
Effect of Devolved Financial Planning on Health Care Service Delivery in Meru Teaching and Referral Hospital.
- Paul Mutwiri Muthomi
- Dr. Judy Mwangi
- 195-211
- Nov 10, 2023
- Finance
Effect of Devolved Financial Planning on Health Care Service Delivery in Meru Teaching and Referral Hospital
Paul Mutwiri Muthomi1, Dr. Judy Mwangi2
1Master of Governance and Ethics, Mount Kenya University, Kenya
2Mount Kenya University, Kenya
DOI: https://doi.org/10.51244/IJRSI.2023.101019
Received: 09 October 2023; Accepted: 14 October 2023; Published: 10 November 2023
ABSTRACT
The Kenyan constitution of 2010 established a decentralized structure of government that upholds health as a fundamental right for every individual. Additionally, it specifies the national governments and county governments’ responsibilities for providing health services as well as the guidelines that should guide their delivery. It became imperative to address the administration, planning, and management of health services in response to the changes after the first general elections held in accordance with the Kenyan constitution (2010) and the establishment of County Governments. Notably, numerous Counties have been plagued with colossal problems including strikes, corruption, and delayed wages that have contributed to subpar service delivery, among other things. The purpose of this study was to analyze the effects of devolved governance on health care service delivery in Meru teaching and referral hospital in Kenya. The objectives of the study were; to examine the effect of devolved financial planning on health care service delivery in Meru teaching and referral hospital, to assess the effect of devolved heath infrastructure on health care service delivery in Meru teaching and referral hospital, to explore the effect of devolved staffing on health care service delivery in Meru teaching and referral hospital and to examine the effect of Policy Framework on service delivery in Meru teaching and referral hospital. The study was based on tanahashi health model and soufflé theory of 1995, and it employed a descriptive research design with a mixed methods targeting 1996 participants comprising of health care workers, at MTReH, outpatient patients visiting the facility, and members of the Meru County Assembly. The study adopted a stratified sampling forming 10 Statas of the respondents, a simple random sampling was subjected to the respondents in their respective Statas to pick the study participant. The study utilized questionnaires for various departments in the hospital and the MCA, interview guide for hospital administrator and CEO and a focus group discussion with the patients for data collection purposes. SPSS version 28 was used to analyze the coded data. The study used both descriptive and inferential statistics for data analysis. Descriptive statistics was presented inform of Mean, frequencies and standard deviations while regression and moment correlation was used for inferential statistics, data presentation was done by use of figures and tables
INTRODUCTION
Background of the study
Devolved governance is the transfer of authority from a senior level of government to a junior level (Tallon, 2020). It is seen as both a concept and a process when looked at theoretically and administratively. In the theoretical perspective, devolution is perceived as decolonization, which conforms to political development literature while, on the other hand, if it is viewed from the administrative perspective, education on devolution matters boosts conceptualization of the general changes in the constitution concerning governance issues. Moreover, devolution can as well be defined as the transfer of significant powers, authorities, and functions from the national government to the local government units where finances are subsequently disbursed for their operation like the central government (Muriisa, 2008).
According to Aslam and Yilmaz (2011) devolved governance has turn out to be the foundation of development reforms in many states with the importance of devolution highly supported and dependent on the political economy to improve service delivery. Lately, majority of developed and developing countries have devolved governance functions with the aim of delivering better services to the public, improving the management of public resources and also being accountable for the disbursed resources to strengthen economic development as well as improving equity in the service delivery (Smoke, 2015). Devolved governance has widely been accepted and embraced as the dominant player of good governance and countries’ economic development in the world.
Globally, the decentralized system of governance has produced a mixed bag of outcomes in terms of performance for the many kinds of local government that have been established. Performance of devolved units has been investigated by a number of academics. Bahl and Bird (2013) found that devolved units outperformed the central government in Colombia when it came to the financing of water projects and the management of water resources, according to their findings. When it comes to the devolution of political leadership to the grassroots in Chile, preserving key public services, such as maternal health, resulted in a negative influence on regional governments’ performance ratings in a study by Hinojosa and Franscechet (2012).
Public hospitals and local community dispensaries in Italy’s administrative areas were negatively affected by inequalities in financing levels for health care provision, according to Cicchetti and Gasbarrini (2016), based on data from Finland. When it comes to service delivery, Dickovick and Riedl (2010) found that although devolved government promised greater service delivery to citizens throughout the continent, individual devolved units in different nations have shown inconsistent outcomes in terms of their overall effectiveness and efficiency.
Sub-national governments in Nigeria exercised extensive discretion in the execution of fundamental components of the policy, according to Eboreime, Abimbola, and Obi (2017), notwithstanding the national government’s view that they were in conformity with the policy. More functional standards like “Finance,” which were completed by just 35 percent of states and “Human Resource Management,” which were met by only 30 percent were not completely complied with by any of the states studied. According to the implementation pattern, state governments may be more interested in executing low-hanging fruit in order to get access to federal incentives than in implementing to improve performance.
