Performance and Comparison of two Malaria Rapid Diagnostic Tests among Symptomatic Patients in Lagos, Southwest Nigeria
- Okangba, C. C.
- Funwei, R.I.
- Solanke, A.O.
- Okangba, G.C.
- Nwadike, V.U.
- Oluwole, T. O.
- Okunbor H.N.
- Okangba, U.G.
- 122-134
- Jun 5, 2024
- Medical research
Performance and Comparison of two Malaria Rapid Diagnostic Tests among Symptomatic Patients in Lagos, Southwest Nigeria
Okangba, C. C.*1,2, Funwei, R.I.2,5, Solanke, A.O.1, Okangba, G.C.1, Nwadike, V.U.1,4, Oluwole, T. O.1, Okunbor H.N.1,3, Okangba, U.G.1
1Department of Medical Microbiology and Parasitology Benjamin Carson (Snr) College of Health and Medical Science, Babcock University. Illisan –Remo, Ogun State, Nigeria.
2Centre for Advanced Medical Research and Biotechnology, Babcock University Ilishan Remo, Ogun State, Nigeria
3Babcock University Teaching Hospital. Ilisan – Remo, Ogun State, Nigeria
4Department of Medical Microbiology, Federal Medical Centre Abeokuta, Ogun State, Nigeria
5Department of Pharmacology Benjamin Carson (Snr) College of Health and Medical Science, Babcock University. Illisan –Remo, Ogun State, Nigeria.
*Corresponding Author
DOI: https://doi.org/10.51584/IJRIAS.2024.905011
Received: 07 April 2024; Revised: 30 April 2024; Accepted: 04 May 2024; Published: 05 June 2024
ABSTRACT
Malaria remains a public health problem in Sub Saharan Africa. Microscopic identification of Plasmodium spp. is the gold standard for malaria diagnosis. However, malaria rapid diagnostic test kits are also available for prompt diagnosis, effective treatment and are important in reducing morbidity and mortality associated with malaria especially among high-risk groups. The use of malaria rapid diagnostic tests (RDTs) has improved Plasmodium falciparum diagnosis, especially in settings where quality microscopy is not available. Field evaluation of RDTs would assist in confirming the potency, performance of the RDTs and in ruling out or confirming malaria parasite. In this study, the performance of two RDTs were assessed for malaria diagnosis, using thick and thin blood smears as the gold standard. A total of 1,271 patients suspected to have malaria who gave consent were enrolled in the study within six months at St Matthew”s Primary Health Center Amukoko in Ajeromi Ifelodun LGA of Lagos state. The study population age range between 2-67years. This is a cross-sectional study involving patients with history of malaria symptoms. The SD Bioline and First Response HRP2 based MRDTs were evaluated in this study. Of the patients 1,271 screened for malaria, 185 were slide positive for malaria parasites. Blood smears and HRP2 First response RDT showed malaria prevalence rate of 14.6%, while the HRP2 SD Bioline RDT showed prevalence rate of 15.5%. The SD Bioline HRP2 RDTs showed a sensitivity of 61.1%, specificity of 92.3%, PPV of 57.4% and NPV of 93.3%, while the First response RDT showed a sensitivity of 58.9%, specificity of 93.1%, PPV of 59.6% and NPV of 92.9%. In this study, the sensitivity of the RDT increased with parasite density (>1000p/µl showed sensitivity >90%). All the malaria rapid diagnostic test kits performed relatively well and can be used in emergencies. Concerning cost-effectiveness, using the malaria RDTs at the hospital is cheaper than light microscopy for diagnosing malaria. However, for malaria diagnosis, malaria RDT kits cannot be relied upon alone; hence, microscopic confirmation is always required.
INTRODUCTION
In malaria-endemic settings, prompt and efficient diagnosis is required for effective disease management (Oyeyemi et al., 2015). The World Health Organization (WHO) recommends that all febrile patients in malaria-endemic settings are appropriately diagnosed before commencing any treatment. This recommendation enhances anti-malarial drugs’ effective and efficient use and prevents unnecessary treatments that could contribute to drug resistance (Abba et al., 2011). Malaria is a major public health concern in Nigeria, with an estimated 68 million cases and 194,000 deaths due to the disease in 2021 contract malaria yearly, with most deaths among children under 5 years (WHO, 2020). At the same time, Plasmodium falciparum malaria remains one of the most significant diseases in Nigeria and sub-Saharan Africa, recording a high burden on health services (Ansah et al., 2010). Generally, examining malaria blood film for Plasmodium spp. identification using a light microscope remains the gold standard for confirming malaria in suspected patients (Mukry et al., 2017; Berzosa, et al., 2020). However, in remote rural settings where skilled personnel or microscopes are unavailable, Rapid Diagnostic Test (RDT) kits are recommended to screen for malaria before commencing anti-malarial treatment (Ajakaye et al., 2020; Odeniyi et al., 2020; Okangba et al., 2020). Hence, in Nigeria, several malaria RDT kits are in the market (Ilesanmi et al., 2017; Oluwaremilekun, et al., 2020; Okangba et al., 2022) and the main difference between these malaria RDT kits is the detected antigen. RDTs do not require much infrastructure or technical expertise and as such can be done easily in remote rural settings, hence discouraging the presumptive treatment of malaria in the absence of microscopy. Malaria RDTs exist in different formats. The major difference between them is in the antigen type detected by the kit. The histidine-rich protein 2 (HRP-2) is specific for the detection of P. falciparum, aldolase for detection of Plasmodium spp in general and plasmodial lactate dehydrogenase (pLDH) either for P. vivax (Pv-pLDH), P. falciparum (Pf-pLDH) or Plasmodium sp in general (pan-pLDH) (Kennedy and Otokunefor 2017). HRP-2 can detect the presence of the Plasmodium protein whether dead or alive and so tends to be very sensitive, but less specific because of it results in false positive occasionally (FMOH 2015). At present, more than 90% of RDT in use are the most common assays that detect HRP-2 These assays are valuable in Sub Saharan Africa where the main causative agent of malaria is P. falciparum (Mouatcho and Goldring 2013). Some RDT kits show different performances in different geographical settings (Ugah et al., 2017). There is, therefore, a need to continually evaluate the performance of malaria RDT kits used in primary healthcare in different geographical settings. This study evaluated two routinely used malaria RDT kits at St. Matthew’s Primary Health Centre Amukoko, Lagos. Amukoko in Ajeromi Ifelodun Local Government Area (LGA) of Lagos State using blood film for P. falciparum parasites identification as the gold standard.
