Case Series to Evaluate the Efficacy of Selected Treatment Modality in the Management of Vātakantaka (Planter Fasciitis)
- Samaranayaka Liyanage Gayani Sewwandi
- FathimaShazminHazari
- KalaniDeneeshaHewage
- 412-418
- Dec 15, 2023
- Health
Case Series to Evaluate the Efficacy of Selected Treatment Modality in the Management of Vātakantaka (Planter Fasciitis)
*Samaranayaka Liyanage Gayani Sewwandi, Fathima Shazmin Hazari, Kalani Deneesha Hewage
Temporary demonstrator, Department of Cikitsa, Faculty of Indigenous Medicine, Gampaha Wickramarachchi University of Indigenous Medicine, Yakkala, Sri Lanka
*Corresponding Author
DOI: https://doi.org/10.51244/IJRSI.2023.1011034
Received: 23 October 2023; Revised: 09 November 2023; Accepted: 15 November 2023; Published: 15 December 2023
ABSTRACT
Heel pain is the most prevalent condition these days, and it affects 1 in 10 people at some point in their lives. Various disorders can cause heel discomfort, but one with a high prevalence rate is plantar fasciitis. Vātakantaka and Plantar Fasciitis may be connected in Ayurveda. Walking on an uneven surface and suffering repeated injuries cause Vāta Prakōpa (vitiation of humor), which develops a stinging pain similar to a thorn in the heel area and ultimately results in Vātakantaka. Adults’ heel pain is frequently brought on by plantar fasciitis. Pain that is particularly intense with the first few steps made in the morning is how the disorder typically shows. Plantar fasciitis typically resolves on its own. However, when there is less time between the onset of symptoms and the start of treatment, symptoms typically go away faster. The purpose of this study is to determine the efficacy of selected treatment modalities in the management of Vātakantaka. Four case presentations with a follow-up of one month were studied. Treatment modality, including Ēranda Saptaka Kwātha, Yōgarāja Guggulu, Dhāthri Chūrna, Navarathna Kalka, Sarshapa Thaila, Ketakēla Pattu, and Agni Karma, was advised for four weeks. Pre- and post-treatment assessments of subjective and objective criteria were made. According to the results, most of the symptoms were healed 100%, while some were reduced up to 66.66% and 33.33%. It may be concluded that the selected treatment modality is a secure and reliable treatment for Vātakantaka.
Key words- Agni Karma, Planter fasciitis, Treatment modality, Vātakantaka, Vāta Prakōpa,
INTRODUCTION
A musculoskeletal disease called plantar fasciitis primarily affects the fascial enthesis. Thought to have a mechanical origin, the development of plantar fasciitis is still poorly understood. Particularly, lower-limb biomechanics and foot types associated with pesplanus that result in a reduced medial longitudinal arch are hypothesized to put too much tension on the fascia, leading to tiny tears and persistent inflammation [1].One of Nānātmaja Vātavyādhi (illness due to VātaDōsha) is VātaKantaka (plantar fasciitis). Vātakantaka and Plantar Fasciitis may be connected in Ayurveda. Walking on an uneven surface and suffering repeated injuries cause VātaPrakōpa, which produces prickling discomfort like a thorn in the heel region and eventually results in Vātakantaka[2], [3]. A common complaint of many people who need expert orthopedic therapy and are mostly experiencing persistent discomfort behind their heels is heel pain, which is typically brought on by plantar fasciitis (PF). According to estimates, one in ten people will experience PF at some point in their lives. A higher incidence of PF, which is more prevalent in middle-aged obese females and young male athletes, is found in the athletic population, although not all cases necessitate medical attention. The terms painful heel syndrome, persistent plantar heel pain, heel spur syndrome, runner’s heel, and calcaneal periostitis have all been used to refer to PF in the literature. [4], [5], [6].Walking on uneven or irregular surfaces can vitiate Vāta, which then builds up in the ankle joint and creates discomfort as though it were pierced by thorns. Vātakantaka (Plantar Fasciitis) is the resultant name [7],[8], [9], [10].
