
Health Professionals’ Awareness of Signs and Symptoms of Oropharyngeal Dysphagia among inpatients at a Level – Six Referral Hospital in Kenya
- Dalphine C. Ndiema
- T. Abuom
- M. Karia
- 369-380
- Apr 8, 2024
- Business Management
Health Professionals’ Awareness of Signs and Symptoms of Oropharyngeal Dysphagia among inpatients at a Level – Six Referral Hospital in Kenya
Dalphine C. Ndiema*, T. Abuom, M. Karia
Department of Early Childhood Studies & Special Needs Education (Speech – Language Pathology), Kenyatta University, Nairobi, Kenya
*Corresponding Author
DOI: https://doi.org/10.51244/IJRSI.2024.1103026
Received: 05 March 2024; Revised: 31 March 2024; Accepted: 04 April 2024; Published: 09 April 2024
ABSTRACT
Background: Oropharyngeal dysphagia is a leading risk factor for multiple health complications, including malnutrition, chest infections, and pneumonia. High dysphagia awareness among health professionals may facilitate early identification and treatment.
Objectives: This study’s objectives were to (i) determine oropharyngeal dysphagia signs/symptoms awareness levels among healthcare professionals attending to adult inpatients in the acute-care facility of a Kenyan level-six referral hospital and (ii) establish whether their awareness levels vary with selected individual characteristics.
Methods: We employed a descriptive, cross-sectional research design, and purposive sampling of 16 health professionals attending to inpatients in the hospital’s acute-care facility. They included five (5) nurses, seven (7) physiotherapists, one (1) speech – language therapists, one (1) oncologist, one (1) neurologist, and one (1) nutritionist. Awareness levels were measured using a 16-item questionnaire. Frequencies, percentages, and means were used to summarize participants’ scores, while the independent samples t-test and one-way ANOVA were used to compare the scores across selected individual characteristics.
Results: The mean proportion of correct responses was 73.0% (SD = 17.49), indicating that on average, participants had moderate awareness. Over half (56.3%, n = 9) had either low or moderate OPD signs/symptoms awareness levels. There were significant differences in mean awareness levels due to age (F = 10.13, p = .002) and educational attainment ( F = 7.44, p = .007).
Conclusions: Health professionals attending to adult inpatients in the hospital’s medical and surgical units have, on average, moderate awareness of oropharyngeal dysphagia signs and symptoms. High educational attainment is associated with increased awareness.
Recommendation: The hospital’s management should implement regular training programs focusing on various OPD management aspects, particularly its signs and symptoms. Priority should be given to nurses, physiotherapists, and HPs without a post-graduate degree. For better client outcomes, and opportunity for continuous professional development
Keywords: awareness; oropharyngeal dysphagia; signs/symptoms; inter-professional collaboration
INTRODUCTION
The swallowing reflex in humans plays a vital role in nutrition and airway protection [1,2]. Difficulty swallowing is a characteristic of a disorder termed as dysphagia [3]. There are various dysphagia types, depending on the positioning of the swallowing impairment [4, 5]. Oropharyngeal dysphagia, which affects over 40% of the world’s population, is among the most prevalent dysphagia forms, and is the focus of this paper [6]. This disorder affects the oral transit phase of the swallowing process, leading to difficulties in mixing the bolus and placing it on the tongue [3]. In Kenya, over 70% of stroke patients are likely to be diagnosed with dysphagia [7]. Persons with dysphagia are highly prone to multiple conditions, including, choking, dehydration, malnutrition, and aspiration pneumonia [3,8]). They are also at increased risk of extended hospital stays, re- admissions, institutionalization, and mortality [9,10,11].
Early OPD identification is critical to improve the autonomy and functional life of patients with this condition [8,12,13,14,15]. Early identification and screening is, in turn, possible only if all health professionals (HPs) interacting with OPD patients are aware of its manifestations. In many healthcare settings, OPD management is traditionally the role of speech- language pathologists or therapists (SLTs). Yet, OPD co-occurs with several conditions and cuts across many healthcare domains [17]. Hence, there is a growing recognition of the need for a multi-disciplinary approach to OPD management, considering today’s complex healthcare delivery systems [18].
The World Health Organization (WHO)’s Inter-professional (IPC) model offers a valuable framework for inter-disciplinary collaboration in OPD management. At its core, IPC emphasizes the importance of collaboration between HPs from varied specialties to deliver effective and comprehensive care to patients [18]. By promoting collaboration and communication between diverse HPs, IPC could facilitate effective dysphagia management and enhanced patient outcomes [19,20,21,22].
