
Review on the Health Impact of Trace Elements Bound in Inhalable Particles
- Ewona I. O.
- Uza, T. I.
- Rabiu B. A.
- Udo, S. O.
- Eka, B.
- Ukam, L. E.
- 450-463
- Aug 3, 2024
- Health
Review on the Health Impact of Trace Elements Bound in Inhalable Particles
*1Ewona I. O., 1Uza, T. I., 3Rabiu B. A., 2Udo, S. O., 2Eka, B., 4Ukam, L. E.
1Physics Department, University of Cross River State, Calabar.
2Physics Department, University of Calabar, Calabar.
3United Nations – African Regional Centre for Space Science and Technology Education – English, (UN-ARCSSTE-E), (affiliated to the United Nations) Obafemi Awolowo University Campus, Ile Ife, 220282, Nigeria
4Department of urban and Regional Planning, University of Cross River State, Calabar
*Corresponding Author
DOI: https://doi.org/10.51244/IJRSI.2024.1107033
Received: 24 May 2024; Revised: 21 June 2024; Accepted: 25 June 2024; Published: 03 August 2024
ABSTRACT
The health impacts of trace elements bound in inhalable particles is attracting global concern as a result of the toxicological and carcinogenic properties some elements carry. This paper is a review of the effects of trace elements on human health. It is reported that trace elements in inhalable particles are often entrained in human respiratory airways, deposited in human nasal cavity and made available for absorption by the human tracheobronchial system. It has been reported that variability and bio accessibility of elements in the serum (blood) correlate with some health and diseases. different kinds of simulated body fluids have been used to demonstrate the bio accessibility of trace elements bound to inhalable particulates. Presented also are evidences of serum (blood) variation in some respiratory diseases, such as chronic obstructive pulmonary disease (with or without hypertension), emphysema, bronchiectasis and bronchial asthma, non-tuberculose mycobacterial (NTM) lung disease, idiopathic pulmonary fibrosis (IPF).
Keywords: trace elements, particulate matter, inhalation bio accessibility, respiratory fluid, health effect, disease.
INTRODUCTION
Since the industrial revolution, a considerable increase in air pollution has been noted. According to a World Health Organization air quality report [1], inhalation of trace elements bound to airborne particulates is worsening air pollution in cities of the world, thereby causing more than 2 million premature deaths annually. By 2016 the World Health Organization [2] already reporting that air pollution is responsible for about 7 million premature deaths globally. In urban centers, particulate matter are major pollutants in the atmosphere, as they present health risk to dwellers. Urban particulates are known for their heterogeneous mix with diverse natural and anthropogenic origins. The composition can vary depending on geographical location, re-suspended soil, atmospheric deposition and other sources, which include traffic related particles such as metallic components, eroded road pavement, building construction and demolition, and power generation [3, 4]. The mean daily concentration of PM of ≤10 μm in diameter (PM10) ranges from <10 μg/m3 to 200μg /m3 [5]. In 2002 the USEPA reported a range of maximal city concentrations of 25–534 μg/m3 [2]. These toxic contaminants originated mainly from the anthropogenic emission sources, through ubiquitous applications of elements in urban centers including automobile, industries and domestic fuels combustion [3]. 2021 WHO [6] reports that air pollution is the 4th leading risk factor for premature death and accounts for about 12 percent of all deaths, worldwide, reducing life expectancy by 2.2 years on average.
Quite a lot of researchers have investigated elemental compositions of suspended particulate matters in cities worldwide [5, 7,8,9,10]. In most of these studies, elevated levels of trace elements have been observed in atmospheric suspended dust in most cities. For example, Okunola et al. [9] reported the presence of Cd, Cr, Ni, Pb, Cu, and Zn in atmospheric settling dust in Kano metropolis of Nigeria. Meanwhile, Mafuyai et al. [10] reported that the concentrations of some trace elements were found to be far above the standard limits prescribed by WHO for respirable dust in Jos, Nigeria. Therefore, urban dwellers are exposed to considerable amounts of these elements through inhalation of airborne particulates. Ewona et al. had worked extensively in Calabar to characterized trace elements in ambient air particulate [11, 12]
Some studies which focused on the health problems associated with exposure to Particulate Matter (PM)) have linked both long-term and short-term health effects, such as declining lung function, increased respiratory problems, chronic pulmonary diseases, heart diseases, lung cancer, damage to other organs and premature death along with a rise in mortality (13,14,15,16, 17,18,19,20].
For instance Oyewale et al. [21] assessed the health risks associated with exposure to particulate matter (PM10), Sulphur dioxide (SO), nitrogen dioxide (NO2), carbon monoxide (CO) and ozone (O3). The study was carried out within an industrial area in Pretoria West, South Africa. By applying the US Environmental Protection Agency human health risk assessment framework, they showed infants and children were most vulnerable even at 8 – hourly exposures. Moreover, for chronic annual exposure, PM10, NO2 and SO2 posed a health risk to sensitive individuals, with the severity of risk varying across exposed groups. Asmamaw et al. [22] indicated that the toxic content of air pollution was traceable to the use of low standard vehicular engines and and fuels, cooking with solid fuels, and burning household waste.
