
Assessment of Health Status Using Anthropometric Studies of Persons Occupationally Exposed to Oil Spillage in Bodo, Gokana Local Government Area, Rivers State, Nigeria.
- Onyetem, M.S.
- Onyeneke, E.C.
- 827-836
- Mar 18, 2025
- Health
Assessment of Health Status Using Anthropometric Studies of Persons Occupationally Exposed to Oil Spillage in Bodo, Gokana Local Government Area, Rivers State, Nigeria.
Onyetem, M.S.* and Onyeneke, E.C.
Department of Biochemistry, Faculty of life sciences, University of Benin, Benin City, Edo State, Nigeria.
*Corresponding Author
DOI: https://doi.org/10.51244/IJRSI.2025.12020064
Received: 09 February 2025; Accepted: 13 February 2025; Published: 18 March 2025
ABSTRACT
Oil spillage poses significant public health challenges, particularly in regions like Bodo, where occupational exposure to such spills is prevalent. This research investigates the health status of individuals occupationally exposed to oil spillage in Bodo, Gokana Local Government area, Rivers State. A total of 93 respondents were enrolled using multistage random sampling techniques. Anthropometric measurements used from the respondents show the population by gender, age, and physical health parameters: height, weight, and BMI. Health challenges: cardiovascular, kidney, respiratory, diabetes, and blood pressure in relation to occupations. Data were analyzed and mean percentage distribution was statistically computed. The study revealed a prevalence of cardiovascular (43.6%), kidney (0.0%), respiratory (2.6%) and diabetes (53.8%) complications. These health defects might be due to the crude oil contaminations in the community. This calls for an urgent need for effective reduction strategies to alleviate the impact of oil spillage in Bodo.
Keywords: Oil spillage, Anthropometric studies, Health challenges, Percentage distribution
INTRODUCTION
In the heartland of the Niger Delta region of Nigeria, Bodo, Gokana Local Government Area, has become a microcosm of the worldwide conundrum posed by oil spillage. This region, rich in crude oil reserves, has both witness to the economic benefits and environmental costs of oil extraction. The people of Bodo have for long time, been intimately connected with the rhythms of the Niger Delta, their livelihoods intricately linked with the waterways and terrestrial ecosystems that have nourished their communities. However, this once harmonious relationship has been profoundly disrupted by the specter of oil spillage.
Heavy metal and PAHs are known to affect nearly every organ system in the body [1], including the nervous, respiratory, excretory, and cardiovascular systems [2]. Further, lead, chronium, and cadnium have been suggested as a potential carcinogen, particularly for breast, gastrointestinal, ovarian, skin, and brain cancers [3]. With growing industrialization and vulnerable occupational communities, exposure to heavy metals is an ongoing problem worldwide. Environmental contaminants generated from oil spillage coupled with anthropogenic activities such as oil exploration and urbanization can cumulate in environmental disasters, such as oil spills, can have a significant impact ecologically. The Bodo Community located within the Niger Delta region of Nigeria is one of such area; the United States Department of Energy estimates that well over 4,000 oil spills have occurred in the Niger Delta in the past 5 decades [4], [5], [6], [7]. Study investigating heavy metal concentrations of fish in Bodo City found elevated levels of lead, cadmium, manganese and iron which were 2–4 fold higher than the World Health Organization (WHO) permissible levels for human consumption of 0.3, 0.01, 5.0, and 0.3 mg/kg respectively [6], [8]. These exposure levels are likely a direct result of exposures to crude oil spillage from the environmental disasters the community has experienced and would be related to increased risks for many diseases previously associated with heavy metal exposures [6].
Crude oil is a mixture of several chemicals, including polycyclic aromatic hydrocarbons (PAH), and volatile organic compounds (VOC) like benzene, toluene, anthracene and xylene. Exposure to PAH be believed to be capable of causing respiratory diseases, diabetes and other health challenges [9]. The oil spills in Bodo have led to severe environmental degradation, loss of livelihood, and increased health risks for the local population. The exposure to the toxic chemicals presents in the oil spills can lead to respiratory problems, skin irritation and pollution including other health challenges [10]. The effects of the oil spills in Bodo City have been devastating and long-lasting, with the community suffering the consequences for years. The situation highlights the need for research, development of policies and stricter regulations on oil exploration and production, as well as better emergency response plans in the event of an oil spill [11]. A study of population health on contaminated area is necessary to better understand the anthropometric survey that are related to liver, kidney, cardiac function and overall health status [12]. Hematological and renal functions have been shown to remain altered, over time following exposures to oil spills [13], [14]. Exposure to crude oil and its derivatives also generates kidney damage [14], [15]. Therefore, we consider it important to evaluate the anthropometric parameters of persons living in Bodo community who are exposed to different levels of risks due to crude oil contamination.
