
Knowledge, Attitudes and Practice Regarding Cervical Cancer and Screening among Women Visiting Selected Primary Health Centres in Ogbomosho, Nigeria
- Solomon Exousia Akintobi
- Olabisi, Elisha Oluwatobi
- Oyediran Thomas
- Oluwarotimi Florence Oluwasolabomi
- Akangbe Mariam Temitayo
- Adeagbo Ayobami. O
- Fawole Israel Opeyemi
- 392-407
- May 9, 2024
- Health
Knowledge, Attitudes and Practice Regarding Cervical Cancer and Screening among Women Visiting Selected Primary Health Centres in Ogbomosho, Nigeria
Solomon Exousia Akintobi; Olabisi, Elisha Oluwatobi; Oyediran Thomas; Oluwarotimi Florence Oluwasolabomi; Akangbe Mariam Temitayo; Adeagbo Ayobami. O; Fawole Israel Opeyemi
Ladoke Akintola University of Technology
DOI: https://doi.org/10.51244/IJRSI.2024.1104029
Received: 29 March 2024; Accepted: 04 April 2024; Published: 09 May 2024
ABSTRACT
Cervical cancer is one of the most preventable cancers in the world and its` prognosis is better when detected early through cervical cancer screening. The study examined the knowledge, attitudes and practice regarding cervical cancer and screening among women visiting selected primary health centres (PHCs) in Ogbomosho. The study was conducted in May 2021, employing a descriptive cross-sectional design. A sample size of 124 respondents was determined using the Taro-Yamane formula and selected through convenience sampling technique. Data collection utilised a validated questionnaire, with analysis performed using descriptive statistics encompassing frequencies and percentages. Relationships between variables were tested using chi-square at a 0.05 significance level. Findings suggest that more than half (55%) had good knowledge of cervical and cervical cancer screening. The majority (70%) had a good attitude towards cervical cancer and cervical cancer screening. Less than one-third (21%) have had cervical cancer screening done before. Self-reported barriers limiting the practice of cervical cancer screening identified include lack of health education on cervical cancer screening (45.5%), lack of knowledge on the screenings (39.3%), absence of signs and symptoms of cervical cancer (39.3%), low socioeconomic status (29.5%), cost of the procedure (17.9%), unavailability of services (17.9%) and religious beliefs (14.3%). Chi-square analysis showed a statistically significant relationship between the educational status of respondents and their knowledge of cervical cancer screening, likewise, a significant relationship exists between the knowledge of respondents and the practice of cervical cancer screening at P< .05. Conclusively, the study has revealed the practice of cervical cancer screening was found to be low, indicating a disparity between knowledge/attitude and actual screening behaviour, although, knowledge was a key predictor of their screening practices. The way forward is to improve the knowledge of women on cervical cancer and screening via health education while efforts are being put in place to make cervical cancer screening services available at affordable cost.
INTRODUCTION
Cervical cancer is the fourth most frequent cancer among women worldwide with an estimated 570,000 new cases in 2018 representing 6.6% of all female cancers and the commonest in developing countries especially in Central America and Sub-Sahara Africa (World Health Organization (WHO), 2018). Cervical cancer is the second most common cancer in Nigerian women and the leading gynaecological malignancy with high mortality among the afflicted (Oluwole et al., 2017). According to WHO (2019), the disease progresses over many years, with an estimated 1.4 million women worldwide living with cervical cancer, and up to 7 million worldwide may have precancerous conditions that need to be identified and treated. Approximately, 90% of deaths from cervical cancer occurred in low- and middle-income countries (WHO, 2019). The high mortality rate from cervical cancer globally could be reduced through a comprehensive approach that includes prevention, early diagnosis, effective screening and treatment programmes (Sowemimo et al., 2017). The disease, which affects the poorest and most vulnerable women, sends a ripple effect through families and communities that rely heavily on women’s roles as providers and caregivers (Sowemimo et al.,2017).
According to Ajibola et al. (2016), cervical cancer is one of the most preventable human cancers because of its slow progression, cytological identifiable precursors, and effective treatments if detected early, but unfortunately, most screening activities in developing countries do not reach the vulnerable women and consequently, a high proportion of cervical cancer cases are diagnosed at an advanced stage. The uptake of cervical cancer screening has remained very low in Nigeria while the mortality and morbidity associated with cervical cancer have remained high (Sowemimo et al., 2017). Despite efforts from governmental and non-governmental organizations to improve access to cervical cancer screening services in Nigeria, uptake has been appalling. Several studies have documented factors associated with the uptake of cervical screening tests worldwide (Butho et al., 2015; Ajibola et. al., 2016). Such factors include the age of the women, their marital status, parity, risk perception, financial constraint, and knowing someone who has cancer of the cervix (Butho et al., 2015).
The association of cervical cancer and HPV infection implies that cervical cancer can be prevented by HPV vaccination. Consequently, HPV vaccines have been developed (Hussain et al., 2016). While all these developments in the prevention and screening of cervical cancer are taking place, the benefits must be utilized by all women including those living in developing countries. Having good knowledge and awareness will help ensure that the disease burden does not increase (Akinfolarin et al., 2017). The prognosis can be improved if screening is embraced and widely employed. For this, the healthcare workers must be educated and well aware so that they can influence the beliefs and actions of the general public. Many studies have been conducted in other developing countries to gauge the knowledge and awareness about cervical cancer and to study the extent of utilization of the screening methods (Hussain., et al., 2016; Jassim et al., 2018). The knowledge assessment of cervical cancer screening and the HPV vaccine emerges as a crucial determinant for the acceptance and utilization of cervical cancer screening, given the considerable impact of cervical screening, its low coverage, the absence of a population-based screening program, and the exclusion of the HPV vaccine from the national vaccination schedule (Hussain et al., 2016; Akinfolarin et al., 2017).
