
Nutritional Status and Dietary Diversity among Adolescent Girls in Rohingya Refugee Camp in Cox’s Bazar, Bangladesh
- Dr. Jami Parvin Nitu
- Syeda Fatima Rezwana
- Dr. Shamima Begum
- 509-515
- Apr 16, 2025
- Education
Nutritional Status and Dietary Diversity among Adolescent Girls in Rohingya Refugee Camp in Cox’s Bazar, Bangladesh
Dr. Jami Parvin Nitu, Syeda Fatima Rezwana, Dr. Shamima Begum
Pundra University of Science and Technology, Bogura, Bangladesh
DOI: https://doi.org/10.51244/IJRSI.2025.121500046P
Received: 11 March 2024; Accepted: 13 March 2025; Published: 16 April 2025
Background:
Adolescent girls, constituting approximately 10% of the entire populace. These girls require special care as they bear significant relevance to the health and shape of the well-being of present and future generations.
Design and Methods:
This cross-sectional study was aimed at evaluating the nutritional status and dietary diversity among adolescent girls (10-19 years) of a particular Rohingya camp in Cox’s Bazar. A pretested, semi-structured questionnaire was implemented to assemble information regarding anthropometric measurements, diversity of diets, and sociodemographic traits. An assessment of nutritional status concerning individual dietary diversity was also done.
Result:
The socio-demographic data show that most of the participants are in middle adolescence, from a lower-middle or middle-class background. Individual dietary diversity reflects that nearly half of the adolescent girls have medium dietary diversity, and another 33.4% have low, showing a general need to improve access to a wider variety of nutritious food. The nutritional status, as indicated by BAZ, 15.6% either severely or moderately thin while 8.7% of the participants are overweight. As indicated by the HAZ, 11% of the adolescent girls are severely stunted, while 24.7% are mildly to moderately stunted; the majority, 55.3%, have a normal height. There were positive relations between nutritional status and individual dietary diversity of the adolescent girls (correlation coefficient of 0.128).
Conclusion:
This will provide substantial insights to support a comprehensive overview of the condition and formulation of appropriate dietary interventions and health education programs for adolescent girls of this endangered segment of inhabitants transported to Rohingya camps.
Key Words: Nutritional status, Dietary diversity, Adolescent, Rohingya refugee
INTRODUCTION
Violence in the Rakhine state of Myanmar has reached a level of brutality that in 2017-2018 drove nearly 700,000 Rohingyas across the border into Bangladesh, where more than 200,000 were already living. The Rohingya refugee crisis, which saw major military clampdowns in 1978, 1991-1992, and most recently in 2017-2018 within Myanmar, has forced large numbers of the Rohingya people to seek refuge in Bangladesh. Today, most of these refugees are housed in very crowded camps in Cox’s Bazar, Bangladesh1. Despite humanitarian international support, most refugees interact with the local markets in procuring goods and services and economically contribute as low-skilled laborers and consumers2. However, due to the denial by Myanmar to recognize the Rohingyas, their fate has remained very uncertain. Gradually, these immediate humanitarian needs of Bangladesh have transformed into developmental ones over time when the population becomes further entrenched in the camps3.
Such humanitarian assistance includes food vouchers that can be used by refugee households at designated food outlets to acquire foodstuffs, besides micro-gardening kits and training to support the production of their food4. Despite this, malnutrition remains high, especially among vulnerable groups such as adolescent girls. According to the WHO, adolescents are young people between the ages of 10 and 195. Adolescents are a significant segment of the population in developing countries like Bangladesh. During this stage, rapid physical growth, cognitive development, and sexual maturation increase nutritional needs for calories, proteins, vitamins, iron, and calcium6. Poor nutrition will result in retarded sexual growth and development, besides predisposing the individual to a high incidence of illness7.
