
Implementing Community Antimicrobial Stewardship Model in Nigeria: Lessons Learned From Ams Outpatient Setting Among Community Pharmacists/Patent and Proprietary Medicine Vendors (PPMVS)
- Danjuma K. ADDA
- Obed Tiwah JOHN
- Barnabas Toge
- Abiodun EGWUENU
- Ridwan YAHAYA
- Tochi OKWOR
- Oscar Facknwie KAHWIR
- Rijimra ANDE
- Joyce C. JOHN
- Lawrence DANIEL
- Mohammed UMARU
- 521-534
- Feb 27, 2024
- Education
Implementing Community Antimicrobial Stewardship Model in Nigeria: Lessons Learned from AMS Outpatient Setting among Community Pharmacists/Patent and Proprietary Medicine Vendors (PPMVS)
Danjuma K. ADDA1, Obed Tiwah JOHN2*, Barnabas Toge3, Abiodun EGWUENU4, Ridwan YAHAYA5, Tochi OKWOR6, Oscar Facknwie KAHWIR7, Rijimra ANDE8, Joyce C. JOHN9, Lawrence DANIEL10, Mohammed UMARU11
1,2,3,7,8,9,10,11Centre for Initiative and Development (CFID) Taraba
4,5,6Nigeria Centre For Disease Control (NCDC)
3Department of Pharmaceutical Science, University of Calabar, Nigeria
DOI: https://doi.org/10.51244/IJRSI.2024.1101038
Received: 08 January 2024; Revised: 13 January 2024; Accepted: 18 January 2024; Published: 23 February 2024
ABSTRACT
Antimicrobial resistance (AMR) is a growing global concern primarily driven by the overuse and inappropriate utilization of antimicrobials. In Nigeria, AMR is exacerbated by the routine sale of prescription-only medicines, including antimicrobials, without proper monitoring. The National Action Plan for Antimicrobial Resistance (2017-2022) highlighted widespread inappropriate antibiotic use, with significant proportions obtained without prescriptions. Antimicrobial stewardship (AMS) in outpatient settings is a novel concept in Nigeria. This interventional study sought to contribute to the reduction of inappropriate antibiotic dispensing and use in community/outpatient settings in Nigeria, focusing on enhancing the skills and capacity of improved rational antibiotic therapy among community pharmacists and Patent and Proprietary Medicine Vendors (PPMVs), with the sole aim of improving patient health outcomes. The CAMS interventional study involves education, quality improvement capacity building, patient empowerment, and a multifaceted AMS strategy. Results from the CFID’s CAMS model indicated a significant improvement in the rational dispensing and use of antimicrobials within the intervention group, emphasizing the effectiveness of CAMS. Notable variations in post-visit actions between the intervention and monitoring groups further support the positive impact of the intervention. Variation in attitudes towards sharing of antibiotic to friends and relatives was reduced among the intervention group, offering clear understanding into the potential impact of CFID AMS outpatient setting (CAMS) intervention. The study’s conclusion underscores the pivotal role of implementing AMS in outpatient and community settings such as the CAMS interventional model in improving antibiotic-related practices in both urban and rural communities in Nigeria, emphasizing its relevance and impact.
Keywords: Community Antimicrobial Stewardship, Nigeria
INTRODUCTION
The main drivers of Antimicrobial resistance (AMR) is the overuse and inappropriate use of antimicrobials, including taking the wrong kinds of antimicrobials, not using them as instructed by the doctors or using them at inap9cpropriate doses (Allison et al. 2020). In Nigeria, prescription monitoring is poorly conducted and prescription only medicines (POM) including antimicrobials are routinely sold Over-The-Counter (OTC) in pharmacies and by patent proprietary medicines vendors (PPMVs) (National Action Plan for Antimicrobial Resistance, 2017-2022). The National Action Plan for Antimicrobial Resistance, 2017-2022, found that bad use of antibiotics was common with 42% of adults and 46.7%–71.1% of five years’ children were given antibiotics without prescription (WHO-Africa, 2021). According to the national guidelines, antibiotics are prescription-only drugs in Nigeria and should only be provided under the supervision of a licensed medical expert. Unfortunately, antibiotics are routinely supplied over the counter among community pharmacies and PPMVs with little or no control due to inadequate prescription monitoring (FMoA, 2017; Adda et al. 2022; Isah et al. 2023). Many reasons have contributed to the occurrence of antimicrobial resistance, including, but not limited to, antimicrobial abuse and overuse, lack of awareness, inadequate information, and lax public health policy (WHO, 2021)
Antimicrobial stewardship in outpatient settings is a relatively new concept in Nigeria’s health care system. Nigeria constitutes a large market for Pharmaceuticals, accounting for 60% of the volume of health products consumed in the Economic Community of West African States (ECOWAS) sub-region, but has limited regulatory capacity. Antimicrobials are sold in the streets by hawkers, or by unregistered premises and, in many cases by non-pharmacists in many communities in Nigeria.