Cervical cancer awareness is generally low worldwide but worse in developing countries despite the increased prevalence of the disease in these countries (Catarino et al., 2015). A previous population-based study conducted in Nigeria revealed that women exhibited a fair knowledge of cervical cancer and cervical cancer screening (43.5%) (Ahmed et al., 2013). Despite the societal expectation that mothers serve as the backbone of both the family and society, possessing crucial information and knowledge about various health-related issues, and acting as role models for their children in accessing preventive services, studies have shown a different reality. In a study by Ajah et al (2015), it was reported that 78% of the women were aware of cervical cancer screening while only 15% had had the screening done before. Also, in another similar study by Adekanle et al. (2011), it was revealed that only 5.4% of the 407 respondents had cervical screening done at the time of the study.
Previous studies have revealed a low level of practice of cervical cancer screening of which their knowledge and attitude towards cervical cancer and cervical cancer screening were the determinants (Adekanle et al., 2011; Ajah et al., 2015). However, there is a paucity of recent studies in the study area. This makes it a necessity to conduct this study to investigate the knowledge, attitude and practice regarding cervical cancer screening among women in Ogbomoso. The study would help in developing problem and location-specific interventions and policies towards promoting the uptake of cervical cancer screening.
RESEARCH METHODOLOGY
Research Design
This study design is a descriptive cross-sectional design which assessed knowledge, attitudes and practice regarding cervical cancer and screening among women visiting selected primary health centres in Ogbomosho. The study was conducted in May 2021.
Research Settings
This study was conducted in Katangua Primary Health Centre (PHC) and Adeniran Primary Health Centre which are located in Katangua and Adeniran in Ogbomoso North Local government respectively. Katangua Primary Health Centre was established in 2005 under the regime of Senator Rashidi Adewolu, Ladoja as the then governor of Oyo state. The PHC had a major improvement in terms of infrastructure in the year 2013 under the regime of Senator Isiaka Abiola Ajimobi as the governor of Oyo state. Adeniran Primary Health Centre was established recently in 2018 still under the regime of Senator Isiaka Abiola Ajimobi as the governor of Oyo state. The two PHCs encompass several units, notably the Maternal and Child Health Unit, the Outpatient Department (OPD), and the Medical Laboratory Science Unit. The primary operations predominantly revolve around maternal and child health services, encompassing antenatal care, childbirth, and family planning, among others. Pregnant women typically attend antenatal visits on Tuesdays, immunization sessions on Mondays, family planning consultations on Wednesdays, and elderly care on Fridays. Additionally, the healthcare facility addresses various other illnesses and diseases within the scope of primary healthcare practices.
Target Population
The research population are women attending Katangua Primary Health Centre (PHC) and Adeniran Primary Health Centre in Ogbomosho, Oyo state at the time of data collection
Inclusion criteria: Adult women of 18 years and above were included in the study
Exclusion criteria: All who were unwilling to participate in the study were excluded
Sampling Technique
The sampling technique employed in this study is convenience sampling, where participants are chosen based on their easy availability and willingness to participate rather than through random selection.
Sample Size Determination
The minimum sample size was determined using the Taro Yamane formula for each study setting. The estimated average monthly total population, based on attendance recorded in the registers three months prior, is 130 collectively across the two PHCs.
n=N/1+N (e)2
Where n=desired sample size.
N=total population=130
1=constant
e=level of precision=0.05
n=130/1+130(0.05)2
n=130/1.325
n= 108
Considering a 15% attrition rate for the sake of non-response or poorly filled questionnaires.
n=124.
Instruments for Data Collection
A structured, pretested self-developed questionnaire was used to gather information about knowledge, attitudes and practices regarding cervical cancer and screening among women visiting selected primary health centres in Ogbomosho.
Scoring: Correct responses to the knowledge-based questions were scored as 1 and incorrect as 0. Respondents with scores greater than or equal to the mean knowledge scores were adjudged to have good knowledge of cervical cancer and cervical cancer screening, otherwise, poor knowledge. The attitude of the respondents towards cervical cancer and cervical cancer screening was on a Likert scale of strongly agreed-5, agreed- 4, undecided-3, disagreed -2, strongly disagreed- 1 for every positive statement, and reverse coded for negative statements. Respondents with scores greater than or equal to the mean total attitude scores were adjudged to have good attitude, otherwise, poor attitude. Furthermore, the practice of cervical cancer screening was based mainly on a “yes or no” question of whether they have undergone any cervical cancer screening in the past.
Psychometric Properties of the Instrument
Validity of Instrument
The questionnaire was subjected to face and content validity. The instrument was constructed following a review of previous works of literature; each section of the instrument was matched with the predetermined objectives. Face and content validity was carried out by the researchers and an expert in public health research. The study supervisor reviewed the content of the instrument ensuring its adequacy to generate data to meet up with the target objectives. Her suggestions and comments received were used to modify the final draft of the instrument before it was finally administered.
Reliability of Instrument
The self-structured KAP questionnaire was subjected to a pilot study at Ikoyi Primary Health Centre in Ogbomosho and was conducted among 10% of the sample population (12 respondents); these respondents were not part of the main study. The data collected was analysed, and the reliability coefficient was computed which yielded a Cronbach alpha value of 0.8 depicting a true reliability index.
Method of Data Collection
Validated instruments were given to the respondents to fill on the site and retrieved back after filled. The respondents were properly guided on how to fill out the questionnaire. Data collected were kept in a secure place for proper data management and analysis.
