
Challenges of Childhood Obesity Interventions in the United Kingdom and Lessons for Public Health Practitioners in the Global South: A Scoping Review
- Bankole Israel Adeyemi
- Oluwaseun Fadeyi
- Moradeyo Abdul Lateef
- Temitayo Adedayo Jejeniwa
- Bethel Oshokhai
- Oladejo Abayomi
- Ebenezer Odji
- 78-110
- Jun 29, 2024
- Health
Challenges of Childhood Obesity Interventions in the United Kingdom and Lessons for Public Health Practitioners in the Global South: A Scoping Review
Bankole Israel Adeyemi1, Oluwaseun Fadeyi*2,3, Moradeyo Abdul Lateef 4, Temitayo Adedayo Jejeniwa4, Bethel Oshokhai3, Oladejo Abayomi5, Ebenezer Odji6
1Ondo State Primary Healthcare Development Agency, Akure Ondo State, Nigeria
2Centre for Environmental Management, University of Free State, Bloemfontein South Africa
3Solina Centre for International Development and Research
4School of sport and health sciences, Cardiff Metropolitan University, Wales, United Kingdom
5Faculty of Economics and Management Science, University of Pretoria South Africa
6Faculty of Environmental Sciences, Lagos State University, Lagos, Nigeria
*Corresponding Author
DOI : https://doi.org/10.51244/IJRSI.2024.1106008
Received: 22 May 2024; Revised: 03 June 2024; Accepted: 11 June 2024; Published: 29 June 2024
ABSTRACT
Childhood obesity is a major health challenge around the world and has been linked to several health and non-health risks. Although significant efforts are in place in the United Kingdom (UK) to reduce the burden of the disease, these efforts suffer fundamental shortcomings that potentially undermine their effectiveness. Drawing upon this understanding, this study examines the existing intervention challenges to childhood obesity interventions in the UK, with the goal of informing improved programmatic solutions in the global south (Africa, the Caribbean and Latin America, Asia excluding Japan, Israel, and South Korea, with Oceania without New Zealand and Australia). A search of five popular health databases was carried out yielding 19 research articles. The study article period is between 2013 and 2023. A scoping review methodology was implemented on the selected reports following a critical appraisal. Children between the ages of 3 to 11 years were considered. Findings suggest that intervention implementers focus mainly on executing school-based programs but fail to involve stakeholders from the wider society which consistently leads to failure. This review also found body mass index to be a popular measure for weight gain or loss. Nevertheless, this measure has been consistently criticized in literature, thus subjecting the accuracy of the results of interventions to serious criticism. Overall, for intervention implementers in developing countries to carry out successful interventions, lessons around perceived standardized but possibly inaccurate procedures and measures must be carefully considered.
Keywords: Childhood, Obesity, Intervention, Health challenges, Childhood obesity, Intervention failure in Childhood Obesity, Intervention failure in the UK, Lessons for the Global South.
INTRODUCTION
Of the many countries of the world where the health of children is prioritized, the United Kingdom (UK) is perhaps one of the most popular. Given a range of health policies aimed at ensuring that children aged 0-5 years enjoy the best of health in their childhood years and eventually grow to become healthy adults. This is one of the ultimate goals of the Government of the United Kingdom as the country moves to actualize Sustainable Development Goals (SDG) 3 alongside its 13 targets. Even though the UK is making significant efforts across all fronts concerning the health of children, it is obvious that the country has consistently struggled to control and manage childhood obesity, a leading disease amongst children in the UK and in many developed countries [1]. Whilst [2] offer compelling evidence suggesting that low socio-economic level is the ultimate cause of obesity, some scholars have identified obesity as the disease of the rich in poorer climes [3]. Nevertheless, the situation is completely different in wealthy nations where the burden of obesity is more pronounced amongst the poor.
The World Health Organization (WHO) has noted increased global rates of obese children since the mid-1970s [4]. This is the exact case in the UK. WHO notes that, globally, more than 30 million children were categorized as obese in 2020 [4]. According to the National Health Service (NHS) report in 2020, at least 1 out of every 5 children is obese, signifying a 2% increase in the obesity rate of children in reception classes, a similar situation is found with children in higher classes [5]. Whilst weight gain in children would not have ordinarily caused any problems, the fact that obesity has been linked to many diseases is worrisome. To name a few, childhood obesity has been researched to be the primary cause of metabolic challenges as well as sleeping problems [6], [7]. Some scholars have also posited the challenges faced by obese children when the need arises to engage in physical activities. Furthermore, [8] maintained that lengthy periods of obesity in childhood may translate into obesity as an adult, increasing the chances of a person suffering from a range of respiratory problems, diabetes, and high blood pressure [9]. Aside from the health implications, obesity has also been found to affect the academic performance of children [10].
One way in which researchers in the global north in general, particularly those in the UK, continue to stay ahead of the obesity scourge is the practice of implementing interventions. This has led to an increased understanding of the disease and its manifestation in children. Amongst the new developments, [11] explained that there is a need for implementers to duly consider the health status as well as the socio-demographic situation of a child as these factors are known to promote the disease. This is why the practice of socio-cultural interventions some of which are implemented in UK schools has become popular. There is also a wide range of other interventions such as breakfast in class among others.
Rationale
The many known implications of childhood obesity in the UK have resulted in significant scholarship about the disease which are presented in the form of interventions designed either to eradicate, control, or manage the disease in the UK. Whilst this is the case in the UK, contrasting evidence from developing countries shows little or no efforts to manage childhood obesity. This presents a learning gap for public health practitioners and policy-makers in developing countries. Premised on this situation, there is an urgent need to examine the challenges faced in childhood obesity intervention implementation across the UK and the lessons that developing countries can learn from them.
Research Aim and Objectives
This study examines the shortfalls of childhood obesity interventions as implemented across the UK, and lessons that public health personnel in developing nations can learn. To achieve this goal, the research will make efforts to answer the following questions:
- What are the common childhood obesity interventions in the UK?
- What are the main challenges of childhood obesity interventions in the UK?
- What critical lessons can public health practitioners in developing countries learn from the challenges of childhood obesity interventions in the UK?
LITERATURE REVIEW
Childhood obesity according to several authors [12], [13], [14], [15] is a major public health issue worldwide, with serious psychological, physical, and social consequences. [16] mentioned that childhood obesity rates in the United Kingdom have been gradually rising, necessitating several intervention initiatives to combat this growing epidemic. Nonetheless, these interventions encounter numerous hurdles, and the lessons acquired are critical for developing countries dealing with similar problems. Within this literature review session of the paper, the researchers delve into the complexities of childhood obesity interventions in the United Kingdom, assess their effectiveness, and draw parallels with the situation in developing nations.
Prevalence and Impact of Childhood Obesity in the United Kingdom
Childhood obesity in the United Kingdom has reached alarming proportions, with various research and reports showing its rising prevalence [16]. Based on statistics from the National Health Service (NHS) Digital, the National Child Measurement Programme (NCMP) indicated that in the 2018/2019 school year, 20.2% of children in Reception (aged 4-5) and 34.3% of children in Year 6 (aged 10-11) were overweight or obese [17]. This pattern has grown significantly during the last several decades. For example, obesity rates among sixth graders increased from 18.7% in 2006/2007 to 20.2% in 2018/2019. The issue is considerably more concerning in some areas along with specific demographics [18]. According to NCMP data, childhood obesity is prevalent in poor communities. For instance, in 2018/2019, 26.9% of children in the poorest districts were obese, whereas 11.4% were in the least impoverished regions [17]. This gap demonstrates the importance of socioeconomic factors in juvenile obesity rates.
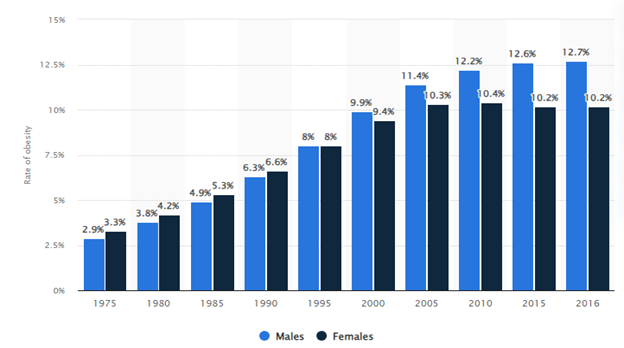
Figure 1: Childhood obesity rate in the UK between 1975 and 2016 [19].
Figure 1 shows the statistics of the prevalence of childhood obesity in the United Kingdom (UK) between 1975 and 2016, broken down by gender. At the start of this time succession, female children in the UK were more inclined to be obese than male children. This changed in 1995, as rates of obesity among both female and male children in the UK hit 8%. In 2010, as depicted in Figure 1, 12.7% of male children reported being obese, compared to 10.2% of female children. It is additionally interesting to note that the rate of obesity among female youngsters has declined from an alarming rate of 10.4% in 2010 [19]. Childhood obesity has a wide range of consequences, including physical health, psychological well-being, and socioeconomic outcomes.