Following the implementation of devolved governance in healthcare in Kenya and Indonesia, the two nations faced comparable issues in maintaining effective governance in the health sector. Power connections were modified as a result of devolved governance changes, which increased duties at subnational levels while also creating possibilities for public engagement. However, in both contexts, the effectiveness of these mechanisms has been undermined by a lack of sufficiently clear guidance, a failure to address pre-existing harmful contextual norms, and practices that are incompatible with the values of decision-makers, a lack of prioritization capacity, and a lack of true community accountability. Therefore, in both instances, the emphasis is too frequently focused on curative rather than preventative health care, which is counterproductive (McCollum, et al, 2018).
The policies regarding health that are responsible for governing development in the health sector in Kenya are directed toward the Sustainable Development Goals (SDGs), and as a result, they are fulfilling the vision 2030 social pillar. These policies are responsible for governing development in the health sector in Kenya. In an effort to enhance the general standard of living for all Kenyans, the national government distributes funds to the counties in order for those counties to offer their inhabitants with health care that is both effective and of a high quality (GoK, 2007). County governments have been empowered by devolution putting them in a position to design the innovative models that match their needs in various sectors, broader views of determining priorities in the health sector and finally allowing the local authorities to make independent decisions on the resource allocations and expenditure (Kenneth, 2014). Those mentioned above can only be fulfilled if the entire devolved governance process is fully embraced and implemented; if not, its effects may not be felt (Muchomba & Karanja, 2015).
In Kenya, the devolution of the health system was anticipated to serve several purposes. It was expected to improve access to health services across the country, eliminate discrimination in the quality of healthcare service between urban areas and ‘low potential areas’, and eliminate bureaucracy in the administration of health services especially in procurement (Murkomen, 2012). Moreover, devolved healthcare was viewed as a way of promoting efficacy in healthcare service delivery while promoting the quality of healthcare services.
The role of devolved governments in Kenya in the administration of healthcare services cannot be understated. Not only are these governments’ custodians of the funding of their healthcare services, but they also have the deterministic powers over the human resource providing these services. Article 235 bestows on county governments the power for: ‘establishing and abolishing offices in its public service,’ ‘appointing persons to hold and act in those offices’ and ‘exercising disciplinary control over and removing persons holding or acting in those offices. The constitution further states county governments are responsible for all healthcare delivery functions, including procurement of medical supplies (Tsofa et al., 2017). However, the ability of devolved governments to provide quality healthcare service is mainly dependent on the nature of governance or administrative efficiency of the semi-autonomous healthcare centers (McCollum et al., 2018). The role of governance in the performance of the health sector and the achievement of futuristic goals such as Universal Health Coverage (UHC) is widely recognized (Fryatt, Bennett, & Soucat, 2017). County governments are also responsible for handling any challenges relating to healthcare services, including capacity building and overcoming industrial actions (Murkomen, 2012).
Meru County has the following public Health facilities; one Level five hospitals, 23 level 4-hospitals, 33 level 3-health centers and 435 level 2-dispensaries serving approximately 1,635,264 million citizens (Meru County Government, 2020). To ensure quality service delivery after the first five years of devolution, the health department under Meru County Government established a five-year strategic plan between 2018 and 2022 to give full commitment and determination in improving the health services provided to its people. Kenya health policy that covers from 2012 to 2030 in the constitution gave the guidelines that were followed by Meru County in modelling the County integrated development plan conforming to the country’s vision 2030.
In 2020, following the announcement of the first covid-19 case in Kenya, a report by the health department that most medical facilities were understaffed and inadequately equipped, with statistics indicating that the whole County had a total bed capacity of 900, the County allocated 34% of its budget to the health department. Due to the budget allocation, the bed capacity increased to 1,700, with development projects being undertaken to shoot the number up to 3,000 by the end of 2022. From the budget estimates, the county government set aside Sh1.76 billion in 2021 to upgrade Meru teaching and referral Hospital to a level six hospital and creation of specialty centers, including cancer, trauma, pediatrics and rental units (Meru County Integrated Development plan 2018 – 2022).
Executives in the national government have also been shown to be resistant to distribute funding intended for county development programs in certain situations, undermining health sector governance and resulting in poor service delivery and development in the counties (Abdumlingo & Mugambi, 2014). According to the Barker, Mulaki, Mwai, and Dutta (2014) research, which evaluated Kenya’s County Health Form, Meru County was less equipped than other counties to provide required health care services under the country’s devolved system of government. After the first five years of devolution in Meru County, Kisumu County was billed Ksh 55 million in 2020 for maternity care that had been delivered in the county, Meru County owned Ksh129 million in debt, which had a significant impact on the county’s ability to acquire medical equipment (Mohamed, 2020). This study aimed to examine the effect of devolved governance on service delivery at Meru Teaching and Referral Hospital.
