
Ophtalmologic, serologic and therapeutic aspects of ocular toxoplasmosis toxoplasmose oculaire: aspects ophtalmologiques, sérologiques et thérapeutiques
- Meriam Bouchekoua
- Manel Mejri
- Dorsaf Aloui
- Azer Ben Salah
- Moez Lazzem
- Mejdi Boukari
- Ilhem Mili
- Sonia Trabelsi
- 211-219
- Jan 6, 2024
- Social Welfare
Ophtalmologic, Serologic and Therapeutic Aspects of Ocular Toxoplasmosis Toxoplasmose Oculaire: Aspects Ophtalmologiques, Sérologiques et Thérapeutiques
*Meriam Bouchekoua1, Manel Mejri2, Dorsaf Aloui3, Azer Ben Salah4, Moez Lazzem5, Mejdi Boukari6, Ilhem Mili7, Sonia Trabelsi8
1Laboratory of Parasitology-Mycology, Charles Nicolle University Hospital, Tunis, Tunisia
2Laboratory of Parasitology-Mycology, Fattouma Bourguiba University Hospital, Monastir, Tunisia
3Department of Ophthalmology, Charles Nicolle University Hospital, Tunis, Tunisia
4University of Tunis El Manar, Faculty of Medicine of Tunis
DOI: https://doi.org/10.51244/IJRSI.2023.1012017
Received: 07 December 2023;; Accepted: 11 December 2023; Published: 05 January 2024
ABSTRACT
Ocular toxoplasmosis (OT) is the most frequent cause of inflammation of the posterior segment of the eye due to infectious causes. It can occur in congenital toxoplasmosis, in the immunocom promised and, more rarely, in the immuno competent. It is a critical disease, as it can lead to blindness. The aim of our study was to investigate the clinical, serological, and therapeutic features of TO.
Methods: A bicentric retrospective study was conducted at the Parasitology-Mycology laboratories of two Tunisian Hospitals(2017-2021), involving toxoplasma serologies performed on 175 patients in the context of exploration for uveitis and on six babies with congenital toxoplasmosis. As screening technique, we used was electrochemilum inescence (Cobas® e411) and Enzyme Linked Filtration Assay (mini-Vidas®). If IgM and/or IgG were positive, and depending on ophthalmo logical signs, we added a comparative Western Blot (WB) of serum and aqueous humor.
Results
Serological results were:
– no immunity in 71 patients, rejecting OT
– long-standing immunity in 103 patients, 15 of whom underwent comparative WB tests, four of which were positive- recent primary infection in one case with a positive WB.
Thus, five cases of OT were confirmed(Three panuveitis and two anterior uveitis). Their respective ages were 14, 25, 33, 43 and 50 years old.Ophthalmological follow-up of five babies during the first year of life (one lost at six months) revealed chorioretinitis in one baby only.
Conclusion
Ocular involvement may represent a late revelation of unrecognized congenital toxoplasmosis. Its occurrence in immuno competent is not exceptional, but remains underestimated, as aqueous humor puncture is not systematically performed due to its invasive nature.
