A Morphosyntactic Analysis of the Speech of Schizophrenic Patients in Cameroon
- FOSSUNG Noutock Gilbert
- 82-99
- Aug 29, 2024
- Health
A Morphosyntactic Analysis of the Speech of Schizophrenic Patients in Cameroon
FOSSUNG Noutock Gilbert, Ph. D, MBA
University of Buea, Faculty of Arts, Department of Linguistics Buea, Cameroon
DOI: https://doi.org/10.51584/IJRIAS.2024.908008
Received: 29 June 2024; Revised: 19 July 2024; Accepted: 23 July 2024; Published: 29 August 2024
ABSTRACT
This work dwelt on the Morphosyntactic analysis of the speech of some Schizophrenic patients in Cameroon. The researcher was poised at giving an analysis of the Morphosyntactic situation in the language of schizophrenic patients. The study included 09 patients who were hospitalized at the Jamot hospital, which is found in Cameroon’s capital city, Yaoundé. The Jamot Hospital is a reference center that handles mental health issues. The problem we set out to solve in this study was that of demystifying the mentality people had about mental health. Many people thought that people suffering from mental illnesses were not capable of communicating appropriately. This study was carried out in Cameroon because there was little or no work done in the country in the domain. The place of the study was appropriate because the Jamot Hospital has a psychiatric center and the unit receives patients nationwide. The researcher chose the Jamot Hospital because of the quasi certainty of finding patients who came from different regions of the country and the diagnosis is up to standard in the place giving that her staff are made up of specialists. The data of this study were collected with the use of interviews. Interviews were recorded and they were later transcribed manually by the researcher. Data were analysed using a qualitative technique. The results from the analysis revealed that the morphosyntax of schizophrenic patients are of good standard. The patients made good declarative utterances. Interrogative, complex as well as affirmative utterances were also properly handled by the patients. However, the patients provided very poor answers to questions. Furthermore, they were also unable to make use of exclamative utterances. The importance of this study is that it will help to demystify the perception people had about mental health and it will also edify public opinion about the language of mental patients.
Keywords: Declarative utterances, Deviation, Interrogative utterances, Morphosyntactic, Negative utterances, Schizophrenia, Psychotic disorders, Synthesis.
INTRODUCTION
Mental illnesses are health conditions involving changes in emotion, thought pattern or behaviour. Mental disorder can be linked to stress and problems of functioning in the society (home, work place, community etc.). We define deviation in this study as a situation whereby a set of rules or expectations are broken in some way (Fossung 2023).
Psychotic disorders such as schizophrenia are characterized by several symptoms, such as delusions, hallucinations, and thought disorders. Thought disorders are described as disturbances in the normal way of thinking, typically presented as various language impairments, such as disorganized speech, which is related to abnormal semantic associations between words (Aloia et al., 1998), and poverty of speech, a thought disorder that is associated with impairments in lexico-semantic retrieval (Nagels et al., 2016).
According to current DSM-5 criteria, a diagnosis of schizophrenia requires the presence of at least one of the following three positive symptoms (DSM-5 295.90, p. 99): Hallucination, Delusions and Disorganized speech (Fossung 2023).
The diagnosis of schizophrenia is mostly based on a professional psychiatric review. However, some studies show that a computational linguistic analysis may help with diagnosis. Fraser et al. (1986), for example, demonstrated that by using a discriminant function analysis of linguistic variables it is possible to predict diagnoses with an accuracy rate of 79%.
According to Laws et al., (1999), there is some evidence that patients with schizophrenia have impaired access to word meanings such that they often prefer denotative to connotative meanings of words. More so, they show less inclination to select metaphorical interpretations of ambiguous adjectives, even when such interpretations are appropriate.
Problem Statement
Mental health seemed to be a mystery in Cameroon especially as many people attributed the illness to witchcraft. There was a lot of ignorance about the illness and many people had issues understanding the language of mental patients. The perception people had was that the language of mental patients was inappropriate, without any tangible reason. This situation made it complex for people to associate with mental patients. The researcher was concerned with the closure of people (family members and the general public) from patients suffering from mental issues, especially in terms of communication. They always considered the patients to be insensible and their language was considered to be gibberish. We therefore set out in this study to have an in-depth analysis of the language of mental patients and to ascertain whether their language differ from the language of healthy people.
Objective of the study
The objective of this study is to find out if there were morphosyntactic deviations in the language of schizophrenic patients in Cameroon. The researcher sought to report different morphosyntactic disorders related to the language of schizophrenic patients. From the observation and experience, the researcher noticed that in Africa and in Cameroon in particular, people have the tendency of associating mental illness to witchcraft (which is not completely false). There is negligence in detecting the onset of illnesses until it is late, and the situation becomes critical. Some people do not know that mental illnesses cause language or linguistic damages (Fossung, 2023). This study also set out to demystify the impression people have about mental illness vis-à-vis the language of mental patients, in this case patients suffering from schizophrenia.
The researcher dwelt on morphosyntactic related deviations caused by schizophrenia. Morphosyntactic deviation is defined in this work as the poor use of grammatical elements.
The main research question of this study is: what are the Morphosyntactic deviations found in the speech of Schizophrenic patients?
LITERATURE REVIEW
Yaara Shriki et al. (2022) carried out a study on “Masking Morphosyntactic Categories to Evaluate Salience for Schizophrenic Diagnosis”. They interviewed 49 patients aged 18-60. These participants were divided into control and patient groups. All the participants spoke Greek as their first language. The patients were diagnosed using the DSM-5 criteria (American Psychiatric Association DSM-5 Force, 2013). The researchers also made use of a full psychiatric interview. Exclusion criteria for all participants included: participants who had Hebrew as their Mother Tongue, participants who had a history of dependence on drugs or alcohol over the past year prior to the study, participants with a past or present neurological illness and participants who used fewer than 500 words in total in their transcribed interview. The patients of this study were interviewed in a quiet room at the hospital, while controlled participants were interviewed in a similar room outside the hospital. Interviews with individuals lasted for about an hour. Interviews were recorded and later on manually transcribed by a native Hebrew speaker.
Thematic Appreciation images were used to test the abilities of the patients and they were all in black and white: including a mixture of men, women, children and adults.
Controlled participants were assessed for symptoms of depression, Post-traumatic stress disorder and anxiety.
Symptoms of depression were assessed using Beck’s Depression Inventory (BDI-II) (Beck’s et al., 1996). Furthermore, the BDI-II is a 21 item inventory rated on a 4-point Likert-type scale. PTSD symptoms were assessed using the PTSD checklist of DSM-5 (PCL-5) (Weathers et al., 2013). The questionnaire contained twenty one items that can be divided into four subscales corresponding to the clusters B-E in DSM 5. They include intrusion, avoidance, negative alterations in cognition and mood and alterations in arousal and reactivity.
Anxiety symptoms were assessed through the State Trait Anxiety Inventory (STAI) (Spielberger et al., 1970). The STAI is made up of a questionnaire which consists of two sets of twenty self-reporting measures.