Although the worst pain usually starts with the first few steps in the morning, this symptom is not always present in patients with plantar fasciitis. Patients frequently experience pain at the start of an exercise that subsides or disappears as they warm up. The pain can occasionally be accompanied by stiffness and can also happen after prolonged standing. In more extreme circumstances, the discomfort will also get worse as the day wears on. The medial tubercle of the calcaneus is the origin of the thickened fibrous aponeurosis known as the plantar fascia, which extends forward to form the longitudinal foot arch [11], [12].
One of the Vātavyādhi is named Vātakantaka. Due to Vāyu, it is characterized by Shūla (pain) and Shōtha(inflammation) in the Khudak (heel). Consuming Mityāhāra (unhealthy food), Rūksha- Sheeta Bhōjana (excessively dry and cold food), Rātri Jāgarana (waking up at night), Vishama Chēsta (doing the incorrect thing), etc., can all be regarded as general Nidāna(causes) for Vātakantaka[13]. VātaKantaka is also known as Pāda Kantaka, according to Yōgaratnākara (classical text). It is clinically distinguished by a prickling sensation in the Pāda (foot). Owing to Dōsha Sansarga (pathological bondage between two Dōshas), localized Kapha (Sthānika Kapha) and aggravated Vāta (Prakupita Vāta) combine to induce stiffness and pain (Stambha), especially in the morning. When PrakupitaVāta is localized in Snāyu (ligaments) and Sandhi (joints) Pradēsha (region), Achārya Sushruta has mentioned Upakramās (treatment modalities) such as Snēhana (unction), Upanāha (poultice), Agnikarma (therapeutic cauterization), and Bandhana (bandaging) under the context of Vātavyādhi Chikitsa. Acharya Charaka suggests Swēdana as a particular therapeutic method to alleviate vitiated Vāta-Kapha Dōsha[14].
The Purpose of the Study
The purpose of this study is to determine the efficacy of selected treatment modality in the management of Vātakantaka.
RESEARCH METHODOLOGY
Case Presentations
Case 1:
A 57-year-old female patient (retired teacher) attended the OPD of Gampaha Wickramarachchi Ayurveda Teaching Hospital (1090 B) with complaints of pricking pain, tenderness, numbness, swelling, and difficulty walking in the morning for five years. Initially, she did not care about that and the condition became worse before one year. Also, the pain persisted the whole day. She had also received injections for this from the National Hospital in Colombo. She had no history of diabetes, hypertension, hyperlipidemia, or any other complaints. Also, she had no family history; as per her dietary history, she had taken an immense amount of “Anleene” milk and calcium-containing foods with calcium tablets. There were no abnormalities in her menstrual history. Her drug history indicated that she had taken “Murunga” tablets for a long time.
Case 2:
A 34-year-old female patient (working aid) attended the OPD of Gampaha Wickramarachchi Ayurveda Teaching Hospital (1098 B) with complaints of pricking pain and difficulty walking in the morning for one and a half years. She had used safety shoes for 12 years abroad. There were no other complaints, like diabetes and hypertension. But she had an indigestion condition. As she worked abroad, she consumed little rice and fish. Also, she overused “Murunga” tablets and had no family history
Case 3:
A 55-year-old female patient (housemaid for eight years and now a housewife) attended the OPD of Gampaha Wickramarachchi Ayurveda Teaching Hospital (1099 B) with complaints of pricking pain, tenderness, swelling, and difficulty walking in the morning for six months. After a few steps, the pain disappeared. She had had a history of hypertension and hypercholesterolemia for two years. Also, she had bilateral knee joint pain for eight years and cataracts in both eyes for one year. Recently, she lived in an apartment at Colombo Grandpas. As she worked as a housemaid abroad, she consumed salads and milk. There is no related family history and no abnormalities in her menstrual history.