Key words: Ocular toxoplasmosis, congenital toxoplasmosis, immuno competent, serology, Tunisia
Introduction
Toxoplasma gondii (T.gondii) is a protozoan parasite that infects up to a third of the world’s population. The frequency of toxoplasmosis varies significantly from one country to another and even from one region to another, due to the mode of contamination by ingestion ofsoiled food by the parasite [1]. T.gondii causes infections, often benign in the immunocompetent subject. However, this parasitosis can be severe in immunocompromised individuals and in pregnant women. In this population, transmission of the parasite to the fetus, can lead to congenital toxoplasmosis (CT). The clinical manifestations of this embryofe to paty are essentially neurological and ocular and may appear several years after maternal-fetal contamination.The eye is the main target organ for the symptomatic manifestations of CT. In case of early maternal infection, ocular involvement is thought to affect about 90% of fetuses, and is essentially in the form of chorioretinitis which may appear late after birth [2]. Ocular involvement during toxoplasmosis occurs in approximately 2% of infected patients. However, it is the most frequent cause of inflammation of the posterior segment of the eye of infectious origin and is responsible for up to 85% of cases of posterior uveitis in immunocompetent subjects [3].In immunocompromised patients, toxoplasmosis may take an acute form of primary infection or secondary after reactivation. Ocular involvement in the form of chorioretinitis is found in the majority of cases [1] The diagnosis of ocular toxoplasmosis [OT] is primarily clinical when it comes to typical symptoms. In atypical cases, biological diagnosis becomes
Material And Methods:
– Study design and setting
We conducted a retrospective, descriptive and bi-centric study at the Parasitology-Mycology laboratory of Charles Nicolle Hospital of Tunis (located in north-eastern Tunisia ), as well as Fattouma Bourguiba Hospital of Monastir (located in the central coast of Tunisia)over a period from May 2017 to November 2021.
– Study population
Inclusion criteria
Immunocompromised patients with chorioretinitis.
– Data collection
We collected the available epidemiological, clinical, biological and therapeutic data for each included patient. The study included confirmed cases of acquired or congenital OT, through toxoplasmosis’s serology. So, we have distinguished two types of population:
-Population 1: patients referred for suspected toxoplasmic uveitis.
-Population 2: new-born or infants aged less than one yearand affected by a confirmed CT.
Non-inclusion criteria
Moreover, for the babies, we collected the results of the antenatal and postnatal diagnosis and the data of the ophthalmological follow-up.
– Screening of toxoplasmosis in population 1
We proceeded by determining the patient’s serological status vis-a-vis to toxoplasmosis by the combined research of immunoglobulins G (IgG) and M (IgM) using immuno-analysis automats. Two assay techniques were used in our study based on the principle of Electrochemiluminescence immunoassay (ECLIA) of the Cobas® e411 automaton (Roche diagnostic, Mannheim, Germany) in the laboratory of Charles Nicolle Hospital and the principle of the Enzyme Linked Fluorescent Assay (ELFA) of the Mini VIDAS® automaton (BioMerieux® S.A., Lyon, France) in the laboratory of Fattouma Bourguiba.
According to the results of the different serological tests, we concluded that:
-Absence of immunity:in case of negative serology. OT was then rejected,
-Old immunity: in case of absence of IgM and stability of IgG between 2 samples taken 21 days apart.
– Certain recent toxoplasmosis: in case of seroconversion or presence of IgM with significant rise of IgG (at least doubling of the titre) between 2 samples spaced 15 to 21 days apart.
-Probable recent toxoplasmosis: in case of positivity of IgM and stability of IgG between two samples taken 15 to 21 days apart.
In case of positive serology in IgG and/or IgM and according to the ophthalmological signs, we completed by a comparative Western Blot (WB) serum/aqueous humor. It was performed using the TOXOPLASMA WB IgG-IgM kit (LDBIO Diagnostics, Lyon, France). The diagnosis of OT was confirmed in case of WB positivity.
– Screening of toxoplasmosis in population 2
This diagnosis was performed in babies whose diagnosis of TC was confirmed in antenatal with PCR by the presence of toxoplasmic DNA in the amniotic fluid and/or presence of ultrasound abnormalities suggestive of embryofetopathy, and in postnatal by a serological profile confirming the TC.
Signs of TO were looked for on ophthalmological examination and fundus, such as retinal lesions of the posterior pole, macular lesions, juxta-papillary lesions and neuroretinitis…
Statistical analysis and bibliographic research
Epidemiological and diagnostic data entry and statistical analysis were conducted using IBM® SPSS® software, version 20. For the bibliographic research, weused by means of Pub Med®, sciences direct® and Google Scholar® with the following keywords: toxoplasmosis, ocular toxoplasmosis, electrochemilumminescence, enzyme linked fluorescent assay, congenital toxoplasmosis, retinochoroiditis.