Patients on the other hand were assessed of psychosis symptoms based on the 6-item Positive and Negative Syndrome Scale (PANSS-6) (Østergaard et al., 2016).
Results of the study showed that all participants used more nouns and third person words than verbs, adverbs, adjectives and first-person words. The high frequency of third-person words is logical because the participants were asked to describe the situation as they understood from the pictures that were presented to them. It was noticed that the inpatients used nouns and verbs slightly more often, whereas controls used more adjectives and adverbs.
Again, a similar study was done by Jayesh Scrivastava et al., (2022) on “High-Order Language Processing Difficulties in Patients with Schizophrenia: Cross-linguistic and Cross-cultural Results from the Hindi Version of Newly Developed Language Test”.
The objective of the study was to detect subtle linguistic performance deficits in patients with Schizophrenia. The researchers developed a test battery in Hindi Vernacular language.
The method used in the study was a replication study of observational, analytical and non-control design. The study made use of 86 participants; with 43 patients suffering from schizophrenia and 43 controls. Patients of the research were analysed using PANSS (Positive and Negative Symptoms Scale for Schizophrenia).
The General Health Questionnaire-12 (GHQ-12) was employed to evaluate participants from the general public. Moreover, comparison was made between the linguistic performances of patients on HLFT (Hindi Linguistic Function Test) to of controls. The HLFT battery was designed, containing 3 blocks by using antonyms, synonyms, homonyms, hyperonyms, hyponyms, distractors and adages.
The results proved that patients scored less than controls in identifying homonyms, distractors and hyponyms, while they scored significantly higher than controls in identifying homonyms.
This current study differs from the above literature in that it deals only with inpatients and excludes controls.
Also, a study was published by Andrea Marini et al. (2008) on The Language of Schizophrenia: An analysis of micro and macrolinguistic abilities and their neuropsychological correlates. The study set out to describe the impairment of micro and macrolinguistic abilities in a group of twenty nine schizophrenic patients during the phase of illness stability compared to forty eight healthy participants and they were matched for age, gender and educational level. Microlinguistic abilities according to the study referred to lexical and morphosyntactic skills while macrolinguistic abilities referred to pragmatic and discourse features. Seventy seven Italian speaking participants were used in the study. The experimental group of the study consisted of twenty nine schizophrenic patients. The patients were diagnosed following the DSM-IV criteria. The patients of study were all in the phase of clinical stability and they were already receiving oral doses of atypical antipsychotics. The researchers added forty eight healthy participants in order to compare the language produced by schizophrenic patients with those of healthy individuals. The groups were matched chronologically by age, gender and level of formal education. The major result of the study revealed that there was a mild problem at the level of microlinguistic processing and a severe deficit on the macrolinguistic level of processing. The speech of schizophrenic patients was quite variable at the microlinguistic level. Some aspects of processing in the language of patients did not significantly differ from the comparison group. There was no problem at the phonetic and phonological levels as far lexical processing analysis was concerned. Macrolinguistic analysis revealed that the narratives of schizophrenic patients were less informative and more tangential compared to those produced by the group of comparison participants. The study concluded that the language of schizophrenic patients was impaired both at the micro and macro linguistic levels of processing.
More so, Matthew Walenski et al. (2011), carried out a study on the Grammatical processing in Schizophrenia: Evidence from morphology. The researchers investigated language in schizophrenia and they focused on inflectional morphology. Forty three patients with diagnosis of schizophrenia, with 21 inpatients and 22 outpatients participated in the study. 12 of the patients were classified to be undifferentiated, 13 were paranoid, 5 were disorganized, 3 had residual subtypes of schizophrenia and 6 had schizoaffective disorder. The other patients were classified based on the DSM-IV; according to the DSM IV criteria, 2 of the patients were chronic, 1 was simple and 1 was atypical with schizophrenia. Data in this study were analysed using a generalized hierarchical linear model (HLM) with a logit link function that was designed for binary outcome data. Results revealed that patients with schizophrenia showed a great deficit relative to healthy control subjects at producing the past tenses of regular and novel verbs than of irregular verbs. A grammatical deficit was also consistently evident in schizophrenia. It was concluded that patients with schizophrenia were worse at producing the past tenses of regular and novel than irregular verbs as compared to healthy control subjects.
Finally, Wolfram and Rossello (2015), did a publication on the linguistics of schizophrenia: thought disturbance as language pathology across positive symptoms. The hypothesis of the study was that schizophrenia is a breakdown of how language configures thought in the normal brain viewed against the un-Cartesian background of what language is. The theory they used was the integrative system. The researchers argued that the origins of the relevant forms of thought and selfhood depend partly on language. They concluded that a linguistic model of positive symptoms may cast fresh light on their pathogenesis and underlying neuropsychology. They posited that thought is not a standard neurocognitive variable.
This current study is descriptive and makes use of interviews as a means of data collection. We also study the morphosyntax of the patients whereas the other studies made use of the identification of preconceived elements, grammatical processing of inflectional morphology and thought disturbance or processes.
The Theories
We used two theories in this study namely the Theory of the Mind (ToM) and the Language of Thought Hypothesis (LOTH). Theory of the mind has been defined as the natural capacity to infer mental states in order to explain and predict behaviour in situations that involve social interaction (Baron-Cohen, Tager-Flusberg and Cohen, 1993). The term was originally coined by primatologists Premack and Woodruff (1978) to suggest the possibility that chimpanzees are capable of inferring the mental states of humans and members of their own species. A great number of developmental psychologists later adopted the term to describe ontogenetic development of the capacity to pretend or simulate in babies and children at the developmental age (Leslie, 1987; Perner 1991). In the field of schizophrenia, Chris Frith and colleagues (Corcoran, Mercer and Frith, 1995; Frith and Corcoran, 1996) carried out an empirical study of ToM deficit in the mid-1990s. The author theorized that autism and schizophrenia could share a common deficit. The impaired capacity for mentalizing in schizophrenia usually appears in adulthood and is generally associated with the first psychotic episode, when all cognitive and linguistic capacities have been fully developed.
The Language of Thought Hypothesis (LOTH) proposes that thinking occurs in a mental language. Usually known as Mentalese, the mental language resembles spoken language in several ways, that is, it has words that can combine into sentences. The words and sentences are meaningful but each meaning depends in the way these words and sentences are combined.
LOTH evolved through the writings of Augustine, Boethius, Thomas Aquinas, John Duns Scotus and several others. The first systematic treatment of LOTH was done by William of Ockham in his work Summa Logicae (c. 1323). LOTH disappeared in the sixteenth century but it had a great revival in the 1970s. Fodor did a publication in 1975 on The Language of Thought (Fodor, 1975). He argued that our current best scientific theories of psychological activity postulate Mentalese and we therefore have a tangible reason to accept that Mentalese exists. According to Fodor (1987:17), thinking consists of chains of mental events that instantiate mental representations, “Thought processes are causal sequences of tokenings of mental representations”.
The choice of these theories was guided by the fact that we dealt with language analysis which has to do with cognitive/mental activities. It is also worth noting that the patients of our study had their first psychotic episodes in adulthood. The illness definitely affected their mental abilities. Schizophrenia is a mental illness and the theories we used in this study deal with language and mental activities.
