
Factors Associated With Ophthalmic Self Medication Among Adult Patients Attending Sabatia Eye Hospital in Vihiga County, Kenya
- Peter Koome Mutuma
- Alloysius Luambo Omoto
- George Muthui
- 317-338
- Jan 10, 2024
- Health
Factors Associated With Ophthalmic Self Medication Among Adult Patients Attending Sabatia Eye Hospital in Vihiga County, Kenya
Peter Koome Mutuma1, Alloysius Luambo Omoto2, George Muthui3
German Doctors-Baraka Health Center, Kenya1,2,3
DOI: https://doi.org/10.51244/IJRSI.2023.1012026
Received: 06 December 2023; Accepted: 15 December 2023; Published: 09 January 2024
ABSTRACT
Background: Self-medication is the selection and use of non-prescription medicines by individuals’ own initiatives to treat self-recognized illnesses or symptoms. Ophthalmic eye drugs are widely used by many people who trickle into drug stores for the most common and readily available eye drugs ignoring the potential danger they expose themselves to.
Objectives: The study sought to determine socioeconomic factors associated with ophthalmic self-medication among adult patients attending Sabatia eye hospital in Vihiga County, Kenya.
Methodology: A descriptive cross-sectional study design was used. The research was carried out at Sabatia eye hospital, Vihiga County, Kenya. The study population for this research was drawn from 322 patients seeking eye services at the study site. Systematic sampling method was used to select the study subject. The study used structured questionnaires to collect data though interviews and analysis was done using SPSS version 25 and results presented in proportions using tables and graphs.
Results: A total of 322 respondents were included into the study which is 101.9% of the 316 participants targeted. Majority of males (49.6%) said they self-medicated because of due to long hospital queues. Respondents aged 40-69 years are more likely to use traditional herbs to treat eye illnesses. Those with college or degree level of education (11.5%) are more likely to self-medicate with antibiotics. Most of the respondents 51.6% presenting with redness of eyes are likely to use antibiotics, while those with trauma 41.8% reported use of drug left overs and were less likely to seek hospital treatment. Those aged 60-69 years reported use of milk as a mode of treatment while the ones aged 18-29 years (8.6%) reported distance as a factor leading to self-medication
Recommendations: Health Providers should have quality time with patient coupled with proper counseling on use of drugs as this is regarded as one of the essential components of the overall medicine use process. Rules and regulations on dispensing of medicines from pharmacies should be reinforced and train and employ more eye health workers
Key terms: self-medication, ophthalmic drugs, rural area
BACKGROUND OF THE STUDY
In our daily lives, we practice self-medication, which is regarded as a component self-care meant to improve our health. Self-medication is the selection and use of non-prescription medicines by individuals’ own initiatives to treat self-recognized illnesses or symptoms (ArulJothi, K et al., 2014). Self-medication poses danger because of the likelihood of abuse of the drugs, coupled by the fact that no doctor’s consultation is sought prior to the use of the medication (ArulJothi, K et al., 2014). A study commissioned by Synovate and published in Daily nation titled ‘Self-medication-rises-as prescription drugs bought over counter’, Establish the incidence of abuse of prescriptions type drugs revealed that of the total 203 pollsters visited various pharmacies in all eight provinces and sought to buy a specific brand of antibiotics which should be sold only on prescription.73% of the pharmacies sold the medicine did not ask for prescription, 9% of the pharmacies asked for the prescription but went ahead and sold the antibiotic anyway even though it was not produced. Only 18% asked for prescription and refused to sell the drug without one being produced(Nation, 2011).
In Ophthalmology the self-medication of patients can be referred as instances when a person uses non-prescribed ophthalmic drugs to treat an ocular disease rather than visiting a specialized care giver for diagnosis, clinical advice and subsequent treatment (E. Marquez, 2014a). The study further observed that the act of ophthalmic self-medicating by patients is as old as history is, done right from our homes, work places and Schools. The practice has been an obvious phenomenon that none can claim to be clean from. Ophthalmic eye drugs are widely used by many people who trickle into chemists and drug stores for most common and readily available eye drugs ignoring the potential danger they expose themselves to (Shabani & Redican, 2017). Ophthalmic Self-medication drugs range from the least toxic and less addictive to most toxic and addictive drugs, depending with one’s exposure and presumed understanding of such drugs despite being non-drug trained specialist (Sarahroodi & Mikaili, 2012). Most shockingly is the repetitive use of antibiotics eye drugs and prolonged use of steroids for eye treatment due to wrong self-diagnosis and lack of prescription of these ophthalmic drugs (Shaikh et al., 2017). There are other patients who tend to self-medicate from ophthalmic left-over drugs that had been prescribed to a previous patient left or worse heed the advice of other former patients or non-specialist with regards to the drugs that they need to use for their treatment.
This being a global problem many have fallen victims of wrong ophthalmic self-medications referred to as ‘drug abuse’ which may result in other undesirable side effects or even permanent and long-lasting harm to the eye and general body (Fainzang, 2013). The habit is deep rooted and wide spread in our society not selective though dependent to some extent with our cultural practices, race, economic or social backgrounds. Fainzang (2013) and (Wafula et al., 2014) describes further that this menace has been becoming increasingly popular due to lack of good will in implementing policies governing drug sale, as well as the tendencies of patients to opt for advices that they obtain from non-clinical sources that includes previous prescriptions, Internet searches and state of body health at a given point in time(Fainzang, 2013; Wafula et al., 2014).
According to a research by Wafula (2014) in Kenya there are various factors that have led to ophthalmic self-medication, some of this include: social demographic factors, literacy, availability of facilities among other things(Wafula et al., 2014).