MATERIALS AND METHODS
Study Design and Study Site
The study is a cross-sectional study and it was conducted from April to October 2017 among persons suspected of malaria during their visit to St. Matthew’s Primary Health Centre Amukoko, Lagos. Amukoko in Ajeromi Ifelodun Local Government Area (LGA) of Lagos State. This hospital serves the indigenes of the Amukoko District in the Southwest Region. Inclusion criteria: Patient with history of malaria symptoms (axillary temperature ≥ 37.5oC), No intake of anti-malaria in the two weeks preceding presentation at clinic, presence of P. falciparum parasite and gave consent. Exclusion criteria: Patient with no history of malaria symptoms, refuse to give consent, recent intake of antimalarials (in the last 2 weeks) and Patient with clinical anaemia
Study Population
All persons suspected of malaria visiting the St. Matthew’s Primary Health Centre Amukoko, Lagos. Amukoko in Ajeromi Ifelodun Local Government Area (LGA) of Lagos State.. The study was conducted at St. Matthew’s Primary Health Centre Amukoko, Lagos. Amukoko in Ajeromi Ifelodun Local Government Area (LGA) of Lagos State. The study area was selected because it is densely populated (estimated population of 684, 105) and is near to the Atlantic Ocean and Lagos Lagoon. The outpatient department of the Primary Healthcare Centre (PHC) handles an average of 150 suspected malaria cases weekly. Children and adults, age between 2- 67years who presented in the health facility with documented fever (≥37.5oC) or symptoms of fever and other related symptoms and who gave consent were recruited into the study.
Sample Size Determination.
The sample size was calculated using a prevalence of malaria reported in Nigeria, 14.7% (Aina et al., 2013), The Assumptions were: Degree of precision is put at 0.05 and the population of people with malaria more than 10,000
n = z2pq/d2
prevalence of malaria in Lagos is 14.7% (Aina et al., 2013);
Minimum sample size of 342
Participants Enrollment
A case report form (CRF) was obtained for each patient presenting with fever after taking verbal consent. The CRF contained information on previous antimalarial used, age, malaria symptoms and age. Three millilitres of venous blood was collected by the laboratory personnel into ethylene diaminetetra acetic acid( EDTA) bottles from the patient for microscopy and rapid diagnostic test. Patients blood were screened with two different Rapid Diagnostic Tests kits. The RDTs were performed and the results were interpreted in the laboratory.
Preparation of blood films for parasite diagnosis /quantification
A. Thin and thick smear preparation
Thin and thick blood films, using a template diameter of 15mm for thick were made on the same frosted end, grease free glass slide, with date, patient’s study 1D number. Also duplicate slides were prepared for each patient, which were stained, dried and boxed. The thin film was fixed in absolute methanol for 1-2 seconds and air dried, while the thick malaria blood film (MBF) were not fixed, this allow the red blood cells (RBCs) to lyse, making the malaria parasites to be left intact and concentrated.
B. Staining Procedure
The MBFs were stained after 48 hours with 3% Giemsa stain solution at pH 7.2. Thereafter the stained slides were rinsed with buffer water of pH 7.0 – 7.2 after 45minutes.
C. Examination of blood films for Parasite Diagnosis
The stained slides were read by first and second microscopist to determine the parasite density; number of malaria parasites (parasite count) and leukocytes were counted per high power field. The absolute parasite density was calculated using the formula below:
No of parasites counted x Total WBC count = No of parasite/µl blood
No of WBC counted
A malaria blood film (MBF) was considered positive when a reddish chromatin dot with a purple or blue cytoplasm of the malaria parasite are seen together. A MBF was declared negative after viewing 500 high power fields, using x100 oil immersion objective lens and no asexual and sexual stages of the parasite were seen.
Performance of the Rapid Diagnostic Test
The test kit contains a membrane strip which is pre-coated with monoclonal antibody with two separate lines, one serves as the control line while the other is for Plasmodium falciparum HRP2. 5ml of blood sample were collected with the kits calibrated dropper and transferred into the sample well of the RDTs This was followed by adding four drops of buffer for SD-bioline and three drop for First response into the buffer well., the test kits have one control line to indicate the validity of the test procedure and its working condition .Control and test lines appeared within 15minutes in a reading window the test was done following the manufacturer’s instructions.
Interpretation of RDT test Results
The principle of reading the colour intensity of the test line is graded as follows: 0= No test line (Negative), 1+ (Positive with very faint test line), 2+ ( Positive equal to test line), 3+ (Strong positive, greater than test line). The presence of two bands indicate a positive result for Plasmodium falciparum, one band for control line and the other is for the test line, while the presence of only one band in the control area indicates a negative result.
ETHICAL CONSIDERATION
Ethical approval for this study was obtained from the Research, Grants and Experimentation Committee of the College of Medicine of the University of Lagos, Nigeria (CM/COM/08/XXIV).. Participants gave informed consent and assent from children with corresponding consent from their Parents/Guardian after explaining the purpose of the research before they were enrolled. Patients that declined to participate were not denied access to the available health care service. The entire study was conducted in line with good clinical laboratory practice.
Data Analysis: The data generated from the study were analyzed using EPIINFO 3:4:3 version statistical software (CDC, Atlanta, USA). Tests for associations and differences were done by chi square analysis, Fisher Exact test and analysis of variance where appropriate. The performance characteristics of the MRDTs was measured using the following performance characteristics: sensitivity, specificity, negative predictive value, positive predictive value, negative likelihood ratio and positive likelihood ratio, recover operator characteristics and area under the curve. Test of statistical significance was set at P value less than 0.05 at 95% confidence interval.