METHODOLOGY
This study makes use of a qualitative research design. The study was done in the Jamot hospital, situated at the Mballa II neighbourhood in the Centre Region of Cameroon (Yaoundé). The Jamot Hospital is a reference hospital that receives patients nationwide. The hospital has a psychiatric unit with trained and specialized psychiatrists who receive and treat patients with different mental health issues throughout the country. This study was carried out in Cameroon because there was little or no work done in this domain in the country.
The purposive sampling technique was used in this work. This permitted the researcher to conveniently analyse the phenomenon under study. The researcher took an active part in the diagnostic process of patients and this permitted us to identify the schizophrenic symptoms and manifestations of the patients. Schizophrenic patients presented a great degree of linguistic irregularities and this motivated the researcher’s choice to work with them. The researcher was able to initiate prior contact with the patients during the diagnosis phase and it facilitated the one on one contact and collaboration during the interview process.
As far as ethical consideration is concerned, authorization was granted by the head of the psychiatric unit, the caregivers and from the patients themselves.
Semi structured interviews were used to collect data. A Semi structured interview was more appropriate because it created a forum for the researcher to interact elaborately with the patients. Interview sessions lasted for a period of one and a half hour per session and per patient. Interviews were recorded and transcribed manually by the researcher. Interviews were done in a quiet room in the hospital with patients individually.
The population of the study was made up of 09 schizophrenic patients. The study population was made up of patients drawn from different cities of the country. As mentioned earlier, we used a qualitative technique in analysing data with the mathematical formula X=∑ actual score/totalscore×100.
The importance of this study is that it will help to demystify the perception people had about mental health and it will also edify public opinion about the language of mental patients.
ANALYSIS, RESULTS AND DISCUSSION
In this section we look at data presentation, results and discussion.
Synoptic Presentation of Identification, Environmental and Speech Data
In this segment we present a synthesis of the various deviations of this study. We present the patients and the different deviations they are suffering from.
Table 1: Synoptic presentation of identification data
| Patient Feature | M1 | M2 | M3 | M4 | M5 | M6 | M7 | M8 | M9 |
| Age | 29 | 29 | 24 | 25 | 43 | 34 | 37 | 20 | 36 |
| Sex | Male | Male | Female | Male | Male | Male | Female | Male | Male |
| Qualification | BACC | BACC | BEPC | CEP | BACC | BACC | O/L | BEPC | BACC |
| Birth Rank | 2/4 | 5/5 | 9/10 | 4/5 | 8/10 | 2/5 | 4/5 | 5/7 | 5/9 |
| Marital status | Single | Single | Single | Single | Single | Single | Single | Single | Single |
| Profession | Brick layer | None | None | None | None | None | None | None | None |
| Pathology | Paranoid Schizo. | Paranoid Schizo. | Paranoid Schizo. | Paranoid Schizo. | Paranoid Schizo. | Paranoid Schizo. | Paranoid Schizo. | Paranoid Schizo. | Paranoid Schizo. |
| LO1 | French | French | French | French | French | French | English | French | French |
Table 1 shows that the average age of the patients is 30 years. It can also be noticed that the illness affects adolescents as well as adults. The table further reveals that all the patients suffered from schizophrenia and there were seven males and two females. It can therefore be concluded that schizophrenia affects more men than women, this eventually confirms studies published by DSM-V. The highest level of education of the patients is the Advanced Level Certificate. An early onset of schizophrenia prevents those attained from having a long academic pursuit; schizophrenia prevents the patients from adequately pursuing an academic career. None of the patients is a trained professional. Their health condition makes it very difficult for them to get any formal training or education.
Synthesis of environmental data
Environmental data permitted us to know if the neighborhood or society in which the patients live plays a role on the health condition of the patients. In the table below, the left column represents the phenomena under study while the first line at the top of the table shows the various codes of patients. In the table proper, the figures ranging from (0) to (3) reveal the degree of vulnerability of patients. While the number (0) shows that a factor is not affected at all, (1) attests that a factor is mildly affected. Numbers (2) and (3) respectively portray that a factor is averagely or gravely affected.
Table 2: Synoptic Presentation of environmental data
| Patient Phenomenon | M1 | M2 | M3 | M4 | M5 | M6 | M7 | M8 | M9 | TOTAL |
| Family life | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 11 |
| Other illnesses | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 0 | 13 |
| Marijuana | 3 | 3 | 0 | 2 | 0 | 2 | 0 | 1 | 2 | 13 |
| Alcohol | 2 | 2 | 0 | 1 | 1 | 2 | 0 | 1 | 2 | 11 |
| Congenital problems | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 00 |
| Family history | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 3 |
| Frequency in hospital | 3 | 3 | 1 | 1 | 2 | 2 | 1 | 1 | 1 | 15 |
| Other treatments | 2 | 1 | 1 | 0 | 2 | 2 | 2 | 1 | 0 | 11 |
| Living condition | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 12 |
| Believe in witchcraft | 3 | 2 | 1 | 1 | 3 | 1 | 3 | 0 | 0 | 14 |
| Interaction | 3 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 13 |
| TOTAL | 23 | 15 | 08 | 10 | 13 | 14 | 12 | 11 | 10 | 116 |
The table above tell us a lot about the life style and history of the patients. Most of the patients are isolated from their families. They are abandoned to themselves in the hospital or with just a poor mother beside them in the hospital. This situation in itself can affect the treatment of the patients because it is in times like this that they need the greatest support from their family members.
Eight of the patients suffered from other illnesses other than schizophrenia. Seven of them are victims of drug and alcohol abuse which has a strong effect on their health condition.
No single patient suffered from a congenital problem which therefore implies that schizophrenia is not inherited or it is not a health condition caused from birth.
All the patients have tried other forms of treatment before coming to hospital. The treatments were traditional and spiritual. The patients have a very low standard of living. They come from poor families and it is not easy for them to follow treatment. Seven of the patients believed that their condition was caused by witchcraft. This belief pattern makes it difficult for them to be completely healed because they are not completely open to modern medicine. Seminars were regularly organized in hospital to dissuade them from such beliefs.
Synthesis of speech data
In the table below, the number (3) depicts grievous degree of a deviation, the number (2) indicates that a feature is averagely affected and (1) unveils that a feature is mildly affected. The number (0) on its part signifies the total absence of a deviation on a feature under study. The total frequency per deviation is represented at the extreme right of the corresponding line; meanwhile the total number of occurrences per patient is represented at the bottom of the table.