Statement of the Problem
Patients are taking a more active role in their healthcare, including through self-medication. A research carried out by World Health Organization through World Self-Medication Industry in 2012 showing 59 percent of Americans polled say they are more likely to treat their own health condition now than they were a year ago. Seventy three percent would rather treat themselves at home than see a doctor, and six in 10 say they would like to do more of this in the future. One research firm estimated 65 percent of people who visited the Internet in a 12-month period went to health-related sites (Bennadi, 2013). Given the growing global resistance for antibiotic and the documented health related issues, inappropriate use of un-prescribed drugs or informal self-medication can leads to serious complications like: panophthalmitis, endophthalmitis, uveitis, cataract and bullous keratopathy. In a study on Incidence and complications of Traditional Eye Medications in a Nigerian Teaching Hospital involving 113 subjects, it conclude that Traditional emergency medicine is a common practice that is harmful and leads to blindness (Ukponmwan & Momoh, 2010). In several studies it has been found that inappropriate ophthalmic self-medication results in wastage of resources, increase resistance of pathogens and generally entails serious health hazards such as adverse reactions, prolonged suffering, drug dependence and worst of all partial or total blindness (E. Marquez, 2014b). Despite all these, very little information is available about ophthalmic self-medication both at the county and national level. Sabatia eye hospital serves the large Western region, that’s former Western, Nyanza, TransNzoia and part of North Rift Valley. The majority of the population has poor socio-economic status among other challenges like poor infrastructure, illiteracy, strong cultural and traditional beliefs to name but a few.
Study Justification
Most of self-medicated ocular complications are borne by rural dwellers that are more likely to use Traditional emergency medicine than urban dwellers (Ukponmwan & Momoh, 2010). Non-specialist treatment of ocular disease poses a huge risk to patients as the choice and timing of use of such drugs is not well informed leading to a great danger to innocent patients. This irresponsible use of non-prescribed drugs can be costly to individuals as they predispose them to life threatening complications or potentially blinding ocular diseases, the cost associated with treatment of these issues arising from self-medication is high not mentioning the visual limitation or blindness and reduction of an individual’s productivity. This threatens progression of a family as it can happen to a key bread winner hence putting the family into jeopardy. To a society it increases the disease burden and reduces the productivity of it people leading to dependency and increases the cost of health care. The study focuses on adult patients who are the working populations and bears significant socioeconomic implications especially in developing countries such as Kenya and hence will act to inform the authorities on resource allocation in offering medical education to prevent ocular complications and potential blinding self-medicating acts. There are few studies on social, economic and cultural factors influencing ophthalmic self-medication done in Kenya and to patients attending Sabatia eye hospital in Vihiga County. This study will serve to identify the factors associated with self-medication among adults’ patients attending Sabatia Eye Hospital, and will inform health and drug policy development and implementation in Vihiga county and Kenya to reduce the incidence of drug abuse and self-medication hence reducing cases of complicated ocular diseases arising from self-medication.
Broad objectives
To determine factors associated with ophthalmic self-medication among adult patients attending Sabatia eye hospital in vihiga county
Specific objectives
- To determine economic factors leading to ophthalmic self-medication among patients attending Sabatia Eye Hospital in Vihiga County.
- To determine social factors influencing ophthalmic self- medication among patients attending Sabatia Eye Hospital.
- To determine cultural factors leading to ophthalmic self-medication by patients attending Sabatia Eye Hospital in Vihiga County
Research questions
- How do economic factors influence ophthalmic self-medication?
- How do social factors affect ophthalmic self-medication?
- How does culture influence ophthalmic self-medication?
METHODOLOGY
Study Design
A descriptive cross-sectional study design was used.
Study area
The research was carried out in Sabatia eye hospital (SEH), Vihiga County, Kenya. SEH is a church based non-profit tertiary eye hospital in Vihiga county of Kenya. It is located 5 km from Chavakali town along Chavakali- Kapsabet road, situated at Wadonga Market. The Hospital can also be accessed through Kisumu-Mbale-Chavakali-Kakamega road through the junction to Kapsabet at Chavakali Town. Sabatia Eye Hospital is a 43-bed capacity Teaching and referral eye hospital in western Kenya serving the western region, north rift, and Nyanza regions. Offering Teaching, promotive, preventive, curative, rehabilitative services to eye patients and students in the region. It boosts of a strong work force composed of various experienced and respected sub-specialties (Pediatric, Vitreal retinal surgeon) working in collaboration with other eye care givers like Ophthalmologists, Ophthalmic Clinical Officers, Ophthalmic Nurses, Anesthetist, Optometrist, pharmacist and many more. The hospital conducts regular sponsored Outreach and medical camps in the communities within and bordering the county. We chose this hospital because of its convenience and it’s serves a large volume of patients being seen per day and the investigator will be doing his clinical selective/attachment at the same facility at the time of the study.
Study Population
The study population for this research was drawn from 322 patients seeking eye services at Sabatia eye hospital in Vihiga County of Kenya and are 18 years and above. The study was carried over duration of one month from Monday to Friday from 8.00am to 5.00pm
Sample size determination
The sample size was determined by fisher et al formula
n=Z2pq/d2
n= desired sample size (if target population is greater than 10,000)
Z=the standard normal deviate at the required confidence level.
p= the proportion in the target population estimated to have characteristics being measured.
q= 1-p
d= the level of statistical significance set
n= (1.96)2(0.5) (0.5)/ (0.05)2 = 384, as per fisher’s population
If the sample size of the study population is less than 10000
Since the study area has a population of less than 10000 persons the second formula was used to calculate sample size. (Fisher et al, 1998)
nf = n/1+{n/N}
where nf = 384
1+ (384/1800) = 1.2133
384 / 1.2133= 316.4922
Sample size = 316
Sampling Method
Systematic sampling method was used to select the study subject. An approximate of 90 patients is seen at Sabatia per day, for a month is approximately 1,800. Since the expected population during the month of study is 1,800 and the calculated sample size is 316, Therefore sample interval is 1800/316 =5.6962 which is every 5th member of the sampling frame will be included in the study.
The first patient was selected through simple random sampling method by writing 10 papers number 1-10. The patients who picks number one starts automatically. If a patient selected fails we shall go to the next number.
Inclusion criteria
All patients seeking eye care services at Sabatia Eye Hospital aged 18 years and above attending the hospital during the month of study starting 8.00 am – 5.00pm Monday to Friday who give consent to participate in the study was included.
Exclusion criterion
Patients below the age of 18 years and who, after explanation of the purpose of the study and assurance that their participation would not harm them in any way and that all the information obtained from them would be confidential, decline to give consent to participate in the study were excluded.
Instrumentation
The study used questionnaires with qualitative and quantitative, open and closed ended questions and standardized to reduce biasness of analyzing and interpretation of the data, ensure reliability, generality, and validity of the results.
