
Care Seeking Behavior and Social Support for Sexual and Reproductive Health Needs of Adolescents in Ibadan, Nigeria.
- Ayo-Dada Oluwaseun Dorcas
- Omobowale Oluwatoyin Mofeyisara
- Akinpelu Oyepeju Adekemi
- Adeyemi Susanna Adebusayo
- 473-483
- Apr 22, 2024
- Sociology
Care Seeking Behavior and Social Support for Sexual and Reproductive Health Needs of Adolescents in Ibadan, Nigeria.
Ayo-Dada Oluwaseun Dorcas1*, Omobowale Oluwatoyin Mofeyisara2, Akinpelu Oyepeju Adekemi3, Adeyemi Susanna Adebusayo4.
1Department of Health Sciences, Bamidele Olumilua University of Education, Science and Technology, Ikere, Ekiti State, Nigeria.
2Social and Behavioural Health Unit, Institute of Child Health, University of Ibadan, Oyo State, Nigeria
3Public health department, Lead City University, Ibadan. Oyo State, Nigeria
4Department of Environmental Health Sciences College of Health Sciences and Technology, Ijero, Ekiti State, Nigeria
*Correspondence Author
DOI: https://doi.org/10.51584/IJRIAS.2024.90343
Received: 29 February 2024; Revised: 11 March 2024; Accepted: 16 March 2024; Published: 22 April 2024
ABSTRACT
Background: The importance of caring and meaningful relationships, as well as social connections with individuals and social institutions cannot be overlooked in addressing the sexual and reproductive health issues(SRH) of adolescents. This is a descriptive cross-sectional study to assess care seeking behaviour and social supports for adolescents’ sexual and reproductive health issues. Their ability to be able to seek and find help from formal or informal sources of social support is a protective factor for adolescent health, development and overall satisfaction in life.
Materials and Methods: The study populations were in and out of schools adolescents between the ages of 10 and 19, from selected secondary schools and community in Ibadan North Local Government Area (IBNLGA) of Oyo State, Nigeria, who gave their consent voluntarily to participate in the study.
Results: Findings from this research work revealed that the sources of social support available for adolescent sexual and reproductive health in this study were supports from family, friends, school teachers and religious leaders. Majority of the respondents have high perception of support for SRH issues from family, friends, school teacher and religious leader.
In conclusion, adolescents in this study rely more on their family for supports than other sources because of their availability, accessibility it is necessary to offer relevant information on sexual and reproductive health of adolescents to family as social support as well as other social supports outside of professional care-giving settings, to best promote the prevention and treatment of SRH problems among Nigerian adolescents. Also, future interventions by Adolescent health care providers on sexual and reproductive health of adolescents, should integrate all of the sources of social support and media to deliver evidence based health interventions.
Keywords: Sexual and Reproductive health, Adolescents, Care seeking behavior, social supports.
INTRODUCTION
Adolescents are individuals between the ages of 10-19 years undergoing transition from childhood to adulthood. Literature has shown that the normative tasks of adolescence are becoming more stressful for them due to urbanization and globalization, which has in turn led to reduced social support from families, increased independence and declining status of traditional cultural standards, these changes have been mentioned as the causes of increasing rates of risky behaviours and psychological problems (Pechmann et al., 2019).
Adolescents are tomorrow’s parents and the reproductive and sexual health decisions they make today will affect their health, the well being of their communities and their countries for decades to come (WHO, 2017). Being able to seek and find help from formal or informal sources of social support is a protective factor for adolescent health, development and overall satisfaction in life. The presence and use of social supports is associated, amongst other things, with lower rates of suicide, safer sexual behaviour, lower rates of substance use, later sexual debut and lower rates of delinquency or execution of violence (Liang, 2019). This study therefore, examined common types of sexual and reproductive health issues amongst adolescents, it also assess their care seeking behaviour towards these issues. It documents their perceived social supports and determines the association between socio demographic factors and adolescents’ care seeking behaviour for sexual and reproductive health issues.
The objective of this study is to assess care seeking behaviour and social supports for adolescents’ sexual and reproductive health issues.
LITERATURE REVIEW
Adolescent sexuality and reproductive health are important and of public health concerns especially for issues such as puberty, pregnancy and sexually transmitted disease, including HIV/AIDS. Often times, adolescents thought themselves to be adult and can make decisions on their own, they think they are grown up enough to have sex, not having adequate knowledge about the consequences of unprotected sex. Most times they do not reveal to anyone about their SRH problems and have a habit of not utilizing the healthcare services they actually need, although this may be as a result of inadequate information on healthcare services for SRH issues, attitude of healthcare providers or limited access to financial resources (Atuyambe et al., 2014).
