
Prevalence of Disseminated Tuberculosis in HIV-Infected Persons Admitted with Sepsis at Moi Teaching and Referral Hospital, Eldoret, Kenya
- Caroline Gituku
- Adrian Gardner
- Lameck Diero
- Mercy Karoney
- Charity Kanyoro
- 142-155
- Jan 5, 2024
- Health
Prevalence of Disseminated Tuberculosis in HIV-Infected Persons Admitted with Sepsis at Moi Teaching and Referral Hospital, Eldoret, Kenya
Caroline Gituku1, Adrian Gardner2, Lameck Diero3, Mercy Karoney4, Charity Kanyoro5
Moi University, Kenya1,2,3,4,5
DOI: https://doi.org/10.51244/IJRSI.2023.1012012
Received: 01 December 2023; Accepted: 09 December 2023; Published: 04 January 2024
ABSTRACT
Background: Disseminated Tuberculosis (TB) is associated with high morbidity and mortality in HIV-infected persons. The clinical presentation mimics that of sepsis hence requires a high index of suspicion to make a diagnosis. Gold standard of diagnosis is blood cultures that have a long incubation period thus delay in initiation of treatment. Current burden of disseminated TB in adult HIV-infected persons is not known in Western Kenya.
Objectives: To determine the prevalence of disseminated TB and the clinical characteristics of HIV-infected persons with disseminated TB.
Methods: A cross sectional study carried out at the Moi Teaching and Referral Hospital (MTRH) medical wards. Within 24 hours of admission the interviewer administered the questionnaire, and blood and urine samples were collected. Independent variables were summarized using frequencies (%), mean (SD) and median (IQR); dependent variables were analyzed using Student t-test, Chi square and Wilcoxon rank sum test. A p ≤ 0.05 was considered significant.
Results: From April to September 2017, 298 participants were recruited; 58% (173) were female, mean age was 41.68 (SD 11.72).
The prevalence of disseminated TB was 26% (95% CI 21.2-31.4). The LAM positive group had a lower hemoglobin level of 9.71g/dl versus 10.47g/dl in the LAM negative group (p0.04). Sixty percent (178) of the participants had lymphopenia with 31% of them having LAM antigen positive versus 69% having LAM antigen negative (p 0.04). One hundred and ninety-three participants (193) were not on antiretroviral therapy with 30% of them having LAM antigen positive versus 70% of them having LAM antigen negative (p 0.02).
Conclusion: The prevalence of disseminated TB in this setting was 26%. Possible factors associated with LAM antigen positivity included anemia, lymphopenia and not on antiretroviral therapy.
Recommendations: LAM antigen assay should be a routine diagnostic test in HIV-infected persons admitted with sepsis
INTRODUCTION
Background
Tuberculosis (TB) was identified as a leading cause of death from a single infectious agent worldwide in the year 2017. Approximately 10 million cases were diagnosed in 2017, with 9% occurring in PLHIV whereby 72% of them occurred in the African region. It was attributed to cause 300,000 deaths in PLHIV. Thus, World health organization (WHO) recommends early detection and appropriate treatment to reduce the burden(1).
Tuberculosis is the 4th leading cause of death in Kenya mainly affecting the young persons between the ages of 15-34 years. A survey conducted by the ministry of health, 26% of cases were missed because they did not present with the classical symptoms. A further 18% were missed due to reliance on smear microscopy for diagnosis. However due to the paucibacillary nature of MTB the smear may be negative in PLHIV(2).
The combination of HIV and TB has been described as a synergistic relationship with both diseases having a high prevalence in resource limited countries that lack finances for diagnosis and treatment(3, 4).
TB is considered to be disseminated when MTB is isolated from blood or bone marrow, or from 2 or more noncontiguous sites(5). Disseminated TB in HIV, has a nonspecific clinical presentation mimicking that of sepsis, thus a high index of suspicion is required to make a diagnosis(6).
Blood culture is the gold standard for diagnosing disseminated TB, however the long incubation period leads to delay in initiating treatment. Most cases are thus diagnosed posthumously(7).
Patients suspected of having disseminated TB are thus started on empiric anti-tuberculosis treatment(8). However, empiric treatments are often initiated after other alternatives treatments have failed hence a high mortality is still associated in these patients.
A reduced time to diagnosis and initiate treatment is required with consequent reduction of the mortality rate.