Physical Health Consequences of Childhood Obesity
Childhood obesity, according to [20], is linked to a variety of unfavourable physical health outcomes that can persist into older age. According to many academic health-related research[21], [22], [23], one of the most evident and concerning consequences is a higher likelihood of acquiring type 2 diabetes. [24] stated that obese youngsters are more likely to develop insulin resistance, an antecedent to diabetes that may result in long-term health issues if not managed effectively. According to a study published by [25], obese youngsters are approximately four times more likely to be diagnosed with type 2 diabetes than their non-obese classmates. [26] also observed that childhood obesity exerts an enormous effect on the cardiovascular health of the victim or the child in question. Obese children tend to be more prone to conditions like dyslipidemia (to develop high levels of cholesterol and triglycerides), high blood pressure, and atherosclerosis (artery stiffness). These factors lead to the early start of cardiovascular disease. According to research, obese children as early as five years old can develop atherosclerosis, which dramatically raises the risk of coronary artery disease and stroke later as adults [27].
Obese children are also prone to respiratory difficulties. Obstructive sleep apnea (OSA), defined as constant episodes of obstructed breathing during sleep, is common in obese children owing to extra fat around the neck clogging airways. This syndrome impairs sleep quality and can cause daytime weariness, poor academic performance, and behavioural problems [28]. Musculoskeletal disorders are another complication, as excess weight strains bones and joints. This can result in Blount’s disease (a growth problem of the shin bone), flat feet, and an increased risk of fractures. These difficulties can induce chronic pain and restrict physical activity, continuing the obesity cycle [29]. Obesity has also been associated with gastrointestinal concerns like non-alcoholic fatty liver disease (NAFLD), which causes fat to build up in the liver, eventually resulting in liver damage and cirrhosis over time. According to multiple studies [26], [30], [31], NAFLD has grown more common in obese youngsters and is associated with major metabolic issues.
Economic Burden of Childhood Obesity
Childhood obesity has significant economic consequences, including both immediate and subsequent healthcare costs, like costs incurred due to loss of productivity as a result of low performance and costs incurred as a result of social care bills or subsidies. As reported by [32], the Government of the United Kingdom spends a significant amount of its revenue on tackling obesity-related health conditions. For instance, the treatment of cardiovascular disease, type 2 diabetes, and orthopaedic issues in children and adolescents living with obesity demands significant state medical resources (funding and equipment). As published by [33] the National Health Service incurs a direct cost of over £5.1 billion annually while treating obesity-related disorders. Also, the Indirect costs incurred may raise a financial burden. Obesity among children typically leads to lowered performance in school and a greater absence rate resulting from health issues, which might influence future job prospects and labour productivity. Based on to report by [34], children’s absenteeism owing to obesity-related issues and lower productivity make the UK economy lose over £28 billion each year. Also, the cumulative economic effect continues until adulthood. As observed by [32], children with obesity are more likely to develop into obese adults, which will increase the probability of chronic conditions requiring continual medical treatment and perpetuating the downward spiral of financial strain on the UK healthcare system.
Psychological and Emotional Impact of Childhood Obesity
As observed by [35], childhood obesity is not only a physical health issue; the author mentioned that it additionally comes with significant emotional and psychological consequences. Children suffering from Obesity as noted by [36] may face considerable social discrimination and stigma, which can lead to a variety of emotional and psychological issues. Low self-esteem is one of the most prevalent concerns or issues. [37] mentioned that children who are overweight/obese frequently get bullied and taunted by their peers, lowering their self-confidence and sense of self-worth. A study by [38] revealed that obese or overweight children are considerably more likely to be ridiculed/bullied than their normal-weight classmates, regardless of colour, gender, or socioeconomic status. When obese kids are bullied, they usually experience emotions of remorse, isolation, and helplessness.
Several authors [37], [39], [40], [41], also observed that children with the health condition of obesity are also more inclined to develop anxiety and depressive disorders. They tend to experience a Long-term strain from battling obesity and its social repercussions and it may further result in worsening these health conditions. According to a study by [38], obese youngsters are more likely to experience symptoms of depression and anxiety-related conditions than their non-obese classmates [42]. This is owing to the constant negative criticism they receive from their social setting, which often leads to experiencing feelings of hopelessness and inadequacy.
In addition, as posited by [37], children with obesity condition have a higher risk of developing eating disorders. [43] explained that they are pressured to lose weight so as to meet societal standards and as such, they tend to over too much which might cause some youngsters to engage in harmful weight-control routines, like excessive dieting or bingeing. These behaviours might compound their physical and mental health problems, resulting in a tough-to-break cycle. Also, [36] mentions that Obesity may damage relationships within the family or family dynamics. Parents may feel guilty or frustrated about their child’s illness, resulting in strained relationships. More importantly, the child’s mental distress could have a bearing on the entire family’s attitude and functioning, resulting in a tense and worrisome family setting.
Ethnic Disparities Associated with Childhood Obesity
As reported by [44], the rate of obesity in children varies greatly by ethnicity, with certain ethnic groups having higher rates than others. According to data from the National Child Measurement Programme, obesity rates amongst Asian and Black children in the United Kingdom are significantly higher than those among White children. According to a poll, the obesity rate among Year 6 children in 2018/2019 was highest in the Black and Asian communities (27.8% and 25.9%, respectively), compared to 16.7% in the White population [45]. These distinctions or variations are attributed to an intricate link of cultural, social, and ecological variables. for instance, Ethnic food habits often have a part, as traditional foods may contain more fats and calories. In addition, socioeconomic variables such as lower educational attainment and income in specific ethnic communities may limit their ability to purchase nutritious meals and afford recreational facilities, which causes higher obesity rates.
Also, some ethnic minorities usually reside in urban centres with barely any open spaces and a high concentration of fast-food outlets, which may increase their risk of being overweight and raising obese children. [46] mentioned that language barriers and an absence of culturally appropriate health education hinder efficient discussion on healthy lifestyles and obesity prevention.
Socioeconomic Disparities Associated with Childhood Obesity
The overall rate of children with obesity varies greatly based on the socioeconomic status (SES) of the parents or caregivers, resulting in youngsters from families with lower earnings getting more susceptible. The variation is caused by several causes, like less availability of nutritious meals, fewer opportunities for aerobic activity, and greater susceptibility to bad food marketing. Lower-income families according to [45], generally are residents in “food deserts area”. Food-deserted areas are characterized by locations with little or no access to inexpensive, nutritional meals [48]. On the contrary, these municipalities are bombarded with convenience stores and eateries that provide highly dense-calorie foods with little or no nutritional value. This scenario poses a challenge for caregivers to provide healthy nourishment to their wards [39]. As a result, as noted by [49], communities with low-income earnings may often lack safe recreational spaces like parks and sports facilities, which restrict the opportunities for children to engage in physical activity for their optimal growth and physical development. Educational institutions within these areas could additionally have less funding for physical and health education programs, which further limits children’s ability to engage in routine physical activity [50]. Financial constraints of the parents as noted by [51] may also encourage households to prefer less costly, more energy-dense diets over expensive vegetable and fruit consumption. The strain of financial uncertainty according to psychologists has the tendency to lead victims to eating disorders as well as reduced attention to healthy lifestyle choices.
UK Government Intervention Strategies for children suffering from Obesity
The United Kingdom adopted several government and policy steps to combat the growing prevalence of childhood obesity. In 2016, the government announced the Childhood Obesity Plan, with the goal of halving childhood obesity rates by 2030 [52]. This comprehensive plan comprises numerous initiatives aimed at both the food environment and lifestyle behaviours. Among the important measures is the Soft Drinks Industry Levy, formerly known as the sugar tax. Introduced in 2018, this levy imposes a tax on sugary soft drinks, incentivizing manufacturers to reformulate their goods to contain less sugar. Early reviews indicate that this strategy has reduced the sugar level of numerous beverages [51].
Also, the UK government is implementing voluntary modification measures to urge food firms and vendors to reduce salt, sugar, and fat content in their manufactured products [54]. Further to that, stricter regulations were placed on the marketing and promotion of junk food/unhealthy food towards youngsters so as to reduce children’s consumption of low-nutrient and high-dense-calorie food products through media. Educational institutions also play a pivotal role in the fight against obesity in children in the UK due to that they offer a structured environment that promotes proper nutrition and physical activity. The UK government also mandated better school meals and increased support through funding for physical education in preschool to guarantee children receive appropriate dietary guidance and exercise during school hours. Part of the government effort is the Daily Mile program, which was initiated to encourage young people to jog or run for 15 minutes every single day, so as to show excellent results in increasing physical activity levels. [55]. Dietary awareness and proper school food guidelines as posited by [56] are also critical components of the aforementioned interventions. Change4Life along with other community-centred initiatives leverage public education campaigns, outreaches and neighbourhood support networks to encourage healthier living [31].
What are the Challenges in Implementing Childhood Obesity Interventions in UK?
Implementing interventions for addressing childhood obesity in the United Kingdom hit several hurdles, the majority of which can be linked and others complex. The key problem as observed by [57] is hostility from the food and beverage businesses. Notwithstanding the government’s efforts to enact regulations such as the Soft Drinks Industry Levy, food and beverage corporations have expressed strong opposition, stating the proposed intervention will have a severe impact on their businesses [58], [59], [60]. Such opposition according to [61] may stymie policy implementation and as such result in policy insignificant, reducing their effectiveness.