Sexual and reproductive health covers a wide range of issues and challenges that are related to one another. They are: human rights related to sexual health such as sexual pleasure and satisfaction, sexual violence, sexual dysfunction, female genital mutilation, unwanted pregnancy, induced abortion, SRH diseases such as sexually transmitted infections and HIV/AIDS and some issues like puberty, age at sexual debut, early marriage, risky sexual behaviour, contraceptive knowledge and use, abortion, female genital cutting, early marriage, preference for the male child and nutritional taboos (WHO, 2015). One characteristic feature of adolescence according to the world health organization is the progression from the appearance of secondary sexual characteristics to sexual and reproductive maturity (Fernández-Bustos et al., 2019). Giving insight into the kind of sexual and reproductive health related information that adolescents would like to have, In Bangladesh, girls aged 10–12 stated a need for information on changes during adolescence, especially menstruation and suggested that this be provided by mothers, teachers or the media while older adolescents expressed a similar desire for information, adding other topics such as reproduction, fertility, marriage, family planning, STIs and reproductive tract infections (RTIs) and their Preferred sources of information being sisters-in-laws, elder sisters, cousins, peers and community field workers (Zakaria et al., 2020). Ivanova et al. (2019) reported that among the list of sexual and reproductive health problems adolescents seek help for and ask questions about in urban India, menstruation tops the list followed by HIV/AIDS, sexual intercourse, white discharge from the private part and sexual abuse to mention few.
Koce (2019) demonstrates that an individual’s decision to attend a particular health care facility is the composite result of personal need, social forces, the actions of health care providers, the location of services, the unofficial practices of doctors, and in some contexts has very little to do with physical facilities at a particular service point. Specific stresses associated with adolescence that are different from the stresses of childhood or adulthood are: adapting to rapid physical changes, clarifying sexual values and behaviours, amongst others. Our culture expects adolescents to organize and make sense of these forces. Yet, our nation is experiencing a time of diverse family ties, economic hardship, and decreased social cohesion.
MATERIAL AND METHODS
Ibadan North Local Government Area (IBNLGA) of Oyo State, Nigeria, is located approximately on longitude 8°5’ East of the Greenwich meridian and latitude 7°23’ North of equators. The local government is located in the south-western region of Nigeria, it is one of the 11 LGA in Oyo State and one of the five local government area located inside the city of Ibadan, It is a highly populated area with its headquarters located in Agodi. It has an area of 27 km² and a population of 306,795 people. The male population is given as 153,039 and female population as 153,756 (source ERN (National Bureau of Statistics)). There are 12 geo-political wards and the majority of the inhabitants are Yoruba-speaking people with other ethnic groups as minority. There are 89 secondary schools in IBNLGA, 53 of which are private secondary schools and 36 public secondary schools.
This study was conducted among adolescents in and out of schools in Ibadan North local government area of Oyo state.
This study was a community based descriptive cross-sectional study that utilized quantitative method of data collection.
The study populations were in-school and out of school adolescents between the ages of 10 and 19 from IBNLGA, who gave their consent voluntarily to participate in the study.
The completed questionnaires were checked for completeness and a serial number was given to each completed questionnaire for easy identification and recall. All open-ended questions in each questionnaire were coded using a coding guide after a careful review of the responses. Data entering and analysis was done using the Statistical Package for Social Sciences (SPSS) version 20.0 (SPSS Inc. Chicago, ILL). Descriptive statistics such as frequency counts, percentages and mean were calculated and tables, graphs and charts were used to present them. Chi-square test was employed to test relationship and p values less than 0.05 were considered as statistically significant.
RESULTS
A total of 405 respondents were studied, of which 46.2% were males and 53.8% females. The ages of respondents ranged from 10-19 with a mean age of 14.07 +0.076 years. The age-group distributions of respondents were 10-13 years (38.0%), 14-16 years (56.8%) and 17-19 years (5.2%). Most (75.6%) of the respondents were Christians and 24.4% were Muslims. Majority (78.8%) were from Yoruba ethnic group, 10.6% from the Igbo ethnic group, 4.7% from the Hausa ethnic group and (5.9%) were from other ethnic groups. Most (77.5%) of the respondents said they live with both parents, 10.1% live with their mothers alone, 4.2% with their father alone, and 8.2% lives with other relatives (Table 1). Most (56.4%) of the respondents were from private secondary schools and 35.3% from public secondary school and 8.3% were currently out of school. Slightly above half (54.8%) of the in school respondents were in the junior secondary classes (JSS1-3) while 45.2% were in senior secondary classes.