The urinary LAM antigen assay has a pooled sensitivity of 44% and specificity of 92% in PLHIV. Its sensitivity increases in inpatient PLHIV with low CD4 counts who have a high risk of disseminated TB with a pooled sensitivity of 61% and specificity of 89%.Thus recommended to aid diagnosis of TB in PLHIV with low CD4 counts (≤100cells/µl) or who are seriously ill regardless of their CD4 counts or with unknown CD4 counts(9).
This study aimed to determine the prevalence of disseminated TB in HIV infected persons admitted with sepsis using urinary LAM antigen assay. Further to characterize the clinical characteristics of PLHIV admitted with sepsis diagnosed with disseminated TB using urinary LAM antigen assay.
METHODOLOGY
Study site
The study was carried out in the adult medical wards at Moi teaching and referral hospital (MTRH) Eldoret, Kenya. MTRH serves as the teaching hospital for Moi University Schools of Medicine. It is a tertiary level hospital serving mainly the north rift and western region of Kenya, plus eastern Uganda, and Southern Sudan. It is the largest referral hospital in the region and the second largest teaching and referral hospital in the country.
Study population
The study population was adult HIV infected persons (PLHIV) admitted with sepsis in the medical wards.
Sepsis was defined by the presence of:
- Suspected infection as per the admitting diagnosis
- Plus 2 or more of the following:
- Respiratory rate >20 beats per minute
- Pulse rate >100beats per minute
- Temperature >39⁰C or <36⁰C
- WBC >12,000/mm or < 4,000/mm(10).
Study design
This was a cross sectional descriptive hospital-based study.
Sampling Technique
Participants were recruited through a consecutive sampling technique until the desired sample size was achieved.
Sample Size.
The sample size was derived using the Fisher et al 1992 formulae.
π= (Z critical) 2 * P (1-P)
d2
Where: (Z critical) 2at 95% confidence interval= 1.96
P = 0.5
Q= (1-P)
D level of precision at 5% = 0.05
Where;
π = sample size
Z = the value corresponding to 95% confidence = 1.96
α = significance level at 5% =0.05
p= estimated prevalence of disseminated TB in PLHIV admitted with sepsis
d= margin of error
Currently in Kenya there are no studies done on the prevalence of disseminated TB in PLHIV admitted with sepsis. However, a similar study was carried out in Uganda, they reported the prevalence of disseminated TB in PLHIV and had been admitted with sepsis at 23%(11).
Since the setting in Uganda is almost similar to our setting:
π = (1.96/0.05)2 *0.5*0.5 = 272
With 10% attrition = 299
Rounded off to = 300
Eligibility Criteria
- Above 18 years
- PLHIV.
- Admitted with sepsis
Study procedure
The study was conducted from April to September 2017.
Upon admission, the principal investigator was informed within 4-12 hours. The participants were then reviewed and those who met the eligibility criteria their consent was obtained.
The interviewer administered the questionnaire that collected data on socio-demographic, HIV associated variables and clinical variables.
Thirty milliliter (30 ml) of urine was collected in a sterile container. Bed bound patients a urinary catheter was inserted, and urine sample was collected under clean sterile technique. Sixty microliters (60µl) of urine was pipetted onto the LAM antigen assay loading bay and incubated for 25 minutes at RTP.
Under standard indoor ambient lighting the strips were then examined for bands within 25-35 minutes of sample loading.
The bands were then compared and graded with the manufacture’s reference card as per the January 2014 guidelines.
Grade 1 was very low intensity while grade 4 was high intensity.
The results were described as follows;
- Positive band was a band equal in intensity with any grade in the reference card.
- Negative band was lack of a band in the patient’s window.
- Equivocal/indefinite was a band that was of lower intensity than any grade in the reference card or an incomplete band.
The LAM antigen assay strips were stored indoors under lock and key at 4-25ºC and were only available to the research assistants. Training on how to undertake the test was done by a certified PhD immunologist at the MTRH laboratory.
Results were immediately provided to the clinicians; positive LAM antigen assay result was accompanied by a recommendation to start TB treatment.
Negative LAM antigen assay result was accompanied with recommendation to consider further diagnostic workup for TB if indicated.
Blood samples were also taken by a trained laboratory technician under aseptic conditions, where 2ml was put in an EDTA bottle for full blood count determination and another 2ml for++
serum keratinize and urea determination.
All the results were provided to the primary clinician.