MATERIALS AND METHODS
Area of Study
The study area is Bodo community located in southeast region of Rivers State, Nigeria, a rural community occupying latitude 4o 36’N and longitude 7o21’E. Bodo is bordered by the Gokana communities of Kpor, Mogho, and Gbe on the North and Andoni people of Rivers State. The community is made up of 24 villages and it is one of the state’s largest zones and commercial areas. (Figure 1) In Bodo, oil spillage occurs on the sea and soil surface directly, during precipitation, runoffs; contaminants may leach out into the groundwater bodies. The climate of the area is a tropical wet and dry climate according to the Koppen-Geiger system of climate classification, with two seasons (the wet season—April to October) and (the dry season —November to March). Average annual temperature for Bodo is 25.9oC – 34oC. The drinking water in the study area is supplied mainly from their rivers. The sea, land and the rivers played a significant part in the development of the community because their major occupation is fishing and farming. It is estimated that Bodo city occupies a landmass of approximately one hundred thousand hectares. Mangrove swamps, some island forests, and brackish water creeks occupy over 65% of the community [16].
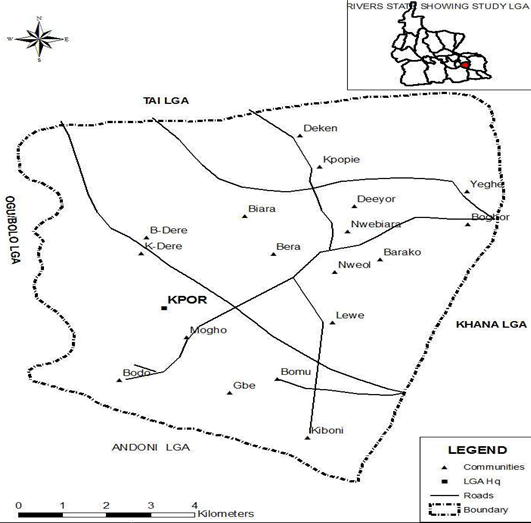
Fig 1: Bodo and environ
Source: Rivers State Ministry of land and Survey
Questionnaire administration
Following informed consent obtained from all willing participants, a well-structured questionnaire was administered to ninety-three selected individuals in the study area, to obtain demographics and general information on the impact of oil spillage on their health status. The questionnaires were administered to randomly selected respondents domiciled in the community. A sample of the questionnaire is included as supplementary data.