Respondents were asked their understanding of social support. Responses provided by respondents included: support an individual gets from a person or group of people in his/her environment (22%), the coming together of people to assist one another (53%), support giving by people in a community to develop the community (16%) and the relationships around an individual (9%).
Table 2 shows the frequency distribution of the different sources of supports. It is interesting to note that all of the respondents had received some form of social support from different sources. Sources of social support listed by respondents include: family (69.1%), school teachers (35.6%); religious leaders (31.4%) and friends (25.2%)
To determine the level of perception of the respondents for each sources of social supports, respondents were asked different questions under each sources (Family, School teacher, Religious leaders and Friends).Their level of perception was calculated usinga 27-item 4-point Likert scale, the four sections (family, friends, school teacher and religious leaders as sources of support) gave a maximum score of 32, 24, 24 and 28 points respectively with a minimum score of 4 points.
Table 3 Shows that Majority (94.8%) of the respondents have a high level of perception of social support from their friend. (93.8%) had high perception of social support from their religious leaders, 57.3% had high perception of social support from their family and 53.8% had high perception of social support from their school teachers. This result shows that the respondents perceive all the sources of social support as able to give them social supports.
Results as seen in table 4.8 shows that adolescents get support such as advice and information on SRH issues (pubertal issues, pregnancy prevention and sexually transmitted infection including HIV/AIDs) from different sources of supports as illustrated in figure 1
Family including father, mother and siblings (76.3%) ranked first as source of support on pubertal issue, friends (8.8%) ranked second and school teacher (8.1%) ranked third; while the three last sources were counselors (4.5%), religious leaders (1.8%) and older adult (0.5%).
The result for sources of support for STIs show that majority of the adolescents had received supports on STIs including HIV/AIDs from family including father, mother and siblings (69.2%); while very few of the respondents receive support on STIs from counselors (14.2%), religious leaders (6.6%), school teacher (4%), friends (3.9%) and older adults in the community (2.1%).
The major sources of support on how to avoid unwanted pregnancy are family including father, mother and siblings (56%) and friends (23.1%). The other sources are counselors (7.5%), school teachers (7%), older adult in the community (5.1%) and religious leaders (1.3%).
These results shows that Adolescents receive social support on sexual and reproductive health issues such as Pubertal issues, STIs including HIV/AIDs and how to avoid unwanted pregnancy mainly from their family members, as family ranked first as source of social supports.
Hypothesis 2 predicted that there will be no significant association between the Adolescent’s sources of support on SRH issues and their care seeking behaviour. The result of the chi-square analysis to test this hypothesis is presented in Table 5, Table 6 and Table 7
Table 5, 6 and 7 Shows that the relationship between the different sources of support for SRH issues and the care seeking behaviour of Adolescents on SRH issues is statistically significant.
There is a statistically significant association between the sources of social support for adolescents on STIs and the care seeking behaviour of adolescents on STIs including HIV/AIDs (x2 = 171.117 and p-value= 0.000). Likewise the relationship between the sources of social support on pubertal issues and the care seeking behaviour of adolescents on pubertal issues is statistically significant (x2= 238.226 and p-value= 0.000) and there is also a statistically significant association between the sources of social support on pregnancy preventions and the care seeking behaviour of adolescents on ways to prevent unwanted pregnancy with a (x2 of 153.341 and a p-value of 0.000).
DISCUSSION
In examining the care seeking behavior of respondents on general health in this study, participants were asked if they had ever sought treatment for a health issue and majority said yes. A greater proportion of those that had sought care for general health issues consulted a trained medical practitioner (doctors and nurses), while few used the chemist and herb seller. The least proportion of respondent consulted a traditional healer. Majority said they had sought treatment for general health issues such as malaria, headaches, fever etc. While only few said they had sought care for sexual and reproductive health issues.