Case 4:
A 48-year-old male police officer attended the OPD of Gampaha Wickramarachchi Ayurveda Teaching Hospital (1201 B) with complaints of pricking pain, tenderness, and difficulty walking in the morning for two years. As others complain, he had gastritis for three years and constipation for three months. He consumed alcohol and cigarettes only at parties. There is no related family or drug history.
Treatment Modality
Treatment was planned for 4 weeks with Agni Karma.
Ēranda Sapthaka Kwātha– 30 ml twice daily after foods
Yōgarāja Guggulu– 2 Guli twice daily with luke warm water
Dhāthri Chūrna– 10 g mixed with 120 ml boiled water at night
Navarathna Kalka– 1 g twice a day with luke warm water
Sarshapaoil- Apply to feet twice a day
Ketakēla Pattu– Apply to feet twice a day
Agnikarma– performed from 2nd week to 4th week
Criteria for Assessment of Symptoms
Assessment was done on improvements in signs and symptoms with the help of a suitable scoring method. Here, cases of Vātakantaka were assessed by comparing the symptoms before and after treatment. Then the data were analyzed by Microsoft Excel. The patients were monitored for one month following treatment. Even after one month of follow-up, no indications or symptoms of PF were noted.
Limitations
Patients with traditional Vātakantaka indications and symptoms as defined by both contemporary science and Ayurveda were chosen. Additionally, men and women between the ages of 30 and 60 were chosen. Excluded from the study were expectant mothers, nursing mothers, patients with life-threatening conditions such as HIV, Hepatitis B, psychiatric disorders, bleeding disorders, and COVID-19-positive patients.
Subjective Criteria: [15].
Table I:VAS Scale (Visual Analogue Scale):- Scale Score Severity of Pain
| Parameters | Grade |
| No pain | 0 |
| Mild pain (discomforting) | 1 |
| Moderate pain (disturbing daily activities) | 2 |
| Severe pain (unbearable pain) | 3 |
Objective Criteria: [15].
Table II: Tenderness
| Parameters | Grade |
| Nil (No tenderness) | 0 |
| Mild tenderness (causing the patient to wince on digital pressure) | 1 |
| Moderate tenderness (causing the patient to wince and withdraw on digital pressure) | 2 |
| Severe tenderness(Patient does not allow to touch) | 3 |
Table III: Swelling
| Parameters | Grade |
| Nil (No swelling) | 0 |
| Mild Swelling (2-4 mm of depression) | 1 |
| Moderate Swelling (4-6 mm of depression) | 2 |
| Severe Swelling(6-8 mm of depression) | 3 |
Table IV: Movability (Difficulty in Walking)
| Parameters | Grade |
| Nil (No difficulty in walking) | 0 |
| Mild (Can walk with a simple aid) | 1 |
| Moderate (Can walk with a strong aid) | 2 |
| Severe (Unable to walk even with a aid) | 3 |
RESULTS AND DISCUSSION
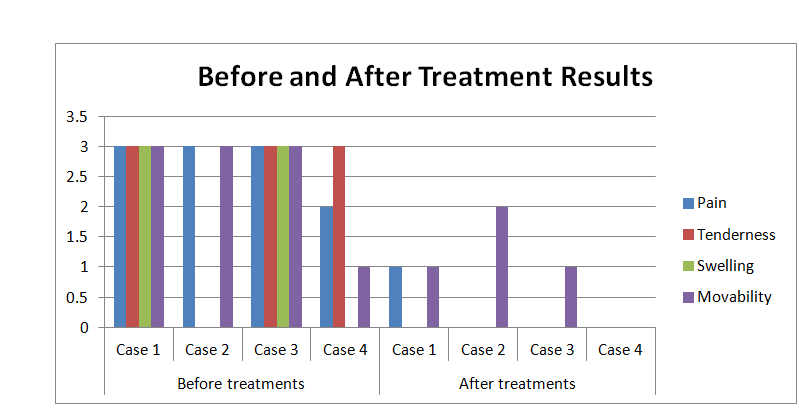
Table V: Before and After Treatment Results
| Parameters | Before treatments | After treatments | ||||||
| Case 1 | Case 2 | Case 3 | Case 4 | Case 1 | Case 2 | Case 3 | Case 4 | |
| Pain | 3 | 3 | 3 | 2 | 1 | 0 | 0 | 0 |
| Tenderness | 3 | 0 | 3 | 3 | 0 | 0 | 0 | 0 |
| Swelling | 3 | 0 | 3 | 0 | 0 | 0 | 0 | 0 |
| Movability | 3 | 3 | 3 | 1 | 1 | 2 | 1 | 0 |