RESULTS
Demographic and Patients Information
A total of 1271 malaria suspected patients participated in the study at St Matthew Primary Health Centre. Their baseline characteristics are summarized in table 1. The study participants had a mean age of 26.3±16.7years and mean temperature of 36.9±0.8oC. The age range of 25-34 had the highest population of 308 (24.3%) followed by 15-24 age range 275(21.70%) and least was <5 age group 156(12.3%) . The study population were more of female 767(60.3%), than male 505(39.7%). Patients with temperature of <37.4oC (afebrile) were more 1025(81.3%) than those with ≥37.5 temperature (febrile patients) 246(18.7%). The major drug taken by participant at home before coming to the health care centre was Agbo 305(23.9%) followed by ACT 208(16.3%) and PCM 165(16.1%). The least drug used at home was Antibiotics 54(5.3%). Most of the study participants 808 (63.5%) had fever, which is the clinical symptom with the highest frequency, this is followed by yellow urine 594(46.6), headache 441(33.6%) and chills 420(33.0%) (table 2a). Diarrheal and itching exhibited the lowest clinical symptoms frequency in the study population (table 2a). In table 2b, among the afebrile patients, those with fever exhibited the highest frequency of 60.6% and 77.1% among the febrile patients while diarrheal was the lowest (1.2%) for afebrile and itching (0%) for febrile patients
Prevalence of malaria and Performance characteristics among study Participants
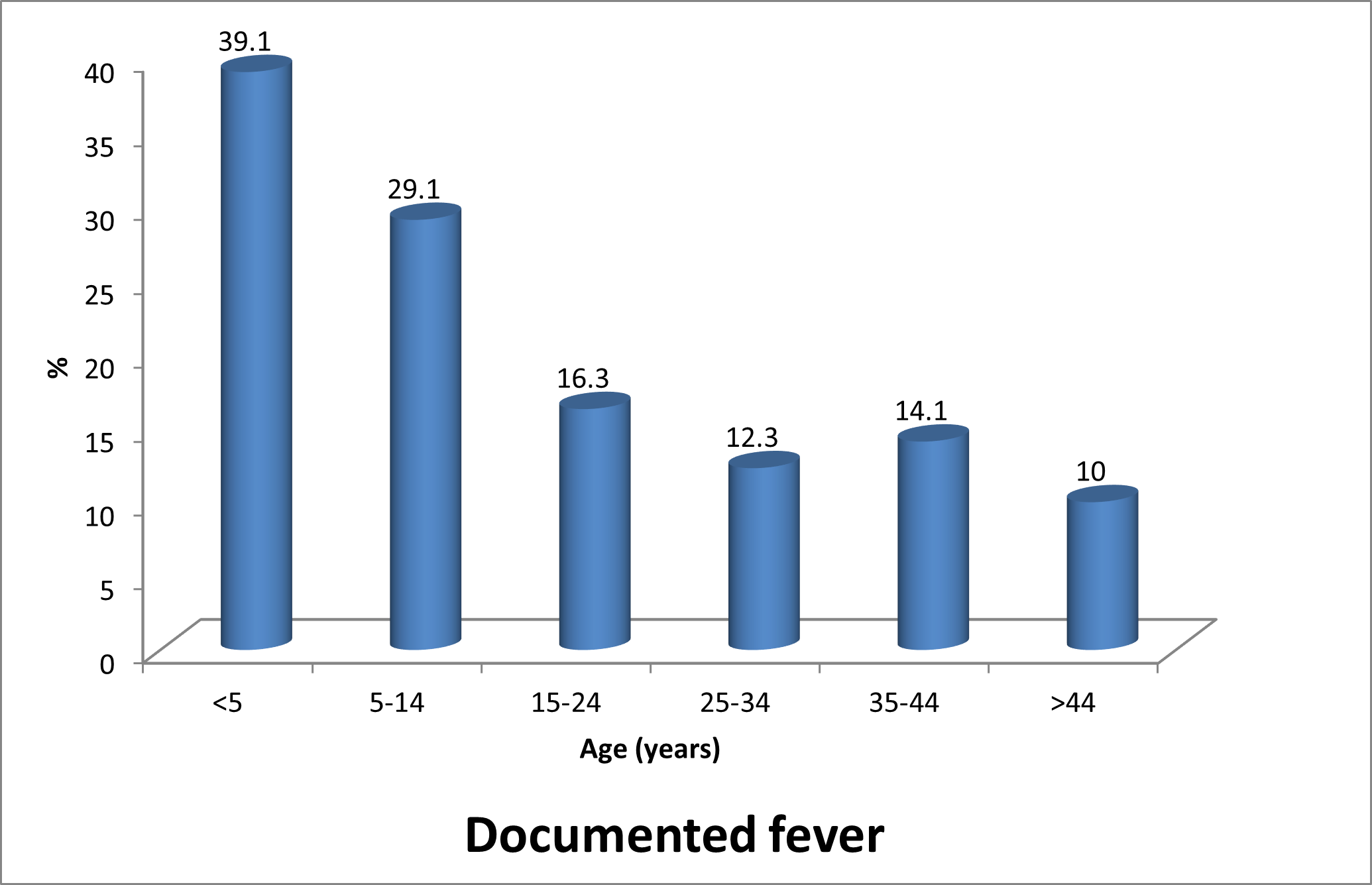
In this study the prevalence of malaria using blood specimen with microscopy method was 14.6%, while SD Bioline HRP2 RDT was 15.5% and First Response RDT was 14.6%. The study showed that participants >5 years had the highest documented fever 61(39.1%), while participants >44 years recorded the lowest among the study population 20(10%) (figure 1). There was a significant difference (c2 = 76.5, df = 5; P= < 0.001) between age groups and documented fever among the study population. The older age group of >44 years had the lowest body temperature (<37.5oC), while for body temperature >=37.5oC had the highest frequency among study population of children < 5 years (figure 1). The comparative performance of the two different RDTs with microscopy method in (table 3) indicated that microscopy method had the prevalence rate of 14.6%, while, SD Bioline and First Response had a prevalence rate of 15.5% and 14.6% respectively. The sensitivity and specificity of the RDTs used for this study varied. SD Bioline RDT showed the highest sensitivity of 61.1% while, FR was 58.9% and their specificities were 92.3% and 93.1% on blood specimen respectively. (Table 4). There was a relationship between age and malaria prevalence among the study group. The age group >5 had malaria prevalence of 13(8.4%), while age group >5-14 years exhibited the highest prevalence of malaria 46 (26.6%), and age group 35-44years had the lowest prevalence of 14(9%) among the study population (table 5). Malaria infection was significantly associated with age (c2 = 41.85, df = 5; P<0.001). There was no significant difference between malaria prevalence and the participants sex (c2 = 1.53, P< 0.216). Although, there was relationship between body temperature group and malaria prevalence (c2 = 22.97; P< 0.001). The participants having >=37.5oC 58(24.6%) exhibited high malaria prevalence than, participants having <37.5oC 126(12.3%). The effect of parasite density on the malaria RDT sensitivity is seen in table 6. The higher the parasitaemia level, the higher the sensitivity of the test.