Professionals across all disciplines should be able to recognize OPD manifestations in various settings if they are to collaborate effectively in its management [22,23]. However, there are global concerns of low OPD awareness among HPs, implying that in many cases, OPD is under-diagnosed, misdiagnosed, and/or over-diagnosed [6,23,24,25,26,27]. Few studies have evaluated dysphagia awareness among HPs in Kenya. However, some studies have shown that most nurses in the country are not actively involved in swallowing disorder management. Instead, they assume that OPD screening is dependent primarily on physicians’ input [7,28,29]. Such findings bring into question the extent to which HPs in Kenya are prepared to offer quality care to patients at risk or diagnosed with OPD.
Drawing on this gap, we designed a study to establish OPD awareness levels among HPs attending to inpatients in the medical and surgical units (acute- care facility) of a level-six, referral hospital in Kenya. Our objectives were to:
- Determine OPD signs/symptoms awareness levels among HPs attending to adult inpatients in the hospitals acute-care facility (ACF), and
- Establish if OPD signs/symptoms awareness levels among the HPs vary with selected individual
The study’s findings may give medical professionals and other caregivers the information needed to treat OPD patients holistically. Their awareness and involvement are essential to guaranteeing that patients are accurately evaluated for OPD treatment and receive appropriate referrals. They could influence future clinical and family training programs and specific algorithms for OPD management in Kenyan hospitals.
METHODS
Study design
We adopted a cross-sectional, descriptive design to help develop a comprehensive understanding of OPD awareness among the hospital’s HPs. Quantitative methods were used to establish HPs’ awareness levels.
Setting
The study was conducted at a level-six referral hospital in Nairobi City County, Kenya. A previous survey on OPD presentation in the hospital showed that about 62.1% of initial adult SLT consultations in the ACF had OPD diagnoses [30]. Yet, no study had assessed dysphagia awareness levels among its HPs.
Sampling strategy
The target population comprised 63 HPs attending to inpatients at the hospital’s medical and or surgical wards. We employed a purposive sampling procedure to select only HPs that were expected to interact with patients with swallowing disorders. We sampled 30% of the 63 HPs [31], making up a sample of 19 individuals. They were distributed proportionately across the various HP categories, as shown in Table 1.
Table 1: Sample matrix
| Category | Population Size (N) | Sample Size (n) | n/N (%) |
| Med. officers/ specialists | 12 | 4 | 33.3 |
| Nurses | 18 | 6 | 30.0 |
| Nutritionists | 4 | 1 | 25.0 |
| Physiotherapists | 25 | 7 | 28.0 |
| SLP/Ts | 2 | 1 | 50.0 |
| Total | 63 | 19 | 30.2 |
Research instrument
We adapted a previously validated structured questionnaire to generate data on participants’ OPD awareness levels [32,33]. The instrument assessed participants’ OPD signs/symptoms awareness levels using 16 items. For quality assurance, a pilot study was conducted in a level – six (national) referral hospital in Nairobi City County, Kenya, with similar participants as the study’s sample but different from the main group. The instruments were probed and individual items reviewed to ensure the tools measured the variables under examination. We also established the questionnaire’s stability by employing the test-retest procedure within a 15-days window. Pearson’s product- moment correlation coefficient showed a high test- retest reliability (r = .834).
Data collection and analysis
The questionnaires were delivered online through Google Forms following approvals by the Kenya National Commission for Science Technology and Innovation (NACOSTI). Responses to the questionnaire items were entered into SPSS (v. 26) and then coded into quantitative values using appropriate scales. Two experts entered and coded the data independently. Their datasets were then compared for inconsistencies, and adjustments were made as appropriate. Finally, the records were checked for missing values and anomalies.
Raw frequencies, percentages, and means were used to summarize the data and identify key patterns. We then employed the independent samples t-test and one-way ANOVA to compare participants’ awareness levels across categories of selected demographic and general characteristic variables. Tests of significance were performed at the 95% confidence level.
Ethical considerations
The study adhered to all ethical guidelines stipulated by Kenyatta University’s Ethical Review Committee.
RESULTS
Participant characteristics
The original sample comprised 19 HPs from different specialties (Table 1). Sixteen (16) completed the questionnaires, translating into an 84.2% return rate. Demographic data included gender, age, education attainment, work experience, and area of specialization (work units) (Table 2). We also asked participants if they had attended a swallowing disorder training program.