Table 3: Synoptic presentation of speech data
| Patient Feature | M1 | M2 | M3 | M4 | M5 | M6 | M7 | M8 | M9 | TOTAL |
| Speech | 3 | 1 | 1 | 1 | 2 | 1 | 1 | 2 | 1 | 13 |
| Agitation | 3 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 17 |
| Soliloquy | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 1 | 2 | 15 |
| Violence | 2 | 1 | 2 | 0 | 1 | 3 | 1 | 3 | 0 | 13 |
| Threats | 2 | 1 | 2 | 1 | 2 | 3 | 2 | 3 | 0 | 16 |
| Non respect | 0 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 2 | 13 |
| Comedy | 3 | 0 | 1 | 1 | 0 | 2 | 2 | 2 | 0 | 11 |
| Loudness | 2 | 1 | 1 | 0 | 1 | 2 | 1 | 2 | 1 | 11 |
| Cohesion | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| Cooperation | 3 | 1 | 3 | 1 | 1 | 1 | 1 | 1 | 3 | 15 |
| Play | 3 | 0 | 2 | 0 | 0 | 1 | 0 | 0 | 0 | 06 |
| Laughter | 2 | 0 | 2 | 2 | 0 | 0 | 2 | 1 | 2 | 11 |
| Hesitation | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 09 |
| Articulation | 1 | 2 | 2 | 1 | 2 | 1 | 1 | 2 | 1 | 13 |
| Availability of words | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 2 | 1 | 14 |
| Gesticulation | 3 | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 17 |
| Recognition | 1 | 2 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 11 |
| Aggressiveness | 1 | 2 | 2 | 0 | 1 | 3 | 2 | 3 | 0 | 14 |
| Friendliness | 3 | 1 | 3 | 1 | 1 | 0 | 1 | 1 | 2 | 13 |
| Silence | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 11 |
| TOTAL | 39 | 26 | 33 | 19 | 23 | 30 | 26 | 33 | 24 | 253 |
This table gives a summary of the nonverbal behaviour of patients. The patients exhibit habits that people portray on a daily basis. It is worth mentioning that communication can be considered to be good when certain conditions are met. The timing and the place must be well chosen for smooth communication. By timing we mean that the patients need to be in a good shape of mind before they are approached. This same aspect must be respected in sane people. If a person is in a bad mood or under pressure, it is normal that the communication or behaviour of the person will be affected. The place where communication has to take place is equally important. These patients do not like to be embarrassed or to be in the midst of people. Once they feel that they are watched, they suddenly become timid or they become agitated.
According to information on the table, we can see that most of the patients are very friendly people. They are usually skeptical at the point of initial contact, but once they get to know people, they become very nice and friendly. This friendly attitude usually renders smooth the task of the researchers.
All the patients used gestures when communicating. They use facial expression properly, thus, we were able to know when they were happy or sad. This could be noticed with a smile or a frown on the faces. Some also portrayed emotional happiness when a loved one or someone they admired came around.
The speech of the patients was relatively good. They talked in such a way that people were able to get what they said. It was on few occasions that they were not audible enough. But once you indicate to them about their audibility, they immediately adjusted they voice.
Furthermore, there are periods that the patients expressed anger and threatened others. This usually occurs when they are approached abruptly without any prior notice. For them to be hospitable to strangers, a familiar person like a family member or a medical staff needs to be around.
Again, most of the patients were not open to play with others. Six of them were introverts. They were strictly out for business and they were not open to jokes. They were interested in getting interviewed and any other activity was important to them. Despite this challenge, all the patients were cooperative.
More so, about 90% of the patients were respectful. They greeted and followed orders. They also respected conversation roles. They spoke when it was their turn to do so and they did not interrupt the conversation of others. Some of the patients laughed when something funny was said, but there were moments that they smiled or laughed without any apparent reason or stimulus. This situation could be explained by the fact that there were periods when patients had hallucination episodes. There were moments when the patients initiated jokes.
In addition, they showed very little moments of hesitation. Hesitation occur when they feel insecure about a particular topic or when they do not feel confident in the presence of certain people. They always requested that the interview sessions remain private. Hesitation further occurred when their invisible counterparts (hallucinations) instructed them not to reveal certain information.
One thing which was strange to the researcher was that the patients were able to recognize people. From the first encounter with them, there was no single day that they failed to recognize the researcher. This therefore tells us that schizophrenia does not affect the memory of its victims. The patients were friendly and not as aggressive as people would expect. They showed a great degree of maturity.
All in all, we can clearly say that schizophrenia does not completely affect the attitude of patients. The patients express speech behaviours like sane people. Though there are slight deviances, schizophrenic patients use nonverbal communication properly.
Evaluation of Morphosyntactic Performances
This section permits the quantification of the different linguistic performances with the use of statistical diagrams and analysis. As such, we analyse language as well as speech data.
Evaluation of morphosyntactic data
Table four (4) contains a synthesis of morphosyntactic deviations which permits the comparison of the performances of patients and it helps in the identification of the most affected patients. This table is presented herein for explanation purposes.
Table 4: Synoptic Presentation of morphosyntactic deviations
| Patient Feature | M1 | M2 | M3 | M4 | M5 | M6 | M7 | M8 | M9 | TOTAL |
| Declarative Utterances | 3 | 2 | 3 | 3 | 3 | 3 | 2 | 2 | 2 | 23 |
| Interrogative Utterances | 3 | 2 | 3 | 2 | 1 | 2 | 1 | 2 | 2 | 18 |
| Exclamative Utterances | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 01 |
| Affirmative Utterances | 3 | 2 | 1 | 1 | 1 | 0 | 1 | 2 | 2 | 13 |
| Negative Utterances | 2 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 04 |
| Poor Answers | 2 | 2 | 3 | 2 | 2 | 0 | 0 | 0 | 0 | 11 |
| Complex Utterances | 3 | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 1 | 15 |
| TOTAL | 17 | 10 | 13 | 11 | 08 | 07 | 05 | 07 | 07 | 85 |
In the table above, the following can be noticed on the horizontal and vertical axes. Note should be taken that examples will been seen in the form of excerpts in the discussion section.
- The features observed indicate that patients use more declarative utterances to communicate with 23 occurrences.
- Interrogative and affirmative are the next most used features with 18 and 13 occurrences respectively. It was realized that M5 and M7 use interrogative utterances lesser than the others. With affirmative utterances, it could be seen that M6 does not make such utterances while M3, M4, M5 and M7 use them minimally.
- It was noticed that only one patient makes use of exclamative utterances which is a serious issue. The absence of exclamation in patients is due to the lack of emotional sentiments and connection. The patients are rarely moved by what happens around them and as such they find it difficult to attach any sense of empathy or sorrow towards others.
- The features which are problematic to patients are poor answers to questions, complex utterances and negative utterances which all have 11, 15 and 04 occurrences respectively.
According to morphosyntactic analysis, it can be clearly seen that all the patients (100%) make good use of declarative utterances. They make sentences which indicate how they feel and what they like or dislike. Nine of the patients (100%) also make use of interrogative sentences. They ask a lot of questions and it shows that they are good at following up discussions and interacting with people. All the patients use affirmative sentences. 100% of the patients also use complex utterances.
Only one patient (11.1%) uses exclamative utterances, while three patients (33.3%) use negative utterances. This shows that most of the patients have great hope about the future. Five patients (55.5%) answer questions poorly and these poor answers make it difficult for interlocutors to understand them, as such it hinders effective communication.