Families including father, mother and siblings were the most used source of information and advice on care of sexual and reproductive health issues such as pubertal issues, ways to prevent unwanted pregnancy and issues relating to sexually transmitted infections. This is consistent with the findings from Baheiraei et al. (2014) which reported that families especially mothers were the primary as well as the preferred source of health information for adolescents
The sources of social support available for adolescent’s sexual and reproductive health in this study were supports from family, friends, school teachers and religious leaders. Majority of the respondents have high perception of support for SRH issues from family, friends, school teacher and religious leader. However, school teacher has the least percentage of those that had high perception of support, this may be because some schools hardly encourage in-depth teaching of sex education, they only allow their teachers to discuss only failure rate in response to student’s questions on issues relating to SRH. Consistent with this report are findings from Zulu (2019) in his study conducted in Zambia that showed how instruction giving to school teachers and their attitude affected the social relationship with their students.
There was a statistically significant association between age of the respondents in this study and their care seeking behaviour on how to prevent pregnancy. Likewise there is a statistically significant association between age of the respondents and their care seeking behaviour on STIs including HIV, younger adolescents preferred to receive information and advice on care of SRH issues from parents, whereas older adolescents preferred friends. This is in line with findings from the study by Baheiraei et al. (2014) conducted in Iran on what sources adolescents turn to for information about their health concern, the study revealed that family were the primary source of health information for adolescents followed by same sex friends. The study also highlighted the significant association between age and schooling status of respondents and their care seeking behavior, in-school adolescents which are much younger depend on the family especially mothers for support in terms of information while out of school older adolescents reported friends as their source of support for most SRH issues .
CONCLUSION
There are different sources of support available for adolescents SRH issues in the community and those adolescents make use of the available social supports. However, a large proportion of the adolescents sought support from family on care of SRH issues, most respondents reported family and friends as their most available, most beneficial and most reliable source of support for SRH issues. It is therefore necessary to offer relevant information on sexual and reproductive health of adolescents to family as social support as well as other social supports outside of professional care-giving settings, to best promote the prevention and treatment of SRH problems among Nigerian adolescents.
RECOMMENDATIONS
- The Ministry of Health should sensitize Adolescents sources of social supports, to encourage adolescents make greater use of professional health care.
- Future interventions by Adolescent health care providers on sexual and reproductive health of adolescents, should integrate all of the sources of social support and media(book and internet) to deliver evidence based health interventions.
REFERENCES
- Atuyambe, L.M., Kibira, P.S., Bukenya, J., Muhumuza, C., Apolot, R.R. and Mulogo, E. 2015.
- Baheiraei, A., Khoori, E., Foroushani, A.R., Ahmadi, F. and Yharre, M.L. 2014. What source do adolescents turn to for information about their health concerns? Int J Adolescents Med Health 26(1): 61-68
- Fernández-Bustos JG, Álvaro Infantes-Paniagua, Irene Gonzalez-Martí, Onofre Ricardo Contreras-Jordán Body dissatisfaction in adolescents: Differences by sex, BMI and type and organisation of physical activity International journal of environmental research and public health 16 (17), 3109, 2019
- Ivanova O, Masna Rai, Wendo Mlahagwa, Jackline Tumuhairwe, Abhishek Bakuli, Viola N Nyakato, Elizabeth Kemigisha Reproductive health 16, 1-11, 2019
- Koce F, Gurch Randhawa, Bertha Ochieng Understanding healthcare self-referral in Nigeria from the service users’ perspective: a qualitative study of Niger state BMC health services research 19, 1-14, 2019
- Liang M, Sandile Simelane, Guillem Fortuny Fillo, Satvika Chalasani, Katherine Weny, Pablo Salazar Canelos, Lorna Jenkins, Ann-Beth Moller, Venkatraman Chandra-Mouli, Lale Say, Kristien Michielsen, Danielle Marie Claire Engel, Rachel Snow, The State of Adolescent Sexual and Reproductive Health, Journal of Adolescent Health, Volume 65, Issue 6, Supplement, 2019, Pages S3-S15, https://doi.org/10.1016/j.jadohealth.2019.09.015.
- Pechmann C, Jesse R. Catlin, Yu Zheng Journal of Consumer PsychologyVolume 30, Issue 1 p. 149-177 First published: 07 August 2019 https://doi.org/10.1002/jcpy.1136
- Understanding sexual and reproductive health needs of adolescents: evidence from a formative evaluation in Wakiso district, Uganda. Reprodoctive Health 12(35): 7-15
- WHO & UNICEF, 2000. Risk and Protective Factors affecting Adolescent Health and Development. Retrieved May. 2015, from http://www.who.int.html.