Data collection and management
The study was conducted through an interview to get primary data. The researcher identified and trained interviewers on data collection prior to material day; he also sensitized them on accuracy and confidentiality of each response from the interviewee and the need for questionnaire and data security by use of passwords. A pretest was conducted to access the interviewer’s preparedness and credibility of the questionnaires. The types of questions that were used include both open and closed ended.
Results
Sex versus respondents self-medicating due to long waiting time or due to long hospital queues.
A total of 322 respondents were included into the study which is 101.9% of the targeted number of 316 participants. Majority of males (51.4%) said they never self-medicated because of long waiting time or due to long hospital queues as shown in the figure 4.1 below. Figure 4.1 Sex versus respondents self-medicating due to long waiting time or due to long hospital queues.

Age versus where the respondents were treated.
Respondents aged 40-49 years (33%) are more likely to buy drugs from a pharmacy whereas respondents aged 30-39 years and 60-69 years are more likely to seek traditional healer/herbalist care 42.9% as shown in Table 4.1 below.
Table 4.1 Age versus where the respondents were treated.
| Age of the respodents | |||||||
| 18-29 YEARS | 30-39 YEARS | 40-49 YEARS | 50-59 YEARS | 60-69 YEARS | 70 YEARS AND OVER | ||
| Where the respondent was treated | HOSPITAL/EYE CLINIC | 15 | 32 | 55 | 55 | 34 | 13 |
| BOUGHT DRUGS FROM A PHARMACY | 6 | 15 | 17 | 6 | 3 | 4 | |
| TREATED BY AN HERBALIST/TRADITIONAL HEALER | 0 | 3 | 1 | 0 | 3 | 0 | |
| OTHERS SPECIFY-LEFT-OVERS, | 14 | 21 | 12 | 6 | 7 | 0 | |
| Total | 35 | 71 | 85 | 67 | 47 | 17 | |
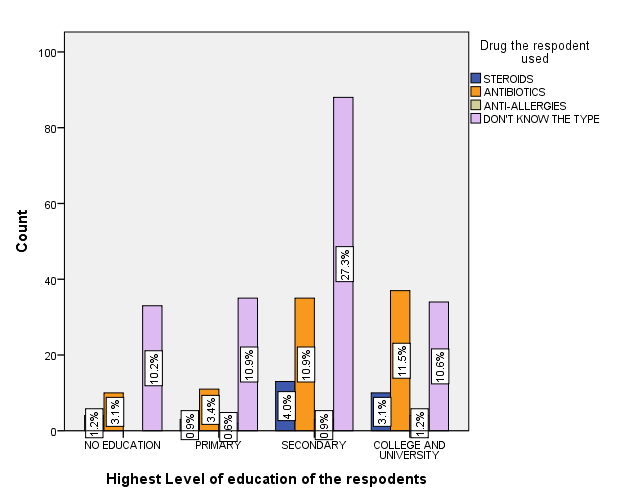
Education versus Drug the respondent used.
Majority of respondents with secondary education (27.3%) don’t know the type of drug used, respondents with a college or degree level of education are more likely to self-medicate with antibiotics (11.5%), as shown in the Figure 4.2 below.
Figure 4.2 Education versus the drug respondents used.
Sex of the respondents versus the respondents self-medicating because of cost of eye services.
More males 5% considered cost as a motivating factor to self-medicate than females 4.7%, as shown in the Figure 4.3 below.
Figure 4.3 Sex versus self-medicating because of cost of eye services.

Sex of the respondents versus respondents who were harassed by a health care giver.
Majority of Males 8.1% reported being harassed by health care giver unlike females 5.3% who reported being harassed by health care givers, as shown in the figure 4.4 below.
Figure 4.4 Sex against Harassed by a health care giver.

Where the respondents were treated versus respondents self-medicating because the eye infection is not a serious illness.
Majority of respondents 57.1% who were treated in a hospital said seriousness of eye infection was not a motivating factor whereas those treated by an herbalist were the minority1.6%, as shown in the Figure 4.5 below.
Figure 4.5 Where treated versus self-medicating because the eye infection is not a serious illness.

Age of the respondents versus respondents who used traditional herbs to treat an eye illness.
Respondents aged 40-69 years are more likely to use traditional herbs to treat an eye illness whereas respondents aged 18-39 years and above 70 years and over are less likely to use herbs, as shown in the Figure 4.6 below.
Figure 4.6 Age versus used traditional herbs to treat an eye illness.

Highest level of education vs where the patients got treated.
Majority of the respondent sought hospital treatment irrespective of highest level of education, as shown in the Table 4.2 below.
Table 4.2 Highest level of education vs where the respondent was treated.
| Where the respondent was treated | Total | |||||
| HOSPITAL/EYE CLINIC | BOUGHT DRUGS FROM A PHARMACY | TREATED BY AN HERBALIST/TRADITIONAL HEALER | OTHERS SPECIFY-LEFT-OVERS, | |||
| Highest Level of education of the respondents | NO EDUCATION | 32 | 8 | 2 | 5 | 47 |
| 68.1% | 17.0% | 4.3% | 10.6% | 100.0% | ||
| PRIMARY | 38 | 8 | 1 | 4 | 51 | |
| 74.5% | 15.7% | 2.0% | 7.8% | 100.0% | ||
| SECONDARY | 90 | 18 | 1 | 30 | 139 | |
| 64.7% | 12.9% | 0.7% | 21.6% | 100.0% | ||
| COLLEGE AND UNIVERSITY | 44 | 17 | 3 | 21 | 85 | |
| 51.8% | 20.0% | 3.5% | 24.7% | 100.0% | ||
| Total | 204 | 51 | 7 | 60 | 322 | |
| 63.4% | 15.8% | 2.2% | 18.6% | 100.0% | ||
Main presenting symptom versus drug the respondents used.
Most of the respondents 51.6% presenting with redness of eyes are likely to use antibiotics though majority of respondents reported not knowing the type of drug used, as shown in Table 4.3 below.