Another bottleneck experienced by the intervention is socioeconomic inequality within the UK communities, which exacerbates obesity rates in low-income households. As observed by [62], some of these families often live in areas with little or limited access to nutritional foods and recreational dispensary alternatives. Notwithstanding government intervention programs to encourage healthier diets and more physical activity, families and caregivers within these neighbourhoods face structural barriers to adopting and sustaining healthier lives for their wards. Also, cultural variances and discrepancies in health literacy across ethnic groups make it difficult to implement a one-size-fits-all intervention strategy by the UK government. According to [62], effective communication along with culturally appropriate strategies are essential but often insufficient during policy implementation. Educational institutions offer a critical platform for preventing obesity among children, nonetheless, these institutions also face particular challenges. According to [63], financial limitations and competing academic interests could hinder the rollout of comprehensive student health campaigns. Also, guaranteeing that educational regulations result in long-term behavioural changes beyond school hours needs regular engagements with parents/caregivers and the general public. Lastly, there is also the issue regarding the sustainability and continuity of the intervention program. Short-term financial cycles and political transitions, according to [62], may undermine the long-term sustainability of health projects by the government. As such, sustained dedication and sufficient financing are essential for preserving the momentum of obesity interventions and attaining long-term success.
What are the Backwardness of Interventions in Developing Countries?
Intervention programs to mitigate childhood obesity in underdeveloped nations regularly face significant hurdles, resulting in poor results and effectiveness. According to [65], the primary major bottleneck is a scarcity of resources. A lot of developing nations like Nigeria lack proper healthcare facilities and financing, which results in restricting their ability to implement complete childhood obesity prevention initiatives. As posited by [66], owing to this limited financing, the government prioritized emergency healthcare above prevention treatments, which put long-term childhood obesity management in the non-essential healthcare priority policy.
Childhood obesity and nutritious eating habits are also overlooked by the general population owing to high illiteracy levels. As such, [67] observed that many developing nations suffer a double burden of malnutrition, with undernutrition and obesity coexisting. The result undermines public health messages and policy desired outcomes. the efforts of the government to promote healthy eating habits and physical activity are usually overlooked by more visible and pressing national issues such as hunger (food inflation and insurgency) and infectious diseases. Also, the socioeconomic factors exacerbate the challenge of implementing these interventions. Poverty and food shortages are major economic problems in developing nations, which often lead to families eating cheaper, calorie-dense meals based on the economic realities [68]. These eating preferences are aggravated by a dearth of leisure opportunities and safe places to exercise, which leads to childhood obesity.
Political unrest and governance issues, according to [69], may hinder the development and execution of effective public health interventions. Developing nations are faced with inconsistent policy enforcement, corruption, and a lack of political will all work to hinder the success of obesity control measures. Moreover, medical facilities in these developed nations are usually fragmented, with limited synergy across various industry segments and institutions, which is essential for a comprehensive approach to childhood obesity prevention interventions [70].
Additionally, cultural attitudes and customary eating behaviours may cause significant complications in terms of childhood obesity intervention. Some cultures in developed countries, especially Africa believe that a higher body weight is a sign of affluence and healthy living, which potentially leads to opposition to obesity control programmes.
RESEARCH DESIGN AND METHODOLOGY
To achieve the study objective in order to determine the efficacy of existing interventions for the prevention, control, and management of childhood obesity in the United Kingdom, it becomes necessary to conduct a thorough literature review to fully understand the situations requiring certain kinds of intervention, their rate of success and/or failure rates, the reason or reasons for inefficiency (if perceived to have failed), and methods of transforming the situation around where necessary. As such, the current research undertakes a scoping review of the available literature. Scoping reviews are effective when the purpose of the study is to map the range of literature on a certain research topic. This provides an overview of academic activities in that area, highlighting areas that have yet to get considerable research for planning further research [71]. Scoping reviews are particularly effective for examining new research information when other more extensive assessments do not provide an accurate representation of potential questions. [72] emphasized that this is attainable by providing findings from research execution, along with the various sorts of evidence that shape policy and practice. In one of the first studies to attempt to establish a baseline framework for undertaking scoping reviews, [73] proposed a few factors that may justify such reviews. [74] fine-tuned these parameters, pointing out that there were no explicit guidelines for executing scoping reviews at the time. Nonetheless, in 2015, the Joannes Briggs Institute published an easy recommendation for authors [75]. [76] interpret this recommendation and declare that a scoping review may be appropriate in the scenarios that follow: i. Identifying existing research evidence in a niche, ii. Clarifying fundamental definitions and concepts, iii. Examining research methods to identify knowledge gaps, iv. Scoring literature for a more detailed review. The current study falls under points (i) and (iv) above, hence a scoping review was chosen, which involves a structured database search using predetermined criteria.
Search Design
The scoping review approach for this research was carried out using five search engines (MEDLINE, Cochrane Library, CINAHL, PubMed and Web of Science), the five of which are well-known for their wide coverage of public and child health-related subjects. According to [77], while choosing databases for searches in evidence-based investigations, researchers must consider indexing and abstracting concerns. This enables the selection of the most appropriate database for optimal time management. A search of each of the listed databases yields a variety of scientific articles on public and child health, particularly in the areas of disease identification description and action for preventing, controlling, or alleviating them. To guarantee that research follows a distinctive framework for answering the research questions as indicated by [78], a SPICE structure (see Table 1) is utilized to organize essential parts of the investigation, which was previously chosen to frame the research questions.
Table 1. The research SPICE structure
| SPICE | |
| Setting | United Kingdom |
| Population | Overweight and Obese children, their parents, and any other individuals participating in programs to prevent, control, and manage the disease |
| Interest | Childhood obesity |
| Comparison | Effective vs. ineffective interventions for childhood obesity |
| Evaluation | Measures to Determine the Effectiveness of Interventions against Childhood Obesity in the UK |
After selecting the databases for this research, [79] stated that the following stage in a scoping review is to establish a set of search criteria. These criteria, also known as inclusion and exclusion requirements, guarantee that the search takes a specific form so that the articles chosen can be traced and tracked to some standardised criterion and that they are indeed relevant to the purpose of the research with regard to interest and study focus. Table 2 explains the criteria used to find and choose literature for this research.
Table 2. Requirement for the selection or rejection of articles
|
Aspect |
Criteria | |
| Inclusion | Exclusion | |
| Year | Publications released between January 2014 and April 2024. | Articles published before 2014 and after April 2024. |
| Location | The United Kingdom only (comprising Scotland, England, Northern Ireland, and Wales) | All the nations in the globe that are not part of the United Kingdom |
| Interest | Childhood obesity and conditions leading to it (e.g., overweight) | All other childhood diseases apart from obesity; obesity in adults |
| Language | English | Spanish, Dutch, Deutsche, and all other languages apart from English |
| Focus | Interventions to prevent, manage, and control childhood obesity; success/failure rates of the interventions; causes of ineffectiveness of the interventions; and ways to improve on the interventions for childhood obesity | Causes and effects of obesity |
| Type of article | Peer-reviewed documents only | All other publication types that do not undergo the peer-review procedure (i.e. year reports, books and their sections, white papers blog posts etc.) |
| Article reputation | Literature is published in trustworthy journals where academic rigour is usually applied. | Articles published in perceived predatory journals |
| Nature of literature | Only empirical literature | Review and narrative studies |
Strategy for Executing Literature Search
To conduct a literature search in each of the specified databases, a few terms identified as keywords, taken from the study’s title and based on the study objectives, were employed. According to [78], the words to employ as search terms (keywords) in a scoping review task must be solely determined by the research objectives/questions, such that papers resulting from the search contain data relevant to the ongoing investigation. The current research’s search criteria include CHILDHOOD, OBESITY, EFFECTIVENESS, INTERVENTION, and UNITED KINGDOM. In addition to selecting search phrases, researchers can obtain reliable search feedback from database searches by looking for words that are synonymous or have a meaning similar to the search terms. As such, words like CHILDREN OR YOUNG PERSON (which is synonymous with childhood), OVERWEIGHT (which is closest in describing obesity), PROFESSIONAL HELP (which is used to substitute intervention) and EFFICACY or SUCCESS (which is synonymous with effectiveness), were all accepted. Aside from using synonymous phrases, using Boolean terms (AND, OR, and NOT), truncation, and MeSH (Medical Subject Heading) terminology. Boolean phrases allow the researcher to widen potential input from database searches or filter them down to the most relevant items. The Aggregate search strings are as follows:
- “ Overweight OR Obesity AND Young Persons OR Children’’ NOT ‘Older people OR Adults’’
- ‘‘ Overweight OR Obesity AND Young Persons OR Children’’ NOT ‘Older people OR Adults AND United Kingdom’’
- “ Effectiveness OR Efficacy OR Success’’ AND Professional help OR Intervention’’ AND “Overweight OR Obesity’’ AND ‘’Children OR Young People’’ NOT ‘Older people OR Adults’’ AND United Kingdom
- “Professional help OR Intervention’’ AND “Overweight OR Obesity’’ AND “Young Persons OR Children’’ NOT ‘Older people OR Adults’’ AND United Kingdom
With regards to wildcard search, the following strings were applied
- Child* AND Obese* AND Interven*
- Obese* AND Child* AND Interven*
- Interven* AND Child* AND Obese*
- Effect* AND Child* AND Obese* AND Interven*
The search for papers for this research matched the inclusion and exclusion criteria outlined in Table 2. The Cochrane Library database was the first to be searched, providing input on 38 publications. The MEDLINE database contained 43 articles, followed by CINAHL with 31, Web of Science with 28 articles, and PubMed with 36. 176 papers were obtained from all five databases. The papers in question were saved using the Zotero platform a bibliography management application.