Plettner introduced the term “calcaneal spur” at the start of the 20th century. The plantar insertion of the plantar fascia and muscles is where the “plantar heel spur” forms, whereas the “dorsal heel spur” forms where the Achilles tendon inserts. These characteristics nearly match Vātakantaka, a disease entity recorded in classical Ayurvedic texts [15]. In this study patients were selected from same geographical areas and from same cultural units. The Omani series was chosen for an external comparison because of its distinct historical-cultural, genetic, and geographic background. It reveals startling distinctions between the Italian group and parallels with the Spanish one. The similar geographical topography of the Italian and Spanish series accounts for these disparate but unexpected outcomes. In light of our findings, a thorough examination of the archaeological investigations from these sites is required to compare our theories—especially the one about the impact of footwear and habits. Every sample is unique because of the geological and geographic features of their surroundings, as well as lifestyle choices related to their daily jobs, travel, and footwear. The disparities are thought to be caused by all of these causes[16].
Pain was healed 100% in all cases except case 1, and it was healed up to 33.33%. Tenderness and swelling were healed 100% in all cases, while difficulty walking was healed 100% in case 4. In cases 1 and 3, difficulty walking was healed up to 33.33%, while in case 2, it was healed up to 66.66%.
Ēranda Saptaka Kwātha is Vātaghna and pacifies Vāta, hence reducing pain and swelling. Yōgarāja Guggulu is indicated in the management of Vāta Vyādhi (disease), which acts as Shūlahara (analgesic) and Shōta Hara (anti-inflammatory). All diseases occurred due to the formation of Āma (undigested food). Both DhātriChūrna and Nawarathna Kalka improve digestion power, as Dhātri Chūrna has Virēchana (purgative) action and Nawarathna Kalka has Pāchana (digestive action) Karma. DhātriChūrna: From which Dhātrihas SheetaVīrya (cold potency), which collectively acts on Tridōsha (three humors).It also acts as Rasāyana (rejuvenation), which means improving the quality of life, Ojadushti (vitiation of essence), and DhātuBalyakar (strength tissues). It also acts as RasaRaktagataSamaDōshaPāchana & Prasādana (balance of blood tissue). So the basic pathology can be stopped. Dhātri is Tridōshashamak is Kaphavātshāmak & Pittashāmakby Tikta (bitter) Rasa (taste). Because of the omega-3 fatty acids in Sharshapa (mustard oil), oil eases stiffness and pain. KetakēlaPattu relieves pain, especially joint and muscle pains.
Because the Ushna (hot) Guna (action) of Agnikarma(cautery) is the polar opposite of the Vāta and KaphaDōshās, it treats all Vātaja and Kaphaja illnesses. Every Dhātu (tissue) has its own Dhātvagni, and when it is low, ailments start to develop, according to Ayurveda. Agnikarma treats the sickness in this situation by supplying external heat and raising Dhātvagni (digestive fire), which aids in digesting the exacerbated Dōshas (body humors). The local thermotherapy may speed up tissue metabolism, which could result in the expulsion of toxic byproducts and undesirable metabolites. Heat may activate the lateral spino-thalamic tract (SST), which activates the descending pain inhibitory fibers (DPI) and releases endogenous opioid peptide. This peptide binds to opioid receptors in the substantiagelatinosarolandi and prevents the release of Psubstance (pre-synaptic inhibition).