Ethical considerations
During data entry and processing of the results, patient’s privacy and anonymity were respected.
No conflict of interest was identified in this work.
RESULTS
Characteristics of the study population
Population 1
We identified 175 suspected cases of OT. The median age was 37 ± 20 years oldwith age extremes ranging from five to 73 years old. The sex ratio was 0.5. Patients were mainly from the ophthalmology and internal medicine departments of the two hospitals. Among the 175 patients, 71 were IgG and IgMseronegative. An old immunity was diagnosed in 103 patients, of which 15 benefited from a comparative serum/aqueous humor western blot.One patient presented a primary infection with positive IgG and IgM leading to a comparative western blot.
Population 2
During the study period, we identified six babies affected by CT.Three of them were IgG and IgM positive. Three had only IgG positive serology and the diagnosis of CT was conducted in view of the elevation of these isotypes during the follow-up in two newborns and the positivity of the comparative mother/baby western blot in another.
Characteristics of patients with ocular toxoplasmosis
Population 1
The diagnosis of TO was confirmed in five patients (2.8%), based on a positive comparative WB. The average age of the patients was 33± 13 years. There were three male and two female patients. All were from the ophthalmology department. Decreased visual acuity and ocular pain were the main motives for consultation.Regarding their serological profile, one patient had a primary toxoplasma infection, the others were immune to toxoplasmosis. Clinically, three patients had panuveitis (Figure 1), and two anterior uveitis (Table 1). Patients were prescribed pyrimethamine sulfadiazine combined with systemic corticosteroids to reduce peri-lesional edema, with good progression under treatment.
Table 1: Characteristics of patients with ocular toxoplasmosis
| Patient | Age (yearsold) | Gender | Motive for consultation | Clinical manifestation | Fundus of the eye | Angiography | Optical coherence tomography |
| Patient 1 | 43 | female | Visual blur, Eye pain | Panuveitis granulomatous | Retro corneal precipitates in lower sheep fat, with an atrophic-pigmented retinal focus and a satellite focus | Scar lesion, bordered by an active lesion | hypodensity between the neuroretina and the pigment epithelium with hyperdense material within the hypodensity in connection with a retinal serous detachment |
| Patient 2 | 14 | female | Visual blur, decreased visual acuity in the right eye | Panuveitis | macular focus complicated by macular edema with serous retinal detachment | hypofluorescent central retinal focus with late diffusion related to macular edema |
/ |
| Patient 3 | 50 | Male | Eye pain | Anterior uveitis | / | / | / |
| Patient 4 | 33 | Male | Eye pain | Anterior uveitis | / | / | / |
| Patient 5 | 25 | Male | Eye pain | Panuveitis | Macular retinal focus and macular edema | / | / |
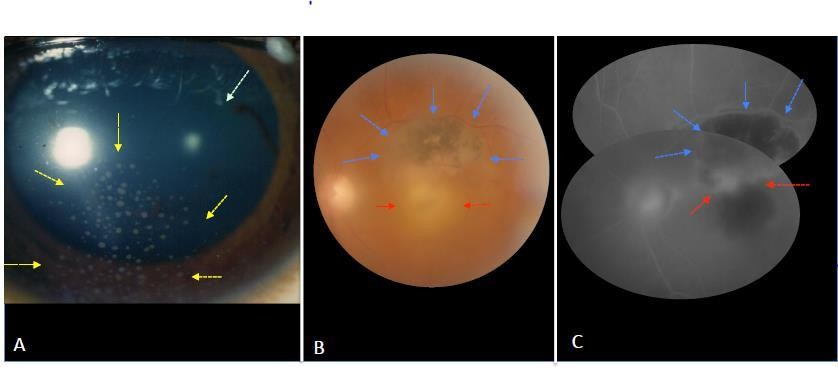
Figure 1: Unilateral granulomatous toxoplasmic panuveitis in an immunocompetent patient
(A): Color photograph of the eye: mutton fat keratic precipitates (yellow arrows), posterior synechia at 2 O’clock clearly visible in dilated pupil (green arrow).
