
Prostate Cancer: Knowledge, Perception and Rate of Screening among Male Artisans in Nnewi-North Local Government Area, Anambra State, Nigeria.
- Solomon M. Ariom
- Ahoma Victor Mbanuzuru
- Alphonsus C. Obi-Okaro
- 419-435
- Dec 16, 2023
- Health
Prostate Cancer: Knowledge, Perception and Rate of Screening among Male Artisans in Nnewi-North Local Government Area, Anambra State, Nigeria.
Solomon M. Ariom, Ahoma Victor Mbanuzuru, Alphonsus C. Obi-Okaro
Department of Community Medicine, Faculty of Medicine, Nnamdi Azikiwe University, Awka Anambra State, Nigeria
DOI: https://doi.org/10.51244/IJRSI.2023.1011035
Received: 01 November 2023; Revised: 15 November 2023; Accepted: 18 November 2023; Published: 16 December 2023
ABSTRACT
Background: Prostate cancer is the number one cancer in males in Africa, both in terms of incidence and mortality, being the most commonly diagnosed malignancy among men in Nigeria. It is of public health importance
Objectives: To determine the knowledge, perception and the rate of screening of prostate cancer among male artisans in Nnewi-North Local Government Area, Anambra State, Nigeria.
Method: This study was a descriptive-cross sectional study carried out among 220 male artisans aged 18 years and above. The respondents were recruited into the study using a multistage sampling technique. Stage 1: Selection of quarter in Nnewi: The four quarters in Nnewi were part of this study. This gave approximately 55 participants for each quarter. Stage 2: Selection of participants: The desired participants were selected using modified clusters sampling method. At the centre of each quarter, a bottle was spun to determine the direction to follow in clockwise for the participants. Where artisans are located were identified until the desired number of participants was recruited. The study tool was a researcher-administered questionnaire written in English language. The data was cleaned, coded and analyzed using statistical package for social sciences (SPSS) version 25. Informed consent was obtained prior to administration of the questionnaire which emphasized the right to none participation. Confidentiality was maintained according to the Helsinki declaration of bioethics.
Result: The mean age of the respondents was 39.78 ± 13.072 years, range of 18-75. Only 124 (56.4%) and 43 (19.5%) of the 220 respondents were aware of prostate cancer and prostate cancer screening respectively. Only 7 (3.2%) have ever screened for prostate cancer, however, 178 (80.9%) are willing to screen if made free. However, 184 (83.6%) perceived prostate cancer to be a serious disease.
Conclusion: The level of knowledge regarding prostate cancer and its screening practices was poor. There was a significant association between educational level and prostate cancer knowledge, indicating that this factor significantly influences people’s knowledge, perceptions, and rates of screening for prostate cancer.
Keywords: knowledge, perception, rate, prostate cancer screening, attitude.
BACKGROUND OF STUDY
Prostate cancer (PCa) is a public health concern. The symptoms vary from person to person and some of them include difficult to start urinating, weak urine flow or interrupted flow, urination on a regular basis, especially at night, difficulty completely emptying the bladder during urination, possible painful urination or a burning sensation.1 At times PCa may come with blood in the urine or sperm, back, hip, or pelvic pain that does not go away, and excruciatingly painful ejaculation.
The prostate is part of the male reproductive system, as well as the penis, seminal vesicles, and testicles. Anatomically, the prostate is anterior to the rectum, directly inferior to the bladder, and surrounds the urethra (the tube that empties urine from the bladder). It is about the size of a walnut and produces a fluid that is a component of sperm.1 Pathological abnormalities occur more frequently in the prostate gland than elsewhere in human males leading to increased morbidity and mortality.2
The prostate gland contains three major glandular regions- the peripheral zone, the central zone, and the transitional zone which differ histologically and biologically. The central zone is relatively resistant to carcinoma and other disease; the transition zone is the main site of origin of prostate hyperplasia.2 There are also several important non-glandular regions concentrated in the anteromedial portion of the gland. Each glandular zone has specific architectural and stromal features. In all zones, both ducts and acini are lined by secretory epithelium. In each zone, there is a layer of basal cells beneath the secretory lining, as well as interspersed endocrine-paracrine cells. Frequent deviations from normal histology include post-inflammatory atrophy, basal cell hyperplasia, benign nodular hyperplasia, atypical adenomatous hyperplasia, and duct-acinar dysplasia. These lesions may at times be confused with carcinoma, especially in biopsy material.3 Prostate cancer causes pain, difficulty in urinating, anomalies of sexual intercourse and erectile dysfunction.2
Benign prostatic enlargement and adenocarcinoma increase in prevalence with increasing age. Prostate cancer is an adenocarcinoma that may be slow growing, aggressively evolving and metastasizing predominantly in the bones and lymph nodes.2 Prostate cancer may be asymptomatic at the early stage and often has an indolent course, and may require minimal or even no treatment4. However, the most frequent complaint is difficulty with urination, increased frequency, and nocturia, all symptoms that may also arise from prostatic hypertrophy.4