Statement of the Problem
In the Kenyan constitution, article 143(1) (a) gives the right to health for every person and that they have the right to access the highest standard of health. The responsibility to achieve quality health services has been passed down to the County governments, which are in charge of the management of health care services. Many counties, on the other hand, have faced severe obstacles in implementing health-care regulations. Following the devolved governance of health care services in Kenya, several cases have been going on, such as the health workers surrendering their duties due to low pay, some due to poor working conditions, inadequate staff, and delayed payment that has often paralyzed the delivery of health services. Underfunding and delayed funding has also been witnessed in some counties. This research sought to assess the effect of devolved governance on health care services on service delivery is at MTReH which is the only referral hospital in the county. The study intended to shed light on how Kenya’s healthcare sector is actually functioning under the devolved governance system, as well as on whether the goals of the Kenya Health Sector Strategic Plan (KHSSP), such as universal and better access to health services, are likely to be achieved under the current health sector management set-up, and what changes need to be made to the Kenya Health Policy Framework (KHPF).
Purpose of the study
The study sought to determine the effect of devolved financial planning on health care service delivery in Meru teaching and referral hospital.
Research question
The study sought to answer the question, what is the effect of devolved financial planning on health care service delivery in Meru teaching and referral hospital?
LITERATURE REVIEW
Theoretical literature review
Tanahashi Theory
The theory of Tanahashi (1978), which outlines a set of prerequisites for the provision of high-quality healthcare services, served as the basis for the research. The theory aimed to connect devolution of governance with the provision of healthcare, which was primarily concerned with resource allocation, the infrastructure of healthcare, and the sufficiency of healthcare personnel. The healthcare policy framework offers direction that is used to determine how devolved governance affects service delivery.
The administration of any business must utilize resources wisely and effectively if it is to provide services to any institution (Buse et al, 2012). This theory was pertinent to the research since it was centered on how Meru Teaching and Referral Hospital delivers healthcare services with decentralized resource allocation and health infrastructure. The theory’s primary focus is on ensuring that all healthcare stakeholders’ needs are met in an equitable manner, as well as how healthcare facilities operate to improve service delivery.
The Tanahashi theory looked at the value of making medical supplies and equipment accessible to the appropriate healthcare stakeholders while also taking their wellbeing into account. The theory went further to examine how the economic situation of these stakeholders affected their ability to pay for these products and their accessibility to the end user, as well as how it affected the provision of healthcare services. The theory also looked at how well the healthcare stakeholders were being treated and generally identified possible bottlenecks that may hinder the efficiency of various operations in the healthcare industry.
This theory was grounded in the Tanahashi theory, which explained why it is crucial to prioritize the allocation of resources, ensure that these resources are easily accessible to the vast majority of healthcare stakeholders, and provide a stable medical infrastructure within the Meru teaching and referral hospital in order to improve the governance of medical care delivered to patients. While the theory has the potential to enhance care delivery, it faces obstacles including insufficient personnel and a lack of commitment to the health policy framework, both of which must be addressed.
Empirical Literature
Effect of Devolved financial planning on Service Delivery
Patients’ key consideration while picking one of many competing public hospitals to visit for medical care is the reliability of the services provided by each facility. Cost spending vote healthcare, lack of preventative services innovations (Covid 19) pandemic, and inadequate insurance coverage for all classes of people are major problems for governments in developed countries like the United States (Papanicolas et al., 2019). Concerns with Europe’s universal health care system include the region’s high rate of health system fragmentation; the high cost of premiums paid even when there are no claims made for a lengthy period; the gap between medical care needs and available resources that varies by income level; delays and inefficiencies in the delivery of health services; and the low allocation of health care funds in the region’s projected budgets (Cherny et al., 2016).
Legal assurance shortcomings include confusing terms on compensations to subscribers, risk pulling shortcomings include excessive claims in one move, and inadequate resources have been allocated in national budgets in countries like Nepal, which is located in Asia (Deloitte, 2019; Ranabhat et al., 2019). In a country like Indonesia, health care program costs have been increasing faster than national revenue, leading to budget deficits and lower profit margins for hospitals (World Health Organization, 2019).
The effect of financial planning choices on health care effectiveness and fairness was investigated by Pooyan et al. (2018) across 11 nations. The United States, Egypt, Greece, China, Australia, Taiwan, and South Africa were all represented. Linear programming, the Markov model, cost-effectiveness analysis, per capita allocation, and modeling the allocation were identified as the most common approaches to financial planning. The research did, however, examine how these asset strategies affected service provision in a few nations, the current study will focus on financial planning in Meru teaching and referral hospital in Meru county Kenya which is a different study location from the above.
Going by a research done in Turkey by Gok and Altnda (2014) thorough evaluation and correction of the health system is unavoidable and is attainable via an analysis of policies, greater efficiency, limited superfluous expenses, and attention to societal demands. Allocating healthcare resources effectively and making good use of existing facilities is seen as crucial. The study did not address how the allocation of the said health resources will affect service delivery a gap this study intends to cover.
Gregory (2009) conducted research on the factors that affect the Malawian Health Department’s financial performance. The study used a descriptive research approach. The research found that increased performance required efficient financial allocation. The two factors were strongly and positively correlated.
Mpakaniye (2017) used the Musanze District as a case study to evaluate the impact of financial allocation on the local government of Rwanda’s budget process and implementation. The effective use of financial allocation, management control, and workforce management to improve the local government’s budgeting process and execution was discovered. The study failed to show the effect of the allocation on the healthcare service delivery.