Context specific barriers that affects successful AMS services in outpatient settings needs to be identified and addressed. Therefore, this interventional study aimed to contribute towards reducing inappropriate dispensing and use of antibiotics in community settings towards improving patient’s health outcomes.
Objective
To promote the rational dispensing and use of antibiotic therapy among community pharmacists/Patent and Proprietary Medicine Vendors (PPMVs), households, youth and adult populations and patients in urban and rural communities in Nigeria to improve patient’s health outcomes.
METHODS
Study design:
Our CAMS approach incorporated education for both the community pharmacy/patent proprietary medicine vendors and the pharmacy users. CFID and NCDC used both educational and health research initiatives to generate data that guided context-specific AMS models. Our innovative interventions adopted community and institutional system strengthening models through the identification and capacity building of community pharmacy/patent proprietary medicine vendors, key community-based organizations, and populations on AMR for effective AMS programming within community settings.
Patient-related factors also played an important role in the design of the intervention, such as self-medication and pressuring providers to prescribe antibiotics when not medically indicated. Our intervention empowered patients and caregivers in the appropriate use of antibiotics, aiming to preserve their effectiveness for as long as possible—for as many patients as possible.
Team Building on AMS in Community Settings:
The multifaceted nature of antimicrobial resistance and antimicrobial stewardship approaches required interdisciplinary and multi-stakeholder engagement to address the drivers of AMR in our communities in Nigeria.
Therefore, CFID worked with the Nigerian Centre for Disease Control (NCDC) as a core implementing partner on this project to build a consortium of partners to improve AMS in community settings in all target locations, building an AMS ecosystem and collaboration from state and non-state actors, including community groups across all target locations, in improving antibiotic appropriateness interventions in community settings across the 6 states in Nigeria.
This was a cross-sectional, interventional study undertaken across all the study locations in Taraba, Nasarawa, Rivers and Enugu states, Nigeria. Questionnaire scripted into ODK and research protocols were validated by subject experts for their content and relevance.
Study Population: The questionnaire (Patients Form A and B) were randomly distributed to the community pharmacists staff and Proprietary Medicine Vendors (PPMVs) staff, the staff further issued about 582 forms to patients in all the target states and communities.
Study procedure: A well-structured questionnaire scripted into ODK was administered by well-trained CPs/PPMVs, a qualitative research method that allowed collection of comprehensive data and deep exploration of views and experiences was used. Signed consent was obtained from the participating community members while confidentiality in data handling was assured and all relevant information was extracted and analyzed from the completed questionnaires (patient Forms A and B) via ODK
Statistical Analysis: Simple percentages and T-test were used for comparison of difference in means and a p-value less than 0.05 was considered as statistically significant
Selection of Community Pharmacists/Patent and Proprietary Medicine Vendors (PPMVs)
The selection of Community Pharmacists/Patent and Proprietary Medicine Vendors (PPMVs) for the study involved CFID, State ministries of Health, Association of Community Pharmacy of Nigeria (ACPN), PCN and NAPPMED to choose beneficiaries of the pilot interventions. CFID and NCDC obtained commitment from 10 community pharmacy/Patent and Proprietary Medicine Vendors (PPMVs) from each of the two local council areas in each state, making a total of 20 per state (120 in total across all 6 states) to pilot the Model for 6-month. CFID supported service providers to adopt the optimal method to increase patients’ knowledge by combining face-to-face education with the provision of a pictorial educational leaflet in all intervention pharmacy/PPMVs outlets. Staff of each outlet were supported through training to deliver on the following AMS services:
- The use of AMR Drug checklist/essential drug list (Antibiotic Checklist designed to follow the prescription’s journey and personalize the patient’s adherence advice).
- Patient AMS education to reduce consumption of antibiotics and improve treatment adherence.
- Health promotion and chronic disease management support within community settings.
- Improved safety netting procedures in all dispensing practices.
- Patient AMS scorecard and feedback on dispensed medications/antibiotics.
In states where CFID implemented the QI AMS Multi-Centre AMS study, the pilot pharmacy and patent and propriety medicine vendors (PPMVs) were linked to the hospital teams for peer leadership and learning for the duration through a “hub and spoke” model. In states where the AMS study was not available, the peer learning platform was between NCDC teams in each state to provide mentorship and supportive guidance on CAMS interventions.
Involvement of the general populations in the study to assess patient/care antibiotic knowledge and adherence behavior:
During the pilot study, the project obtained consent and enrolled 0ver 400 randomly selected general populations from each state (visiting any of the stores) in each location into the study cohort to assess outcomes of patient/carer antibiotic knowledge and adherence behavior education by Pharmacy/Patent and Proprietary Medicine Vendors (PPMVs) after each visit to the stores.