Once inhaled, trace elements in air particles are deposited in the lung and thereby cause serious health effects. Ruby et al [23] reported that more than 80% of the binding mass of particles smaller than 2.5 μm reaches the pulmonary alveoli, where a small fraction is deposited and can stay for months to years. Zwozdziak et al [24] has also observed that elements deposition in human respiratory tract decreases with increase depth. Recognizing that dissolution of inhaled particulate-bound metal in the body has been observed to depend on the ability of such metal to be solubilized in body fluids [9], therefore it is only such soluble fraction of the elements which can be taken across the cell membrane through lung pathway that have direct effects on health. Hence, it is important to assess the bio accessibility of trace elements bound to inhale particles over total metal concentration in particle’s matrix.
1. Trace Elements
The names heavy metals, trace elements and trace metals are often used interchangeably by many authors but from elementary Chemistry, there are differences. Methods commonly used to detect metals include: Atomic absorption spectroscopy (AAS) and spectrophotometry. AAS is a fast and precise technique for detecting metallic elements. Most nonmetals cannot be readily detected by AAS. The challenge is that non-metal resonance lines are all located in the vacuum ultraviolet wavelength region and ASS has limited accessibility. However, non-metals can be detected through molecular absorption using high-resolution continuum source absorption spectrometry and graphite furnace atomization. Trace elements are elements present in natural materials at concentrations of <1000 mgkg−1 [24,25] Some of them are essential micronutrients that exist in very low concentrations in the body, forming 0.01% of the total body weight [7,12]. But, in higher concentrations, they are toxic to organisms, including humans [1,7]. Metals such as lead [8,9] and cadmium [9,10] are harmful in any amounts because they exhibit a high degree of toxicity, interfering with metabolic processes in the human body [25]. Some however, are classified as non-essential. Trace elements are categorized into metals, nonmetals and metalloids.
2. The Role of Trace Elements in Biological Processes
Some trace elements are necessary for proper body metabolism such as regulating cell metabolism, activation or inhibition of enzymatic reactions, and regulation of gene and membrane functions. Essential structural parts of many enzymes have trace elements where they function as a cofactor [25]. By their activator or inhibitor and antioxidant activities, these enzymes play the role of protecting the body against diseases by producing defense system molecules. For example, Iron is an important constituent of succinate dehydrogenase as well as part of heme of the haemoglobin, myoglobin and the cytochromes [26].
Trace elements are distributed based on the underlying geological formation and industrial activities. Both natural processes and anthropogenic factors are responsible for trace element distribution and concentration in ambient air [27,28,29]. Their effects on biological processes also differ according to the nature of the element. For instance, Zinc is involved in carbonic acid (Carbonic anhydrase) and in alcohol (alcohol dehydrogenase) formation, and in proteolysis (Carboxypeptidase, leucine, aminopeptidase etc) [30]. Copper is present in many enzymes involved in oxidation (tyrosinase, ceuloplasmin, amino oxidase, cytochrome oxidase) [31]. Changes in the levels of these trace elements decrease the efficiency of the antioxidants systems and lead to hyper-reactivity and inflammation in the respiratory tract [32,33].
Through trace elements play important roles in various physiological processes including the body immune system, excessive accumulation or deficiency of some of these elements in the human body have been associated with metabolic disturbances, tissue damage and respiratory and cardiovascular diseases.
3. Sources of Particulate Matter and Trace Elements in Urban Atmosphere
Human activities have been found to contribute more to environmental pollution due to the everyday manufacturing of goods to meet the demands of population growth [34]. Particulate matter in general could either come from natural sources such as marine water sprays, and volcanic eruption and winds or human-derived sources like pesticides, paints, bush burning, vehicular emission, land preparation and a variety of industrial processes, like cement and metals manufacturing, fumes from incinerators, power plants, refineries, smelting, etc. Figure 1. illustrates the cycle of trace elements in the atmosphere of a typical urban center.

Fig. 1. Cycling of trace elements in the urban atmosphere in (new)
Increase in trace elements in the atmosphere has been traced to anthropogenic emission sources such as vehicular emission, automobile, industrial fumes and domestic fuels combustion [35]. Trace elements emitted in wind-blown dusts are mostly from industrial areas. For instance, automobile exhaust emits lead; smelting produces arsenic, copper and zinc; insecticides also give out arsenic and burning of fossil fuels generally releases nickel, vanadium, mercury, selenium and tin. Other metals found in air particles are iron (Fe), (Zn), and Nickel (Ni), and recently with the use of the catalytic converters Platinum (Pt), Paladium (Pd) and Rhodium (Rh) have been reported.