Method of Data Analysis
The data was analysed through descriptive statistics (mean, standard deviations, and frequencies) and inferential statistical measures such as Chi-square to establish the relationship between variables. The data was presented using frequency tables and charts. Variables were considered statistically significant at P<0.05. Data was entered using Microsoft Excel version 2016 and exported to IBM Statistical Package for Social Sciences (SPSS package) 25th edition for analysis.
Ethical Consideration
Ethical approval was granted by the Ogbomosho North Local Government ethical review committee. A letter of introduction was obtained from the Faculty of Nursing Science, Ladoke Akintola University of Technology, Ogbomosho and submitted alongside the study proposal to the ethical board of the local government authorities for approval. Verbal permissions were also sought from the community health officers of the settings who gave their consent for the collection of data. Also, verbal and written informed consent was obtained from the respondents having explained the aim and goals of the research to them. The selected respondents were informed about the questionnaire and assured of confidentiality and non-maleficence. They were also made to know they had the right to pull out of the study if at any time they needed to do so.
ANALYSIS AND PRESENTATION OF DATA
A total of 124 respondents were recruited but 112 respondents completed the questionnaires and had adequate data for analysis. This translates to a response rate of 90.3%.
Table 1 Sociodemographic Characteristics of Respondents (n=112)
| Variables | Categories | n(%) |
| Age | < 25 years | 29(25.9) |
| 26-35 | 56(50.0) | |
| 36-45 | 21(18.8) | |
| > 46 years | 6(5.4) | |
| Education status | No formal education | 7(6.3) |
| Primary | 26(23.2) | |
| Secondary | 59(52.7) | |
| Tertiary | 20(17.9) | |
| Religion | Islam | 28(25.0) |
| Christianity | 79(70.5) | |
| Traditional | 5(4.5) | |
| Ethnicity | Yoruba | 84(75.0) |
| Hausa | 23(20.5) | |
| Igbo | 5(4.5) | |
| Marital status | Single | 42(37.5) |
| Married | 64(57.1) | |
| Divorced | 3(2.7) | |
| Widowed | 3(2.7) | |
| Occupation | Employed | 35(31.3) |
| Self-employed | 62(55.4) | |
| Full housewife | 15(13.4) |
Source: (Field Survey, 2021)
From Table 1 above, half 56(50%) of the respondents were between the ages 26-35 years, as regards their level of education, more than half 59(52.7%) had secondary education and 20(17.9%) had tertiary education; about their religion, majority 79(70.5%) were Christians; the three ethnic groups were represented with majority 84(75%) being Yoruba. The majority 64(57.1%) were married. More than half 62(55.4%) were self-employed
Table 4.2: Knowledge of Cervical Cancer and Cervical Cancer Screening
| Variables | Responses (n=112) | |
| Yes n(%) | No n(%) | |
| Have you heard of cervical cancer | 89(79.5) | 23(20.5) |
| Excess alcohol intake can lead to cervical cancer | 44(39.3) | 68(60.7) |
| Human papillomavirus infection can cause cervical cancer | 51(45.5) | 61(54.5) |
| Having multiple sexual partners predisposes one to cervical cancer | 79(70.5) | 33(29.5) |
| Early exposure to sex is one of the causes of cervical cancer | 82(73.2) | 30(26.8) |
| Cervical cancer can manifest as abnormal vaginal bleeding | 86(76.8) | 26(23.2) |
| Foul-smelling discharge from the vagina is one of the symptoms of cervical cancer | 83(74.1) | 29(25.9) |
| Cervical cancer can also present as post-coital bleeding | 68(60.7) | 44(39.3) |
| Cervical cancer can be prevented by immunization | 62(55.4) | 50(44.6) |
| Awareness of cervical cancer screening | 70(62.5) | 42(37.5) |
| Early detection of cervical cancer helps in the treatment | 89(79.5) | 23(20.5) |
| Human papillomavirus (HPV) testing is one of the screening techniques for cervical cancer | 70(62.5) | 42(37.5) |
| Pap smear is done to screen for cervical cancer | 70(62.5) | 42(37.5) |
| Visual inspection with acetic acid (VIA) is part of cervical cancer screening methods. | 47(42) | 64(58) |
From Table 2 above on the knowledge of respondents on cervical cancer and cervical cancer screening, majority 89(79.5%) have heard of cervical cancer before, more than one-third 44(39.3%) knew that excess alcohol intake can lead to cervical cancer, about half 51(45.5%) knew that human papillomavirus infection can cause cervical cancer, majority 79(70.5%) knew that having multiple sexual partners predisposes one to cervical cancer, majority 82(73.2%) knew that early exposure to sex is one of the causes of cervical cancer, majority 86(76.8%) were of the opinion that cervical cancer can manifest as abnormal vaginal bleeding, majority 83(74.1%) knew that foul smelling discharge from the vagina is one of the symptoms of cervical cancer, majority 68(60.7%) knew that cervical cancer can present as post coital bleeding, more than half 62(55.4%) knew that cervical cancer can be prevented by immunization, majority 70(62.5%) were aware of cervical cancer screening, majority 89(79.5%) knew that early detection of cervical cancer helps in the treatment, more than half 62(55.4%) knew that Human papillomavirus (HPV) testing is one of the screening techniques for cervical cancer, more than half 62(55.4%) knew that pap smear is done to screen for cervical cancer, more than one-third 47(42%) knew that visual inspection with acetic acid (VIA) is part of cervical cancer screening methods.

Fig 1: Source of Health Information on Cervical Cancer and Cervical Cancer Screening.