Medical forms were reviewed, and relevant clinical and laboratory data was obtained and entered in the interviewer administered structured questionnaire. The variables collected included demographic characteristics including age and gender; and HIV descriptors that included the knowledge of their HIV status prior to admission, and whether they were on HAART. Other variables that were collected included; laboratory parameters (CBC, serum urea and creatinine), and the admitting vital signs (axillary body temperature, pulse rate, respiratory rate, and blood pressure).
Data analysis
Data was entered into Epidata version 13.
Continuous variables were summarized as means and standard deviation while categorical data were summarized as frequencies and percentages. Data that was not normally distributed was presented as medians and inter quartile ranges.
The statistical tests that were used were student T test or parametric equivalent (Wilcoxon rankson) and Chi square. Ninety five percent (95%) confidence interval was calculated for the prevalence.
Ethical consideration
This study was conducted with ethical approval of the Institutional Research and Ethic Committee (IREC) of MTRH and Moi University. Permission was also obtained from the management of MTRH.
A written informed consent was obtained from each participant that was recruited for the study.
Confidentiality was maintained throughout the study period and recruitment was carried out in privacy.
All participants including those that declined received the same level of care. There was minimal risk exposed to the participants except the physical pain and discomfort experienced during blood sample collection.
There was no conflict of interest in this study and no incentives were used to recruit the participants.
The results were availed to all the participants and their primary clinicians.
RESULTS
The study was carried out between the months of April and September 2017.
A total of 300 participants were recruited. Upon attaining consent, a spot urine sample was taken for LAM antigen assay testing. The results were provided to the clinician and recommendations to start treatment were made. Data describing the demographics and clinical characteristics were collected.
The results are summarized below.
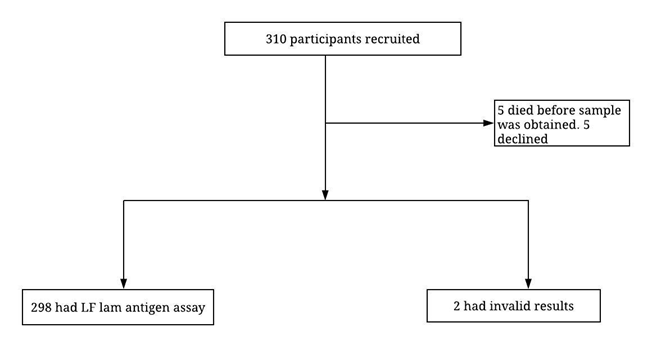
Figure 1: Recruitment schema
Prevalence
Using LAM antigen assay the prevalence of disseminated TB in PLHIV admitted with sepsis was 26% (95% CI 20.96% to 31.20%)
The 298 participants that had LAM antigen assay done, 77 of them had a positive result while 221 had a negative result.
Demographic Characteristics
The median age was 41.68 (SD 11.72), with no difference in age between the LAM positive and LAM negative groups 41.62 (SD 10.58) versus 41.70 (SD 12.13) respectively).
There were more female participants than the male (173 (58%) versus 125 (42%) respectively). However, there was no significant association between sex and LAM positivity.
Table 1: Social demographic characteristics
| Participant Characteristic | Total N= 298 | LAM positive n=77 | LAM negative N=221 | P value | |
| Age | 41.68 (11.72) | 41.62 (10.58) | 41.70 (12.13) | 0.96 | |
| Mean (SD) | |||||
| Sex | Male | 125 (41.95%) | 39 (31.20%) | 86 (68.80%) | |
| Female | 173 (58.05%) | 38 (21.97%) | 135 (78.03%) | 0.072 | |
Table 2: Clinical Characteristics-Admission vital signs
| Participant Characteristic | Total N= 298 | LAM positive n=77 | LAM negative n=221 | P value |
| Systolic BP (mmHg) | 100.89 (19.40) | 97.70 (18.11) | 101 (19.75) | 0.09 |
| Median (IQR) | ||||
| Diastolic BP (mmHg) | 64 (22) | 64 (23) | 66 (23) | 0.54 |
| Median (IQR) | ||||
| Temp (0C) | 37.08 (1.40) | 37.16 (1.61) | 37.06 (1.32) | 0.59 |
| Mean (SD) | ||||
| Respiratory rate(b/m) | 22 (4) | 22 (4) | 22 (2) | 0.93 |
| Median (IQR) | ||||
| Pulse (b/m) | 110 (15) | 110 (14) | 114 (17) | 0.02 |
| Median (IQR) |
The LAM positive group had a lower blood pressure with a median systolic of 98mmHg and diastolic of 64mmHg versus systolic of 101mmHg and diastolic of 64mmHg in the LAM negative group.