RESULTS AND DISCUSSIONS
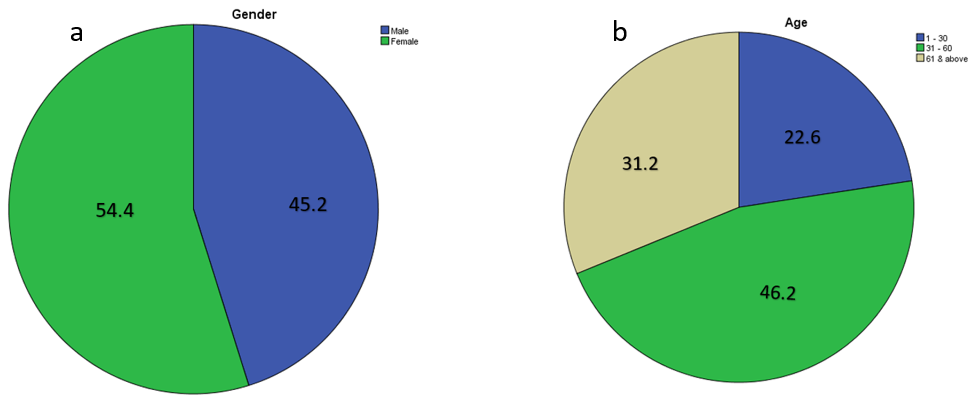
Figure 2: Mean percentage distribution of Bodo population by age and gender
The mean percentage distribution of the Bodo population by gender (Figure 2a), age (Figure 2b), education (Figure 3a,b,c), marital status, the number of years living or working in Bodo, physical health parameters (BMI) (figure 5), health challenges (cardiovascular, kidney, respiratory, diabetes and blood pressure) (Figure 4) and occupation are shown in Figure 4c. Most respondents within Bodo were males 54.4%, while the females constituted 45.2% of the population. The majority of respondents were between the ages of 31–60 years (figure 2b), with a mean percentage distribution of 46.2%. This was closely followed by the 61 & above age range (31.2%) and 1-30 years (22.6%) to which adolescents belong. The age bracket with the least number of respondents was1-30 years. Considering the generally recognized age of an adult at 21 years, it implies that 89.2% of the population sampled was adults, while 10.8% were adolescents. A limitation of the study was that infants could not be included in the questionnaire survey due to their young age. The survey shows that most of the respondents sampled (61.3%) had stay in the Bodo for more than 20 years while (36.6%) had stayed for 10-20 years and only (2.2%) had live for 1 -10 years. Figure 3c shows the occupation (civil servant, business owners, farmers, fishermen/women, students & others) of which fishing and farming shows the highest respondents with 21.5% and 43.0% respectively while students revealed the least of 1.1%. however, the mean distribution for occupation shows that 93.5% respondents had lived and worked in Bodo.