Ngetich (2017) studied how devolution implementation affected the success of road development projects in Kenya’s Kericho County. The goal of the research was to assess how well road development projects in Kericho County were affected by devolved financial planning. Institutional theory and systems theory were used in the research to analyze project success behaviors in the county. The research found that increased financial devolution has improved the provision of necessary resources to road building projects and increased local contractors’ interest in road construction and maintenance contracts. The study focused on one partially devolved unit of governance ‘road’ the current study will focus on a full devolved unit of health care.
Gimoi (2017) evaluated Nairobi County Health Facilities as a case study for the effects of devolution on healthcare systems. The evaluation’s goal included determining how devolution will affect the health system’s infrastructure. This aimed to determine if devolution has benefited the infrastructure. The results showed that the condition of the medical equipment had improved and that new equipment had been purchased. There were covered placenta disposal pits, access to piped water, and efficient trash disposal. Restoring the public’s impression of high-quality treatment and reaching devolution objectives for improving primary healthcare facilities depend on the health infrastructure. This study was conducted in Nairobi County while the current study will be conducted in a different location Meru county.
Similar to Tsofa (2017), who wanted to assess the effects of health workers and the supply management in the County government of Kilifi. Over the course of four years, from the years 2012 to 2014, the research collected data by reading the documents, conducting knowledgeable interviews, and using both participatory and non-participatory interpretation. This research found that the administrative duties for health workforce (HRH) and essential medical supplies and medications (EMMS) were progressively being delegated before the counties had the appropriate structures in place and the necessary capacity to carry out these activities. This led to more frequent disruptions in paying employees, disruption caused by politics and HRH administration tasks, and confusion over HRH administrative roles. On functions, duties, labor strikes, mass acquiescence, and important stakeholders, it was seen that there were no clear guidelines at the national and county levels of government. The study provided a methodological gap and contextual gap to the current study.
Conceptual Framework
This is a diagrammatic representation of interactions among the existing variables in the study, it provides a connection between the independent and dependent variables in the study (Mugenda & Mugenda, 2013).

Figure 1: conceptual framework
RESEARCH METHODOLOGY
Research design
This study adopted a descriptive research design with a mixed-method approach that combined both qualitative and quantitative methods. According to Omari (2011), such a design is essential in establishing the “what is” question, enabling the researcher to employ different approaches in data collection from the study sample asking about perceptions; attitudes thus adequately describing the existing phenomena. This design was relevant to this study in obtaining information on the current status of the study phenomenon and to describe what exists regarding the variables of the study as well as the conditions of the study.
Target population
The target population is the entirety of homogenous individuals, objects or items pertinent to answering the research question and for which a sample can be drawn for actual measurement or data collection (Kombo and Tromp, 2006). The study drew its target a population of 1996 composed of health practitioners working in MTREH, patients visiting the facility, and members of the county assembly.
Sample and sampling size
A sample refers to a subset of entities from which the target population is defined by a given sampling criterion (Resnik 2011). The representative selection of this subset of entities from the study target population, to enable the generalization of study findings to the entire population of interest thus entails sampling. Sampling techniques are associated with reduced cost and higher accuracy of results.
The study adopted stratified sampling. In this sampling procedure the target population was subdivided into ten groups otherwise referred to as strata under stratification. Under this method of sampling, the common features of the participants form a basis for formulating the strata, these strata was composed of health administrators and practitioners, MCAs and patients Accordingly, a figure comparative to the stratum’s size against the population was obtained from each strata to form a random sample. According to Singh and Masuku (2014), these subsections are consequently combined resulting to a random sample. The researcher used a purposive sampling technique to sample hospital top management and the MCAs from the wards near the MTReH. A simple random sampling technique was used to sample patients attending the facility, nurses and clinical officers. This stratified sampling technique ensured the representativeness of desired characteristics of the population in the study sample by giving equal chances to all the elements in the population to be selected in the sample. The method reduced the chance of biases when selecting the sample.
Research Instruments
Quantitative and qualitative data collection approaches were utilized in this study. The study used questionnaires to collect data from health practitioners, and MCA’s. The advantage of the questionnaire for this study was that it enabled the collection of large volumes of data from the respondents at the same time and also concealed the identity of the respondents reducing biases associated with a given respondent characteristic. While an interview guide was used to collect data from the top hospital administrators and focus group discussion from patients.
The interview schedule was used to generate qualitative data for this study. This provided flexibility that allowed the interviewer to get a comprehensive understanding of the research problem and gaps not filled by closed-ended questions. The flexibility for open-ended questions was significantly an advantage for this chosen design since the interviewer was able to fully establish the opinions and behavior of some of the respondents (Neuman, 2013). The open-ended questions were essential in the questionnaires since they allowed the respondents to express their opinion fully without any limitations, unlike the closed-ended questions which were restrictive to the respondents. Moreover, this enabled the researcher to fully explore the ideas in as far as the subject was concerned which would then be reduced to different categories through coding and recording.
