
Outcomes of Patients with Acute Kidney Injury at Moi Teaching and Referral Hospital, Eldoret, Kenya
- Dr. Ngami Mutwa, MBCHB. Resident
- Dr. Mathew Koech, MBCHB, MMED
- Prof. Lameck Diero, MBCHB, MMED
- 53-64
- Feb 28, 2024
- Health
Outcomes of Patients with Acute Kidney Injury at Moi Teaching and Referral Hospital, Eldoret, Kenya
Dr. Ngami Mutwa, MBCHB. Resident*1, Dr. Mathew Koech, MBCHB, MMED.2, Prof. Lameck Diero, MBCHB, MMED.3
1Department of Medicine, School of Medicine, Moi University.Eldoret.
2Nephrologist and Lecturer, Department of Medicine, School of Medicine, Moi University. Eldoret.
3Associate Professor, Department of Medicine, School of Medicine, Moi University. Eldoret.
*Corresponding Author
DOI: https://doi.org/10.51244/IJRSI.2024.1102006
Received: 08 January 2024; Revised 24 January 2024; Accepted: 29 January 2024; Published: 28 February 2024
ABSTRACT
Background: Incidence of acute kidney injury (AKI) based on data from high income countries is about 1 in 5 admissions; 1 in 4 of those that develop AKI die from its complications. Developing countries assume same incidence and outcome of AKI as developed countries.
Objective: To describe the clinical presentation and determine the 90 day outcomes of patients with AKI at Moi Teaching and Referral Hospital (MTRH).
Design: Prospective cohort study.
Setting: MTRH General Wards.
Participants: 103 patients consecutively recruited from January to July 2018.
Interventions: Data was collected using a structured questionnaire and the patients were followed up from admission to discharge.
Main Outcomes: Dialysis need, duration of hospitalization, recovery and mortality.
Results: Mean age of the patients was 46.7±18.3 years. Majority were males at 61(60%) and most were in stage 3 disease at 65(63%). Main comorbidities were hypertension at 31(36.9%) and human immunodeficiency virus at 28(33.3%). Need for dialysis was at 31(30%) and strongly related to the AKI stage (p<0.0001). Complete recovery was observed in 29(52.7%) of the patients while 8(14.5%) had partial recovery and 18(32.7%) progressed to end stage renal disease. Recovery status was not determined by AKI stage (p=0.306). We had a 35(34%) mortality, most deaths occurred in stage 3 disease but statistically not significant (p=0.149). AKI causes were multifactorial, the most common being pre-renal with vomiting at 50(48.5%) and sepsis at 31(30%).
Conclusion: Most patients presenting at MTRH with AKI had severe disease associated with high mortality.
Keywords: Acute Kidney Injury, Recovery, Dialysis, Mortality.
BACKGROUND
The global burden of AKI is estimated to be 13 million cases per year, 85% of which occur in the low- to middle- income countries (1), assuming the same incidence and outcome as the developed countries because of paucity of data. In 2013, the International Society of Nephrology (ISN) launched the 0by25 initiative in response to this concern, to compile data on the prevalence of AKI in order to improve management of AKI and eliminate the preventable AKI-related deaths globally by 2025 (2).
Majority of AKI in Sub-Saharan Africa (SSA) is community acquired hence potentially preventable and treatable, yet it’s here that AKI is reported to be more aggressive with worse outcomes. This is attributed to late presentation to hospital and reliance on clinical criteria to make a diagnosis, which only become apparent at an advanced stage (3).
AKI is a global problem that occurs both in the communities and in the hospitals. Community-acquired acute kidney injury tends to occur in low-income countries, and in young people with few comorbidities, whereas hospital-acquired acute kidney injury occurs mostly in high-income settings, and in older people (45–80 years), often with several comorbidities (6). In a world meta-analysis, the pooled incidence of AKI was 21.6% and mortality was 23.9% in adults. Only one of 154 included studies was from sub-Saharan Africa (12).
A multicenter study done in acute medical units of hospitals in England and Scotland identified a prevalence of AKI at 17.7%, with sepsis, hypovolemia, chronic kidney disease and diabetes mellitus identified as the major risk factors (19).