The situation is especially dire among adolescent girls in the Rohingya refugee camps. More than 60% of the school-age girls between 10 and 16 years old in Cox’s Bazar have an intake of less than 75% of the recommended dietary allowance, RDA (Adolescent Malnutrition in Developing Countries: A Close Look at the Problem and at Two National Experiences | Request PDF, n.d.). Minerals include very vital nutrients like proteins, iron, and calcium. Nutritional deficiencies like this could result in long-term health consequences, such as intergenerational malnutrition8. Put differently, malnourished adolescent girls grow into malnourished women giving birth to under-nourished babies. They have to face a multitude of problems, starting with poor infrastructure, including a lack of health facilities and a lack of awareness about the long-term consequences brought about by malnutrition9.
This is exacerbated by the living conditions in camps characterized by abject poverty, child labor, inadequate infrastructure, and poor living standards that exacerbate their nutritional status10. Most girls in this refugee population have chronic deficiencies in energy and micronutrients, which are manifested as stunting and wasting11. Poor environmental conditions and an inadequate level of opportunities for nutrition and health-care services have resulted in a vicious circle of poverty, ill health, and malnutrition12.
The current study estimated the nutritional status and dietary diversity of adolescent girls residing in Rohingya refugee camps in Cox’s Bazar; usually, girls in this setting are among the most vulnerable. This research reviewed dietary habits and nutritional health in adolescent girls, unlike previous surveys that have targeted the broader refugee population in general. The study will therefore be of great value in ascertaining the prevailing status of food security within the camps and highlighting areas of acute intervention.
Overall, the aim is to determine the nutritional status and dietary patterns among these girls; whereas its specific objectives are to ascertain their socio-demographic characteristics and household information, to assess the nutritional status, and to determine the diversity of their diets. The study will also explore the association that exists between nutritional condition and dietary diversity. The findings will be crucial for decision-makers in informing them of the need to devise relevant strategies and interventions required for improving household food security and health conditions. The latter creates a unique nutritional challenge among these adolescents that will also help design effective nutrition-related programs to help break the cycle of malnutrition for improved long-term health and well-being among adolescent girls in refugee camps.
METHODOLOGY
The present study was a cross-sectional analysis undertaken to assess the nutritional condition and dietary diversity of adolescent girls in the Rohingya refugee camp in Cox’s Bazar, Bangladesh. Data was obtained through a previously evaluated semi-structured questionnaire. Written consent was collected from participants after explaining the purpose of the study.
Study Design and Population: The population targeted was adolescent girls aged 10-19 years living in the selected refugee camp. This excluded those with chronic illnesses, unable to give informed consent, or were below or above the age bracket. From literature reviews, at a prevalence of nutritional problems of 24.8%, the sample size calculated was 317 and this was adjusted for a non-response rate of 10%.
Methods of Data Collection: Data collection was done through face-to-face interviews. Information on socio-demographics included age, education, income, family structure, etc., and household data included house structure, water source, availability of toilet, food expenditure, etc. Dietary diversity was measured using a previously validated FFQ with nine food groups. The nutritional variety score was categorized as low ≤ 3 food groups, medium (4-5 groups), and high ≥ 6 groups.
Anthropometrical variables were measured using standard techniques such as height being evaluated to the closest 0.1 cm on a stadiometer, while weight was recorded to the nearest 0.1kg on a digital scale. BMI was thereafter computed as weight in kilograms divided by height in meters squared (m²), and categorized using WHO standards.
Data Management and Analysis: The data was cleaned and entered into SPSS software, version 26, for analysis. Descriptive statistics were used to summarize socio-demographic and dietary information, while logistic regression was employed to assess the association between dietary diversity and nutritional status. Some of the variables included in the analysis were age, income level, and household characteristics.
Validity and Reliability: The questionnaire was pretested on 10% of the sample to ascertain that items were clear, with necessary modifications effected before the main data collection. The measurements were taken accurately, instruments were calibrated, and continuous supervision was done. The data collection and analysis were supervised by the principal investigator. This was to ensure that the data quality was maintained.
Ethical Considerations: The approval was sought from the BUHS Ethical Review Board. Participation was entirely voluntary, and written informed consent was obtained from participants, who were assured of the confidentiality of their responses and allowed to discontinue interaction at their convenience.