The community members were divided into two groups:
Intervention Group: The intervention group members were provided with patient education on AMR and were requested to fill in two feedback questionnaires during the visit to the store and after consultation by any staff:
1st knowledge-based questionnaire for AMR/AMS on the first visit to the pharmacy and after receiving dispensed medication.
2nd behavior-based questionnaire to be given to the patient and requested to delay filling until after completing medications or treatment regimen received from the store.
Closed Monitoring Group: Patients under the closed monitoring group were not provided with patient education; however, they were required to fill in the behavior-based feedback questionnaire after the completion of medication therapy after 10-14 days.
CFID or NCDC field staff were responsible for obtaining feedback and retrieving questionnaires for both groups for the behavior change questionnaire after the duration of therapy on antibiotic adherence or consumption. Study population confidentiality was maintained as no personal information was shared by the Pharmacy/Patent and Proprietary Medicine Vendors (PPMVs) or CFID.
Full Implementation of Promising CAMS Model Practices in Target States:
After the pilot phase and testing of interventions across all states, CAMS Models were implemented for a period of 8 months until the end of December 2023. Interventions were held in 3 states where CFID was currently implementing hospital-based QI AMS interventions, and the remaining 3 were in different geographic locations to scale and increase the reach of AMS interventions in Nigeria. CFID and the NCDC supported each AMS Model through trainings, ongoing measurement, and feedback. These elements all supported making changes that adopted system change that would be permanent and sustainable in all communities.
RESULTS
Figure 1: Distribution of Respondents Based on States
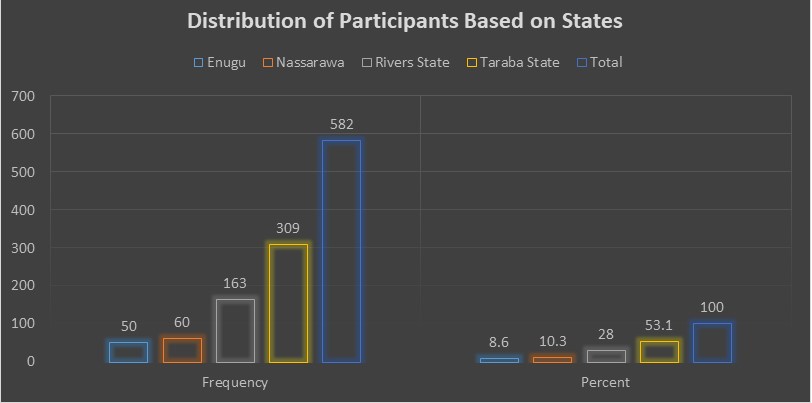
Figure 2: Distribution of Respondents Based on LGAs
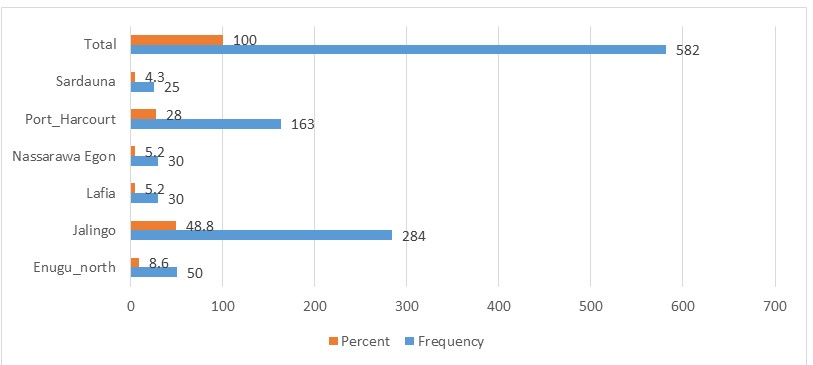
Figure 3: Distribution of Respondents Based on Groups
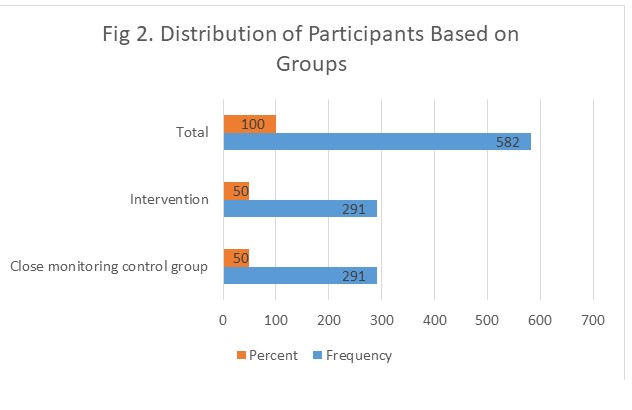
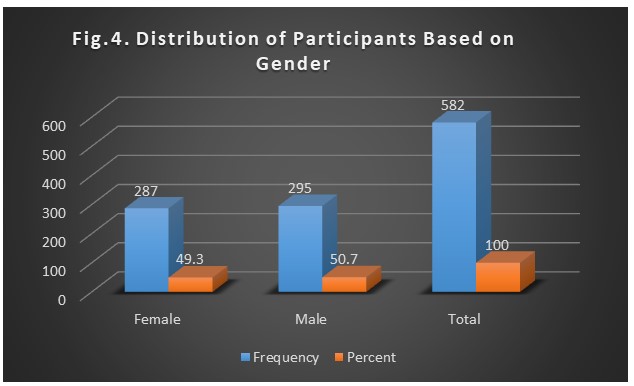
Table 1: For whom Antibiotics is Purchased?