From the table above, it can be noticed that there are some characteristics that all the patients have deviations in, but the nonconformities do not occur in the same degree. Features such as declarative, interrogative and affirmative utterances are used by all the patients, but in different degrees. Though they score 100% in all three, declarative utterances have twenty three (23) occurrences, interrogative eighteen (18) while affirmative utterances have thirteen (24) occurrences.
In addition, complex utterances have fifteen occurrences, poor answers eleven, negative four and exclamative has only one with the smallest occurrence. These utterances are maximal with M1.
The diagrams below clearly translate the explanations that are given above. While the first shows the most affected patients, the second shows the most affected deviations.
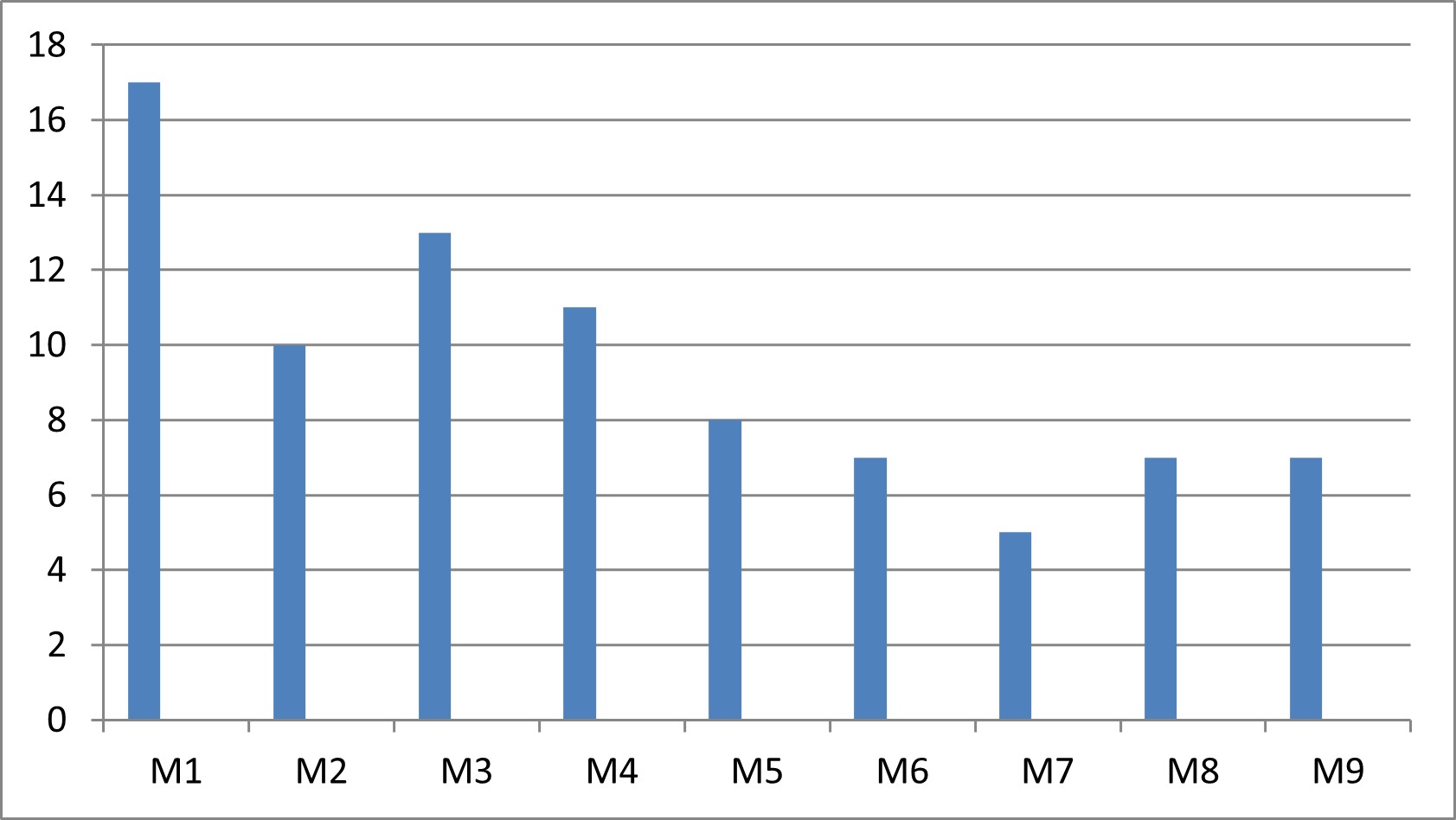
Figure 1: Graphic representation of most affected patients
Diagram 1 shows the degree of affection of each patient. It can be clearly seen that M1 is the most affected patient, followed by patient M3. Meanwhile the least affected patient is M7. Patients M2, M4 and M5 are moderately affected. Patients M6, M8 and M9 are significantly affected.
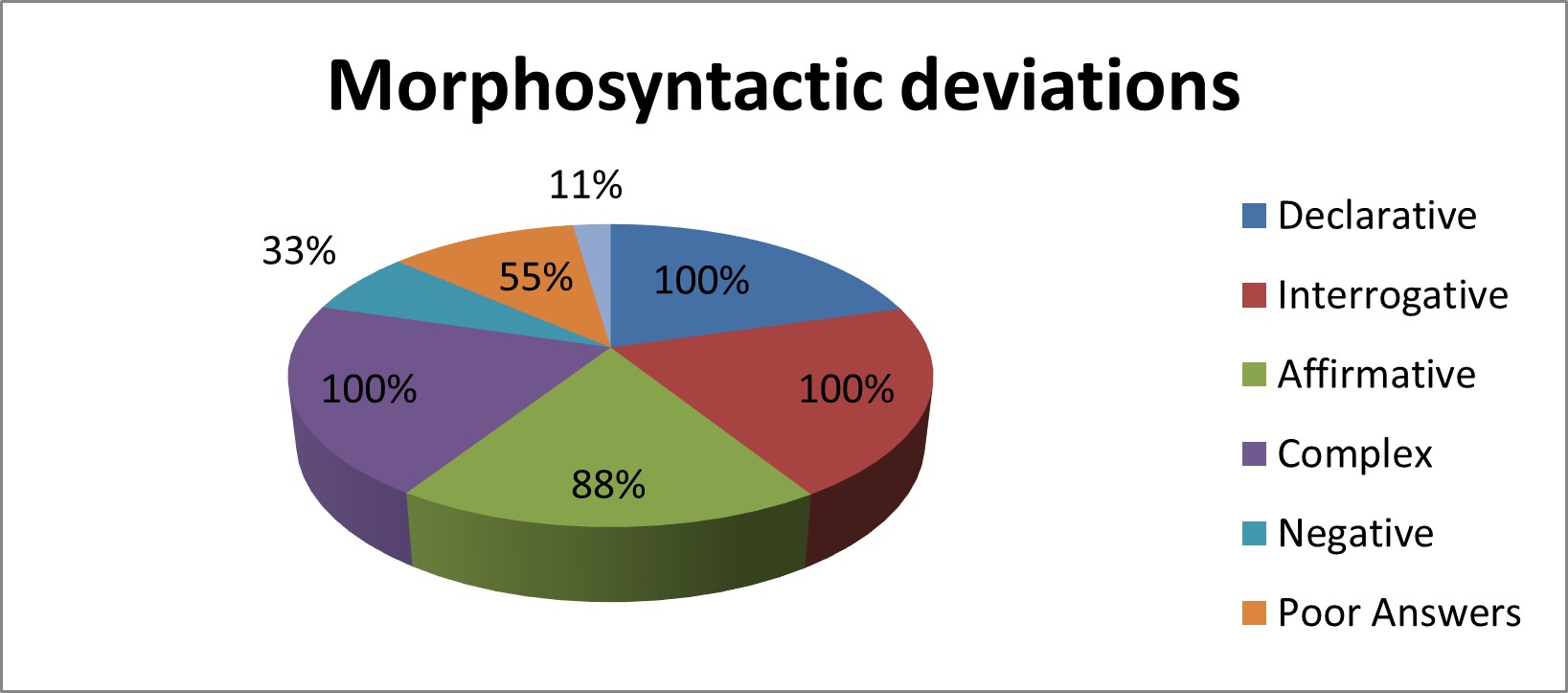
Figure 2: Graphic representation of morphosyntactic performances
The diagram above indicates the following percentages: declarative, interrogative and complex utterances have 100% of usage rate. Affirmative utterances have 88%, poor answers 55% and negative utterances 33%. The feature with the least percentage rate is exclamative utterances with 11%. The different percentages were arrived at using the following formula: Actual number of features divided by total number of features multiplied by one hundred. As such: X= Σ actual score/ total score x 100.
