: current and future diagnostic techniques. American journal of dentistry. 2014;27(6):333-8.
- Kuriakose MA, Sankarankutty S, Cherian T. Odontomes. Oral and maxillofacial pathology. Indian journal of dentistry. 2014;5(2):81.
- Shafer WG, Hine MK, Levy BM. A Textbook of Oral Pathology. 4th ed. Philadelphia, PA: WB Saunders Company; 1993.
- Tomislav Ćabov , Department of Oral Surgery, University of Rijeka, Faculty of Dental Medicine, Rijeka, Croatia;