The aetiology of the prostate cancer is unknown however; androgens and ageing, environment, meat and animal fat intake among other factors are important risk factors for prostate cancer development.2 Old age, a positive family history, and black race are the strongest risk factors for prostate cancer development.5
The prostate gland in men is capable of undergoing malignant changes leading to prostate cancer. Prostate cancer is the second most common cancer in male, it is the second leading cause of cancer related death worldwide being, the commonest cancer in males in Nigeria accounting for 11-12% of all cancers in males.6 It is commoner in blacks compared to Asians and Caucasians. The lowest yearly incidence rates are seen in Asia, while the highest incidence is seen in North America and Scandinavia, especially among African-Americans.7 The most commonly diagnosed malignancy among men in Nigeria is prostate cancer, with a hospital prevalence of 182.5 per 100,000 male admissions, recorded in 2010 in Osun State.7
A man has about a 16% chance (1 in 6) of being diagnosed with prostate cancer and 3% (1 in 33) chance of dying of prostate cancer in his lifetime.6 In the United States of America (USA), the estimated lifetime risk of being diagnosed with the disease is 17.6% for Whites and 20.6% for African-Americans.6 The risk of death from prostate cancer in lifetime is 2.8% and 4.7%, respectively while the lifetime risk of being diagnosed with prostate cancer in the United Kingdom (UK) is 1 in 26.6 In Nigeria, the prostate cancer risk was 2% of all patients based on a pool of 110,000 men; consequently, cancer of the prostate is likely to impact the life of a significant proportion of men that are alive today.6 In sub-Saharan Africa, late presentation of prostate cancer is common with attendant high morbidity and mortality, however, to prevent late presentation and its management challenges, a good knowledge level of prostate cancer and prostate cancer screening services is paramount.8
Decreased prostate cancer–specific mortality and metastatic disease and an increased chance of finding localized disease are potential benefits of early detection of prostate cancer.9 Prostate cancer screening goal is to lower the morbidity and mortality associated with this disease through early detection.10 Digital rectal examination (DRE) and serum prostate specific antigen (PSA) measurement are screening techniques for prostate cancer.6 Screening and treatment for prostate cancer in both developed and developing countries, may be influenced by negative attitudes and perceptions toward prostate cancer.11
The American Cancer Society recommends that men over 50 years undergo either PSA or DRE, prostate cancer screening every year.12 Reduction in cancer-related mortality and morbidity can be achieved by early detection and appropriate treatment of majority of solid tumours, including cancer of the Prostate (CAP). When patients are aware of the disease, present early and are willing to be treated when diagnosed, such goals can then be attained.13
1.1. Problem Statement
The rate of incidence of prostate cancer varies across the regions and populations.4 Based on Global Cancer Observatory (GLOBOCAN) 2018 estimates, 1,276,106 new cases of prostate cancer were registered worldwide, representing 7.1% of all cancers in men.4 Prostate cancer incidence rates are highly variable worldwide which increases with age, although only 1 in 350 men below 50 years of age will be diagnosed with prostate cancer.4 The incidence rate increases up to 1 in every 52 men for ages 50 to 59 years and this is nearly 60% in men above 65 years of age.4 In the United States alone, prostate cancer affects approximately 230,000 men and causes the death of 30,000 American men annually.5
According to The economic burden of prostate cancer – a Swedish prevalence-based register study by Shuang Hao et al, the societal costs due to prostate cancer in Stockholm in 2016 were estimated to be 64 million Euro.14 The total annual costs extrapolated to Sweden were calculated to be 281 million Euro. These estimates were sensitive to assumptions related to the proportion of primary care visits associated with PSA testing and the evaluation method for informal care.14
Prostate cancer reports have been hospital-based in Sub-Saharan Africa, and as such very few studies, have been conducted on indigenous populations.2 The lack of knowledge on the disease and the low uptake of routine screening among men most at risk of developing prostate cancer compound the problem.2 In addition, little is known about the factors predisposing men at increased risk of prostate cancer as well as hindering awareness and uptake of screening and early diagnosis.2
1.2 Objectives Of the Study:
To determine the knowledge, perception and the rate of screening of prostate cancer among male artisans in Nnewi-North LGA, Anambra state, Nigeria.
METHODOLOGY
2.1 Study Area
This work was done at Nnewi, a commercial and industrial city in Anambra State, Southeastern Nigeria. It is the second largest and second most populated city in Anambra State located in the southern part of the State. Nnewi as a metropolis has one Local Government Area, which is Nnewi North. Nnewi North comprises four quarters: Otolo, Uruagu, Umudim, and Nnewichi.15 The population of Nnewi according to 2006 census is 391,227 with population growth of 2.1%, and a projected population at 2022 of 547,459.15
2.2 The Study Population
The study population consisted male artisans aged 18 years and above in Nnewi North LGA Anambra State, Nigeria.