(B): Color fundus photograph: a dense hyalite making the fundus blurry. A typical superomacular retinal lesion: an atropho-pigmentary inactive lesion (blue arrows), and below, active lesion with blurred border (red arrows).
(C): Fluorescein angiogram: hypofluorescent scar lesion without leackage (blue arrows), and below, active lesion with hypo and hyperfluorescence with staining and leackage(red arrows).
Photos taken in the ophthalmology department of Charles Nicolle Hospital. Tunis)
Population 2
Ophthalmologic follow-up of five babies during their first year of life (one baby lost at six months of age) revealed chorioretinitis in only one baby. The diagnosis of TC was made antenatally by the positivity of the conventional PCR for toxoplasmic DNA and confirmed at day 10 of life by the comparative The fundus showed an upper temporal retinal focus in the right eye with atrophic retinitis pigmentosa. A trans-fontanellar ultrasound done at the seventh day of life showed a cystic formation of the frontal horn of the left lateral ventricle. The baby was put under antiparasitic treatment with Adiazine-Malocide and folinic acid at the age of six months (due to the unavailability of these molecules in Tunisia).
Discussion
For long time, OT was considered as a late revelation of CT.Nowadays, it is currently admitted that ocular involvement during toxoplasmosis can be acquired and can be seen as well in the immunocompromised subject as in the immunocompetent. In our population, the diagnosis was confirmed in six cases. Their respective ages were seven days, 14, 25, 33, 43 and 50 years old.
TO occurs more frequently between the second and fourth decade of life. Indeed, a study conducted in a university hospital department in Tunisia on 60 cases of TO reported an average age of 25 years [5]. Bosch-Driessen et al concluded that among 274 episodes of active TO, 78% were discovered in patients aged between 15 and 45 years with a mean age of 31.1 years [6].
Thus, it appears that TO is a disease of the young subject. Is it a postnatal acquired TO or of congenital origin given the young age of the patients? This question remains unanswered because we do not have the history of these patients regarding the follow-up of the pregnancy of their mothers. The occurrence of ocular involvement after toxoplasmosis could be explained by infestation with virulent genotype T. gondii strains.
Toxoplasmosis is the most frequent etiology of posterior uveitis in immunocompetent subjects. The frequency of ocular toxoplasmosis found in this series is 2.8%. It is comparable with a study conducted at the regional university hospital of Nancy between January 2005 and December 2016 on a sample of 690 patients with uveitis [7]. Our resultsare significantly lower than the study in Kinshasa conducted over a 3-year period where OT presented 25.1% of uveitis cases. In other African series, it is found in 34% to 58% of patients consulting for uveitis [8]. In studies carried out in Europe and the USA, toxoplasmosis is reported to be responsible for 4 to 8% of patients consulting ophthalmology departments for uveitis [9]. Another study conducted in Tunisia between September 2003 and October 2009 reported a percentage of 10.2 of all uveitis cases [10]. A disparity between these different frequencies could be explained by the patient’s inclusion criteria. Indeed, in our study, the prevalence could be underestimated since we only collected cases of TO confirmed by serology. The diagnosis of ocular toxoplasmosis is essentially clinical [11], without having recourse to puncture of the aqueous humor or the vitreous, a procedure that is not considered innocuous. Typically, OT is responsible for active, whitish, edematous retinochoroiditis lesions, which can be distinguished from cicatricial, pigmented or atrophic lesions. Active lesions lead to contiguous hyalitis and sometimes granulomatous anterior uveitis of variable intensity [12]. The association of a scarring lesion with the evolving focus is in favor of recurrent ocular toxoplasmosis, in favor of toxoplasmosis of congenital origin[6]. The discovery of retinal involvement is either fortuitous or occurs with visual symptoms such as myodesopsia, visual blur or decreased visual acuity.