- WHO. Maternal, newborn, child and adolescent health. 2017. http://www.who.int/maternal child adolescent/topics/adolescence/development/en/
- Zakaria M, Farzana Karim, Subarna Mazumder, Feng Cheng, Junfang Xu Knowledge on, attitude towards, and practice of sexual and reproductive health among older adolescent girls in Bangladesh: an institution-based cross-sectional study International Journal of Environmental Research and Public Health 17 (21), 7720, 2020
- Zulu JM, Astrid Blystad, Marte ES Haaland, Charles Michelo, Haldis Haukanes, Karen Marie Moland International journal for equity in health 18, 1-10, 2019
Table 1: Socio-demographic characteristics of secondary school adolescents in Ibadan North local government area of Oyo state, Nigeria.
| Socio-Demographic
Characteristics of Respondents |
Frequency (n)
N=405 |
Percentage
(%) |
| Age group (years) | ||
| 10-13 | 154 | 38.0 |
| 14-16 | 230 | 56.8 |
| 17-19 | 21 | 5.2 |
| Gender | ||
| Male | 187 | 46.2 |
| Female | 218 | 53.8 |
| Class in group | ||
| JSS1-3 | 203 | 54.8 |
| SS1-3 | 168 | 45.2 |
| School status | ||
| Private secondary schools | 228 | 56.4 |
| Public secondary schools | 143 | 35.3 |
| Out of school |
34 |
8.3 |
| Religion | ||
| Christianity | 306 | 75.6 |
| Islam | 99 | 24.4 |
| Ethnic Group | ||
| Yoruba | 319 | 78.8 |
| Igbo | 43 | 10.6 |
| Hausa | 19 | 4.7 |
| Others | 24 | 5.9 |
| Living with | ||
| Both parents | 314 | 77.5 |
| Father alone | 17 | 4.2 |
| Mother alone | 41 | 10.1 |
| Other relatives | 33 | 8.2 |
Table 2: The frequency distribution of the respondents that know the different types of social support
| Sources of social support | Frequency (n)
N= 405 |
(%) |
| Family | ||
| Yes | 280 | 69.1 |
| No | 125 | 30.9 |
| School Teacher | ||
| Yes | 144 | 35.6 |
| No | 261 | 64.4 |
| Religious leaders | ||
| Yes | 127 | 31.4 |
| No | 278 | 68.6 |
| Friends | ||
| Yes | 102 | 25.2 |
| No | 303 | 74.8 |
Table 3: Frequency distribution of Adolescents that are perceived to have high and low source of support from each sources of support
| Variable | Frequency (n)
N= 405 |
(%) |
| Perception of Family as source of social support
High Low |
232 173 |
57.3 42.7 |
| Perception of Friends as source of social support
High Low |
384 21 |
94.8 5.2 |
| Perception of School teacher as source of social support
High Low |
218 187 |
53.8 46.2 |
| Perception of Religious leaders as source of social support
High Low |
380 25 |
93.8 6.2 |
Table 4: The frequency distribution of the different sources of social supports for sexual and reproductive health issue
| Sources of social support | Frequency (n)
N= 405 |
(%) |
| Puberty
Family Friends Older adult in the community Religious leaders School teacher Counsellors |
n=396
302 35 2 7 32 18 |
76.3 8.8 0.5 1.8 8.1 4.5 |
| STIs including HIV/AIDs
Family Friends Older adult in the community Religious leaders School teacher Counsellors |
n=377
261 15 8 25 15 53 |
69.2 3.9 2.1 6.6 4.0 14.2 |
| Pregnancy prevention
Family Friends Older adult in the community Religious leaders School teacher Counsellors |
n=373
209 86 19 5 26 28 |
56.0 23.1 5.1 1.3 7.0 7.5 |
Table 5: Associations between Adolescent’s sources of social support for STIs and their care seeking behaviour for sexually transmitted infections.