Although there is paucity of data on the epidemiology of AKI in Africa (18), a systematic review to assess outcomes of AKI in sub-Saharan Africa identified an overall pooled mortality of 32% in adults (3).
In South Africa, the incidence of AKI in the population studied by Dlamini et al, was 3.4% of hospital admissions and AKI carried a high mortality risk, most significant risk factors being sepsis, late dialysis initiation and mechanical ventilation (4). A study done in Malawi that looked at the incidence, etiology and outcomes of community acquired AKI in the medical admissions had an incidence of AKI of 17.2% (11) while in Cameroon a similar study found a global incidence of AKI of 22.3% (8)
To describe the clinical presentation and determine the 90 day outcomes of patients with AKI as seen at MTRH.
- To describe the clinical presentation of patients with AKI at MTRH.
- To determine the severity of AKI as seen at MTRH using KDIGO criteria.
- To determine the 90 day outcomes (need for dialysis, progression to CKD, recovery and mortality) in patients with AKI at MTRH.
METHODOLOGY
Study Setting
Prospective cohort study done at MTRH general wards. MTRH is a National Teaching and Referral Hospital in Kenya with a bed capacity of 1600 patients, an average number of 1,200 patients at any time and about 1,500 outpatients per day. It serves about 40% of Kenya’s population in Western Kenya and is the primary care site for the 300,000 urban population of Eldoret town
Participants
Adults with a diagnosis of AKI were recruited consecutively between January and July 2018, achieving a total of 103 patients. Those with history of renal transplant were excluded because acute organ rejection can mask as AKI.
The aim of the study was to determine the 90 day outcomes of the patients with AKI admitted at MTRH. One such expected outcome is mortality, whose rate has been shown to be 38.8% (4) among AKI patients. At 95% confidence interval, Cochrane Formula was used to determine the sample size;
However, the cases of AKI developed by patients while in the hospital is scarce and ranges between 10 and 15 per month, end points inclusive. This gives a total of 60-90 patients in 6 months. Given the population size is smaller than the calculated sample size, we conducted a census on everyone who met the inclusion criteria during our study period with 103 participants being recruited.
Sampling
Purposive sampling approach was used to recruit the participants who meet the inclusion criteria into the study during the 6 month study period. A purposive sampling method known as criterion sampling method was used to select the cases of acute kidney injury that met this criterion (Patton, 2001, p. 238). This was combined with the need to have reference from the in-charge clinician to an acute kidney injury case.
Eligibility Criteria
- Patients aged eighteen years and above.
- Those admitted and have acute kidney injury as per KDIGO 2012 criteria.
History of kidney transplant. This is because patients with history of kidney transplant are at risk of graft rejection that can present as AKI and it’s a different end point from the general population.
Definition of terms
AKI was defined according to KDIGO 2012 as an increase in serum creatinine by ≥26.5 μmol/l within 48 hours in the absence of a prior history of, or clinical features to suggest the presence of CKD or a 1.5‑fold increase in serum creatinine from baseline which is known or presumed to have occurred within the prior 7 days. Severity of AKI was graded using the KDIGO 2012 classification (20).
Baseline creatinine was the last known serum creatinine of the patient within 3 months before falling ill or in case that was not available, the first serum creatinine after admission was presumed to be the baseline creatinine. Where the first serum creatinine was deranged, in absence of prior history of CKD, a normal baseline was presumed as recommended by KDIGO assuming a GFR of 75ml/ min/1.73m2
Data Collection
Data was collected using a structured questionnaire. Patients were then followed up while in the hospital on alternate days until discharge for assessment of dialysis need, duration of hospitalization, recovery and mortality. Once discharged, patients were contacted at thirty days for survival assessment, and at or after ninety days following the AKI episode, to present themselves for a repeat serum creatinine level. Patients with abnormal serum creatinine level were referred for follow up at the Renal Unit.
Data captured by the questionnaire included: demographic characteristics, risk factors for the AKI, hydration status at presentation, KDIGO stage, dialysis need, indication for dialysis, and days to the start of dialysis, duration of dialysis, days to complete recovery, date of death (where applicable), and duration of hospital stay.
The dependent variables included: Severity of AKI, need for dialysis, recovery, progression to CKD and mortality. The independent variable included: Age, sex, potential precipitators for AKI, serum creatinine levels and comorbidities.