RESULTS AND DISCUSSIONS
Response Rate
Seventy-eight (78) questionnaires were issued to the sampled employees at Meru teaching and referral hospital. However, 75 questionnaires were filled following the instructions. This translated to a response rate of 96.2% that is acceptable for descriptive surveys, as postulated by Nulty (2008). The study also sampled the hospital chief executive officer (CEO) and the county health administrator for an interview which was successful. Further, the researcher managed a focus group discussion with the targeted 240 out patients who had visited the health facility during the research time.
Respondent Demographic Information
The study considered respondents social demographic characteristics on gender, age, length of service and educational background.
Gender of the Respondents
The respondents were asked to indicate their gender. The results were presented in Figure 2.

Figure 2: Gender of the Respondents
The respondents were fairly even whereby 54.67% were male and 45.33% were females. This means that the questionnaires were evenly distributed and there was no gender bias present in the study. Burns and Veeck (2020) noted that males were predominantly favored in both formal and informal research sectors. However, Ragab and Arisha (2018) emphasized the significance of women’s contributions to the informal sector, even in the context of male dominance in the formal sector. This underscores the importance of considering both genders in research studies.
Age of the Respondents
The respondents were further asked to indicate their age. The results were presented in Figure 3.
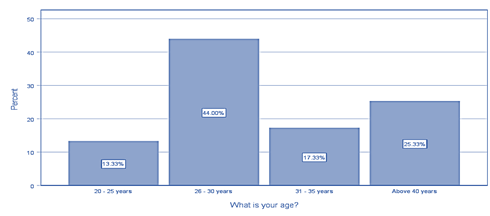
Figure 3: Age Respondents
Majority of the respondents who were 44.0%% as indicated in the figure were aged between 26-30 years, 25.33% were above 40 years of age, 17.33% showed respondents aged between 31 – 35 years and 13.33% of respondents aged between 20 – 25 years. This implies that the respondents were adults and therefore in a position to effectively understand the subject matter under study and gave reliable responses.
Employees experience in the health sector
Respondent’s length of service in healthcare sector in Meru County was assessed by the researcher through a questionnaire and the responses were as in table.
Table 1: Employee Experience
| Frequency | Percent | ||
| Valid | Less than 1 year | 27 | 36.0 |
| 1 – 6 years | 27 | 36.0 | |
| Above 6 years | 21 | 28.0 | |
| Total | 75 | 100.0 | |
Results from table indicate that majority 36.0% of the respondents had worked for a period of 1 -6 years, however the same proportion had worked for a period less than one year in their respective facilities. 21.0% of the respondents had worked for more than 6 years. The presences of newly employed staff may have been due to change of county government leadership which may have brought in new employees. Nevertheless 64.0% of the respondents had worked for significant time in the healthcare facilities to address the study variable. Thus most of the respondents were able to answer the questionnaire with ease.
Level of education
The respondents were asked to indicate their highest level of education. The results were presented in Figure 4.
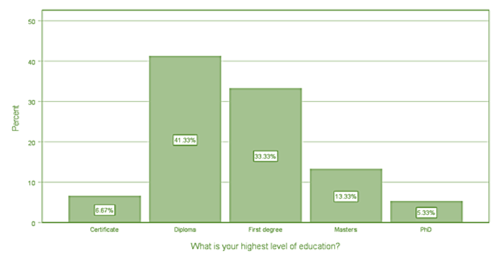
Figure 4: Respondent’s Education Level
Findings from Figure 4 indicate that majority 41.3% of the respondents indicated that they a diploma holders in various fields as their highest academic qualification, 33.3% of the respondents revealed that they hold first degree as their highest education level. The study also indicate that 13.3% of the respondents hold master degree as their highest education level while 5.33% had PhD. Those with certificate from various fields accounted for 6.67% of the respondents. This showed that the majority of the respondents had attained tertiary level of education and were knowledgeable in matters regarding the study thus providing reliable information.
Descriptive Analysis of Study Variables
In this section, the study sought to analyze the effects of devolved governance on health care service delivery in Meru teaching and referral hospital. The study sought to know from respondents how devolution of financial planning has affected healthcare service delivery, further the study also assed the effect of devolution of medical policy framework on healthcare service delivery at Meru Teaching and Referral hospital. The views of participants were on a 5-point Likert Scale where: 1=Strongly Disagree (SD), 2= Disagree (D), 3= Neutral (N), 4=Agree (A), 5=Strongly Agree (SA). The views were then consolidated to compute each of the study variables using the compute function in SPSS version 27. The results are as presented in the succeeding sections.
Devolved Financial Planning and Health Care Service Delivery
The first objective of the study was to examine the effect of devolved financial planning on health care service delivery in Meru teaching and referral hospital. The respondents were asked to respond to statements on financial planning. The responses were rated on a five likert scale as presented in Table 2.