RESULT
Table 1: Socio-Demographic Features of Study Subject
| Characteristics | Frequency | Percent (%) |
| Age group | ||
| 10-13 years | 96 | 30.2 |
| 14-16years | 128 | 40.5 |
| 17-19years | 93 | 29.3 |
| Socioeconomic status | ||
| Lower class (Less than 14000tk) | 52 | 16.3 |
| Lower middle class (14000-17000tk) | 112 | 35.4 |
| Middle class (17000-25000tk) | 99 | 31.3 |
| Upper class (More than 25000tk) | 54 | 18.0 |
| Occupation | ||
| Housewife | 24 | 7.6 |
| Student | 230 | 72.7 |
| Farmer | 11 | 3.3 |
| Garments worker | 52 | 16.4 |
The socio-demographic data show that most of the participants are between 14 and 16 years old, from a lower-middle and middle-class background. Out of them, 72.7% were identified as students, though other smaller groups had also been involved in domestic or labor roles, indicating an adolescent population with limited economic resources.
Table 2: Nutritional condition of adolescent girls based on their HAZ (Height for age score)
| Nutritional condition | Frequency | Percent (%) |
| Severely stunted | 64 | 11.0 |
| Normal height | 175 | 55.3 |
| Mild to moderate stunted | 78 | 24.7 |
| Total | 317 | 100 |
As indicated by the nutritional status using HAZ, 11% of the adolescent girls are severely stunted, while 24.7% are mildly to moderately stunted; the majority, 55.3%, have a normal height, reflecting varied growth outcomes among participants.
Table 3: Nutritional condition of adolescent girls based on their BAZ (Body Mass Index for age)
| Nutritional Condition | Frequency | Percent (%) |
| Severely thin | 12 | 3.5 |
| Moderately thin | 38 | 12.1 |
| Normal weight | 240 | 75.7 |
| Overweight | 27 | 8.7 |
| Total | 317 | 100 |
The nutritional status, as indicated by BAZ, is normally weighted for 75.7%, while 15.6% fall either under the severely thin or moderately thin category. Another 8.7% of the participants are overweight, thus showing that both undernutrition and overweight coexist among this population.
Table 4: Correlation between nutritional status (BAZ) and individual dietary diversity (IDD)
| Factors | Correlations | BAZ category | IDD category |
| BAZ category | Correlation Coefficient | 1 | 0.128 |
| Sig.(2-tailed) | . | 0.06 | |
| IDD category | Correlation Coefficient | 0.128 | 1 |
| Sig.(2-tailed) | 0.06 | . | |
| N | 317 | 317 |
The correlation analysis between BAZ and IDD has indicated a weak positive association with a correlation coefficient of 0.128, suggesting that increased dietary diversity may have a small effect on improving nutritional status. Nevertheless, the level of p = 0.06 indicates that the correlation is not statistically significant, and this would mean that other determinants are more explanatory of the entire nutritional condition of adolescent girls.
Table 5: Relationship between individual dietary diversity score and nutritional status (HAZ):
| Individual Dietary Diversity | Nutritional Status (HAZ) | Test of Significance ꭓ2 | P value | ||
| Severely Stunted | Moderately Stunted | Normal Height | |||
| Lowest Dietary Diversity | 10.3% | 28.3% | 61.4% | 58.801* | (P<0.001) |
| Medium Dietary Diversity | 7.6% | 19.0% | 73.4% | ||
| High Dietary Diversity | 4.2% | 36.9% | 58.9% | ||
Table 5 shows relationship between individual dietary diversity score and nutritional status (HAZ) where individual dietary diversity score is associated with height for age of the respondents. Result showed statistically significant relationship (p<0.001).
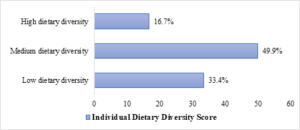
Figure 1: Nutritional condition of adolescent girls based on their Individual Dietary Diversity (IDD)
Individual dietary diversity, as indicated by IDD, reflects that nearly half of the adolescent girls 49.9%-have medium dietary diversity, and another 33.4% have low dietary diversity, pointing to food intake with limited varieties. Only 16.7% of the participants fall into the category of high dietary diversity, showing a general need to improve access to a wider variety of nutritious food.