Table 4.3: Main presenting symptom versus drug the respondents used crosstabulation.
| Drug the respondent used | Total | |||||
| STEROIDS | ANTIBIOTICS | ANTI-ALLERGIES | DON’T KNOW THE TYPE | |||
| Main presenting symptom | REDNESS | 9 | 33 | 2 | 20 | 64 |
| 14.1% | 51.6% | 3.1% | 31.3% | 100.0% | ||
| PAIN | 9 | 28 | 2 | 18 | 57 | |
| 15.8% | 49.1% | 3.5% | 31.6% | 100.0% | ||
| DISCHARGE | 3 | 13 | 3 | 35 | 54 | |
| 5.6% | 24.1% | 5.6% | 64.8% | 100.0% | ||
| SWELLING | 2 | 7 | 2 | 44 | 55 | |
| 3.6% | 12.7% | 3.6% | 80.0% | 100.0% | ||
| REDUCED VISION | 7 | 12 | 0 | 72 | 91 | |
| 7.7% | 13.2% | 0.0% | 79.1% | 100.0% | ||
| OTHERS=FOREIGN BODY SESANTION | 0 | 0 | 0 | 1 | 1 | |
| 0.0% | 0.0% | 0.0% | 100.0% | 100.0% | ||
| Total | 30 | 93 | 9 | 190 | 322 | |
| 9.3% | 28.9% | 2.8% | 59.0% | 100.0% | ||
Highest level of education of respondents versus used traditional herbs to treat an eye illness.
Respondents with no education 25.5% (n=12) reported use of traditional herbs whereas respondents with primary education and above are less likely to use herbs, as shown in the Table 4.4 below.
Table 4.4 Highest level of education versus used traditional herbs to treat an eye illness
| Used traditional herbs to treat an eye illness. | Total | |||
| YES | NO | |||
| Highest Level of education of the respondents | NO EDUCATION | 12 | 35 | 47 |
| 25.5% | 74.5% | 100.0% | ||
| PRIMARY | 5 | 46 | 51 | |
| 9.8% | 90.2% | 100.0% | ||
| SECONDARY | 12 | 127 | 139 | |
| 8.6% | 91.4% | 100.0% | ||
| COLLEGE AND UNIVERSITY | 2 | 83 | 85 | |
| 2.4% | 97.6% | 100.0% | ||
| Total | 31 | 291 | 322 | |
| 9.6% | 90.4% | 100.0% | ||
The cause of the illness versus where the respondents were treated.
Majority 63.4% (n=204) reported treatment in a hospital. Respondents with trauma 41.8% reported use of drug left overs and were less likely to seek hospital treatment, as shown in the table 4.5 below.
Table 4.5 The cause of the illness versus where the respondents were treated.
| Where the respondent was treated | Total | |||||
| HOSPITAL/ EYE CLINIC | BOUGHT DRUGS FROM A PHARMACY | TREATED BY AN HERBALIST/ TRADITIONAL HEALER | OTHERS SPECIFY-LEFT-OVERS, | |||
| The cause of the illness | INFECTION | 128 | 15 | 1 | 12 | 156 |
| 82.10% | 9.60% | 0.60% | 7.70% | 100.00% | ||
| TRAUMA | 26 | 24 | 3 | 38 | 91 | |
| 28.60% | 26.40% | 3.30% | 41.80% | 100.00% | ||
| BAD OMEN IN THE COMMUNITY | 37 | 6 | 2 | 1 | 46 | |
| 80.40% | 13.00% | 4.30% | 2.20% | 100.00% | ||
| OTHERS SPECIFY-INSECTS, ALLERGY, | 13 | 6 | 1 | 9 | 29 | |
| 44.80% | 20.70% | 3.40% | 31.00% | 100.00% | ||
| Total | 204 | 51 | 7 | 60 | 322 | |
| 63.40% | 15.80% | 2.20% | 18.60% | 100.00% | ||
Age of the respondents versus used milk as a mode of eye treatment.
Respondents aged 60-69 years reported use of milk as a mode of treatment 40.4% (n=19), as shown in the Table 4.6 below.
Table 4.6 Age of the respondents versus Used milk as a mode of eye treatment.
| Used milk as a mode of eye treatment. | Total | |||
| YES | NO | |||
| Age of the respondents | 18-29 YEARS | 3 | 32 | 35 |
| 8.6% | 91.4% | 100.0% | ||
| 30-39 YEARS | 16 | 55 | 71 | |
| 22.5% | 77.5% | 100.0% | ||
| 40-49 YEARS | 18 | 67 | 85 | |
| 21.2% | 78.8% | 100.0% | ||
| 50-59 YEARS | 13 | 54 | 67 | |
| 19.4% | 80.6% | 100.0% | ||
| 60-69 YEARS | 19 | 28 | 47 | |
| 40.4% | 59.6% | 100.0% | ||
| 70 YEARS AND OVER | 3 | 14 | 17 | |
| 17.6% | 82.4% | 100.0% | ||
| Total | 72 | 250 | 322 | |
| 22.4% | 77.6% | 100.0% | ||
Age of the respondents versus self-medicating because of distance.
Respondents aged 18-29 years8.6% reported distance as a factor leading to self-medicating and none of the respondents aged 70 years reported distance as a factor, as shown in the Table 4.7 below.
Table 4.7 Age of the respondents versus self-medicating because of distance.
| Self-medicating because of distance | Total | |||
| YES | NO | |||
| Age of the respondents | 18-29 YEARS | 3 | 32 | 35 |
| 8.6% | 91.4% | 100.0% | ||
| 30-39 YEARS | 4 | 67 | 71 | |
| 5.6% | 94.4% | 100.0% | ||
| 40-49 YEARS | 7 | 78 | 85 | |
| 8.2% | 91.8% | 100.0% | ||
| 50-59 YEARS | 5 | 62 | 67 | |
| 7.5% | 92.5% | 100.0% | ||
| 60-69 YEARS | 4 | 43 | 47 | |
| 8.5% | 91.5% | 100.0% | ||
| 70 YEARS AND OVER | 0 | 17 | 17 | |
| 0.0% | 100.0% | 100.0% | ||
| Total | 23 | 299 | 322 | |
| 7.1% | 92.9% | 100.0% | ||
Where the respondents were treated versus harassed by health care giver.