The mean percentage distribution of male relative to health problems shows 26.6%, 5.9% & 76.5% had health challenges with cardiovascular, respiratory and diabetes respectively. While female relative to health problems shows 61.4%, 2.3% & 36.4% had health problems with cardiovascular, respiratory and diabetes respectively, which depicts that highest respondent of males have challenges with diabetes and highest respondents of females had issues with cardiovascular diseases. However, the health challenges cross tabulated with duration of stay indicates that 10-20 years and 21 years and above with mean percentage distribution 68.0%, 4.0%, 28.0% and 32.1%, 1.9%, 66.0% had problems with cardiovascular, respiratory and diabetes respectively. In the same vein, the studies show farmers having highest with cardiovascular diseases (67.2%) followed by fishermen/women having highest in diabetes (33.3%) with regards to the occupations of the respondents. The results also show those that have being in Bodo for 21 years and above having high blood pressure (51.8%) with farmers (47.4%) and fishermen/women (28.9%) showing signs of high blood pressure (figure 5a&c).
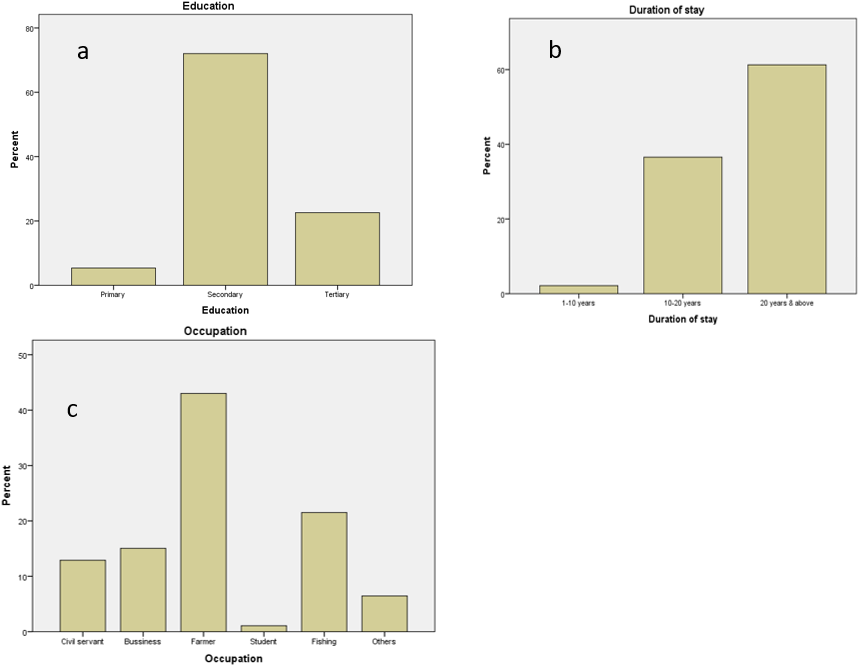
Figure 3: Mean percentage distribution of Bodo population by education, duration of stay and occupation
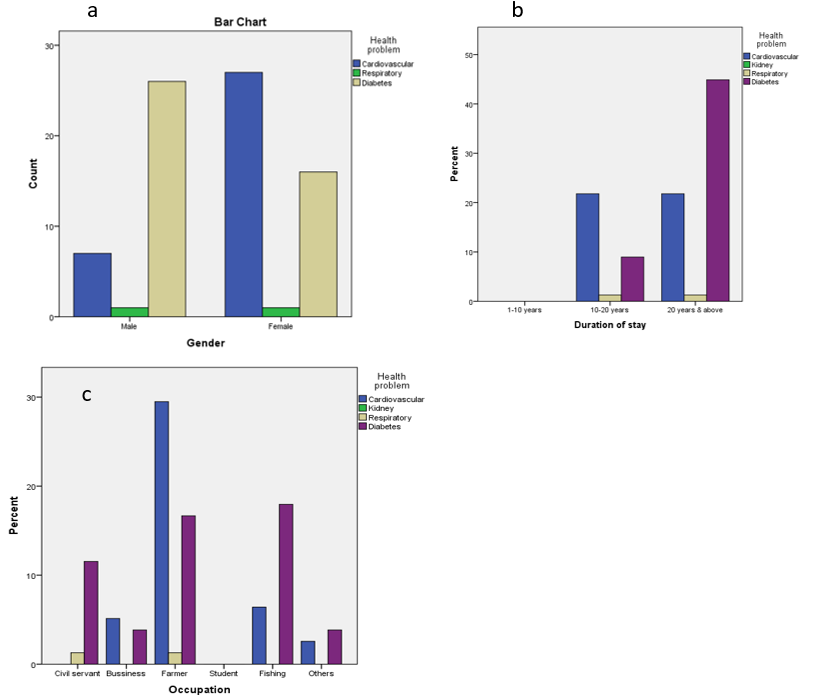
Figure 4: Mean percentage distribution of Bodo population by occupation and duration of stay relative to health challenges and gender.
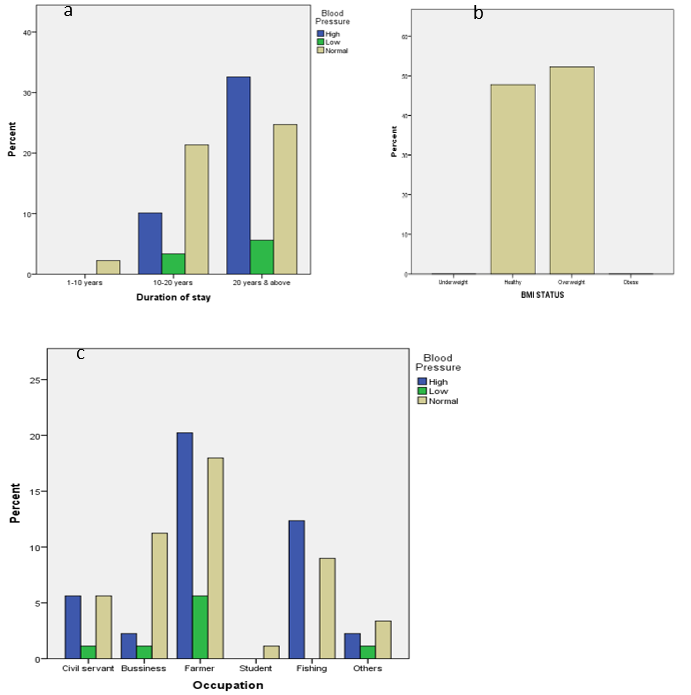
Figure 5: Mean percentage distribution of Bodo population by occupation and stay relative to blood pressure and BMI status.