Table 2: effect of financial planning on Healthcare Service Delivery
| Statements | N | Min | Max | Mean | Std. Deviation |
| Since devolution, the County has seen timely funding provision for healthcare. | 75 | 1 | 5 | 4.20 | 1.078 |
| It is crucial to include facilities committees, who are in charge of budgeting monies and estimating costs. | 75 | 1 | 5 | 3.88 | 1.294 |
| Healthcare in the County is given enough funding. | 75 | 1 | 5 | 4.09 | 1.210 |
| The funds allotted for the provision of healthcare services are used sensibly. | 75 | 1 | 5 | 4.27 | 1.004 |
| The County’s healthcare sector receives equitable budgetary funding allocations. | 75 | 1 | 5 | 4.07 | 1.131 |
| Valid N (LISTWISE) | 75 |
Findings from table indicated that the respondents agreed that since devolution, the County has seen timely funding provision for healthcare as supported by a mean of 4.20 and a standard deviation of 1.078. This finding supports that of Munywoki et al., (2020) who found that since devolution, the allocation of financial resources to county governments has been fast as compared to pre-devolution era. On utilization of the disbursed finances, the respondents agreed with the statement that the funds allotted for the provision of healthcare services are used sensibly with an average score of 4.27 recorded and a standard deviation of 1.004, the low value of standard deviation indicating that the respondent’s responses did not varying much. This finding tallies with that of Ngigi and Busolo (2019) who found that devolution has enhanced equality in distribution of funds across counties. This was further supported by the focus group discussions where member agreed that since devolution they have seen a lot of development in their hospital and added services. Group5 “devolution brought cancer centre in Meru County, there were pictures (x-rays) which used to be taken at Kenyatta but today we have them at Meru hospital”.
The results also showed that the respondents agreed that Healthcare in the County is given enough funding as supported by a mean score of 4.09 and a varying responses as accounted for by a standard deviation of 1.210. The study findings concur by those of study by Odera (2014) who found that adequate finances had significant influence on health service delivery in Kisumu County, Kenya. The respondents also agreed that the County’s healthcare sector receives equitable budgetary funding allocations and they found it crucial to include facilities committees, who are in charge of budgeting monies and estimating costs as supported by an average score of 4.07 and 3.88 respectively and a standard deviation of 1.131 and 1.294. The respondent’s findings were also supported by the interview responses where study1 indicated that “Devolution has made it easier for the healthcare facilities to access funds and make good accountability for the process of requisition and accountability has been brought nearer.”
Study 2
“Devolution gave the hospital a bit of autonomy to raise some funds to take care of some day today running of the facility without necessarily going to the allocated county revenue, this has reality improved the financial position of the facility and has a positive effect on the healthcare service delivery”.
Inferential Statistics
Inferential analysis was conducted to generate correlation results, model of fitness and analysis of the variance and regression coefficients.
Correlation Analysis
Table 3 below shows the results of the correlation analysis.
Table 3: Correlational Analysis
| Service Delivery | Financial Planning | Health Infrastructure | Staffing | Policy Framework | ||
| Service Delivery | Pearson Correlation | 1 | ||||
| Sig. (2-tailed) | ||||||
| N | 75 | |||||
| Financial Planning | Pearson Correlation | .912** | 1 | |||
| Sig. (2-tailed) | 0.000 | |||||
| N | 75 | 75 | ||||
** Correlation is significant at the 0.01 level (2-tailed).
The results in table 3 revealed that financial planning and healthcare services are positively and significant related (r=0.912, p=0.000). this implies that the more finances the more the health service delivery improved. The results were also consistent with that of Adebisi et al., (2020) whose results indicated that effective financial allocation is a very important factor to the process of achieving sustainable health services delivery. WHO (2020) established that financial allocation has a positive and significant influence on quality of healthcare.
Regression Analysis
The results in Table 4 presented the fitness of model of regression model used in explaining the study phenomena.
Table 11: Model summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .966a | 0.933 | 0.929 | 0.0306 |
- Predictors: (Constant), financial planning
From Table 4 above financial planning framework was found to be satisfactory variable in explaining healthcare service delivery in Meru teaching and referral hospital. This was supported by coefficient of determination also known as the R square of 93.3%. This meant that predictor variables explain 93.3% of the variations in the dependent variable which was healthcare services delivery. The results further meant that the model applied to link the relationship of the variables was satisfactory.
In statistics significance testing the p-value indicates the level of relation of the independent variable to the dependent variable. If the significance number found is less than the critical value also known as the probability value (p) which is statistically set at 0.05, then the conclusion would be that the model is significant in explaining the relationship; else the model would be regarded as non-significant. Table 5 provided the results on the analysis of the variance (ANOVA).
Table 5: Analysis of Variance
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 4.583 | 5 | 1.146 | 232.32 | .000b |
| Residual | 119.417 | 70 | 1.706 | |||
| Total | 124.000 | 75 | ||||
- Dependent Variable: healthcare service delivery
- Predictors: (Constant), financial planning
The results in Table 5 indicated that the overall model was statistically significant. Further, the results implied that the independent variable was good predictor of healthcare services delivery. This was supported by an F statistic of 232.32 and the reported p value (0.000) which was less than the conventional probability of 0.05significance level.