Articles Screening
After completing the paper search and archiving, the researchers began scanning and screening. The first database search in a systematic or scope review generally yields a large number of irrelevant items that must be carefully but thoroughly screened. As a result, the 176 objects underwent a comprehensive scanning and screening process. This was done again following the predetermined guidelines for inclusion and exclusion. First, after searching five databases, several overlaps were discovered (i.e., certain publications were counted twice). This is primarily due to the ability to extract an article from two or more databases. As such, the first scanning process consisted of removing duplicates or triplicates, leaving only one copy. This approach resulted in the removal of 58 papers from the 176, retaining 118 reports that advanced to the first round of screening.
The first screening stage required thoroughly reviewing the papers stored in Zotero to look for paper abstracts and titles that did not correspond with this research’s aims. Another 43 papers were excluded. For instance, some studies mentioned interventions that were not particular regarding child obesity but rather addressed adult obesity or other medical conditions. Other studies that addressed the causes and effects of obesity did not match the inclusion requirements. In general, only 75 papers advanced to the next stage of screening. In the following phase, the researchers concentrated on removing papers whose publication year did not fit the inclusion requirements. As such, every paper published before 2014 (8 articles) was eliminated, resulting in only 67 publications. Of the 67 papers, 11 possessed all the elements required for a thorough review. Still, it focused on obesity in developing nations or high-income nations other than England, Scotland, Wales, and Northern Ireland, comprising the United Kingdom. Another 10 items were either white papers, books, book sections, or year reports, which are often not peer-reviewed. As a result, 21 papers were eliminated simultaneously based on their location and nature, retaining 46 reports. Among the 46 papers that eventually made it to the final screening phases, 9 publications were identified to have been published in Afrikaans or Korean, 8 were narrative or systematic reviews, and another 10 were published in predatory journals. Figure 2 depicts the methods for scanning and screening (resulting in a final 19 publications) adopting the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
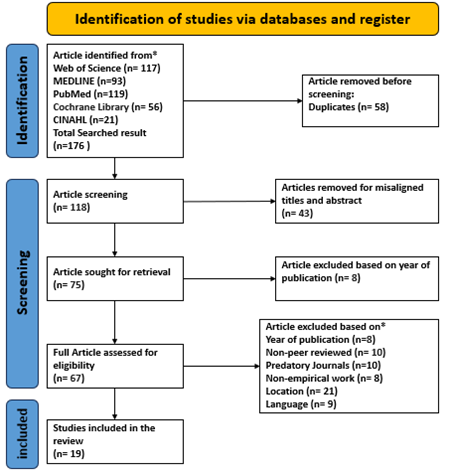
Figure 2. PRISMA flowchart for article screening
RESULTS
Data extraction (see Table 3) from the selected studies reveals approximately five interventions used to manage or control childhood obesity in different parts of the UK (see Appendix 1 for more information on the selected papers). These interventions either take place in the child’s school, at home [80], within the community [81], in places of worship [82], or are nationally directed [83], so that the naming convention follows where they are implemented. For example, school-based are carried out in the school, family or home-based are implemented at home, etc. Interventions are generally implemented
Table 3. Data extraction from searched articles
| Author | Intervention type | Location | Research method | Sample | Measure | Intervention tool |
| [84] | School-based | About a dozen districts in Lancashire | RCT | Mother and child only | BMI | Healthy Heroes |
| [81] | Community-based | Golborne area of Greater Manchester, England | Qualitative | Child, mother, and any school-based Stakeholder | Height and weight | Go-Golborne |
| [83] | National | England | Quantitative | Child and any young adults within the home or wider community | BMI | National Institute of Health and Care Excellence guidelines |
| [85] | School-based | Southwest, England | Qualitative | Child only | BMI | Healthy Lifestyles Programme (HeLP) |
| [86] | School-based | Southwest, England | RCT | Child only | BMI | Healthy Lifestyles Programme (HeLP) |
| [87] | School-based | West Midlands | RCT | Child only | BMI | WAVES |
| [88] | School-based | Southwest, England | RCT | Child only | BMI | The Active for Life Year 5 |
| [89] | School-based | Birmingham | RCT | Child only | BMI | The Birmingham Healthy Eating and Active Lifestyle for Children Study |
| [90] | Community-based | London | Quantitative | Child only | Physical activities and diet | The Diet and Active Living (DEAL) exploratory phase of obesity intervention |
| [91] | National | Birmingham | Qualitative | Child, mother, and any school-based Stakeholder | Physical activities | Analysis Grid for Environments Linked to Obesity (ANGELO) framework |
| [82] | Family/home-based | Bradford and Birmingham | Qualitative | Children, mothers, fathers, and other stakeholders (e.g., religious leaders) | Physical activities and diet | – |
| [92] | Family/home-based | Southwest, England | RCT | Child only | BMI | Healthy Lifestyles Programme (HeLP) |
| [93] | Community-based | Bradford | Mixed-method | Mother and child only | BMI | Healthy and Active Parenting Programme for Early Years (HAPPY) (Intervention Mapping) |
| [94] | School-based | Southwest, England | RCT | Child only | Physical activities | The Active for Life Year 5 |
| [95] | Family/home-based | Scotland | Mixed-method | Child only | BMI | Healthy Habits, Happy Homes Scotland (4H-S) |
| [96] | School-based | Scotland | RCT | Child only with a professional | BMI | ToyBox-Scotland |
| [97] | Family/home-based | Northeastern and Southwestern parts of England | Qualitative | Child, mother, and any school-based Stakeholder, and a professional | Not applicable | – |
| [98] | School-based | The northwestern part of England | Qualitative | Not specified | Not applicable | Mind, Exercise, Nutrition…Do It! (MEND) 7-13 programme |
| [99] | Family/home-based | The northwestern part of England | Mixed-method | Both parents and child | Dietary behavioral changes | Getting Our Active Lifestyles Started (GOALS) |
RCT-Randomized Controlled Trials, BMI-Body Mass Index
using tools or frameworks. For example, Healthy Heroes, Go-Golborne (with RE-AIM framework), Guideline of the National Institute of Health and Care Excellence (NICE), Healthy Lifestyles Programme (HeLP), WAVES, The Active for Life Year 5 (AFLY5), ToyBox-Scotland, Mind, Exercise, Nutrition…Do It! (MEND) 7-13 program, Getting Our Active Lifestyles Started (GOALS) etc. Of all the frameworks adopted within childhood obesity interventions, the Healthy Lifestyles Programme is the UK’s most prominently used. Furthermore, the frameworks adopt procedures that ensure that implementers can link intervention outcomes to the procedures adopted. For instance, HeLP is typically implemented in UK schools and uses behavioral change [85]. By implication, implementation would typically encourage teachers who are crucial stakeholders on the program, to train children on how to make healthier choices with regards to meals. This means that the focal person is the child, and the implementers try all they can to wield some influence on him/her through instilling of discipline on meal choices capable of combating obesity as well as encouraging parents to act as role models [87]. Overall, behavioral change in this instance would imply that the child gives preferences to physical activities
A popular step amongst childhood obesity intervention implementers is the involvement of other individuals to ensure the success of the programs. For example, in interventions based in schools, at least one parent and one teacher are usually present. The same can be said of interventions implemented at home where the mother of the obese child or any other close relative is present, as well as community and religious leaders for programs carried out within the immediate community or at worship centers respectively. Findings also reveal that programs carried out in the school as well as those around the home are the most popular and contribute about 80% of the reported interventions. This is justifiable mainly because the average child typically tends to spend more time at these places and, hence, learns the first eating habits from parents and/or teachers (in cases where meals are served in school)
Concerning the challenges of childhood obesity interventions in the UK, a major finding is the use of body mass index (BMI) as a yardstick to determine normal weight and overweight/obesity. At least 12 of the selected articles focused on this idea. Hence, BMI before and after the intervention was the basis to conclude the success or failure of the program. According to [100], BMI refers to a person’s weight-height ratio in anthropometric terms per. Square metre. Nevertheless, this measure of a person’s weight has been the subject of significant research backlash, as some authors have argued that the BMI calculation does not fully consider fat to muscle mass. As another noteworthy challenge, context is a fundamental factor that determines whether a program will lead to success or failure. This is so because while some interventions performed well in some settings [92] e.g., South-west England, these successes could not be replicated in others [80], e.g., Devon and Plymouth. One way to explain this challenge is to think around the overarching influence of context in the public health sphere [101], so that a childhood obesity intervention that perf program that succeeded in a community A, may be flawed in another community, B. Apart from the issue of context potentially intervention, as slight differences in their ages may also influence outcomes. Nevertheless, the research by [92] as well as that of [80] adopted similar children age group of 9-10 years.