| Frequency | Percent | ||
| Valid | Relative | 52 | 8.9 |
| My child | 70 | 12.0 | |
| Myself | 436 | 74.9 | |
| Others | 8 | 1.4 | |
| Prefer not to say | 16 | 2.7 | |
| Total | 582 | 100.0 | |
Table 2: Frequently Purchased Antibiotics from CPs/PPMVs
| Frequency | Percent | ||
| Valid | Amoxicillin | 261 | 44.8 |
| Clarithromycin | 11 | 1.9 | |
| Co_amoxiclav | 27 | 4.6 | |
| Doxycycline | 44 | 7.6 | |
| Flucloxacillin | 25 | 4.3 | |
| Metronidazole | 56 | 9.6 | |
| Nitrofurantoin | 16 | 2.7 | |
| Others | 120 | 20.6 | |
| Phenoxymethylpenincillin peni | 12 | 2.1 | |
| Trimethoprim | 10 | 1.7 | |
| Total | 582 | 100.0 | |
Table 3. Commonly Experienced side effect
| Frequency | Percent | ||
| Valid | abdominal_pain | 53 | 9.1 |
| all_of_the_above | 72 | 12.4 | |
| Diarrhea | 22 | 3.8 | |
| don_t_know | 77 | 13.2 | |
| nausea__feeling_like_you_may_vomit | 118 | 20.3 | |
| there_are_no_side_effects_from_antibioti | 201 | 34.5 | |
| Vomiting | 39 | 6.7 | |
| Total | 582 | 100.0 | |
Table 4: Following your Visit to the CPs/PPMVs what will be your actions on taking Antibiotics
| Group | Total | |||
| close_monitoring__control_group | Intervention | |||
| @_14_Following_your_v_o_you_
intend_to_take |
to_keep_antibiotics_for_future_illnesses | 14 | 0 | 14 |
| to_return_unused_antibiotics_to_the_cp_p | 14 | 20 | 34 | |
| to_share_antibiotics_with_friends__famil | 7 | 0 | 7 | |
| to_take_my_antibiotics_as_advised_by_my_ | 263 | 264 | 527 | |
| Total | 291 | 291 | 582 | |
Table 5. Distribution of participants full course of medication based on groups and Gender
| Group | @_5_Did_you_take_the_full_cours | Total | |||||
| i_can_t_remember | No | Yes | |||||
| close_monitoring_group | Gender | Female | Count | 82 | 70 | 152 | |
| % of Total | 28.2% | 24.1% | 52.2% | ||||
| Male | Count | 72 | 67 | 139 | |||
| % of Total | 24.7% | 23.0% | 47.8% | ||||
| Total | Count | 154 | 137 | 291 | |||
| % of Total | 52.9% | 47.1% | 100.0% | ||||
| intervention_group | Gender | Female | Count | 0 | 24 | 131 | 155 |
| % of Total | 0.0% | 8.2% | 45.0% | 53.3% | |||
| Male | Count | 2 | 13 | 121 | 136 | ||
| % of Total | 0.7% | 4.5% | 41.6% | 46.7% | |||
| Total | Count | 2 | 37 | 252 | 291 | ||
| % of Total | 0.7% | 12.7% | 86.6% | 100.0% | |||
| Total | Gender | female | Count | 0 | 106 | 201 | 307 |
| % of Total | 0.0% | 18.2% | 34.5% | 52.7% | |||
| Male | Count | 2 | 85 | 188 | 275 | ||
| % of Total | 0.3% | 14.6% | 32.3% | 47.3% | |||
| Total | Count | 2 | 191 | 389 | 582 | ||
| % of Total | 0.3% | 32.8% | 66.8% | 100.0% | |||
Table 6. Did you take the full course of your Antimicrobials?