The results obtain from this study is consistent with Van Sprang and Colin [17] as regards to effects of heavy metals from crude oil spills. The most potentially harmful of these heavy metals are lead, mercury, cadmium etc. Studies on heavy metal levels in water and sediment of coastal waters have been a major environmental focus especially in the last decades [18], [19]. The kidney is the critical organ of intoxication following long-term exposure to cadmium, and some studies suggest that at moderate exposure of cadmium may exacerbate the agE – related decline in renal function [20]. In humans and other mammals, cadmium exposure can also result in a variety of adverse effects including, pulmonary edema and hepatic dysfunction [21], [22] showed that the pulmonary function of the respondents in the oil-spilled community were lower. In work by Ovuakporaye et al [23] conducted in six gas flared and non-gas flared communities in the Niger Delta region, it was argued that gas flaring increases blood pressure of residents in gas flaring communities but decreases the lung functions of the occupants. Other researches have reported that the lung functions of residents in oil-spilled communities were lower than those in communities not affected by oil-spillage and gas-flaring [23], [24]. The likely explanation for the differences could be environmental factors such as those associated with crude oil contaminated waters and crops. The study by Ovuakporaye et al [23] concluded that the pulmonary functions of children in a non-gas flaring community were higher than those in the flaring communities. These results corroborated with 43.6% of cardiovascular complications from this study and other previous studies [25], [26]. Nickel generated from oil spillage is potentially toxic to human health [27]. The contact with contaminants generated by the oil spill have been attributed to the symptoms of cardiovascular and perhaps kidney diseases and even occupational injuries [28]. The most chronic toxicity affects the kidneys, cardiovascular organ and lungs as presents mainly in post‑menopausal women as “Itai‑Itai” disease with severe renal [28].
Atmospheric mercury from crude oil spills deposit straight into water, wherever it can be washed into bodies of water is rapidly incorporated into aquatic ecosystems and food webs [29]. The gastrointestinal area absorbs about 95% of ingested methyl mercury wherever it may be able then come in the red blood cells and the brain through binding covalently toward glutathione and cysteine protein group [30]. Inhale mercury vapor simply cross the pulmonary alveolar membranes to come in the circulatory system, wherever it invades primarily red blood cells and the kidneys [31]. Cobalt is seen to cause cardio myopathy [32], the report agrees with this study of 43.6% cardiovascular complications. Meo et al. [33] investigated lung function directly following oil spill exposures. Compared to controls, oil spill workers initially had lower lung functions, they exhibited better lungs function measures 1 year later. Studies on fishermen, following the Prestige oil spill after follow-up shows adverse respiratory symptoms persisted [34]. Findings are also consistent with analyses from this study of 2.6% respiratory complications of Bodo occupants and other researchers also revealed that workers exposures to oil spillage shows decline in functions of lungs [35]. and undesirable physiological responses [36], [37], [38].
Cadmium has been reported to accumulate primarily in the liver and kidney because these organs are rich in metallothionein [39]. Cadmium toxicity of the kidney has been associated with the impairment of renal tubular and glomerular functions [40]. This may account for the elevated levels of urea and creatinine in the plasma of cadmium-exposed rats [41]. In renal cells, lead binds to several proteins, where some have been associated in lead toxicity [3].
The accumulation of vast numbers of spilled crude related substances associated with crude exploitation and spillage are major sources of petrogenic PAHs [42]. Polycyclic aromatic hydrocarbons (PAHs) concentrations can be potentially toxic and dangerous when they cross the food chain into the biological system. PAHs are classified as environmentally hazardous pollutants due to their known hydrophobic, mutagenic, and carcinogenic characteristics [43]. However, crude oil generally pollutes both surface and groundwater with benzene as well as other toxic PAHs [44]. The environmental health consequences are far reaching, particularly in most areas of the Niger Delta where residents are dependent on very shallow wells [45]. This implies that Bodo, will continue to experience diverse range of illnesses arising from exposure to oil pollution [46]. Type 1 diabetes (T1D) is an autoimmune disease mediated by the destruction of insulin-secreting pancreatic β cells [47]. Exposure to anthracene, an individual PAH, was recently considered to be one of the factors that increase TID [48]. O’Driscoll concluded in his review that particulate matters exposure may upregulate the incidence of T1D in children and worsens diabetes in adults [49] which agrees with this study of 53.8% diabetic respondents. Jardel et al., [50] showed an apparent exposure-response relationship of increasing diabetes incidence with increasing maximum crude oil exposure level, which appeared stronger among males. Additionally, there was a significant exposure-response relationship among overweight participants, but not among obese participants which correlated with this study. Research shows increase exposure to PAHs from oil spillage is a strong indication of myocardial infarction. This is similar to the finding of Wedemeyer et al., [50], where alterations in the level of plasma enzymes, which have been exposed to the lowest concentration of stressors, showed the highest effect. A related work has been recorded by Begum [51], where fresh water fish was exposed to crude oil products. There are several reports on changes in cells, tissues and organs of fish for alteration of plasma enzyme activities [51], [52].