2.2.1 Inclusion Criteria
All adult male artisans aged 18 years and above who gave their consent to participate in the study.
2.2.2 Exclusion Criteria
Those who met inclusion criteria but has not stayed up to 6 months in Nnewi.
2.3 Study Design
This study was a descriptive cross sectional study on the knowledge, perception and the rate of screening of prostate cancer among male artisans in Nnewi North, Anambra State, Nigeria
2.4 Sample Size Determination
The sample size was calculated using the Cochrane formula, which is given as; n = z2pq/d2
Where n = minimum sample size,
z= the standard normal deviate (1.96) at 95% confidence level.
p =0.149.7
q=1-p
d= the degree of precision is usually set at 5% (0.05)
n= (1.96)2×0.149×0.851/0.0025
n= 194.85
Adjusting for non-response, sample size was
n = ![]()
n = 194.85/0.9
n = 216.5
Minimum sample size was 217, which was rounded up to 220.
2.5 Sampling Technique
Multistage sampling technique was employed in this study. In Stage 1, there was selection of the Quarter/Village for the study. All the four quarters in Nnewi were part of this study. This gave approximately 55 participants for each quarter employing equal allocation. Stage 2 involved selection of participants from each Quarter: The desired participants were selected using the modified World Health Organization (WHO) cluster sampling method. This involved spinning a bottle at the center of each Quarter/Village to determine the direction to follow. Then in clockwise, the participants (artisans) were located and recruited. Where an artisan objected to the study, the next artisan was identified and recruited until the desired number of participants was recruited.
2.6 Data Collection
The data were collected through researcher-administered questionnaires with the help of research assistants who were trained in order to avoid bias. The questionnaire was adopted and adapted with guidance from several works already done on the subject/related or similar works.16,17 Research assistants were carefully selected and trained on how to administer the questionnaires. The questionnaire was divided into four sections A, B, C and D. Section A contains questions on socio-demographics; Section B contains questions on awareness of prostate cancer; Section C contains questions on awareness and practice of prostate cancer screening; and Section D contains questions on the perception and rate of screening of prostate cancer.
2.7 Data Management
The data was cleaned, coded and analyzed using statistical package for social sciences (SPSS) version 25. Descriptive and inferential statistics were applied where necessary. Continuous variables like age, duration in artisanship, etc. were reported as mean; median and standard deviation, while categorical data like marital status, religion, and tribe were reported using proportion and percentages. Associations between categorical variables were tested using chi-square. Significance level was set at 95% confidence interval. P-value less than or equal to 0.05 were considered statistically significant.
2.8 Duration of Study
The study lasted for a period of six weeks.
2.9 Ethical Considerations
This research work was done with approval from the Nnamdi Azikiwe University Teaching Hospital Ethics Committee (NAUTHEC) through the Head of Department of Community Medicine, Nnamdi Azikiwe University. Participants were well-oriented on the objectives of the study; informed consent was obtained prior to administration of the questionnaire which emphasized the right to none participation. Data confidentiality was maintained according to the Helsinki declaration of bioethics.
RESULT
3.1 Section A: Socio-Demographic Characteristics
Table 1 below shows the socio-demographic characteristics of the respondents. The mean age of the participants was 39.78 years, and the age group with the largest number of responses was 30-39 years 53(24.1%) followed by age group 40-49 years 52(23.6%). However, 100(45.5%) of the respondents have secondary school as their highest level of education. The mean age in artisanship of the respondents is 12.68 years, and most of the respondents 119 (54.1%) have spent 10 years and below in artisanship, however, only 3 (1.4%) have spent 41 years and above in artisanship.
Table 1: Socio-demographic characteristics of the respondents
| Variables | Frequency | Percentage | |
| Age (years) | <20
20-29 30-39 40-49 50-59 60-69 70+ Mean age ± SD Age range |
9
50 53 52 37 13 6 39.78 ± 13.072 18-75 |
4.1
22.7 24.1 23.6 16.8 5.9 2.7 |
| Marital status | Single
Married |
75
145 |
34.1
65.9 |
| Religion | Christian
Muslim Traditional None |
212
5 2 1 |
96.4
2.3 0.9 0.5 |
| Highest educational level | Primary
Secondary Tertiary Postgraduate |
82
100 31 7 |
37.3
45.5 14.1 3.2 |
| Tribe | Igbo
Hausa Yoruba Others |
212
6 0 2 |
96.4
2.7 0.0 0.9 |
| How long in artisanship (years) | <=10
11-20 21-30 31=40 >=41 |
119
58 35 5 3 |
54.1
26.4 15.9 2.3 1.4 |
SD: Standard deviation
3.2 Section B: Awareness of Prostate Cancer Among Respondents
Table 2 shows the awareness of prostate cancer as identified by the respondents. One hundred and twenty four (124) (56.4%) of the respondents have ever heard of prostate cancer before. Majority of the respondents (67.3%) do not know the location of the prostate gland, and only 57(25.9%) knew the location of prostate gland.