All the participants had tachypnea with a median overall respiratory rate of 22 breaths/min with no difference in the two groups.
The radial pulse rate was the only admission vital sign that was statistically significant (p0.02). All the participants had tachycardia with an overall median pulse rate of 110 beats/min. However, the LAM negative group had a relatively lower median pulse rate of 110 beats/min in comparison to 114 beats/min in the LAM negative group.
Table 3: Clinical characteristics- Laboratory markers
| Participant Characteristic | Total N= 298 | LAM Positive n=77 | LAM negative n=221 | P value | |
| White blood cells(109/l) | Normal | 127 (42.62%) | 31 (24.41%) | 96 (75.59%) | |
| Leukopenia | 105 (35.23%) | 27 (25.71%) | 78 (74.29%) | 0.8 | |
| Leucocytosis | 66 (22.15%) | 19 (28.71%) | 47 (71.21%) | ||
| Absolute lymphocyte count (/ml) | Normal
(1001 – 3000) |
114 (38.26%) | 20 (17.54%) | 94 (82.46%) | |
| Lymphopenia
(< 1000) |
178 (59.73%) | 55 (30.90%) | 123 (69.10%) | 0.04 | |
| Lymphocytosis
(> 3000) |
6 (2.01%) | 2 (33.33%) | 4 (66.67%) | ||
| Haemoglobin | Mean (SD) | 10.28 (2.76) | 9.71 (2.93) | 10.47 (2.68) | 0.04 |
| (g/dl) | |||||
| eGFR(ml/min) | Median (IQR) | 95.6(83.9) | 86.8(97) | 96.8(77.65) | 0.53 |
Sixty percent (60%) of all the participants had lymphopenia that was defined as absolute lymphocyte count less than 1000 cells/ml. Of those with lymphopenia, 31% had a positive LAM antigen assay result(p0.04).
All participants had anemia with a median hemoglobin level of 10.28g/dl with the LAM positive group having a lower median hemoglobin level of 9.71g/dl versus 10.47g/dl in the LAM negative group (p 0.04).
The median estimated glomerular filtration rate (eGFR) that was calculated using the CKD EPI formula was 95.6ml/min overall. The LAM positive group had a lower median eGFR at 86.8ml/min versus 96.8ml/min in the LAM negative group though this was not statistically significant (p 0.53).
Table 4: LAM and HIV diagnosis
| Participants characteristics | Total N=298(%) | LAM positive
n=77(%) |
LAM negative
n=221(%) |
P value | |
| HIV Status | Newly diagnosed | 88 (29.53%) | 26 (29.55%) | 62 (70.45%) | |
| Known | 210 (70.47%) | 51 (24.29%) | 159 (75.71%) | 0.344 | |
Seventy percent (70%) of all the participants were aware of their HIV status prior to admission, 24% of them had a LAM antigen assay positive.
Table 5: LAM and HAARTs use
| Participants characteristics | Total
N=298(%) |
LAM Positive n=77(%) | LAM negative n=221(%) | P value | |
| HAART use | Not on HAART | 193 (64.77%) | 58 (30.05%) | 135 (69.95%) | |
| On HAART | 105 (35.23%) | 19 (18.10%) | 86 (81.90%) | 0.02 | |
One hundred and ninety-three (64.8%) participants were not on antiretroviral therapy at the time of admission despite 70% of participants being aware of their status prior to admission. Not being on HAART was significantly associated with having a positive LAM assay result (p0.02).
DISCUSSION
Prevalence
The prevalence of disseminated TB in PLHIV admitted with sepsis at MTRH, in this study was 25.84 % (95% CI 20.96% to 31.20%).
Similar findings were reported in a study carried out in Uganda. Investigators recruited HIV infected persons who had been admitted with sepsis at two Ugandan hospitals and found a disseminated TB prevalence of 23%(11).
The slight difference in prevalence between these two studies could be explained by the fact that the Ugandan study relied on the gold standard to diagnose disseminated TB (MTB blood cultures) while this study utilized urinary LAM antigen assay.
A study conducted in South Africa found a prevalence of 10% among PLHIV attending outpatient clinic using urinary TB LAM(12). A lower prevalence is expected in outpatients compared with inpatients presenting with signs of sepsis(12).
Currently the WHO clearly recommends that the LAM antigen assay should not be used as a screening tool in asymptomatic individuals(9).