Apart from the variation in some intervention outcomes in separate locations, some intervention tools have consistently failed regardless of the setting. For example, [88] report that the Active for Life Year-5 did not change the obesity status of children participants with regards to leading them to take up physical activities, shun sedentary lifestyles, or develop the habit of eating fruits and vegetables. The study by [94] found the same results just less than five years later. A major surprise is that even though the studies were two years apart, the location did not change and remained southwest England, and the participants’ ages also were the same (8-9 years old) baseline and (9- 10 years) old) end line. A potential reason is that behavior change did not occur over the period, as 2years may be quite short for any drastic behavior change to happen. As in the case of the Active for Life Year-5 framework, the WAVES framework as adopted by [87] also did not produce any significant changes amongst school children when combined with home-based interventions across more than 50 schools. An intervention implemented in West Midlands, the study adopted children between 5-6years of age but no improvement in diet nor physical activities was recorded at the end of the intervention.
DISCUSSION
Themes found from study review
The results section has focused extensively on what the different selected studies contribute the current one. Albeit, this section goes a step further to discuss in clear terms, the thematic areas found. As listed below, the themes perceived from the articles are:
- Childhood obesity interventions are complex and may not always produce positive results
- School-based childhood obesity interventions are not the only solutions
- BMI may be unreliable in childhood obesity interventions
The complexity of interventions for controlling and managing childhood obesity
The findings from the reviewed literature domiciled in the UK show how complex childhood obesity interventions are. Specifically, it details the fact that a one-size-fits-all approach may never yield the desired results. The reason for this is the uniqueness of communities and family make-up which are fundamental aspects of context (differences in culture and religion). A notable finding that clarifies this assertion is the failure of HeLP in one setting and its success in another. Even though Plymouth where the intervention by [80] was implemented and failed is located in southwest England, there may also have been a part of the study by [80] where the intervention succeeded. This is rightly so because [80] did not specify the part of the southwest of England where the research was carried out. Apart from focusing on the child, [80] involved parents in their intervention procedure. This may have led to a positive outcome given that [89] maintained how important it is for implementers of school-based interventions not to ignore components of the broader society when the need arises to get better outcomes. There is a chance that culture may also play a role in shaping the differences in results in both areas where the interventions were implemented.
The complexity of childhood obesity interventions is further deepened in that regardless of whether stakeholders all combine through a wholesome approach, this does not directly guarantee that the success of the intervention is certain. The reason for this is that successful childhood obesity interventions are nuanced and hinge on many different considerations that ultimately impact results. One critical factor is the length of time for which the intervention is implemented and whether the implementers considered a follow-up on the children after the initial phase. Overall, when a childhood obesity intervention is too short, gathering sufficient evidence may be far-fetched. Similarly, when it takes too long a time, the attrition rate may be high.
School-based childhood obesity interventions are not the only solutions
There seems to be an excessive focus on schools as a perceived best setting for childhood obesity interventions in the UK. Whilst this is understandable given the time the child spends at school; it does not necessarily mean that successful interventions cannot happen in other places as noticed across some of the reviewed articles. The massive focus on schools is linkable to the existence of a school feeding program which makes it easy to implement interventions. Nevertheless, we found that there is an increasing rate of failed school-based interventions [88], [89], [94], [80]. Surprisingly, whilst there were several other interventions domiciled at home and in the community, there was never a mention of failed interventions in any of these settings. This is why some authors have suggested the need to involve individuals from the wider society through the wholesome method.
The unreliable nature of body mass index
A popular finding across the literature reviewed is the adoption of body mass index as the standard for determining normal weight or obesity. Unfortunately, many researchers have criticized this approach and have suggested other techniques with high level of accuracy. These new methods such as waist-to-hip ratio and waist circumference are likely to better ascertain whether a child is truly losing weight in an intervention. According to the study by [102], body mass index does not consider the body-fat/muscle comparison which is fundamental in obesity calculation. The authors further noted that when used for obesity measurement, a person who exercises daily and trains the muscles may likely be tagged as fat. In addition, [103] reports that body mass index was never designed as a measure for health or any other health-related purpose. Adolphe Quetelet who came up with the idea of body mass index was mainly keen to understand certain physical characteristics of an average individual, hence took a sample of many Belgians. The scholar therefore failed to consider persons of different ethnicities whose stature and make-up may differ significantly from the Belgians [103]. Overall, [104] suggest that body mass index does not duly consider the spread of body fat around the human body. Based on some of the identified flaws of body mass index which was adopted as the primary source of childhood obesity measurement across the reviewed studies, the accuracy of these studies can be contested, given that some researchers have tagged the use of body mass index as unethical within public health discourse [105].
Lessons for public health practitioners in developing climes
There is much to learn for public health practitioners in developing countries seeking to implement CHO-I. As revealed by this study, there is a need for a critical appraisal of certain facts that may turn out incorrect. One such is using dietary changes in school feeding programs to combat childhood obesity. Even though this may be a good idea, this study has shown that such planning must involve the parents and where necessary community representatives. This is mainly because while the child’s meals are well-planned in the school, without the parents in the picture, there is a chance that the child may be served unhealthy meals at home. Aside from focusing largely on the school, this study perceives religious, community, and home-based interventions as superior to the school-based ones. While this assertion is yet to be established, it is noteworthy to emphasize that none of the interventions carried out in religious settings, communities or at home reported failure. Given that a large percentage of persons in many developing countries (e.g., Nigeria) prioritize religion [106], religious leaders could be pivotal in raising awareness of the dangers associated with childhood obesity as well as participate actively in interventions.
Regarding the standardization of CHO measurement and the adoption of tools to do so, this study has revealed the shortcomings associated with the use of body mass index in the UK. As a result, proponents of CHO interventions in developing countries may look to adopt other more accurate measures. This helps to increase the accuracy level of CHO-I programs, thereby positively influencing intervention outcomes. Lastly, [107] explained that undermining the importance of context in public health interventions may be detrimental to primary healthcare programs designed to strengthen health systems. Hence, in the planning of CHO-I programs, implementers must fully understand and preempt the possibilities of significant changes in response and outcome across different communities.
CONCLUSIONS
Within the framework of global and public health discourse, child health remains a priority given the vulnerability of children to many known diseases which leads to increasing morbidity and mortality statistics. This study which evaluates interventions of CHO in the UK with the intent to draw up lessons for practitioners in resource-scarce nations has revealed that adhering to certain existing practices and standards without taking into cognizance their associated shortcomings may affect intervention outcomes. Nevertheless, in circumstances where the goal is to strengthen health systems, several lessons abound with regard to practices around interventions in general, and CHO-I in particular. Future researchers may concentrate on developing and evaluating culturally adapted interventions that tackle the unique environmental and socioeconomic circumstances of different demographics. Investigating the efficacy of multisectoral methods that include communities, schools, and policymakers is critical. Also, longitudinal research studies are required to understand the long-term implications of early-life obesity treatments. Furthermore, further studies can look into the function of technology, like mobile health apps and telemedicine, in encouraging healthy behaviours. Finally, studying the genetic and epigenetic components contributing to obesity may offer insights into individualised preventive and treatment techniques.
REFERENCES
- Hruby and F. B. Hu, (2015). The Epidemiology of Obesity: A Big Picture, PharmacoEconomics, vol. 33, no. 7, pp. 673–689, doi: 10.1007/s40273-014-0243-x.
- Templin, T. Cravo Oliveira Hashiguchi, B. Thomson, J. Dieleman, and E. Bendavid, (2019). The overweight and obesity transition from the wealthy to the poor in low- and middle-income countries: A survey of household data from 103 countries, PLoS Med., vol. 16, no. 11, doi: 10.1371/journal.pmed.1002968.
- Dinsa, Y. Goryakin, E. Fumagalli, and M. Suhrcke,(2012). Obesity and socioeconomic status in developing countries: a systematic review, Obes. Rev., vol. 13, no. 11, pp. 1067–1079, doi: 10.1111/j.1467-789X.2012.01017.x.
- WHO, (2024). Obesity and overweight. Accessed: May 22, 2024. [Online]. Available: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
- National Health Service,(2024). Statistics on Obesity, Physical Activity and Diet, England, 2020, NHS England Digital. Accessed: May 22. [Online]. Available: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-obesity-physical-activity-and-diet/england-2020
- T. Cote, K. C. Harris, C. Panagiotopoulos, G. G. S. Sandor, and A. M. Devlin, (2013) Childhood obesity and cardiovascular dysfunction, J. Am. Coll. Cardiol., vol. 62, no. 15, pp. 1309–1319, Oct. doi: 10.1016/j.jacc.2013.07.042.
- Narang and J. L. Mathew, (2012). Childhood obesity and obstructive sleep apnea, Nutr. Metab., vol. 2012, p. 134202, doi: 10.1155/2012/134202.
- Minos, (2020).‘Eat, my child.’ Obesity among children in developing countries: Evidence from South Africa, Rev. Dev. Econ., vol. 24, no. 4, pp. 1300–1311, doi: 10.1111/rode.12696.
- M. Fruh, (2020). Obesity: Risk factors, complications, and strategies for sustainable long‐term weight management, J. Am. Assoc. Nurse Pract., vol. 29, no. Suppl 1, pp. S3–S14, Oct. x, doi: 10.1002/2327-6924.12510.
- Sanyaolu, C. Okorie, X. Qi, J. Locke, and S. Rehman,(2019). Childhood and Adolescent Obesity in the United States: A Public Health Concern, Glob. Pediatr. Health, vol. 6, p. 2333794X19891305, Dec. doi: 10.1177/2333794X19891305.