From Fig 1 above, out of the proportion that have heard of cervical cancer, sources of health information on cervical cancer were health workers 40(50.6%), colleague 23(29.1%), media 8(10.1%), school 6(7.6%) and family 2(1.8%). Likewise, sources of health information on cervical cancer screening were health workers 37(52.9%), media 14(20%), colleagues 11(15.7%), family 4(5.7%) and school 4(5.7%).
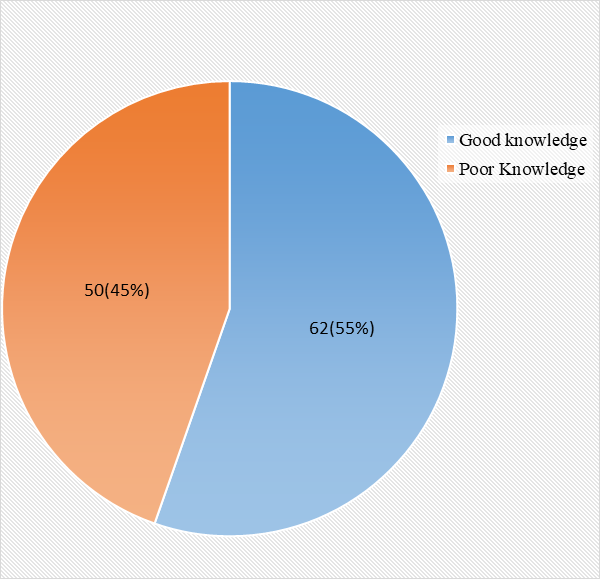
Fig 2: Overall Knowledge of Respondents on Cervical Cancer and Cervical Cancer Screening
From Fig 2 above, more than half 62(55%) of the respondents had good knowledge of cervical cancer and its` screening while 50(45%) had poor knowledge of cervical cancer and cervical cancer screening.
Table 3: Attitude towards Cervical Cancer and Cervical Cancer Screening
| Variables | Strongly agreed n(%) | Agreed n(%) | Undecided n(%) | Disagreed n(%) | Strongly disagreed n(%) |
| Cervical cancer is preventable | 61(54.5) | 25(22.3) | 3(2.7) | 9(8.0) | 14(12.5) |
| I would prefer to not give birth to more than 4 children to reduce my risk of cervical cancer | 54(48.2) | 30(26.8) | 5(4.5) | 9(8.0) | 14(12.5) |
| Intermenstrual bleeding should be considered normal | 14(12.5) | 9(8.0) | 3(2.7) | 30(26.8) | 56(50) |
| I will keep a distance from a neighbourhood female suffering from cervical cancer | 15(13.4) | 8(7.1) | 7(6.3) | 25(22.3) | 57(50.9) |
| I am willing to be screened for cervical cancer if screening services are made available. | 64(57.1) | 22(19.6) | 3(2.7) | 7(6.3) | 16(14.3) |
| I am willing to have Human papillomavirus immunization or recommend it to others to prevent cervical cancer. | 58(51.8) | 25(22.3) | 4(3.6) | 9(8.0) | 16(14.3) |
| Total n(%) | 112(100) | ||||
From Table 3 above, majority 61(54.5%) strongly agreed, 25(22.3%) agreed that cervical cancer is preventable, majority 54(48.2%) strongly agreed, 3(26.8%) agreed that they would prefer to not give birth to more than 4 children to reduce their risk of cervical cancer, majority 30(26.8%) disagreed, 56(50%) strongly disagreed that intermenstrual bleeding should be considered as normal, majority 25(22.3%) disagreed, 57(50.9%) strongly disagreed that they will keep a distance from a neighbourhood female suffering from cervical cancer; majority 64(57.1%) strongly agreed, 22(19.6%) agreed that they are willing to be screened for cervical cancer if screening services are made available, majority 58(51.8%) strongly agreed, 25(22.3%) agreed that they are willing to have Human Papilloma Virus immunization or recommend it to others to prevent cervical cancer.

Fig 3: Attitude of Respondents towards Cervical Cancer and Cervical Cancer Screening
From Fig 3 above, the majority 78(70%) had a good attitude towards cervical cancer and cervical cancer screening while the remaining 34(30%) had a poor attitude.
Table 4: Practice of Cervical Cancer Screening among the Respondent (n=112)
| Variables | Categories | n(%) |
| Ever had cervical cancer screening done | Yes | 24(21.4) |
| No | 88(78.6) | |
| Where the screening was done | Government hospital | 19(79.2) |
| (n=24) | Private hospital | 5(20.8) |
| Pap smear Papanicolaou being a screening method used (n=24) | Yes | 22(91.7) |
| No | 2(8.3) | |
| Visual inspection with acetic acid being a screening method (n=24) | Yes | 14(58.3) |
| No | 10(41.7) | |
| HPV DNA testing being a screening method(n=24) | Yes | 14(58.3) |
| No | 10(41.7) | |
| Reasons for screening | Prescribed | 11(45.8) |
| (n=24) | Voluntary | 13(54.2) |
| Last time screening was done | This year | 3(12.5) |
| (n=24) | Last year | 10(41.7) |
| 2 years ago | 5(20.8) | |
| 3 years ago | 6(25.0) |
From Table 4 above on the practice of cervical cancer screening, 24(21.4%) had ever been screened for cervical cancer in the past, out of this proportion, the majority 19(79.2%) had the screening done at a government hospital while 5(20.8%) had it done at a private hospital, the screening methods used were Pap smear Papanicolaou 22(91.7%), visual inspection with acetic acid 14(58.3%) and HPV DNA testing 14(58.3%). About half 11(45.8%) of the proportion that have had cervical cancer screening did it based on a doctor`s prescription while more than half 13(54.2%) did it voluntarily, more than one-third 10(41.7%) of the proportion have had cervical screening done before had it done last year, 5(20.8%) had it done 2 years ago, and 6(25%) had it 3 years ago.