| @_5_Did_you_take_the_full_cours | Total | |||||
| i_can_t_remember | no | Yes | ||||
| Group | close_monitoring_group | Count | 0 | 154 | 137 | 291 |
| % of Total | 0.0% | 26.5% | 23.5% | 50.0% | ||
| intervention_group | Count | 2 | 37 | 252 | 291 | |
| % of Total | 0.3% | 6.4% | 43.3% | 50.0% | ||
| Total | Count | 2 | 191 | 389 | 582 | |
| % of Total | 0.3% | 32.8% | 66.8% | 100.0% | ||
Table 6b. Chi-Square Tests of taking full course of medication based on Groups
| Value | Df | Asymp. Sig. (2-sided) | |
| Pearson Chi-Square | 107.668a | 2 | .000 |
Table 7. How_long_were_you asked to take antibiotics
| How_long_were_your_antibiot | Total | |||||||
| 3_days | 5_days | 7_days | i_don_t_know | others | ||||
| Group | close_monitoring_group | Count | 69 | 168 | 45 | 0 | 9 | 291 |
| % of Total | 11.9% | 28.9% | 7.7% | 0.0% | 1.5% | 50.0% | ||
| intervention_group | Count | 71 | 177 | 36 | 1 | 6 | 291 | |
| % of Total | 12.2% | 30.4% | 6.2% | 0.2% | 1.0% | 50.0% | ||
| Total | Count | 140 | 345 | 81 | 1 | 15 | 582 | |
| % of Total | 24.1% | 59.3% | 13.9% | 0.2% | 2.6% | 100.0% | ||
Table 8: Bivariate Analysis of Participants on sharing antibiotics with friends, family or pets
| Questions | Responses | Close Monitoring Group | Intervention Group | Total | p-value | |
| Would you share antibiotics with your friends, family or pets?/ Yes, if my friends or family are sicker than me | No | Count | 225 | 274 | 499 | 0.00021 |
| % of Total | 38.7% | 47.1% | 85.7% | |||
| Yes | Count | 66 | 17 | 83 | ||
| % of Total | 11.3% | 2.9% | 14.3% | |||
| Count | 291 | 291 | 582 | |||
| % of Total | 50.0% | 50.0% | 100.0% | |||
| Would you share antibiotics with your friends, family or pets?/ Yes, if my friends or family have similar symptoms to me | No | Count | 157 | 266 | 423 | 0.0023 |
| % of Total | 27.0% | 45.7% | 72.7% | |||
| Yes | Count | 134 | 25 | 159 | ||
| % of Total | 23.0% | 4.3% | 27.3% | |||
| Count | 291 | 291 | 582 | |||
| % of Total | 50.0% | 50.0% | 100.0% | |||
| Would you share antibiotics with your friends, family or pets?/ Yes, if I have any leftover | No | Count | 240 | 277 | 517 | 0.00010 |
| % of Total | 41.2% | 47.6% | 88.8% | |||
| Yes | Count | 51 | 14 | 65 | ||
| % of Total | 8.8% | 2.4% | 11.2% | |||
| Count | 291 | 291 | 582 | |||
| % of Total | 50.0% | 50.0% | 100.0% | |||
| Would you share antibiotics with your friends, family or pets?/ Yes, I would give my antibiotics to my pets | No | Count | 240 | 289 | 529 | 0.000 |
| % of Total | 41.2% | 49.7% | 90.9% | |||
| Yes | Count | 51 | 2 | 53 | ||
| % of Total | 8.8% | 0.3% | 9.1% | |||
| Total | Count | 291 | 291 | 582 | ||
| % of Total | 50.0% | 50.0% | 100.0% | |||
| Would you share antibiotics with your friends, family or pets?/ Yes, I would give my antibiotics to my pets | No | Count | 140 | 237 | 377 | 0.000 |
| % of Total | 24.1% | 40.7% | 64.8% | |||
| Yes | Count | 151 | 54 | 205 | ||
| % of Total | 25.9% | 9.3% | 35.2% | |||
| Total | Count | 291 | 291 | 582 | ||
| % of Total | 50.0% | 50.0% | 100.0% |
Description of Results
In Figure 1, the distribution of respondents based on states indicates that 8.6% of the patients populations were sampled from Enugu, 10.3% from Nassarawa, 28.0% from Rivers State, and the majority, accounting for 53.1%, are from Taraba State, summing up to a total of 582 respondents. Results in Figure 2, revealed the distribution of respondents based on LGAs results shows that 8.6% are from Enugu North, 48.8% from Jalingo, 5.2% from Lafia, 5.2% from Nassarawa Egon, 28.0% from Port Harcourt, and 4.3% from Sardauna, making a total of 582 respondents.
Fig. 3 delineates the distribution of respondents based on groups, with 50.0% each for the Close Monitoring Control Group and the Intervention group, amounting to a total of 582 respondents. Fig. 3, revealed the distribution of respondents across states based on gender and the result shows that 49.3% are female, 50.7% are male, constituting the entire set of 582 respondents.
Table 1, elucidates the purpose for which antibiotics are purchased, 8.9% acquire them for relatives, 12.0% for their children, 74.9% for themselves, 1.4% for others, and 2.7% prefer not to disclose, with the table accounting for a total of 582 respondents.