4. Routes of Exposure and Safety Limits of Some Trace Elements
We are exposed to trace elements in the environment through different routes including ingestion, inhalation of dusts, gases, aerosols and dermal absorption (through skin). The knowledge of these routes may help us appreciate the impact of trace elements on health and perhaps lead us to appropriate safety measures. For trace metals in urban centers the routes are occupational based and element specific. Below are some of the impacts some trace elements have in the human body when one is exposed particulate matter (PM)containing them.
- Cadmium (Cd): Cd is an environmentally widespread toxic element. It is classified as a group I carcinogen by IARC (International Agency for Research on Cancer) and has been associated with lung cancer [36]. The modes of human exposure are contamination of food, drinking water, occupational or by inhalation in polluted air. Occupational exposure to cadmium primarily takes place in industrial factories such as zinc smelting, battery manufacturing and metal-recovering, cadmium-refining, production units for paint and pigment. The threshold safety cadmium exposure level has been set at 2.5 μg/kg body weight per week [36]. Cadmium (Cd) exposure is known to induce pulmonary damage such as emphysema and lung cancer [37].
- Lead (Pb): Lead in the atmosphere comes from sources such as; gasoline additive, paints, cosmetics, ceramic glaze, etc. [38]. Lead enters the human body by ingestion or inhalation. According to the WHO-OSHA, the established safety standard for blood lead in workers is 40 μg/dL. However, it has been suggested that the criterion for elevated blood levels in children is too high in adults therefore recommended a new set of guidelines levels >15 μg/dL [39].
- Manganese (Mn): Atmospheric Manganese originates from gasoline additive, methylcyclopentadienyl manganese tricarbonyl (MMT) is a putative modulator of dopamine biology (the primary target of Mn neurotoxicity) [40].
- Chromium (Cr): Chromium is widely used in the industry for the production of stainless steel, chromium plating, and spray-painting. According to World Health Organization (WHO) [41], the long term exposure of Cr (VI) levels of over 0.1 ppm causes respiratory problems, liver and kidney damage, and carcinogenicity. According to epidemiological study [42], the hexavalent form [Cr (VI)] of this metal, appears to be drastically toxic and carcinogenic, thus it has been classified as carcinogenic to humans by the IARC.
- Aluminum (Al): Aluminum and its compounds [43] are released into the atmosphere during activities such as aluminum mining, processing, production and recovery. The skin, nose, lung and gastrointestinal tract is a route for the uptake of aluminum in the body [44]. Therefore, people close to industrial areas may be exposed to aluminum through inhalation of airborne particulates.
- Arsenic (As): Elemental arsenic is a metalloid that exists in two valence states; trivalent, pentavalent states. The main sources of exposure to arsenic include; occupational, environmental and medicinal sources. The safety level of arsenic has been lowered from 50 ppb to 10 ppb by United State Environmental Protection Agency [45]. The presence of arsenic in airborne particulate matter is considered a risk for certain diseases. All the potential pathways of its exposure seem to have adverse effect on human health [46]. Arsenic exposure has been repeatedly associated with lung carcinogenesis [47].
- Vanadium: Vanadium is a major transition element that is released primarily by the burning of fossil fuels, including petroleum, oil, coal, tar, bitumen, and asphaltite. Among Vanadium compounds, Vanadium pentoxide is highly toxic [48]. The IARC classified it as a possible carcinogen to humans (Group 2B) in 2003 [49].
- Zinc: Occupational studies of workers exposed to zinc by inhalation (usually in the presence of other trace elements such as copper, lead, arsenic, and chromium) have not implicated zinc as a risk factor for cancer [50].
5. Impact on the Respiratory System
The fate and behavior of trace elements in the respiratory tract are fundamental to understanding of their health effects and in recent time has become a key aspect of potential health risk assessment. Particulate matter is inhaled during breathing. Upon inhalation, deposition of the particles in the lung may occur through five different mechanisms: sedimentation (gravity), inertial impaction, interception (particle-surface contact), electrostatic deposition, and diffusion. These mechanisms generally occur in different regions of the respiratory tract [17,51,52]. Human respiratory tract can be divided into the upper respiratory region (nasal airway, pharynx and larynx), the lower respiratory region (trachea and bronchi) and the alveolar region. Figure 2a shows the particle size distribution in human respiratory tract. Meanwhile figure 2b illustrates the health risk of trace elements and bioaccessibility questions. The extent of particle deposition in the lung is determined by the physicochemical properties of the particles, such as size, shape, density, and surface chemistry [53] (see figure 2a). Breathing conditions, like ventilation rate, mouth or nose breathing, and airway geometry are other factors that affect particle deposition [54]. The transportation of particles into the lung can be explained by their aerodynamic diameter [55]. Meanwhile, materials with an aerodynamic diameter below 5 μm are predominantly deposited in the alveolar regions of the airways [56].