According to official statistics, 28% of all major crude oil spillage in Nigeria are due to sabotage [46] Therefore probabilities are that the respondents in the exposed communities might amplify the health effects to attract compensations. This study was however able to handle this possible partiality through the use of focus group discussions for data collection, that started only after the relationships between cause and effects were clearly established.
CONCLUSION
Exposure to the heavy metals and PAHs generated from crude oil spill can generate some acute health effects, albeit mild and transient. This disease burden of the exposed communities should be recognized and given adequate attention by all the stakeholders to alleviate the impact of oil spillage in the exposed population.
REFERENCE
- Caito, S. and Aschner, M. (2011). Neurotoxicity of metals. Handbook of Clinical Neurology. 131:169–89.
- Nigra, A., Ruiz-Hernandez, A., Redon, J., Navas-Acien, A. and Tellez-Plaza, M. (2016). Environmental metals and cardiovascular diseases in adults: a systemic review beyond lead and cadmium. Current environmental health reports. 3: 416-433.
- Agency for Toxic Substances and Disease Registry (2007). Toxicological Profile for Lead, US Department of Health and Human Services, Atlanta.
- Boele, R.,Fabig, P. and Wheeler, D. (2001). Shell, Nigeria and the Ogoni. A study in unsustainable development: I. The story of Shell, Nigeria and the Ogoni people – environment, economy, relationships: conflict and prospects for resolution1, Sustainable Development. 9:74–86.
- Osuyi, L.C. and Adesiyan, S.O. (2005). The Isiokpo oil pipeline leakage. Total organic carbon/organic matter contents of affected soils. Chemistry and Biodiversity. 2: 1097-1085.
- Nkpaa, K., Wegwu, M. and Essien, B. (2013). Heavy metals concentrations in four selected seafood from crude oil polluted waters of Ogoniland, Rivers State, Nigeria. Archives of Applied Science Research.5: 97–104.
- Nwaichi, O., Wegwu, M. and Nwosu, U. (2014). Distribution of selected carcinogenic hydrocarbon and heavy metals in an oil-polluted agriculture zone. Environmental Monitoring and Assessment. 186:8697-8706.
- World Health Organization, (1984). Guidelines for Drinking Water Quality; Health criteria and information.
- Bosch, X. (2003). Exposure to oil spill has detrimental effect on clean-up workers’ health. Medicine and Health Policy. 361: 140-147.
- Kponee, Z., Andrea C., Kakulu, I., Donna, V. and Wendy H. (2015). Petroleum contaminated water and healthsymptoms: a cross-sectional pilot study in arural Nigerian community. Environmental Health. 14: 50 – 86.
- Zabbey, N., Sam, K. and Onyebuchi, A. (2017). Remediation of contaminated lands in the Niger Delta, Nigeria: Prospects and challenges. Science of Total Environment. 2: 1-75.
- Coronel Vargas, G. Au, W. and Izzotti, A. (2020). Public health issues from crude-oil production in the Ecuadorian Amazon territories. Science of the Total Environment. 719: 134 – 147.
- D’Andrea, M. and Reddy, G. (2018). The development of long-term adverse health effects in oil spill cleanup workers of the Deepwater Horizon offshore drilling rig disaster. Frontiers in Public Health. 6: 10 – 117.
- Owusu, B., Lim, A. and Intawong, C. (2022). Haematological, renal, and hepatic function changes among Rayong oil spill clean-up workers: a longitudinal study. International Archives of Occupational and Environmental Health. 1: 1 – 9.