Table 2 gives details on the frequently purchased antibiotics from CPs/PPMVs, Amoxicillin stands out at 44.8%, with various percentages allocated to Clarithromycin, Co_amoxiclav, Doxycycline, Flucloxacillin, Metronidazole, Nitrofurantoin, Phenoxymethylpenincillin__peni, Trimethoprim, while 20.6% opt for other antibiotics which included A.c.t, Acycor plus, Albendazole, Amoxicillin, Ampiclox (caps), Ampicloxacillin, Aqumentine, Augmentin, Azithromycin tablets, Ceberiaxone, Cefixime suspension, Ceftriaxone, Certrezol, Ciprofloxacin, Ciprofloxacin Hydrochloride, Clindamycin, Erythromycin, Ethiclav, Fluconazole, Gentamicin, Levofloxacin, Lincomycin, Metronidazole, Mirafix Cefixine, Norfloxacin, Ofloxacin, P.alaxin, Tab Azithromycin 500mg, Tab Ciprofloxacin 500mg, Tetracycline and Tinidazole.
Table 3: Following your Visit to the CPs/PPMVs, what will be your actions on taking Antibiotics
This table provides insights into respondents’ intended actions after visiting CPs/PPMVs, distinguishing between the Close Monitoring Control Group and the Intervention Group. In the Close Monitoring Control Group, 14 respondents intend to keep antibiotics for future illnesses, 14 plan to return unused antibiotics to the CP/PPMVs, 7 contemplate sharing antibiotics with friends or family, and 263 express their commitment to taking antibiotics as advised. For the Intervention Group, 20 individuals plan to return unused antibiotics to the CP/PPMVs, and 264 indicate their intention to take antibiotics as advised.
Table 4 -6: Did you take the full course of your Antimicrobials?
This table further explores whether participants took the full course of antimicrobials, categorized by group. In the Close Monitoring Control Group, 154 respondents did not take the full course, 137 completed the full course, while in the Intervention Group, 37 did not take the full course, and 252 completed the full course. The total distribution indicates that out of 191 respondents who did not take the full course, 106 are females and 85 are males, while out of 389 who completed the full course, 201 are females, and 188 are males. This result was supported by Chi-Square test showing a statistically significant association between taking the full course of medication and the two groups (Close Monitoring Control Group and the Intervention Group).
Table 7: How long were you asked to take antibiotics?
This table provides the distribution of respondents based on the duration for which they were instructed to take antibiotics. In the Close Monitoring Control Group, 168 respondents were instructed to take antibiotics for 5 days, while 177 in the Intervention Group received the same instruction. The total distribution indicates that out of 345 respondents instructed to take antibiotics for 5 days, 106 are females, and 85 are males.
Furthermore, Table 8 presents the outcomes of a bivariate analysis investigating participants’ willingness to share antibiotics in different scenarios, with a focus on responses from the Close Monitoring Group and the Intervention Group. The analysis considers situations such as sharing when others are sicker, experiencing similar symptoms, having leftovers, or giving antibiotics to pets. A statistically significance association was observed in all scenarios, indicating the differences between the two groups (intervention and close monitoring). Overall, the results highlight varied attitudes towards antibiotic sharing, offering clear understanding into the potential impact of CFID outpatient setting CAMS intervention on participants’ perspectives (Intervention group).
Following visitation to CPs/PPMVs, the following information were Obtained from patients
A very unique arrangement for easy check and drug choice from the counter was observed by many patients who accessed the intervention stores some of which include: antibiotics checklist, posters, and other materials used in the community were found to be very useful. Some customers initially expressed frustration with Pharmacy/Patent Proprietary Medicine Vendors (PPMVs) when denied specific medications, only later realizing that the medications belonged to the antibiotic class. The intervention aimed to empower patients and caregivers in the appropriate use of antibiotics. The team built awareness of antimicrobial stewardship in community settings, involving interdisciplinary and multi-stakeholder engagement.
The implementation of CAMS models across all states involved ongoing measurement, feedback, and training to make changes that adopted a system change permanently. The sustainability plan included creating AMS communities of practice, enhancing local expertise, and integrating CAMS interventions into Nigeria’s AMR Strategic Plan. The CAMS approach incorporated education for both PPMVs and pharmacy users.
Feedback from community members revealed improved knowledge of antibiotics, satisfaction with services, and increased awareness due to the campaign. The initiative received positive responses, with participants expressing gratitude for the enlightening program and committing to responsible antibiotic use. Some suggestions included more awareness through posters, stickers, radio, and extending the campaign to rural areas. Overall, the program contributed to public education and awareness of the use and importance of antibiotics in treatment processes.