Table 2: Participant demographic and general characteristics
| Characteristic | Category | n | % |
| Gender | Male | 8 | 50.0 |
| Female | 8 | 50.0 | |
| Age group | 25-30 years | 6 | 37.5 |
| 31-35 years | 5 | 31.3 | |
| 36-40 years | 5 | 31.3 | |
| Educational attainment | Diploma | 4 | 25.0 |
| Bachelor | 8 | 50.0 | |
| Post-graduate | 4 | 25.0 | |
| Experience | 4-6 years | 5 | 31.3 |
| 7-9 years | 5 | 31.3 | |
| > 9 years | 6 | 37.5 | |
| Specialization | Nurse | 5 | 31.3 |
| Physiotherapist | 7 | 43.8 | |
| Other (SLT, neurologist, oncologist,
nutritionist) |
4 | 25.0 | |
| Training | No | 10 | 62.5 |
| Yes | 6 | 37.5 |
Awareness levels of oropharyngeal dysphagia signs and symptoms
Our first objective was to determine OPD signs and symptoms awareness levels among HPs attending to adult inpatients in the hospital’s ACF. Participants were presented with 16 signs/symptoms items and asked to pick the ones that applied to OPD. The assumption was that the number of correctly identified items would reflect their awareness of OPD signs and symptoms. Table 3 shows the responses. The table gives raw frequencies and percentages of the totals (in brackets). The “N” column shows the number of participants who responded to an item. The maximum possible value of N is 16.
All participants agreed that coughing or choking during or after swallowing and feeling food getting stuck in the throat are OPD manifestations. The majority considered choking on saliva during non-meal times, food remaining in the mouth, weight loss, drooling, increased mealtime, and multiple swallows as OPD manifestations. Only a slight majority agreed that poor tongue movement, poor chewing, and coughing during aspiration are OPD signs or symptoms. On the other end, the majority of the 15 who answered the “skin irritations” item (80%, n = 12) disagreed it is an OPD sign or symptom. The responses to the remaining items were near-equally distributed between those who agreed and those who disagreed.
Awareness levels were then assessed by computing the number of correct responses for each participant and sign/symptom item. The mean proportion of correct responses was 73.0% (SD = 17.49). Stated differently, on average, each participant responded correctly to 73.0% of the questions. The study used the following scheme to categorize awareness levels: < 50% = low, 50-75% = moderate, and > 75% = high awareness. Based on this classification, the sample had, on average, moderate awareness of OPD signs/symptoms. The participant with the lowest awareness level scored 43.8% (low), while only 12.5% (n = 2) matched all the items correctly. Slightly over half (56.3%, n = 9) had low-moderate OPD signs or symptoms awareness levels, while the other 43.8% had high awareness (Figure 1).
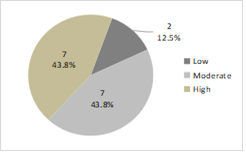
Figure 1: Signs/symptoms awareness levels grouped as low, moderate, or high
The researcher then computed aggregate awareness levels of specific OPD signs/symptoms by determining the number of participants who responded correctly to each item (Table 4). The symptoms with the highest scores were coughing/choking during/after swallowing and feeling of food getting stuck in the throat. All participants answered correctly to these two items. High awareness levels were reported for nine (9) symptoms/signs. Over 75% participants responded correctly to these items.
The lowest-scored items were always coughing during aspiration, difficulty closing lips, and chest pain. Although coughing during silent aspiration is not an OPD symptom, 73.3% (n = 11) selected it as an OPD symptom. On the other end, 53.6% (n = 9) did not feel that difficulty closing lips and chest pains are OPD symptoms, although these two are among the primary OPD manifestations. These results highlight the need for ongoing training on signs/symptoms awareness among the HPs in the hospital’s ACF.