- R. Carey, G. K. Singh, H. S. Brown III, and A. V. Wilkinson,(2015). Educational outcomes associated with childhood obesity in the United States: cross-sectional results from the 2011–2012 National Survey of Children’s Health,.Int. J. Behav. Nutr. Phys. Act., vol. 12, no. 1, p. S3, Jul., doi: 10.1186/1479-5868-12-S1-S3.
- Llewellyn, M. Simmonds, C. G. Owen, and N. Woolacott,(2016). Childhood obesity as a predictor of morbidity in adulthood: a systematic review and meta-analysis, Obes. Rev., vol. 17, no. 1, pp. 56–67, doi: 10.1111/obr.12316.
- J. Morales Camacho, J. M. Molina Díaz, S. Plata Ortiz, J. E. Plata Ortiz, M. A. Morales Camacho, and B. P. Calderón,(2019). Childhood obesity: Aetiology, comorbidities, and treatment, Diabetes Metab. Res. Rev., vol. 35, no. 8, p. e3203, doi: 10.1002/dmrr.3203.
- Poorolajal, F. Sahraei, Y. Mohamdadi, A. Doosti-Irani, and L. Moradi, (2020). Behavioral factors influencing childhood obesity: a systematic review and meta-analysis, Obes. Res. Clin. Pract., vol. 14, no. 2, pp. 109–118, Mar. doi: 10.1016/j.orcp.2020.03.002.
- Qiao et al., (2015) “Birth weight and childhood obesity: a 12-country study,” Int. J. Obes. Suppl., vol. 5, no. 2, pp. S74–S79, Dec. doi: 10.1038/ijosup.2015.23.
- K. Chrissini and D. B. Panagiotakos, (2022). Public health interventions tackling childhood obesity at European level: A literature review,” Prev. Med. Rep., vol. 30, p. 102068, Dec. doi: 10.1016/j.pmedr.2022.102068.
- M. Viner et al., (2020). Improving the assessment and management of obesity in UK children and adolescents: the PROMISE research programme including a RCT, Programme Grants Appl. Res., vol. 8, no. 3, Art. no. 3, Apr.
- Van Staden,(2019). A longitudinal study on the effect of overweight, obesity, stunting and wasting on academic performance of primary school boys: the NW-CHILD study, Thesis, North-West University. Accessed: May 21, 2024. [Online]. Available: https://repository.nwu.ac.za/handle/10394/34101
- Conor,(2019). “Prevalence of childhood obesity in the UK 2016, Statista. Accessed: May 21, 2024. [Online]. Available: https://www.statista.com/statistics/1017560/prevalence-of-childhood-obesity-in-the-uk/
- M. Fruh,(2017). Obesity: Risk factors, complications, and strategies for sustainable long‐term weight management, J. Am. Assoc. Nurse Pract., vol. 29, no. S1, p. S3, Oct., doi: 10.1002/2327-6924.12510.
- Forsén, J. Eriksson, J. Tuomilehto, A. Reunanen, C. Osmond, and D. Barker, (2000). The Fetal and Childhood Growth of Persons Who Develop Type 2 Diabetes, Ann. Intern. Med., vol. 133, no. 3, pp. 176–182, Aug., doi: 10.7326/0003-4819-133-3-200008010-00008.
- Chen, D. J. Magliano, and P. Z. Zimmet, (2000). The worldwide epidemiology of type 2 diabetes mellitus—present and future perspectives, Nat. Rev. Endocrinol., vol. 8, no. 4, pp. 228–236, Apr. 2012, doi: 10.1038/nrendo.2011.183.
- [V. Bellou, L. Belbasis, I. Tzoulaki, and E. Evangelou,(2018). Risk factors for type 2 diabetes mellitus: An exposure-wide umbrella review of meta-analyses, PLOS ONE, vol. 13, no. 3, p. e0194127, Mar., doi: 10.1371/journal.pone.0194127.
- Al-Beltagi, A. S. Bediwy, and N. K. Saeed, (2022).Insulin-resistance in paediatric age: Its magnitude and implications,” World J. Diabetes, vol. 13, no. 4, pp. 282–307, Apr., doi: 10.4239/wjd.v13.i4.282.
- Serbis, V. Giapros, S. A. Paschou, and E. Siomou, (2021). Children with metabolically healthy obesity have a worse metabolic profile compared to normal-weight peers: a cross-sectional study, Endocrine, vol. 73, no. 3, pp. 580–587, Sep., doi: 10.1007/s12020-021-02762-6.
- T. Nga et al., (2019).School education and childhood obesity: A systemic review, Diabetes Metab. Syndr. Clin. Res. Rev., vol. 13, no. 4, pp. 2495–2501, Jul., doi: 10.1016/j.dsx.2019.07.014.
- Herouvi, E. Karanasios, C. Karayianni, and K. Karavanaki, (2013).Cardiovascular disease in childhood: the role of obesity, Eur. J. Pediatr., vol. 172, no. 6, pp. 721–732, Jun., doi: 10.1007/s00431-013-1932-8.
- L. Marcus et al., (2012). Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome, Pediatrics, vol. 130, no. 3, pp. e714–e755, Sep., doi: 10.1542/peds.2012-1672.
- J. Towbin, (2022). Chapter 7 – Musculoskeletal,” in Fundamentals of Pediatric Imaging (Third Edition), L. F. Donnelly, Ed., Academic Press, pp. 175–256. doi: 10.1016/B978-0-12-822255-3.00009-5.
- Liu, C. Mu, K. Li, H. Luo, Y. Liu, and Z. Li, (2021). Estimating Global Prevalence of Metabolic Dysfunction-Associated Fatty Liver Disease in Overweight or Obese Children and Adolescents: Systematic Review and Meta-Analysis, Int. J. Public Health, vol. 66, p. 1604371, Oct., doi: 10.3389/ijph.2021.1604371.
- Drummond, G. Stratton, and J. Cade, (2018). Public health and the prevention of obesity, in Advanced Nutrition and Dietetics in Obesity, John Wiley & Sons, Ltd, pp. 329–354. doi: 10.1002/9781118857991.ch7.
- Luli et al., (2023). The implications of defining obesity as a disease: a report from the Association for the Study of Obesity 2021 annual conference, eClinicalMedicine, vol. 58, Apr., doi: 10.1016/j.eclinm.2023.101962.
- Scarborough, P. Bhatnagar, K. K. Wickramasinghe, S. Allender, C. Foster, and M. Rayner,(2011). The economic burden of ill health due to diet, physical inactivity, smoking, alcohol and obesity in the UK: an update to 2006–07 NHS costs, J. Public Health, vol. 33, no. 4, pp. 527–535, Dec., doi: 10.1093/pubmed/fdr033.
- P. T. James and K. McPherson, (2017). The costs of overweight, Lancet Public Health, vol. 2, no. 5, pp. e203–e204, May, doi: 10.1016/S2468-2667(17)30068-3.
- Rankin et al.,(2016). Psychological consequences of childhood obesity: psychiatric comorbidity and prevention, Adolesc. Health Med. Ther., vol. 7, pp. 125–146, Nov., doi: 10.2147/AHMT.S101631.
- H. Sanders, A. Han, J. S. Baker, and S. Cobley,(2015). Childhood obesity and its physical and psychological co-morbidities: a systematic review of Australian children and adolescents, Eur. J. Pediatr., vol. 174, no. 6, pp. 715–746, Jun., doi: 10.1007/s00431-015-2551-3.
- Aparicio, J. Canals, V. Arija, S. D. Henauw, and N. Michels, (2016).The role of emotion regulation in childhood obesity: implications for prevention and treatment, Nutr. Res. Rev., vol. 29, no. 1, pp. 17–29, Jun., doi: 10.1017/S0954422415000153.
- J. Pont, R. Puhl, S. R. Cook, and W. Slusser,(2017). Stigma Experienced by Children and Adolescents With Obesity, SECTION ON OBESITY, and THE OBESITY SOCIETY,Pediatrics, vol. 140, no. 6, p. e20173034, Dec., doi: 10.1542/peds.2017-3034.
- E. Vazquez and C. Cubbin, (2020). Socioeconomic Status and Childhood Obesity: a Review of Literature from the Past Decade to Inform Intervention Research, Curr. Obes. Rep., vol. 9, no. 4, pp. 562–570, Dec., doi: 10.1007/s13679-020-00400-2.
- Sagar and T. Gupta, (2018). Psychological Aspects of Obesity in Children and Adolescents, Indian J. Pediatr., vol. 85, no. 7, pp. 554–559, Jul., doi: 10.1007/s12098-017-2539-2.
- Sahoo, B. Sahoo, A. K. Choudhury, N. Y. Sofi, R. Kumar, and A. S. Bhadoria, (2015). Childhood obesity: causes and consequences,” J. Fam. Med. Prim. Care, vol. 4, no. 2, p. 187, Jun., doi: 10.4103/2249-4863.154628.
- Kokka, I. Mourikis, and F. Bacopoulou, (2023). “Psychiatric Disorders and Obesity in Childhood and Adolescence—A Systematic Review of Cross-Sectional Studies,” Children, vol. 10, no. 2, Art. no. 2, Feb., doi: 10.3390/children10020285.