| Variable | Sources of social support for STIs | ||||||||
| Care-seeking for STIs | N= 251 | Family
n=167(%) |
Friends
n=12(%) |
Older adult
n=6(%) |
Religious leaders
n=21(%) |
School teacher
n=11(%) |
Counsellors
n=34(%) |
x2 |
p-value |
| Family
Friends Teacher Counsellors Chemist Internet Medical practitioner Traditional healer |
64
7 28 31 4 15 100 2 |
61(36.1)
4(2.4) 18(10.7) 20(11.8) 0(0.0) 6(3.6) 58(34.3) 0(0.0) |
0(0.0)
0(0.0) 1(8.3) 0(0.0) 2(16.7) 0(0.0) 7(58.3) 2(16.7) |
0(0.0)
0(0.0) 0(0.0) 1(16.7) 2(33.3) 0(0.0) 3(50.0) 0(0.0) |
2(9.5)
2(9.5) 1(4.8) 6(38.6) 0(0.0) 0(0.0) 10(47.6) 0(0.0) |
0(0.0)
0(0.0) 4(36.4) 0(0.0) 0(0.0) 2(18.2) 5(45.5) 0(0.0) |
2(5.7)
1(2.9) 4(11.4) 4(11.4) 0(0.0) 7(20.0) 17(48.6) 0(0.0) |
171.117 | |
* Statistically significant as p value < 0.05
Table 6: Associations between Adolescent’s sources of social support for puberty related issues and their care seeking behaviour for puberty related issues
| Variable | Sources of social support on puberty related issues | ||||||||
| Care-seeking on puberty related issues | N= 375 | Family
n=287(%) |
Friends
n=31(%) |
Older adults
n=2(%) |
Religious leaders
n=5(%) |
School teacher
n=32(%) |
Counsellors
n=18(%) |
x2 |
p-value |
| Family
Friends Teacher Counsellors Chemist Internet Medical practitioner |
213
18 35 18 4 14 73 |
190(65.7)
8(2.8) 28(9.7) 12(4.2) 4(1.0) 4(1.4) 41(14.2) |
7(22.6)
10(32.3) 0(0.0) 2(6.5) 0(0.0) 6(19.4) 6(19.4) |
0(0.0)
0(0.0) 0(0.0) 0(0.0) 0(0.0) 0(0.0) 2(100.0) |
0(0.0)
0(0.0) 0(0.0) 0(0.0) 0(0.0) 2(33.3) 3(50.0) |
12(37.5)
0(0.0) 5(15.6) 0(0.0) 0(0.0) 1(3.1) 14(43.8) |
4(22.2)
0(0.0) 2(11.1) 4(22.2) 0(0.0) 1(5.6) 7(38.9) |
238.226 | 0.000 |
* Statistically significant as p value < 0.05
Table 7: Associations between Adolescent’s sources of social support for pregnancy preventions and their care seeking behaviour for ways to prevent pregnancy
| Variable | Sources of social support for pregnancy preventions | ||||||||
| Care-seeking onpregnancy prevention | N = 277 | Family
n=195(%) |
Friends
n=11(%) |
Older adults
n=7(%) |
Religious leaders
n=19(%) |
School teacher
n=12(%) |
Counsellors
n=33(%) |
x2 | p-value |
| Family
Friends Teacher Counselors Chemist Internet Medical practitioner Traditional healer |
124
28 46 11 3 16 47 2 |
98(44.7)
21(9.6) 26(11.9) 3(1.4) 2(0.9) 12(5.5) 33(15.1) 0(0.0) |
5(41.7)
2(16.7) 1(8.3) 3(16.7) 0(0.0) 0(0.0) 0(0.0) 0(0.0) |
1(14.3)
0(0.0) 2(28.6) 0(0.0) 0(0.0) 0(0.0) 2(28.6) 2(28.6) |
5(22.7)
0(0.0) 5(22.7) 0(0.0) 0(0.0) 3(13.6) 6(27.3) 0(0.0) |
4(28.6)
0(0.0) 6(42.0) 0(0.0) 0(0.0) 0(0.0) 2(14.3) 0(0.0) |
11(27.5)
5(12.5) 6(15.0) 5(12.5) 1(2.5) 1(2.5) 4(10.0) 0(0.0) |
153.341 | 0.000 |
* Statistically significant as p value < 0.05
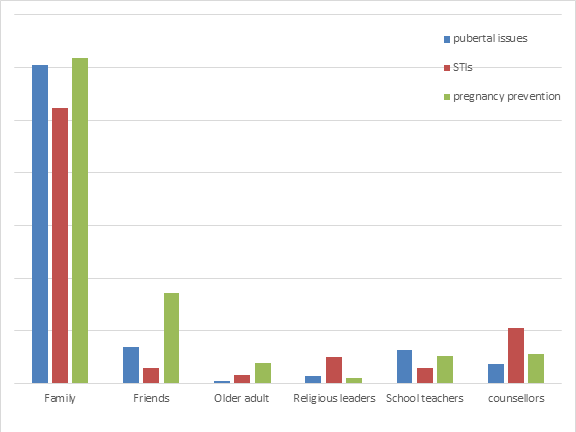
Figure 1: Proportion of the sources of social supports for Adolescents SRH issues