Body weakness had a significant association with age (c2 = 14.49; P< 0.001). Age group <5 years had the least frequency of body weakness 156(26%), while age >44years showed the highest frequency of 200 (56%). There was relationship between age and fever (c2 = 32.9; P< 0.001). The frequency of fever among the study participants reduced as the age increases. There was also significant association with joint ache (c2 = 84.81; P< 0.001). The least frequency was seen among participants of age <5 years and the highest value was seen in age group >44 years (table 7).
Table 1: Baseline characteristics of the study participants
| Description | n (%) Afebrile Febrile Total
(n=1,023) (n=246) (n=1249) |
| No of Participants | 1271 |
| Sex
Female Male |
767(60.30) 620(81.8) 138(18.2) 758
505(39.70) 402(80.4) 98(19.6) 500 |
| Age (years)
Mean±SD <5 5-14 15-24 25-34 35-44 >44 |
26.3±16.7
156(12.30) 95(60.9) 61(39.1) 156 173(13.60) 122(70.9) 50(29.1) 172 275(21.70) 226(83.7) 44(16.3) 270 308(24.30) 265(87.7) 37(12.3) 302 157(12.40) 134(85.9) 22(14.1) 156 200(15.80) 180(90.0) 20(10.0) 200 |
| Temperature(OC)
Mean±SD |
Chi square =76.5 df = 5; P <0.001
36.9±0.8 36.1±0.6 36.9±1.1 |
| Home treatment drugs
ACTs Agbo Paracetamol SP Chloroquinine Antibiotics |
208(16.3) 128(60.1) 80 (39.9)
305(23.9) 200(67.2) 105(32.8) 165(16.1) 112(74.0) 53(24.0) 24 (1.9) 16(66.7) 8 (33.3) 133(10.5) 97(76.9) 36(23.1) 54 (5.3) 44(80.5) 10(19.5) |
Table 2a: Frequency of Clinical symptoms among Study Participants
| Symptoms | Frequency | Percent | 95% Conf Limits | |
| Fever | 808 | 63.5% | 60.8% | 66.1% |
| Yellow urine | 594 | 46.6% | 43.9% | 49.4% |
| Joint ache | 549 | 43.1% | 40.4% | 45.9% |
| Headache | 441 | 34.6% | 32.0% | 37.3% |
| Chills | 420 | 33.0% | 30.4% | 35.7% |
| Body weakness | 320 | 25.1% | 22.8% | 27.6% |
| Loss of Appetite | 221 | 17.4% | 15.3% | 19.6% |
| Stomach ache | 194 | 15.2% | 13.3% | 17.3% |
| Cough | 191 | 15.0% | 13.1% | 17.2% |
| Vomiting | 146 | 11.5% | 9.8% | 13.4% |
| Dizziness | 107 | 8.4% | 7.0% | 10.1% |
| Isomnia | 49 | 3.8% | 2.9% | 5.1% |
| Nausea | 43 | 3.4% | 2.5% | 4.6% |
| Chest pain | 28 | 2.2% | 1.5% | 3.2% |
| Diarrhea | 16 | 1.3% | 0.7% | 2.1% |
| Itching | 16 | 1.3% | 0.7% | 2.1% |
Table 2b: Frequency of Clinical symptoms among Afebrile and Febrile Study Participants
| Symptoms | Frequency for Afebrile Patients (%) | 95% Conf. Limits (Afebrile) | Frequency for Febrile Patients (%) | 95% Conf. Limits (Febrile) |
| Body weakness | 257(25.1) | 22.5 – 27.9 | 58(24.6) | 19.2 -30.6 |
| Cough | 148(14.5) | 12.4 -16.9 | 48(18.2) | 13.5 – 23.7 |
| Chill | 323(31.6) | 28.8 -34.5 | 91(38.6) | 32.3 – 45.1 |
| Chest pain | 26 (2.5) | 1.7 – 3.7 | 1 (0.4) | 0.0 – 2.3 |
| Diarrhea | 12(1.2) | 0.6 -2.1 | 4(1.7) | 0.5 -4.3 |
| Dizziness | 95(9.3) | 7.6 -11.3 | 10(4.2) | 2.1 -7.7 |
| Fever | 620(60.6) | 57.5 – 63.6 | 182(77.1) | 71.2 – 82.3 |
| Headache | 355(34.7) | 31.8 – 37.7 | 78(33.1) | 27.1 – 39.4 |
| Isomnia | 40(3.9) | 2.8 – 5.3 | 8(3.4) | 1.5 -6.6 |
| Itching | 16 (1.6) | 0.9 – 2.6 | 0(0.0) | 0.0 -1.6 |
| Joint ache | 456(44.5) | 41.5 – 47.6 | 85(36.0) | 29.9 – 42.5 |
| Loss of Appetite | 182 (17.8) | 15.5 -20.3 | 34(14.4) | 10.2 – 19.5 |
| Nausea | 37(3.6) | 2.6 -5.0 | 3 (1.3) | 0.0 – 1.6 |
| Stomach ache | 170 (16.6) | 14.4 – 19.1 | 22(9.3) | 5.9 -13.8 |
| Vomitting | 103(10.1) | 8.3 -12.1 | 43 (18.2) | 13.5 – 23.7 |
| Yellow urine | 472(46.1) | 43.0 – 49.2 | 116(49.2) | 42.6 – 55.7 |
X2 = 76.5; P < 0.001
Figure 1: Comparison of documented fever (Body temperature ≥37.5oC) versus age of study participants
Table 3: Prevalence of malaria using different malaria RDTs and Microscopy Method
| Specimen | Diagnostic method | Total | Positive for malaria | Prevalence |
| Blood | Microscopy | 1271 | 185 | 14.6 |
| Hs_SD | 1269 | 197 | 15.5 | |
| Hs_FR | 1251 | 183 | 14.6 |
Hs_SD=HRP2 single SD Bioline, Hs_FR =HRP2 single First response Hs
Table 4: Performance characteristics of RDTs using Blood specimen
| RDTs | Sensitivity | Performance characteristic | ||||
| Specificity | PPV | NPV | LR(+) | LR(-) | ||
| Hs_SD | 61.1 | 92.3 | 57.4 | 93.3 | 7.9 | 0.4 |