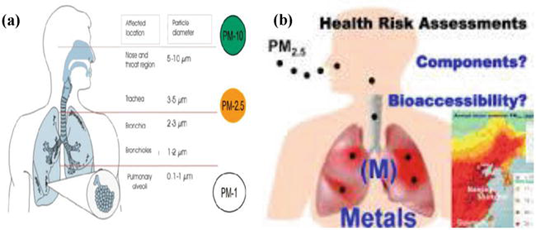
Figure 2. (a) Dust particle sizes distribution in human respiratory tract (b) human health risk and bio accessibility questions. source
When trace elements are absorbed through the respiratory tract, they are transported in blood bound to metallothionen [60]. Figure 3 shows they form a Glutathione-trace element complex with glutathione. This is then followed by alteration of homeostasis [61], thus directly increasing the oxidative stress and lipid peroxidation.

Figure 3. Glutathione-trace element complex
6. Mechanisms of Inhaled Trace Elements Toxicity
A primary mechanism for most trace elements toxicity is their effects on cells which has been ascribed to the oxidative stress promoting actions, as observed in in vivo [62] and most importantly, the inactivation of enzyme systems by binding to sulfhydryl groups [63] of proteins. The mechanisms of their actions include genetic change reactions; reactive oxygen free radicals and adduct formations, oxidative stress, and inflammation [64].
i. Reactive oxygen species (ROS) generation
Reactive oxygen species (ROS) such as superoxide, hydroxyl radical, nitric oxide radical are byproducts of metabolic processes. External substances such as cigarette smoke, pesticides and inhalation of trace elements -bound particulate matter can also cause the formation of free radicals in the body. Trace elements in particulate matter have been reported to cause oxidative stress. For example, pentavalent form of vanadium is reported to cause ROS generation, thus induce oxidative stress, DNA damage, and activation of hypoxia signaling [65]. Oxidation stress is a phenomenon caused by an imbalance between production and accumulation of oxygen reactive species in cell and tissues and the ability of a biological system to detoxify these reactive products [66]. Cadmium causes liver damage mainly by induction of ROS inducing lipoperoxidation via Fenton reaction [67]. The increment of ROS induces DNA damage, proteins oxidation and lipid peroxidation. Copper ions are well suited to facilitate formation of ROS that can damage biomolecules, including DNA and chromatin
ii. DNA adducts formation
The genetic changes reaction of trace elements involves the formation of DNA-protein cross-links, single and double strand DNA breaks [67,68]. The reaction of elemental ions with nucleic acid lead to a variety of dramatic effects on the nucleic acid structure e.g. crosslinking of polymer strands, degradation to oligomer and monomers, stabilization or destabilization, and the mispairing of bases. For example, Copper can directly bind with high affinity to DNA molecule; this binding can modify the conformational structure of DNA promoting carcinogenesis [69]. Cadmium also produces genotoxicity by the production of DNA single strand breaks and damage and competes for binding at sites (specifically with some zinc finger motifs that are important in gene regulation, enzyme activity, or maintenance of genomic stability [70].
7. Concept of Bioavailability and Bio Accessibility
In toxicological study, the potential health risks of individual elements bound to inhale particulate matter depend on particle size, inhalability, bioavailability/bio accessibility, exposure dose and deposition/retention in respiratory tract [71,72]. It has been emphasized that bio-toxicities of trace metals depend not only on the concentration as expressed by total amount, but also on their geochemical fractions and bioavailability [73]. Bioavailability is the fraction of total elements that can enter the human systemic circulation and exert toxicity on the organs [74] Meanwhile, bio accessibility refers to the fraction of contaminant that may become available for absorption e.g., solubilized in the respiratory tract fluid or volatilized into inhaled air and released from the matrix in a topically absorbable form. Bio accessibility. (%) can be defined as the ratio of soluble fraction of trace elements in simulated lung fluids (SLF) to the total concentrations.
8. Bio accessibility of trace elements bound to particulate matter
The dissolution of particulate-bound metal in the body has been observed to depend on the ability of such element to be bio accessible (solubilized) in body fluids after inhalation [75]. Different particulate-bound elemental species behaves differently in human body after inhalation and deposition, depending on their bio accessibility in lung fluids. In general, high bio accessible elements are easily taken up by the lung fluids and get introduced to human circulatory system. Recognizing that only soluble fraction of the metals which can be taken across the cell membrane through lung pathway has more direct effects on health. Thus, bio accessibility of trace elements bound to inhale particles over total metal concentration in particle’s matrix is being considered important for assessment of the overall health risk associated with inhalation of particulate matters.