Table 3: Responses to OPD signs/symptoms awareness items
| Sign or Symptom | Agree, n (%) | Undecided, n (%) | Disagree, n (%) | N |
| Coughing/choke during or after a swallow | 16 (100) | 0 (0.0) | 0 (0.0) | 16 |
| Skin irritations | 1 (6.7) | 2 (13.3) | 12 (80.0) | 15 |
| Feeling of food getting stuck in the throat | 16 (100) | 0 (0.0) | 0 (0.0) | 16 |
| Choking on saliva during non-mealtimes | 14 (87.5) | 2 (12.5) | 0 (0.0) | 16 |
| Poor movement of the tongue | 10 (62.5) | 4 (25.0) | 2 (12.5) | 16 |
| Oral residue | 14 (87.5) | 1 (6.3) | 1 (6.3) | 16 |
| Poor chewing | 10 (62.5) | 1 (6.3) | 5 (31.3) | 16 |
| Patients cough if aspirating | 11 (73.3) | 0 (0.0) | 4 (26.7) | 15 |
| Difficulty closing lips | 7 (43.8) | 1 (6.3) | 8 (50.0) | 16 |
| Weight loss | 13 (81.3) | 1 (3.3) | 2 (12.5) | 16 |
| Frequent throat clearing after swallowing | 14 (17.5) | 2 (12.5) | 0 (0.0) | 16 |
| Hoarse voice | 9 (56.3) | 5 (31.3) | 2 (12.5) | 16 |
| Chest pain | 7 (43.8) | 2 (12.5) | 7 (43.8) | 16 |
| Anterior leakage (drooling) | 15 (93.8) | 0 (0.0) | 1 (6.3) | 16 |
| Increased meal-time duration | 13 (81.3) | 0 (0.0) | 3 (18.8) | 16 |
| Multiple swallows | 13 (81.3) | 3 (18.8) | 0 (0.0) | 16 |
Table 4: Number and percentage of correct responses to the signs/symptoms awareness items
| Sign or Symptom | n | % |
| Coughing/choke during/after a swallow | 16 | 100 |
| Skin irritations | 12 | 75.0 |
| Feeling of food getting stuck in throat | 16 | 100 |
| Choking on saliva during non- mealtimes | 14 | 87.5 |
| Poor movement of the tongue | 10 | 62.5 |
| Oral residue | 14 | 87.5 |
| Poor chewing | 10 | 62.5 |
| Patients cough if aspirating | 4 | 25.0 |
| Difficulty closing lips | 7 | 43.8 |
| Weight loss | 13 | 81.3 |
| Frequent throat clearing after swallowing | 14 | 87.5 |
| Hoarse voice | 9 | 56.3 |
| Chest pain | 7 | 43.8 |
| Anterior leakage (drooling) | 15 | 93.8 |
| Increased meal-time duration | 13 | 81.3 |
| Multiple swallows | 13 | 81.3 |
Differences in awareness levels due to individual characteristics
For the second objective, the researcher sought to establish whether signs/symptoms awareness levels depended on individual HPs characteristics. Awareness scores were compared across six participant characteristics: gender, age, educational attainment, work experience, specialization, and having attended a training program. For each variable, a test of significance was used to compare the signs/symptoms awareness scores (% of correct answers) across its categories. The distribution of the scores was first checked for normality using Shapiro-Wilk’s test. The test revealed that the distribution did not deviate significantly from the normal curve at the 95% confidence level (SW = .944, p = .403), allowing for the use of parametric methods. Specifically, the independent samples t-test was used for gender and training attendance comparisons, while one-way ANOVA was used for other variables. Table 5 presents the results.
Table 5: Awareness levels by participant characteristics
| Characteristic | Category | n | M | SD | t/F | p |
| Gender | Male | 8 | 68.75 | 19.19 | -0.98 | .343 |
| Female | 8 | 77.34 | 15.64 | |||
| Age group | 25-30 years | 6 | 59.38 | 10.27 | 10.13 | .002 |
| 31-35 years | 5 | 91.25 | 8.385 | |||
| 36-40 years | 5 | 71.25 | 15.68 | |||
| Education | Diploma | 4 | 60.94 | 5.916 | 7.44 | .007 |
| Bachelor | 8 | 68.75 | 5.148 | |||
| Post-graduate | 4 | 93.75 | 4.419 | |||
| Experience | 4-6 years | 5 | 61.25 | 10.27 | 2.21 | .149 |
| 7-9 years | 5 | 82.50 | 19.46 | |||
| 10 years and above | 6 | 75.00 | 17.23 | |||
| Specialization | Nurse | 5 | 65.00 | 13.69 | 6.52 | .011 |
| Physiotherapist | 7 | 66.94 | 14.75 | |||
| Other | 4 | 93.75 | 8.839 | |||
| Training | No | 10 | 73.75 | 14.37 | 0.201 | .844 |
| Yes | 6 | 71.88 | 23.30 |
The mean (M) values and standard deviations (SD) are in the fourth and fifth columns, respectively. The last two columns show the test statistics (t for the t- test and F for ANOVA) and corresponding p-values. All the models showed significant homogeneity in their variances based on Levene’s test (p > .050).