Both the WHO and Kenyan government currently recommend the LAM antigen assay as a point of care diagnostic tool in those who have advanced HIV determined either by low CD4 counts or WHO stage 3/4. They also recommend that it can be used regardless of the WHO staging or CD4 counts in the setting of severe illness requiring admission.
Demographics
There was no difference in age between the LAM antigen assay positive group and the negative group with a median age of 41.68 in this study.
Similarly, in the Uganda study there was no difference in age between the two groups. However, the age in the Ugandan study was more widely distributed with a median age of 34 years unlike this study that which was more evenly distributed(11).
A South African study also found no difference in age between the two groups. The age like the Ugandan study was more widely distributed with a median age of 36years (12).
All the three studies had more female participants than males(11, 13). This finding may be explained by differences in health seeking behavior(14).
Despite more female participants, there were more male participants (51%) with LAM antigen assay positivity in comparison to 49% females. Though this was not statistically significant (p 0.072) it is clinically significant. Male gender has been identified to be an independent risk factor for MTB bacteremia(11).Moreover women are more likely to be tested for HIV during antenatal care thus more uptake of antiretroviral treatment and hence less associated LAM antigen positivity(15).
Clinical Characteristics: Admission Vital Signs
The admission vital signs that were taken into consideration were; blood pressure, axillary body temperature, radial pulse rate and respiratory rate.
The statistically significant finding was participants who were LAM antigen assay negative had a higher pulse rate at 114 beats/min in comparison to 110 beats/min in the LAM antigen assay positive group. (p 0.02).
Tachycardia is a common presentation in sepsis and is attributable to sympathetic overdrive. This finding explains why all participants in this study had tachycardia which for the purpose of this study was defined as a pulse rate >100 beats/min. The degree of tachycardia depends on the severity of illness(16).
Similarly, participants with MTB bacteremia had a higher pulse rate than the counterparts and was associated as a non-HIV predictor of MTB bacteremia. However the small sample size in this and the Uganda study limits the generalization of this findings(11).
Laboratory Markers: Hemoglobin Level
Participants with urinary LAM antigen assay positive group had lower hemoglobin concentrations at 9.71g/dl versus 10.47g/dl in the LAM antigen negative group (p 0.04).++Urinary LAM antigen sensitivity increases in patients who are severely ill, hospitalized and anemic in addition to their HIV status CD4 count(17, 18).
Participants with disseminated TB have varying degrees of anemia ranging between severe to moderate with median hemoglobin level at 7.7g/dl (13).
Similar to tachycardia, anemia has been identified as one of the non-HIV predictors of MTB bacteremia(11).
Anemia is the most common hematological abnormality in HIV setting with a prevalence of approximately 70% in HAART naïve individuals(19, 20).
The etiology of anemia in HIV infection is multifactorial but the most common mechanism is through anemia of chronic disease, whereby there is redistribution of iron mediated by hepcidin. Hepcidin is an acute phase reactant that inhibits the absorption of iron in the duodenum and the release of iron from hepatocytes and macrophages (21)
Like all other pathogens MTB requires iron for growth, hence high hepcidin concentrations ensures loading of iron in the macrophages thus promoting growth of MTB. Thus anemia occurring prior to TB diagnosis has been identified as an independent predictor of early incident TB in HIV setting, due to the fact that it allows a conducive environment for the growth of TB bacilli in the macrophages (22)
Thus the prevalence of TB in HAART naïve PLHIV is strongly and directly correlated with the severity of anemia, whereby those with severe anemia have a higher prevalence of TB (23).
TB also causes anemia of chronic disease also by increasing the synthesis of hepcidin from hepatocytes. Hepcidin has already been alluded to traps iron in macrophages and inhibits intestinal absorption of iron.
These two facts explain why despite an overall low hemoglobin level in all participants, the participants that had HIV/TB co-infection had even lower hemoglobin levels.
Anemia in the setting of HIV/TB co-infection has also been associated with increased mortality and progression to AIDS (24). Similar findings were reported in the South African study, where those with severe anemia were found to have lower CD4 counts, higher viral loads and more likely to be in WHO stage 3/4, thus more likely to be immunosuppressed. These same participants with severe anemia and TB/HIV had also higher 90 day mortality and poorer prognosis (23).
Absolute Lymphocyte Count
Lymphopenia was a common finding in 60% of all participants with approximately 30% of them having a LAM antigen assay positive (p 0.04).