Explanations
As far as morphosyntax is concerned, it was realized that patients did not have a lot of difficulties. Only a few morphosyntactic aspects were affected. The analysis showed that features such as declarative and interrogative utterances were handled averagely by the patients. Even though they did use them in different degrees, they were all able to produce these features in their speech just as it is the case with sane speakers. Affirmative utterances were highly avoided by patients. Only one patient made use of them.
Table 4 shows that patients M1, M3, M4, M5, and M6 handle declarative utterances well. They have issues with interrogative and affirmative utterances. As for patients M2, M7, M8 and M9, the three features just mentioned were averagely handled. It can therefore be concluded that as far as the morphosyntactic features are concerned, three out of the seven features seen on table 4 were averagely handled by patients.
With the exclamative utterances, it was realized that only one patient (M1) actually used such utterances. This shows that the patients hardly show any sign of surprise and are generally very indifferent to what happens around them. Three patients (M1, M3 and M4) use negative utterances. The speech of these patients shows that they do not really have much hope for the future. It is these same patients who have made several returns to the hospital after relapsing. All the patients use complex sentences which are too long and winded. These long and complex sentences make their communication difficult to understand. Complex utterances occur because the thought process of patients is usually disorganized.
DISCUSSION OF RESULTS
In this section explanations are given to the different performances observed through data collected (identification, environmental, speech and language). It begins with explanation of language data, followed by speech performances, gives details of probable causes, consequences and existing therapies.
Explanation of morphosyntactic deviations.
Analysis of performances through language data amounted to the following conclusions.
Declarative utterances
As far as morphosyntactic deviations are concerned, declarative utterances are considered to be a positive feature. All the patients under study use declarative utterances properly just like any other sane user. It should be emphasized that some of the patients express themselves better than their fellow patients.
Excerpt:
Examiner: What is your base?
Patient: According to my basis I am 29 years old and I will be 30 years old on October 15, 2024, I will be 30 years old.
Examiner: What is the cause of spiritual warfare?
Patient: The cause of spiritual warfare is that the bible has been falsified.
Examiner: Are you initiated?
Patient: I was not initiated by anyone because in 2007 these people killed me, the Bamiléké sect affiliated with a Nigerian sect, they killed me in 2007. So if we go back in time, if we go back in time, if we go back in time, back, back, back, back, back, back, back, back, back, back, back, back, back we fall in 2007, we see that I was a goat with the rope about to be slaughtered. So all the rest of my body was the goat, there was only the head which was the head and a rope ready to be slaughtered.
Examiner: Tell me a little about yourself?
Patient: What I like. I don’t like being disturbed, I like being alone, I like music, I like cinema, I smoke cigarettes, I also smoke drugs.
Examiner: So there are people talking to you in your head?
Patient: Yes there are people who talk to me in my head.
Examiner: What are the things you like in life?
Patient: My things I like in life; I want a calm room, a calm room. Whether it is one or two; a calm room with a cement floor, tiled. Put tiles and even a carpet. Then I have a musical set, I have my radio and then what else again? I have my pot and stove.
Interrogative utterances
Again, all nine patients make use of interrogative utterances. Occasionally, the questions they ask are well placed, but other times the questions come as a response to other questions posed to them. The general English rule is that when a question is posed, it should be accompanied by a response; be it positive or negative. It can be clearly said that the interrogative utterances the patients use are not in direct response to the questions posed, and that leads to poor communication because the questions end up without having proper answers.
Excerpt:
Examiner: How old are you?
Patient: According to what chronological basis?
Examiner: What system are you talking about?
Patient: Have you ever heard of the Jurassic?
Examiner: Is it hot?
Patient: Do you feel the heat there?
Examiner: There are 33 shots in total?
Patient: No, there are 33 spiritual planes…, in my theory there are 33 spiritual planes in the negative sense. Where is Marie then? Where is Mary, the mother of Jesus?
Examiner: What did he do?
Patient: Yes, yes precisely in 2003 he carried out an attack to destroy Iraq. But why? For what? This is the question I ask myself. Why did he attack to destroy and then take steps to rebuild? So what is that for? It’s for… What did he do that for? Why did he do that? Why did he do that? Why did he do that? Why did he do that?
Examiner: What is a stadium?
Patient: A football stadium, a competition stadium, a game stadium and you can’t stand me, can you be my friend?
Examiner: What is your first language?
Patient: My first language is Ewondo. When the child is born in the womb, how does it cry?
Examiner: Tell me about yourself?
Patient: Even before talking about me, do you know what we call peanut?
With the interrogative utterances above, it can realized that it is either the patients follow up what is being discussed with them or they are just completely lost. Most often they ask these questions not because they require feedback or a response, but it is their manner of approach. At times these questions are directed to that hallucination partners. It can be seen that the interrogative aspect of the patients’ communication is not properly handled.
Exclamative utterances
Exclamations are used to express emotions and to give a sense of feeling. They are used to express surprise or joy or even sadness. Only one patient uses exclamation. This simply goes a long way to show that schizophrenia affects the psychic of those attained. It is therefore rational to say that the patients show little or no emotions. It makes it difficult for people to read their nonverbal language.
Excerpt:
Examiner: I thought Option-X was about women?
Patient: Ah ya! Hey! You’re not sure. Even women who have never had the pleasure, they will tell you.
Examiner: Are you going to do it hard to him?
Patient: Ah! I’m doing it hard. I put this on, I carry it in the air, I do po, po, po, po in the air eh, not sitting, in the air.