There was a significant difference in the mean signs/symptoms awareness levels due to age (F = 10.13, p = .002). The mean scores suggested that those aged 31-35 (M = 91.25%, SD = 8.385) and 25-30 (M = 59.38%, SD = 10.270) had, on average, the highest and lowest awareness levels, respectively. Post-hoc comparisons using Turkey’s honest significant difference (HSD) test revealed that the mean awareness level for the 31-35 years age group was significantly higher than those of groups 25-30 years (p = .002) and 36-40 years (p = .045). The difference between groups 25-30 and 36-40 was non-significant. Hence, for this sample, signs/symptoms awareness levels were higher among persons aged 31- 35 years than the other categories.
There was a significant difference in the mean awareness levels due to educational attainment (F = 7.44, p = .007). On average, those with a post-graduate degree and a diploma certificate had the highest and lowest symptoms/signs awareness levels, respectively. Post-hoc comparisons showed that the mean awareness level for post-graduates was significantly higher than for those with a diploma certificate (p =.008) and a bachelor’s degree (p = .018). The difference between awareness levels of those with a diploma certificate and a bachelor’s degree was non-significant (p = .583). Hence, for this sample, symptoms/signs awareness increased with educational attainment.
There was a significant difference in the mean awareness due to participants’ specialization areas (F = 6.52, p = .011). The values suggested that awareness levels were highest among HPs of the “other” category (neurologists, oncologists, nutritionists, and speech therapists) and almost equal for nurses and physiotherapists. Post-hoc comparisons indicated that the mean for “other” HPs was significantly higher than for both nurses and physiotherapists (p < .05), while the difference between nurses and physiotherapists was non-significant (p = .965). Hence, for this sample, symptoms/signs awareness was higher for neurologists, oncologists, nutritionists, and speech therapists than for nurses and physiotherapists. The differences due to other factors were non-significant.
DISCUSSION
There are increasing calls for a multi-disciplinary approach to dysphagia management, considering its multi-faceted nature [27,34]. Meeting this goal requires all HPs to have adequate dysphagia awareness levels. Drawing on the IPC model, we assessed OPD awareness levels among HPs attending to adult inpatients in the medical and surgical units of a level-six hospital in Kenya. This study, for the first time, reports on dysphagia awareness levels among HPs working in the hospital.
Participants had varied views on what constitutes OPD manifestations. They were not unanimous in their responses to all but two items (Table 3). Notably, some were unable to decide on some manifestations. The items with the most “unable to decide” responses were hoarse voice during/after swallowing (31.3%, n = 5) and poor tongue movement (25.0%, n = 4). Given that these two are critical OPD manifestations [3,42], participants’ inability to pick them out items suggests that they would likely fail to identify OPD patients manifesting them but not having other indicators obvious to most HPs. In that case, some patients with OPD may go unidentified. This observation draws support from past research that has raised concerns over frequent instances of OPD under-diagnoses, misdiagnoses, and/or over-diagnoses, partly due to inadequate awareness levels on the part of HPs tasked with screening patients for the condition [6,27].
On average, each participant responded to 73% of the questions correctly, suggesting moderate signs/symptoms awareness levels. Over half of the participants had either low or moderate OPD signs/symptoms awareness levels. Only 44% had high awareness (Figure 1). These results are comparable to those of a similar study conducted in Iran, which reported that on average, Iranian physician identified 70.3% of dysphagia signs/symptoms correctly [27]. Another study in Nepal found that about 60% of nurses in a university hospital in the country had only moderate knowledge of dysphagia signs and symptoms [41]. In South Africa, Knight et al. [22] established an average OPD signs/symptoms awareness of only 67%.
Such findings suggest that in many countries worldwide, HPs have, on average, only moderate OPD signs/symptoms awareness. Low or moderate symptoms/signs awareness may lead to wrong diagnoses and delayed or missed referrals, which, in turn, could increase the risks of complications, hospital stays, and treatment costs [43]. There is a need for the hospital’s management to implement interventions for increasing OPD signs/symptoms awareness levels among HPs in the hospital’s surgical and medical wards.
Age, educational attainment, and specialization influenced HPs’ awareness of OPD signs and symptoms (Table 5). There was no consistency in differences in awareness levels due to age. The levels increased from the youngest to the middle group and then declined for the oldest category. However, there was a clear trend in the influence of education. Professionals with a post-graduate degree had the highest OPD signs/symptoms awareness. This finding highlights the importance of post-graduate qualifications in OPD management. According to Holloway et al. [44], post-graduate education increases HPs’ ability to understand and apply specialty-related evidence. This increased understanding may explain the high awareness levels observed among post-graduates.