Table 2 Awareness of prostate cancer among respondents
| Variables | Frequency | Percentages | |
| Ever heard of prostate cancer | Yes
No |
124
96 |
56.4
43.6 |
| Location of prostate gland | In the chest
In the anus In the intestine Immediately below the bladder I don’t know |
10
2 3 57 148 |
4.5
0.9 1.4 25.9 67.3 |
| Prostate cancer affects
which gender |
Men only
Women only Both men and women I don’t know |
72
7 45 96 |
32.7
3.2 20.5 43.6 |
| Knows anyone that
has had prostate cancer before |
Yes
No |
35
185 |
15.9
84.1 |
| Have had a family member
Who had/has prostate cancer |
Yes
No |
15
205 |
6.8
93.2 |
Figure 1 below shows the sources of information about prostate cancer. The major source of information of prostate cancer is television or radio (21%), this is followed by social media/internet (15.5%), 14.4% heard about prostate cancer from family or friends, only 13.2% heard about prostate cancer from doctor or health worker, while 1.8% heard from church/mosque.

Figure 1: sources of information as demonstrated by the respondents.
The most perceived risk factors of prostate cancer as indicated by the respondents as shown in figure 2 below are alcoholism 43(19.5%) and tobacco 43(19.5%), followed by age above 40 years (18.6%). While 10% of the respondents knew that positive family history of prostate cancer is a risk factor for developing prostate cancer; male gender (15.5%), low level of education (14.5%), obesity/overweight (11.8%), African race (7.7%), spiritual projection (0.9%).
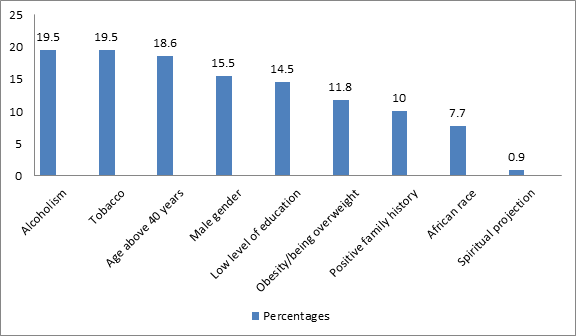
Figure 2: Risk factors of prostate cancer as demonstrated by the respondents
The most common symptom of prostate cancer as identified by respondents in figure 3 below is difficulty in urination (38.2%), followed by blood in the urine (10.9%) and feeling of incomplete voiding (10.9%); hesitancy (9.1%), weak or intermittent urine (8.6%), frequent urination (7.7%), dribbling after urination (6.8%), excessive urine at night (6.8%).
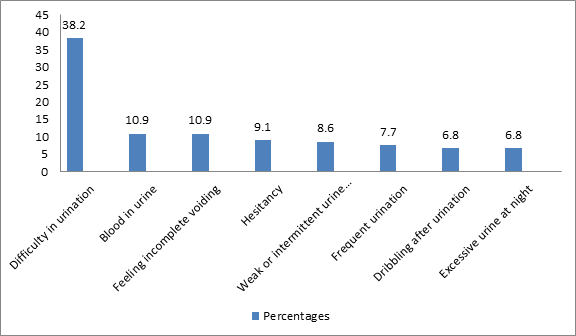
Figure 3: Symptoms of prostate cancer as demonstrated by the respondents
The table below (Table 3) shows the association between some selected socio-demographic variables and awareness of PCa. Age and marital status did not seem to affect level of awareness of PCa screening (p> 0.05), however there is statistical significance between levels of education and awareness of PCa (P<0.001).
Table 3: Association between some selected socio-demographic variables and awareness of Prostate cancer.
| VARIABLES | Awareness of Prostate cancer | CHI SQUARE | P-VALUE | ||
| AGE (YEARS) | <20
20-29 30-39 40-49 50-59 60-69 70+ |
YES
4 30 29 33 22 5 1 |
NO
5 20 24 19 15 6 5 |
7.595 | 0.269 |
| MARITAL STATUS | SINGLE
MARRIED |
47
77 |
28
68 |
1.838 | 0.175 |
| HIGHEST EDUCATIONAL LEVEL | PRIMARY
SECONDARY TERTIARY POSTGRADUATE |
37
53 29 5 |
45
47 2 2 |
22.747 | 0.001 |
3.3 Section C: Awareness and Practice of Prostate Cancer Screening Among Respondents
Table 4 below shows the awareness and practice of prostate cancer screening among respondents. From the table 3 below, only 43(19.5%) of the respondents were aware of prostate cancer screening. Most of the respondents 213(96.8%) had never screened for prostate cancer before. However, majority of the respondents 178(80.9%) are willing to be screened if prostate cancer screening is made free.