The respondents treated from a pharmacy 19.6% (n=10) reported being harassed and none reported being harassed from herbalist/traditional healer, as shown in the Table 4.8 below
Table 4.8 Where the respondents were treated versus Harassed by health care giver.
| Harassed by a health care giver. | Total | |||
| YES | NO | |||
| Where the respondent was treated | HOSPITAL/EYE CLINIC | 27 | 177 | 204 |
| 13.2% | 86.8% | 100.0% | ||
| BOUGHT DRUGS FROM A PHARMACY | 10 | 41 | 51 | |
| 19.6% | 80.4% | 100.0% | ||
| TREATED BY AN HERBALIST/TRADITIONAL HEALER | 0 | 7 | 7 | |
| 0.0% | 100.0% | 100.0% | ||
| OTHERS SPECIFY-LEFT-OVERS, | 6 | 54 | 60 | |
| 10.0% | 90.0% | 100.0% | ||
| Total | 43 | 279 | 322 | |
| 13.4% | 86.6% | 100.0% | ||
Highest level of education of the respondents versus Sex of the respondents
The level of education is uniform across the sex with majority being respondents with secondary level of education and being males 23.3% (n=75), as shown in the Figure 4.7 below.
Figure 4.7 Highest level of education of the respondents in correlation to the sex of the respondents.

For validation purposes, the researcher initially submitted a sample of the set of survey questionnaires and after approval; the survey was conducted to 31 respondents which is a 10% of the total sample size. This carried out randomly at the Sabatia Sub County Hospital. The essence of the pilot testing is to get preliminary results on the understanding of the questionnaires by the respondents which aided in further improvement of the tool.
Main presenting symptom versus drug the respondents used.
Most of the respondents 51.6% presenting with redness of eyes are likely to use antibiotics though majority of respondents reported not knowing the type of drug used, as shown in Table 4.3 below.
Table 4.3: Main presenting symptom versus drug the respondents used crosstabulation.
| Drug the respondent used | Total | |||||
| STEROIDS | ANTIBIOTICS | ANTI-ALLERGIES | DON’T KNOW THE TYPE | |||
| Main presenting symptom | REDNESS | 9 | 33 | 2 | 20 | 64 |
| 14.1% | 51.6% | 3.1% | 31.3% | 100.0% | ||
| PAIN | 9 | 28 | 2 | 18 | 57 | |
| 15.8% | 49.1% | 3.5% | 31.6% | 100.0% | ||
| DISCHARGE | 3 | 13 | 3 | 35 | 54 | |
| 5.6% | 24.1% | 5.6% | 64.8% | 100.0% | ||
| SWELLING | 2 | 7 | 2 | 44 | 55 | |
| 3.6% | 12.7% | 3.6% | 80.0% | 100.0% | ||
| REDUCED VISION | 7 | 12 | 0 | 72 | 91 | |
| 7.7% | 13.2% | 0.0% | 79.1% | 100.0% | ||
| OTHERS=FOREIGN BODY SESANTION | 0 | 0 | 0 | 1 | 1 | |
| 0.0% | 0.0% | 0.0% | 100.0% | 100.0% | ||
| Total | 30 | 93 | 9 | 190 | 322 | |
| 9.3% | 28.9% | 2.8% | 59.0% | 100.0% | ||
Highest level of education of respondents versus used traditional herbs to treat an eye illness.
Respondents with no education 25.5% (n=12) reported use of traditional herbs whereas respondents with primary education and above are less likely to use herbs, as shown in the Table 4.4 below.
Table 4.4 Highest level of education versus used traditional herbs to treat an eye illness
| Used traditional herbs to treat an eye illness. | Total | |||
| YES | NO | |||
| Highest Level of education of the respondents | NO EDUCATION | 12 | 35 | 47 |
| 25.5% | 74.5% | 100.0% | ||
| PRIMARY | 5 | 46 | 51 | |
| 9.8% | 90.2% | 100.0% | ||
| SECONDARY | 12 | 127 | 139 | |
| 8.6% | 91.4% | 100.0% | ||
| COLLEGE AND UNIVERSITY | 2 | 83 | 85 | |
| 2.4% | 97.6% | 100.0% | ||
| Total | 31 | 291 | 322 | |
| 9.6% | 90.4% | 100.0% | ||
The cause of the illness versus where the respondents were treated.
Majority 63.4% (n=204) reported treatment in a hospital. Respondents with trauma 41.8% reported use of drug left overs and were less likely to seek hospital treatment, as shown in the table 4.5 below.
Table 4.5 The cause of the illness versus where the respondents were treated.
| Where the respondent was treated | Total | |||||
| HOSPITAL/EYE CLINIC | BOUGHT DRUGS FROM A PHARMACY | TREATED BY AN HERBALIST/TRADITIONAL HEALER | OTHERS SPECIFY-LEFT-OVERS, | |||
| The cause of the illness | INFECTION | 128 | 15 | 1 | 12 | 156 |
| 82.1% | 9.6% | 0.6% | 7.7% | 100.0% | ||
| TRAUMA | 26 | 24 | 3 | 38 | 91 | |
| 28.6% | 26.4% | 3.3% | 41.8% | 100.0% | ||
| BAD OMEN IN THE COMMUNITY | 37 | 6 | 2 | 1 | 46 | |
| 80.4% | 13.0% | 4.3% | 2.2% | 100.0% | ||
| OTHERS SPECIFY-INSECTS, ALLERGY, | 13 | 6 | 1 | 9 | 29 | |
| 44.8% | 20.7% | 3.4% | 31.0% | 100.0% | ||
| Total | 204 | 51 | 7 | 60 | 322 | |
| 63.4% | 15.8% | 2.2% | 18.6% | 100.0% | ||
Age of the respondents versus used milk as a mode of eye treatment.
Respondents aged 60-69 years reported use of milk as a mode of treatment 40.4% (n=19), as shown in the Table 4.6 below.