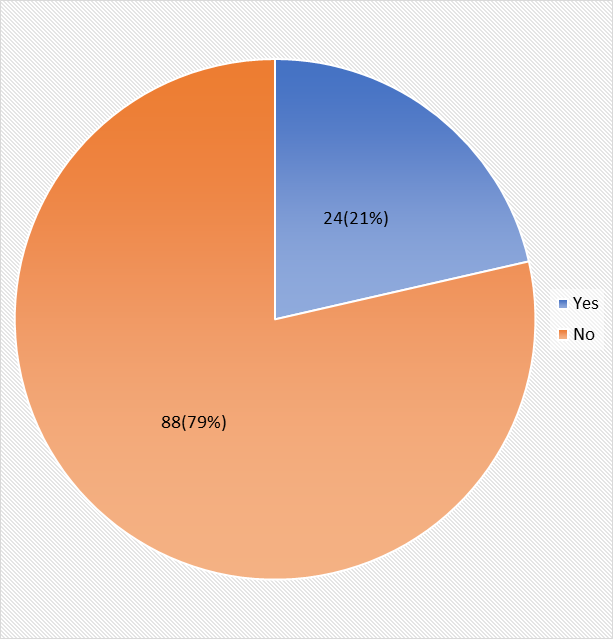
Fig 4: Practice of Cervical Cancer Screening among the Respondent
From Fig 4 above on the practice of cervical cancer screening, 24(21%) have had cervical cancer screening before while 88(79%) have not had it done before.
Table 5: Barriers to the Practice of Cervical Cancer Screening among the Respondents
| Variables | Responses (n=112) | |
| Yes n(%) | No n(%) | |
| Lack of knowledge on cervical cancer screening | 44(39.3) | 68(60.7) |
| Lack of health education or health sensitization on cervical cancer screening. | 51(45.5) | 61(54.5) |
| Absence of signs and symptoms that look like cervical cancer | 44(39.3) | 68(60.7) |
| Low socioeconomic status | 33(29.5) | 79(70.5) |
| Cost of Procedure | 20(17.9) | 92(82.1) |
| Service is unavailable at times | 20(17.9) | 92(82.1) |
| Religious beliefs | 16(14.3) | 96(85.7) |
From Table 5 above on the barriers to the practice of cervical cancer screening among the respondents, the self-reported barriers identified include lack of health education or health sensitization on cervical cancer screening.51(45.5%), lack of knowledge on the screenings 44(39.3%), absence of signs and symptoms of cervical cancer 44(39.3%), low socioeconomic status 33(29.5%), cost of procedure 20(17.9%), unavailability of services 20(17.9%) and religious beliefs 16(14.3%).
Hypothesis Testing
Hypothesis One
Ho – There is no significant relationship between the educational status of respondents and their knowledge of cervical cancer screening.
Table 6: Relationship Educational Status of Respondents and their Knowledge of Cervical Cancer Screening.
| Variables | Knowledge of Cervical Cancer and Cervical Cancer Screening | x2 | df | P | ||
| Good knowledge | Poor Knowledge | |||||
| Educational status | No formal education | 0(0%) | 7(100%) | 55.296 | 3 | 0.000 |
| Primary | 1(3.8%) | 25(96.2%) | ||||
| Secondary | 42(71.2% | 17(28.8%) | ||||
| Tertiary | 19(95%) | 1(5%) | ||||
| Total | 62(55.4%) | 50(44.6%) | ||||
x2=Pearson chi-square value, df=degree of freedom, P =Probability value
Inference: From Table 6 above, the null hypothesis is rejected, therefore, there is a significant relationship between the educational status of respondents and their knowledge of cervical cancer screening (x2=55.296, P=.000) at P< .05.
There exists a positive association between the educational status of respondents and their knowledge of cervical cancer and its` screening as their level of knowledge increases with increasing level of education.
Hypothesis Two
Ho – There is no significant relationship between the knowledge of respondents on cervical cancer screening and their practice of cervical cancer screening.
Table 7: Relationship between Knowledge of Respondents on Cervical Cancer Screening and Practice of Cervical Cancer Screening.
| Variables | Practice of Cervical Cancer Screening | x2 | df | P | ||
| Yes | No | |||||
| Knowledge of Cervical Cancer and Cervical Cancer Screening | Good knowledge | 20(32.3%) | 42(67.7%) | 9.674 | 1 | 0.002 |
| Poor Knowledge | 4(8%) | 46(92%) | ||||
| Total | 24(21.4%) | 88(78.6%) | ||||
x2=Pearson chi-square value, df=degree of freedom, P =Probability value
Inference: From Table 7 above, the null hypothesis is rejected, therefore, there is a significant relationship between the knowledge of respondents on cervical cancer screening and the practice of cervical cancer screening with (x2=9.674, P=.002) at P< .05.
The practice of cervical cancer screening is influenced significantly by respondents` level of knowledge, the practice of cervical cancer screening increases with increasing level of good knowledge of cervical cancer.
Hypothesis Three
Ho – There is no significant relationship between the attitude of respondents towards cervical cancer and their practice of cervical cancer screening.