| Hs_FR | 58.9 | 93.1 | 59.6 | 92.9 | 8.5 | 0.4 |
Hs_SD=HRP2 single SD Bioline, Hs_FR =HRP2 single First response RDT kit, PPV=Positive Predictive Value, NPV=Negative Predictive Value, PLR=Positive Likelihood Ratio, NLR= Negative Likelihood Ratio
Table 5: Comparison of malaria prevalence by age, sex and body temperature
| Microscopy | TOTAL | Chi square | P | ||
| NEG | POS | ||||
| Age (n=1265) | |||||
| <5 | 141 (91.6) | 13 (8.4) | 154 | 41.85 | <0.001 |
| 5-14 | 127 (73.4) | 46 (26.6) | 173 | ||
| 15-24 | 218 (79.6) | 56 (20.4) | 274 | ||
| 25-34 | 271 (88.0) | 37(12.0) | 308 | ||
| 35-44 | 142 (91.0) | 14 (9.0) | 156 | ||
| >44 | 181 (90.5) | 19 (9.5) | 200 | ||
| SEX (n=1268) | |||||
| Female | 661 (86.4) | 104 (13.6) | 765 | 1.53 | 0.216 |
| Male | 422 (83.9) | 81 (16.1) | 503 | ||
| Temp (n=1257) | |||||
| <37.5(Afebrile) | 895(87.7) | 126 (12.3) | 1021 | 22.97 | <0.001 |
| >=37.5 (febrile) | 178 (75.4) | 58(24.6) | 236 | ||
Table 6: Effect of parasite density on malaria RDT sensitivity
| Parasite density group | n | Sensitivity of RDTs at different parasite densities | |
| Hs_SD_bld | Hs FR_bld | ||
| 1-200 | 61 | 26.2 | 21.3 |
| 201-500 | 26 | 61.5 | 61.5 |
| 501-1000 | 19 | 73.7 | 73.7 |
| >1000 | 79 | 84.8 | 83.5 |
Hs_SD_bld=HRP2 single sd bioline blood, Hs_FR_bld =HRP2
Table 7: Presenting signs and symptoms in relation to age of the study participants
| agegp | Presenting signs and symptoms | ||||||||||||||||
| TOTAL | BWK | CGH | CHL | CHP | DIA | DZN | FEV | HAC | ISM | ITCH | JAC | LAP | NAU | SAC | VOM | YELURI | |
| <5 | 156 | 26 | 35 | 48 | 2 | 2 | 6 | 121 | 45 | 3 | 1 | 31 | 31 | 3 | 13 | 30 | 62 |
| Row % | 100 | 16.7 | 22.6 | 30.8 | 1.3 | 1.3 | 3.8 | 77.6 | 28.8 | 1.9 | 0.6 | 19.9 | 19.9 | 1.9 | 8.3 | 19.2 | 39.7 |
| 5-14 | 172 | 35 | 22 | 58 | 3 | 1 | 13 | 129 | 56 | 3 | 5 | 55 | 33 | 8 | 18 | 33 | 84 |
| Row % | 100 | 20.3 | 12.9 | 33.7 | 1.7 | 0.6 | 7.5 | 75 | 32.7 | 1.7 | 2.9 | 32 | 19.2 | 4.6 | 10.5 | 19.2 | 48.8 |
| 15-24 | 275 | 69 | 32 | 83 | 8 | 7 | 25 | 170 | 88 | 7 | 2 | 107 | 37 | 5 | 57 | 20 | 125 |
| Row % | 100 | 25.1 | 11.6 | 30.2 | 2.9 | 2.5 | 9.1 | 61.8 | 32 | 2.5 | 0.7 | 38.9 | 13.5 | 1.8 | 20.7 | 7.3 | 45.5 |
| 25-34 | 307 | 95 | 44 | 102 | 7 | 4 | 30 | 179 | 108 | 12 | 5 | 143 | 62 | 13 | 49 | 35 | 141 |
| Row % | 100 | 30.9 | 14.3 | 33.2 | 2.3 | 1.3 | 9.7 | 58.3 | 35.1 | 3.9 | 1.6 | 46.4 | 20.2 | 4.2 | 15.9 | 11.4 | 45.8 |
| 35-44 | 157 | 38 | 20 | 51 | 2 | 1 | 11 | 92 | 55 | 11 | 2 | 83 | 29 | 4 | 28 | 13 | 77 |
| Row % | 100 | 24.2 | 12.7 | 32.5 | 1.3 | 0.6 | 7 | 58.6 | 35 | 7 | 1.3 | 52.9 | 18.5 | 2.5 | 17.8 | 8.3 | 49 |
| >44 | 200 | 56 | 38 | 76 | 6 | 1 | 22 | 113 | 85 | 13 | 1 | 126 | 27 | 10 | 29 | 12 | 102 |
| Row % | 100 | 28 | 19.1 | 38 | 3 | 0.5 | 11 | 56.5 | 42.5 | 6.5 | 0.5 | 63 | 13.5 | 5 | 14.5 | 6 | 51 |
| TOTAL | 1267 | 319 | 191 | 418 | 28 | 16 | 107 | 804 | 437 | 49 | 16 | 545 | 219 | 43 | 194 | 143 | 591 |
| Row % | 100 | 25.2 | 15.1 | 33 | 2.2 | 1.3 | 8.4 | 63.5 | 34.5 | 3.9 | 1.3 | 43 | 17.3 | 3.4 | 15.3 | 11.3 | 46.6 |
| chi square | 14.4731 | 13.2993 | 3.6672 | 7.3967 | 32.8742 | 8.928 | 84.8121 | 7.9645 | 6.47 | 16.2 | 32 | 5.4543 | |||||
| P | 0.013 | 0.021 | 0.598 | 0.193 | <0.001 | 0.112 | <0.001 | 0.158 | 0.26 | .006 | <0.001 | 0.363 | |||||
BWK=Body weakness; CGH=Cough; CHL=Chill; CHP=Chest pain; DIA= Diarrhea; DZN=Dizziness; FEV=Fever; HAC= Headache; ISM=Isomnia; ITCH=Itching; JAC=Joint pain; LAP=Loss of appetite; NAU=Nausea; SAC= Stomach ache; VOM=Vomitting; YELURI= Yellow urine
DISCUSSION
Malaria remains a major public concern, with over 90% of global cases occurring in Africa. Prompt and accurate diagnosis of malaria is the fundamental first step to effectively identify, treat and interrupt disease transmission (Lander et al., 2016). An excellent modelling analysis predicts that > 100,000 malaria-associated deaths would be averted by a 95% sensitive and 95% specific diagnostic tool that require minimal infrastructure. (Rafael et al., 2006). Among children, the prevalence and mortalities associated with malaria are higher than among adults, and in 2019, about 67% of children died of malaria worldwide (Prah et al., 2021; Mohammed et al., 2022). Studies have shown that many anti-malarial drugs have been misused on patients with non-malarial diseases due to a lack of prompt and accurate laboratory diagnosis (Bell et al., 2006). Hence, in malaria-endemic settings, RDT kits are essential in remote areas where microscopes or skilled personnel are unavailable to ensure the effective use of anti-malarial drugs. It has been reported that temperatures in the tropics can denature antibodies in the membrane or damage the nitrocellulose membrane forming the strip of the RDT kits, thereby changing its flow characteristics or causing the antibody to detach from the membrane (Chiodini et al., 2007). Hence, evaluating the performance of these RDT kits in different geographical settings is imperative. In this current study, the sensitivities of the RDT kits was 61.1% for the First Response Malaria AgPf kit to 58.9% for the SD Bioline Ag Pf kit. In other parts of the world, sensitivities of RDT kits ranging from 96.0% to 97.6% have been reported (Msellem et al., 2009; Stauffer et al., 2009; Niscarti et al., 2009; Ajumobi et al., 2015; Domfeh et al., 2023), which implies that the evaluated RDT kits have lower sensitivities. The specificities of RDT kits in this current study was 93.1% for the First Response Malaria Ag Pf kit to 92.3% for the SD Bioline Malaria Ag Pf kit, and specificities of RDT kits within the ranges of 87%–100% have also been reported in previous studies (Buchachart et al., 2004; Msellem et al., 2009; Dougnon et al., 2015). Considering the WHO standard of choosing malaria RDT kits, based on 95% sensitivity (Ajakaye et al., 2020), the SD Bioline Ag Pf kit is the preferred choice. However, all the malaria RDT kits evaluated recorded specificities lower than the WHO recommendation of 97% specificity (Ajakaye et al., 2020), . Hence, microscopic confirmation of malaria is always required after using RDT kits in primary healthcare settings. The sensitivities observed in this study is similar to results obtained by several field studies (Houze et al., 2009, Buchachart, 2010; Ameh et al., 2012; Oyeniran et al., 2014; Ilesanmi et al., 2017; Oluwaremilekun et al., 2020 ) which reported sensitivity ranging from 50.3% -74.3%, but different from the results obtained from several other studies ( Bharti et al., 2008; Khainar, 2009; Okonko, et al., 2009; Ansah, 2010, Chinkhumba et al., 2010; Kalu et al., 2012; Sani et al., 2014; Adekunle et al., 2014; Oboh, et al., 2021), which reported a variable sensitivity of 84.2-100%, but considerably favourable with specificity of 82.8%-98%. Variations in test sensitivity between these studies may be due to differences in the types of RDTs formats used or due to variations in epidemiologic characteristics of the study population, level of parasitaemia, test methodology and skill of microscopists (Oboh et al., 2021).
The sensitivity and specificity value recorded in this study is lower than the WHO recommendation of 95% sensitivity and 97% specificity for malaria RDTs. This is a major issue to be considered when using RDTs in diagnosis of malaria in primary health care or for malaria control programmes (WHO, 2019). Several factors have been reported to be responsible for low performance of RDTs in field conditions which includes effect of environmental conditions such as high temperatures during transportation and storage, quality issues, disease related factors e.g. parasite species and density etc., and also host factors such as treatment history (Emmanuel et al. 2018). The Federal Ministry of Health, National Malaria and Vector Control Division, Nigeria has recommended that RDTs cannot be used to replace microscopy as the only means of diagnosis for malaria (FMOH, 2015). This is because there are variations in the performances of RDTs. The effect of high temperature and humidity which is characteristic of tropical regions on RDTs is a serious limitation. As such, microscopy remains the gold standard for malaria diagnosis and should be used for diagnosis of malaria where possible especially in severe illness where malaria is suspected.