Table 4.6 Age of the respondents versus Used milk as a mode of eye treatment.
| Used milk as a mode of eye treatment. | Total | |||
| YES | NO | |||
| Age of the respondents | 18-29 YEARS | 3 | 32 | 35 |
| 8.6% | 91.4% | 100.0% | ||
| 30-39 YEARS | 16 | 55 | 71 | |
| 22.5% | 77.5% | 100.0% | ||
| 40-49 YEARS | 18 | 67 | 85 | |
| 21.2% | 78.8% | 100.0% | ||
| 50-59 YEARS | 13 | 54 | 67 | |
| 19.4% | 80.6% | 100.0% | ||
| 60-69 YEARS | 19 | 28 | 47 | |
| 40.4% | 59.6% | 100.0% | ||
| 70 YEARS AND OVER | 3 | 14 | 17 | |
| 17.6% | 82.4% | 100.0% | ||
| Total | 72 | 250 | 322 | |
| 22.4% | 77.6% | 100.0% | ||
Age of the respondents versus self-medicating because of distance.
Respondents aged 18-29 years8.6% reported distance as a factor leading to self-medicating and none of the respondents aged 70 years reported distance as a factor, as shown in the Table 4.7 below.
Table 4.7 Age of the respondents versus self-medicating because of distance.
| Self-medicating because of distance | Total | |||
| YES | NO | |||
| Age of the respondents | 18-29 YEARS | 3 | 32 | 35 |
| 8.6% | 91.4% | 100.0% | ||
| 30-39 YEARS | 4 | 67 | 71 | |
| 5.6% | 94.4% | 100.0% | ||
| 40-49 YEARS | 7 | 78 | 85 | |
| 8.2% | 91.8% | 100.0% | ||
| 50-59 YEARS | 5 | 62 | 67 | |
| 7.5% | 92.5% | 100.0% | ||
| 60-69 YEARS | 4 | 43 | 47 | |
| 8.5% | 91.5% | 100.0% | ||
| 70 YEARS AND OVER | 0 | 17 | 17 | |
| 0.0% | 100.0% | 100.0% | ||
| Total | 23 | 299 | 322 | |
| 7.1% | 92.9% | 100.0% | ||
Where the respondents were treated versus harassed by health care giver.
The respondents treated from a pharmacy 19.6% (n=10) reported being harassed and none reported being harassed from herbalist/traditional healer, as shown in the Table 4.8 below
Table 4.8 Where the respondents were treated versus Harassed by health care giver.
| Harassed by a health care giver. | Total | |||
| YES | NO | |||
| Where the respondent was treated | HOSPITAL/EYE CLINIC | 27 | 177 | 204 |
| 13.2% | 86.8% | 100.0% | ||
| BOUGHT DRUGS FROM A PHARMACY | 10 | 41 | 51 | |
| 19.6% | 80.4% | 100.0% | ||
| TREATED BY AN HERBALIST/TRADITIONAL HEALER | 0 | 7 | 7 | |
| 0.0% | 100.0% | 100.0% | ||
| OTHERS SPECIFY-LEFT-OVERS, | 6 | 54 | 60 | |
| 10.0% | 90.0% | 100.0% | ||
| Total | 43 | 279 | 322 | |
| 13.4% | 86.6% | 100.0% | ||
Highest level of education of the respondents versus Sex of the respondents
The level of education is uniform across the sex with majority being respondents with secondary level of education and being males 23.3% (n=75), as shown in the Figure 4.7 below.
Figure 4.7 Highest level of education of the respondents in correlation to the sex of the respondents.
DISCUSSION
The research found out majority, (54.7%) of self-medicating respondents are males compared to females (45.3%). This is consistent with findings from other studies such as Marquez, et al, (2014), (33%) of the males reported self-medicating whereas (20%) of females reported self-medicating(E. Marquez, 2014a). About 51.3% of the patients were male, and 48.7% were female, in their study they both argue that among adults, falling in the ages between 18-70 years, the prevalence of self-medicating is higher among males than females(Carvalho et al., 2009). This higher prevalence level of ocular self-medicating in males is largely attributed to ignorance whereby, the male counterparts tend to believe that they are endowed with good knowledge about ocular drugs hence they believe to be at a position to make reasonable ocular self-medicating decisions. Another study observed that in families consisting of only one parent in which case the parent was a father, there were a highly likely that the children would be subjected to self-medication (12%) than in the case where the parent was a mother at (4%)(Ayanniyi et al., 2010). However, Asiedu K. (2016) in his studies found out that there was a high prevalence level of self-medicating among female participants than men with the results indicating that females are twice as likely to self-medicate more than their male counterparts. Additionally, the researcher suggests that females who use contraceptives were four times likely to self-medicate using topical ocular medication due to the possible symptoms of dry eyes as a result of contraceptive use(Ezinne et al., 2023).
Among the total respondent, 26.4% were in the age group 40-49 years while 5.3% (n=17) were aged 70 years or more years across the gender. Respondents aged 40-49 years (33%) are more likely to buy drugs from a pharmacy whereas respondents aged 30-69 years are more likely to seek traditional healer/herbalist care 42.9%. This shows that self-medication increases as a person ages reaching peak level at mid-life before dropping again to its lowest in respondents above the age of 70 years. Generally according to Kyei et al., (2014) self-medication at ages 17-25 years was (94.9%) and above 25years (5.1%). Observes that as people age, their tendencies to visit medical practitioners for health checkup tends to increase which leads to the low prevalence of ophthalmic self-medication(Kyei et al., 2014). Majority of the respondent are patient with a secondary level of education 43.2% while patients with no education 14.6% are the least, with the Males as the majority with Secondary education 23.3% compared to females 19.9% and on the other hand Females with no education are more 7.8% and males 6.8%. Majority of respondents with secondary education (27.3%) don’t know the type of drug used, respondents with a college or Degree level of education are more likely to self-medicate with antibiotics (11.5%). This is backed by, Asiedu K. et al (2016), they noted in their study that among undergraduate students 77% were self-medicating in the University of Cape Coast in Ghana(Ezinne et al., 2023).