DATA ANALYSIS
Data was analyzed using R Core Team (21) software for statistical computation. Categorical variables like gender, hydration status, occurrence of AKI, severity of illness, need for renal replacement therapy, and death among others were summarized using frequencies and percentages. Continuous variables like age and serum creatinine level were summarized using mean ± standard deviation or using median (interquartile range).
Categorical data was assessed for associations using Chi Square test. Continuous variables were compared using independent samples t-test. Statistical significance was set at p values of <0.05.
Approval to conduct the study was sought from MTRH/ Moi University – Institutional Research and Ethics Committee and the IREC approval number was FAN: IREC 2006.
RESULTS
Recruitment schema.
The study was carried out between January 2018 and July 2018 at Moi Teaching and Referral Hospital and 103 patients were recruited.
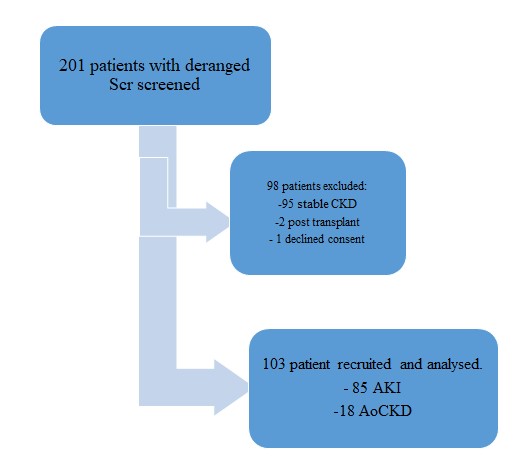
103 patients were analyzed. The mean age of occurrence was 46.7±18.3 years.
Table 1: Baseline characteristics of patients with AKI at MTRH.
| Female (n=42) |
Male (n=61) |
Total (n=103) |
|
| Ward of Admission | |||
| Medical | 31 (73.8%) | 51 (83.6%) | 82 (79.6%) |
| Gynecology | 11 (26.2%) | 0 (0%) | 11 (10.7%) |
| Surgical | 0 (0%) | 10 (16.4%) | 10 (9.7%) |
| Age category | |||
| 18-25 Years | 7 (16.7%) | 9 (14.8%) | 16 (15.5%) |
| 26-35 Years | 9 (21.4%) | 5 (8.2%) | 14 (13.6%) |
| 36-45 Years | 13 (31.0 %) | 13 (21.3 %) | 26 (25.2 %) |
| 46-65 Years | 10 (23.8%) | 19 (31.1%) | 29 (28.2%) |
| 65+ Years | 3 (7.1%) | 15 (24.6%) | 18 (17.5%) |
Clinical characteristics and precipitators of AKI
The mean systolic blood pressure was 117 mmHg (SD 30.8). 80% of the patients had underlying comorbidities. 53% of the cases had pre-renal AKI while 15% had post-renal AKI (Table 2).
Table 2: Clinical Characteristics and Precipitators of AKI in MTRH
| Clinical Indicator | n=103 (%) |
| Hydration Status | |
| Euvolemia | 78 (75.7) |
| Fluid Overloaded | 13 (12.6) |
| Volume Depleted | 12 (11.7) |
| SBP Mean (SD) | 116 (30.8) |
| DBP Mean (SD) | 72.6 (18.1) |
| Comorbidities | n=84 (%) |
| Hypertension | 31 (36.9) |
| HIV | 28 (33.3) |
| Chronic Kidney Disease | 18 (21.4) |
| Malignancy | 13 (15.5) |
| Congestive Cardiac Disease | 13 (15.5) |
| Diabetes Mellitus | 11 (13.1) |
| Liver Disease | 6 (7.1) |
| Connective Tissue Disease | 3 (3.6) |
| Others | 6 (7.1) |
| Precipitators | n=103 (%) |
| Pre-renal | |
| Vomiting | 50 (48.5) |
| Diarrhoea | 20 (19.4) |
| Blood Loss | 12 (11.7) |
| NSAID | 0 |
| Intrinsic/Renal | |
| Sepsis | 31 (30.1) |
| Glomerulonephritis | 16 (15.5) |
| Prolonged Pre-renal | 14 (13.6) |
| Drugs | 11 (10.7) |
| Muscle Injury | 1 (1.0) |
| Post-Renal | |
| BPH | 8 (7.7) |
| Cervical Cancer | 8 (7.7) |
AKI-Acute Kidney Injury, BPH-Benign Prostatic Hypertrophy, DBP-Diastolic Blood Pressure, HIV-Human Immunodeficiency Virus, MTRH-Moi Teaching and Referral Hospital, NSAID-Non-Steroidal Anti-Inflammatory Drug, SBP-Systolic Blood Pressure, SD-Standard Deviation.