CONCLUSION
In conclusion, RDTs are very useful in areas where microscopic diagnosis of malaria is not feasible however they should not be used to replace microscopy. The performance of the RDTs evaluated in this study had a very low sensitivities when compared with other studies. This is linked to the low parasitaemia seen in the microscopy results. There is need for further investigation on the RDTs used in this study to determine the reason for the low sensitivity recorded
FUNDING/ACKNOWLEDGEMENT
This study was funded by Office of Research Innovation and International Cooperation (RIIC) Babcock and University. The author wishes to express her profound appreciation to Babcock University for providing financial support through RIIC to execute this research. The Research Grant Number: BU/RIIC/2016/008
COMPETING INTERESTS
The authors declare no competing interests
REFERENCES
- Abba, K., Deeks, J.J., Olliaro, P. et al. (2011) “Rapid diagnostic tests for diagnosing uncomplicated P. falciparum malaria in endemic countries,” Cochrane Database of Systematic Reviews, vol. 7, pp. 7–19.
- Adekunle NO, Sam-Wobo SO, Dedeke GA, Ojo DA, Abimbola WA, Adeleke MA, Surakat OA (2014) Evaluation of rapid methods in malaria diagnosis from persons attending primary health facil ities, Ogun State, Nigeria. Niger J Parasitol 35(1–2):19–25
- Ameh J, Ahmad RM, Ekeh N, Linga P, Mangoro Z, Imam AU, Akeredolu P, Hudu S (2012) Laboratory diagnosis of malaria: comparing giemsa stained thick blood films with rapid diagnos tic test (RDT) in an endemic setting in North-west Nigeria. J Med Lab Diagn 3(2):10–15
- Ajakaye, O., Ibukunoluwa, A.R. (2020).“Performance evaluation of a popular malaria RDT in Nigeria compared with microscopy,” Journal of Parasitic Diseases, vol. 44, no. 1, pp. 122–125
- Ajumobi, O., Sabitu, K., Nguku, P. et al. (2015). “Performance of an HRP-2 rapid diagnostic test in Nigerian children less than 5 years of age,” The American Journal of Tropical Medicine and Hygiene, vol. 92, no. 4, pp. 828–833.
- Ansah, E.K., Narh-Bana, S. Epokor, M (2010). “Rapid testing for malaria in settings where microscopy is available and peripheral clinics where only presumptive treatment is available: a randomised controlled trial in Ghana,” British Medical Journal, vol. 340, no. mar051, p. c930.
- Aina, O.O., Agomo, C.O., Olukosi, Y.A., Okoh, H.I., Iwalokun, B.A., Egbuna. K.N., Orok, A.B., Ajibaye, O., Enya, V.N.V., Akindele, S.K., Akinyele, M.O., and Agomo, P.U. (2013). Malariometric Survey of Ibeshe Community in Ikorodu, Lagos State: Dry Season. Malaria Research and Treatment, 1-9.
- Berzosa P, de Lucio A, Romay‑Barja M, Herrador Z, González V, García L, et al. (2018). Comparison of three diagnostic methods (microscopy, RDT, and PCR) for the detection of malaria parasites in representative samples from Equatorial Guinea. Malar J. 17:333.
- Bharti, P.K., Chandel, H.S., Ahmad, A., Krishna, S., Udhayakumar, V. and Singh, N. (2016). Prevalence of pfhrp2 and/or pfhrp3 gene deletion in Plasmodium falciparum population in eight highly endemic states in India. PLoS One. 11(8)
- Buchachart, P.K., Silawat, N., and Singh, P.P. (2010). The usefulness of a new rapid diagnostic test, the First Response® MalariaM Combo (pLDH/HRP2) card test, for malaria diagnosis in the forested belt of central India. Malar J. 7:126.
- Chiodini, P.L., Bowers, K., Jorgensen, P., Barnwell, J.W., Grady, K.K., Luchavez, J., Moody, A.H., Ceniza, A., Bell, D. (2007). The stability of Plasmodium lactate dehydrogenase-based and histidine-rich protein II based malaria rapid diagnostic tests. Transaction of the Royal Society of Tropical Medicine and hygiene. 91:479-483
- Chinkhumba, J., Skarbinski, J., Chilima, B., Campbell, C., Ewing, V., San Joaquin, M., Sande, J., Ali, D., and Mathanga (2010). Comparative field performance and adherence to test results of four malaria rapid diagnostic tests among febrile patients more than five years of age in Blantyre, Malawi. Malaria Journal, 9: 209-214
- Domfeh, S.A., Boateng Y. Darkwa, Y., Raymond K. G., Adu-Asamoah, E., Obirikorang, C.(2023.) Evaluation of Four Malaria Rapid Diagnostic Test Kits Used at the Enyiresi Government Hospital in the Eastern Region of Ghana Journal of Parasitology Research Volume Article ID 4226020, 6 pages https://doi.org/10.1155/2023/4226020
- Dougnon,T.,Bankole,H.S.,Hounmanou,Y.M.G.,Echebiri,S.,Atchade,P.,Mohammed,J.(2015).“Comparative study of malaria prevalence among travellers in Nigeria (West Africa) using slide microscopy and a rapid diagnosis test,” Journal of Parasitology Research, vol. , p. 4, .
- Emmanuel, I.O., Chijioke, U.O., Ekelozie, I.S., (2018). Malaria rapid dagnostic test (RDTs). Ann Clin Lab Res 6(4):275. https://doi.org/10.21767/2386-5180.100275
- Federal Ministry of Health (2015) National guidelines for diagnosis and treatment of malaria—3rd edition. Publications of the Federal Ministry of Health, Nigeria, The Federal Ministry of Health, National Malaria and Vector Control Division. Available at Publications nmcp.gov.nh. accessed
- Houzé, S., Boly, M.D., Le Bras, J., Deloron, P., Faucher, J.F.(2009). PfHRP2 and PfLDH antigen detection for monitoring the efficacy of artemisinin-based combination therapy (ACT) in the treatment of uncomplicated falciparum malaria. Malar J 8:211
- Ilesanmi, R.I., Olalubi, O.A., Ilesanmi, A.O., Effedua, H., Amoo, A.O., (2017). Comparative assessment of some rapid diagnostic test (RDT) kits for malaria diagnosis in Ibadan, Nigeria. MWJ 8:17
- Kalu, K.M., Obasi, N.A., Nduka, F.O., Otuchristian, G. (2012). A comparative study of the prevalence of malaria in Aba and Umuahia urban areas in Abia State, Nigeria. Res J Parasitol 7:17–24
- Kennedy, T. and Otokunefor, K (2017). “Diagnostic efficiency of rapid diagnosis test kits in malaria diagnosis- the Nigerian story,” Gazette of Medicine, vol. 5, no. 2, pp. 1–15.