However, atypical forms presenting as focal involvement or optic neuropathy may be confused with other differential diagnoses. Diagnostic confirmation is crucial because chorioretinal foci may be located in the macula. Hence, the use of biological diagnosis withinthe immunocompetent patients, is based on toxoplasmic serology [13]. It is also applied for cases of ocular damage resistant to presumptive treatment.
In our study, it was not posterior uveitis, the most frequent form of TO, but rather panuveitis in three cases and anterior uveitis in two other cases. This led to the use of serology to confirm of the suspected OT.
First-line treatment is based on pyrimethamine and sulfadiazine. Combined with antiparasitic treatment, corticosteroid therapy is primarily aimed at reducing perilesional edema. Selection of the treatment for active TO depend on the location of the lesions. Today, no cysticide molecule has been approved for the treatment of TO, which explains the frequency of recurrence [14]. Our patients were treated with pyrimethamine sulfadiazine combined with systemic corticosteroids, with good progression under treatment.
In this study, we have included six cases of CT. Fundus monitoring up to 1 year of age revealed a superior temporal retinal focus in the right eye in one infant.
Of the six cases, one infant was lost to follow-up. All babies had good neurological and psychomotor development. A similar study conducted at the Pasteur Institute found that 3 out of 11 babies with CT developed TO [15]. In fact, It is currently admitted that the prognosis of congenital toxoplasmosis is primarily ocular [16].
Indeed, 80% of newborns who acquired the infection during fetal life are asymptomatic at birth. However, according to several studies, 85% of these babies will later develop one or more sequelae, mainly chorioretinitis [17, 18]. Ophthalmic damage occurs regardless of the date of maternal infection and presents a risk of recurrence and disruption of cognitive performance, hence the need for rigorous monitoring during the first month of life, then every three months until one year of age, then every six months until two years of age and once a year until puberty [19]. Strabismus, microphthalmia, cataract, retinal detachment, glaucoma, nystagmus and optic atrophy can all be seen in a TO [20].
Our paper is the only study in Tunisia focused on TO, that covered two distinct centers located in different regions of the country (the North and the Sahel), in order to collect a substantial number of patients. However, it is a retrospective study and does not reflect the true prevalence of TO because the diagnosis was made on the basis of serological confirmation, without taking into account cases diagnosed by ophthalmological examinations in the ophthalmology departments.
CONCLUSION
TO was identified in six cases, among the included populations. Therefore, we canconclude that prevention from toxoplasmosis is important, through conducting systematic screening of pregnant women for toxoplasmosis,as well as planning a close follow-up of at-risk babies to avoid potential visual complications that may occur even in adulthood.
Conflict of interest: None reported
A better understanding of the mechanisms of this disease is necessary to better adapt preventive methods and therapeutic strategies.
REFERENCES
- Sauer A, Villard O, Bourcier T, Speeg-Schatz C, Candolfi E. Toxoplasmose oculaire : de la physiopathologie au diagnostic microbiologique. JFr Ophtalmol 2013;36(1):76‑ 81.
- Montoya J, Liesenfeld O. Toxoplasmosis. The Lancet 2004;363(9425):1965‑ 76.
- Nsiangani Lusambo N, Kaimbo Wa Kaimbo D. Profil clinique et épidémiologique de la toxoplasmose oculaire à Kinshasa. JFrOphtalmol2019;42(8):900‑ 6.
- Rachdi I, Hajjam N, Aydi Z, Daoud F, Ben Dhaou B, Boussema F. Toxoplasmose oculaire chez un immunocompétent. La PresseMédicale 2018;47(5):480‑ 2.
- Stanford MR. Reliability of expert interpretation of retinal photographs for the diagnosis of toxoplasma retinochoroiditis. Br Jof Ophthalmol 2002;86(6):636‑ 9.
- Bosch-Driessen LEH, Berendschot TTJM, Ongkosuwito JV, Rothova A. Ocular toxoplasmosis. Ophthalmology 2002;109(5):869‑ 78.