DISCUSSION
The study presents a detailed analysis of the socio-demographic and nutritional status of 317 adolescent girls and found that there was a high challenge to malnutrition.
The socio-demographic background of adolescent girls includes a wide age distribution, with most falling in the age category of 14-16 years. As far as socioeconomic backgrounds go, most belong to the lower-middle or middle-class family category, while 16.3% are from lower- income categories. Most girls in the sample, or 72.7%, were students, though some were garment workers (16.4%) or housewives (7.6%), reflecting economic pressures. The socioeconomic determinants include the need for income and household responsibilities that might affect their nutritional and health status, thus targeted health and nutrition intervention. According to a different survey, 11.4 % of adolescent households made less than 10,000 takas per month, whereas 51% of adolescent households made more than 20,000 takas9.
Nutritional assessment is a showstopper, with outlandish rates for stunting: 11% were classified as severely stunted, and 24.7% as mildly to moderately stunted, where this can easily detract from physical and cognitive development. In a different study, the results were almost identical: 9% of the girls were extremely thin, while 74.7 % were of normal weight. 3% were overweight13.
Equally, the BAZ presented a double burden of malnutrition: though 75.7% were normally weighted, 15.6% were moderately or severely thin, and 8.7% were overweight, signifying both dietary patterns and lifestyle factors at work. While the individual dietary diversity assessment estimated 16.7% with high dietary diversity, as is often related to socioeconomic constraints and cultural practices, 33.4% reported low dietary diversity due to inadequate intake of several essential nutrients.
Accordingly, the weak positive correlation between BAZ and IDD, r = 0.128, p = 0.06, can suggest that dietary diversity might not singly control the nutritional status but also could be modified by other factors such as SES, physical activity, and access to healthcare. The study recommends focused interventions that enhance dietary diversity and food security, while also addressing the socio-economic factors contributing to malnutrition, as an approach to mitigate both undernutrition and overweight in this at-risk group.
Food availability may influence consumption habits to a large amount, according to collected data, because people generally have limited resources, knowledge, and markets. At the food distribution point, gender inequalities may cause malnutrition, particularly among adolescent girls. In a related study, over 40% of Bangladeshis who live below the poverty line have inadequate dietary intake and nutritional deficiencies, with one of the main reasons being insufficient income14.
CONCLUSION
In conclusion, the educational status of adolescent girls in a selected refugee camp aged 10-19 years was quite satisfactory: 80% maintained normal weight, though one-third were still stunted. A good individual dietary diversity correlates positively with nutritional status. These results imply that community-oriented, adolescent-friendly dietary and healthcare education might boost these girls’ basic nutritional habits in conjunction with financial growth. The information obtained will be useful in formulating appropriate dietary interventions and health education programs for adolescent girls within the refugee camp.
RECOMMENDATION
The recommendations may be considered for Community-based adolescents friendly education programs for the FDMN families living in Bangladesh encouraging more diversified food.
