
Organizational Citizenship Behavior and Workplace Incivility towards Performance of Nurses: A Mixed Method Analysis
- Malou C. Contridas
- Resty L. Picardo
- 1187-1238
- Mar 25, 2025
- Corporate
Organizational Citizenship Behavior and Workplace Incivility towards Performance of Nurses: A Mixed Method Analysis
Malou C. Contridas, RN, MANM; Resty L. Picardo, DM, JD, MAN
College of Allied Health Sciences, University of the Visayas
DOI: https://doi.org/10.51244/IJRSI.2025.12020095
Received: 21 February 2025; Accepted: 24 February 2025; Published: 25 March 2025
ABSTRACT
For nurses to deliver better performance, workplace incivility should be low and organizational citizenship behavior should be high. There appears to be a scarcity of studies where convergent parallel design was used and finding the interrelationship among organizational citizenship behavior, workplace incivility, and work performance of nurses. This convergent parallel research design was used to assess the interrelationship among organizational citizenship behavior, workplace incivility, and work performance and explored the relevant experiences of nurses in Ormoc District hospital, Leyte for the year 2024. Findings revealed that the organizational citizenship behavior was high. Qualitative data on organizational citizenship converges with the quantitative data where organizational citizenship behavior pertaining to exceeding beyond one’s job description or going above and beyond, being friendly, virtuous, having a helping attitude and collaborative skills, and the importance of role modelling. The general, nurse, supervisor, and physician incivilities were low while the patient/visitor incivility was moderate. Overall, the workplace incivility was low. Qualitative data on workplace incivility also converges with the qualitative data where there was no incivility experienced by some, the presence of gossip, patient incivility, co-worker incivility, and physician incivility on few occasions only which converges with the low workplace incivility. Task and contextual performance were rated as high while counterproductive work behavior was very low. Quantitative data on work performance converges with the qualitative data where work performance is also characterized by having time management, being effective and efficient, giving one’s best, possessing problem-solving and leadership skills, having a healthy environment as a factor to good performance, learning from co-workers, having a good and very satisfactory performance. Organizational citizenship behavior was correlated with overall workplace incivility. Overall workplace incivility was not correlated with task and contextual performance but was correlated with counterproductive work behavior. Organizational citizenship behavior was correlated with task and contextual performance. In order to address the findings of the study, a performance sustenance plan was proposed.
Keywords: Convergent parallel, Organizational citizenship behavior, Nurses, Work performance; Workplace incivility.
INTRODUCTION
Organizational citizenship behavior, nursing incivility, and work performance are a few measures that can impact nurses’ performance. Organizational citizenship behavior for example has the potential to improve teamwork, problem-solving, and information sharing, which can ultimately lead to higher quality work outcomes, improved customer service, and increased organizational effectiveness. Nursing incivility on the other hand, produces a severe disruption in the delivery of high-quality patient care, which has a detrimental effect on both patient safety and patient outcomes. Lastly, those nurses who are content with their professions are able to carry out their responsibilities effectively, result in higher levels of productivity, and deliver high-quality care. The importance of organizational citizenship behavior of nurses cannot be denied, in the study by Özlük and Baykal (2020), it was determined that organizational citizenship behavior levels of nurses were high. It was determined that the nurses demonstrated the highest organizational citizenship behavior with regard to conscientiousness, and they demonstrated the lowest organizational citizenship behavior with regard to courtesy. It was determined that organizational citizenship behavior had a significant positive relationship with organizational trust and job satisfaction.
Workplace incivility (WPI) on the other hand is a significant problem in healthcare centres, disturbing not only the clinicians enduring the negative behaviors but also the care that is delivered under the shadow of incivility (Kodjebacheva, 2014). Hutton and Gates (2018) stated that “incivility is characteristically rude and disrespectful, revealing a lack of respect for others. Lastly, Individual work performance (IWP) is defined as “employee behaviors or actions that are relevant to the goals of the organization” (Campbell, 1990 as cited in Koopmans et al. (2014), is an important outcome measure in studies in the workplace. The dimensions – task, contextual, and adaptive performance and counterproductive work behavior – are reflected in the literature on job performance in healthcare. Adaptive performance and counterproductive work behavior appear to be under-researched. The studies were conducted in different healthcare organizations and pertain to a variety of healthcare professionals. Organizations can affect job performance on the macro-, meso-, and micro-level to achieve transformation and improvement (Krijgsheld et al., 2022).
Based on experience of the researcher in the hospital, organizational citizenship behavior is not one aspect that nurses are not very concerned of nurses are very much focused on caring for patients that this concept is somewhat unfamiliar to them. Such behaviors are actually being done by nurses but without knowing that these behaviors are important in gaining teamwork, problem-solving, and sharing information. It is thus, important that nurses should gain awareness of these behaviors for them to cultivate it and achieve better and positive outcomes. Nursing incivility on the other hand is a common experience by nurses. Nurses are sometimes exposed to a hostile climate which may be brought about by everyone being so busy at work. Sometimes nurses are victims of inappropriate jokes from their co-nurses or from the physicians or other health and non-health care professionals. Lastly, nurses experiences incivility from their patients as they lack respect for nurses which may be contributed to their conditions. It is also important that baseline information about incivility should be determined so that appropriate measures can be undertaken. Lastly, on work performance, though nurses are being periodically evaluated based on their performance. The tool is one that is only developed by the hospital. There is a need to standardize the tool and to make sure that performance evaluation is not just done for the sake of evaluation but should also be used for salary increase for example. All these observations support the need to conduct the study as there is an empirical gap.
The study delves into assessing the interrelationship among organizational citizenship behavior, nursing incivility, and work performance. The assessment of the interrelationship among the variables is identified to be the methodological gap of the study. While there are studies already available in the international arena, none had been done at the micro-level. Also, the experiences of the participants will be looked into whether the data converges with the quantitative data as the experiences are actual encounters which can validate the quantitative findings, making the findings of the study more trustworthy.
The effects of organizational citizenship behavior, nursing incivility, and work performance will redound to the patients which has an impact on their well-being and health. Thus, this study is aligned with the third sustainable developmental goals on good health and well-being. It is also the intention of the researcher to create a performance enhancement plan as a means of addressing the gap. This plan will greatly help nursing administrators gain better organizational behavior, resolving incivilities, and gaining high work performance for their nurses which in turns yields positive effects to patient outcomes.
RESEARCH OBJECTIVES
The main purpose of the study was to assess the interrelationship among organizational citizenship behavior, workplace incivility, and work performance and further explore the relevant experiences of nurses in Ormoc District hospital, Leyte for the year 2024.
Specifically, the study answered the following queries:
1. What was the organizational citizenship behavior of the nurses?
2. What was the nursing incivility of the nurses in terms of:
2.1 general;
2.1.1 hostile climate;
2.1.2 inappropriate jokes; and
2.1.3 inconsiderate behavior.
2.2 nurse;
2.2.1 hostile climate;
2.2.2 gossip and rumors; and
2.2.3 free-riding.
2.3 supervisor;
2.3.1 abusive supervision; and
2.3.2 lack of respect.
2.4 physician;
2.4.1 abusive supervision; and
2.4.2 lack of respect.
2.5 patient;
2.5.1 lack of respect; and
2.5.2 displaced frustration?
3. What was the work performance of the nurses in terms of:
3.1 task performance
3.2 contextual performance; and
3.3 counterproductive work behavior?
4. Was there a significant relationship between:
4.1 organizational citizenship behavior and nursing incivility;
4.2 nursing incivility and work performance; and
4.3 organizational citizenship behavior and work performance?
5. How did the participants describe their experiences on organizational citizenship behavior, nursing incivility, work performance?
6. How did the experiences relate with the quantitative findings?
7. What performance enhancement plan was proposed based on the findings of the study?
Statement of Null Hypotheses
Ho1: There was no significant relationship between organizational citizenship behavior and nursing incivility.
Ho2: There was no significant relationship between nursing incivility and work performance.
Ho3: There was no significant relationship between organizational citizenship behavior and work performance.
REVIEW OF RELATED LITERATURE AND STUDIES
Organizational Citizenship Behavior (OCB). In the study of Alabbas et al. (2023) nurses had an overall high level of OCB and high mean scores for all dimensions. However, the highest weighted mean was for courtesy, with a mean percentage of 82.63 percent, while the lowest was for civic virtue, with a mean percentage of 70.86 percent. Furthermore, nurses’ OCB levels differ significantly according to their nationalities and years of experience. One of the most studied organizational performance research subjects in recent years and one of the fundamental issues in organizational behavior is organizational citizenship behavior (OCB) which enhances efficiency, increases productivity, reinforces teamwork, and cooperation within the organization, decreases the costs of errors, and, in general, maintains a good environment in the workplace (Chib, 2016).
An employee with a high OCB level will support his/her co-workers and work to his/her maximum potential to achieve organizational goals and help the organization deal with change and unexpected circumstances, which is one reason for the organization’s success (Sinha & Negi, 2019). In the study of Zeng et al. (2023), nurses’ psychological capital, organizational commitment and organizational citizenship behavior scores were in the upper-middle level. Additionally, organizational commitment partially mediates between psychological capital and organizational citizenship behavior. According to the study of Hossain (2020), organizational citizenship behavior becomes one of the significant factors that enhance the organizational efficiency. Organizational citizenship behavior has been defined as behaviors that an employee voluntarily engages in organization that promote the effectiveness of clearly rewarded by the organization. There were statistically positive significant relationships between organizational citizenship behavior with organizational commitment, organizational citizenship behavior with working ward and organizational commitment with working ward. Based on the results of this study, it is indicated that lack of OCB & OC among nurses’ is moderate level. The findings of this study will suggest reducing organizational hazard, and developing citizenship behavior and organizational commitment that enhance high outcome in health care organizations and quality of care.
The data analysis of Khajoei et al. (2024) revealed the nurses’ experiences of OCB under nine subcategories and three main categories, including (i) “helping behavior”, comprised of four subcategories of helping colleagues at work, helping colleagues outside of work, boosting morale, and creating a culture of support and appreciation, (ii) “extra-role behavior” with two subcategories of cooperation in advancing tasks, and creativity and efforts to promote services, and (iii) “contribution to professional growth and development”, consisting of two subcategories of individual professional development and support for colleagues’ professional development. The findings of the study of Nanang AS et al. (2021) indicated that transformational leadership did not significantly affect organizational citizenship behavior, but this has substantial implications for learning culture and job satisfaction. Both learning culture and job satisfaction significantly and positively predict organizational citizenship behavior. In addition, learning culture and job satisfaction act as perfect mediators between transformational leadership and organizational citizenship behavior. This study suggests leaders to maximize a systematic learning program and to pay attention to the nurses’ job satisfaction rate to improve organizational citizenship behavior.
Nursing Incivility. In the study of Keller et al. (2020), results were mostly inconsistent regarding individual characteristics of targets of incivilities (e.g., age, gender, ethnicity), but less experienced healthcare professionals were more exposed to incivility. In most studies, participants reported experiencing incivilities mainly within their own professional discipline (e.g., nurse to nurse) rather than across disciplines (e.g., physician to nurse). Evidence of specific medical specialties particularly affected by incivility was poor, with surgery as one of the most cited uncivil specialties. Finally, situational and cultural predictors of higher incivility levels included high workload, communication or coordination issues, patient safety concerns, lack of support and poor leadership.
In the study of Abdollahzadeh et al. (2017) data analysis revealed 417 codes, ten categories, three subthemes and one theme, that is, A Need for a Comprehensive Attempt. Attempt of organization, nurses, and public as subthemes are needed to prevent workplace incivility. The findings of the study indicated that a comprehensive and systematic attempt was needed to prevent incivility. Nurses should try to improve their skills; officials should try to show the real image and position of nurses and hospitals to the community. According to the study of Woo and Kim (2020), workplace incivility was negatively associated with compassion competence of nurses. Furthermore, psychological capital had a conditional moderating effect on the relationship between workplace incivility and nurses’ compassion competence. The negative associations of workplace incivility with compassion competence were significant at low and medium levels of psychological capital but not at high psychological capital. Moreover, the association was stronger for those with low psychological capital. Workplace incivility is negatively associated with compassion competence among nurses, and psychological capital has conditional moderating effects in its relationship.
Also in the study of Armstrong (2018), workplace incivility is a well-documented issue in nursing in the health care setting. It has the potential to cause emotional and physical distress in victims and potentially affects the quality of care provided. The purpose of this study was to critique and summarize the most recent, available evidence related to interventions in assisting nursing staff working in health care settings in managing incivility. This systematic review of literature yielded 10 studies meeting the criteria. The studies were mostly identified as lower quality research. Despite the lower quality of research, the collection of evidence suggests the use of a combination of educational training about workplace incivility, training about effective responses to uncivil workplace behaviors, and active learning activities to practice newly learned communication skills, in assisting nurses in improving their ability to manage incivility in the workplace. Workplace incivility and bullying were significantly related to authentic leadership, structural empowerment, worklife fit, and psychological capital. Bullying was more strongly related to job satisfaction, emotional exhaustion, and mental and physical health outcomes than supervisor and co-worker incivility. New graduate nurses’ experiences of 3 types of workplace mistreatment are related to organizational and health factors, although bullying appears to have stronger negative effects (Read & Laschinger, 2013).
In the study of Alquwez (2020), the highest mean score was recorded for patient or visitor incivility, whereas the lowest score was recorded for supervisor incivility. Regarding patient safety competence, the dimension “communicating effectively” received the highest mean score, whereas “working in teams with other health professionals” was rated lowest. General and nurse incivilities had multivariate effects on the six dimensions of patient safety competence. Nurses’ experiences of uncivil acts from nurses and from general incivility negatively impact nurses’ patient safety competence. The results indicated that nurses did have experiences with incivility at the facility with the sources being identified as General Hostile Climate, Nurse Gossip and Rumors, Physician Abusive Supervision and Patient and Visitor Displaced (Gillian, 2015).
Sources of Workplace Incivility. In developing an incivility measure for nurses it is important that the scale address the number of sources from whom nurses commonly experience incivility. Previous research has found that uncivil behavior is likely to differ according to the instigator (Jackson, Clare, & Mannix, 2002 as cited in Guidroz et al., 2010; Nabb, 2000 as cited in Guidroz et al., 2010). Verbal abuse by a physician, for example, may affect nurses differently than verbal abuse by a patient. We were particularly interested in measuring nurses’ experiences of incivility with physicians, nurse supervisors, other nurses, and patients as distinct experiences. In the following section, we review research conducted both within and outside of hospital settings by the source of incivility (Guidroz et al., 2010).
Incivility from Physicians. Poor working relationships between nurses and physicians are a long observed and widely researched topic in nursing and medicine (Faigin, 1992 as cited in Guidroz et al., 2010; Porter, 1991 as cited in Guidroz et al., 2010; Sirota, 2007 as cited in Guidroz et al., 2010; Stein, 1967 as cited in Guidroz et al., 2010; Stein et al., 1990 as cited in Guidroz et al., 2010). Poor nurse–physician relationships are often attributed to inappropriate, disruptive, or abusive behavior by physicians (Rosenstein & O’Daniel, 2005 as cited in Guidroz et al., 2010); physicians holding dismissive attitudes toward nurses (Faigin, 1992 as cited in Guidroz et al., 2010; Rosenstein, 2002 as cited in Guidroz et al., 2010); power and gender issues in the workplace (Porter, 1991 as cited in Guidroz et al., 2010; Zelek & Phillips, 2003 as cited in Guidroz et al., 2010); and communication and collaboration issues (Leonard et al., 2004 as cited in Guidroz et al., 2010; Sirota, 2007 as cited in Guidroz et al., 2010). Although the reasons are numerous, the negative outcomes for nurses when nurses and physicians have poor working relationships are significant. Rosenstein and O’Daniel (2002, 2005) as cited in Guidroz et al. (2010) have shown that mistreatment by a physician was negatively related to job satisfaction and positively related to work distress and turnover intentions. Hillhouse and Adler (1997) as cited in Guidroz et al. (2010) found in their research that physician and co-worker conflict was equally common, however, physician conflict was associated with more severe psychological distress.
Incivility from Supervisors. Interpersonal mistreatment received from a figure higher in the organizational hierarchy is common within workplaces. In a survey of nearly 1,200 public sector employees, Cortina and colleagues (2001) as cited in Guidroz et al. (2010) found that one-third of the most powerful individuals within the organization were the instigators of workplace incivility. Researchers (e.g., Frone, 2000 as cited in Guidroz et al., 2010; Tepper, 2000 as cited in Guidroz et al., 2010) have found that when people experience incivility from their supervisor this can result in lower commitment to the organization, low job satisfaction, high psychological distress, and stronger intentions to find another job. For example, Tepper (2000) as cited in Guidroz et al. (2010) found in a sample of employees from a wide variety of occupations and industries that those who reported more uncivil behavior from their supervisor also reported lower commitment to the organization, more dissatisfaction with their job, more psychological distress, and higher intentions to quit. Frone (2000) as cited in Guidroz et al. (2010) also found similar results; when participants experienced high levels of conflict with their supervisor they reported lower job satisfaction and organizational commitment, and higher intentions to quit (Guidroz et al., 2010).
Incivility from Other Nurses. Several researchers have found that mistreatment from co-workers can lead to psychological distress. Frone (2000) as cited in Guidroz et al. (2010) found that co-worker incivility led to feelings of depression, somatic symptoms, and low self-esteem. Within health care organizations this type of common low-level aggression has been well-documented in nursing samples and has been linked to both personal and organizational outcomes. Duffy (1995) as cited in Guidroz et al. (2010) coined the term horizontal aggression as the aggression experienced from one’s own coworkers and found this to be highly prevalent within hospitals. Horizontal aggression is particularly distressful for nurses (Farrell, 1997 as cited in Guidroz et al., 2010) and has been cited as the one form of workplace mistreatment that is most concerning to nurses (Farrell, 1998 as cited in Guidroz et al., 2010). McKenna et al. (2003) as cited in Guidroz et al. (2010) measured the frequency of horizontal aggression experienced by nurses during the first year of practice. Their research indicated that not only does horizontal aggression affect a high number of the respondents, it is also associated with increased absenteeism and thoughts about quitting the field of nursing all together (McKenna et al., 2003 as cited in Guidroz et al., 2010).