Table 4 Awareness and practice of prostate cancer screening among respondents
| Variables | Frequency | Percentages | |
| Awareness of PCA screening | Yes
No |
43
177 |
19.5
80.5 |
| Ever screened for prostate cancer | Yes
No |
7
213 |
3.2
96.8 |
| Screened for PCA in the last one year | Yes
No |
4
216 |
1.8
98.2 |
| Willing to screen for PCA if made free | Yes
No |
178
26 |
80.9
11.6 |
PCA: prostate cancer, DRE: digital rectal examination
Figure 4 above shows the screening methods as demonstrated by the respondents. Those who are aware of PSA and DRE as screening methods for prostate cancer are 8.4% and 5.9% respectively; others (0.9%).
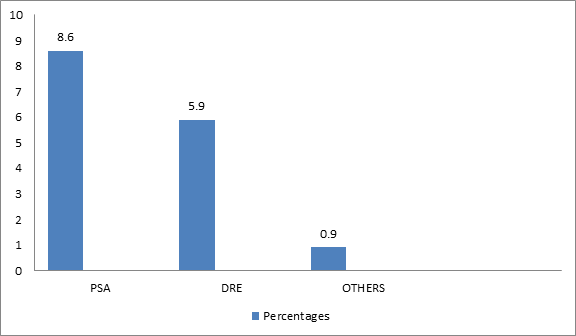
PSA: prostate specific antigen, DRE: digital rectal examination
Figure 4: Screening methods as demonstrated by the respondents
Figure 5 below shows that the majority of the respondents (89.5%) know that prostate cancer screening can be done in the hospital; health centre (15%), home/homeopathic doctor (3.2%), chemist shop (2.3%).
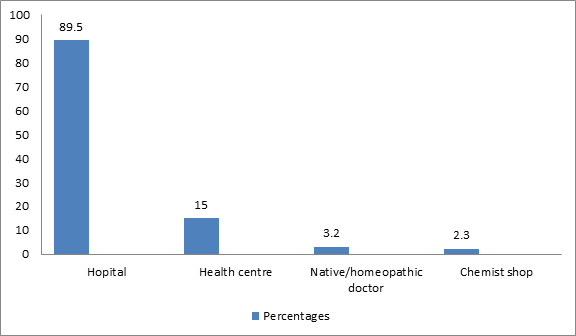
Figure 5: Where screening can be done as demonstrated by the respondents
The table below (Table 5) shows the association between some selected socio-demographic variables and awareness of PCa. Age did not seem to affect level of awareness of PCa screening (p> 0.05), however there is statistical significance between marital status and levels of education and awareness of PCa screening (P<0.05).zz
Table 5: Association between some selected socio-demographic variables and awareness of Prostate cancer screening
| VARIABLES | AWARENESS OF PCA SCREENING | CHI SQUARE | P-VALUE | ||
| Age category | <20
20-29 30-39 40-49 50-59 60-69 >=70 |
YES
1 15 10 7 9 1 0 |
NO
8 35 43 45 28 12 6 |
8.278 | 0.218 |
| Marital status | Single
Married |
23
20 |
52
125 |
8.950 | 0.003 |
| Highest level of education | Primary
Secondary Tertiary Postgraduate |
10
84 15 2 |
72
84 16 5 |
20.378 | 0.001 |
3.4 Section D: Perception of Prostate Cancer and Prostate Cancer Screeening Among Respondents
From table 6 below, the majority of surveyed participants seemed to have a good perception of prostate cancer; 83.6% indicated that PCa is a serious disease, 84.1% reported that it can be cured when detected early. However, 60% of surveyed respondents reported that a man diagnosed early with PCa can live a normal life if well managed.
Table 6: Perception of prostate cancer among respondents
| Variables | Frequency | Percentages | |
| Prostate cancer is a serious disease | Yes
No Not sure |
184
13 23 |
83.6
5.9 10.5 |
| Prostate cancer can be cured if detected early | Yes
No I don’t know |
185
9 26 |
84.1
4.1 11.8 |
| A man diagnosed early with PCA can have a normal life if well managed | Yes
No I don’t know |
157
25 38 |
71.4
11.4 17.3 |
| PCA would affect sexual function | Yes
No I don’t know |
132
36 58 |
60.0
13.6 58 |
Table 7 below shows the perception of prostate cancer screening among respondents. Those who were afraid of the procedures were 45%, fear the doctor will find cancer were 42.7%. However, 63.6% perceived that the screening is too expensive.