The mean urea and creatinine at presentation were 49.18 mmol/l (SD 192.19) and 817.145 mmol/l (SD 745.76) while at 90th day were 15.03 mmol/l (SD 8.46) and 168.977 mmol/l (SD 149.68) respectively (Table 3).
Table 3: Kidney function tests of patients with AKI at MTRH
| Admission Mean (SD) | 90th day Mean (SD) | |
| Urea | 49.18(192.19) | 15.03(8.46) |
| Creatinine | 817.1456(745.76) | 168.977(149.68) |
| K+ | 5.13(1.23) | 3.35(2.17) |
Majority (65%) of the patients presented in stage 3 AKI disease while about 5% had stage 1 AKI according to KDIGO classification.
Table 4: The Severity and Outcomes of AKI in MTRH
| SEVERITY OF AKI | OUTCOMES | |||||||
| Stage | Freq.
(%) |
LOH: Median (IQR) | Dialysis Need (%) | Recovery:
Frequency (%) |
Mortality: Frequency (%) | |||
| Complete | Partial | ESRD | Alive | Dead | ||||
| 1 | 5 (4.9) | 10
(10,14) |
0 | 2 (3.6) | 0 | 0 | 2 (1.9) | 3 (2.9) |
| 2 | 31 (30.1) | 10 (8,18) | 6.3 | 13 (23.6) | 3 (5.5) | 4 (7.3) | 19 (23.3) | 7 (6.8) |
| 3 | 67 (65) | 11 (7,15) | 43.3 | 14 (25.5) | 5 (9.1) | 14 (25.5) | 34 (40.8) | 25 (24.3) |
| p=0.733 | p<0.0001 | p=0.306 | p=0.149 | |||||
AKI-Acute Kidney Injury, ESRD-End Stage Renal Disease, Freq.-Frequency, IQR-Interquartile Range, LOH-Length of Hospital Stay, MTRH-Moi Teaching and Referral Hospital
Length of hospitalization
The median length of hospital stay was 9.5 days, IQR (7, 17.8). When the length of hospitalization is grouped by AKI staging, stage 1 and 2 had a median length of hospitalization of 10 days while in stage 3 was 11 days (Table 4).
Dialysis need
There were 31 patients who required dialysis, with a mean time to dialysis of 3.7 days, IQR (0-7). Of these patients requiring dialysis, the mean number of sessions was 3.8 ranging from one session to seven sessions while admitted in the hospital. A strong relation does exist between need for dialysis and the AKI staging, p-value<0.0001 (Table 4).
Recovery
52.7% of the cases had complete recovery while 14.5% had partial recovery. About one in three of the cohort developed End Stage Renal Disease. When recovery was grouped by AKI staging, all the patients presenting in stage 1 had complete recovery. The recovery status was not determined by the AKI staging (Table 4).
Mortality
There were 35 reported deaths, representing about 34% of the patients. Majority of the deaths occurred to patients with AKI stage 3, with 25 deaths in this group. Association between the AKI staging and mortality was statistically non-significant, at 95% level of significance (p-value=0.149) (Table 4).
Associations: Univariate Analysis
The univariate analysis of the patients, stratified by mortality status indicated no statistical significance for all the variables collected. This finding could be attributed to our small sample size.
DISCUSSION
The mean age of the patients was 46.7 (SD 18.3) years. This is similar to what was reported in a similar study done in South Africa where they had a median age of 44 (IQR 14, 82) years (4). Studies in developed countries report a higher mean age, for example, a study done in the USA by Chertow et al. had a mean age of 58.8 years (5). AKI in developing countries is usually community-acquired, occurring in young people with few comorbidities, whereas in developed countries it’s hospital-acquired and occurs mostly in older people (45–80 years), often with several comorbidities (6).