- Öz and A. C. Kıvrak, (2023). Evaluation of depression, anxiety symptoms, emotion regulation difficulties, and self-esteem in children and adolescents with obesity, Arch. Pédiatrie, vol. 30, no. 4, pp. 226–231, May, doi: 10.1016/j.arcped.2023.02.003.
- Zilanawala, P. Davis-Kean, J. Nazroo, A. Sacker, S. Simonton, and Y. Kelly, (2015).Race/ethnic disparities in early childhood BMI, obesity and overweight in the United Kingdom and United States, Int. J. Obes., vol. 39, no. 3, Art. no. 3, Mar., doi: 10.1038/ijo.2014.171.
- T. Leon Guerrero et al.,(2020). Prevalence and Predictors of Overweight and Obesity among Young Children in the Children’s Healthy Living Study on Guam, Nutrients, vol. 12, no. 9, Art. no. 9, Sep., doi: 10.3390/nu12092527.
- A. Isong, S. R. Rao, M.-A. Bind, M. Avendaño, I. Kawachi, and T. K. Richmond, (2018). Racial and Ethnic Disparities in Early Childhood Obesity, Pediatrics, vol. 141, no. 1, p. e20170865, Jan., doi: 10.1542/peds.2017-0865.
- C. Skinner and J. A. Skelton, (2014). Prevalence and Trends in Obesity and Severe Obesity Among Children in the United States, 1999-2012, JAMA Pediatr., vol. 168, no. 6, pp. 561–566, Jun., doi: 10.1001/jamapediatrics.2014.21.
- D. Guerrero, C. Mao, B. Fuller, M. Bridges, T. Franke, and A. A. Kuo, (2016). Racial and Ethnic Disparities in Early Childhood Obesity: Growth Trajectories in Body Mass Index, J. Racial Ethn. Health Disparities, vol. 3, no. 1, pp. 129–137, Mar., doi: 10.1007/s40615-015-0122-y.
- Assari, (2018). Family Income Reduces Risk of Obesity for White but Not Black Children, Children, vol. 5, no. 6, Art. no. 6, Jun., doi: 10.3390/children5060073.
- Rogers et al., (2015). The Relationship between Childhood Obesity, Low Socioeconomic Status, and Race/Ethnicity: Lessons from Massachusetts, Child. Obes., vol. 11, no. 6, pp. 691–695, Dec., doi: 10.1089/chi.2015.0029.
- C. Chooi, C. Ding, and F. Magkos, (2019). The epidemiology of obesity, Metabolism, vol. 92, pp. 6–10, Mar., doi: 10.1016/j.metabol.2018.09.005.
- E. Mason, A. Alexiou, D. L. Bennett, C. Summerbell, B. Barr, and D. Taylor-Robinson, (2021). Impact of cuts to local government spending on Sure Start children’s centres on childhood obesity in England: a longitudinal ecological study, J Epidemiol Community Health, vol. 75, no. 9, pp. 860–866, Sep., doi: 10.1136/jech-2020-216064.
- R. z. Theis and M. White, (2021). Is Obesity Policy in England Fit for Purpose? Analysis of Government Strategies and Policies, 1992–2020, Milbank Q., vol. 99, no. 1, pp. 126–170, doi: 10.1111/1468-0009.12498.
- Belc, I. Smeu, A. Macri, D. Vallauri, and K. Flynn, (2019). Reformulating foods to meet current scientific knowledge about salt, sugar and fats, Trends Food Sci. Technol., vol. 84, pp. 25–28, Feb., doi: 10.1016/j.tifs.2018.11.002.
- A. Chesham et al., (2018). The Daily Mile makes primary school children more active, less sedentary and improves their fitness and body composition: a quasi-experimental pilot study, BMC Med., vol. 16, no. 1, p. 64, May, doi: 10.1186/s12916-018-1049-z.
- [56] Adab et al., (2018). Effectiveness of a childhood obesity prevention programme delivered through schools, targeting 6 and 7-year-olds: cluster randomised controlled trial (WAVES study), BMJ, vol. 360, p. k211, Feb., doi: 10.1136/bmj.k211.
- Fleming-Milici and J. L. Harris, (2020). Food marketing to children in the United States: Can industry voluntarily do the right thing for children’s health?,Physiol. Behav., vol. 227, p. 113139, Dec., doi: 10.1016/j.physbeh.2020.113139.
- George, (2019). Not so sweet refrain: sugar-sweetened beverage taxes, industry opposition and harnessing the lessons learned from tobacco control legal challenges, Health Econ. Policy Law, vol. 14, no. 4, pp. 509–535, Oct., doi: 10.1017/S1744133118000178.
- Forde, (2021). Changes to marketing in response to sugary beverage taxation: the Soft Drinks Industry Levy in the United Kingdom, Aug., Accessed: May 22, 2024. [Online]. Available: https://www.repository.cam.ac.uk/handle/1810/326405
- A. Roache, C. Platkin, L. O. Gostin, and C. Kaplan, (2018). Big Food and Soda versus Public Health: Industry Litigation against Local Government Regulations to Promote Healthy Diets, Fordham Urban Law J., vol. 45, p. 1051, 2017.
- A. Dana and J. Nadler, (2018). Soda Taxes as a Legal and Social Movement, Northwest. J. Law Soc. Policy, vol. 13, p. 84, 2017.
- Falkner and N. D. F. H. Cossrow, (2014). Prevalence of Metabolic Syndrome and Obesity-Associated Hypertension in the Racial Ethnic Minorities of the United States, Curr. Hypertens. Rep., vol. 16, no. 7, p. 449, May, doi: 10.1007/s11906-014-0449-5.
- Stryjecki, A. Alyass, and D. Meyre, (2018). Ethnic and population differences in the genetic predisposition to human obesity, Obes. Rev., vol. 19, no. 1, pp. 62–80, doi: 10.1111/obr.12604.
- C. Skinner, S. N. Ravanbakht, J. A. Skelton, E. M. Perrin, and S. C. Armstrong, (2018). Prevalence of Obesity and Severe Obesity in US Children, 1999–2016, Pediatrics, vol. 141, no. 3, p. e20173459, Mar., doi: 10.1542/peds.2017-3459.
- C. Jambholkar, A. Joshi, and S. G. Choudhari, (2024). Addressing the Challenge: A Review of Effective Prevention Strategies for Childhood Obesity in India, Cureus, vol. 16, no. 3, p. e56257, doi: 10.7759/cureus.56257.
- M. Popkin, C. Corvalan, and L. M. Grummer-Strawn, (2020). Dynamics of the double burden of malnutrition and the changing nutrition reality, The Lancet, vol. 395, no. 10217, pp. 65–74, Jan., doi: 10.1016/S0140-6736(19)32497-3.
- S. Kulkarni, V. S. Kulkarni, and R. Gaiha, (2017). ‘Double Burden of Malnutrition’: Reexamining the Coexistence of Undernutrition and Overweight Among Women in India, Int. J. Health Serv., vol. 47, no. 1, pp. 108–133, Jan., doi: 10.1177/0020731416664666.
- S. Guldan, (2020).Undernutrition and Overnutrition: The Challenging Double Burden of Malnutrition, in Good Health and Well-Being, W. Leal Filho, T. Wall, A. M. Azul, L. Brandli, and P. G. Özuyar, Eds., Cham: Springer International Publishing, pp. 747–759. doi: 10.1007/978-3-319-95681-7_50.
- Mahmudiono, C. Segalita, and R. R. Rosenkranz, (2019). Socio-Ecological Model of Correlates of Double Burden of Malnutrition in Developing Countries: A Narrative Review,” Int. J. Environ. Res. Public. Health, vol. 16, no. 19, Art. no. 19, Jan., doi: 10.3390/ijerph16193730.
- HAWKES, J. HARRIS, and S. GILLESPIE, (2017). Urbanization and the Nutrition Transition., Accessed: May 21, 2024. [Online]. Available: https://core.ac.uk/reader/237086590
- C. Tricco et al., (2016). A scoping review on the conduct and reporting of scoping reviews, BMC Med. Res. Methodol., vol. 16, no. 1, p. 15, Feb., doi: 10.1186/s12874-016-0116-4.
- K. Anderson, E. Howarth, M. Vainre, A. Humphrey, P. B. Jones, and T. J. Ford, (2020). “Advancing methodology for scoping reviews: recommendations arising from a scoping literature review (SLR) to inform transformation of Children and Adolescent Mental Health Services,” BMC Med. Res. Methodol., vol. 20, no. 1, p. 242, Sep., doi: 10.1186/s12874-020-01127-3.
- Arksey and L. O’Malley, (2005). Scoping studies: towards a methodological framework, Int. J. Soc. Res. Methodol., vol. 8, no. 1, pp. 19–32, Feb., doi: 10.1080/1364557032000119616.
- Levac, H. Colquhoun, and K. K. O’Brien, (2010). Scoping studies: advancing the methodology, Implement. Sci., vol. 5, no. 1, p. 69, Sep., doi: 10.1186/1748-5908-5-69.
- D. J. Peters et al., (2020). Updated methodological guidance for the conduct of scoping reviews, JBI Evid. Synth., vol. 18, no. 10, p. 2119, Oct., doi: 10.11124/JBIES-20-00167.