DISCUSSION OF RESULTS
The results presented in the tables provide a comprehensive overview of the distribution of respondents and their behaviors concerning antibiotic use across various states, local government areas (LGAs), gender, and groups. In Figure 1, it is evident that the majority of respondents were from Taraba State, comprising 53.1% of the total sample, indicating a substantial representation from this region. Similarly, Fig 2 breaks down the distribution of respondents based on LGAs, with Jalingo having the highest percentage at 48.8%, followed by Port Harcourt at 28.0%.
Fig. 3 highlights an equal distribution of respondents between the Close Monitoring Control Group and the Intervention Group, indicating a balanced representation in the study. The gender distribution in Fig. 3 reveals almost an equal split, with 49.3% females and 50.7% males, ensuring a diverse sample for analysis. Table 1 delves into the purpose for which antibiotics are purchased, revealing that the majority (74.9%) acquire antibiotics for themselves, emphasizing self-medication practices.
The details on frequently purchased antibiotics in Table 2 show Amoxicillin as the most commonly acquired antibiotic at 44.8%, with various other antibiotics contributing to the overall antibiotic usage pattern. Table 3 sheds light on the intended actions of respondents following their visits to CPs/PPMVs, indicating a significant commitment to taking antibiotics as advised, particularly in the Intervention Group.
Tables 4 and 6 provide a nuanced analysis of participants’ completion of the full course of antimicrobials, showcasing the distribution across gender and groups. The Chi-Square test in Table 8 underlines a statistically significant association between completing the full course of medication and the two groups.
Table 9 further explores the duration for which respondents were instructed to take antibiotics, revealing that a significant number were instructed to take antibiotics for 5 days, highlighting a common prescription duration in the sample.
Overall, the results suggest diverse patterns in antibiotic acquisition, usage, and adherence to prescribed courses, with notable variations across different demographic and intervention groups. The feedback and responses from community members emphasize the positive impact of the CAMS program on knowledge, awareness, and responsible antibiotic use, indicating a successful initiative that contributes to public education and awareness.
CONCLUSION
This interventional study sought to assess the impact of CFID CAMS intervention between two groups (close monitoring and intervention groups) across 24 urban and rural communities in Nigeria. Findings across communities of interest effectively demonstrated the tangible impact of the CAMS intervention on the two distinct groups. Specifically, the Intervention Group, which exhibited significant advancements in the dispensing/prudent use of antibiotics and adherence to follow-up prescription advice.
The data further shows the correlation between completing the full antibiotic course of medication among the intervention group and close monitoring group.
This results, emphasizing discernible differences between the two groups, suggest that the CFID’s CAMS intervention in Nigeria had a notable effect, particularly within the Intervention Group.
The relevance of the CAMS intervention extended beyond urban settings to encompass rural communities in Nigeria. The results emphasized that patients within the intervention group, regardless of their location, displayed a higher level of awareness concerning the importance presenting drugs prescription to Community Pharmacists/PPMVs and rational use of Antimicrobials. Patients within the intervention group received essential guidance on antibiotic usage, contrasting starkly with the closely monitored group.
In essence, the findings from this highlight its effectiveness across diverse settings, emphasizing the crucial role of AMS in improving antibiotic-related practices in both urban and rural communities in Nigeria.
RECOMMENDATION
Based on the conclusion of the study, CFID/NCDC proposed the following recommendation which is believed to have a substantial opportunity to sustain and amplify the positive impact observed in the CAMS intervention and ultimately contributing to improved antibiotic-related practices in diverse healthcare settings across Nigeria.
Promotion and Expansion of CAMS Intervention
Given the tangible impact observed in both urban and rural communities, it is recommended that the CAMS intervention be further promoted and expanded across Nigeria. This can be achieved through collaboration with healthcare stakeholders, governmental bodies, and community leaders to ensure widespread implementation and awareness.
Training for Healthcare Providers
Considering the notable advancements in the prudent use of antibiotics and adherence to follow-up prescription advice within the Intervention Group, there is a need for comprehensive training programs for healthcare providers, especially Community Pharmacists/Primary Health Care Providers (CPs/PPVs). This training should focus on the importance of providing guidance on antibiotic usage and encouraging the rational dispensing of antimicrobials.
Community Education and Awareness
Implementing awareness campaigns within communities is crucial to ensuring that patients are well-informed about the importance of presenting drug prescriptions to Community Pharmacists/PPMVs and practicing rational use of antimicrobials. This can be achieved through informational sessions, pamphlets, and other educational materials distributed in both urban and rural areas.
Monitoring and Evaluation
Establishing a robust monitoring and evaluation framework is essential to track the ongoing impact of the CAMS intervention. Regular assessments should be conducted to measure the adherence to recommended practices and identify areas for improvement. This will contribute to the continuous enhancement of the intervention’s effectiveness.