Table 7: Perception of prostate cancer screening among respondents
| Variables | Frequency | Percentage | |
| Fear of procedure | Yes
No |
99
121 |
45.0
55.0 |
| Fear the doctor will find cancer | Yes
No |
94
126 |
42.7
57.3 |
| PCA screening is too expensive | Yes
No |
140
80 |
63.6
36.4 |
| PCA screening will be embarrassing | Yes
No |
65
155 |
29.5
70.5 |
| Long waiting time
for appointment |
Yes
No |
111
109 |
50.5
49.5 |
DISCUSSION
The percentage of respondents who are aware of prostate cancer (56.4%) and prostate cancer screening (19.5%) was generally low among male artisans in Nnewi similar to some other studies carried out in Southern Nigeria that also reported low knowledge among their respondents.7,8,18 However, in a study done at University of Nigeria among male staff of the institution suggests that the respondents had a good knowledge of prostate cancer.19 This good knowledge could be attributed to these men having better education levels and more access to knowledge. In a similar study by Oranusi et al among male public servants of Anambra state also revealed a higher knowledge of prostate cancer.20 In a similar work by Wachira et al, majority of the respondents (80%) were aware of the existence of prostate cancer.21 A similar study by Nancy et al also found low levels of awareness and knowledge of prostate cancer.22 A similar work by Ebuehi et al revealed that the majority of the respondents were aware of prostate cancer (65.6%).6 This high knowledge could be attributed to the fact that it was done among male staff of the University of Lagos, who are more educated than our study population. A study by Awosan et al showed poor knowledge of prostate cancer (5.0%) and prostate cancer screening (1.3%) and zero uptake of prostate cancer screening among their participants.23 A study by Adibe et al, 57.8% of their respondents had a high knowledge level of prostate cancer.24 This high knowledge could be attributed to the fact that it was done among male staff of the University of Nigeria, who are more educated than our study population. In a study by Oladepo et al they obtained high awareness of prostate cancer in their study (80.0%).25 This high awareness could be linked to the older men which were their study population because older men usually seek hospital care. Atulomah et al in their study reported low level of awareness about prostate cancer among men of South-West Nigeria.18 Low knowledge of prostate cancer, low prostate cancer screening practice were recorded in a Zambian study by Sakala et al; 33.5% had heard about prostate cancer and 29% expressed knowledge of prostate cancer.22 This low knowledge was observed even though the study was carried out in a teaching hospital. According to a study by Morlando et al on prostate cancer screening: Knowledge, attitudes and practices in a sample of men in Italy, their respondents had an adequate knowledge about prostate cancer (82.1%).26 However, in a similar study done among young Black men in Austin, Texas, low knowledge of prostate cancer was obtained.19
The sources of information about prostate cancer as demonstrated by the respondents in this study were mostly television/radio (21.4%), the social media/internet sources (15.5%), family or friends (14.5%), and doctor or health worker (13.2%). Similar work by Ebuehi et al demonstrated that health workers were the major sources of information of prostate cancer (57.9%), internet and books (6.2%).6 This could be attributed to the fact that their work was done among male staff of the University of Lagos. In a similar work done by Morlando et al in Italy, the sources of information about prostate cancer were television/newspapers (49.6%), physicians (36.2%), family (31.4%) and the internet (11.4%).26 According to Nartey et al in similar work, majority of their respondents heard of prostate cancer from television, radio and internet while 17.4% heard of prostate cancer from health workers.12 According to a Zambian study by Sakala et al; the sources of information from the respondents include; TV (1.9%), radio (25.4%), nurse (25.4%), doctor (29.9%), read about it (1.5%), family and friends (3.0%).22 Similar study done by Waseem et al in Pakistan, the majority of their respondents heard of prostate cancer from family and friends (21.7%) with internet sources of 0.5%.27
Most of the respondents in this study did not know the location of the prostate gland (67.3%) while 25.9% correctly identified the location of the prostate gland, 16.6% could do so in the study by Atulomah et al.18 A similar study by Agbugui demonstrated that lower number knew of its physiological function, its position in the male anatomy and its accessibility via a digital rectal examination. Few of the respondents (32.7%) in this study identified prostate cancer as unique to the male gender.18,20,28 Difficulty in urination was the most commonly identified symptom of PCa in this study (38.2%) and similar findings have been noted in studies done.20,25,28 Age above 40years (18.6%) was mentioned as the main risk factor for developing prostate cancer. A similar study by Olademeji et al showed sexual activity (62.7%) as the main risk factor for developing prostate cancer.25