- Munn, M. D. J. Peters, C. Stern, C. Tufanaru, A. McArthur, and E. Aromataris, (2018). Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach, BMC Med. Res. Methodol., vol. 18, no. 1, p. 143, Nov., doi: 10.1186/s12874-018-0611-x.
- M. Bramer, M. L. Rethlefsen, J. Kleijnen, and O. H. Franco, (2017). Optimal database combinations for literature searches in systematic reviews: a prospective exploratory study, Syst. Rev., vol. 6, no. 1, p. 245, Dec., doi: 10.1186/s13643-017-0644-y.
- L. Morgan, P. Whaley, K. A. Thayer, and H. J. Schünemann, (2018). Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes, Environ. Int., vol. 121, no. Pt 1, p. 1027, Dec., doi: 10.1016/j.envint.2018.07.015.
- M. Patino and J. C. Ferreira, (2018). Inclusion and exclusion criteria in research studies: definitions and why they matter, J. Bras. Pneumol. Publicacao Of. Soc. Bras. Pneumol. E Tisilogia, vol. 44, no. 2, p. 84, Apr., doi: 10.1590/s1806-37562018000000088.
- Lloyd and K. Wyatt, (2015). The Healthy Lifestyles Programme (HeLP) — An Overview of and Recommendations Arising from the Conceptualisation and Development of an Innovative Approach to Promoting Healthy Lifestyles for Children and Their Families, Int. J. Environ. Res. Public. Health, vol. 12, no. 1, Art. no. 1, Jan., doi: 10.3390/ijerph120101003.
- W. Gadsby, S. Hotham, T. Eida, C. Lawrence, and R. Merritt, (2020). Impact of a community-based pilot intervention to tackle childhood obesity: a ‘whole-system approach’ case study, BMC Public Health, vol. 20, no. 1, p. 1818, Nov., doi: 10.1186/s12889-020-09694-2.
- A. Dogra, K. Rai, S. Barber, R. RC. McEachan, P. Adab, and L. Sheard, (2021). Delivering a childhood obesity prevention intervention using Islamic religious settings in the UK: What is most important to the stakeholders?,Prev. Med. Rep., vol. 22, p. 101387, Jun., doi: 10.1016/j.pmedr.2021.101387.
- J. Russell, O. T. Mytton, and R. M. Viner, (2023). Estimating the effects of preventive and weight-management interventions on the prevalence of childhood obesity in England: a modelling study, Lancet Public Health, vol. 8, no. 11, pp. e878–e888, Nov., doi: 10.1016/S2468-2667(23)00216-5.
- Hodgkinson, J. Abbott, M. A. Hurley, N. Lowe, and P. Qualter, (2019). An educational intervention to prevent overweight in pre-school years: a cluster randomised trial with a focus on disadvantaged families, BMC Public Health, vol. 19, no. 1, p. 1430, Nov., doi: 10.1186/s12889-019-7595-2.
- Lloyd et al., (2013). Effectiveness of the Healthy Lifestyles Programme (HeLP) to prevent obesity in UK primary-school children: a cluster randomised controlled trial, Lancet Child Adolesc. Health, vol. 2, no. 1, pp. 35–45, Jan. 2018, doi: 10.1016/S2352-4642(17)30151-7.
- M. Wyatt et al., “The Healthy Lifestyles Programme (HeLP), a novel school-based intervention to prevent obesity in school children: study protocol for a randomised controlled trial,” Trials, vol. 14, no. 1, p. 95, Apr., doi: 10.1186/1745-6215-14-95.
- Adab et al., (2018). Effectiveness of a childhood obesity prevention programme delivered through schools, targeting 6 and 7 year olds: cluster randomised controlled trial (WAVES study), BMJ, vol. 360, p. k211, Feb., doi: 10.1136/bmj.k211.
- R. Kipping et al., (2014). Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: Active for Life Year 5 (AFLY5) school based cluster randomised controlled trial,” BMJ, vol. 348, p. g3256, May, doi: 10.1136/bmj.g3256.
- Adab et al.,(2014). Preventing childhood obesity, phase II feasibility study focusing on South Asians: BEACHeS, BMJ Open, vol. 4, no. 4, p. e004579, Apr., doi: 10.1136/bmjopen-2013-004579.
- Maynard, G. Baker, and S. Harding, (2017). Exploring childhood obesity prevention among diverse ethnic groups in schools and places of worship: Recruitment, acceptability and feasibility of data collection and intervention components, Prev. Med. Rep., vol. 6, pp. 130–136, Jun., doi: 10.1016/j.pmedr.2017.02.019.
- Pallan, J. Parry, K. K. Cheng, and P. Adab, (2013). Development of a childhood obesity prevention programme with a focus on UK South Asian communities, Prev. Med., vol. 57, no. 6, pp. 948–954, Dec., doi: 10.1016/j.ypmed.2013.08.025.
- Lloyd, C. McHugh, J. Minton, H. Eke, and K. Wyatt, (2017). The impact of active stakeholder involvement on recruitment, retention and engagement of schools, children and their families in the cluster randomised controlled trial of the Healthy Lifestyles Programme (HeLP): a school-based intervention to prevent obesity, Trials, vol. 18, no. 1, p. 378, Aug., doi: 10.1186/s13063-017-2122-1.
- J. Taylor et al., (2013). Using intervention mapping to develop a culturally appropriate intervention to prevent childhood obesity: the HAPPY (Healthy and Active Parenting Programme for Early Years) study, Int. J. Behav. Nutr. Phys. Act., vol. 10, no. 1, p. 142, Dec., doi: 10.1186/1479-5868-10-142.
- A. Lawlor et al., (2016). The Active for Life Year 5 (AFLY5) school-based cluster randomised controlled trial: effect on potential mediators, BMC Public Health, vol. 16, no. 1, p. 68, Jan., doi: 10.1186/s12889-016-2734-5.
- Gillespie et al., (2020). Healthy Habits, Happy Homes Scotland (4HS) feasibility study: Translation of a home-based early childhood obesity prevention intervention evaluated using RE-AIM framework, Public Health Pract., vol. 1, p. 100026, Jun., doi: 10.1016/j.puhip.2020.100026.
- Malden et al., (2019). A feasibility cluster randomised controlled trial of a preschool obesity prevention intervention: ToyBox-Scotland,” Pilot Feasibility Stud., vol. 5, no. 1, p. 128, Nov., doi: 10.1186/s40814-019-0521-7.
- J. Lucas, K. Curtis-Tyler, L. Arai, S. Stapley, J. Fagg, and H. Roberts, (2014). What works in practice: user and provider perspectives on the acceptability, affordability, implementation, and impact of a family-based intervention for child overweight and obesity delivered at scale, BMC Public Health, vol. 14, no. 1, p. 614, Jun., doi: 10.1186/1471-2458-14-614.
- L. Turner, S. Owen, and P. M. Watson, (2016). Addressing childhood obesity at school entry: Qualitative experiences of school health professionals, J. Child Health Care, vol. 20, no. 3, pp. 304–313, Sep., doi: 10.1177/1367493515587061.
- M. Watson et al., (2015). Service evaluation of the GOALS family-based childhood obesity treatment intervention during the first 3 years of implementation, BMJ Open, vol. 5, no. 2, p. e006519, Feb., doi: 10.1136/bmjopen-2014-006519.
- Q. Nuttall, (2015). Body Mass Index: Obesity, BMI, and Health: A Critical Review, Nutr. Today, vol. 50, no. 3, p. 117, Jun., doi: 10.1097/NT.0000000000000092.
- Viehbeck, E. Di Ruggiero, and N. Edwards, (2015). The context for reporting on context in public health: An analysis of existing guidance and guidelines, Eur. J. Public Health, vol. 25, no. suppl_3, Oct., doi: 10.1093/eurpub/ckv167.027.
- Yang, Z. Xin, J.-P. Feng, and J.-K. Yang, (2017).Waist-to-height ratio is better than body mass index and waist circumference as a screening criterion for metabolic syndrome in Han Chinese adults, Medicine (Baltimore), vol. 96, no. 39, p. e8192, Sep., doi: 10.1097/MD.0000000000008192.
- Paddock, (2024). Waist To Height Ratio Better Than BMI, Medical News Today. Accessed: Feb. 24,. [Online]. Available: https://www.medicalnewstoday.com/articles/245328
- Khan et al., (2023). Surrogate Adiposity Markers and Mortality, JAMA Netw. Open, vol. 6, no. 9, p. e2334836, Sep., doi: 10.1001/jamanetworkopen.2023.34836.
- [105] Humphreys, (2010). The unethical use of BMI in contemporary general practice, Br. J. Gen. Pract., vol. 60, no. 578, pp. 696–697, Sep., doi: 10.3399/bjgp10X515548.
- B. Berkessel et al., (2021). National religiosity eases the psychological burden of poverty, Proc. Natl. Acad. Sci. U. S. A., vol. 118, no. 39, p. e2103913118, Sep., doi: 10.1073/pnas.2103913118.
- van Weel and M. R. Kidd, (2018). Why strengthening primary health care is essential to achieving universal health coverage, CMAJ Can. Med. Assoc. J., vol. 190, no. 15, pp. E463–E466, Apr., doi: 10.1503/cmaj.170784.
APPENDIX 1