9. Variation in serum trace elements levels and induced respiratory tract diseases and health problems
Unlike other organs, lungs are directly and continuously exposed to high oxygen concentrations, exogenous oxidants, and pollutants: thus, they have the greatest susceptibility to oxidative stress and pollutant toxicity. The existence of concentration gradient within the lung and inter-individual concentration differences reveals the existence of two groups of elements: (i) homogeneously distributed over the lung e.g. elements Br, Cs, Cu, K, Na, Rb, Se and Zn, and (ii) heterogeneously distributed e.g. elements such as Cd, Co, Cr, Pb, Sb, Sc and V [76].
i. Chronic obstructive pulmonary disease (COPD): The enrichment of trace elements in the lung tissue is known to result to a number of lung diseases. Diseases such as chronic obstructive pulmonary disease (with or without hypertension), emphysema, bronchiectasis and bronchial asthma, non-tuberculose mycobacterial (NTM) lung disease, idiopathic pulmonary fibrosis (IPF) have been associated with disturbance of trace elements balance [77]. Many trace elements have activator or inhibitory roles in the antioxidants defensive mechanism in diseases. Recent study [78] showed that serum levels of Co, Cu and Fe were higher in COPD patients with pulmonary hypertension compared to COPD patients without pulmonary hypertension. Similarly, [78] reported that the serum copper (Cu) in COPD patients were higher than the control group.
ii. Bronchial asthma: Bronchial asthma is a chronic inflammatory disease of the respiratory tract with an unknown etiology where inflammation is often associated with an increase generation of ROS [79]. Several trace elements are known to be capable of causing bronchial asthma, such as nickel (Ni), Chromium (Cr), Cobalt (Co) etc. Table 2 presents the variations in concentrations of some trace elements (Zn, Cu and Se) in serum of asthmatic, as observed in a study [80]. The results showed higher Cu concentration, and Cu/Zn and lower Cu/Se ratios.
Table 1. Variation of trace elements in serum of asthmatic patients [80, 81].

iii. Idiopathic pulmonary fibrosis (IPF): Idiopathic pulmonary fibrosis is an interstitial lung disease with poor prognosis and an undefined etiopathogenesis [82] leading rapidly to death. It is the most common lung disease with estimated incidence of 2.8–9.3% per 100,000 per year in Europe and America [83]. Particulate matter bound trace elements deposited in the lung may give rise to more or less marked pulmonary fibrosis, depending on intrinsic properties and amount of the particulate matter. Oxidative stress by trace elements contributes to alveolar injury and fibrosis development in patients. A study [84] reported that IPF patients show significant increase in sputum levels of Cd, Cr, Cu and Pb. Table 3 presents the variations in concentrations of some trace elements in serum in patents with NTM, TB withy healthy as control [84].
Table 2. Serum levels of trace elements in patents with NTM, TB and healthy [85].

iv. Non-tuberculose mycobacterial lung diseases (NTM): Non-tuberculose mycobacterial lung diseases are emerging cause of pulmonary infection and are becoming more common in the clinical setting. One study [85] showed that serum concentration of copper and molybdenium (Table 4) were higher in patients with NTM lung disease (109 vs. 91 μg/dL, p < 0.001 and 1.70 vs. 0.96 μg/L, p < 0.001). In contrast, the media serum concentrations of Selenium and Zinc were significantly lower in patients with non-tuberculose mycobacterial lung diseases than in healthy control (105 vs. 115 μg/L, p < 0.001 and 94 vs. 102 μg/dL, p < 0.001).
Table 3. Serum levels of trace elements in patents with Haemodialysis compare with control [86].

v. Haemodialysis: Oxidants-antioxidants balance is essential for the normal lung function. Both, an increased oxidant and/or decrease antioxidant may reverse the physiologic oxidants-antioxidants balance, leading to lung injury. Available data (86) suggested that the levels of Cd, Cr, Pb, and V were higher and the levels of Se, Zn and Mn were lower in hemodialysis patients compared with controls [86].
vi. Parkinson disease: Parkinson disease, also known as manganism is an extrapyramidal neurological disease characterized by rigidity action tremor, bradykinesia, memory and cognitive dysfunction that occurs in workers exposed to airborne Mn. The element (Mn) in blood crosses the blood brain barrier and accumulates inside the neuron disrupting the synaptic transmission and inducing glial activation [87].
10. Health and environmental impacts of trace elements
The list of most common trace metals includes: lead, zinc, cadmium, nickel, copper, cobalt, chromium, barium and strontium. Metalloids, on the other hand, are antimony and arsenic, while non-metals are bromine and sulfur. Their concentration may however, be in amounts that can be considered to be infinitesimal or at levels equivalent to those of major elements. Both natural processes and anthropogenic activities such as agriculture, urbanization, industry and services [88,89,90,91] have greatly affected their distribution in in the natural environment.
Increase in pollutant levels have been linked to human activities which have had adverse effect on the environment by polluting the water we drink, the air we breathe, and the soil in which plants grow. Although the industrial revolution was a great success in terms of technology, society, and the provision of multiple services, it also introduced the production of huge quantities of pollutants as by products emitted into the environment. Without any doubt, the global environmental pollution is considered an international public health issue with multiple facets. Social, economic, and legislative concerns and lifestyle habits are related to this major problem. Clearly, urbanization and industrialization are reaching unprecedented and upsetting proportions worldwide. Anthropogenic air pollution has become one of the biggest public health hazards worldwide, accounting for about 9 million deaths per year [11,12, 88,89,90].