Despite the awareness of the prostate cancer by the respondents in this study, only 19.5% are aware of prostate cancer screening. This is quite low, however, this is in line with similar studies done across the country.18,20,28 This indicates that knowledge about PCa has not been transferred into knowledge of PCa screening. This might be because knowledge is often lacking despite great awareness, as seen in Atulomah et al and Agbugui et al.18,28 This low level of awareness of prostate cancer screening could be associated to the low level of education of the participants of this study. This claim appears to be supported by Oranusi’s study of better educated civil officials in Anambra state, South East Nigeria, which found that 56.8% of them were aware of PCa screening; this figure is the highest among the Nigerian studies that are currently accessible.20 Only 3.2% of the respondents have ever screened for prostate cancer. Similar studies done in Nigeria also demonstrated low rate of screening with no available studies exceeding the 6.4% recorded in the study by Oranusi et al.3,18,20,28 Majority of the respondents (80.9%) are willing to be screened for prostate cancer if made free. A similar study by Enemugwem et al, half of their respondents (51.5%) were willing to screen for prostate cancer.7 In a similar study by Ozoemena et al, 3.2% indicated their willingness to be treated in the event of being diagnosed with asymptomatic CAP.13 In a study by Oladepo Olademeji et al, majority of the respondents (81.5%) were willing to routinely screen for prostate cancer.25 According to a similar study done in Kenya by Mbugua et al, the percentage of responders who had never been screened who said they would be willing to do so in the future was high, at 81%.29 In a similar study by Ogbetere et al, the majority of the respondents (86.7%) are willing to know more about prostate cancer and prostate cancer screening as well as to be screened for prostate cancer disease.8 A study done in Italy by Morlando et al, about 60% of respondents expressed their willingness to receive a PSA-test.26 Other studies done in Africa and other parts of the world showed willingness of participants to screen for prostate cancer.6,16,17,20,22–25
Most of the respondents (83.6%) perceived that prostate cancer is a serious disease. A similar study by Wachira et al.24 99% of the respondents perceived prostate cancer as a serious disease.21 According to a study by Atulomah et al, for the perception of seriousness, (64.6%) admit that prostate cancer is a deadly disease.18 In a study by Adibe et al, all the participants have a positive perception of prostate cancer screening and treatments. This is obviously because of information and knowledge on prostate cancer possessed by these individuals in the field of medical sciences field of study. However, according to Husaini et al in Belize district study, poor and negative perceptions toward PCa screening were seen with a negative attitude toward PCa screening by the participants.17 In a study by Oluwole et al, only 9% of the respondents to this survey believed they were at danger of acquiring prostate cancer; as a result, few of them underwent prostate cancer screenings.16 According to a similar study by Vapiwala et al, the Black organizations supported false beliefs about prostate cancer therapy and had divergent views on its curability.30
The knowledge, perception and the rate of screening of prostate cancer among male artisans in Nnewi-North Local Government Area, Anambra State, Nigeria is generally low. Majority of the respondents in this study are willing to be screened for prostate cancer if made free.
LIMITATIONS OF STUDY
This work studied only artisans within Nnewi South-East Nigeria within a short period, may not be generalized for every artisan in Nigeria, or Sub-Saharan Africa or the whole population. There could also be possibility of interviewer bias as interviewer-administered approach was employed following that most of the artisans were not well educated. This challenge was surmounted by proper training of research assistants and using standard study instrument adopted and adapted as appropriate.
CONCLUSION AND RECOMMENDATION
6.1 Conclusion
The level of knowledge regarding PCa and its screening practices was poor. There was a significant association between education level and PCa knowledge, indicating that this factor significantly influences people’s knowledge, perceptions, and rates of screening for PCa.
6.2 Recommendations.
- To increase awareness, perceptions, and the rate of prostate cancer screening in the Nnewi community, extensive education about the disease is advised.
- The government should permit unlimited access to prostate cancer screening programs for people who are at risk of developing prostate cancer.
- Government and healthcare providers must educate the public about prostate cancer and how to prevent it.
- It would also be helpful to periodically review Nigerians’ knowledge and perception towards prostate cancer screening.
- Early detection and treatment of prostate cancer is important for reducing mortalities in men.
FUNDING
There was no funding from any resource in this study.
REFERENCES
- What Is Prostate Cancer? | CDC. Accessed March 16, 2022. https://www.cdc.gov/cancer/prostate/basic_info/what-is-prostate-cancer.htm
- Mba WP. Prostate cancer awareness, knowledge, perception on self-vulnerability and uptake of screening. Published online 2013.
- Ikuerowo SO, Omisanjo OA, Bioku MJ, Ajala MO, Nonyelim Mordi VP, Esho JO. Prevalence and characteristics of prostate cancer among participants of a community-based screening in Nigeria using serum prostate specific antigen and digital rectal examination. Pan African Medical Journal. 2013;15:1-7.
- Rawla P. Epidemiology of prostate cancer. World Journal of Oncology. 2019;(April);10(2):63-69.
- Wilson SS, Crawford ED. Screening for prostate cancer. The New England Journal of Medicine. 2004;3(1):21-25.
- Ebuehi OM, Otumu IU. Prostate Screening Practices Among Male Staff of the University of Lagos, Lagos, Nigeria. African Journal of 2011;17(4):122-134.
- Enemugwem RA, Eze BA, Ejike U, Asuquo EO, Tobin A. Prostate cancer screening : assessment of knowledge and willingness to screen among men in Obio Akpor LGA , Rivers State , Nigeria. African Journal of 2019:10-13.
- Ogbetere FE, Ogbetere YN. Sociodemographic determinants of the level of knowledge of prostate cancer and prostate cancer screening services among patients attending a sociodemographic determinants of the level of knowledge of prostate cancer and prostate cancer screening services. 2021;4(1):15-22.
- Mulhem E, Beaumont W, Heights S, Fullbriht MN, Hospital P, Lyon S et al. Prostate Cancer Screening. American Family Physician 2015;92(8):683-688.