Incivility from Patients. Uncivil treatment from the patients one cares for is an additional source of workplace conflict that can result in negative effects on nurses. Outside of a health care setting, researchers have found that customer-related social stressors, such as verbal aggression or unusual customer demands, were significant predictors of burnout (Dormann & Zapf, 2004 as cited in Guidroz et al., 2010); decreased employees ability to regulate their emotions when dealing with subsequent, hostile customers (Grandey et al.,, 2004 as cited in Guidroz et al., 2010); and occurred more frequently than aggression with one’s co-workers or supervisor (Grandey et al., 2007 as cited in Guidroz et al., 2010). Within health care organizations the findings are similar. A recent hospital study found that the majority of nurses identified their patients as the main perpetrators of verbal or physical abuse (Farrell et al., 2006 as cited in Guidroz et al., 2010). This abuse influenced the severity of distress that nurses experienced, their overall productivity, and increased sentiments for withdrawing from the career of nursing. Additionally, researchers have found that nurses who receive high levels of verbal aggression from patients are more prone to experience emotional exhaustion and depersonalization, two of the components of burnout (Winstanley & Whittington, 2002 as cited in Guidroz et al., 2010).
Work Performance of Nurses. Within the field of occupational health, there is a focus on instruments that measure losses in individual work performance due to health complaints. These include for example the Stanford Presenteeism Scale (Koopman et al., 2002 as cited in Koopmans, 2014), Work Productivity and Activity Impairment questionnaire (Reilly, 1993 as cited in Koopmans, 2015), and the Health and Performance Questionnaire (Kessler et al., 2003 as cited in Koopmans, 2014). A loss in individual work performance due to health complaints is usually expressed as absenteeism (absence from work due to health complaints) or presenteeism (being present at work but ill). Absenteeism or presenteeism measures are then taken as proxies for losses in individual work performance. The question is, however, whether the equation of a loss in individual work performance with absenteeism or presenteeism is just.
As Johns (2010) pointed out in his review, a loss in individual work performance is a result of being absent, or of being present at work while ill, rather than the same thing. Also, within the field of occupational health, the terms of individual work performance and productivity are often used interchangeably. This is perhaps driven by the goal to relate losses in performance or productivity to costs, as productivity usually refers to objective output. The unclear definitions and content of the terms individual work performance, productivity, absenteeism, and presenteeism – and their interchangeable use – have resulted in a multitude of instruments with heterogeneous content. Also, many of these instruments are specifically developed for workers with health complaints. When applied to workers without health complaints, a pronounced ceiling effects in these scales is created. Therefore, these measures are unsuitable for a general, mostly healthy, working population (Koopmans, 2014).
Within the field of work and organizational psychology, defining the construct of individual work performance, and attempting to understand its underlying structure, has received much attention (Dalal, 2005 as cited in Koopmans, 2014). Traditionally, the focus has been on task performance, which can be defined as the proficiency with which individuals perform the core substantive or technical tasks central to his or her job (Campbell, 1990 as cited in Koopmans, 2014). More recently, there has been an increasing interest in discretionary, positive work behaviors that indirectly contribute to the goals of the organization. Various labels have been used for this type of behavior, such as organizational citizenship behavior, extra-role behavior, and contextual performance (LePine et al., 2002 as cited in Koopmans, 2014). Also, counterproductive work behaviors that harm the well-being of the organization have received attention (Rotundo & Sackett, 2002 as cited in Koopmans, 2014).
Numerous scales have also been developed to measure task performance (Williams & Anderson, 1991 as cited in Koopmans, 2014), contextual performance (Podsakoff & MacKenzie, 1989 as cited in Koopmans, 2014), or counterproductive work behavior (Bennett & Robinson, 2000 as cited in Koopmans, 2014). The multitude of scales in this research field is perhaps best illustrated by LePine et al., (2002) as cited in Koopmans (2014), who identified more than 40 different measures of contextual performance. However, heterogeneous content between scales measuring the same dimension, and overlapping content between scales measuring a different dimension, can be observed. Also, the scales are often developed based on a specific type of occupation, making these scales less suitable for use in a generic working population (Koopmans, 2014).
Within the field of management and economics, performance measurement mostly focuses on the company level, using key performance indicators such as employee turnover, customer satisfaction, and financial performance. Especially in the United States of America, performance measurement has taken off since President Clinton signed the National Performance Review Act in 1993. Within companies, human resource management has developed performance measurement systems to determine individual work performance. Thus, these performance measurement systems are often specific to the job or company. Also, human resource managers have drawn on research from work and organizational psychology to measure individual work performance (Den Hartog et al., 2004). The conceptualization of IWP has a long history, and many frameworks have been proposed to describe the construct domain of IWP. In the field of occupational health, for example, the main focus is on sickness absenteeism or presenteeism, i.e., work absence or losses in IWP due to health impairments. In the field of work and organizational psychology, traditionally, the main focus of the IWP construct has been on task performance, which can be defined as “the proficiency with which individuals perform the core substantive or technical tasks central to his or her job” (Campbell, 1990 as cited in Koopmans et al. (2014). It is now generally agreed upon that, in addition to task performance, the IWP domain consists of contextual performance and counterproductive work behavior (Viswesvaran & Ones, 2000 as cited in Koopmans et al., 2014; Rotundo & Sackett, 2002 as cited in Koopmans et al., 2014; Koopmans et al., 2011). Contextual performance can be defined as “behaviors that support the organizational, social and psychological environment in which the technical core must function” (Borman & Motowidlo, 1993 as cited in Koopmans et al., 2014). Counterproductive work behavior can be defined as “behavior that harms the well-being of the organization” (Rotundo & Sackett, 2002 as cited in Koopmans et al., 2014).
The results in the study of Umrani et al. (2019) indicated that job security and organizational support positively affected job performance of hospital physicians. Moreover, job satisfaction mediated the link between job security and job performance as well as between organizational support and job performance. Institutional stress was negatively related to job performance for hospital employees without managerial responsibilities. The motivational resources autonomy, competence development and social support partly mediated the relationship between institutional stress and job performance in the group of employees without managerial responsibilities. In the leader group, the motivational resources fully mediated the relationship between institutional stress and job performance. Social support from leaders had a non-significant influence on job performance in both groups (Bjaalid et al., 2020). The study of Abun et al. (2021) found that their self-efficacy is high and it affects the work performance specifically task and contextual work performance but no correlation with the counterproductive behavior. The study found that work environment affects self-efficacy and work performance along with the three dimensions such as task performance, contextual performance, and counterproductive work behavior. Therefore, the hypotheses of the study are accepted.
Why is individual work performance such a popular and interesting topic? Several trends in the labor market are responsible. First of all, individual work performance is important because of ongoing globalization of the economy. Economic globalization is the increasing economic integration and interdependence of national economies across the world through a rapid increase in cross-border movement of goods, service, technology, and capital (Joshi, 2009). As a result, competition between companies from all over the world increases. Therefore, it is essential for companies to maintain or improve their competitive ability. Individual work performance is one of the key indicators for team and company performance, and consequently, it contributes to the productivity and competitive ability of companies (Koopmans, 2014). Second, individual work performance is important in the light of the current economic recession. Recession refers broadly to “a period of reduced economic activity” (Merriam-Webster, 2022). It is characterized by a greater supply than demand in products, a drop in international trade, debts, bankruptcies, high unemployment rates, and low consumer confidence. Companies have to cut costs to stay afloat in these times of economic hardship, for example by employee reductions and/or outsourcing work to cheaper markets. Also, company employees will be encouraged to increase their individual work performance levels, in order to boost company performance and productivity. In addition, employees will tend to increase their individual work performance levels, in order to increase chances to survive possible reorganizations with reductions of personnel (Koopmans, 2014).
Third, individual work performance is important considering sustainable employability. The ‘grey wave’ in Europe means that there is an accelerated growth of the older working population and a decline in numbers of the younger working population. As a result, a scarcity of workers in the labor force threatens to arise (United Nations, 2008). Consequently, a shrinking number of workers will have to do the same – or an even larger – amount of work. Also, they will have to pay for the increasing costs associated with a growing elderly population, such as retirement pensions, social security, and health care (World Health Organization, 2009 as cited in Koopmans, 2014). It is therefore essential to improve the individual work performance of workers in the labor force. Also, the retirement age of workers will be increased in coming years, in order to prolong the stay of older workers in the work force (European Commission, 2010). This means that employees have to work at the same – or even higher – level of individual work performance, despite possible limitations caused by an older age, such as reduced health (Koopmans, 2014).
While the majority of nurses rated their job performance as good, it is important to note that a relevant proportion of nurses rated their job performance as poor. The findings of this study identified that nurses’ performance is influenced by several key factors, including workload, remuneration, rewards, objectives to be achieved, and feedback on performance appraisals (Daba et al., 2024). In the study of Dirdjo et al. (2023), majority of nurses are satisfied with their work, while just over half of nurses still have poor performance. This study has revealed a significant relationship between job satisfaction and the performance of nurses in the surgical treatment room with OR showing 6.188 meaning that nurses who are dissatisfied with their work have the opportunity to perform less well 6.2 times, when compared with nurses who are satisfied in their jobs. These results can be used by hospital nursing managers that in order to improve nurse performance they must consider the job satisfaction of their nurses. Participating nurses got average scores from the critical thinking and job performance scale and sub-scales, and there was a positive, mid-level and statistically significant correlation between the scale scores. According to the multiple linear regression analysis results, personal critical thinking, interpersonal and self-management critical thinking and the total critical thinking scores positively affected the job performance scores of nurses. As critical thinking predicts nurses’ job performance, managers of hospitals and nursing services should consider training programs or activities to increase nurses’ essential thinking competencies, thus improving clinical nurses’ performances (Ateş et al., 2023).
Results in the study of Ibrahim et al. (2023) revealed that majority of studied staff nurses had moderate level of perception toward work related stress and more than half of studied staff nurses had fair level of job performance. There was no statistically significant correlation between work related stress and job performance of the studied staff nurses. Establishing a committee represented from staff nurses that discuss nursing staff problems, continuing education programs for nurses should include topics about work related stress and its preventive measures to decrease its negative outcomes and Enhance job performance of nurses by creating and organizing training program on job performance as a managerial skill for head nurses to maintain improving patient care. The study of Doloh et al. (2023) revealed that the performances of the doctors and the nurses are especially important in accomplishing health care in a continuous and effective way. It is important to examine all organizational, individual, social factors that especially affect the performances of the doctors and nurses holistically. Work performance was affected by work satisfaction, work motivation, and supervision. Work performance was also indirectly affected by motivation. Finding of the study of Rastegari et al. (2010) showed that the most common kind of quality of working life in the nurses was moderate one. The most frequent nurses’ task performance was also related to the moderate performance. There was a direct and significant relationship between job performance and quality of working life in all the aspects. According to the research findings, it is important to consider the workplace and quality of working life of the nurses for improving productivity and performance of the nurses.
In a study made by Krijgsheld et al. (2022), the authors conclude that job performance in healthcare can be conceptualized into four dimensions: task, contextual and adaptive performance, and counterproductive work behavior. Generally, these dimensions correspond with the dimensions discussed in the job performance literature. This implies that these dimensions can be used for further research into job performance in healthcare. Many healthcare studies on job performance focus on two dimensions: task and contextual performance. However, adaptive performance, which is of great importance in constantly changing environments, is under-researched and should be examined further in future research. This also applies to counterproductive work behavior. To improve job performance, interventions are required on the macro-, meso-, and micro-levels, which relate to governance, leadership, and individual skills and characteristics.
Organizational Citizenship Behavior and Workplace Incivility. Multiple regression analyses revealed that workplace incivility (from supervisor and client) positively predicted workplace stress. At the same time, coworker incivility did not predict workplace stress. On the contrary, workplace incivility (supervisor, coworker, and clients) did not predict OCB significantly. JH and work self-efficacy positively predicted OCB, while PO negatively predicted OCB. This research provides new directions for future research that workplace stress is predicted by supervisor and client incivility, and OCB is not predicted by workplace incivility (Annalakshmi et al., 2022). The results of the study of Altuntas and Baykal (2010) showed that nurses had a higher than average level of trust in their managers and coworkers and they trusted more in their managers and coworkers than their institutions. The Organizational Citizenship Level Scale indicated that the behavior most frequently demonstrated by the nurses was conscientiousness, followed by courtesy and civic virtue, whereas sportsmanship was displayed to an average extent. An analysis of relationships between nurses’ level of organizational trust and their organizational citizenship behaviors revealed that nurses who trust in their managers, institutions, and coworkers demonstrated the organizational citizenship behaviors of conscientiousness, civic virtue, courtesy, and altruism more frequently.
According to the findings of the study of Mahmood et al. (2023), interpersonal deviance acts as a partial mediator between incivility shown by coworkers and supervisors and behavior that demonstrates organizational citizenship. In addition, the findings demonstrated that the perception of organizational support moderates the association between incivility shown by coworkers and supervisors and behavior that demonstrates organizational citizenship.
Workplace Incivility and Performance of Nurses. The study’s findings rejected hypotheses one and two showing workplace incivility (WPI) has a detrimental effect on employee engagement and employee performance (Singh et al., 2023). The results of the study of Saleem et al. (2022) affirmed that incivility is harmful to the performance of employees, and that trust in supervisors helps employees to perform well. The trust in the supervisor significantly mediates the incivility–performance relationship. Findings of the study of Aruoren and Ugbeghene (2023) revealed that workplace incivility was negatively related to both task and adaptive performance, but only significantly related to task performance. Furthermore, workplace incivility was found to be positively related to counterproductive work behavior and contextual performance, however, this relationship was only significant for counterproductive work behavior. Coworker incivility and customer incivility reduced work engagement and job performance. The effects of coworker incivility on the work engagement and job performance are greater than those of customer incivility. Furthermore, work engagement has a positive effect on the job performance (Wang & Chen, 2020).
Organizational Citizenship Behavior and Performance of Nurses. The results in the study of Triani et al. (2020) showed that organizational citizenship behavior has a positive and significant effect on employee performance. The results of study one revealed that occupational efficacy (OE) emerged as an antecedent of OCB in predicting performance. In study two, OCB positively predicted employee performance above and beyond and the effects of their managers’ tenure in position, and Collective Efficacies (CEs). In addition, both employees’ and managers’ CEs moderated the effects of OCB on performance: the performance effects of OCB increased as employees’ and managers’ CE increased, and specifically performance efficiency and performance creativity (Yaakobi & Weisberg, 2020).
The study of Abun et al. (2021) found that organizational citizenship, the work performance of employees and the work environment is high and there is a significant correlation between organizational citizenship behavior and work performance and there is a correlation between work environment and organizational citizenship behavior and work performance. Therefore, the hypothesis of the study is accepted. OCB on Employee Performance is related to task performance, organizational justice, job satisfaction, organizational performance, and organizational culture. OCB on Employee Performance is related to Task Performance, where OCB refers to voluntary behavior performed by employees outside of their official or formal duties. Meanwhile, employee performance can be divided into two main aspects: task performance and overall organizational performance. OCB can influence both organizational and individual contexts, improve teamwork by promoting a positive and supportive atmosphere in the workplace, and impact employees to complete their tasks correctly (Luthfiyana et al., 2024). Asgari et al. (2020) as cited in Luthfiyana et al. (2024) research showed organizational support plays a vital role in promoting task performance and OCB among secondary school teachers, providing insight for principals to design strategies for continuous quality improvement that will improve the Employee Performance of teachers. Tahir (2015) as cited in Luthfiyana et al. (2024) highlighted the importance of understanding the interaction between psychological empowerment, organizational citizenship behavior, and task performance to improve employee and organizational outcomes.
Synthesis
Literature and studies were one in emphasizing the importance of organizational citizenship behavior. Considering that nurses are the most important human resources in healthcare systems, organizational citizenship behavior (OCB) among nurses is of the utmost significance to both the quality of nursing care and the outcomes for patients. Nursing incivility on the other hand results in a major interruption in the provision of quality patient care, which in turn has a negative influence on both the welfare of patients and the outcomes they experience. Workplace morale, productivity, and job satisfaction are all negatively impacted by uncivil behavior, which also leads to an increase in employee turnover. Nursing work performance is a reflection of the quality of care that is provided to patients and, as a result, the outcomes for those patients. Poor job performance is considered a risk factor from the perspective of patient safety. While the literature and studies emphasized the importance of the three variables as independent variables, there appears to be a lack of studies on assessing the interrelationship of the three variables especially at the local level. Thus, the conduct of this study.
RESEARCH METHODOLOGY
Design
This mixed method research design utilized the convergent parallel design where the quantitative design utilized the descriptive, correlational research design and the descriptive qualitative design will be used. The descriptive design was used in determining the organizational citizenship behavior, nursing incivility, and work performance of the nurses. The correlational design was used in assessing the interrelationship among organizational citizenship behavior, nursing incivility, and work performance of the nurses. The descriptive qualitative design was used also in the study to explore the experiences of the nurses on organizational citizenship behavior, nursing incivility, and work performance. This will be done to converge the findings of the quantitative design.
Environment
The study was conducted in Ormoc District Hospital. It is a Level 1 government hospital situated in Ormoc City, Leyte.
Participants
Participants of the study were the 61 nurses of the hospital.
Sampling Design. A complete enumeration was done where, those who qualify based on the inclusion and exclusion criteria were invited to participate in the study for the quantitative part of the study. Purposive sampling was used for the qualitative part of the study. There were 10 informants for the qualitative aspect of the study.