- Mohammed, K., Salifu, M.G., Batung, E. et al. (2022) “Spatial analysis of climatic factors and plasmodium falciparum malaria prevalence among children in Ghana,” Spatial and Spatio-temporal Epidemiology, vol. 43, p. 100537.
- Landier, J., Parker, D. M., Thu, A.M., Carrara, V.I,, Lwin, K. M, Bonnington CA, et al. (2016). The role of early detection and treatment in malaria elimination. Malar J. 15:363.
- Moody, A.(2002) Rapid diagnostic tests for malaria parasites Clinical Microbiology Revolution 15:66-78.
- Mouatcho J. C, Goldring J. D (2013). Malaria rapid diagnostic tests: challenges and prospects. J Med Microbiol 62(10):1491–1505
- Mukry, S.N., Saud, M., Sufaida, G., Shaikh, K., Naz, A., Shamsi,T.S. (2017). “Laboratory diagnosis of malaria: comparison of manual and automated diagnostic tests,” Canadian Journal of Infectious Diseases & Medical Microbiology, vol. pp. 1–7.
- Msellem, M.I., Mårtensson, A., Rotllant, G., Bhattarai, A., Strömberg, J., Kahigwa, E., et al (2009). Influence of rapid malaria diagnostic tests on treatment and health outcome in fever patients, Zanzibar — a crossover validation study. PLoS Med;6(4).
- Oboh, A.M., Orieroa, E.C., Ndiayeb, T., Badianeb, A.S., Ndiayeb, D., Amambua-Ngwa, A. (2021). Comparative analysis of four malaria diagnostic tools and implications for malaria treatment in Southwestern Nigeria International Journal of Infectious Diseases 108; 377–381
- Odeniyi, O . M. , Agomo C. O. , Okangba, C. C., Olaniyan, K. , Oyibo, W. A. Comparison of Performance Characteristics of Two Malaria Rapid Diagnostic Tests in Detecting malaria infection among febrile patients in urban Area of Lagos, Nigeria Ife Journal of Science vol. 22, no. 2 (2020)
- Okangba, C. C, Oyibo W.A., Thompson, E. T., Ejime E., Ajani, T.A., Elikwu, C.J., Okangba, K. K (2020). The Relevance of Positive Control Wells in Monitoring the Performance of Malaria Rapid Diagnostic Test in the Field for Effective Case Management of Malaria International Journal of Research and Scientific Innovation.| Volume VII, Issue X, | ISSN 2321–2705
- Okangba, C. C., Funwei, R. I., Elikwu, C. J., Nwadike, V. U., Okangba, K. K., Osinowo, A. O., Tayo, B., Taiwo, A. A. and Ogunsola, A. O. (2022). Comparative Evaluation of BinaxNOW™ Malaria Rapid Diagnostic Test, Microscopy and Polymerase Chain Reaction for Plasmodium falciparum Detection among Individuals Suspected with Malaria in Lagos, Southwest Nigeria. Nigerian Journal of Parasitology 43(2) 324-334
- Okonko, I.O., Soleye, F.A., Amusan, T.A., Ogun, A.A., Udeze, A.O., Nkang, A.O., Ejembi, J., Faleye, T.O.C (2009). Prevalence of malaria plasmodium in abeokuta Nigeria. Malays J Microbiol 5(2):113–118
- Oyeniran OA, Ajayi OO, Afolabi AY, Oladipo EK, Adepeju AA (2014) Comparison of rapid diagnostic tests and microscopy for malaria. Afr J Clin Exper Microbiol 15(3):158–174. https://doi.org/10.4314/ajcam.v15i3.7
- Oyeyemi, O.T., Ogunlade, A.F., Oyewole, A. (2015). “Comparative assement of microscopy and rapid diagnostic test (RDT) as malaria diagnostic tools,” Research Journal of Parasitology, vol. 10, no. 3, pp. 120–126.
- Prah, J.K., Amoah, S., Yartey, A.N., Ampofo-Asiama, A and Ameyaw, A.E. (2021) “Assessment of malaria diagnostic methods and treatments at a Ghanaian health facility,” Pan African Medical Journal, vol. 39, no. 1, p. 251.
- Rafael, A.M.E., Taylor, T., Magill, A., Lim, Y., Girosi, F., Allan, R. (2006). Reducing the burden of childhood malaria in Africa : the role of improved diagnostics. Nature. 444(Suppl 1):39–48.
- Sani, U.M., Jiya, N.M., and Ahmed, H. (2013). Evaluation of malaria rapid diagnostic test among febrile children in Sokoto, Nigeria. Int. J. Medi Sci., ISSN 2167, 3(5), 434-440.
- Stauffer, W.M., Cartwright, C.P., Olsonetal, D.A. (2009) “Diagnostic performance of rapid diagnostic tests versus blood smears for malaria in US clinical practice,” Clinical Infectious Diseases, vol. 49, no. 6, pp. 908–913.
- Ugah, U.I., Alo, M.N., Owolabi, J.O et al (2017).“Evaluation of the utility value of three diagnostic methods in the detection of malaria parasites in endemic area,” Malaria Journal, vol. 16, no. 1, pp.1–8
- WHO (2019). The use of malaria rapid diagnostic tests. Second edition. WHO Library cataloguing in Publication Data Geneva.
- WHO (2020). Guideline for the treatment of malaria, second edition, (http:/whqlibdoc.who.int/publications/2020/9789241547925.eng.pdf)
- WHO (2011) Universal access to malaria diagnostic testing, An operational manual. https://www.who.int/malaria/publications/ atoz/9789241502092/en/. Accessed 12 Sept, 2018
- WHO (2015) Guidelines for the treatment of malaria. 3rd edition. https://www.who.int/malaria/publications/atoz/9789241549127/ en/. Accessed 12 Sept, 2018