Policy Integration
Advocacy efforts should be directed towards integrating the CAMS intervention findings and principles into national and regional healthcare policies. This integration will ensure sustained support, resource allocation, and institutionalization of practices that promote rational antibiotic use.
Research and Adaptation
Continuous research efforts should be encouraged to adapt the CAMS intervention to evolving healthcare landscapes. Tailoring the intervention based on new research findings will enhance its applicability and effectiveness in addressing emerging challenges related to antibiotic use.
Collaboration with CPs/PPMVs
Strengthening collaboration with Community Pharmacists/PPMVs is critical. Providing ongoing support, resources, and training to these healthcare providers will empower them to play a pivotal role in guiding patients on antibiotic usage and promoting rational dispensing practices.
FUNDING
Financial support for this study was provided by Pfizer Independent Quality Improvement grant to Centre for Initiative and Development (CFID) NGO in Nigeria. Pfizer had no role in the study design or data collection, analysis, or interpretation. The authors have access to all study data and have final responsibility for the writing and decision to submit for publication.
ACKNOWLEDGMENT
The authors acknowledge all recruited CSOs, Communities and states of interest who actively participated in CAMS project activities.
Ethics approval and consent to participate
Ethics approval was received from the National Health Research Ethics Committee with NHREC Protocol Number: NHREC/01/01/2007-01/11/2021 and NHREC Approval Number NHREC/01/01/2007- 22/11/2022B. Informed consent was obtained from each participants prior to the observation of any consultations. Consent was also obtained from Ministries of Health and Education in all the six target states
REFERENCE
- Allison, R., Chapman, S., Howard, P., Thornley, T., Ashiru-Oredope, D., Walker, S., Jones, L. F., & McNulty, C. A. M. (2020). Feasibility of a community pharmacy antimicrobial stewardship intervention (PAMSI): an innovative approach to improve patients’ understanding of their antibiotics. JAC-antimicrobial resistance, 2(4), dlaa089. https://doi.org/10.1093/jacamr/dlaa089
- WHO Africa-Nigeria, (2021). Experts caution Nigerians against indiscriminate use of antibiotics to reduce future health crisis, available at: https://www.afro.who.int/news/experts-caution-nigerians-against-indiscriminate-use-antibiotics-reduce-future-health-crisis#:~:text=The%20National%20Action%20Plan%20for,used%20antibiotics%20following%20the%20 prescription.Accessedon 8/12/2023
- Federal Ministries of Agriculture H and E. Antimicrobial Use and Resistance in Nigeria: Situation Analysis and Recommendations. 2017; 158.
- Okoro RN, Nmeka C, Erah PO. Antibiotics prescription pattern and determinants of utilization in the national health insurance scheme at a Tertiary Hospital in Nigeria. Afr Health Sci. 2019;19:2356–2364. doi: 10.4314/ahs.v19i3.8. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Antimicrobial resistance, https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance; 2021. Accessed 8 December 2023.
- Isah, A., Aina, A. B., Ben-Umeh, K. C., Onyekwum, C. A., Egbuemike, C. C., Ezechukwu, C. V., Umoru, D. O., & Nechi, R. N. (2023). Assessment of public knowledge and attitude toward antibiotics use and resistance: a community pharmacy-based survey. Journal of pharmaceutical policy and practice, 16(1), 107. https://doi.org/10.1186/s40545-023-00619-z
- ADDA et al. (2023). Community knowledge and practices regarding antibiotic use Across Five States in Nigeria, International Journal of Research and Innovation in Applied Science (IJRIAS) volume-7-issue-8, pp.37-42
- ADDA et al. (2023). Antimicrobial Prescription Habits among Community Pharmacists and PPMVs in Nigeria: A Rational Use of Drugs Survey” International Journal of Research and Innovation in Applied Science (IJRIAS) volume-7-issue-8, pp.10–17
- ADDA et al. (2022). A Multi-Center Study to Measure the Performance of Antimicrobial Stewardship in 14 Hospitals Across Nigeria: Needs Assessment, International Journal of Research and Innovation in Applied Science (IJRIAS) volume-7-issue-8, pp.32-36. DOI: https://dx.doi.org/10.51584/IJRIAS.2022.7804
- ADDA et al. (2022). Implementing Antimicrobial Stewardship Program in Pediatrics Across Six Hospitals in Six States in Nigeria: Needs Assessment, International Journal of Research and Innovation in Applied Science (IJRIAS) volume-7-issue-8, pp.37-42 DOI: https://dx.doi.org/10.51584/IJRIAS.2022.7805
- AlAhmad, M. M., Rabbani, S. A., Al-Salman, R., Alameri, H., Al Namer, Y., & Jaber, A. A. S. (2023). Antimicrobial Stewardship Practices of Community Pharmacists in United Arab Emirates. Antibiotics (Basel, Switzerland), 12(8), 1238. https://doi.org/10.3390/antibiotics12081238