- Kuppusamy, S., Maddela, N., Megharaj, M. and Venkateswarlu, K. (2020). Total Petroleum Hydrocarbons: Environmental Fate, Toxicity, and Remediation. Springer. 1: 1-10.
- Onwugbuta-Enyi, J.,Zabbey, N. and Erondu, E. (2008). Water quality of Bodo Creek in the lower Niger Delta basin. Advances in Environmental Biology.2:132–136.
- VanSprang, P. and Colin, J. (2001). Toxicity identification of metals: Development of toxicity identification fingerprints. Environmental Toxicology and Chemistry. 20: 26-2604.
- Moruf, R.O. and Adekoya, K.O. (2018). Molluscan and crustacean genetic and biotechnology interventions: A review. Animal Research International. 15: 2906 – 2917.
- Afolayan, O., Moruf, R. and Lawal-Are, O. (2020). Bacterial contamination and heavy metal residues in frozen shellfish retailed within Lagos metropolis, Nigeria. Science World Journal. 15: 5-15.
- Hutton, M. (1987). Lead, Mercury, Cadmium and Arsenic in the Environment, Human Health Concerns of Lead, Mercury, Cadmium and Arsenic. SCOPE. John Wiley & Sons Ltd. 53-68.
- Arroyo, S., Flores, M., Ortiz, B., Gómez-Quiroz, E. and Gutiérrez-Ruiz, M.C. (2012). Liver and cadmium toxicity. Journal of Drug Metabolism and Toxicology. 5: 1-40.
- Aweto, H., Saro-bakpo, M. and Aiyegbusi, A. (2019). Cardiopulmonary Functions of School Children in Oil-Spilled and Gas-Flared NigerDelta and Rural-Riverine Lagos Communities. Journal of Applied Science and Environmental Management. 23: 1529-1534 .
- Ovuakporaye, S., Aloamaka, P., Ojjeh, E., Ejebe, E. and Mordi, C. (2012). Effects of gas flaring on lung functions among residents in Gas planning community in Delta State, Nigeria. Research Journal of Environmental Health Science. 4: 525-528.
- Webb, E., Hays, J., Dtrszka, L, Rodriguez, B., Cox, C., Huffling, K. and Bushkin-Benient, S. (2016). Potential hazards of air pollutant emissions from unconventional oil and natural gas operating on the respiratory health of children and infants. Reviews on Environmental Health 31: 225-243.
- Adienbo, O. (2013). Correlation between body mass index and peak expiratory flow rate of an indigenous Nigerian population in the Niger Delta Region. Research Journal of Recent Science. 2: 28-32.
- Egwurugwu, N., Nwafor, A., Shinko, C., Oluronfemi, J., Iwuji, C. and Nwankpa, P. (2013). Effects of prolonged exposure to gas flares on the lipid profile of humans in the Niger Delta Region, Nigeria. American Journal of Research Communication. 1: 115‐145.
- World Health Organization, (1996). Guidelines for Drinking Water Quality; second ed.2. Health criteria and other supporting information. WHO, Geneva.
- Nowaga, K., Etsuko, K., Yasushi, O. and Yasushi, S. (2004). Environmental cadmium exposure, adverse effects and preventive measures in Japan. BioMetals. 17: 7 – 581.
- Keeler, J., Glinsorn, G. and Pirrone N. (1995) Particulate mercury in the atmosphere: its significance, transport, transformation and sources. Water, Air, and Soil Pollution. 80: 159-168.
- Holmes, P., James, F. and Levy, S. (2009) Is low-level environmental mercury exposure of concern to human health? Science of the total environment. 408: 171-82.
- Mahaffey, K. R. (2000) Recent advances in recognition of low-level methylmercury poisoning. Current Opinion Neurology. 13: 699–707.
- Simonsen, L.O., Harbak, H. and Bennekou, P. (2012). Cobalt metabolism and toxicology-A brief update. Science of Total Environment. 432: 210–215.
- Meo, A., Al-Drees, M., Meo, M., Al-Saadi, M. and Azeem, A. (2008). Lung function in subjects exposed to crude oil spill into sea water. Marine Pollution Bulletin. 56: 88–94.
- Zock, P., Rodriguez-Trigo, G., Rodriguez-Rodriguez, E., Souto-Alonso, A., Espinosa, A, Pozo-Rodriguez, F and Barbera, J. (2014). Evaluation of the persistence of functional and biological respiratory health effects in clean-up workers 6 years after the prestige oil spill. Environment International. 62: 72–77.