MATERIALS AND METHODS (SEARCH PROCESS)
This article uses keywords such as trace elements, particulate matter, inhalation bio accessibility, respiratory fluid, health effect, disease. “search Web of Science, PubMed and Google Scholar include SCI and SSCI indexed papers, research reports, and works from 2012 to 2024.
A literature search done in 2020 was repeated in 2024 using “PubMed” and “Web of Science” database sources that cover health, medical, and environmental literature. We attempted to assess the effects of air-pollution and weather events on mortality and hospital admission in Europe by searching original research articles published in peer-reviewed journals in the last 10 years (between 06/02/2012 and 06/02/2022 inclusive). We chose to review research published in the last 10 years because in March 2007, the European Union (EU) Heads of State and Government endorsed an “integrated climate change and energy strategy” that will come into action post the expiry of Kyoto Protocol targets in 2012 and that aims to combat climate change and weather fluctuations and cut air-pollution emissions to 30% below the 1990 levels
Our search strategy was divided into the following conceptual categories:
i. Routes of exposure and safety limit of some trace elements
ii. Behavior, fate, and effects of trace elements in the respiratory tract
iii. Variation in serum (blood) trace elements levels and induced respiratory tract diseases and health problems
CONCLUSION
Trace elements bound to particulate matter could be trapped and deposited along the nasal cavity through inhalation of air-borne particulate matter. In this review, we attempted to show the grave impact trace elements have human health. There was also an attempt to review the influence of serum levels and bio accessibility of trace elements in some respiratory fluids. Our investigation provides evidence are responsible for oxidative stress, various cancers and internal organ failure. Additionally, the review reveals that enrichment of trace elements in the lung tissue is responsible for a number of lung diseases, such as chronic obstructive pulmonary disease (with or without hypertension), bronchial asthma, non-tuberculose my cobacterial (NTM) lung disease, and idiopathic pulmonary fibrosis (IPF). The findings suggest that serum Cu were higher in asthmatic patients and COPD patients than the healthy. Meanwhile, the levels of Se, Zn and Mn were lower in hemodialysis patients and non-tuberculose mycobacterial lung diseases than in healthy control sample.
ACKNOWLEDGEMENT
The Authors are grateful to the Nigerian Government for sponsoring the Air Quality project through the National Research Fund (NRF) under the Tertiary Education Trust Fund (TET Fund)
REFERENCES
- WHO (World Health Organization), 2014. Ambient Air Quality and Health, hppp://www.who.int/mediacentre/factsheets/fs313(access). [PubMed | Google Scholar]
- WHO Exposure to ambient air pollution [internet] WHO.2016 [cited 2016 Dec 29]. Available from http://www.who.int/gho/phe/outdoor-air-pollution/exposure). [PubMed | Google Scholar]
- Kelly FJ, Fussell JC. Size, source and chemical composition as determinants of toxicity attributable to ambient particular matter. Atmospheric Environment, 2012; 60, 504-526). [PubMed | Google Scholar]
- Grobéty B, Gieré R, Dietze V, Stille P. Airborne particles in the urban environment. Elements, 2010; 6: 229-234). [Pubmed | Google Scholar]
- Amato F, Pandolfi M, Moreno T, Furger M, Pey J, Alastuey A, Bukowiecki N, Prevot ASH, Baltensperger U, Querol X. Sources and variability of inhalable road dust particles in three European cities. Atmos. Environ. 2011; 45: 6777-6787). [PubMed | Google Scholar]
- WHO 2021. New WHO Global Air Quality Guidelines aim to save millions of lives from air pollution. Downloaded from https://www.dw.com/en/who-air-pollution-causes-7-million-premature-deaths-a-year/a-59264198 on 31ST May 2022 [Pubmed | Google Scholar]
- Caroline Kiai, Christopher Kanali, Joseph Sang and Michael Gatari, (2021). Spatial Extent and Distribution of Ambient Airborne Particulate Matter (PM5) in Selected Land Use Sites in Nairobi, Kenya. Journal of Environmental and public health, (2021),11. [Pubmed | Google Scholar]
- Celik I, Gallicchio L, Boyd K, Lam TK, Matanoski, G, Tao X, et al. Arsenic in drinking water and lung cancer: a systemic review. Environ. Res. 2008; 108: 48-55). [PubMed | Google Scholar]
- Li F, Zhang J, Huang J, Huang D, Yang J, Song Y, Zeng G. Heavy metals in road dust from Xiandao District, Changsha City, China: Characteristics, health risk assessment, and integrated source identification. Environ. Sci. Pollut. Res., 2016; 23: 13100-13113). [Web of Science, PubMed and Google Scholar]
- Obioh IB, Ezeh GC, Abiye OE, Alpha A, Ojo EO, Ganiyu AK. Atmospheric particulate matter in Nigerian megacities, Toxicol Environ Chem. 2013; 95 (3): 379-385). [PubMed | Google Scholar]
- Ewona, I.O, Ibor I.E, Egor A.O. (2021). Evaluation of Trace Metals in Particulate Matter from the Ambient Air of Calabar Metropolis, Cross River State, Nigeria. International Journal of Engineering Sciences & Research Technology, IJISRT 6(12). [Pubmed | Google Scholar]
- Ewona, Igwe Otaba and Ibor, Iwara Edet (2022). Health Risk Assessment of Heavy Metals in Ambient Air around Calabar Metropolis, Nigeria. Journal of Contemporary Research (JOCRES) 1 (1)153 – 162. Available online www.unicrossjournals.com.