Much of the differences in signs/symptoms awareness levels due to specialties may be attributed to the degrees of contact with OPD patients. According to Hady et al. [38], practitioners who interact frequently with OPD patients are likely to have high awareness of this disorder. Although all HP categories in the present study analysis should be involved in OPD management, SLTs are the ones who interact with dysphagia patients the most. If Hady et al.’s observation holds, speech therapists should have the highest awareness levels. Consistent with this prediction, individual records (not shown in the above analysis) showed that the SLT matched all OPD signs and symptoms correctly. Hence, high interactions with OPD patients may translate to high awareness. Nevertheless, this finding should be interpreted cautiously, given the low representation of speech therapist in the sample (the only SLT employed on contract), a factor that likely introduced bias.
Past research indicates that years of experience and training predict HPs’ knowledge, awareness, and participation in OPD management [40,41]. However, for this sample, none of these factors influenced signs/symptoms awareness levels significantly. While it was beyond the study’s scope to explore the reasons for these inconsistencies, they may have been introduced by biases emerging from the relatively small sample size. Alternatively, the non-significant effect of training may indicate that existing training programs in the hospital were not sufficiently effective to influence OPD awareness. There is a need for additional research to establish the source of the observed inconsistencies.
LIMITATIONS
A major limitation of the study was its relatively small sample size which was maximized by using purposive sampling to select only the participants with required information for data analysis to fulfill the objectives of the study. Besides, the study was descriptive and did not control for other factors that could influence OPD awareness. Either of these factors could have introduced biases in the results.
CONCLUSION
This study assessed the level of awareness of OPD signs and symptoms among HPs attending to adult inpatients in the ACF (surgical and medical wards) of a level-six hospital in Kenya. Analyses of questionnaire responses showed that HPs in the facility have, on average, moderate awareness of OPD signs and symptoms. Mean comparisons across different participant categories indicated that, on average signs/symptoms awareness scores increased with educational attainment. The highest and lowest awareness levels were reported among post-graduates and diploma certificate holders, respectively. Thus, it may be concluded that high educational attainment is associated with increased awareness of OPD signs/symptoms.
RECOMMENDATION
To improve the clients autonomy and quality of life, the hospital’s management should implement regular training programs focusing on various OPD management aspects, particularly its signs and symptoms. Although such training should target all HPs in the hospital’s ACF, priority should be given to nurses and physiotherapists, as well as HPs without a post-graduate degree. These categories had significantly lower awareness levels than HPs in other groups.
ACKNOWLEDGEMENT
The authors are grateful to God through the health professionals who took part in the study, for their valuable inputs.
REFERENCES
- Takizawa, C., Gemmell, E., Kenworthy, J., & Speyer, R. (2016). A systematic review of the prevalence of oropharyngeal dysphagia in stroke, Parkinson’s disease, Alzheimer’s disease, head injury, and Dysphagia, 31(3), 434-441. https://doi.org/10.1007/s00455-016-9695-9
- Nishino T. (2013). The swallowing reflex and its significance as an airway defensive reflex. Frontiers in Physiology, 3(489), 1- https://doi.org/10.3389/fphys.2012.00489
- Cook, J. (2009). Oropharyngeal Dysphagia. Gastroenterology Clinics, 38(3), 411-431.
- Azer, S. A., Kanugula, A. K., & Kshirsagar, R. K. (2023). Dysphagia. In StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK559174/
- Wolf, C. D. (1990). Dysphagia. In K., Walker, W. D. Hall, & J. W. Hurst (eds.), Clinical methods: The history, physical, and laboratory examinations (3rd ed.). Butterworths. https://www.ncbi.nlm.nih.gov/books/NBK408/
- Rajati, , Ahmadi, N., Naghibzadeh, Z. A., & Kazeminia, M. (2022). The global prevalence of oropharyngeal dysphagia in different populations: A systematic review and meta-analysis. Journal of Translational Medicine, 20(1), 175-189. https://doi.org/10.1186/s12967-022-03380-0.
- Omondi, G. (2017). A quality audit on the management of acute ischaemic stroke at Kenyatta National Hospital (unpublished thesis). University of Nairobi. http://erepository.uonbi.ac.ke/handle/11295/154214
- Bolinger, C., & Dembowski, J. (2022). Speech language pathology consultations and medical outcomes for patients with aspiration pneumonia. Journal of Medical and Health Studies, 3(3), 45- https://doi.org/10.32996/jmhs.2022.3.3.8.
- Adkins, C., Takakura, W., Spiegel, B. M. R., Lu, M., Vera-Llonch, M., Williams, J., & Almario, C. V. (2020). Prevalence and characteristics of dysphagia based on a population-based survey. Clinical Gastroenterology and Hepatology, 18(9), 1970-9, https://doi.org/10.1016/j.cgh.2019.10.029
- Altman, K. W., Yu, G. P, Schaefer, S. D. (2010). Consequence of dysphagia in the hospitalized patient: impact on prognosis and hospital resources. Archives of Otolaryngology: Head Neck Surgery, 136(8),784–9.