- Agbo CA, Shuaibu SI. Review article: prostate cancer screening using prostate specific antigen: controversies and recommeandations. Jos Journal of Medicine. 10(1):32-34.
- Aluh DO, Anyachebelu OC, Azubuike EA, Abdulmuminu I. Knowledge, attitudes, and perception of prostate cancer among male outpatients of a tertiary care hospital in south-east Nigeria. Journal of Appllied Pharmaceutical Sciences. 2018;8(11):64-68.
- Nartey Laweh V, Manortey S. Assessment of knowledge and practices of prostate cancer screening among men in the lower Manya Krobo Municipality in the Eastern Region of Ghana. Cancer Research Journal. 2021;9(1):41-52.
- N Ozoemena OF, Ayogu BO, Ugonabo M, Ugwumba FO, Udeh EI, Nnabugwu II,et al. Awareness of prostate cancer and the use of PSA as a screening test among the Black Race: South -South and South-East Nigeria, Nigerian Experience. IOSR Journal of Dental and Medical Sciences Version IV. 2015;14(4):25-29.
- Hao S, Östensson E, Eklund M, Gronberg H, Nordstrorm T, Heintz E, et al. The economic burden of prostate cancer – a Swedish prevalence-based register study. BMC Health Serices Research 2020;20(448):1-15.
- Nnewi – Wikipedia. Accessed February 3, 2022. https://en.wikipedia.org/wiki/Nnewi
- Oluwole TG. Risk Perception and uptake of prostate cancer screening among a population of civil servants in Ibadan , Nigeria. African Journal of Biomedical Research. 2021;24(2003):231-237.
- Husaini DC, Harris-thurton L, Brown NT, Noelo JC, Pot SV, Humes A, et al. Prostate cancer awareness , knowledge , and perception of screening among men aged 40 – 70 in the Belize district. Journal of Public Health From Theory to Practical. 2021:1-9.
- Atulomah NO, Olanrewaju MF, Amosu AM, Adedeji O. Level of awareness , perception and screening behavior regarding prostate cancer among men in a rural community of Ikenne Local Government Area , Nigeria. Primary Prevention Insight. 2010;2:11-20.
- Ogunsanya ME, Brown CM, Odedina FT, Barner JC, Adedipe TB, Corbell B. Knowledge of prostate cancer and screening among Young Multiethnic Black Men. American Journal of Men’s Health. 2017;11(4):1008-1018.
- Oranusi CK, Mbieri UT, Oranusi IO, Nwofor AME. Prostate cancer awareness and screening among male public servants in Anambra state, Nigeria. African Journal Urology. 2012;18(2):72-74.
- Wachira BW, Wankuru L, Ruth MG. Knowledge , perception and uptake of prostate cancer screening : A cross sectional study at a level III Hospital in Kenya. 2018;8(4):81-87.
- Gift S, Nancy K, Victor M. Assessment of knowledge, practice and attitude towards prostate cancer screening among male patients aged 40 years and above at Kitwe Teaching Hospital, Zambia. African Journal Uroloy. 2020;26(1):1-7.
- Awosan KJ, Yunusa EU, Agwu NP, Taofiq S. Knowledge of prostate cancer and screening practices among men in Sokoto , Nigeria. Asian Journal Medical Sciences. 2018;9(6):51-56.
- Adibe MO, Aluh DO, Isah A, Anosike C. Knowledge , attitudes and perceptions of prostate cancer among male staff of the University of Nigeria. Asian Pacific Journal Cancer Prevention. 2017;18:1961-1966.
- Oladepo O, Yusuf BO, Akinola Y, Arulogun OS. Prostate Cancer Awareness , Knowledge , and Screening Practices among Older Men in Oyo State , Nigeria. International Quarterly Community Health Education. 2009;30(3):271-286.
- Morlando M, Pelullo CP, Giuseppe G Di. Prostate cancer screening : Knowledge , attitudes and practices in a sample of men in Italy . A survey. PLOS ONE 2017:1-11.
- Waseem Y, Jatoi NN, Khan BA, Butt SJ, Wasif KU, Mirza N. Knowledge and perception regarding prostate cancer among men in Karachi , Pakistan. Journal of Pakistan Medical Association. 2022;72(1):194-198.
- Agbugui JO, Obarisiagbon EO, Nwajei CO, Osaigbovo EO, Okolo JC, Akinyele AO. Awareness and knowledge of prostate cancer among men in Benin city, Nigeria. Journal of Medicine and Biomedical Research. 2013;12(2):42-47.
- Mbugua RG, Oluchina S, Karanja S. Prostate cancer awareness and screening among men in a rural community in Kenya: a cross-sectional study. African Journal of Urology. 2021;27(1):1-10.
- Vapiwala N, Miller D, Laventure B, Woodhouse K, Kelly S, Avellis J, et al. Stigma , beliefs and perceptions regarding prostate cancer among Black and Latino men and women. BMC Public Health. 2021:1-11.