Inclusion Criteria. For one to be included in the study they had to be nurses and connected with Ormoc District Hospital regardless of age, sex, socio-economic status, employment status, and educational attainment, and religion, Respondents must be willing to provide voluntary consent to participate in the study. For the qualitative aspect, similar inclusion criteria applied and should have been connected with the hospital for at least one year already.
Exclusion Criteria. Excluded in the study were those holding managerial positions such as nurse supervisors and the chief nurse. Excluded further were those who are just hired and had not been with the hospital for at least 3 months already. Furthermore, those who had submitted their resignation letters and retirement intentions are also excluded from the study. For the qualitative aspect of the study, similar exclusion criteria applied.
Instruments
The study made use of adopted questionnaires. Part one of the questionnaire is the Organizational Citizenship Behavior Checklist (OCB-C) by Fox and Spector (2011). It is a 20-item questionnaire. The OCB-C uses a 5-point frequency scale ranging from 1 = Never to 5 = Every day. Scores are computed by summing responses across items. A total score is the sum of responses to all items. Subscale scores are the sum of items within each subscale. The OCB-C is a causal indicator scale that consists of items that are not all parallel assessments of a single underlying construct. For such scales items are not necessarily expected to be highly related and thus internal consistent reliability is not a good indicator of reliability (Bollen & Lennox, 1991; Edwards & Bagozzi, 2000). Fox et al. (2009) reported coefficient alphas for the 20-item version of the OCB-C of .89 and .94 for two self-report samples, and .94 for a coworker sample (coworkers reporting on the target employee). Parametric score and interpretations are as follows: 20 to 36 is very low, 37 to 52 is low, 53 to 68 is moderate, 69 to 84 is high, and 85 to 100 is very high.
Part two of the instrument was the nursing incivility scale (NIS) by Guidroz et al. (2010). The instrument is composed of 43 items which are divided into five sources of incivility (General, Nurse, Supervisor, Physician, and Patient). Specifically, the General Incivility scale contains three subscales, each with three items (total of nine items). The three subscales of the General Incivility factor include Hostile Climate (e.g., do employees raise their voices when frustrated or blame others for mistakes?), Inappropriate Jokes (e.g., people making jokes about minority, religious groups), and Inconsiderate Behavior (e.g., taking things without asking, talking too loudly). The second source of incivility, Nurse Incivility, contains 10 items divided into three subscales. These subscales are Hostile Climate (e.g., nurses arguing frequently or screaming at each other), Gossip and Rumors (e.g., nurses gossiping about each other, spreading rumors), and Free-riding (e.g., nurses claiming credit for others work).
The Supervisor and Physician factors each contain seven items, which are divided into two subscales. All of the Supervisor and Physician items are identical and only differ by the source of incivility that is referred to in the question. The subscales for these two factors are Abusive Supervision (e.g., verbally abusive) and Lack of Respect (e.g., treats nurse as if time is not important). Finally, the Patient Incivility scale contains 10 items divided into two subscales: Lack of Respect (e.g., does not trust information from a nurse, is condescending) and Displaced Frustration (e.g., treats nurses as if they were inferior or stupid, takes frustrations out on nurses). It is important to note that although the Supervisor, Physician, and Patient incivility factors share a subscale by the same name (e.g., Lack of Respect), the Patient Incivility Lack of Respect items are entirely different from the items on the Supervisor and Physician Incivility scales. The NIS can be administered via paper and pencil or through an electronic survey platform. Within the instructions respondents are prompted as to which source of incivility they should consider when responding to the item and asked to consider how much they agree with the statement. Agreement is made on a 5-point Likert-type scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree).
Scoring of the NIS is best done at the source level. Items from the subscales can be averaged together to create a subscore (e.g., average Nurses’ Hostile Climate subscale), to glean more specific information for targeting interventions. But the source-level may be an ideal scoring method for understanding source-specific differences in incivility. Reliability testing results revealed the following Cronbach alpha values: General Incivility is .85, Inappropriate Jokes is .92, Hostility and Rudeness is .81, Nurse Incivility is .89, Inconsiderate Behavior is .87, Gossip and Rumors is .88, Free-riding is .89, Supervisor Incivility is .94, Physician Incivility is .94, and Patients/Visitor Incivility is .91. Parametric scores and interpretation for the workplace incivility are as follows: a score of 1.00 – 1.80 is very low, 1.81 to 2.60 is low, 2.61 – 3.40 is moderate, 3.41 – 4.20 is high, and 4.21 – 5.00 is very high.
Part three of the instrument was The Individual Work Performance Questionnaire (IWPQ) by Koopmans (2014). It is a self-report individual work performance based on the individual rating. The questions relate to how the employee carried out the work for the past three months. It is a 27-item tool answered using a five-point Likert Scale where 0 is seldom, 1 is sometimes, 2 is regularly, 3 is often, and 4 is always. The questionnaire has three sub-scales namely: task performance (TP) scale (7 items); contextual performance (CP) scale (12 items); and the counterproductive work behavior (CWB) scale (8 items). For the IWPQ subscales, a mean score is calculated by adding the item scores, and dividing their sum by the number of items in the subscale. Hence, the IWPQ yields three subscale scores that range between 0 and 4, with higher scores reflecting higher task and contextual performance, and higher counterproductive work behavior. The reliability of the IWPQ scales varied from 0.74 for the CWB scale to 0.85 for the contextual performance scale. Parametric scores and interpretation for the performance are as follows: a score of 0.00 – 0.80 is very low, 0.81 – 1.60 is low, 1.61 – 2.40 is average, 2.41 – 3.20 is high, and 3.21 – 4.00 is very high.
The researcher served as the instrument of the study when it comes to the qualitative portion of the study. The researcher was guided and directed by the semi-structured interview guide, which was made up of open-ended questions, in order to elicit replies for the variables that were being investigated. Regarding the interview guide, kindly refer to the appendix.
Data Gathering Procedures
The first step in the research process involved submitting three different research titles for approval. When a title had been accepted, the process of creating the manuscript can then begin. For the purpose of obtaining approval to carry out the study, transmittal letters were also required to be filed. Under the direction of a group of experts, the study was subjected to a design hearing. After the design hearing, the manuscript was submitted for ethical approval, and the recommendations and suggestions that were made during the design hearing were incorporated. The process of recruitment started after it had been approved by the ethics committee. As soon as the notice to proceed was given, the first respondent was recruited accordingly. Participants were recruited by either in-person intercepts or through online platforms, depending on the preference of the researcher. A messaging program (messenger) was utilized for online platforms, and a Google form was constructed specifically for this purpose. The criteria for inclusion and exclusion, as well as the sampling methodology, served as the guiding principles for the recruitment process. Participants who were recruited through face-to-face intercept were given the opportunity to answer the questionnaire in a location of their choosing, which ensured that they were allowed the right to privacy. Everything was carried out in this manner until the desired sample size was reached. After the collection of quantitative data, the next step was the collection of qualitative data. By utilizing the semi-structured interview guide, interviews were carried out. A total of ten individuals who were members of the organization were selected for an interview. There were in-person interviews that were recorded, and they were conducted. The duration of the interview ranges from thirty to sixty minutes.
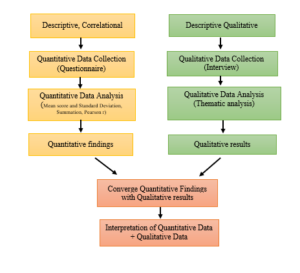
As reflected in Figure 1, there was quantitative data collection using the questionnaire. Alongside there was also qualitative data collection through interview as aided by the semi-structure interview guide. This was followed by quantitative and qualitative data analysis leading to the quantitative findings and qualitative results where the qualitative results validate or converge with the quantitative findings. Lastly, the quantitative and qualitative data were interpreted.
Figure 1: The Mixed Method Research
After all the data had been collected, data were collated using excel format. It was submitted to a statistical for statistical treatment. Data were presented in tables along with their respective interpretations, implications, and supporting literature. At the end of the final defense all raw data and answered questionnaires including the recordings were deleted, shredded, and destroyed.
Data Analysis
For the quantitative data, the following descriptive and inferential statistics were used to treat the data: (a) Mean score and Standard Deviation was used to determine the nursing incivility and work performance of the nurses; (b) Summation was used to determine the organizational citizenship behavior of the nurses; and (c) Pearson r was used to assess the interrelationship among organizational citizenship behavior, nursing incivility, and work performance of the nurses. For the qualitative data, thematic analysis was used. There was proper integration, or converging or diverging of the two types of data to allow the strengths of both to shine as they should in mixed methods research. The qualitative data were weaved with the quantitative data where the quantitative data were presented first and the qualitative data served as a supporting data for the quantitative data.
Ethical Considerations
The researcher made sure that the respondents’ welfare were protected and that their ethical rights were observed. Thus, the study was submitted for ethical review. The study only proceeded with data gathering once an approval from the ethics committee was obtained. Discussion of the ethical considerations is attached in the appendices.
PRESENTATION, ANALYSIS, AND INTERPRETATION OF DATA
Table 1 Organizational Citizenship Behavior of Nurses
| Organizational Citizenship Behavior | Average Score | f | % |
| Very low | 0.00 | 0 | 0.00 |
| Low | 44.78 | 9 | 14.75 |
| Moderate | 61.55 | 20 | 32.79 |
| High | 77.14 | 21 | 34.43 |
| Very High | 91.09 | 11 | 18.03 |
| Average Score | 69.77 | High |
Note: n=61.
Legend: A score of 20 to 36 is very low, 37 to 52 is low, 53 to 68 is moderate, 69 to 84 is high, and 85 to 100 is very high.
The table shows that the organizational citizenship behavior of the nurses was high. Most of them had a high organizational citizenship behavior while almost the same number had a moderate level of organizational citizenship behavior. Few of the respondents had a very high organizational citizenship behavior and very few had a low level of organizational citizenship behavior. This finding implies that nurses believed that once to twice per week they picked up meal for others at work, took time to advise, coach, or mentor a co-worker, helped co-worker learn new skills or shared job knowledge, and helped new employees get oriented to the job. Further, once or twice per week they lent a compassionate ear when someone had a work problem, they lent a compassionate ear when someone had a personal problem, they had changed vacation schedule, work days, or shifts to accommodate co-worker’s needs, and offered suggestions to improve how work is done. Also, once or twice a week they offered suggestions for improving the work environment, finished something for co-worker who had to leave early, helped a less capable co-worker lift a heavy box or other object and a co-worker who had too much to do, and volunteered for extra work assignments.
The nurses in the institution care for others. And by caring for others, this is a reflection of nurses having high levels of organizational citizenship behavior. It is not surprising that the findings of the study revealed a high level of organizational citizenship behavior. This is also evident in the nurses working as team players, they have a way of supporting the entire nursing department and even extends to the other departments. They are advocates of teamwork, collaboration, and coordination which they find a very important component in caring for patients. They are mature individuals who are caring, committed, compassionate, and competent individuals which are reflections of having high organizational citizenship behaviors.
Furthermore, once or twice a week they took phone messages for absent or busy co-worker, said good things about their employer in front of others, gave up meal and other breaks to complete work, and volunteered to help a co-worker deal with a difficult customer, vendor, or co-worker. Lastly, once or twice per week, nurses went out of the way to give co-workers encouragement or express appreciation, they also decorated, straightened up, or otherwise beautified common work space, and defended a co-worker who was being “put-down” or spoken ill of by other co-workers or supervisor.
On top of establishing good working relationships with their co-workers, healthcare and non-healthcare professionals, they show compassion to their co-employees. Nurses clearly understood that fact that establishing a good working relationship with everyone including their patients and families, is one great factor that can contribute to positive patient outcomes.
Data from the qualitative aspect of the study revealed that the informants know what organizational citizenship behaviors is and how it helps the hospital in accomplishing its goals. By having knowledge about organizational citizenship behavior it is also evident that they understood clearly what organizational citizenship behavior is. And with this the qualitative data converges with the quantitative data. Along with the items of the organizational citizenship behavior, a high level of this is a way of performing their jobs in a manner that they exceed beyond one’s job description or they are going above and beyond, they are friendly to their co-workers, they are guided by several virtues, that it is all about helping and collaborating, and that role modelling plays a role.
Exceeding Beyond One’s Job Description / Going Above and Beyond. To the informants, having a high level of organizational citizenship behavior means gaining a clear understanding of their jobs. They do things which are over and beyond what is dictated by their job descriptions.
According to Jose “my experience from the employees of XXX Hospital is that they exceed the level of formality from their resume, from their job descriptions.” (L6-L8)
As expressed by Pedro “organizational citizenship behavior is a person’s full entire commitment to an organization that goes beyond their contractual responsibilities. Or should we say an employee’s willingness to go above and beyond in the workplace.” (L3-L6)
According to Jess “I have experienced organizational citizenship behavior in the workplace since we are always short staffed so we go beyond our job duties in order for us to deliver a safe and quality patient care. We go beyond our duties like being a patient advocate, since I am working in a public hospital so our patient are mostly indigent, I help them by making sure they are given medications when they can’t afford to buy and also by referring them to people or organizations that can help them facilitate their laboratories or any medical assistance.” (L3-L10)
Friendliness. Being friendly is one of the benefits gained when one is having a high level of organizational citizenship behavior. By being friendly, it facilitates good working relationship and it is important when one is working in a profession that is characterized by collaboration and teamwork.
According to Jose “they’re the most friendliest people and co-workers I have experienced with.” (L9-L10)
Virtuousness. Virtues guide a person in the performance of his or her duties. They lead the person in the right direction which is a very nature of a person having a high level of organizational citizenship behavior.
As mentioned by Juan “the employees help each other. what we call being altruistic. There’s also civic virtue. When there is a scheduled event. The employers participate. Participate willingly. They’re also the legends. Some employees. Go to hospital early for punctual. Other virtue or behavior that I observe is being sportsmanship. When there’s a little inconvenience during work, the people involved in the scenes or scenario tend to understand and be more empathetic towards each other.” (L5-L12)
Helping and Collaborating. One major characteristic of a person with high organizational citizenship behavior is being able to work well in teams and being able to collaborate. Caring for patients is undeniably interdisciplinary and collaborative in nature. So, when nurses develop a helping attitude and collaboration, then he or she has a high level of organizational citizenship behavior.
As expressed by Pedro “as for my opinion, people who are actually practicing this brings a sense of unity in a work environment. I see it as a form of helping as long as you can do it and you see yourself as responsible and reliable. Then that can be beneficial in the workplace.” (L6-L9)
Maria mentioned that “when I applied in this hospital, there is one thing that they have emphasized. That when your coworker is in need of help, you should extend one to them. When I was still new here, I have always been asked to help other areas, especially their emergency department since it since it is one of the busiest departments in this hospital. That’s when I realized how important it is to extend help, because doing things all by yourself is really unbearable. And when it was my time to experience being busy, my coworkers never fail to help me, man. Especially the supervisors when there’s a procedure you fail to do. For example IV insertions, or if. Doctor’s order anyone is willing to help you. And sometimes when we’re not busy in our own areas, we go to other areas to help voluntarily as long as it doesn’t interrupt our own work.” (L6-L17)
Jessa verbalized that “I think organizational citizenship behavior or I know that organizational citizenship behavior is very evident in my workplace, especially in normal District Hospital. We, employees of the hospital help each other out, even though it’s not part of our task or assignment to do so, but we help each other out to make things more efficient. And more of a benefit to organization. For example, senior nurses, supervisors and co-working nurses help each other to achieve tasks even though they’re not actually tasked to do it. So I think it’s very evident in my workplace.” (L4-L16)
According to Josefa “my experience about organizational citizenship behavior in my organization. There this one time during my morning shift I was feeling unwell and tired and my patients required more attention so my colleague stopped by at my station. Where I work to help me feel less worried and even encourage me to take some rest. And my colleague. Do the work in my behalf.” (L13-L18)
Joana said that “throughout my career I have developed a strong passion for providing patient care, solving complex problems, and working together with my colleagues and all I can say is that I am proud of myself, that I have developed more on strong communication skills. Allowing me to collaborate effectively with the physicians, social workers and other nurses.” (L6-L11)
Role modelling. This is an important component of organizational citizenship behavior especially if one has long been connected with an institution. It is important to role model as new employees will look up to the person and sees the person as role model. Being able to understand this role is a characteristic of organizational citizenship behavior.
As verbalized by Andres “as one of the older nurses in my organization, I am to be a good example with the least experience for younger nurses. We are a very busy hospital and we sometimes need to limit the time spend with each patient. However, I try to allocate as much time as possible to do who need the most care. That sometimes means that I go. Without my break or stay later than my official finishing time.” (L9-L14)
In the study of Alabbas et al. (2023) nurses had an overall high level of OCB and high mean scores for all dimensions. However, the highest weighted mean was for courtesy, with a mean percentage of 82.63 percent, while the lowest was for civic virtue, with a mean percentage of 70.86 percent. Furthermore, nurses’ OCB levels differ significantly according to their nationalities and years of experience. In support to the findings, in the study of Zeng et al. (2023), nurses’ psychological capital, organizational commitment and organizational citizenship behavior scores were in the upper-middle level. Additionally, organizational commitment partially mediates between psychological capital and organizational citizenship behavior.