- Bonilha, H. S., (2014). The one-year attributable cost of post-stroke dysphagia. Dysphagia; 29(5), 545–52.
- Hinchey, J. , Shephard, T., Furie, K., Smith, D., Wang, D., & Tonn, S. (2005). Formal dysphagia screening protocols prevent pneumonia. Stroke, 36(9), 1972-1976.
- Cichero, A., Heaton, S., & Bassett, L. (2009). Triaging dysphagia: Nurse screening for dysphagia in an acute hospital. Journal of Clinical Nursing, 18(11), 1649-1659. https://doi.org/10.1111/j.1365-2702.2009.02797.x
- Jacobsson, , Axelsson, K., Österlind, P. O., & Norberg, (2000). How people with stroke and healthy older people experience the eating process. Journal of Clinical Nursing, 9(2), 255-264. https://doi.org/10.1046/j.1365- 2702.2000.00355.x
- Rosenvinge, S. K., & Starke, I. D. (2005). Improving care for patients with dysphagia. Age and Ageing, 34(6), 587-593. https://doi.org/10.1093/ageing/afi187
- Meng, N. H., Wang, T. G., & Lien, I. N. (2000). Dysphagia in patients with brainstem stroke: Incidence and outcome. American Journal Of Physical Medicine & Rehabilitation, 79(2), 170–175. https://doi.org/10.1097/00002060-200003000-00010
- Rivelsrud, M. C., Hartelius, L., Bergström, L., Løvstad, M., & Speyer, R. (2023). Prevalence of oropharyngeal dysphagia in adults in different healthcare settings: A systematic review and meta-analyses. Dysphagia, 38(1), 76–121. https://doi.org/10.1007/s00455-022-10465-x
- World Health Organization. (2010). Framework for action on interprofessional education and collaborative practice. https://interprofessional.global/wp- content/uploads/2019/11/WHO-2010-Framework-for- Action-on-Interprofessional-Education-and-Collaborative- Practice.pdf
- Johnson, Alex. (2016). Interprofessional Education and Interprofessional Practice in Communication Sciences and Disorders: An Introduction and Case Based Examples.
- Reeves, S., Pelone, F., Harrison, R., Goldman, J., & Zwarenstein, M. (2017). Interprofessional collaboration to improve professional practice and healthcare outcomes. The Cochrane Database of Systematic Reviews, 6(6), https://doi.org/10.1002/14651858.CD000072.pub3
- Bakhtiyari, J., Ghorbani, R., Salmani, M., Asadi, M., Irani, S., & Esmaee, A. R. (2019). Physicians’ perspective on a multidisciplinary approach to dysphagia management. Iranian Journal of Otorhinolaryngoly, 31(104), 141-146.
- Dondorf, K., Fabus, R., & Ghassemi, A. K. (2015). The interprofessional collaboration between nurses and speech-language pathologists working with patients diagnosed with dysphagia in skilled nursing facilities. Journal of Nursing Education and Practice, 6(4), 17-20. http://dx.doi.org/10.5430/jnep.v6n4p17
- Knight, K., Pillay, B., Van der Linde, J., & Krüger, E. (2020). Nurses’ knowledge of stroke-related oropharyngeal dysphagia in the Eastern Cape, South Africa. The South African Journal of Communication Disorders, 67(1), e1–e7. https://doi.org/10.4102/sajcd.v67i1.703
- Sánchez-Sánchez, E., Avellaneda-López, Y., García- Marín, E., Ramírez-Vargas, G., Díaz-Jimenez, J., & Ordonez, F. J. (2021). Knowledge and practice of health professionals in the management of dysphagia. International Journal of Environmental Research and Public Health, 18(4), 2139-49. https://doi.org/10.3390%2Fijerph18042139
- Obembe, A., Adebayo, A. M., Ojo, O. T., & Adebayo, I. (2017). Awareness and utilization of outpatient services among residents of Odno West local government area, Ondo State, Nigeria. Annals of African Medicine, 16(1), 10-16.
- Khan, M. A., Moazzam, M., Shehzad, A. (2021). Assessment of awareness among speech and language pathology regarding dysphagia. Journal of Allied Health Sciences, 6(2), 3-8.