There were 61(60%) males and 42(40%) females. Fouda et al. in their study on the epidemiology of acute kidney injury in a tertiary hospital in Cameroon found that 61(56.5%) were males (7). Other similar studies from both developed and developing countries have found a slightly higher male preponderance (8)(9). This could be a reflection of the health care access discrimination against women who lack economic and decision making power in the developing countries, or a true increased susceptibility to renal disease in males because of possible urogenital abnormalities (3).
Pre-renal causes accounted for the majority of AKI with hypovolemia from diarrhea and vomiting accounting for 70% of the presumed precipitating factors, while sepsis from bacterial infections accounted for 31% of cases. In Cameroon, a similar study had pre-renal AKI at 61.4% with sepsis from bacterial infections as the main precipitating factor (8). We found 11% cases of drug- induced AKI, mainly associated with amphotericin B. This was close to the reported prevalence of 18% of drug- induced AKI in sub- Saharan Africa (3). HIV is prevalent in sub- Saharan Africa. This predisposes people living with HIV to various opportunistic infections which present with diarrhea, vomiting and inability to eat and drink well leading to volume depletion. In addition, use of nephrotoxic drugs like amphotericin B in treating HIV- related infections such as Cryptococcal infections leads to drug- induced AKI (3).
In our study, cervical cancer and benign prostate enlargement at 16% were implicated as causes of obstruction. A similar study by Fouda et al. that looked at the epidemiology of acute kidney injury in a tertiary hospital in Cameroon, had obstructive AKI at 11.1% (7). This high proportion of cancer can be explained by the fact that our hospital is a referral center for oncology cases, and patients are usually referred to it at a late stage of the disease and with complications.
The most common comorbidities among our patients were hypertension at 36.9% and HIV at 33.3%. This finding may be due to the high prevalence of hypertension in Kenya that stands at 24.5% – 47% increasing with age (STEPS survey, 2015). Similar study in South Africa by Dlamini et al. had hypertension as the major comorbidity at 41.5% (4). According to World Health Organization (WHO) data, 27.4% men and 26.1% female in South Africa have hypertension. Hypertension is a potential cause of CKD and a recognized risk factor for AKI. The proportion of patients with HIV in this study was higher than the national prevalence in the general population of 4.6% – 21% in Kenya (10). This is because MTRH is a referral Centre for AMPATH catchment areas. In Malawi, a similar study had HIV as the major comorbidity at 58.8% compared to their national prevalence of HIV at 10% (11). HIV increases the risk of AKI through direct renal injury, antiretroviral drugs nephrotoxicity, especially tenofovir in our setting, and susceptibility to acute infective illnesses.
Severity of AKI
Most of our patients had severe disease. This was similar to a study in Malawi done by Evans et al. that looked at the incidence, etiology and outcomes of community acquired AKI in the medical admissions to a tertiary hospital, and found stage 1 disease at 21.6%, stage 2 at 17.7% and stage 3 at 60.8% (11). Our findings were similar to a study done in Cameroon by Halle et al. that found half of their patients had AKI stage 3 (8). This is mainly due to late presentation of patients in our hospital, being a referral facility or due to limited awareness of the kidney injury related to the silent nature of the disease. However, this was different from similar studies done in the developed countries that have majority of their patients in stage one of AKI at 80% (2). This is because most AKI in developed countries is hospital acquired, therefore picked early.
The median length of hospital stay in stage 1 and stage 2 disease was 10 days, while in stage 3 was 11 days. There was no statistical significance between severity of AKI and the length of hospitalization in our study. This was different from a study done by Ali et al. that found a median duration of stay for AKI at 17 days, and this was significantly shorter in mild forms and longer in severe AKI (Ali et al., 2007). Chertow et al. in another study found that the severity of AKI was consistently associated with an independent increase in length of hospital stay (5). The differences could be due to the fact that our study was not powered to assess for severity of AKI on the length of hospital stay.