Table 2
Workplace Incivility as perceived by the Nurses
| Facets | Mean score | SD | Interpretation |
| General Incivility | |||
| General Incivility: Hostile Climate | 2.42 | .919 | Low |
| General Incivility: Inappropriate Joke | 1.83 | .732 | Low |
| General Incivility: Inconsiderate Behavior | 2.31 | .841 | Low |
| Factor mean | 2.19 | .708 | Low |
| Nurse Incivility | |||
| Nurse Incivility: Hostile Climate | 1.65 | .660 | Very low |
| Nurse Incivility: Gossip and Rumors | 2.40 | .997 | Low |
| Nurse Incivility: Free-Riding | 2.17 | .910 | Low |
| Factor mean | 2.07 | .714 | Low |
| Supervisor Incivility | |||
| Abusive Supervision: Supervisor Incivility | 1.62 | .708 | Very low |
| Lack of Respect: Supervisor Incivility | 2.03 | .822 | Low |
| Factor mean | 1.83 | .717 | Low |
| Physician Incivility | |||
| Abusive Supervision: Physician Incivility | 1.95 | .838 | Low |
| Lack of Respect: Physician Incivility | 2.07 | .873 | Low |
| Factor mean | 2.01 | .808 | Low |
| Patient/Visitor Incivility | |||
| Patient/Visitor Incivility: Lack of Respect | 2.89 | .990 | Moderate |
| Patient/Visitor Incivility: Displaced Frustration | 2.45 | .851 | Low |
| Factor mean | 2.67 | .877 | Moderate |
| Grand mean | 2.15 | .658 | Low |
Note: n=61.
Legend: a score of 1.00 – 1.80 is very low (strongly disagree), 1.81 to 2.60 is low (disagree), 2.61 – 3.40 is moderate (neither agree nor disagree), 3.41 – 4.20 is high (agree), and 4.21 – 5.00 is very high (strongly agree).
General Incivility
Hostile Climate. The table shows that this was rated as low. This means that respondents disagree that hospital employees raised their voices when they get frustrated, people blamed others for their mistakes or offense, and basic disagreements turned into personal verbal attacks on other employees.
Inappropriate Joke. This was rated as low. Respondents strongly disagree that people made jokes about religions groups. However, they disagreed that people made jokes about minority groups and employees made inappropriate remarks about one’s race or gender.
Inconsiderate Behavior. This was rated as low. Respondents disagreed that some people took things without asking, employees did not stick to an appropriate noise level, and employees displayed offensive body language.
Overall, the general incivility was low. This is an affirmation that indeed in the hospital there is a low general incivility. The hospital does not have a hostile climate, in fact it promotes a helping and healthy climate where each one is friendly to one another. There are no giving of inappropriate jokes as the hospital is not a place for that. The nurses understood that they are dealing with lives and that inappropriate jokes may cost the life of a patient. Lastly, nurses are professionals and they know how to act accordingly. Inconsiderate behaviors are not tolerated in the area.
The qualitative data somehow affirms the low level of general incivility experienced by the nurses, for some nurses, they have not experienced any incivility of any type.
No Incivility. It can be deduced from the findings, that the workers in the hospitals are professionals. They are professional in their dealings with one another and with their clients. There may be occasions when incivilities are present but it shows that these incivilities are properly addressed even to the point of making it big.
According to Jose “none. My workplace is like a friendly environment, like a family. It’s warm and there’s no discrimination, just a family type of workplace.” (L11-L12)
According to Jose “I have not experienced any incident regarding incivilities from my co-workers, from my co-nurses, from my supervisors or managers, from physicians and especially from my patients. They treated me as equal as I am, as a person and as an individual. I am treated as how a nurse should be and how an individual should be.” (L16-L20)
As expressed by Pedro “workplace incivility is a type of low intensity deviant behavior that violates workplace norms for me to respect. That includes being rude or discourteous, gossiping, spreading false rumors and sabotaging someone’s work. I haven’t really encountered such in my workplace and if ever I get to encounter such behaviors, I don’t see myself joining in or indulging in such acts.” (10-L15)
As verbalized by Andres “no workplace in civility. In my previous position, there were some nurses who were and pleasantly competitive and this often led to a difficult working environment. I occasionally experienced this and learn to keep to myself and not become involved.” (21-L25)
Jessa verbalized that “working for one year in a few months, I haven’t really experienced workplace incivility in my workplace. … Uh, I think I haven’t really experienced first hand workplace and civility, so therefore I cannot tell anything about the general thought of work and civility.” (L16-L17; L21-L23)
Co-worker Incivility. The organization is not a perfect organization, considering that people working in the hospital are coming from different backgrounds. A few times there may be incivilities caused by the co-workers, but this does not however mean that it is the end of everything. Nurses are able to address incivilities so well and that moving forward they know when incivilities arise.
As explained by Joana “I have encountered situations where colleagues might interrupt each other’s talk over one another during discussions, or even fail to acknowledge the efforts of others. It can be challenging, especially in high stress environments like in emergency departments where everyone is under pressure to deliver quality care.” (L12-L16)
According to Jess “I’ve experienced workplace incivility back then when one of my colleague tattle on me when she told our chief nurse that I didn’t helped her in charting. She was the supervisor that time and she extended help in the ward. She told them that I didn’t help her in charting and I just used my phone the entire time. She told them that she was the one who charted most of the charts which wasn’t true. She should’ve just confronted me in the station instead of making it a big deal and immediately told our head. I observed in our workplace that gossip is very common which is not a healthy behavior since it can damage morale and trust, decrease productivity, and increase conflict.” (L10-L20)
Contrary to the findings, In the study of Abdollahzadeh et al. (2017) data analysis revealed 417 codes, ten categories, three subthemes and one theme, that is, A Need for a Comprehensive Attempt. Attempt of organization, nurses, and public as subthemes are needed to prevent workplace incivility. The findings of the study indicated that a comprehensive and systematic attempt was needed to prevent incivility. Nurses should try to improve their skills; officials should try to show the real image and position of nurses and hospitals to the community.
Nurse Incivility
Hostile Climate. This was rated as very low. Respondents disagreed that nurses argued with each other frequently, that nurses had violent outbursts or heated arguments in the workplace, and that nurses screamed at other employees.
Gossip and Rumors. This was rated as low. Supporting the findings, the respondents disagreed that nurses gossiped about their supervisor at work, that nurses bad-mouthed others in the workplace, and nurses spread bad rumors around here. However, the neither agree not disagree that the nurses gossiped about one another.
Free-Riding. This was rated as low. Respondents disagreed that nurses made little contribution to a project but expect to receive credit for working on it, nurses claimed credit for their work, and nurses took credit for work they did not do.
Overall, nurse incivility was low. Nurses are able to show a great deal of collaboration and coordination. They do not cause troubles. They also act professionally and make sure that everything is in place in the wards. This is also evidenced by nurses not having reported conflicts among nurses. They coordinate so well in times of hands off and indorsements. They promote a health working environment which fosters camaraderie. They know that there is no time for gossips and rumors and that they work so hard to be able to contribute to the nursing department and the hospital in general.
A low level of nursing incivility is being affirmed by the qualitative findings, for few of the informants expressed that they have experienced gossip and a form of incivility. A low level of nursing incivility could mean that there is at some point an incivility but not rampant.
Gossip. Indeed, it is perhaps part of the Filipino culture to do gossips. It would be very difficult to avoid such incivility being a part of the culture.
As mentioned by Juan “so far, for my past 11 months working in this organization. The only incivility that I observe is the social practice, where people tend to gossip, which is in civil for me.” (L13-L16)
As mentioned by Juan from coworkers or converses, I think it’s pretty normal for Filipinos to talk about an incident or passive space related to corners is another place involved. From supervisor so far I have not yet experienced any incivility. From physicians? I think if they want to know the whole story that involve personal information that are confidential. And for patients, the civilities that I witness, they tend to gossip versus with their incompetence, which is probably subjective and a matter of uh discussion.” (L17-25)
Contrary to the findings, in the study of Keller et al. (2020), results were mostly inconsistent regarding individual characteristics of targets of incivilities (e.g., age, gender, ethnicity), but less experienced healthcare professionals were more exposed to incivility. In most studies, participants reported experiencing incivilities mainly within their own professional discipline (e.g., nurse to nurse) rather than across disciplines (e.g., physician to nurse). Evidence of specific medical specialties particularly affected by incivility was poor, with surgery as one of the most cited uncivil specialties. Finally, situational and cultural predictors of higher incivility levels included high workload, communication or coordination issues, patient safety concerns, lack of support and poor leadership.
Supervisor Incivility
Abusive Supervision. This was rated as very low by the respondents. Respondents strongly disagree that their supervisor was verbally abusive, their supervisor yelled at them about matters that were not important, and their supervisor shouts or yells at me for making mistakes, and their supervisor took his/her feelings out on them.
Lack of Respect. This was rated as low. Supporting the findings, the nurses disagree that their supervisor did not respond to their concerns in a timely manner, their supervisor factored gossip and personal information into personnel decisions, and their supervisor was condescending to them.
Overall supervisor incivility was low. Indeed, the supervisors are professional individuals. They practice management functions to the best of their abilities. They are technically competent when it comes to managing their units and provides respect to every member therein. They conduct periodic meetings and emergency meetings should issues arise needing immediate attention. They are very capable in handling their units.
Validating the quantitative findings is the fact that an informant was not able to experience supervisor incivility which only mean s the this incivility is really low.
No Incivility. It would show that the supervisors are well-mannered as they are not causes of incivility among nurses.
As explained by Ana “I don’t experience workplace incivility from my workmate.” (L7) She added that “Some coworkers, nurses, some supervisors, managers and some physicians. Some patients, I didn’t experience any workplace incivilities and my co-workers, especially my supervisor. They understand us, teach us if we don’t know what to do in that situation. And they teach us to correct other mistakes.” (L9-L13)
Supporting the finding, in the study of Alquwez (2020), the highest mean score was recorded for patient or visitor incivility, whereas the lowest score was recorded for supervisor incivility. Regarding patient safety competence, the dimension “communicating effectively” received the highest mean score, whereas “working in teams with other health professionals” was rated lowest. General and nurse incivilities had multivariate effects on the six dimensions of patient safety competence. Nurses’ experiences of uncivil acts from nurses and from general incivility negatively impact nurses’ patient safety competence.
Physician Incivility
Abusive Supervision. This was rated as low. Supporting the finding, the respondents disagreed that some physicians were verbally abusive, physicians yelled at nurses about matters that were not important, physicians shouted or yelled at them for making mistakes and physicians took their feelings out on them.
Lack of Respect: Physician Incivility. This was rated as low. Respondents disagree that physicians did not respond to their concerns in a timely manner, they were treated as though their time was not important, and physicians were condescending to them.
Overall physician incivility was low. It had been observed that physicians are professional in their dealings whether with patients or with co-workers. They did not verbally abuse or yelled anyone. They make sure that they communicate properly with everyone. Every time there is an error, they take proactive measures to make sure that errors are appropriately addressed.
Converging the findings is the finding of the qualitative data. Physician incivility is not a rampant event in the hospital. At some points, informants may have experienced this.
Physician Incivility. At times, doctors may be a source of incivility. It is just normal at times that doctors get angry as they are only looking at the welfare of their patients. This may just be an initial reaction and not personally directed to the nurses.
According to Joana “one incident I recall involved a situation where a physician spoke quite harshly to nurse during a shift change the nurse had made a minor mistake with medication documentation and instead of offering constructive feedback to physicians. She decides her in front of the team in a very demeaning way. It really created an uncomfortable atmosphere and made the nurse visibly upset, which impacted her confidence and performance for the rest of the shift. All I can say is that I try to stay calm and focused on my work, but I also make an effort to support my colleagues.” (L17-L25)
Also, in the study of Armstrong (2018), workplace incivility is a well-documented issue in nursing in the health care setting. It has the potential to cause emotional and physical distress in victims and potentially affects the quality of care provided. Despite the lower quality of research, the collection of evidence suggests the use of a combination of educational training about workplace incivility, training about effective responses to uncivil workplace behaviors, and active learning activities to practice newly learned communication skills, in assisting nurses in improving their ability to manage incivility in the workplace.
Patient/Visitor Incivility
Lack of Respect. This was rated as moderate by the nurses. This means that nurses neither agree nor disagree that patients had taken out their frustrations on nurses, patients showed that they were irritated or impatient, patients made insulting comments to nurses, and patients treated nurses as if they were inferior or stupid.
Displaced Frustration. This was rated low. Supporting this finding, the respondents disagreed that the patients were condescending to them, patients criticized their job performance, patients made personal verbal attacks against then, and patients did not trust the information they gave them and asked to speak with someone of higher authority. However, they neither agree nor disagree that patients posed unreasonable demands and patients made comments that question the competence of nurses.
Overall, patient/visitor incivility was moderate. It is quite understandable that patients or their family members have issues of incivility to nurses. This should be understood as a response to the patient having an illness or disease. This could be a result of the grieving process where patients or their families are at the denial or anger stage.
Overall, the workplace incivility was low as perceived by the nurses. This only shows that the employees along with the patients in the hospital are having a good relationship. The low levels of workplace incivility simply indicates that everyone is professional in the execution of their respective jobs. Also, it means that they are bounded by their respective professions, through the code of ethics and the different las governing their professions. This also shows that patients are very understanding of the hospital employees.
This moderate finding is affirmed by the qualitative findings of the study.
Patient Incivility. It is quite notable that patients are the main sources of incivility that nurses face. However, it is also understandable why they go through this phase as this could be a reaction to their illnesses and not personally directed to the nurse.
As expressed by Pedro “so far, the incivilities that I have experienced working as a nurse came from our patients and their significant others. Some of them wouldn’t listen to us when we gave them directions and would sometimes give us a negative answer. Even though we communicate with them in the most courteous and gentle way. But I don’t blame them for how they behave. Maybe it’s simply the result of the situation that they are in at the moment.” (L16-L22)
As verbalized by Andres “before, when I was at a large private hospital which was very busy, the patient to nurse ratio was very high and we need to limit the time as. We spend with each patient. Some patients were not happy with this and expected much more time and personal attention. This was very stressful and difficult to manage.” (L21-L25)
Maria mentioned that “then the son of the patient kept coming back to the station, saying different demands and requests. At first they want to transfer to VMC. They want to transfer as soon as possible, so I explained how it’s going to work after my reference to doctor code so. They decided to transfer to a private hospital since they couldn’t wait for the code. So I explained the both to them.” (L30-35)
Maria also mentioned that “he was yelling. He looked down on me, the hospital and even to the physicians. Mu shagit man siya then dako kaayo iya voice tapos adto ko na shock kay ni ingon man siya na maam unsa man maam inyo pani insertan ug NGT maam if dili mo kay ako nalang mu insert kay sayon ra bitaw na kahibaw man ko mu insert (He shouted and he was raising his voice and I was shocked when he ask if we will still insert the patient with NBT because if not then he will be the one who will insert since he knows how to insert it). (L52-L56)
Supporting the findings, the results indicated that nurses did have experiences with incivility at the facility with the sources being identified as General Hostile Climate, Nurse Gossip and Rumors, Physician Abusive Supervision and Patient and Visitor Displaced (Gillian, 2015).
Table 3 Work Performance of the Nurses
| Dimensions | Mean score | SD | Interpretation |
| Task Performance | 3.14 | .746 | High |
| Contextual Performance | 2.97 | .735 | High |
| Counterproductive Work Behavior | .650 | .502 | Very low |
Note: n=61.
Legend: A score of 0.00 – 0.80 is very low (seldom), 0.81 – 1.60 is low (sometimes), 1.61 – 2.40 is average (regularly), 2.41 – 3.20 is high (often), and 3.21 – 4.00 is very high (always).
Task Performance (TP) Scale. The table shows that this was rated as high. This means that respondents always managed to plan their work so that it was done on time, they knew how to set the right priorities, and collaboration with others was very productive. However, it is often that their planning was optimal, they kept in mind the results that they had to achieve in their work, was able to separate main issues from side issues at work, and they were able to perform their work well with minimal time and effort.
Nurses need not be reminded, they have been given their respective job descriptions and given an orientation from the time that they joined the institution. As nurses, they know too well that their work is not only with patients but to make sure to be working with the healthcare team. They know too well that caring for patients entails the use of planning through the development of care plans and that their ultimate goal is to make sure that patients have shorter stay in the hospital and that they return to the community as healthy individuals.
This finding converges with the qualitative data that indeed time management is important for nurses to be able to perform their task.
Time Management. Time is a very important factor in nurses being able to accomplish their task. With the number of patients that they handle, they need to manage their time correctly and appropriately for them to be able to complete their task.
According to Jose “work performance in general, I could say it’s the time management, your responsibilities as a nurse, how you take care of your patients, how you render care through their health needs by physical, mental, spiritual. That is my idea of work performance as a nurse and as a professional.” (L24-L28)
As mentioned by Juan “by showing their time management skills, being a team member, where he or she can communicate is in some information that benefits the organization, patient, coworkers and other people involved.” (L32-L35)
Contrary to the findings, the finding of the study of Rastegari et al. (2010) showed that the most common kind of quality of working life in the nurses was moderate one. The most frequent nurses’ task performance was also related to the moderate performance. There was a direct and significant relationship between job performance and quality of working life in all the aspects. According to the research findings, it is important to consider the workplace and quality of working life of the nurses for improving productivity and performance of the nurses.
Also, in the study of Dirdjo et al. (2023), majority of nurses are satisfied with their work, while just over half of nurses still have poor performance. This study has revealed a significant relationship between job satisfaction and the performance of nurses in the surgical treatment room with OR showing 6.188 meaning that nurses who are dissatisfied with their work have the opportunity to perform less well 6.2 times, when compared with nurses who are satisfied in their jobs. These results can be used by hospital nursing managers that in order to improve nurse performance they must consider the job satisfaction of their nurses.
Contextual Performance (CP) Scale. This was rated as high. This means that they often took on extra responsibilities, they started new tasks themselves, when their old ones were finished, they took on challenging work tasks, when available, and they worked at keeping their jobs knowledge up-to-date. Also, they often worked at keeping their job skills up-to-date, they came up with creative solutions to new problems, and kept looking for new challenges in their job. Lastly, they often did more than was expected of them, they actively participated in work meetings, grasped opportunities when they presented themselves, and they often knew how to solve difficult situations and setbacks quickly. However, they always actively looked for ways to improve their performance at work.