Patient: At that moment I did not yet hear the voices that speak to me now, as they speak to me a lot now. Imagine me getting ready to go and get five hours of sleep, poh!
Only patient M1 uses exclamative utterances in his speech. This shows that the patients are not really concerned with what is happening around them.
Affirmative utterances
Affirmative sentences are used to confirm what has been said. It helps to reinforce a statement or an answer. The patients of this study use this feature appropriately.
Excerpt:
Examiner: Is she an English speaker?
Patient: Yeah, she is English speaking.
Examiner: Cameroon was sold?
Patient: Cameroon was sold by the Bamilékés.
Examiner: Are you initiated?
Patient: I was not initiated by anyone because in 2007 these people killed me, the Bamiléké sect affiliated with a Nigerian sect, they killed me in 2007. So if we go back in time, if we go back in time, if we go back in time, back, back, back, back, back, back, back, back, back, back, back, back, back we fall in 2007, we see that I was a goat with the rope about to be slaughtered. So all the rest of my body was the goat, there was only the head which was the head and a rope ready to be slaughtered.
Examiner: Why do you put Jesus on the spiritual level 33?
Patient: Yes because he is the way, the truth, the life, no one can go to the Father without going through him.
Examiner: So there are people talking to you in your head?
Patient: Yes there are people who talk to me in my head.
Examiner: How is it going? Do you fight wars or small fights?
Patient: I do normal small fights, not big fights, so small challenges. I managed to win untill Kennedy Avenue.
Examiner: Do you love your mother?
Patient: I like my mother.
Examiner: Do you cry?
Patient: I cry when I am thinking. I don’t even do anything and you see tears coming around.
Seven patients (M1, M2, M4, M5, M7, M8, and M9) use affirmative sentences. These sentences revealed that their language is very similar to that of normal speakers. The affirmative utterances tell us that the patients actually know what they are saying and what they actually want. Their point of view cannot be taken from them. It also tells that the patients truly use their minds and are able to analyse things on their own.
Negative utterances
Negative utterances are used to express a sense of frustration, lost, betrayal and dissatisfaction.
Excerpt:
Examiner: Why do you smell water before drinking?
Patient: I don’t trust anyone.
Examiner: You don’t trust your brother?
Patient: No, in my system you shouldn’t trust anyone.
Examiner: Cameroon was sold?
Patient: Cameroon was sold by the Bamilékés.
Examiner: What kind of cigarette do you smoke?
Patient: Any cigarette because I’m hiding, because I’m an atomic bomb, watch out. I’m an atomic bomb.
Examiner: Does your girl friend love you?
Patient: I don’t know if she hates me sometimes.
Examiner: Where was it sold?
Patient: In witchcraft.
It can be noticed that negative utterances come as a result of lack of trust and frustration on the part of patients. They believe in persecution which makes them not to trust people, not even their family members. Due to the fact that some family members have abandoned them and due to the fact that life is not easy as evident in the lifestyle of patients, they try as much as possible to protect themselves and as a result, they resort to using negative utterances and having negative believes. It is quite comprehensible why they act this way because any lonely person will have the tendency of being over protective and not trusting others easily.
Poor Answers
Generally, answers to questions permit us to know what is happening with people and with the society. They help us to understand what is happening around us.
Excerpt:
Examiner: In which forest did you farm?
Patient: We can take everything from you except the dirt, we can take everything from you except the dirt, we can take everything from you except the dirt, we can take everything from you except the dirt, we can take everything from you except the dirt, we can take everything from you take everything from you except the earth, we can take everything from you except the earth, we can take everything from you except the earth.
Examiner: Are you tired?
Patient: Good because he actually thought that Saddam Hussein was the devil. G. W. Bush therefore acted without thinking, he acted without thinking.
Examiner: What is ngolewondo?
Patient: That means we are, her name is Mballa II. It’s just Mballa II now. Why did the whites only come and put CRTV in contact with the mad men, Mballa II. You know why?
Examiner: Where is she?
Patient: She knows my idiot. My name is X, born in 1994, born in 1984 and I lived with her in 1995 and since 1995 we have never seen each other, she knows me. It was only recently that I was called to him. She called my name and my hazard.
Examiner: Are you often agitated or tense?
Patient: That’s not…, life, life has already done tricks on me at a level where people only find me in tension you see a little, that when someone only arrives and they find me tensed. As you have arrived today, I have some time to think. Well, as you have come here, the next person who says something to me I will no longer be happy. Well today you say hello to me, I say hello, what’s the matter? It’s after I think about it that I say why am I
answering him like that, he and I don’t have a problem, that’s why I came to talk to you.
Examiner: Are you tired?
Patient: Good because he actually thought that Saddam Hussein was the devil. G. W. Bush therefore acted without thinking, he acted without thinking.
Examine: But the atomic bomb is made of atoms?
Patient: (Silence)
Examiner: You didn’t know that?
Patient: (Silence)
Examine: Where is she?
Patient: Does she know my idiot? My name is X, born in 1994, born in 1984 and I lived with her in 1995 and since 1995 we have never seen each other, she knows me. I called her just recently. She called my name and my hazard.
Five patients (M1, M2, M3, M4, and M5) answer questions or respond to discussions poorly. The reason for these poor answers is because they do not fully understand what people say and they have problems in comprehending and grasping information. Another reason why they react poorly is because they are easily distracted and do not actually know how to filter external stimuli in order to avoid distraction. Sometimes, they are even aggressive with their responses especially when they do not want to be disturbed or when they are in the company of strangers.
These poor responses make it difficult for people to comprehend and integrate what they say. In order to deal well with these patients, one has to repeat the questions. People equally need to be patient with them. If you do not take things gradually with them, you will encounter serious difficulty getting any information or a proper response from them.
Complex Answers
All patients use complex utterances. The easiest way to answer questions or to communicate is by using short sentences and by going straight to the point. It was realized that the patients make this task very difficult.
Excerpt:
Examiner: Did you say it was part of your system?
Patient: No, my system allows me to define all subsystems. So that is to say, knowing how the CIA works, knowing how the FBI works, how to know who the Albert Einsteins are, who the Isaac Newtons are, who the Bin Ladens are, who the George Walker Bushes are, the Galileos. Do you know Galileo?
Examiner: You don’t like him looking at you?
Patient: No, when he stares at me it’s dangerous, it’s dangerous, it’s dangerous. So we don’t know who Beelzebub is, who the devil is, who Satan is, who Lucifer is. We don’t know who the big Jesus is, who the little Jesus is and we don’t even know who God is.
Examiner: How are you?
Patient: I am in perfect health but it is true that before I took the medication it was killing me but after wards I understood; that is to say they took four injections the first day. Hey! You can send me a little bit of my calendar there. There are references in there. That is to say, when was that already? E…h it was, it was, it was Saturday, Saturday March 1st I received two injections, Sunday two injections ok. Which already makes four injections. Between Saturday and Sunday there were four injections, which completely paralyzed me. But there is one thing that chasics must know and that is that any movement involves a modification of space and time. A thing, a thing, a thing, a thing in the mathematical sense means what? A thing, well an object in the mathematical sense; here is yet another bird.