Lymphocytes are broadly classified into B and T lymphocytes. The T lymphocytes are further classified into the helper CD4 T lymphocytes and cytotoxic CD8 T lymphocytes.
HIV virus targets the CD4 T lymphocytes in the gut associated lymphoid tissue leading to overall reduction of the CD4 T lymphocytes in the circulation. Initiation of HAART plus the cytotoxicity of the CD8 T lymphocytes helps to control the viremia and in so doing increases the CD4:CD8 ratio above 1.
T lymphocytes are central in controlling the replication of MTB; thus, the low T lymphocytes count in PLHIV increases their susceptibility to MTB infection.
A CD4 count and percentage measurement helps determine the level of immune suppression, and the risk of developing opportunistic infections, with increased risk with CD4 counts <200cells/μl.
The normal reference range for absolute lymphocyte count is between 1.0–3.0×109/l while that for a total lymphocyte count ranges between 4.0-10.0×109/l.
Similar findings were reported in the Uganda study whereby the participants with MTB bacteremia had a lower lymphocyte count (0.8 versus 1.1) compared with the non-MTB bacteremia group (p0.007)(11).
HIV Descriptors
One hundred and ninety-three (193) participants were not on HAART at the time of admission, However, for the purpose of this study it was difficult to ascertain when the participants were diagnosed and if they were defaulters or HAART naive. The only character of interest that was taken to consideration was whether they were taking HAART at the time of admission.
Participants not on HAART, 30% of them had LAM antigen assay positive versus 18% who were on HAART with LAM antigen assay positive (p 0.02).
Absence of HAART in PLHIV as one of the independent predictors for MTB bacteremia(11).
Further characterization of the participants in this study found that 71% of them were actually aware of their status prior to admission despite 65% of them not being on HAART. The Ugandan study also reported almost similar findings whereby 67% of the participants were actually aware of their status prior to admission with 77% of them not being on HAART(11). This goes to show that there is a good uptake of HIV testing however there could be loss of linkage between those who are tested and those who are started on HAART.
However, a South African study, 81% of the participants were aware of their HIV status at the time of recruitment with 58% of them not on HAART. Further characterization of the participants who were not on HAART, only 12% of them had disseminated TB. This finding in contrast to the current study and the Ugandan study, was not statistically significant (p0.11)(13).
Currently the WHO recommends testing and treating for HIV; however, in all 3 countries there was discrepancy between those who were aware of their HIV status and those on HAART.
Uptake of HIV testing has increased in Sub Saharan countries hence the discrepancy is not in the uptake of testing but rather the linkage of treatment(15, 25).
Currently the Kenyan government recommends initiation of HAART therapy once a diagnosis of HIV is confirmed regardless of the CD4 counts or WHO staging.
Participants not on HAART had a higher rate of having LAM antigen assay positive in comparison to those who were on HAART (30% versus 18% (p0.02). This is despite the fact that a quite majority of them were aware of their status prior to admission, thus further research is required to identify why there is a discrepancy between the number tested and those actually on HAART.
Renal Involvement
This study aimed to describe whether there were any renal derangements in participants who had urine LAM antigen assay positive. We calculated the estimated glomerular filtration rate (eGFR) using the CKD EPI formula, the median overall eGFR was 95.6ml/min in all participants, with LAM++
antigen positive having a lower median eGFR at 86.8m/min versus 96.8ml/min in those who had LAM antigen assay negative, though this was not statistically significant it is clinically significant (p 0.53).
Previous studies had postulated that LAM antigenuria is caused by simple ultrafiltration mechanisms, however recent studies have not supported this hypothesis.
Hypothesis that have been postulated include; first LAM being an antigen in circulation it has to be bound to either anti-LAM antibodies or high-density lipoproteins. Hence this immune-complex of bound LAM cannot pass an intact glomerular basement membrane due to the tight fenestrations junctions(26).
Secondly it was thought that the LAM antigenuria was due to high disease burden. However, this too has been proven to be null and void due to the findings on initiation of TB treatment, serum LAM increases however urine LAM has not been shown to increase. This is further supported by the fact that LAM antigen assay has been found to have a low sensitivity in the diagnosis of pulmonary TB even in high burden disease states(27).
Third it was thought that participants with LAM antigenuria could be having an underlying glomerular pathology. This too has been proven to be null and void since no studies have shown any association between urine LAM antigen positivity and proteinuria considering that proteinuria is a marker of glomerular damage. Also postmortem studies that have assessed renal biopsies of participants who had LAM antigen positive have not reported any glomerular damage(28).