Nurses are very aware of their responsibilities towards their profession. They know that they have a responsibility to maintain their competence through continuing professional education. They have a responsibility to go for evidence-based practice and make use of recent research findings in their practice. The different trainings, seminars, and workshops will help them maintain competence but also allow them to renew their licenses. They have developed, critical-thinking and problem-solving skills to address every problem of their different patients.
This quantitative findings converges with the qualitative data where informants were able to emphasize being effective and efficient in their work. By being effective and efficient, they are able to accomplish greater heights in terms of their contextual performance.
Being Effective and Efficient. For nurses to be able to perform contextually, they have to be effective and efficient at the same time. When nurses take extra responsibilities, take challenging work tasks, work at keeping their job knowledge and skills up-to-date, and coming up with creative solutions to new problems, these are clear manifestation of being effective and efficient.
As mentioned by Juan “my idea of work performance refers to a set of attributes where an employee can show such as being effective, efficient, and productive.” (L31-L32)
Maria mentioned that I” think our performance is how you perform your job. Like, do you perform your job well or you just do it? Doing it is different from doing it well. For example, in giving medications, do you just give medications to your patients? I think. It’s really different from doing it, but no you should not judge. Just give medications. You should give the right medication to the right patient, the right dosage, the right time. You should then just give. Performance is how you perform your job well. You. Give the right medications and time’s up. Aside from being effective, you’re also being efficient. Like. I think it’s also important to be efficient. Go on like doing it at the same time effectivity and efficiency. You cannot pronounciate efficient. I think those two must go. Well with each other like efficiency or effectivity. If you’re effective that, but you should also be efficient if you’re efficient that, but it should also be effectively like it goes. (L71-L85)
Jessa also mentioned that “for me, work performance is the act of doing and accomplishing things without any hassle. Everything is planned out, even though there are minor inconveniences, tasks are still effectively accomplished.” (L33-L36)
According to Joana “first and foremost, it’s about providing safe, effective and compassionate care to patients. This means that you have to follow your clinical protocols, administering medications correctly and ensuring that patient assessments and interventions are timely. And accurate, but it’s also about being responsive to patients, needs like listening actively and showing empathy, so they feel valued and understood.” (L26-L31)
Also, being a problem-solver and possessing leadership skills is a component of the contextual performance and this is affirmed by the qualitative findings.
Possessing Problem-solving and Leadership Skills. When nurses are able to come up with creative solutions to new problems and them knowing how to solve difficult situations and setbacks quickly, clearly encompasses that they have high contextual performance.
As mentioned by Juan “also, it may include problem solving skills and leadership skills.” (L35-L37)
Contrary to the findings, results in the study of Ibrahim et al. (2023) revealed that majority of studied staff nurses had moderate level of perception toward work related stress and more than half of studied staff nurses had fair level of job performance. There was no statistically significant correlation between work related stress and job performance of the studied staff nurses. Establishing a committee represented from staff nurses that discuss nursing staff problems, continuing education programs for nurses should include topics about work related stress and its preventive measures to decrease its negative outcomes and Enhance job performance of nurses by creating and organizing training program on job performance as a managerial skill for head nurses to maintain improving patient care.
Counterproductive Work Behavior (CWB) Scale. This was rated as very low. This means that respondents seldom complained about unimportant matters at work, made problems greater than they were at work, they focused on the negative aspects of a work situation, instead of on the positive aspects and they spoke with colleagues about the negative aspects of my work. Also, they seldom spoke with people from outside the organization about the negative aspects of their work, they did less than was expected of them, and sometimes did nothing, while they should have been working. However, they sometimes managed to get off from a work task easily.
A low counterproductive work behavior would only mean that nurses are not doing their jobs. This would mean that there will be more patients and patients would have a longer stay in the hospital. However, looking at the current state of the hospital, nurses are doing their jobs and making sure that patients become well and they have shorter stays in the hospital. This is evidenced by the number of discharges that the hospital is having and therefore, nurses are doing their jobs and they are very productive individuals.
A very low counterproductive work behavior would also been that nurses are being productive in their work. And by being productive this would mean that they were able to execute their jobs very satisfactorily and in a good manner. Converging this quantitative finding is the qualitative data.
Good Performance. A low counterproductive performance could be understood as being productive. Nurses were productive because they had a good performance.
As pressed by Pedro “so far, I think I’m doing a good job at work. I am able to finish my task and be of help to my colleagues. Work performance is the act of carrying out or completing an action task or function without difficulty. Employees can easily accomplish their work tasks and meet their organization’s goals on schedule.” (L27-L32)
As verbalized by Andres “I started my nursing career with a busy private hospital. The standard and work expectation were very high. This taught me to be completely patient focused. My best work performance is what I aim to maintain every day.” (L42-L45)
Very Satisfactory. Similarly, by performing very satisfactorily, this would mean that the nurses are not counterproductive but instead they are productive.
Jessa verbalized that “as a nurse who has been working for. More than a year. I think my experience about work performance as a nurse is very satisfactory, I guess because we are able to carry out and accomplish any task or action without any hassle at our institution, at our hospital. We, the staff, the persons and the employees are part of the institution work each other work with each other to help things. Get done quickly without hassle, so I guess my work experience and my work performance as a nurse has been really great.”(L35-L36)
Giving your Best. It also means that because they are able to give their best to their respective jobs, they become productive and not counterproductive.
As expressed by Pedro “I always see to it that I am doing my best every day as I work. Most especially because we’re dealing with people’s lives. That means that we have to be really careful and when in doubt and ask for somebody’s help.” (L24-L27)
Healthy Environment as a Factor to Good Performance. A good working environment can greatly help in person being productive. A supportive environment allows accomplishment of tasks.
According to Jess “I believe that work performance as a nurse depends on the work environment, if the employee has a healthy work environment, it can make the work easier. In my case, I can say that I have a healthy work environment since my colleagues and I treat each other as family. Thus despite having tons of work and increasing patient census, we can avoid work burnout because of the healthy environment that the workplace offers. As a nurse, work performance is very important since it can measure the quality of work the nurse gives, how well the nurse manages time, punctuality, efficiency and productivity also team work and collaboration.
Learning from Co-workers. Being open to learning is a good characteristic of a person. This only shows that by being receptive the person is really working on being productive.
According to Ana “my work performance, I learned a lot from my co-work mates. I can now handle workloads and I can constantly contribute positively to tilted activity.” (L17-L18)
Supporting the findings, while the majority of nurses rated their job performance as good, it is important to note that a relevant proportion of nurses rated their job performance as poor. The findings of this study identified that nurses’ performance is influenced by several key factors, including workload, remuneration, rewards, objectives to be achieved, and feedback on performance appraisals (Daba et al., 2024).
Table 4
Relationship between Organizational Citizenship Behavior and Nursing Incivility
| Variables | r value | p value | Decision | Interpretation |
| General Incivility | ||||
| hostile climate | -.337 | .008 | Reject Ho | Significant |
| inappropriate jokes | -.189 | .145 | Failed to reject Ho | Not significant |
| inconsiderate behavior | -.229 | .076 | Failed to reject Ho | Not significant |
| overall general incivility | -.302 | .018 | Reject Ho | Significant |
| Nurse Incivility | ||||
| hostile climate | -.150 | .247 | Failed to reject Ho | Not significant |
| gossip and rumors | -.273 | .033 | Reject Ho | Significant |
| free-riding | -.194 | .135 | Failed to reject Ho | Not significant |
| overall nurse incivility | -.256 | .040 | Reject Ho | Significant |
| Supervisor Incivility | ||||
| abusive supervision | -.172 | .184 | Failed to reject Ho | Not significant |
| lack of respect | -.196 | .130 | Failed to reject Ho | Not significant |
| overall supervisor incivility | -.198 | .127 | Failed to reject Ho | Not significant |
| Physician Incivility | ||||
| abusive supervision | -.157 | .227 | Failed to reject Ho | Not significant |
| lack of respect | -.116 | .372 | Failed to reject Ho | Not significant |
| overall physician incivility | -.144 | .269 | Failed to reject Ho | Not significant |
| Patient Incivility | ||||
| lack of respect | -.451 | .000 | Reject Ho | Significant |
| displaced frustration | -.352 | .005 | Reject Ho | Significant |
| overall patient incivility | -,424 | .001 | Reject Ho | Significant |
| Overall Workplace Incivility | -.312 | .014 | Reject Ho | Significant |
Legend: Significant if p value is < .05. Dependent Variable: Nursing Incivility. Pearson r interpretation: A value greater than .5 is strong (positive), between .3 and .5 is moderate (positive), between 0 and .3 is weak (positive), 0 is none, between 0 and –.3 is weak (negative), between –.3 and –.5 is moderate (negative), and less than –.5 is strong (negative).
General Incivility. The p values for the relationship between organizational citizenship behavior and hostile climate and overall general incivility were lesser than the significant value of .05. These values were interpreted as significant leading to the decision of rejecting the null hypothesis. Thus, organizational citizenship behavior was significantly correlated with hostile climate and overall general incivility. The correlations were moderate and negative. This means that an increase in organizational citizenship behavior leads to a decreased in hostile climate and overall general incivility. Having a high level of organizational citizenship behavior would mean that the person has better appreciation of things in their work. It may also mean that the person is more mature and more responsible, this way this will not allow a hostile climate and incivility to set in. This is very well observed in the hospital and as supported by the findings on incivility which are low in the previous table.
Supporting the findings, the study’s findings rejected hypotheses one and two showing workplace incivility (WPI) has a detrimental effect on employee engagement and employee performance (Singh et al., 2023).
However, the p values for the relationship between organizational citizenship behavior and inappropriate jokes and inconsiderate behavior were greater than the significant value of .05. These values were interpreted as not significant leading to the decision of failing to reject the null hypothesis. Thus, organizational citizenship behavior was not significantly correlated with inappropriate jokes and inconsiderate behavior. This means that an increased organizational citizenship behavior can lead to low inappropriate jokes and inconsiderate behavior. Similarly, a person with high organizational citizenship behavior would mean that the person is more mature and more responsible and this way incivility will not prosper.
Nurse Incivility. The p values for the relationship between organizational citizenship behavior and gossip and rumors and overall nurse incivility were lesser than the significant value of .05. These values were interpreted as significant leading to the decision of rejecting the null hypothesis. Thus, organizational citizenship behavior was significantly correlated with gossip and rumors and overall nurse incivility. The correlations were weak and negative. This means that an increase in organizational citizenship behavior leads to a decreased in gossip and rumors and overall nurse incivility. Nurses with high organizational citizenship behavior allows them to be more mature and more responsible. They can have better appreciation of things. By being mature and responsible, they disregard gossips and rumors and that they would rather be more productive than waste their time. This is further supported by the findings in the previous table where the nurse incivility is low.
Supporting the findings, the results of the study of Saleem et al. (2022) affirmed that incivility is harmful to the performance of employees, and that trust in supervisors helps employees to perform well. The trust in the supervisor significantly mediates the incivility–performance relationship.
However, the p values for the relationship between organizational citizenship behavior and hostile climate and free-riding were greater than the significant value of .05. These values were interpreted as not significant leading to the decision of failing to reject the null hypothesis. Thus, organizational citizenship behavior was not significantly correlated with hostile climate and free-riding. This means that an increased organizational citizenship behavior can lead to low hostile climate and free-riding. Gaining a high level of organizational citizenship behavior will pre-suppose that the person is more mature, wise, and responsible. They also become more proactive and this way they will be able to collaborate better and work as a team, thus, a hostile climate or environment and free-riding are discouraged.
Supervisor Incivility. The p values for the relationship between organizational citizenship behavior and abusive supervision, lack of respect, and overall supervisor incivility were greater than the significant value of .05. These values were interpreted as not significant leading to the decision of failing to reject the null hypothesis. Thus, organizational citizenship behavior was not significantly correlated with abusive supervision, lack of respect, and overall supervisor incivility. This means that an increased organizational citizenship behavior can lead to low abusive supervision, lack of respect, and overall supervisor incivility. A well-developed organizational citizenship behavior can reap a multitude of benefits and advantages. They allow employees to be better individuals where abuse and lack of respect cannot foster. This is also supported by the findings in the previous table where the supervisor incivility was low. Evidently, supervisors were very professional in their dealings.
Findings of the study of Aruoren and Ugbeghene (2023) revealed that workplace incivility was negatively related to both task and adaptive performance, but only significantly related to task performance. Furthermore, workplace incivility was found to be positively related to counterproductive work behavior and contextual performance, however, this relationship was only significant for counterproductive work behavior.
Physician Incivility. The p values for the relationship between organizational citizenship behavior and abusive supervision, lack of respect, and overall physician incivility were greater than the significant value of .05. These values were interpreted as not significant leading to the decision of failing to reject the null hypothesis. Thus, organizational citizenship behavior was significantly correlated with abusive supervision, lack of respect, and overall physician incivility. This means that an increased organizational citizenship behavior can lead to low abusive supervision, lack of respect, and overall physician incivility. A high organizational citizenship behavior foster good working relationship and when harmonious relationship exists this would also mean that everyone is given due respect as member of the team. There will also be no abuse that will foster as everyone is respected. This is further supported by the findings in the previous table where the physician incivility was low.
Coworker incivility and customer incivility reduced work engagement and job performance. The effects of coworker incivility on the work engagement and job performance are greater than those of customer incivility. Furthermore, work engagement has a positive effect on the job performance (Wang & Chen, 2020).
Patient Incivility. The p values for the relationship between organizational citizenship behavior and lack of respect, displaced frustration, and overall patient incivility were lesser than the significant value of .05. These values were interpreted as significant leading to the decision of rejecting the null hypothesis. Thus, organizational citizenship behavior was significantly correlated with lack of respect, displaced frustration, and overall patient incivility. The correlations were moderate and negative. This means that an increase in the organizational citizenship behavior leads to an increased lack of respect, displaced frustration, and overall patient incivility. Similarly, high levels of organizational citizenship behavior allow good working relationship and this can be used as a tool to also establish good working relationship with patients. Patients are given a chance to partake in his or her care, this way they will be respected and when they are being called to partake, they will have a sense of belongingness and ownership. This way this will prohibit then from feeling frustrated.
A recent hospital study found that the majority of nurses identified their patients as the main perpetrators of verbal or physical abuse (Farrell et al., 2006 as cited in Guidroz et al., 2010). This abuse influenced the severity of distress that nurses experienced, their overall productivity, and increased sentiments for withdrawing from the career of nursing.
Overall Workplace Incivility. The p values for the relationship between organizational citizenship behavior and overall workplace incivility was lesser than the significant value of .05. This value was interpreted as significant leading to the decision of rejecting the null hypothesis. Thus, organizational citizenship behavior was significantly correlated with overall workplace incivility. The correlation was moderate and negative. This means that an increase in the organizational citizenship behavior leads to a decreased overall workplace incivility.
Supporting the findings, according to the findings of the study of Mahmood et al. (2023), interpersonal deviance acts as a partial mediator between incivility shown by coworkers and supervisors and behavior that demonstrates organizational citizenship. In addition, the findings demonstrated that the perception of organizational support moderates the association between incivility shown by coworkers and supervisors and behavior that demonstrates organizational citizenship.
Contrary to the findings, workplace incivility (supervisor, coworker, and clients) did not predict OCB significantly. JH and work self-efficacy positively predicted organizational citizenship behavior (OCB), while PO negatively predicted OCB. This research provides new directions for future research that OCB is not predicted by workplace incivility (Annalakshmi et al., 2022).
A well-developed organization citizenship behavior would allow employees to be more mature and responsible. With maturity, they will gain better understanding of things and appreciate them well. Thus, they will also develop good working relationships with all the other employees. It will not allow incivility to come in.