Examiner: Tell me about your dating life?
Patient: If I have people, friends in relation to… Well, I thought far away or because it’s difficult to understand the stories. So you talked about close collaboration with the environment. There you have it, I told you about Geremi and Mathieu. I have settled with the environment. I have technology, it’s very big eh. It’s not a small town, it’s a big town with Hoysala, I’m talking about HISA, superior to Hysacam.
Examiner: What level of education do you have?
Patient: I have the level…, I…, even any level. I can express myself in Spanish, English, it is enough that God blessed my language because my language is my favorite… They say that when someone has memory problems like me they say lisbanteke, which means you are a bastard, he who is a bastard, the Bamiléké is a bastard.
The above analysis showed that 100% of the patients answered questions in a complex way. It is called complex answers because they did not go straight to the point. Their answers are winded and deviate from the questions asked. This situation makes it very difficult for a listener to pick up anything from their answers. At times they even give a response and actually get confused themselves.
In order to understand what the patients said, the researcher usually asked them to repeat what they said.
What is interesting about the speech of the patients is that they are not just interested in saying short sentences, but they are able to say long and complete sentences like sane speakers. It is also important to say that the speech of these patients is very rich and permit us to be able to learn and analyze from them.
More so, the grammatical aspect of their language is not really affected. They actually follow the sentence structure of English language. They furthermore do not have a lot of problems with conjugation and the use of parts of speech.
The area where they mostly find problems is with the punctuation. They do not actually respect the rules of punctuation which makes it difficult for someone to comprehend their speech.
At times their speech can be compared to a reckless driver who does not respect the Highway Code. With this type of driver there is bound to be accident. In our own situation, there is bound to be poor communication, misunderstanding and misinterpretation.
As a conclusion to this section, it can be conveniently said that the morphosyntax of schizophrenic patients does not have a lot of deficiencies. The patients are able to handle morphology and syntax properly. Analyses attest that they are able to handle aspects such as declarative, interrogative, exclamative and negative utterances. Schizophrenics are able to use complex utterances and they answer some questions properly.
CONCLUSION
This study was based on A Morphosyntactic Analysis of the Speech of Schizophrenic Patients in Cameroon. Our findings showed that males are more affected than females. The structure of the patients’ language is in a good form because they respect general grammatical rules. The patients have issues with some morphosyntactic elements. However, the state of their morphosyntax is above average. The most affected features are poor answers to questions, absence of exclamatory utterances and the use of negative utterances. They use declarative, affirmative and interrogative utterances relatively well. The environments of the patients play a great role in their health condition. People should learn to treat and handle the patients professionally, a situation that will improve their health condition. As we mentioned earlier, this study is important in the sense that it will help to demystify the perception people had about mental health and it will also edify public opinion about the language of mental patients.
REFERENCES
- Aloia, M. S., Gourovitch, M. L., Missar, D., Pickar, D., Weinberger, D. R., & Goldberg, T. E. (1998). Cognitive substrates of thought disorder, II: specifying a candidate cognitive mechanism. American Journal of Psychiatry, 155(12), 1677-1684.
- American Psychiatric Association DSM-5 Task Force (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: American Psychiatric Association.
- Baron-Cohen, S., Tager-Flusberg, H., & Cohen, D. (1993). Understanding other minds: Perspectives from autism. Oxford, England: Oxford University Press.
- Corcoran, R., Mercer, G., & Frith, C.D. (1995). Schizophrenia, symptomatology and social inference: investigating “theory of mind” in people with schizophrenia. Schizophrenia Research, 17, 5-13.
- Corcoran, R., & Frith, C.D. (1996). Conversational conduct and the symptoms of schizophrenia. Cognitive Neuropsychiatry, 1(4), 305-318.
- Fodor, Jerry A. (1975). The Language of Thought, New York: Thomas Y. Crowell.
- Fodor, Jerry A. (1987). Psychosemantics, Cambridge, MA:MIT Press.
- Frank W. Weathers, Brett T. Litz, Terence M. Keane, Patrick A. Palmieri, Brian P. Marx, and Paula P. Schnurr. (2013). The PTSD checklist for DSM-5 (PCL5). Scale available from the National Center for PTSD at ptsd.va.gov.
- Fraser, W. I., King, K. M., Thomas, P., & Kendell, R. E. (1986). The diagnosis of schizophrenia by language analysis. The British Journal of Psychiatry, 148(3), 275-278.
- Fossung, N. G. (2023). Lexical Deviations in the Speech of Schizophrenic Patients in Cameroon. International Journal of Social Work, 10(1), 62-82.
- Hinzen, W., & RossellÓ, J. (2015). The lingustics of schizophrenia: thought disturbance as language pathology across positive symptoms. Frontiers in Psychology, 6.
- Laws, K. R. (1999). A meta-analytic review of Wisconsin Card Sort studies in schizophrenia: general intellectual deficit in disguise?. Cognitive Neuropsychiatry, 4(1), 1-30.
- Leslie, A.M. (1987). Pretense and representation – the origins of theory of mind. Psychological Review, 94(4), 412-426.
- Marini, A., Spoletini, I., Rubino, I. A., Ciuffa, M., Bria, P., Martinotti, G., … & Spalletta, G. (2008). The language of schizophrenia: an analysis of micro and macrolinguistic abilities and their neuropsychological correlates. Schizophrenia Research, 105(1-3), 144-155.
- Nagels, A., Fährmann, P., Stratmann, M., Ghazi, S., Schales, C., Frauenheim, M., … & Kircher, T. (2016). Distinct neuropsychological correlates in positive and negative formal thought disorder syndromes: the thought and language disorder scale in endogenous psychoses. Neuropsychobiology, 73(3), 139-147.
- Østergaard, Soren Dinesen, et al. “PANSS‐6: a brief rating scale for the measurement of severity in schizophrenia.” Acta Psychiatrica Scandinavica 133.6 (2016): 436-444.
- Perner, J. (1991). Understanding the representational mind. Cambridge, MA: MIT Press.
- Premack, D., & Woodruff, G. (1978). Does the chimpanzee have a “theory of mind”? Behavioural and Brain Sciences, 4, 515-526.
- Shriki, Y., Ziv, I., Dershowitz, N., Harel, E., & Bar, K. (2022, July). Masking Morphosyntactic Categories to Evaluate Salience for Schizophrenia Diagnosis. In Proceedings of the Eighth Workshop on Computational Linguistics and Clinical Psychology (pp. 148-157).
- Spielberger, C. D. (1970). Manual for the State-Trait Anxiety Inventory (self-evaluation questionnaire). (No Title).
- Srivastava, J., Sinha, V., Ketteler, D., & Jagtiani, A. (2022). High-Order Language Processing Difficulties in Patients With Schizophrenia: Cross-linguistic and Cross-cultural Results From the Hindi Version of a Newly Developed Language Test. Schizophrenia Bulletin Open, 3(1), sgac029.
- Walenski M., Weickert T.W., Maloof C.J., &Ullman M.T. (2010). Grammatical processing in schizophrenia: evidence from morphology. Neuropsychologia 48:262-69.