A sizeable number of the respondents 9.6% felt cost was a leading factor to self-medication. Most of the males (49.7%) never considered cost as a motivating factor towards self-medication, however more males were likely to self-medicate (5%) than females (4.7%). Kumar, R., et al (2017), they noted that traditional eye medicine was commonly used (25.7%) in the Rural set up in India as they would rather self-medicate to save a few pennies in the process(Sánchez et al., 2020). Kyei et al., (2014) assert that people in a high socioeconomic class (73.9%) are likely to be more aware of their ocular health needs compared to (41.9%) of people of low social economic status which implies why they are more likely to self-medicate. He noted that financial implications of a community determine the likely mode of treatment that a patient is likely to undertake in case one suffers from an ocular condition (37.0%) of the respondents(Kyei et al., 2014). It was noted majority of the respondents (59%) didn’t know the type of ocular drug used,28.9% had used antibiotics,9.3% used steroids and 2.8% used anti-allergies. 80% of the patients presenting with swelling reported not knowing the type of drug used and 51.6% presenting with redness reported using antibiotics while respondents with reduced vision reported no use of anti-allergies.
Traditional practices were found to be significant methods used to cure eye illnesses (9.6%) of the respondents.10.2% of the respondents reporting having broken a stick in front of the eye to cure a certain eye illness and 22.4% reported use of milk as a means of treatment and respondents at the age bracket 60-69 years (40.4%) reported use of milk as a mode of treatment while 18-29 years (8.6%) was the least. Respondents aged 40-69 years are more likely to use traditional herbs to treat eye illness. Noopur Gupta, et al, (2017) in their population-based study in rural India, noted that traditional eye medicine was commonly used (25.7%) in this rural population in the form of ‘surma/kajal’ honey, ghee, rose water and other plant, dairy and animal products. He goes ahead to say the commonest sources of eye-related health information in this study population were villagers themselves that included neighbor’s, relatives and traditional healers (73.5%)(Gupta et al., 2017). This correlates with findings of Regina Souza Carvalho et al. (2009), study that noted (40.5%) of patients with conditions considered to be ocular emergencies reported self-medicating with homemade medicines or preparations before seeking professional emergency care. The most frequently used products included a boric acid solution (53.3%, a normal saline solution (35.7%), herbal infusions (6.1%) and breast milk (4.8%). Majority 63.4% of the respondents reported treatment in a hospital, Pharmacies 15.8%, Traditional/Herbalist 2.2% and from other sources like drug-left overs 18.6%. Noopur Gupta, et al, (2017) noted that 14.2% did not consult an eye care provider in their study at a Rural India. 41.8% of respondents with trauma as the cause of illness reported use of drug left overs and it is noted all patients reporting trauma as cause of illness were less likely to seek hospital treatment than all other causes. Noopur Gupta et al (2014) noted that no treatment was sought by patients of ocular injury 41.2% and that (18%) presented to non-ophthalmologist while (14%) took treatment from traditional healers. Traditional eye medicine was used by 16.4% of patients with ocular injury (Gupta et al., 2017).
The study also revealed that 25.5% of total respondents with no education reported use of traditional herbs whereas only 2.4% of respondents with college and university education reported using herbs for treatment. Kumar R et al in a study Around Kishangani, Bihar (59.4 %) of the patients misusing eye drops who had basic education, (59.4%), (19.8%) were illiterates, and (20%) were graduates and above. (Gupta et al., 2017).
This shows that education is a strong factor that broadens ones thinking and reasoning. Reduced vision 28.3% was the chief complain redness 19.9%, pain17.7%, swelling 17.1%, discharge 16.8% and others like foreign body sensation 0.3%. Catherine U et al (2004) (50.4%) patients presented with poor vision Ajayi et al (2013) noted that blurry vision (49.2%), itchiness 23.7%, reddening 9.8%, pain 9.8%, growth 4.3% and watery eyes (2.7%). Majority of respondents (90.4%) never considered the seriousness of the illness as a motivating factor to self-medicating whereas 9.1% said the seriousness of the illness contributed to self-medication. Majority of respondents 57.1% who were treated in a hospital said seriousness of eye infection was not a motivating factor whereas those treated by an herbalist were the minority1.6%. The considerations that some ocular symptoms could be minor ailments that can be easily treated are one of the reasons that people resort to self-medicating, according to Kyei et al., (2014) (32.1%), most of self-medicated ocular complications are borne by rural dwellers who are more likely to use Traditional emergency medicine than urban dwellers (54.9%)(Kyei et al., 2014).This is largely contributed by ignorance and illiteracy.
A sizeable number of respondents 7.1% said distance contributed to self-medication. Kyei et al noted that (3.1%) of respondent said distance to the health facility contributed to self-medication(Kyei et al., 2014). Nwosu and Obidiozor (2011) observe that (13.2%) of ocular patients who visited a tertiary eye hospital in Nigeria had previously sought treatment by using traditional eye medicines which the researcher suggests was due to long distances that the patients have to cover to visit an ophthalmic eye clinic(Nwosu & Obidiozor, 2011).Waiting time or length of queue led 4.7% of the respondents to self-medication, with a missing factor respondent. Majority of males (51.4%) said they never self-medicated because of long waiting time or due to long hospital queues. Omotoye et al., (2017) goes on to suggest that patients can easily be discontented by the numerous procedures and processes that they may have to undergo before finally seeing the eye care specialist(Ajayi et al., 2013). Some respondents13.4% reported harassment by healthcare givers. Majority of Males 8.1% reported being harassed by health care givers unlike females 5.3% who reported being harassed by health care givers. Kyei et al noted that (3.1%) of the respondents reported lack of trust in medical care. Multiple studies concluded that the prevalence of ocular self-medication among eye patients living in rural areas was influenced and facilitated by lack of readily available quality ophthalmic services(Ajayi et al., 2013; Gupta et al., 2017). Harassment influenced choice of treatment as 19.6% of respondents who bought drugs from the pharmacy reported harassment by a health care giver whereas none reported harassment by herbalist/traditional healer. Nwosu and Obidiozor, (2011) observed that although in most cases it is the elderly people in the community who prefer self-medicating using traditional eye medicine, their influence as senior and respected members of the society could influence other community or family members to try the traditional medicine which may result to high prevalence of ocular self-medicating(Nwosu & Obidiozor, 2011). In another study, (54.8%) in a study Incidence and complications of Traditional Eye Medications in Nigeria in a Teaching Hospital(Ukponmwan & Momoh, 2010). They conclude that Traditional emergency medicine is a common practice that is harmful and lead to blindness.
CONCLUSION
- Males 54.7% are more likely to self-medicate than females 45.3% with the age group between 40-49 years (43.2%), being the most likely to self-medicate and those with secondary education 43.2%.