Table 8: Relationship between Attitude of Respondents and their Practice of Cervical Cancer Screening.
| Variables | Practice of Cervical Cancer Screening | x2 | df | P | ||
| Yes | No | |||||
| Attitude of Respondents towards Cervical Cancer and Cervical Cancer Screening | Good attitude | 20(25.6%) | 58(74.4%) | 2.708 | 1 | 0.100 |
| Poor attitude | 4(11.8%) | 30(88.2%) | ||||
| Total | 24(21.4%) | 88(78.6%) | ||||
x2=Pearson chi-square value, df=degree of freedom, P =Probability value
Inference: From Table 8 above, the null hypothesis is accepted, therefore, there is no significant relationship between the attitude of respondents and their practice of cervical cancer screening with (x2=2.708, P=.100) as P>.05.
DISCUSSION OF FINDINGS
Cervical cancer is one of the most preventable cancers in the world and its` prognosis is better when detected early through cervical cancer screening. This study assessed the knowledge, attitude and practices regarding cervical cancer and screening among women in selected primary health care centres (PHCs) in Ogbomosho. In this present study, half (50%) of the respondents were between age 26-35 years implying that young adults dominate the study population. However, research evidence reveals that all age groups starting from the late teens are at risk of cervical cancer (WHO, 2018). The level of literacy of the study population can be estimated to be moderate as more than half (52.7%) had secondary education and (17.9%) had tertiary education. This may be because the study was conducted in the urban regions of the city. More than two-thirds were Christians and all three main ethnic groups were represented with Yoruba being the majority because the study was conducted in a Yoruba-dominated region.
Findings from Knowledge of Respondents on Cervical Cancer and Cervical Cancer Screening.
This present study has shown that more than two-thirds and about two-thirds were aware of cervical cancer and cervical cancer screening respectively. Contrastingly, Olubodun, et al (2019) who conducted a similar study in Lagos, southwestern Nigeria found out the majority of the study participants had not heard of cervical cancer. However, a study in India by Ghosh et al. (2021) revealed a similar level of awareness with 82% of the population having heard of cervical cancer before. Furthermore, Dulla et al. (2017) in a similar view found a similar level of awareness.
As regards the knowledge of respondents on cervical cancer, more than half (55%) of the respondents had good knowledge of cervical cancer and cervical cancer screening which includes the causes, risk factors, prevention and signs and symptoms of cervical cancer. More than half (55%) were able to identify foul-smelling discharge, abnormal vagina bleeding, and post-coital bleeding as signs of cervical cancer, likewise, the majority knew about having However, the only significant gap in knowledge was noticed as regards visual inspection with acetic acid (VIA) being a screening method for cervical cancer as less than half (42%) were able to identify it as a screening method, also, less than half were able to identify smoking and HPV as causes of cervical cancer, meanwhile, the majority (70.5%) were able to identify other screening methods such as PAP smear and other causes of cervical cancer such as early exposure to sex and having multiple sex partner. The level of knowledge of participants in this study is consistent with the study by Jassim et al. (2017) with many of their study participants having good knowledge of various concepts of cervical cancer such as causes, symptoms, and prevention and screening methods. However, the level of knowledge of participants in this study is not consistent with Olubodun et al (2019) who found out the majority of their study participants had a low level of knowledge of cervical cancer and its` screening. Likewise, in a systematic review by Malhotra, et al. (2020), the majority of the women had a low level of knowledge on cervical cancer. This varied level of knowledge may be due to the sociocultural context of the study settings, level of sensitization and health seeking behaviour. Differences in assessment tools could influence their knowledge level as there is no standardized instrument for the assessment of knowledge of women on cervical cancer.
Findings from Attitude of Respondents towards Cervical Cancer and Cervical Cancer Screening
This present study has shown that the majority (70%) had a good attitude towards cervical cancer and cervical cancer screening. This was evidenced as the majority (76.8%) thought that cervical cancer is preventable and that intermenstrual bleeding should not be considered normal, and more than two-thirds (75%) would prefer to not give birth to more than 4 children to reduce their risk of cervical cancer, majority (73.2%) agreed they would not keep a distance from a neighbourhood female suffering from cervical cancer; majority (76.8%) were willing to be screened for cervical cancer if screening services are made available, majority (74.1%) were willing to have Human Papilloma Virus immunization or recommend it to others to prevent cervical cancer. These findings are somewhat close to Dahiya, et al. (2019) who found more than half of their study participants to exhibit similar attitudinal features such as not keeping distance from a neighbourhood female suffering from cervical cancer, intermenstrual bleeding not being considered normal and desire to be screened when services are available. Furthermore, the findings corroborate Olubodun et al. (2019) who found out the majority (93.8%) were willing to be immunized or recommend HPV immunization to a friend or relative. The overall evaluation of the attitudes of the respondents towards cervical cancer and cervical cancer screening in this study is consistent with Malhotra, et al. (2020) who found the majority (59.97%) to have positive attitudes towards cervical cancer and cervical cancer screening. These findings provide an evidence base for policymakers and the government to ensure availability of the screening services considering the wide level of acceptance.
Findings from Practice of Cervical Cancer Screening among the Respondents.
This present study reveals a cervical cancer screening uptake rate of 21% as few (21.4%) had ever been screened for cervical cancer in the past. Supportively, Seyoum et al. (2017) in a similar study in Ethiopia found that few of the women had utilized cervical cancer screening services. Furthermore, this finding is somewhat close to Olubodun et al. (2019) who found out just (0.7%) of the women had done cervical cancer screening before. However, this finding is not consistent with Frank and Ijeoma (2017) in a similar study in Port Harcourt who found out about half (46%) of the respondents had practised cervical cancer screening. This difference may be because the study was conducted among health workers who might have better practices regarding cervical cancer screening.