Table 5 Relationship between Nursing Incivility and Work Performance
| Variables | r value | p value | Decision | Interpretation |
| Task Performance | ||||
| General incivility | ||||
| hostile climate | -.149 | .253 | Failed to reject Ho | Not significant |
| inappropriate jokes | -.223 | .084 | Failed to reject Ho | Not significant |
| inconsiderate behavior | -.089 | .495 | Failed to reject Ho | Not significant |
| Overall general incivility | -.177 | .172 | Failed to reject Ho | Not significant |
| Nurse incivility | ||||
| hostile climate | -.260 | .043 | Reject Ho | Significant |
| gossip and rumors | .015 | .906 | Failed to reject Ho | Not significant |
| free-riding | -.208 | .108 | Failed to reject Ho | Not significant |
| Overall nurse incivility | -.162 | .212 | Failed to reject Ho | Not significant |
| Supervisor incivility | ||||
| abusive supervision | -.227 | .079 | Failed to reject Ho | Not significant |
| lack of respect | -.300 | .019 | Reject Ho | Significant |
| Overall supervisor incivility | -.285 | .026 | Reject Ho | Significant |
| Physician incivility | ||||
| abusive supervision | -.160 | .218 | Failed to reject Ho | Not significant |
| lack of respect | -.223 | .085 | Failed to reject Ho | Not significant |
| Overall physician incivility | -.204 | .115 | Failed to reject Ho | Not significant |
| Patient incivility | ||||
| lack of respect | -.134 | .303 | Failed to reject Ho | Not significant |
| displaced frustration | -.141 | .279 | Failed to reject Ho | Not significant |
| Overall patient incivility | -.143 | .273 | Failed to reject Ho | Not significant |
| Overall Workplace Incivility | -.217 | .093 | Failed to reject Ho | Not significant |
| Contextual Performance | ||||
| General incivility | ||||
| hostile climate | -.299 | .019 | Reject Ho | Significant |
| inappropriate jokes | -.176 | .176 | Failed to reject Ho | Not significant |
| inconsiderate behavior | -.288 | .024 | Reject Ho | Significant |
| Overall general incivility | -.276 | .031 | Reject Ho | Significant |
| Nurse incivility | ||||
| hostile climate | -.122 | .350 | Failed to reject Ho | Not significant |
| gossip and rumors | -.279 | .030 | Reject Ho | Significant |
| free-riding | -.239 | .064 | Failed to reject Ho | Not significant |
| Overall nurse incivility | -.265 | .039 | Reject Ho | Significant |
| Supervisor incivility | ||||
| abusive supervision | -.290 | .023 | Reject Ho | Significant |
| lack of respect | -.107 | .412 | Failed to reject Ho | Not significant |
| Overall supervisor incivility | -.285 | .026 | Reject Ho | Significant |
| Physician incivility | ||||
| abusive supervision | -.180 | .166 | Failed to reject Ho | Not significant |
| lack of respect | -.302 | .018 | Reject Ho | Significant |
| Overall physician incivility | -.153 | .239 | Failed to reject Ho | Not significant |
| Patient incivility | ||||
| lack of respect | -.306 | .016 | Reject Ho | Significant |
| displaced frustration | .769 | .000 | Reject Ho | Significant |
| Overall patient incivility | -.318 | .013 | Reject Ho | Significant |
| Overall Workplace Incivility | -.300 | .109 | Failed to reject Ho | Not significant |
| Counterproductive Work Behavior | ||||
| General incivility | ||||
| hostile climate | .308 | .016 | Reject Ho | Significant |
| inappropriate jokes | .211 | .103 | Failed to reject Ho | Not significant |
| inconsiderate behavior | .292 | .022 | Reject Ho | Significant |
| Overall general incivility | .270 | .036 | Reject Ho | Significant |
| Nurse incivility | ||||
| hostile climate | .280 | .029 | Reject Ho | Significant |
| gossip and rumors | .362 | .004 | Reject Ho | Significant |
| free-riding | .331 | .009 | Reject Ho | Significant |
| Overall nurse incivility | .374 | .003 | Reject Ho | Significant |
| Supervisor incivility | ||||
| abusive supervision | .363 | .004 | Reject Ho | Significant |
| lack of respect | .317 | .013 | Reject Ho | Significant |
| Overall supervisor incivility | .371 | .003 | Reject Ho | Significant |
| Physician incivility | ||||
| abusive supervision | .349 | .006 | Reject Ho | Significant |
| lack of respect | .312 | .014 | Reject Ho | Significant |
| Overall physician incivility | .353 | .005 | Reject Ho | Significant |
| Patient incivility | ||||
| lack of respect | .342 | .007 | Reject Ho | Significant |
| displaced frustration | .002 | .987 | Failed to reject Ho | Not significant |
| Overall patient incivility | .342 | .007 | Reject Ho | Significant |
| Overall workplace Incivility | .390 | .002 | Reject Ho | Significant |
Legend: Significant if p value is < .05. Dependent Variable: Work Performance. Pearson r interpretation: A value greater than .5 is strong (positive), between .3 and .5 is moderate (positive), between 0 and .3 is weak (positive), 0 is none, between 0 and –.3 is weak (negative), between –.3 and –.5 is moderate (negative), and less than –.5 is strong (negative).
Task Performance
General Incivility. The p values for hostile climate, inappropriate jokes, inconsiderate behavior, and overall general incivility were greater than the significant value of .05 which were interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, hostile climate, inappropriate jokes, and inconsiderate behavior, and overall general incivility were not significantly correlated with task performance. Task performance can still be high despite a high level of hostile climate, inappropriate jokes, inconsiderate behavior, and overall general incivility. This would imply that despite the presence of incivility, there can still be high task performance because nurses know for a fact that the patient is the priority and patients cannot be compromised. So despite the presence of incivility, nurses tend to divert to prioritizing their patients. After all, caring for patients is main reason why they are there in the first place.
Nurse Incivility. The p value for hostile climate was lesser than the significant value of .05 which was interpreted as significant which led to the decision of rejecting the null hypothesis. Thus, hostile climate of nurse incivility was significantly correlated with task performance. The correlation with hostile climate was weak negative. This means that the lower the hostile climate, the higher the task performance. A hostile climate does not promote good working environment. In its absence there will be no complications and issued, this way the nurses will be able to concentrate on their work and perform well for the betterment of their patients.
However, the p value for gossip and rumors, free-riding, and overall nurse incivility were greater than the significant value of .05 which were interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, gossip and rumors, free-riding, and overall nurse incivility were not significantly correlated with task performance. This means that a high level of task performance can still be achieved despite high levels of gossip and rumors, free-riding, and overall nurse incivility. Again it would show that despite the gossips and rumors, the patient will be the priority. Caring for patients cannot be compromised just because of the presence of gossips and rumors.
Supervisor Incivility. Supervisor incivility was significantly correlated with task performance. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was weak and negative. The lower the supervisor incivility, the higher the task performance. If nurses are being led by managers that are professional, then they will be able to work well and execute their respective jobs for the attainment of the hospital goals and mission and vision. Professional leaders and managers are essential to achieving a direction that is directed towards achieving the mission and vision of the hospital.
More specifically, lack of respect of supervisor incivility was significantly correlated with task performance as evidenced by the p value of lesser than .005. This value was interpreted as significant which led to the rejection of the null hypothesis. The correlation with lack of respect was weak negative. This means that the lower the lack of respect, the higher the task performance. Respect is a very important component in every discipline that is characterized by coordination and collaboration. When nurses are respected, it means that they are given importance and being a a part of the team. This will allow them to accomplish their respective jobs and therefore they become more productive. As nurses are being respected they also respect others.
However, the p value for abusive supervision was greater than the significant value of .05 which was interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, abusive supervision was not significantly correlated with task performance. This means that a high level of task performance can still be achieved despite high levels of abusive supervision. Though this is a possible scenario but the supervisors in the hospital are never abusive. They make use of different leadership styles which are fitted to every given situation. They know that it is unethical to be abusive and that they can face possible consequences of being abusive. Thus, the supervisors are highly professional in managing the nurses.
Physician Incivility. The p values for abusive supervision, lack of respect, and overall physician incivility were greater than the significant value of .05 which were interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, abusive supervision, lack of respect, and overall physician incivility were not significantly correlated with task performance. This means that a high level of task performance can still be achieved despite high levels of abusive supervision, lack of respect, and overall physician incivility. Doctors are never abusive, they respect nurses and everyone. It clearly shows that in the hospital doctors are very professional in their dealing with their patients and co-workers. Thy know too well what is dictated of them by their code of ethics despite the workload and number of patients that they have. They maintain composure despite the odds. By showing this professionalism, they allow nurses to be more productive members of the healthcare team.
Patient Incivility. The p values for lack of respect, displaced frustration, and overall patient incivility were greater than the significant value of .05 which were interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, lack of respect, displaced frustration, and overall patient incivility were not significantly correlated with task performance. This means that a high level of task performance can still be achieved despite high levels of lack of respect, displaced frustration, and overall patient incivility. It only shows that despite that incivility shown by the patients, nurses are able to maintain their composure, they know too well how to handle their patients. They understand too well their patients that if they show incivility, it is not directed to them but to the situation that patients are in. Nurses show professionalism in dealing with their patients and that they respect their patients, they advocate for them and they make sure that everything they do is for the benefit of the patient.
Overall Workplace Incivility. Overall workplace incivility was not significantly correlated with task performance. This was supported by the finding of p value which was greater than the significant value of .005 which led to the decision of failing to reject the null hypothesis. This means that a high level of task performance can still be achieved despite high levels of workplace incivility. It would imply that incivilities may be considered as part of work and that if they are being handled professional through proper communication and professionalism, they can be resolved and therefore cannot affect the work of nurses. Nurses work for the patients and they make sure that they do this at all cost.
Contrary to findings, the study’s findings rejected hypotheses one and two showing workplace incivility (WPI) has a detrimental effect on employee engagement and employee performance (Singh et al., 2023). Also, the results of the study of Saleem et al. (2022) affirmed that incivility is harmful to the performance of employees, and that trust in supervisors helps employees to perform well. The trust in the supervisor significantly mediates the incivility–performance relationship.
Contextual Performance
General Incivility. General incivility was significantly correlated with contextual performance. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was weak and negative. This means that the lower the general incivility, the higher the contextual performance. Indeed, there is better performance from the nurses as their time is fully allocated to the performance of their jobs. Incivility can cause conflicts and take valuable time of the nurses, instead of caring for patients, time will be allocated to solving the incivility. Thus, in the absence of incivility, nurses will be able to have concentration and therefore become more productive.
More specifically, hostile climate and inconsiderate behavior of general incivility were significantly correlated with contextual performance as evidenced by the p values of lesser than .005. These values were interpreted as significant which led to the rejection of the null hypothesis. The correlation with hostile climate and inconsiderate behavior were weak negative. This means that the lower the hostile climate and inconsiderate behavior, the higher the contextual performance. There is no room for a hostile climate and inconsiderate behavior. These are two negative things that will hinder nurses to become productive. A working environment that fosters good relationship and appropriate behavior will greatly contribute to productivity.
However, the p value for inappropriate joke of general incivility was greater than the significant value of .05 which was interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, inappropriate joke of general incivility was not significantly correlated with contextual performance. This means the contextual performance can still be high despite high levels of inappropriate jokes. Inappropriate jokes are not welcomed in the wards. The nature of the clients that nurses are handling cannot be subjected to any inappropriate jokes. In reality, it can cost the life of a patient.
Nurse Incivility. Nurse incivility was significantly correlated with contextual performance. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was weak negative. This means that the lower the nurse incivility, the higher the contextual performance. Members of the nursing department work collaboratively and they work together as a team. They work harmoniously with each other as evidenced by not having issues or conflicts among them.
More specifically, gossip and rumors were significantly correlated with contextual performance as evidenced by the p value of lesser than .005. This value was interpreted as significant which led to the rejection of the null hypothesis. The correlation with gossip and rumors was weak negative. This means that the lower the gossip and rumors, the higher the contextual performance of the nurses. Gossips and rumors do not bring any good. These are baseless information and purely a waste of time. Nurses cannot afford to waste their time. Instead of gossiping, nurses would rather do bedside care and become more productive.
However, the p values for hostile climate and free-riding were greater than the significant value of .05 which were interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, hostile climate and free-riding of nurse incivility were not significantly correlated with contextual performance. This means that contextual performance can still be high despite high levels of hostile climate and free-riding. A hostile climate and free-riding are two negative things that nurses would rather not be in. Caring for patients does not require a hostile climate nor allow free-riding by nurses. These are two unproductive situations which will not contribute to the nurses being contextually productive.
Supervisor Incivility. Supervisor incivility was significantly correlated with contextual performance. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was weak negative. This means that the lower the supervisor incivility, the higher the contextual performance. Supervisors are vital to managing the nursing department. They led the team and if they practice incivility, it will cause chaos. It is important that supervisors are professional in their leading and management for nurses to become more productive.
More specifically, abusive supervision was significantly correlated with contextual performance as evidenced by the p value of lesser than .005. This value was interpreted as significant which led to the rejection of the null hypothesis. The correlation with abusive supervision was weak negative. This means that the lower the abusive supervision, the higher the contextual performance. As mentioned before none of the supervisors are abusive. They know the metes and bounds of their being a supervisor and they practice ethics in supervising their team. With this, they allow nurses to be more productive.
However, the p value for lack of respect was greater than the significant value of .05 which was interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, lack of respect of supervisor incivility was not significantly correlated with contextual performance. This means that a high level of contextual performance can still be achieved despite high levels of lack of respect. As mentioned before, respect is very important in a team. Without it, there can be no collaboration. Poor collaboration means that nurses will not be able to carry out their respective jobs in the team.
Physician Incivility. The p value for lack of respect was lesser than the significant value of .05 which was interpreted as significant which led to the decision of rejecting the null hypothesis. Thus, lack of respect of physician incivility was significantly correlated with contextual performance. The correlation with lack of respect was moderate negative. This means that the lower the lack of respect, the higher the contextual performance. Relationship is essential in every relationship and that respect begets respect. Respect will allow or foster good working relationship where the nurse opinions are respected as well as the doctor’s. There is better communication which are all for the benefit of the patient.
However, the p value for abusive supervision and overall physician incivility were greater than the significant value of .05 which were interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, abusive supervision and overall physician incivility were not significantly correlated with contextual performance. This means that a high level of contextual performance can still be achieved despite high levels of abusive supervision and overall physician incivility. Though based on the observation of the researcher, doctors are never abusive to nurses. They know that they have to work hand-in-hand with nurses as they are the professionals who carry their orders. By establishing good relationship with nurses, collaboration and discussions will be easy for the management and benefit of their patients.
Patient Incivility. Patient incivility was significantly correlated with contextual performance. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was strong positive. This means that contextual performance is high with high patient incivility.
The incivility may be brought about by the fact that the patient is facing a health problem. This could be brought about by denial and anger and nurses are trained on how to address this grieving process that the patient is undergoing. The nurses understand that this is just a phase that patients go through and thus, nurses should never give-up but instead do more to be more empathetic and caring for these patients.
More specifically, lack of respect and displaced frustration of patient incivility were significantly correlated with contextual performance as evidenced by the p values of lesser than .005. These values were interpreted as significant which led to the rejection of the null hypothesis. The correlation with lack of respect was moderate negative while for displaced frustration was strong positive. High levels of contextual performance is very possible with low levels of lack of respect and displaced frustration. When there is respect and no frustration from the patients, nurses will be able to develop good working relationship with their patients. They can work with their patients collaboratively, they allow patients to be part of their care and therefore will allow productivity of the nurses.
Overall Workplace Incivility. Overall workplace incivility was not significantly correlated with contextual performance. This was supported by the finding of p value which was greater than the significant value of .005 which led to the decision of failing to reject the null hypothesis. High contextual performance is achievable despite the high levels of work place incivility. Incivility is one of the things that nurses encounter in the workplace. However, despite the presence of workplace incivility, they cannot compromise their patients. Nurses tend to ignore the presence of incivilities, if not, bring these incivilities through proper channeling and proper forum to be addressed. The periodic meetings held in the hospitals especially on the nursing department is a great way to address incivilities. They can be raised, discussed and addressed professionally. As professional individuals, nurses know how to prioritize and deal with incivilities.
Contrary to the findings, the findings of the study of Aruoren and Ugbeghene (2023) revealed that workplace incivility was negatively related to both task and adaptive performance, but only significantly related to task performance. Furthermore, workplace incivility was found to be positively related to counterproductive work behavior and contextual performance, however, this relationship was only significant for counterproductive work behavior.
Counterproductive Work Behavior
General Incivility. General incivility was significantly correlated with counterproductive work behavior. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was weak and positive. This means that the lower the general incivility, the lower the counterproductive work behavior. When there is a positive working environment and absence of incivility, nurses will not be bothered in the performance of their tasks. There will be no hindrance to performing their duties. This way they can think of better ways to help their patients. This is evidently shown to be true also in relation to the previous table where counterproductive work behavior was low.
More specifically, hostile climate and inconsiderate behavior of general incivility were significantly correlated with counterproductive work behavior as evidenced by the p values of lesser than .005. These values were interpreted as significant which led to the rejection of the null hypothesis. The correlation with hostile climate was moderate positive while for inconsiderate behavior was weak positive. This means that the lower the hostile climate and inconsiderate behavior, the lower the counterproductive work behavior. Consequently, when the working environment is non-hostile an there is an absence of inconsiderate behaviors, these will allow a smooth execution of the nurses’ job. They become more productive.
However, the p value for inappropriate joke of general incivility was greater than the significant value of .05 which was interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, inappropriate joke of general incivility was not significantly correlated with counterproductive work behavior. This means that a low counterproductive work behavior is made possible even the presence of high inappropriate jokes. Jokes are not meant to be taken seriously. Nurses are mature individuals, they know when a joke is given or delivered. At the end of the day, they are always after the welfare of their patients. So despite the jokes, prioritizing the patient’s welfare cannot be compromised.
Nurse Incivility. Nurse incivility was significantly correlated with counterproductive work behavior. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was moderate positive. This means that with low nurse incivility, there is also low counterproductive work behavior. It only means that there is no hindrance to performing their work. Incivility ca greatly take the time of nurses and without it, they can focus more on helping their patients. This way they become more helpful and productive at the same time.
More specifically, hostile climate, gossip and rumors, and free-riding of nurse incivility were significantly correlated with counterproductive work behavior as evidenced by the p values of lesser than .005. These values were interpreted as significant which led to the rejection of the null hypothesis. The correlation with hostile climate and free-riding were weak positive while for gossip and rumors was moderate positive. This means that with low hostile climate, gossip and rumors, and free-riding, there is also low counterproductive work behavior. When one gossips or spread rumors, he or she is just wasting his or her time. One cannot be productive by doing these things, in the same way as doing free-riding. Similarly, creating a hostile environment will only cause strained relationships and thus, will not promote better coordination and collaboration. If all these are eliminated then nurses would be more productive.
Supervisor Incivility. Supervisor incivility was significantly correlated with counterproductive work behavior. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was moderate positive. This means that with low supervisor incivility, there is also low counterproductive work behavior. When supervisors are positively providing support to the nurses, this will induce nurses to be more participative and will create enthusiasm to do their jobs. This way they become more productive.
More specifically, abusive supervision and lack of respect of supervisor incivility were significantly correlated with counterproductive work behavior as evidenced by the p values of lesser than .005. These values were interpreted as significant which led to the rejection of the null hypothesis. The correlation with abusive supervision and lack of respect were moderate positive. This means that with low abusive supervision and lack of respect, there is also low counterproductive work behavior. When nurses are given due respect and not abused, this will allow them to work independently and interdependently. Thus, they become more productive.
Physician Incivility. Physician incivility was significantly correlated with counterproductive work behavior. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was moderate positive. This means that with low physician incivility, there is also low counterproductive work behavior. Doctors act as team leaders in the healthcare team. If they become abusive and do not respect nurses, nurses will not cooperate or collaborate with them. So if nurses are given the right amount of respect, then they will get the cooperation of the nurse and they can work as a team.