It is thus hypothesized that the LAM antigenuria is due to actual detection of the MTB bacilli in urine. This has been shown in a study that reported that urine that was LAM positive; Gene Xpert MTB/RIF assay done on the same urine sample was able to detect more that 50% of the cases. Gene Xpert MTB/RIF assay detects whole MTB bacilli by amplification of the DNA and not just the MTB antigens(29).
This was further shown in a study conducted in Uganda where they assessed the kidney biopsy of participants who had urinary LAM antigen assay positive. There was histological evidence consistent with renal TB involvement in 62% of the biopsies. It is now postulated urinary LAM antigen assay positive is due to the haematogenous spread of the MTB bacilli and the associated renal involvement. This is further supported by the fact that urine LAM antigen assay has been shown to have increased sensitivity in those who have advanced HIV and have a high risk of developing renal TB hence disseminated TB(30).
The South African study also assessed the eGFR and the median overall eGFR was 125ml/min (IQR 18-227) with participants with disseminated TB having a lower median eGFR of 126ml/min (IQR 80-167) versus 129ml/min (IQR 95-166) (p 0.96)(12).
The Ugandan study however assessed only the creatinine levels and didn’t calculate the eGFR, the median overall creatinine level was at 97.24 (IQR 0.8-1.7) with no much difference reported in those with MTB bacteremia(11).
However, in all three studies the sample size of those with disseminated TB was small, this study had a sample size of 77, Kerkoff et al in South Africa had a sample size of 41 and Shevin et al in Uganda had a sample size of 86. All these studies were thus not powered to assess for correlation between urinary LAM antigen positivity with eGFR. Further studies with a larger sample size are thus required to further assess for this association(11, 12).
CONCLUSION AND RECOMMENDATIONS
Conclusion.
There is a high prevalence of disseminated TB (26%) in PLHIV admitted with sepsis in the medical wards at Moi Teaching and Referral Hospital. The associated risk factors in our setting included: not being on HAART, anemia, tachycardia, and lymphopenia.
Recommendations
- LAM antigen assay should be a routine diagnostic test in PLHIV who are admitted with sepsis.
- Further exploration of the possible associated risk factors in a study with a larger sample size is recommended
REFERENCES
- Organisation WH. Global Tuberculosis report. 2018.
- Enos M, Sitienei J, Ong’ang’o J, Mungai B, Kamene M, Wambugu J, et al. Kenya tuberculosis prevalence survey 2016: Challenges and opportunities of ending TB in Kenya. PLoS One. 2018;13(12):e0209098.
- Juffermans NP, Speelman P, Verbon A, Veenstra J, Jie C, van Deventer SJ, et al. Patients with active tuberculosis have increased expression of HIV coreceptors CXCR4 and CCR5 on CD4(+) T cells. Clin Infect Dis. 2001;32(4):650-2.
- Nakata K, Rom WN, Honda Y, Condos R, Kanegasaki S, Cao Y, et al. Mycobacterium tuberculosis enhances human immunodeficiency virus-1 replication in the lung. Am J Respir Crit Care Med. 1997;155(3):996-1003.
- Jolobe OMP. Disseminated tuberculosis. QJM: An International Journal of Medicine. 2017;110(5):331-.
- Wang JY, Hsueh PR, Wang SK, Jan IS, Lee LN, Liaw YS, et al. Disseminated tuberculosis: a 10-year experience in a medical center. Medicine (Baltimore). 2007;86(1):39-46.
- Gupta RK, Lucas SB, Fielding KL, Lawn SD. Prevalence of tuberculosis in post-mortem studies of HIV-infected adults and children in resource-limited settings: a systematic review and meta-analysis. Aids. 2015;29(15):1987-2002.
- Organisation WH. Global Tuberculosis Control Surveillance, Planning, Financing. 2007.
- Organisation WH. The use of lateral flow urine lipoarabinomannan assay (LF-LAM) for the diagnosis and screening of active tuberculosis in people living with HIV 2015.
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644-55.
- Jacob S, Pavlinac P, Nakiyingi L, Banura P, Baeten J, Morgan K, et al. Correction: Mycobacterium tuberculosis Bacteremia in a Cohort of HIV-Infected Patients Hospitalized with Severe Sepsis in Uganda–High Frequency, Low Clinical Suspicion and Derivation of a Clinical Prediction Score. PLoS One. 2013;8(8):10.1371/annotation/0a53f994-bfe2-45db-9dbb-97fdfea023c5. doi 10./annotation/0a53f994-bfe2-45db-9dbb-97fdfea023c5. eCollection 2013.