- Kaylor, S.A., & Singh, S.A. (2023). Clinical outcomes associated with speech, language and swallowing difficulties post-stroke. South African Journal of Communication Disorders, 70(1), a957. https://doi. org/10.4102/sajcd.v70i1.957
- Martino R., Foley, N., & Bhogal, S. (2005). Dysphagia after stoke: incidence, diagnosis, and pulmonary complications. Stroke. 36 (12): 2756-63.
- Oduor, O., Keter, A., Diero, L. O., Siika, A. M., Williams, L. S. (2015). Stroke types, risk factors, quality of care and outcomes at a referral hospital in Western Kenya. East Africa Medical Journal; 92 (7): 324 – 32.
- Ndiema, D. C., Abuom, T., & Karia, M. (2023). A descriptive retrospective review on the epidemiology of oropharyngeal dysphagia in the acute-care facility of a Kenyan (level-six) national hospital. IOSR Journal of Nursing and Health Science, 12(6), 20-28. https://doi.org/10.9790/1959-1206062028
- Mugenda, A., & Mugenda, O. (2013). Research methods: Quantitative and qualitative approaches. ACTS Press.
- Rhoda, A., & Pickel-Voight, A. (2015). Knowledge of nurses regarding dysphagia in patients post stroke in Curationis, 38(2), 1564-71. https://doi:10.4102/curationis.v38i2.1564
- Yong, X., Affizal, A., & Malarvini V. (2018). Medical officers’ awareness, involvement, and training in dysphagia management. Journal Sains Kesihatan Malaysia, 16 (1), 7-
- Jalal B., Raheb G. Masoomeh S., Mozhgan A. & Sadaf R. (2019). Physicians’ perspective on a multidisciplinary approach to dysphagia management. Iranian Journal of Otorhinolaryngology, 31(104), 141-146.
- Robbertse, A., & De Beer, A. (2020). Perceived barriers to compliance with speech-language therapist dysphagia recommendations of South African nurses. The South African journal of communication disorders = Die Suid- Afrikaanse tydskrif vir Kommunikasieafwykings, 67(1), e1– e6. https://doi.org/10.4102/sajcd.v67i1.686
- Grossmeier, J., Castle, P. H., Pitts, J. S., Saringer, C., Jenkins, K. R., Imboden, M. T., Mangen, D. J., Johnson, S. S., Noeldner, S. P., & Mason, T. (2020). Workplace well-being factors that predict employee participation, health and medical cost impact, and perceived support. American Journal of Health Promotion, 34(4), 349-358. https://doi.org/10.1177/0890117119898613
- Ary, D., Jacobs,L. , & Sorensen, C. K. & Walker, A. (2014). Introduction to research in education. Wadsworth Cengage Learning.
- Hady, A. F., Farag, H. M., & Sheikhany, A. R. (2023). The awareness and knowledge of dysphagia among health care practitioners in Egypt. Egyptian Journal of Otolaryngology, 39(25), 1-18. https://doi.org/10.1186/s43163-023-00387-2
- Sivertsen, J., Graverholt, B., & Espehaug, B. (2017). Dysphagia screening after acute stroke: A quality improvement project using criteria-based clinical BMC Nursing, 16(1), 1-8. https://doi.org/10.1186/s12912-017-0222-6
- Andrea P. (2014). Knowledge of nurses regarding dysphagia in patients with stroke (master’s thesis). University of the Western Cape, Namibia.
- Nepal G. M. & Sherpa M. D. (2019). Knowledge of dysphagia in stroke among nurses working in tertiary care hospital. Kathmandu University of Medicine.
- Wakabayashi, H., Kishima, M., Itoda, M., Fujishima, I., Kunieda, K., Ohno, T., Shigematsu, T., Oshima, F., Mori, T., Ogawa, , Nishioka, S., Momosaki, R., Yamada, M., & Ogawa, S. (2022). Prevalence of hoarseness and its association with severity of dysphagia in patients with sarcopenic dysphagia. The Journal of Nutrition, Health & Aging, 26(3), 266–271. https://doi.org/10.1007/s12603-022-1754-3
- Anderle, , Rech, R. S., Pasqualeto, V. M., & de Goulart, N. (2018). Knowledge of the medical and nursing teams about the management of oral medications in hospitalized adult dysphagic patients. Audiology: Communication Research, 23(1), e1933 http://dx.doi.org/10.1590/2317- 6431-2017-1933
- Holloway, S., Taylor, A., & Tombs, M. (2020). Impact of postgraduate study on healthcare professionals’ academic and clinical practice. British Journal of Healthcare Management, 26(7), 171- http://dx.doi.org/10.12968/bjhc.2019.005