More specifically, abusive supervision and lack of respect of physician incivility were significantly correlated with counterproductive work behavior as evidenced by the p values of lesser than .005. These values were interpreted as significant which led to the rejection of the null hypothesis. The correlation with abusive supervision and lack of respect were moderate positive. This means that with low abusive supervision and lack of respect, there is also low counterproductive work behavior.
Absence of abuse and presence of respect are two ingredients that will foster good working relationship. If doctors are able to show these to nurses, for sure they will get the same respect and cooperation from the nurses. They will be able to work with them and nurses will become more productive.
Patient Incivility. Patient incivility was significantly correlated with counterproductive work behavior. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was moderate positive. This means that with low patient incivility, there is also low counterproductive work behavior. If patients will collaborate and cooperate with the nurses, this will greatly help. Patients will gain autonomy and develop a sense of respect and belongingness. They will eagerly cooperate in his or her management or care and in return allows nurses to be more helping and more productive.
More specifically, lack of respect of patient incivility was significantly correlated with counterproductive work behavior as evidenced by the p value of lesser than .005. This value was interpreted as significant which led to the rejection of the null hypothesis. The correlation with lack of respect were moderate positive. This means that with low lack of respect, there is also low counterproductive work behavior. Wherever one goes, with respect, one goes a long way. Though respect is earned, it should be essential in a nurse-patient relationship. By respecting each other, they will be able to take their respective roles in the care or management of the patient. They will not only be able to establish a good partnership but also help in the fast recovery of the patient through the productivity of the nurse.
However, the p value for displaced frustration was greater than the significant value of .05 which was interpreted as not significant which further led to the decision of failing to reject the null hypothesis. Thus, displace frustration of patient incivility was not significantly correlated with counterproductive work behavior. This means that a low counterproductive work behavior is possible despite the high levels of displaced frustration. Frustration will not have positive effects. With frustration, this will only allow patients not to cooperate in his or her care. The patient becomes difficult to handle. If frustration will be removed, this will allow patients to be more participative in his care and this will facilitate the nurse to be more productive.
Overall Workplace Incivility. Overall workplace incivility was significantly correlated with counterproductive work behavior. This was supported by the finding of p value which was lesser than the significant value of .005 which led to the rejection of the null hypothesis. The correlation was moderate positive. A low level of counterproductive work behavior is achievable with a low workplace incivility.
Supporting the findings, coworker incivility and customer incivility reduced work engagement and job performance. The effects of coworker incivility on the work engagement and job performance are greater than those of customer incivility. Furthermore, work engagement has a positive effect on the job performance (Wang & Chen, 2020).
It is just right that in the absence of any incivility, nurses will be able to perform their tasks well. They will have no problems with dealing with their colleagues and with their patients or clients. When everything goes smoothly In the ward or in the workplace, nurses become productive and they will be able to deliver. Collaboration and coordination will be very possible, thus, they become productive individuals who contributes to the hospital’s goals, and mission and vision.
Relationship between Organizational Citizenship Behavior and Work Performance
Table 6 is the presentation of the data on whether organizational citizenship behavior is significantly correlated with work performance.
Table 6 Relationship between Organizational Citizenship Behavior and Work Performance
| Variables | r value | p value | Decision | Interpretation |
| Organizational Citizenship Behavior vs. Task Performance | .425 | .001 | Reject Ho | Significant |
| Organizational Citizenship Behavior vs. Contextual Performance | .502 | .000 | Reject Ho | Significant |
| Organizational Citizenship Behavior vs. Counterproductive Work Behavior | .145 | .266 | Failed to reject Ho | Not significant |
Legend: Significant if p value is < .05. Dependent Variable: Work Performance. Pearson r interpretation: A value greater than .5 is strong (positive), between .3 and .5 is moderate (positive), between 0 and .3 is weak (positive), 0 is none, between 0 and –.3 is weak (negative), between –.3 and –.5 is moderate (negative), and less than –.5 is strong (negative).
The table shows that the p value for the relationship between organizational citizenship behavior and task performance was lesser than the significant value of .05. This value was interpreted as significant leading to the decision of rejecting the null hypothesis. Thus, organizational citizenship behavior was significantly correlated with task performance. The correlation was moderate positive. This means that the higher the organizational citizenship behavior, the higher the task performance.
Organizational citizenship behavior develops a sense of belongingness. When nurses feel that they belong to the team, this triggers them to perform their tasks and contribute to the welfare of their patients. Organizational citizenship behavior also fosters good relationship and collaboration. Nurses become more of a team player and contributes to the team for the betterment of their patients.
Asgari et al. (2020) as cited in Luthfiyana et al. (2024) research showed organizational support plays a vital role in promoting task performance and OCB among secondary school teachers, providing insight for principals to design strategies for continuous quality improvement that will improve the Employee Performance of teachers. Tahir (2015) as cited in Luthfiyana et al. (2024) highlighted the importance of understanding the interaction between psychological empowerment, organizational citizenship behavior, and task performance to improve employee and organizational outcomes.
Also, the table shows that the p value for the relationship between organizational citizenship behavior and contextual performance was lesser than the significant value of .05. This value was interpreted as significant leading to the decision of rejecting the null hypothesis. Thus, organizational citizenship behavior was significantly correlated with contextual performance. The correlation was strong positive. This means that the higher the organizational citizenship behavior, the higher the contextual performance.
Similarly, nurses become more involved with their jobs if they develop high level of organizational citizenship behavior. A feeling of belongingness can be developed through the conduct of organizational citizenship. It is easier for nurses to carry out their duties and make a positive contribution to the well-being of their patients when they have the sense that they are a part of the organization. Behavior that demonstrates organizational citizenship also helps to build positive relationships and teamwork. Nurses develop a greater capacity for teamwork and contribute to the team in order to improve the quality of care they provide to their patients.
The study of Abun et al. (2021) found that organizational citizenship, the work performance of employees and the work environment is high and there is a significant correlation between organizational citizenship behavior and work performance and there is a correlation between work environment and organizational citizenship behavior and work performance. Therefore, the hypothesis of the study is accepted.
OCB on Employee Performance is related to task performance, organizational justice, job satisfaction, organizational performance, and organizational culture. OCB on Employee Performance is related to Task Performance, where OCB refers to voluntary behavior performed by employees outside of their official or formal duties. Meanwhile, employee performance can be divided into two main aspects: task performance and overall organizational performance. OCB can influence both organizational and individual contexts, improve teamwork by promoting a positive and supportive atmosphere in the workplace, and impact employees to complete their tasks correctly (Luthfiyana et al., 2024).
Lastly, the table shows that the p value for the relationship between organizational citizenship behavior and counterproductive work behavior was greater than the significant value of .05. This value was interpreted as not significant leading to the decision of failing to reject the null hypothesis. Thus, organizational citizenship behavior was not significantly correlated with counterproductive work behavior. A low counterproductive behavior can still be achieved despite the low levels of organizational citizenship behavior.
Contrary to the findings, the results in the study of Triani et al. (2020) showed that organizational citizenship behavior has a positive and significant effect on employee performance. The results of study revealed that occupational efficacy (OE) emerged as an antecedent of OCB in predicting performance. In study two, OCB positively predicted employee performance above and beyond and the effects of their managers’ tenure in position, and Collective Efficacies (CEs). In addition, both employees’ and managers’ CEs moderated the effects of OCB on performance: the performance effects of OCB increased as employees’ and managers’ CE increased, and specifically performance efficiency and performance creativity (Yaakobi & Weisberg, 2020).
Nurses will never be counterproductive in the absence or presence of a high level of organizational citizenship behavior. Though it can be implied that organizational citizenship behavior is a tool that can help develop collaboration and good working relationship. But at the end of the day, the nurses cannot be counterproductive, as patients are more important. Caring for patients is why nurses are there.
CONCLUSION AND RECOMMENDATIONS
Conclusion
In conclusion, workplace incivility is influenced by organizational citizenship behavior. The higher the organizational citizenship behavior the lower the workplace incivility. Further, task and contextual performance are not influenced by workplace incivility but counterproductive work behavior is influenced by workplace incivility. There can still be high task and contextual performance despite the presence of work incivility while counterproductive work behavior is low when workplace incivility is also low. Furthermore, task and contextual performance are influenced by organizational citizenship behavior while counterproductive work behavior does not. This means that the higher the organizational citizenship behavior, the higher the task and contextual performance, whereas a high counterproductive work behavior is not dependent on the level of organizational citizenship behavior.
The findings affirmed the use of the Social Exchange Theory which analyzed relationships and human behavior relating to the organizational citizenship behavior of the nurses which was high. Further, the findings affirmed the Workplace Incivility Theory where uncivil behaviors were experienced by the nurses in general, from co-nurses, from supervisors, from physicians to be low and from patients to be moderate. Lastly, The findings affirmed the Heuristic Conceptual Framework of Individual Work Performance where the performance of the nurses were high task performance, high contextual performance, and low counterproductive work behavior. To address the findings of the study a performance enhancement plan is proposed.
Recommendations
Nursing Practice. It is important that this research be utilized by making sure that the output of the study will be recommended for use by the hospital where the study was conducted. But prior to the recommendation, the study will be presented in the nursing department along with the hospital administrators to disseminate the findings of the study. Other healthcare institutions may also adopt the output in part or in whole as they deemed it proper and applicable to their respective institutions. When such plan is already available, it may call for the review and revision of the already established staff development, operational, and strategic plans of the institution.
Nursing Policy. As a matter of policy, the findings will greatly support modifications and creation of new national and even institutional policies that protects the welfare of the nurses by looking into the aspects of organizational citizenship behavior, workplace incivility, and work performance. Policies punishing acts of workplace incivility may also be updated to include all aspects therein. Also, policies on performance evaluation may also be modified to include the utilization of the standard tool.
Nursing Education. This study will be a good contribution to the field of research as the entire study can serve as a reference where topics relating to organizational citizenship behavior, workplace incivility, and work performance. The findings can serve as a supporting study and a resource material such as activities requiring students to make a reaction paper. The statistical treatments being used can serve as an example when discussing statistics. Also, the ethical considerations observed can also be a reference in discussing ethics in research.
Nursing Research. To disseminate the findings of the study, the study abstract will be posted in Facebook to allow researcher get a glimpse what the study is all about. It will further be submitted for publication in a refereed journal either local or international. Lastly, it will be submitted for either a possible oral or poster presentation in any local or international research forum. Further research should explore why this occurs, its psychological effects on nurses, and strategies to mitigate it. The following research titles are also suggested for future researchers to undertake:
- Organizational citizenship behavior and workplace incivility as predictors of work performance among nurses;
- Personal characteristics influencing organizational citizenship behavior, workplace incivility, and work performance among nurses;
- A comparative analysis on the organizational citizenship behavior, workplace incivility, and work performance among public and private nurses; and
- A meta-analysis on the workplace incivility among nurses.
PERFORMANCE SUSTENANCE PLAN
Rationale
Increased job performance and enthusiasm in the workplace are two outcomes that can be brought about by organizational citizenship behavior, which can have an effect on how a person handles a task. The person is able to tackle a challenge from a different and creative perspective if he has a more open and cheerful mindset. Another way for them to obtain further information is by working together as a team. On the contrary, there is a growing prevalence of rudeness, rage, and toxic behavior in health care settings, which may be a reflection of the trends that are occurring. The obligation to protect employees from potentially harmful and abusive contacts with patients, family members, and members of the general public, as well as with coworkers, falls on organizations that provide health care services. Despite the fact that it is impossible to anticipate everything, it is necessary to take measures to ensure the physical and mental safety of each and every employee. Lastly, performing well at work is not simply about meeting deadlines and completing tasks; rather, it is about thriving in the sector that you have chosen and discovering fulfillment in the efforts that you make on a daily basis. Your capacity to accomplish your objectives, make a positive contribution to the success of your organization, and advance professionally are all included in it. Findings of the study revealed a need to sustain the high levels of organizational citizenship behavior, low levels of workplace incivility, and high levels of work performance. Thus, the creation of this sustenance plan.
General Objectives
The main purpose of this sustenance plan is to sustain high levels of organizational citizenship behavior, low levels of workplace incivility, high levels of work performance of nurses.
Specific Objectives
Specifically, this sustenance plan aims to achieve the following specific objectives, to wit:
- To decrease the moderate level of patient/visitor incivility experienced by nurses;
- To sustain the low levels of general incivility, nurse incivility, supervisor incivility, and physician incivility or decrease to very low level;
- To sustain the high level of organizational citizenship behavior or improve to very high level among nurses;
- To sustain the high levels of task performance and contextual performance or improve to very high among nurses;
- To sustain the very low level of counterproductive work behavior among nurses;
- To sustain the very low level of supervisor incivility while sustaining the very high level of task performance among nurses;
- To sustain the very low levels of general incivility, nurse incivility, supervisor incivility, and patient incivility while sustaining a very high level of contextual performance among nurses; and
- To sustain the very low levels of general incivility, nurse incivility, supervisor incivility, and patient incivility while sustaining a very low level of counterproductive work behavior among nurses; and
- To sustain the very high level of organizational citizenship behavior while sustaining a very high level of task performance and contextual performance among nurses.
| Concern | Specific Objectives | Activities | Persons responsible | Resources | Time Frame | Success indicators |
| · Patient/visitor incivility being moderate | · To decrease the moderate level of patient/visitor incivility experienced by nurses. | Hospital-initiated activities:
· Implement safety training for nurses. · Provide a create a support group for nurses. · Provide activities in the ward that create awareness of patient incivility. · Provide leaflets about patient incivility to patients and visitors. · Re-assess the level of patient incivility six months following the implementation of this plan. |
· Patients/Visitors
· Staff Nurses · Nurse Supervisors · Chief Nurse · HRDM Director · Hospital Administrators |
· Budget for the safety training (Php 10,000.00).
· Support group. · Visual aides. · Leaflets. · Evaluation forms. · Instrument to measure workplace incivility. |
· First quarter of 2025 | · Approved schedule for the safety training.
· Created a group chat for the support group. · Patient evaluation of the awareness program. · Re-assessment result – very low to low levels of patient incivility. |
| · The need to sustain the low levels of general incivility, nurse incivility, supervisor incivility, and physician incivility. | · To sustain the low levels of general incivility, nurse incivility, supervisor incivility, and physician incivility or decrease to very low level. | Personally-initiated activities:
· Institute de-escalation strategies like taking time-out, not taking things personally and by being proactive. · Avoid gossips and rumors. · Read articles or view videos about workplace incivility. · Attend seminars about workplace incivility.
Hospital-initiated activities: · Conduct a seminar on Establishing Good Working Relationships, Teamwork and Collaboration. · Conduct a seminar about: Respect begets respect and the Dangers of Gossips and Rumors. · Conduct a seminar about Maintaining Composure Despite the Odds in Healthcare. · Conduct a seminar on the 8 Habits of an Effective Person. · Issue a memorandum about encouraging other caregivers to take breaks when they can and promote self-awareness and gratitude. · Update bulletin or Facebook account about ways to avoid incivility through the use of infographics. · Establish a strict zero-tolerance policy for violence, in addition to behavioral guidelines following the Code of Ethics for healthcare professionals through the development of a standard operating procedures and policies (SOPPs). · Provide education and continuing education programs. · Provide counseling programs for stress management and conflict resolution. · Conduct seminar on Cope with Disruptive or Inappropriate Behaviors at Work. · Conduct seminar on Stress Management and Conflict Resolution. · Create a reporting system for incivility cases and closely monitor those incidents. · Advocate for open communication between leadership and staff to improve trust and help support resolution of inappropriate behavior. · Educate leaders on how to act as role models of appropriate behavior through a seminar-workshop. · Conduct periodic meetings to raise issues on incivility. · Re-assess the level of workplace incivility six months following the implementation of this plan. |
· Staff Nurses
· Nurse Supervisors · Chief Nurse · Physicians · Hospital Employees · HRDM Director · Hospital Administrators |
· Internet connectivity.
· Desktops, laptops, tablets or android phones. · Leave credits. · Budget for every seminar or training or webinar (Php 10,000.00) · Nursing Service DEvelopment Plan. · Bulletin board and Facebook account. · Memorandum · Instrument to measure workplace incivility. |
· First quarter of 2025 | · Saved articles or videos.
· Certificate of attendance or participation in the webinar or seminar. · Issued memorandum. · Developed and updated SOPPs. · Updated Nursing Service Development Plan. · Updated bulletin board and Facebook account. · Counselling records. · SOPPS on incivility reporting. · Minutes of the meetings. · Re-assessment results – sustained low to very low workplace incivility in all dimensions. |
| · The need to sustain the high level of organizational citizenship behavior | · To sustain the high level of organizational citizenship behavior or improve to very high level among nurses. | Personally-initiated activities:
· Read articles or view videos about organizational citizenship behavior. · Attend webinars or seminars about organizational citizenship behavior. · Make use of leave credits wisely. · Practice positive reinforcements and gratitude.
Hospital-initiated activities: · Provide standard operating procedures and policies on advising, coaching, or mentoring programs especially to new hires. · Conduct a seminar for nurses about The 4 C’s of Nursing (caring, Commitment, Competence, and Compassion · Conduct a seminar about Organizational Citizenship Behavior of Nurses · Conduct a seminar on Sympathy versus Empathy. · Provide a policy on request for change of shift. · Conduct a seminar on the Art of Delegation, Teamwork and Collaboration · Re-orientation of the Philippine Nursing Act of 2002, Code of Ethics for Nurses and Code of Conduct Government Employees · Provide a support group for nurses. · Conduct periodic meetings to allow suggestions and recommendations on how to improve work. · Re-assessment of the organizational citizenship behavior six months following the implementation of this plan. |
· Staff Nurses
· Nurse Supervisors · Chief Nurse · HRDM Director · Hospital Administrators |
· Internet connectivity.