REFERENCES
- Rahman, R., Faiz, M. A., Nu, M. Y., Hassan, R., Chakrabarty, A. K., Kabir, I., Islam, K., Jafarullah, A. K. M., Alakabawy, M., Khatami, A., & Rashid, H. (2020). A Rapid Assessment of Health Literacy and Health Status of Rohingya Refugees Living in Cox’s Bazar, Bangladesh Following the August 2017 Exodus from Myanmar: A Cross-Sectional Study. Tropical Medicine and Infectious Disease 2020, Vol. 5, Page 110, 5(3), 110. https://doi.org/10.3390/TROPICALMED5030110
- Alix-Garcia, J., Bartlett, A., & Saah, D. (2012). Displaced Populations, Humanitarian Assistance and Hosts: A Framework for Analyzing Impacts on Semi-urban Households. World Development, 40(2), 373–386. https://doi.org/10.1016/J.WORLDDEV.2011.06.002
- Alloush, M., Taylor, J. E., Gupta, A., Rojas Valdes, R. I., & Gonzalez-Estrada, E. (2017). Economic Life in Refugee Camps. World Development, 95, 334–347. https://doi.org/10.1016/J.WORLDDEV.2017.02.030
- Hoddinott, J., Dorosh, P., Filipski, M., Rosenbach, G., & Tiburcio, E. (2020). Food transfers, electronic food vouchers and child nutritional status among Rohingya children living in Bangladesh. PLoS ONE, 15(4). https://doi.org/10.1371/JOURNAL.PONE.0230457
- De Onis, M., Onyango, A. W., Borghi, E., Siyam, A., Nishida, C., & Siekmann, J. (2007). Development of a WHO growth reference for school-aged children and adolescents. Bulletin of the World Health Organization, 85(9), 660–667. https://doi.org/10.2471/BLT.07.043497
- Hyder, S. M. Z., Haseen, F., Khan, M., Schaetzel, T., Jalal, C. S. B., Rahman, M., Lönnerdal, B., Mannar, V., & Mehansho, H. (2007). A Multiple-Micronutrient-Fortified Beverage Affects Hemoglobin, Iron, and Vitamin A Status and Growth in Adolescent Girls in Rural Bangladesh. Journal of Nutrition, 137(9),2147–2153. https://doi.org/10.1093/JN/137.9.2147
- Meier, P. R., Nickerson, H. J., Olson, K. A., Berg, R. L., & Meyer, J. A. (2003). Prevention of iron deficiency anemia in adolescent and adult pregnancies. Clinical Medicine & Research, 1(1), 29–36. https://doi.org/10.3121/CMR.1.1.29
- Ahmed, F., Zareen, M., Khan, M. R., Banu, C. P., Haq, M. N., & Jackson, A. A. (1998). Dietary pattern, nutrient intake and growth of adolescent school girls in urban Bangladesh. Public Health Nutrition, 1(2), 83–92. https://doi.org/10.1079/PHN19980014
- Alam, N., Roy, S. K., Ahmed, T., & Ahmed, A. M. S. (2010). Nutritional Status, Dietary Intake, and Relevant Knowledge of Adolescent Girls in Rural Bangladesh. Journal of Health, Population, and Nutrition, 28(1), 86. https://doi.org/10.3329/JHPN.V28I1.4527
- Viteri, F. E., & Gonzalez, H. (2002). Adverse outcomes of poor micronutrient status in childhood and adolescence. Nutrition Reviews, 60(5 Pt 2). https://doi.org/10.1301/00296640260130795
- Khuri, J., Wang, Y., Holden, K., Fly, A. D., Mbogori, T., Mueller, S., Kandiah, J., & Zhang, M. (2022). Dietary Intake and Nutritional Status among Refugees in Host Countries: A Systematic Advances in Nutrition, 13(5), 1846. https://doi.org/10.1093/ADVANCES/NMAC051
- Rahman, M. A., Halder, H. R., Rahman, M. S., & Parvez, M. (2021). Poverty and childhood malnutrition: Evidence-based on a nationally representative survey of Bangladesh. PLoS ONE, 16(8). https://doi.org/10.1371/JOURNAL.PONE.0256235
- Alam, S. S., Rahman, M. N., Mia, M. A., Haque, M. M., & Islam, K. (2018). Dietary Diversity and Nutritional Status of Adolescent Girls in Selected Urban Slum of Dhaka City in Bangladesh. Nutrition & Food Science International Journal, 7(3), 1–5. https://doi.org/10.19080/NFSIJ.2018.07.555711
- Braun, B., & Aßheuer, T. (2011). Floods in megacity environments: Vulnerability and coping strategies of slum dwellers in Dhaka/Bangladesh. Natural Hazards, 58(2), 771–787. https://doi.org/10.1007/S11069-011-9752-5/TABLES/9