Furthermore, out of this proportion that has practised cervical cancer screening, the majority (79.2%) had the screening done at a government hospital while the rest (20.8%) had it done at a private hospital, the screening methods used were mostly Pap smear Papanicolaou (91.7%), visual inspection with acetic acid (58.3%) and HPV DNA testing (58.3%). About half (45.8%) of the proportion that have had cervical cancer screening done before did it based on a doctor’s prescription while the rest (54.2%) did it voluntarily. Supportively, Olubodun et al. (2019) found out half of their study participants who practised cervical cancer screening had a pap smear done in a government tertiary hospital and it was based on a doctor’s request. More than one-third (41.7%) of the proportion that have had cervical cancer screening had it done the previous year, and about half had it done 2-3 years ago. This range of periods is acceptable as it is recommended that a PAP smear be done at least, once every three years (Dahiya, et al.,2019).
Findings from Barriers to the Practice of Cervical Cancer Screening among the Respondents.
This present study has shown the self-reported barriers to the practice of cervical cancer screening among the respondents to include lack of health education or health sensitization on cervical cancer screening (45.5%), lack of knowledge on the screenings (39.3%), absence of signs and symptoms of cervical cancer (39.3%), low socioeconomic status (29.5%), cost of procedure (17.9%), unavailability of services (17.9%) and religious beliefs (14.3%). This finding is keeping in view with Malhotra, et al. (2020) who found out the most common barrier to undergoing screening was no signs and symptoms of cervical cancer (32.78%) followed by no or low level of knowledge (28.21%). Similarly, a study in Lagos, southwestern Nigeria by Olubodun, et al. (2019) revealed that not being aware of screening (91.4%), lack of symptoms (15.9%), and not being requested by health workers (2.6%). Furthermore, keeping in view the findings of this study, Frank and Ijeoma (2017) in a similar study in Lagos, Nigeria found out not knowing about the test (6.4%) and cost consideration 27(8.2%) were barriers influencing the utilization of cervical cancer screening services. The consistency of the factors identified in this present study across all the studies reviewed makes it a necessity to develop interventions to control or modify the factors to promote the practice of cervical cancer screening among women.
Findings from the Study Hypotheses
The study hypotheses tested revealed that there is a significant relationship between the educational status of respondents and their knowledge of cervical cancer screening at P< .05. There exists a positive association between the educational status of respondents and their knowledge of cervical cancer and its` screening as their level of knowledge increases with increasing level of education. Furthermore, there exists a significant relationship between the knowledge of respondents on cervical cancer screening and the practice of cervical cancer screening at p< .05. Practice of cervical cancer screening is influenced significantly by respondents` level of knowledge, the practice of cervical cancer screening increases with increasing level of good knowledge of cervical cancer. This finding is supported by Frank and Ijeoma (2017) who found a significant association between the knowledge of respondents and the uptake of cervical cancer screening. However, there is no significant relationship between the attitude of respondents and their practice of cervical cancer screening with (x2=2.708, p=.100) as p> .050. This finding is not consistent with Seyoum, et al. (2017) who found out significant association between attitude of respondents and their utilization of cervical cancer screening services. These differences may be due to the presence of one or more confounding factors such as the knowledge of respondents on cervical cancer and, the cost of the procedure among others.
CONCLUSION
Conclusively, this study has shown that the knowledge and attitude of women towards cervical cancer and cervical cancer screening was good, however, it is not commensurate to their level of practice of cervical cancer screening which is low. However, factors responsible for this include level of education and knowledge The most prevalent barriers identified include lack of health education and knowledge on the screenings, absence of signs and symptoms of cervical cancer, low socioeconomic status, cost of procedure, unavailability of services and religious beliefs. The way forward is to improve the knowledge of the women on cervical cancer and screening by the instrumentality of health education while efforts are being put in place to make cervical cancer screening services available cheaply.
LIMITATION OF STUDY
This study is subject to several limitations which should be acknowledged. Firstly, financial constraints restricted the researchers from covering a larger population, limiting the ability to generalize findings to a national scale. Secondly, time constraints hindered the researchers’ ability to administer instruments to respondents adequately. Additionally, some respondents displayed reluctance in responding to questions, although reassurances of confidentiality and anonymity were provided. This may have impacted the completeness and accuracy of the data collected. Furthermore, the study’s generalizability is limited as it was conducted in only two primary healthcare centres within the state. This narrow scope affects the broader applicability of the research findings. Moreover, the cross-sectional design employed in this study inherently prohibits establishing causal relationships. Furthermore, the analytical method utilized did not account for confounding variables, potentially influencing the accuracy of results. Lastly, employing a mixed-method approach could have provided greater depth and understanding of the study, enhancing its overall quality and comprehensiveness.
RECOMMENDATIONS
The study’s recommendations based on findings for enhancing cervical cancer knowledge and screening include comprehensive education campaigns targeting diverse demographics, health education programs to dispel misconceptions, and making screening services more accessible and affordable, particularly in rural areas. Integrating screening into existing healthcare programs and addressing barriers like religious beliefs are essential. Promoting HPV vaccination and regular monitoring of screening programs are advised. Empowering women through self-care education can improve prevention efforts, leading to earlier detection and better treatment outcomes, ultimately reducing cervical cancer mortality rates. These measures aim to increase awareness, improve attitudes, and promote proactive health management. Future researchers must shed more light on the sociocultural factors influencing the attitude and the practice of women regarding cervical cancer and screening. Also, the study population and sample size should be enlarged in future research to capture more towns.
REFERENCES
- Adekanle, D. A., Adeyemi, A. S., & Fadero, F. F. (2011). Ante-Partum haemorrhage and pregnancy outcome in LAUTECH teaching hospital, southwestern Nigeria. J Med Sci, 2(12), 1243-7.