- Most respondents don’t know the type of drugs used in self-medication.
- Rampant use of antibiotics and other remedies without specialized advice,
- Some respondents attempt to treat ophthalmic emergencies like ocular trauma that require ophthalmologic care.
- Respondents waiting time and harassment by healthcare givers had a significant effect on the self-medication practices.
- Pharmacies allow over the counter purchase of prescription only drugs
RECOMMENDATIONS
- Health Providers should have quality time with patient coupled with proper counseling on use of drugs as this is regarded as one of the essential components of the overall medicine use process.
- Rules and regulations on dispensing of medicines from pharmacies should be reinforced.
- Expansion of health insurance services hence reducing the prevalence of self-medication practices and help in realization of vision 2020.
- Train and employ more eye care providers.
REFERENCES
- Ajayi, I. A., Omotoye, O. J., Ajite, K. O., Fadamiro, C. O., & Ajayi, E. A. (2013). Self Medication Practices among Patients seen in A Suburban Tertiary Eye Care Centre in Nigeria. Asian Journal of Medical Sciences, 5(2), 85–90. https://doi.org/10.3126/AJMS.V5I2.8452
- ArulJothi, K, N., Irusappan, S., Amarnath, G., Chandrasekaran, S., K, S. A. B., Harishankar, M., Babu, J. V, & A, D. (2014). Self–medication and Over–The–Counter medicine usage among the University students in Chidambaram. IJSR – International Journal of Scientific Research, Volume 3 Issue 1(2), 63–65. https://doi.org/10.36106/IJSR
- Ayanniyi, A. A., Olatunji, F. O., Mahmoud, A. O., & Ayanniyi, R. O. (2010). Knowledge and attitude of guardians towards eye health of primary school pupils in Ilorin, Nigeria. The Nigerian Postgraduate Medical Journal, 17(1), 1–5. https://doi.org/10.4103/1117-1936.181414
- Bennadi, D. (2013). Self-medication: A current challenge. Journal of Basic and Clinical Pharmacy, 5(1), 19. https://doi.org/10.4103/0976-0105.128253
- Carvalho, R. S., Kara-José, N., Temporini, E. R., Kara-Junior, N., & Noma-Campos, R. (2009). Self-Medication: Initial Treatments Used by Patients Seen in an Ophthalmologic Emergency Room. Clinics, 64(8), 735–741. https://doi.org/10.1590/S1807-59322009000800005
- Marquez, G. (2014a). Eye Drop Self-medication: Comparative Questionnaire-based Study of Two Latin American Cities. Journal of Clinical & Experimental Ophthalmology, 05(02). https://doi.org/10.4172/2155-9570.1000330
- Marquez, G. (2014b). Eye Drop Self-medication: Comparative Questionnaire-based Study of Two Latin American Cities. Journal of Clinical & Experimental Ophthalmology, 05(02). https://doi.org/10.4172/2155-9570.1000330
- Ezinne, N., James, S., Alemu, H. W., Cheklie, T., Ekemiri, K., & Mohammed, R. (2023). High Prevalence of Symptomatic Dry Eye Disease Among University Students During the COVID-19 Pandemic in University of West Indies, Trinidad and Tobago. Clinical Optometry, 15, 37–43. https://doi.org/10.2147/OPTO.S396135
- Fainzang, S. (2013). The Other Side of Medicalization: Self-Medicalization and Self-Medication. Culture, Medicine and Psychiatry, 37(3), 488–504. https://doi.org/10.1007/s11013-013-9330-2
- Gupta, N., Vashist, P., Tandon, R., Gupta, S. K., Kalaivani, M., & Dwivedi, S. N. (2017). Use of traditional eye medicine and self-medication in rural India: A population-based study. PLoS ONE, 12(8). https://doi.org/10.1371/JOURNAL.PONE.0183461
- Kyei, S., Ocansey, S., Abu, E. K., & Gyedu, B. N. (2014). Appraisal of the practice of ocular self-medication in Cape Coast Metropolis, Ghana. Optometry Reports, 4(1). https://doi.org/10.4081/optometry.2014.2164
- Nation, D. (2011). Self-medication rises as prescription drugs bought over counter | Nation. https://nation.africa/kenya/news/self-medication-rises-as-prescription-drugs-bought-over-counter–758962
- Nwosu, S. N. N., & Obidiozor, J. U. (2011). Incidence and risk factors for traditional eye medicine use among patients at a tertiary eye hospital in Nigeria. Nigerian Journal of Clinical Practice, 14(4), 405–407. https://doi.org/10.4103/1119-3077.91744
- Sánchez, M., González-Burgos, E., Iglesias, I., & Gómez-Serranillos, M. P. (2020). Pharmacological Update Properties of Aloe Vera and its Major Active Constituents. Molecules, 25(6). https://doi.org/10.3390/MOLECULES25061324
- Sarahroodi, S., & Mikaili, P. (2012). Self-medication with antibiotics: A global challenge of our generation. Pakistan Journal of Biological Sciences, 15(14), 707–708. https://doi.org/10.3923/pjbs.2012.707.708
- Shabani, Z., & Redican, K. (2017). Evaluation of Self-medication with Antibiotics among Adults in Kosovo. Annals of Global Health, 83(1), 7. https://doi.org/10.1016/j.aogh.2017.03.015
- Shaikh, S., Saleem, Y., Noushad, S., & Ahmed, S. (2017). Pain, Self-Medication and Administration of Over-The-Counter Analgesics: An Observational Study. Annals of Psychophysiology, 4(1), 78–83. https://doi.org/10.29052/2412-3188.v4.i1.2017.78-83
- Ukponmwan, C., & Momoh, N. (2010). Incidence and complications of traditional eye medications in Nigeria in a teaching hospital. Middle East African Journal of Ophthalmology, 17(4), 315. https://doi.org/10.4103/0974-9233.71596
- Wafula, F., Abuya, T., Amin, A., & Goodman, C. (2014). The policy-practice gap: Describing discordances between regulation on paper and real-life practices among specialized drug shops in Kenya. BMC Health Services Research, 14(1), 1–11. https://doi.org/10.1186/1472-6963-14-394