CONCLUSION
From this case series, it can be concluded that Vātakantaka can be effectively managed with a selected treatment modality. However, further clinical research with a larger sample size may be needed to further authenticate the efficacy.
REFERENCES
- Wearing S C, Smeathers J E, Urry S R, Hennig EM, Hills AP. The patho mechanics of plantar fasciitis. Sports medicine. 2006 Jul;36:585-611.
- Ganatra, R. J., Kapadiya, M. M., &Dudhamal, T. S. (2021). Agnikarma (therapeutic heat burn) an unique approach in the management of vatakantakawsr to plantar fasciitis-A single Case Report. International Journal of AYUSH Case Reports, 5(1), 30-35.
- Hiremata, V., &Balaraddi, S. L. (2020). A randomized controlled trial to evaluate the effect on pain by Agnikarma with Madhuchista (bee wax) and Panchaloha Shalaka in Vatakantaka. Journal of Ayurveda and Integrated Medical Sciences, 5(05), 78-88.
- Tahririan, M. A., Motififard, M., Tahmasebi, M. N., &Siavashi, B. (2012). Plantar fasciitis. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences, 17(8), 799.
- Amarprakash, D., Amarsingh, R., &Gajanan, M. S. International Journal of Applied Ayurved Research ISSN: 2347-6362 TO EVALUATE THE ROLE OF SIRAVYADHA IN VATAKANTAKA.
- Hakkandi, S. N., & KS, M. A. D. B. CONCEPTUAL STUDY ON THE MANAGEMENT OF VATAKANTAKA.
- Misar, S. (2017). Agnikarma in the management of Vatakantaka (planter fasciitis). Journal of Indian System of Medicine, 5(2), 126-129.
- Kuchanur, S., &Santosh, Y. M. (2014). Innovative Practice Of Agnikarma In Vatakantaka. Journal of Ayurveda, 8(4).
- Astagimath, S., Chavana, S. G., &Prashanth, A. S. (2021). To evaluate the effect of Dashamula Churna Pinda Sweda a touchstone procedure in the management of Vatakantaka. Journal of Ayurveda and Integrated Medical Sciences, 6(3), 01-05.
- Sahoo, C. P., & Kumar, M. A. (2023). An Open-Label Clinical Study to Evaluate the Effectiveness of Padapichubandhana with Nirgundi Taila in Vatakantaka. Journal of Ayurveda, 17(3), 206-212.
- Young, C. C., Rutherford, D. S., & Niedfeldt, M. W. (2001). Treatment of plantar fasciitis. American family physician, 63(3), 467-475.
- Diwan, S. (2013). A Comparative Study of Agnikarma with Loha and Panchaloha Shalaka in Vatakantaka(Doctoral dissertation, Rajiv Gandhi University of Health Sciences (India)).
- Vitthalrao, A. V., &Kadam Rahul, V. (2022). ROLE OF AGNIKARMA IN VATAKANTAKA (CALCANEAL SPUR)-A CASE STUDY.
- Gupta, A. K., Mahanta, V., Sherkhane, R., & Gupta, S. K. (2020). Iontophoresis with Murivennakwatha as an adjunctive therapy in the management of Vatakantaka (Plantar fasciitis): A case report. Journal of Ayurveda Case Reports, 3(4), 148-152.
- Sonekar, R., Ballal, S. T., &Sonekar, A. (2021). EFFICACY OF SIRAVEDHANA IN THE MANAGEMENT OF VATAKANTAKA–A CASE STUDY.
- Saldías, E., Isidro, A., Martínez‐Labarga, C., Coppa, A., Rubini, M., Vila, B., &Malgosa, A. (2022). Pathological and normal variability of foot bones in osteological collections from Catalonia (Spain) and Lazio (Italy). International Journal of Osteoarchaeology, 32(1), 215-228.
CONSENT FORM