Globally, mortality from AKI is estimated to be at 23.9%, and in sub- Saharan Africa, at 32% (12) (3). In our study, the overall mortality at 90 days was 34%. This was higher than what was previously reported in a retrospective study done by Munyu, at a private facility in Kenya that used RIFLE criteria to diagnose AKI and had an overall mortality of 16.6% (13). The mortality rate was however much lower than what Evans et al. in Malawi found, at 44.4% but similar to what Halle et al. in Cameroon reported, a mortality rate of 36.9% (11)(8). The high mortality could be attributed to the late presentation, or the reliance of clinical criteria to make a diagnosis, which may only become apparent at an advanced stage. This high mortality is alarming given the ISN goal of zero deaths from AKI by 2025.
In this study, mortality was seen to increase with increasing severity of AKI. Most deaths were observed in stage 3 at 24.3%, even though this was statistically non-significant (p value = 0.149). Similarly, Evans et al. in Malawi found that the crude mortality in patients with AKI was higher with increasing AKI severity [n = 18 (30.0%) in stage 1 and 2 vs. n = 46 (49.5%) in stage 3; p = 0.017] (11). Another study by Bagshaw et al. also showed a significant relationship between crude mortality and increasing severity of AKI (30.4% for risk, 72.7% for injury, 90% for failure, P < 0.001) while using the RIFLE criteria (18). This underscores the importance of early detection and treatment of AKI.
Renal recovery could not be ascertained in 19% of the participants due to loss to follow-up. Majority of our patients (52.7%) had complete recovery of renal functions at 3 months, while 14.5% had partial recovery, and 32.7% progressed to ESRD. The recovery status was not determined by the AKI (p=0.306). Mohammed in KNH, in a similar study had a complete recovery rate of 18.6% and partial recovery rate of 28.3% (14). This was much lower compared to our study because his recovery outcome was assessed at 2 weeks, while we assessed recovery at 3 months. The recovery rate in our study was much lower than what Halle et al., in Cameroon found (84.2%), possibly because we included patients with baseline CKD whose prognosis is worse (8). The percentage of patients with partial recovery comprises of an important group that needs long term follow up because of the risk of deterioration to ESRD.
A significant percentage of our patients progressed to ESRD. It is noteworthy that all patients with baseline CKD progressed to ESRD. This is in keeping with data that an episode of AKI accelerates progression of CKD to ESRD (15).
Thirty percent of our patients needed dialysis with a mean time to dialysis of 3.7 days (0-11 days). This was higher than the pooled dialysis requirement for AKI in the world that was estimated to be 2.3% (12). This was because most patients in the world meta-analysis had stage 1 disease, hence of good prognosis. The mortality was also much lower than the reported rate of 70% in most studies in sub Saharan Africa (3), possibly because this was a prospective study, patients were screened on admission and therefore AKI was diagnosed and managed earlier, reducing need for dialysis. Dialysis was realized on all patients that needed it, possibly due to dialysis machines availability.
Some of our baseline serum creatinine were based on estimations because of lack of previous known baselines, therefore, we may have diagnosed AKI in place of missed CKD.
CONCLUSION
Most patients presenting at MTRH with acute kidney disease had severe disease. Whereas majority of the patients recovered their renal functions, a significant number had partial recovery of renal functions and mortality was still high.
This study therefore describes the clinical presentation and outcomes of AKI in a tertiary hospital in Western Kenya. It builds on the knowledge of AKI in SSA, providing useful data in decision making and mitigation strategies against AKI.
ACKNOWLEDGEMENT
Gratitude to Mr. Ngeresa for his support on data analysis.
Conflict of interest
Authors declare no conflict of interest.
REFERENCES
- Ponce D, Balbi A. Acute kidney injury: Risk factors and management challenges in developing countries. Int J Nephrol Renovasc Dis. 2016;9:193–200.
- Mehta RL, Cerda J, Burdmann EA, Tonelli M, Garcia-Garcia G, Jha V, et al. International Society of Nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): a human rights case for nephrology. Lancet (London, England). 2015 Jun;385(9987):2616–43.
- Olowu WA, Niang A, Osafo C, Ashuntantang G, Arogundade FA, Porter J, et al. Outcomes of acute kidney injury in children and adults in sub-Saharan Africa: a systematic review. Lancet Glob Heal [Internet]. 2017 Apr 26;4(4):e242–50. Available from: http://dx.doi.org/10.1016/S2214-109X(15)00322-8
- Dlamini TAL, Heering PJ, Chivese T, Rayner B. A prospective study of the demographics, management and outcome of patients with acute kidney injury in Cape Town, South Africa. 2017;145:1–12. Available from: http://dx.doi.org/10.1371/journal.pone.0177460
- Chertow GM, Burdick E, Honour M, Bonventre J V, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365–70.