- Kerkh off AD, Barr DA, Schutz C, Burton R, Nicol MP, Lawn SD, et al. Disseminated tuberculosis among hospitalised HIV patients in South Africa: a common condition that can be rapidly diagnosed using urine-based assays. Sci Rep. 2017;7(1):10931.
- Muriithi MK. The determinants of health-seeking behavior in a nairobi slum, kenya. European Scientific Journal, ESJ. 2013;9.
- Sarah Staveteig SW, Sara K. Head, Sarah E.K. Bradley, Erica Nybro of ICF Macro. Demographic patterns of HIV testing uptake in sub-saharan africa. 2013.
- Waitt PI, Mukaka M, Goodson P, SimuKonda FD, Waitt CJ, Feasey N, et al. Sepsis carries a high mortality among hospitalised adults in Malawi in the era of antiretroviral therapy scale-up: a longitudinal cohort study. J Infect. 2015;70(1):11-9.
- Lawn SD. Point-of-care detection of lipoarabinomannan (LAM) in urine for diagnosis of HIV-associated tuberculosis: a state of the art review. BMC Infect Dis. 2012;12:103.
- Lawn SD, Dheda K, Kerkhoff AD, Peter JG, Dorman S, Boehme CC, et al. Determine TB-LAM lateral flow urine antigen assay for HIV-associated tuberculosis: recommendations on the design and reporting of clinical studies. BMC infectious diseases. 2013;13(1):407.
- Anyabolu E. Prevalence and Associated Factors of Anemia in Treatment-na?ve HIV-positive Subjects in Southeast Nigeria. American Journal of Medical Sciences and Medicine. 2016;4(2):41-6.
- Meidani M, Rezaei F, Maracy MR, Avijgan M, Tayeri K. Prevalence, severity, and related factors of anemia in HIV/AIDS patients. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences. 2012;17(2):138.
- Ganz T, Nemeth E. Iron homeostasis in host defence and inflammation. Nature Reviews Immunology. 2015;15(8):500.
- McDermid JM, Hennig BJ, van der Sande M, Hill AV, Whittle HC, Jaye A, et al. Host iron redistribution as a risk factor for incident tuberculosis in HIV infection: an 11-year retrospective cohort study. BMC infectious diseases. 2013;13(1):48.
- Kerkhoff AD, Wood R, Vogt M, Lawn SD. Predictive value of anaemia for tuberculosis in HIV-infected patients in sub-Saharan Africa: an indication for routine microbiological investigation using new rapid assays. Journal of acquired immune deficiency syndromes (1999). 2014;66(1):33.
- Mocroft A, Kirk O, Barton SE, Dietrich M, Proenca R, Colebunders R, et al. Anaemia is an independent predictive marker for clinical prognosis in HIV-infected patients from across Europe. Aids. 1999;13(8):943-50.
- Rosen S, Fox MP. Retention in HIV care between testing and treatment in sub-Saharan Africa: a systematic review. PLoS Med. 2011;8(7):e1001056.
- Haraldsson B, Nyström J, Deen WM. Properties of the glomerular barrier and mechanisms of proteinuria. Physiol Rev. 2008;88(2):451-87.
- Wood R, Racow K, Bekker LG, Middelkoop K, Vogt M, Kreiswirth BN, et al. Lipoarabinomannan in urine during tuberculosis treatment: association with host and pathogen factors and mycobacteriuria. BMC Infect Dis. 2012;12:47.
- Peter JG, Theron G, Muchinga TE, Govender U, Dheda K. The diagnostic accuracy of urine-based Xpert MTB/RIF in HIV-infected hospitalized patients who are smear-negative or sputum scarce. PLoS One. 2012;7(7):e39966.
- Lawn SD, Kerkhoff AD. Rapid diagnosis of TB in HIV-positive in-patients with M. tuberculosis bacteraemia in sub-Saharan Africa. Int J Tuberc Lung Dis. 2015;19(12):1557-9.
- Lawn SD, Gupta-Wright A. Detection of lipoarabinomannan (LAM) in urine is indicative of disseminated TB with renal involvement in patients living with HIV and advanced immunodeficiency: evidence and implications. Trans R Soc Trop Med Hyg. 2016;110(3):180-5.