- Gam, B., Kwok, K., Engel, S., Curry, D., Stewart, A., Stenzel, R. and Sandler, P.(2018). Lung Function in oil spill response workers 1–3 years after the deepwater horizon disaster. Epidemiology: 29: 315–322.
- Ulrici W. (2000) Contaminant soil areas, different countries and contaminant monitoring of contaminants. Resource Journal of Environment and Toxicology. 8: 16-19.
- Vyskocil, A., Fiala, Z., Chenier, V., Krajak, L., Ettlerova, E. and Bukac, J. (2000). Assessment of multi pathway exposure of small children to PAH. Environmental and Toxicological Pharmacology. 8: 111–118.
- Maskaoui, K, and Hu, Z. (2009) Contamination and Ecotoxicology risks of Polycyclic Aromatic Hydrocarbons in Shantou Coastal Waters, China. Bulletin of Environmental Contamination and Toxicology. 8: 172–178.
- Shibutani, M., Mitsomori, K, Satoh, S, Hiratsuka, H, Satoh, M, Sumiyoshi, M, Nishijima, M, Katzuki, J, Nakagawa, J, Akagi, T, Imazawa, T and Ando, M (2001). Relationship between toxicity and cadmium accumulation in rats given low amounts of cadmium chloride or cadmium polluted rice for 22 months. Journal Toxicology Science. 26: 337-358.
- Hollis, L., Hogstrand, C. and Wood, M. (2001). Tissue-specific cadmium accumulation, metallothionein induction and tissue zinc and copper levels during chronic sublethal cadmium exposure in juvenile rainbow trout. Archives of Environmental Contamination and Toxicology 41: 468-474.
- Adaikpoh, M. and N. Orhue, J. (2012). Cadmium-induced hepatorenal-toxicity in rats: Possible ameliorative effect of Talinum triangulare. Nigerian Society for Experimental Biology Journal. 12: 1 -20.
- Abdel-Shafy, H. and Mansour, M. (2016). A review on polycyclic aromatic hydrocarbons: Source, environmental impact, effect on human health and remediation. Egyptian Journal of Petroleum. 25: 107 – 123.
- Almatari M. (2017) Energy absorption and exposure build up factors for some bioactive glasses samples: penetration depth, photon energy, and atomic number dependence. Journal of Optoelectronics and Biomedical Materials. 9: 95-105.
- Godson, A. R., Sridhar, M. K. and Bamgboye, E. A. (2009) Environmental Risk Factors and Health Outcomes in Selected Organism.
- Shrestha, S. and Kazama, F. (2007) Assessment of surface water quality using multivariate statistical techniques: A case study of the Fuji River basin, Japan. Environmental Modelling and Software. 2: 464-475.
- Ordinioha, B. and Brisibe, S. (2013). The human health implications of crude oil spills in the Niger delta, Nigeria: An interpretation of published studies. Nigeria Medical Journal. 54: 10–16.
- Pugliese, A. (2017). Autoreactive T cells in type 1 diabetes. Journal of Clinical Investigation. 127: 2881–2891.
- O’Driscoll, C. and Mezrich, D. (2018). The aryl hydrocarbon receptor as an immune-modulator of atmospheric particulate matter-mediated autoimmunity. Frontiers in Immunology. 9: 2800-2833.
- Seise, I. (2020). Dietary ingestion of 2-aminoanthracene (2AA) and the risk for type-1 diabetes (T1D) Journal of Environmental Science and Health. Part A Toxic Hazardous Substance Environment. 55:1638–1645.
- Wedemeyer, A. and Yasutake, T. (1977). Clinical methods of the effect of environmental stress on fish health. Aquaculture Science. 15: 47-49.
- Begum, G. (2004). Carbofuran insecticide induced biochemical alternations in linear and muscle tissue of Clariasbotrachus and recovery respond. Aquatic Toxicology. 66: 83-91.
- Gabriel, U. and George, A. (2005). Plasma enzymes in Clariasgariepinus exposed to chronic level of round up (glyphosate). Journal of Environment and Ecology. 23: 271-276.