- Ibrahim A, Ahmed MM, Kedir S, Bekele D. Clinical profile and outcome of patients with acute kidney injury requiring dialysis – An experience from a haemodialysis unit in a developing country. BMC Nephrol [Internet]. 2016;17(1):1–5. Available from: http://dx.doi.org/10.1186/s12882-016-0313-8
- Fouda H, Ashuntantang G. The Epidemiology of Acute Kidney Injury in a Tertiary Hospital in Cameroon: A 13 Months Review. J Nephrol Ther. 2016;6(3):1–6.
- Halle MPE, Chipekam NM, Beyiha G, Fouda H, Coulibaly A, Hentchoya R, et al. Incidence, characteristics and prognosis of acute kidney injury in Cameroon: a prospective study at the Douala General Hospital. Ren Fail. 2018 Nov;40(1):30–7.
- Wang HE, Muntner P, Chertow GM, Warnock DG. Acute Kidney Injury and Mortality in Hospitalized Patients. Am J Nephrol [Internet]. 2012;35(4):349–55. Available from: https://www.karger.com/DOI/10.1159/000337487
- National AIDS Control Council. Kenya HIV Estimates Report 2018. Kenya HIV Estim [Internet]. 2018;1–28. Available from: http://www.nacc.or.ke/attachments/article/428/HIV estimates report Kenya 2014_print.pdf%5Cnpapers2://publication/uuid/16BC3DFC-19CF-4A11-B518-5F6B77E329C6
- Evans RDR, Hemmilä U, Craik A, Mtekateka M, Hamilton F, Kawale Z, et al. Incidence, aetiology and outcome of community-acquired acute kidney injury in medical admissions in Malawi. Vol. 18, BMC Nephrology. London; 2017.
- Susantitaphong P, Cruz DN, Cerda J, Abulfaraj M, Alqahtani F, Koulouridis I, et al. World incidence of AKI: a meta-analysis. Clin J Am Soc Nephrol. 2013;8(9):1482–93.
- Munyu P (AghaKhan U. Prevalence, risk factor and outcomes of acute renal failure in Agha Khan University Hospital, Nairobi. unpublished. 2008;
- Mohammed T (UON). Prevalence, severity and outcomes of community acquired acute kidney injury in medical patients at Kenyatta National Hospital. Kenya Assoc Physicians. 2018;
- Waikar SS, Liu KD, Chertow GM. Diagnosis, epidemiology and outcomes of acute kidney injury. Clin J Am Soc Nephrol. 2008;3(3):844–61.
- Ali, T., Khan, I., Simpson, W., Prescott, G., Townend, J., Smith, W., & MacLeod, A. (2007). Incidence and outcomes in acute kidney injury: a comprehensive population-based study. Journal of the American Society of Nephrology, 18(4), 1292–1298.
- Bagshaw, S. M., Uchino, S., Bellomo, R., Morimatsu, H., Morgera, S., Schetz, M. … Kellum, J. A. (2009). Timing of renal replacement therapy and clinical outcomes in critically ill patients with severe acute kidney injury. Journal of Critical Care, 24(1), 129–140. https://doi.org/10.1016/j.jcrc.2007.12.017
- Naicker, S., Aboud, O., & Gharbi, M. B. (2008). Epidemiology of acute kidney injury in Africa. Seminars in Nephrology, 28(4), 348–353. Journal Article. https://doi.org/10.1016/j.semnephrol.2008.04.003
- Finlay, S., Bray, B., Lewington, A. J., Hunter-Rowe, C. T., Banerjee, A., Atkinson, J. M., & Jones, M. C. (2013). Identification of risk factors associated with acute kidney injury in patients admitted to acute medical units. Clinical Medicine, Journal of the Royal College of Physicians of London, 13(3), 233–238. https://doi.org/10.7861/clinmedicine.13-3-233
- http://www.kidney-international.org VOLUME 2 | ISSUE 1 | MARCH 2012
- R Core Team (2016) R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/