- Christopher F. Rider and Chris Carlsten, (2019). Air pollution and DNA methylation: effects of exposure in humans. Rider and Carlsten Clinical Epigenetics, 11; 131. [Pubmed | Google Scholar]
- Ala’a Hamed Emran Al-Husseini (2021), Evaluation Effect of Inhalable Particulate Matter Exposure on Human Health in Center of Karbala City. International Journal of Engineering Research & Technology (IJERT). Vol. 10 Issue 07, July-2021. ISSN: 2278-0181. [Pubmed | Google Scholar]
- Energy & Environment (2021). Air pollution shaves off 2.2 years of average life expectancy worldwide, 2021 – from https://www.axios.com/air-pollution-global-life-expectancy- report-fb6a821c-95aa-4671-8005-caac8be0e69b.html downloaded on 20th November [Pubmed | Google Scholar]
- Abdulaziz, M., Alshehri, A., Yadav, I. C. and Badri, H. (2022). Pollution level and health risk assessment of heavy metals in ambient air and surface dust from Saudi Arabia: asystematic review and meta-analysis. [Pubmed | Google Scholar]
- Guittikunda, K., Sarath and Ramani V. Kopakka (2014). Source emisions health impacts of Urban air Pollution in Hyderabad, India air Quality Atmosphere and Heath, 195 – 207. [Pubmed | Google Scholar]
- Population Review (2021). Most Polluted Countries 2021-World Population Review. From https://worldpopulationreview.com/country-rankings/most-polluted-countries downloaded on 24th December 2021. [Pubmed | Google Scholar]
- SOGA (2020). Air Pollution’s Impact on Health: A Global Snapshot from https://www.stateofglobalair.org/ downloaded on 27th December, 2021. [Pubmed | Google Scholar]
- Encyclopedia of Geology (Second Edition), 2021. Science Direct. Here is the link to “Medical Geology”: https://www.sciencedirect.com/science/article/pii/B9780124095489125230).
- Oyewale Mayowa Morakinyo,Ayo Stephen Adebowale, Matlou Ingrid Mokgobu, Murembiwa Stanley Mukhola1, (2022). Health risk of inhalation exposure to sub-10 µm particulate matter and gaseous pollutants in an urban-industrial area in South Africa: an ecological study. Department of Environmental Health, Faculty of Science, Tshwane University of Technology, Pretoria, South Africa. Department of Epidemiology and Medical Statistics, Faculty of Public Health, College of Medicine, University of Ibadan, Ibadan, Nigeria. [Pubmed | Google Scholar]
- Asmamaw Abera, Johan Friberg, Christina Isaxon, Michael Jerrett, Ebba Malmqvist, Cheryl Sjöström, Tahir Taj, and Ana Maria Vargas, (2021). Annual Review of Public Health. 2:193–210. [Pubmed | Google Scholar]
- Ruby MV, Lowney YW, Bunge AL, Roberts SM, Gomez-Eyles JL, Ghosh U, Kissel JC, Tomlin-son P, Menzie C. Oral Bioavailability, Solubility or dissolution, and Dermal Absorption of PAHs from Soil-State of the Science. Environ. Sci. Technol., 2016; 50: 2151-2164). [PubMed | Google Scholar]
- Zwozdzaik A, Gini MI, Samek L, Rogula-Kozlowka W, Sowka L, Eleftheriadis K. Implications of the aerosols size distribution modal structure of trace and major elements on human exposure, inhaled dose and relevance to the PM2.5 and PM10 metrics in European pollution hotspot urban area. J. Aerosol Science. 2017; 103: 38-52). [PubMed | Google Scholar]
- Fraga C.G. Relevance, essentiality and toxicity of trace elements in human health. Asp. Med. 2005; 26:235–244. doi: 10.1016/j.mam.2005.07.013. [PubMed] [Cross Ref] [Google Scholar]
- Rzętała M.A. Assessment of toxic metal contamination of bottom sediments in water bodies in urban areas. Soil Sediment Contam. Int. J. 2015; 24:49–63. doi:10.1080/15320383.2014.911721.[Cross Ref] [Google Scholar]
- Mafuyai GM, Eneji IS, Sha’ Ato R. Concentration of Heavy Metals in respiratory Dust in Jos Metropolitan Area, Nigeria. Open Journal of Air Pollution, 2014; 3: 10-19 http://dx.doi.org/10.4236/ajop.2014.31002). [PubMed | Google Scholar]
- Okunola OJ, Uzairu A, Uba S, et al. Distribution Pattern of Metals in Atmospheric Settling Dust along Roads in Kano Metropolis, Nigeria. Journal of Applied Chem., 2015, Article ID 739325, 12Pages). [PubMed | Google Scholar]