- Ahmed, S. A., Sabitu, K., Idris, S. H., & Ahmed, R. (2013). Knowledge, attitude and practice of cervical cancer screening among market women in Zaria, Nigeria. Nigerian medical journal: journal of the Nigeria Medical Association, 54(5), 316–319. https://doi.org/10.4103/0300-1652.122337
- Ajah, L. O., Iyoke, C. A., Ezeonu, P. O., Ugwu, G. O., Onoh, R. C., & Ibo, C. C. (2015). Association between knowledge of cervical cancer/screening and attitude of teachers to immunization of adolescent girls with human papillomavirus vaccine in Abakaliki, Nigeria. American Journal of Cancer Prevention, 3(1), 8-12.
- Ajibola, I. Samuel, A. Olowookere, A. Tolulope, F. & Olumuyiwa, A. (2016). Determinants of Cervical Cancer Screening Uptake among Women in Ilorin, North Central Nigeria: A Community-Based Study.
- Akinfolarin, A. C., Olusegun, A. K., Okunola, T. O., Go, O., & Onwundiegu, U. (2017). Age and pattern of Pap smear abnormalities: Implications for cervical cancer control in a developing country. Journal of Cytology, 34(4), 208. https://doi.org/10.4103/joc.joc_199_15
- Butho, N, Amita, B., Jeremy, K., Patricia, B. &Paulina, J (2015) “Factors associated with the uptake of cervical cancer screening among women in Portland Jamaica,” New American Journal of Medical Sciences, 7(3). pp. 104–113.
- Catarino, R., Petignat, P., Dongui, G., & Vassilakos, P. (2015). Cervical cancer screening in developing countries at a crossroads: Emerging technologies and policy choices. World journal of clinical oncology, 6(6), 281–290. https://doi.org/10.5306/wjco.v6.i6.281
- Dahiya, N., Aggarwal, K., Singh, M., Garg, S., & Kumar, R. (2019). Knowledge, attitude, and practice regarding the screening of cervical cancer among women in New Delhi, India. Tzu Chi Medical Journal, 31(4), 240. https://doi.org/10.4103/tcmj.tcmj_145_18
- Dulla, D., Daka, D., & Wakgari, N. (2017). Knowledge about cervical cancer screening and its practice among female health care workers in southern Ethiopia: a cross-sectional study. International Journal of Women’s Health, 9, 365–372. https://doi.org/10.2147/ijwh.s132202
- Ghosh, S., Mallya, S. D., Shetty, R. S., Pattanshetty, S. M., Pandey, D., Kabekkodu, S. P., Satyamoorthy, K., & Kamath, V. G. (2020). Knowledge, Attitude and Practices Towards Cervical Cancer and its Screening Among Women from Tribal Population: a Community-Based Study from Southern India. Journal of Racial and Ethnic Health Disparities, 8(1), 88–93. https://doi.org/10.1007/s40615-020-00760-4
- Hussain, A., Alkhenizan, A., McWalter, P., Qazi, N., Alshmassi, A., Farooqi, S., & Abdulkarim, A. (2016). Attitudes and perceptions towards HPV vaccination among young women in Saudi Arabia. Journal of Family and Community Medicine, 23(3), 145. https://doi.org/10.4103/2230-8229.189107
- Jassim, G., Obeid, A. & Al Nasheet, H.A. (2018). Knowledge, attitudes, and practices regarding cervical cancer and screening among women visiting primary health care Centres in Bahrain. BMC Public Health. https://doi.org/10.1186/s12889-018-5023-7
- Malhotra, N., Taneja, N., Shankar, R., Pal, A., Chawla, B., Awasthi, A. A., & Janardhanan, R. (2020). Knowledge, Attitude & Practice towards Cervical Cancer Screening among Women Globally – A Systematic Review. Journal of Womens Health and Development, 3(3), 194–210. https://www.fortunejournals.com/articles/knowledge-attitude-amp-practice-towards-cervical-cancer-screening-among-women-globally-ndash-a-systematic-review.html
- Mohammed A, Ahmed SA, Oluwole OP&Avidime S. (2017). Malignant tumours of the female genital tract in Zaria, Nigeria: Analysis of 513 cases. Ann Afr Med
- Olubodun, T., Odukoya, O.O. & Balogun, M.R. (2019) Knowledge, attitude and practice of cervical cancer prevention, among women residing in an urban slum in Lagos, South West, Nigeria. Pan African Medical Journal. 32(130).
- Seyoum, T., Yesuf, A., Kejela, G., & Gebremeskel, F. (2017). Utilization of Cervical Cancer Screening and Associated Factors among Female Health Workers in Governmental Health Institution of Arba Minch Town and Zuria District, Gamo Gofa Zone, Arba Minch, Ethiopia, 2016. Archives in Cancer Research, 05(04). https://doi.org/10.21767/2254-6081.100165
- Sowemimo, O. O., Ojo, O. O., & Fasubaa, O. B. (2017). Cervical cancer screening and practice in low resource countries: Nigeria as a case study. Tropical Journal of Obstetrics and Gynaecology, 34(3), 170. https://doi.org/10.4103/tjog.tjog_66_17
- World Health Organisation (2018). WHO Director-General calls for all countries to take action to help end the suffering caused by cervical cancer. 2018.https://www.who.int/reproductivehealth/call-to-action elimination cervical-cancer/en/
- World Health Organization. (2019). Cervical Cancer. World Health Organization; World Health Organization. https://www.who.int/news-room/fact-sheets/detail/cervical-cancer