· Desktops, laptops, tablets or android phones. · Leave credits. · SOPPs · Budget for the seminars (Php 10,000.00 for every seminar). · Policy on request for change of shift. · Support group in Facebook. · Instrument to measure organizational citizenship behavior. |
· First quarter of 2025 | · Saved articles or videos.
· Certificate of attendance or participation in the webinar or seminar. · Approved leaves. · · · Approved policy on change of shift. · Created support group. · Minutes of the meetings · Re-assessment results – sustained high to very high organizational citizenship behavior. |
| · The need to sustain the high levels of task performance and contextual performance.
· The need to sustain the very low level of counterproductive work behavior. |
· To sustain the high levels of task performance and contextual performance or improve to very high.
· To sustain the very low level of counterproductive work behavior among nurses. |
Personally-initiated activities:
· Read articles or videos about how to increase performance and be productive. · Attend webinars and seminars relating to productivity as a nurse. Hospital-initiated activities: · Provide a re-orientation of the job description and provide a copy to the nurses. · Re-orient nurses about the metrics for the performance evaluation. · Create an environment that supports and promotes constructive organizational citizenship behavior. · Conduct seminar on Good Behavior at Workplace · Revisit, review, and revise reward system. · May need to revisit, review, and revise performance evaluation and integrate organizational citizenship behavior. · Train nurses on the use of organizational citizenship behavior and include the benefits. · Conduct periodic meetings to discus organizational citizenship behavior concerns. · Re-assess the organizational citizenship behavior six months following the implementation of this plan. |
· Staff Nurses
· Nurse Supervisors · Chief Nurse · HRDM Director · Hospital Administrators |
· Internet connectivity.
· Desktops, laptops, tablets or android phones. · Copies of Job Descriptions. · Policy on reward system. · Performance evaluation forms. · Instrument to measure organziational citizenship behavior |
· First quarter of 2025 | · Saved articles or videos.
· Certificate of attendance or participation in the webinar or seminar. · Revised reward system. · Revised performance evaluation form. · Received copies of job descriptions. · Re-orientation attendance reports. · Minutes of the meeting · Re-assessment results – sustained high to very high task and contextual performance and low to very low counterproductive work behavior. |
| · supervisor incivility was significantly correlated with task performance.
· General incivility, nurse incivility, supervisor incivility, and patient incivility were significantly correlated with contextual performance. · General incivility, nurse incivility, supervisor incivility, physician incivility and patient incivility were significantly correlated with counterproductive work behavior. · Organizational citizenship behavior was significantly correlated with task performance and contextual performance. |
· To sustain the very low level of supervisor incivility while sustaining the very high level of task performance among nurses.
· To sustain the very low levels of general incivility, nurse incivility, supervisor incivility, and patient incivility while sustaining a very high level of contextual performance among nurses. · To sustain the very low levels of general incivility, nurse incivility, supervisor incivility, and patient incivility while sustaining a very low level of counterproductive work behavior among nurses. · To sustain the very high level of organizational citizenship behavior while sustaining a very high level of task performance and contextual performance among nurses. |
· Note: All activities mentioned in all the concerns are applicable here. | · Note: All persons responsible mentioned in all the concerns are applicable here. | · Note: All resources mentioned in all the concerns are applicable here. | · First quarter of 2025. | · Note: All success indicators mentioned in all the concerns are applicable here. |
REFERENCES
- Abdollahzadeh, F., Asghari, E., Ebrahimi, H., Rahmani, A., & Vahidi, M. (2017). How to prevent workplace incivility?: Nurses’ perspective. Iranian Journal of Nursing and Midwifery Research, 22(2), 157–163. https://doi.org/10.4103/1735-9066.205966
- Abun, D., Basilio, G., Magallanes, T., Encarnacion, M. J., & Sallong, M. (2021). Examining the link between organizational citizenship behavior and work performance of employees in the private schools, mediated by workplace environment. International Journal of Research in Business and Social Science (2147- 4478), 10, 85-98. https://doi.org/10.20525/ijrbs.v10i4.1229
- Abun, D., Nicolas, M. T., Apollo, E., Magallanes, T., & Encarnacion, M. J. (2021). Employees’ self-efficacy and work performance of employees as mediated by work environment. International Journal of Research in Business and Social Science, 10, 01 – 15. https://doi.org/ff10.20525/ijrbs.v10i7.1470ff
- Alabbas, A. M., & Mahran, S. M. (2023). Nurse’s perspective of organizational citizenship behavior during the COVID-19 pandemic in Saudi Arabia. Evidence-Based Nursing Research, 5(2), 35-44. http://doi.org/10.47104/ebnrojs3.v5i2.286.1
- Alquwez, N. (2020). Examining the influence of workplace incivility on nurses’ patient safety competence. Journal of Nursing Scholarship, 52(3), 292-300. https://doi.org/10.1111/jnu.12553
- Altuntas, S., & Baykal, U. (2010). Relationship between nurses’ organizational trust levels and their organizational citizenship behaviors. Journal of Nursing Scholarship, 42, 186 – 194. https://doi,org/10.1111/j.1547-5069.2010.01347.x
- Annalakshmi, N. ., Roshni, P., Abhirami, S., & Udita, P. (2022). The consequence of workplace incivility among IT employees: Workplace stress or organizational citizenship behavior? Humanitas: Indonesian Psychological Journal, 19(1), 51–66. https://doi.org/10.26555/humanitas.v19i1.6
- Andersson, L. M., & Pearson, C. M. (1999). Tit for tat? The spiraling effect of incivility in the workplace. Academy of Management Review, 24,452– 471.
- Armstrong, N. (2018). Management of nursing workplace incivility in the health care settings: A systematic review. Workplace Health Safety, 66(8), 403-410. https://doi.org/10.1177/2165079918771106
- Aruoren, E. E., & Ugbeghene, J. (2023). Relationship between workplace incivility and employee performance. International Journal of Academic Research in Business and Social Sciences, 13(6), 927 – 942.
- Ateş, N., Erdal, N., & Harmancı Seren, A. K. (2023). The relationship between critical thinking and job performance among nurses: A descriptive survey study. International Journal of Nursing Practice, 29(5), e13173. https://doi.org/10.1111/ijn.13173
- Bhandari, P. (2023). Correlational research. When and how to use. https://www.scribbr.com/methodology/correlational-research/#:~:text=What%20is%20correlational%20research%3F,experimental%20type%20of%20quantitative%20research.
- Bjaalid, G., Olsen, E., Melberg, K., & Mikkelsen, A. (2020). Institutional stress and job performance among hospital employees. International Journal of Organizational Analysis, 28(2).
- Bollen, K., & Lennox, R. (1991). Conventional wisdom on measurement: A structural equation perspective. Psychological Bulletin, 110, 305-314.
- Chib, S. (2016). Study on organizational commitment and workplace empowerment as predictors of organization citizenship behavior. International Journal of Management & Development, 3(3). https://doi.org/10.19085/journal.sijmd030301.
- Daba, L., Beza, L., Kefyalew, M., Teshager, T., Wondimneh, F., Bidiru, A., & Ketema, I. (2024). Job performance and associated factors among nurses working in adult emergency departments at selected public hospitals in Ethiopia: a facility-based cross-sectional study. BMC Nursing, 23, 312. https://doi.org/10.1186/s12912-024-01979-w
- Dalal, R. S. (2005). A meta-analysis of the relationship between organizational citizenship behavior and counterproductive work behavior. Journal of Applied Psychology, 90, 1241-1255.
- Dirdjo, M., Syahab, S., Sureskiarti, E., & Suwanto, S. (2023). Job satisfaction and nurse performance. Jurnal Ilmu Kesehatan, 11, 25-40. https://doi.org/10.30650/jik.v11i1.3700
- Doloh, N., Tamtomo, D., & Sulaeman, E. S. (2018). Factors affecting work performance among nurses in delivering health service for the National Health Insurance patients at Dr. Moewardi Hospital, Surakarta. Journal of Health Policy and Management, 3(1), 20-25. https://doi.org/10.26911/thejhpm.2018.03.01.03
- Edwards, J. R., & Bagozzi, R. P. (2000). On the nature and direction of relationships between constructs and measures. Psychological Methods, 5, 155-174.
- European Commission (2010). Europe 2020: A strategy for smart, sustainable and inclusive growth. European Commission.
- Fox, S., Spector, P. E., Goh, A., Bruursema, K., & Kessler, S. R. (2009). The deviant citizen: Clarifying the measurement of organizational citizenship behavior and its relation to counterproductive work behavior. Loyola University Chicago.
- Fox, S., Spector, P. E., Goh, A., Bruursema, K., & Kessler, S. R. (2012). The deviant citizen: Measuring potential positive relations between counterproductive work behaviour and organizational citizenship behaviour. Journal of Occupational and Organizational Psychology, 85, 199-220.
- Fox, S., Spector, P. E. (2011). Organizational Citizenship Behavior – Checklist. https://paulspector.com/assessments/pauls-no-cost-assessments/organizational-citizenship-behavior-checklist-ocb-c/
- Gillian, L. A. (2015). Exploring incivility among registered nurses in the hospital setting. [Unpublished thesis type] Nursing Theses and Capstone. Projects. 221. https://digitalcommons.gardner-webb.edu/nursing_etd/221.
- Griffin, M. A., Neal, A., & Parker, S. K. (2007). A new model of work role performance: positive behavior in uncertain and interdependent contexts. Academy of Management Journal, 50, 327–347.
- Guidroz, A., Geimer, J., Clark, O., Schwetschenau, H., & Jex, S. (2010). The Nursing Incivility Scale: Development and validation of an occupation-specific measure. Journal of Nursing Measurement, 18, 176-200. https://doi.org/10.1891/1061-3749.18.3.176
- Hershcovis, M. S. (2011). Incivility, social undermining, bullying . . . ohmy!: A call to reconcile constructs within workplace aggression re-search. Journal of Organizational Behavior, 32, 499 –519. http://dx.doi.org/10.1002/job.689
- Hossain, M. (2020) Organizational Citizenship Behavior and Organizational Commitment among Clinical Nurses in Bangladesh. Open Journal of Nursing, 10, 693-704. https://doi.org/10.4236/ojn.2020.107049
- Hutton, S, & Gates, D. (2018). Workplace incivility and productivity losses among direct care staff. American Association of Occupational Health Nurses Journal, 56, 168–75.
- Indeed (2024). Recognizing Social Exchange Theory in the workplace. https://www.indeed.com/hire/c/info/social-exchange-theory#:~:text=Social%20exchange%20theory%20is%20essentially,within%20a%20multitude%20of%20relationships
- Ibrahim, M., Mohamed Zakaria, A., Moustafa, A., & Ghani, A. (2023). Work related stress and job performance among staff nurses introduction. Mansoura Nursing Journal, 10. https://doi.org/10.21608/mnj.2023.340376
- Joshi, R. M. (2009). International business. Oxford University Press. Keller, S., Yule, S., Zagarese, V., & Parker, S. H. (2020). Predictors and triggers of incivility within healthcare teams: a systematic review of the literature. BMJ Open, 10, e035471. https://10.1136/bmjopen-2019-035471
- Khajoei, R., Jokar, M. & Vasli, P. (2024). Nurses’ experiences of the attributes of the organizational citizenship behavior: a qualitative content analysis. BMC Health Services Research 24, 538. https://doi.org/10.1186/s12913-024-10939-8
- Kim, H., Sefcik, J. S., & Bradway C. (2017) Characteristics of qualitative descriptive studies: A systematic review. Research in Nursing & Health, 40, 23–42.
- Kodjebacheva, D. G. (2014). Workplace incivility affecting CRNAs: A study of prevalence, severity, and consequences with proposed interventions. American Association of Nurse Anesthetists Journal, 82, 437–45
- Koopmans, L. (2014). Measuring Individual Work Performance. file:///C:/Users/Admin/Downloads/koopmans-2014-measuring%20(1).pdf
- Koopmans, L., Bernaards, C. B., Hildebrandt, V. H., Schaufeli, W. B., De Vet, H. C. W., & Van der Beek, A. J. (2011). Conceptual frameworks of individual work performance: a systematic review. Journal of Occupational and Environmental Medicine, 53(8), 856–866. https://doi.org/10.1097/JOM.0b013e318226a763
- Krijgsheld, M., Tummers, L. G., & Scheepers, F. E. (2022). Job performance in healthcare: a systematic review. BMC Health Services Research, 22, 149. https://doi.org/10.1186/s12913-021-07357-5
- Luthfiyana, D. A., Widowati, R., & Surwanti, A. (2024). A Meta-analysis of the relationship between organizational citizenship behavior and employee performance. Asian Journal of Management Analytics (AJMA), 3(2), 283-298. https://doi.org/10.55927/ajma.v3i2.8489
- Mahmood, B., Yasmeen, B., & Zafar, J. (2023). Workplace incivility and organizational citizenship behaviour: An empirical assessment of female banking personals. Journal of Arts & Social Sciences, 10, 28-33. https://doi.org/10.46662/jass.v10i1.310
- McCombes, S. (2023). Descriptive research. Definition, types, methods and examples. https://www.scribbr.com/methodology/descriptive-research/
- Merriam-Webster (2022). Headword recession. http://www.merriam-webster.com/dictionary/recession
- Morrow, R., Rodriguez, A., & King, N. (2015). Colaizzi’s descriptive phenomenological method. The Psychologist, 28(8), 643-644.
- Nanang AS, I., Soetjipto, B. E., & Supriyanto, A. S. (2021). Predicting factors of `organizational citizenship behavior in Indonesian nurses. Heliyon, 7(12), e08652. https://doi.org/10.1016/j.heliyon.2021.e08652
- Özlük, B., & Baykal, Ü. (2020). Organizational citizenship behavior among nurses: The influence of organizational trust and job satisfaction. Florence Nightingale Journal of Nursing, 26, 28(3), 333-340. https://doi.org/10.5152/FNJN.2020.19108
- Rastegari, M., Khani, A., Ghalriz, P., & Eslamian, J. (2010). Evaluation of quality of working life and its association with job performance of the nurses. Iranian Journal of Nursing and Midwifery Research, 15(4), 224-8.
- Read, E., & Laschinger, H. K. (2013). Correlates of new graduate nurses’ experiences of workplace mistreatment. Journal of Nursing Administration, 43(4), 221-8. https://doi.org/10.1097/NNA.0b013e3182895a90
- Rotundo, M., & Sackett, P. R. (2002). The relative importance of task, citizenship, and counterproductive performance to global ratings of performance: A policy capturing approach. Journal of Applied Psychology, 87, 66–80.
- Saleem, F., Malik, M. I., Asif, I., & Qasim, A. (2022). Workplace incivility and employee performance: Does trust in supervisors matter? (A dual theory perspective). Behavioral Science (Basel), 12(12), 513. https://doi.org/10.3390/bs12120513
- Shan, Y. (2021). Philosophical foundations of mixed methods research. Philosophy Compass, 17(1), e12804. https://doi.org/10.1111/phc3.12804
- Singh, S., Meghrajani, I., Vijh, G., Thomas, J., & Mohite, S. (2023). Relationship between workplace incivility, employee performance and employee engagement in healthcare institutions: – Global conference on emerging technologies, business, sustainable innovative business practices, and social well-being. Asia Pacific Journal of Health Management. https://doi.org/10.24083/apjhm.v18i2.2409
- Sinha, A., & Negi, K. (2019). Workplace empowerment perceived organizational support and their impact on organizational citizenship behavior: A study of Garhwal Region in Uttarakhand State of India. OPUS: HR Journal, 10(1), 101.
- Spector, P. E., Bauer, J. A., & Fox, S. (2010). Measurement artifacts in the assessment of counterproductive work behavior and organizational citizenship behavior: Do we know what we think we know? Journal of Applied Psychology, 95, 781-790.
- Stefurak, T., Johnson, R. B., & Shatto, E. (2015). ‘Mixed methods and dialectical pluralism’. In Jason, L. A., & Glenwick, D. S. (eds), Handbook of methodological approaches to community-based research: Qualitative, quantitative, and mixed methods. Oxford Academic. https://doi.org/10.1093/med:psych/9780190243654.003.0034, accessed 25 Jan. 2024
- Tittenbrun, J. (2012). The Theory of Social Exchange of G.C. Homans. https://www.researchgate.net/publication/254936722_The_the_Theory_of_Social_Exchange_of_GC_HomansEnter_Paper_Title
- Triani, F., Halin, H., & Wadud, M. (2020). Effect of organizational citizenship behavior on employee performance at PT Surya Dermato Medica Palembang. International Journal of Community Service & Engagement, 1(1).
- Tulane University, School of Social Work (2024). What is Social Exchange Theory? https://socialwork.tulane.edu/blog/social-exchange-theory/
- Umrani, W. A., Afsar, B., Khan, M., & Ahmed, U. (2019). Addressing the issue of job performance among hospital physicians in Pakistan: The role of job security, organizational support, and job satisfaction. Journal of Applied Biobehavioral Research, 24(3). https://doi.org/10.1111/jabr.12169.
- Wang, C.-H., & Chen, H.-T. (2020). Relationships among workplace incivility, work engagement and job performance. Journal of Hospitality and Tourism Insights. https://doi.org/10.1108/JHTI-09-2019-0105
- Woo, C. H., & Kim, C. (2020). Impact of workplace incivility on compassion competence of Korean nurses: Moderating effect of psychological capital. Journal of Nursing Management, 28(3), 682-689. doi: https://10.1111/jonm.12982
- Yaakobi, E., & Weisberg, J. (2020). Organizational citizenship behavior predicts quality, creativity, and efficiency performance: The roles of occupational and collective efficacies. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.00758
- Zeng, L., Feng, F., Jin, M. et al. Psychological capital and organizational citizenship behavior among nurses during the COVID-19 epidemic: mediation of organizational commitment. BMC Nursing, 22, 172). https://doi.org/10.1186/s12912-023-01332-7