- Robert-Gangneux F, Dardé ML. Epidemiology of and Diagnostic Strategies for Toxoplasmosis. ClinMicrobiolRev 2012;25(2):264‑ 96.
- Villard O, Cimon B, L’Ollivier C, Fricker-Hidalgo H, Godineau N, Houze S, et al. Help in the Choice of Automated or Semiautomated Immunoassays for Serological Diagnosis of Toxoplasmosis: Evaluation of Nine Immunoassays by the French National Reference Center for Toxoplasmosis. J Clin Microbiol 2016;54(12):3034‑ 42.
- Bonfioli AA, Orefice F. Toxoplasmosis. SeminOphthalmol 2005;20(3):129‑ 41.
- Villard O, Filisetti D, Roch-Deries F, Garweg J, Flament J, Candolfi E. Comparison of Enzyme-Linked Immunosorbent Assay, Immunoblotting, and PCR for Diagnosis of Toxoplasmic Chorioretinitis. J Clin Microbiol 2003;41(8):3537‑ 41.
- Neiter E, Conart JB, Baumann C, Rousseau H, Zuily S, Angioi-Duprez K. Caractéristiques épidémiologiques et étiologiques des uvéites dans un centre hospitalier universitaire. JFr Ophtalmol 2019;42(8):844‑ 51.
- Ronday MJ, Stilma JS, Barbe RF, McElroy WJ, Luyendijk L, Kolk AH, et al. Aetiology of uveitis in Sierra Leone, west Africa. Br J of Ophthalmol 1996;80(11):956‑ 61.
- Maenz M, Schlüter D, Liesenfeld O, Schares G, Gross U, Pleyer U. Ocular toxoplasmosis past, present and new aspects of an old disease. ProgRetin Eye Res2014;39:77‑ 106.
- Delair E, Brézin A.P. Toxoplasmose oculaire. Encycl Med Chir. (Elsevier Masson, Paris). Les uvéites, 2010.
- Ben Abdallah R, Aoun K, Siala E, Souissi O, Maatoug R, Hlioui S, et al. La toxoplasmose congénitale en Tunisie : analyse clinique et biologique de 11 cas. Archives de Pédiatrie 2009;16(2):118‑ 21.
- Robert-Gangneux F, Dion S. Toxoplasmose de la femme enceinte. J Pediatr Pueric 2020;33:209-20.
- Mets MB, Holfels E, Boyer KM, Swisher CN, Roizen N, Stein L, et al. Eye Manifestations of Congenital Toxoplasmosis. Am Journal Ophthalmol 1997;123(1):1‑ 16.
- Kieffer F, Wallon M, Garcia P, Thulliez P, Peyron F, Franck J. Risk factors for retinochoroiditis during the first 2 years of life in infants with treated congenital toxoplasmosis. Pediatr Infect Dis J 2008;27:27-32.
- Roizen N, Kasza K, Karrison T, Mets M, Noble AG, Boyer K, et al. Impact of Visual Impairment on Measures of Cognitive Function for Children With Congenital Toxoplasmosis: Implications for Compensatory Intervention Strategies. Pediatrics 2006;118(2):e379‑ 90.
- Rorman E, Zamir C, Rilkis I, Bendavid H. Congenital toxoplasmosis—prenatal aspects of Toxoplasma gondii infection. Reprod Toxicol 2006;21(4):458‑ 72.
Figure Click here to access/download; Figure; figure 1.docx
- Color photograph of the eye: mutton fat keratic precipitates (yellow arrows), posterior synechia at 2 O’clock clearly visible in dilated pupil (green arrow).
- Color fundus photograph: a dense hyalite making the fundus blurry. A typical superomacular retinal lesion: an at ropho-pigmentary inactive lesion (blue arrows), and below, active lesion with blurred border (red arrows).
- Fluorescein angiogram: hypo fluorescent scar lesion without leackage (blue arrows), and below, active lesion with hypo and hyper fluorescence with staining and leackage (red arrows).
Photos taken in the ophthalmology department of Charles Nicolle Hospital. Tunis)