Table 6: Regression of Coefficients
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | ||
| B | Std. Error | Beta | ||||
| 1 | (Constant) | 3.246 | 1.077 | 3.014 | 0.000 | |
| Financial planning | 0.336 | 0.124 | 0.002 | 0.019 | 0.001 | |
- Dependent Variable: healthcare service delivery
The results presented in Table 6 demonstrate a positive and statistically significant relationship between financial planning factor and healthcare service delivery. Specifically, an increase in financial planning within county government is associated with an improvement in healthcare service delivery, with a coefficient of 0.336 (p=0.001). This suggests that a unit change in financial planning will have 0.336 effect on the healthcare service delivery. These findings align with previous research by Gimoi (2011), Mabonga (2017), and Odhiambo (2015), all of whom also highlighted the importance of this factor in health service delivery.
SUMMARY OF THE RESULTS
This section outlines the primary findings of the research objective in the investigation. The study aimed to analyze the effect of devolved financial planning on health care service delivery in Meru teaching and referral hospital. The participants in the research significantly bolstered the credibility of each objective, owing to their Age, commendable educational backgrounds and substantial work experience. The participants had accumulated one year of experience, which serves as a positive indicator and source of confidence in obtaining trustworthy outcomes.
The first objective of the study was to examine the effect of devolved financial planning on health care service delivery in Meru teaching and referral hospital. The findings showed that there was a significant association between the financial planning and healthcare service delivery in Meru teaching and referral hospital. The findings were also consistent with the statements in the questionnaire which majority of the respondents agreed. This was also supported by the regression results which revealed that adequate financial planning had a positive and significant impact on the healthcare services delivery.
CONCLUSION
Based on the study findings, the research revealed that the timely allocation of financial resources, appropriate financial allocation, responsible utilization of allocated funds, and the allocation of budgets for finances all have a positive and significant impact on the delivery of healthcare services in Meru teaching and referral hospital.
REFERENCES
- Abdumlingo, H., & Mwirigi, M. F. (2014). Business & Management: A case study of Mombasa County’s challenges in handling devolved monies in the provision of services. An Interdisciplinary Journal of Theory and Practice.
- Abe, T., (2014). Reaction techniques took on by the service of wellbeing to difficulties of degenerated medical care administrations in Kenya. College of Nairobi repository.
- Ahakwa, I., Afotey Odai, L., & Dartey, S. (2021). Public sector workers’ commitment to their organizations in the Ashanti Region of Ghana, as affected by job autonomy, organizational learning, and the quality of their working environment. International Journal of Scientific Research and Management, 9(1), 2099-2110.
- Andrews, R. (2013). Evaluation of the neighborhood’s efficiency, responsiveness, value, and viability in light of the new, more transparent management. Public Management Review, 15(5), 762-783.
- Aslam, G. (2019). Evidence from Pakistan suggests that decentralization measures in authoritarian governments might help them stay in power. International Political Science Review, 40(1), 126-142.
- Aslam, G., (2011). An empirical analysis of how devolution reforms in Pakistan have impacted the delivery of aid. Policy implementation and Development, 31(3), 159-171.
- Awino, E. (2016). Reaction techniques took on by the service of wellbeing to difficulties of degenerated medical care administrations in Kenya. College of Nairobi erepository.
- Barker, C., (2014). Surveying County wellbeing framework status in Kenya: An audit of chosen wellbeing inputs. Recovered from www.healthpolicyproject.com
- Caplan, S., Garces-King, J., Queen, K., & Nahar, R. (2018). Provider perspectives on mental health treatment in the Dominican Republic. Global public health, 13(7), 874-898.
- Creswell, J. W., (2017). Reaction techniques took on by the service of wellbeing to difficulties of degenerated medical care administrations in Kenya. College of Nairobi repository.
- De los Santos, J. A. A., Tsaras, K., & Labrague, L. J. (2020, November). The toll taken on nurses’ productivity and mental health by workplace bias and secrecy. In Nursing Forum (Vol. 55, No. 4, pp. 782-792).
- Eboreime, E. A., (2017). Assessing the sub-public loyalty of public Initiatives in decentralized wellbeing frameworks.
- Elcock, H. (2013). Local government: Policy and management in local authorities. Routledge.
- Essendi, H. (2015). Public perceptions of development and relationship with wellbeing: the case of Makueni County in Kenya (Doctoral dissertation, University of Southampton).
- Gatumo, M., Sayed, A. R., & Scheibe, A. (2018). Cervical cancer screening and women’s understanding of the disease in the Kenyan counties of Isiolo and Tharaka Nithi: a cross-sectional research. BMC cancer, 18(1), 1-9.
- Gimoi T. (2017). The effect of devolution on medical services frameworks: a contextual investigation of Nairobi area
- GoK, (2016). Kenya conceptive, maternal, infant, kid and juvenile wellbeing (RMNCAH) speculation system. Nairobi: Government Printer.
- Ibok, E. E. (2014). The effect of devolution on medical services frameworks: a contextual investigation of Nairobi area
- Kombo, D. K., and Tromp, D. L. (2006). Proposition and theory composing: A presentation. Nairobi: Paulines Publications Africa, 5, 814-30.
- Kothari, C.R. (2004) Methodologies and techniques for doing research New Age Edition, Second Edition
- KPMG (2014). Devolution of medical care administrations in Kenya. Recovered from kpmgafrica.com
- Manyisa, Z. M., & van Aswegen, E. J. (2017). Public hospital employment factors: a literature study. International journal of Africa nursing sciences, 6, 28-38.
- Ministry of Health (MoH) (2015). Kenya Service Availability and Readiness Assessment Mapping
- Miriti, A, K. (2016). Devolution on medical services frameworks: a contextual investigation of Nairobi area Ace proposition college of Nairobi.
- Mohamed, K. A. (2020). Universal Health Care in Kenya: Challenges and Opportunities for NHIF in Kisumu, Machakos, Nyeri, and Isiolo Counties (Doctoral dissertation, United States International University-Africa).
- Muchomba, F. G. (2015). Impact of regressed administration and execution of the wellbeing area in Kenya. Vital Journal of Business and Change Management, 2(2).
- Mugenda, O. M., and Mugenda, A. G. (2003). Methods of investigation include quantitative and qualitative approaches. African Center for Technology Studies Press is based in Nairobi, Kenya.
- Ndung’u, G. J. (2014). Assessing Devolution’s Effect on Kenya’s Economic Growth Prospects. Foreign relations and Global Strategy Journal, 26 (6), 79-94.
- Neuman, W. L. (2013). Social examination strategies: Qualitative and quantitative methodologies. Essex,
- Ngigi, S., & Busolo, D. N. (2019). The ups and downs of devolution in Kenya. Examining the research of Public Administration and Policy, 9(6), 9-21.
- Rondinelli, D. A., Nellis, J. R., and Cheema, G. S. (2016). Decentralization in non-industrial nations. World Bank staff working paper, 581.
- Rotich, J., & Mulongo, L. (2014). Kenya as a Case Study of Devolution and Governance Conflicts in Africa.
- Singh, A. S., & Masuku, M. B. (2014). Overview of sampling strategies and sample size calculations for researchers in applied statistics. International Journal of economics, commerce and management, 2(11), 1-22.
- Smoke, P. (2015). Reevaluating decentralization: Assessing difficulties to a well-known public area change. Policy implementation and Development, 35(2), 97-112.
- Trust, K. R. (2014). Lapsed government and nearby administration in Kenya: Implementing decentralization supported by the 2010 constitution. African and Asian Studies.
- Wagana, D. M., & Iravo, M. A. (2017). A literature study and analysis of the connection between devolved governance, political decentralization, and service provision.
- World Health Organization. (2018). Disparities in rural primary health care: a systematic study focusing on the WHO European Region.
- Nulty, D. D. (2008). The adequacy of response rates to online and paper surveys: what can be done?. Assessment & evaluation in higher education, 33(3), 301-314.
- Burns, A. C., & Veeck, A. (2020). Marketing research. Pearson.
- Ragab, M. A., & Arisha, A. (2018). Research methodology in business: A starter’s guide.
- Munywoki, J., Kagwanja, N., Chuma, J., Nzinga, J., Barasa, E., & Tsofa, B. (2020). Tracking health sector priority setting processes and outcomes for human resources for health, five-years after political devolution: a county-level case study in Kenya. International Journal for Equity in Health, 19(1), 1-13.
- Ngigi, S., & Busolo, D. N. (2019). Devolution in Kenya: the good, the bad and the ugly. Public Policy and Administration Research, 9(6), 9-21.
- Binder, C. C. (2019). Redistribution and the individualism–collectivism dimension of culture. Social Indicators Research, 142(3), 1175-1192.
- World Health Organization. (2018). HIV self-testing strategic framework: a guide for planning, introducing and scaling up.
- Creswick, N., & Westbrook, J. I. (2019). Social network analysis of medication advice-seeking interactions among staff in an Australian hospital. International journal of medical informatics, 79(6), e116-e125.
- Gerston, L. N. (2014). Public policy making: Process and principles. Routledge.
- Adebisi, Y. A., Umah, J. O., Olaoye, O. C., Alaran, A. J., Sina-Odunsi, A. B., & Lucero-Prisno III, D. E. (2020). Assessment of health budgetary allocation and expenditure toward achieving universal health coverage in Nigeria. International Journal of Health and Life Sciences, 6(2).
- World Health Organization. (2020). Health policy and system support to optimize community health worker programmes for HIV, TB and malaria services: an evidence guide.
- Okoroafor, S. C., Ongom, M., Mohammed, B., Salihu, D., Ahmat, A., Osubor, M., … & Alemu, W. (2021). Estimating frontline health workforce for primary healthcare service delivery in Bauchi State, Nigeria. Journal of Public Health, 43(Supplement_1), i4-i11.
- Cinaroglu, S. (2019). Politics and health outcomes: A path analytic approach. The International Journal of Health Planning and Management, 34(1), e824-e843.
- Grorud-Colvert, K., Sullivan-Stack, J., Roberts, C., Constant, V., Horta e Costa, B., Pike, E. P., … & Lubchenco, J. (2021). The MPA Guide: A framework to achieve global goals for the ocean. Science, 373(6560), eabf0861.