- Burke, Marshall, Lindsay Filgas & Rob Jordan (2020). Nature Sustainability downloaded from https://news.stanford.edu/2020/06/29/air-pollutions-connection-infant-mortality/ ON 31ST May,2022. [Pubmed | Google Scholar]
- Duruibe J.O., Ogwuegbu M.O.C., Egwurugwu J.N. Heavy metal pollution and human biotoxic effects. J. Phys. Sci. 2007; 2:112–118. doi: 10.5897/IJPS.9000289. [Cross Ref] [Google Scholar]
- Debnath B., Singh W.S., Manna K. Sources and toxicological effects of lead on human health. Indian J. Med. Spec. 2019; 10:66–71. doi: 10.4103/INJMS.INJMS_30_18. [Cross Ref] [Google Scholar]
- Kumar A., Kumar A., M.M.S. C.-P., Chaturvedi A.K., Shabnam A.A., Subrahmanyam G., Mondal R., Gupta D.K., Malyan S.K., Kumar S.S., et al. Lead Toxicity: Health Hazards, Influence on Food Chain, and Sustainable Remediation Approaches. J. Environ. Res. Public Health. 2020; 17:2179. doi: 10.3390/ijerph17072179. [PMC free article][PubMed] [Cross Ref] [Google Scholar]
- Dokmeci A.H., Ongen A., Dagdeviren S. Environmental toxicity of cadmium and health effect. Environ. Prot. Ecol. 2009; 10:84–93. [Google Scholar]
- Klaassen C.D., Liu J., Diwan B.A. Metallothionein protection of cadmium toxicity. Appl. Pharmacol. 2009; 238:215–220. doi: 10.1016/j.taap.2009.03.026. [PMC free article][PubMed] [Cross Ref] [Google Scholar]
- Naseri K., Tahergorabi Z., Khazdair M.R., Sadeghi M. Toxic Mechanisms of Five Heavy Metals: Mercury, Lead, Chromium, Cadmium, and Arsenic. Pharmacol. 2021; 12:643972. doi: 10.3389/fphar.2021.643972. [PMC free article][PubMed] [Cross Ref] [Google Scholar]
- Moynier F., Vance D., Fujii T., Savage P. The Isotope Geochemistry of Zinc and Copper. Mineral. Geochem. 2017; 82:543–600. doi: 10.2138/rmg.2017.82.13. [Cross Ref] [Google Scholar]
- Clark G., Jacks D. Coal and the industrial revolution, 1700–1869. Rev. Econ. Hist. 2007; 11:39–72. doi: 10.1017/S1361491606001870. [Cross Ref] [Google Scholar]
- Solarski M., Machowski R., Rzetala M., Rzetala M.A. Hypsometric changes in urban areas resulting from multiple years of mining activity. Rep. 2022; 12:2982. doi: 10.1038/s41598-022-06847-8. [PMC free article][PubMed] [Cross Ref] [Google Scholar]
- Foster WM, Langenback E, Bergofsky EH. Measurement of tracheal and bronchial mucus velocities in man: relation to lung clearance. J Appl Physiol., 1980; 48: 965-971). [PubMed | Google Scholar]
- Stöber WKW. A simple pulmonary retention model accounting for dissolution and macrophage-mediated removal of deposited polydisperse particles, Inhal. Toxicol., 2001; 13: 129-148). [Pubmed | Google Scholar]
- Sharareh Dehghani. Farid Moore. Luba Vasiluk. Beverley A. Hale the influence of physicochemical parameters on bio accessibility-adjusted hazard quotients for copper, lead and zinc in different grain size fractions of urban street dusts and soils. Environ Geochem Health DOI 10.1007/s10653-017-9994-6). [PubMed | Google Scholar]
- Forbes B, O’ Lone R, Allen PP, Cahn A, Clarke C, Collinge M, et al. Challenges for inhaled drug discovery and development: Induced alveolar macrophage responses. Adv. Drug Deliv. Rev. Elsevier B.V. 2014; 71:15-33). [PubMed | Google Scholar]
- Guha Mazumder DN. Chronic arsenic toxicity: clinical features, epidemiology, and treatment: experience in West Bengal, J. Environ. Sci. Health, Part A. 2003; 38 (1): 141e163.). [PubMed | Google Scholar]
- Guha Mazumder DN. Chronic arsenic toxicity & human health, Indian J. Med. Res. 2008; 128: 436e447[Web of Science, PubMed and Google Scholar]
- Chung JY, Yu SD, Hong YS, Environmental Source of Arsenic Exposure, Journal of Preventive Medicine & Public Health (2014); 253-256). [PubMed | Google Scholar]
- Emmanuel Gbenga Olumayede, B. Babalola and I. Oghenovo (2021). Trace Elements in Urban Particulate Matters: Variations in Serum Levels, Inhalation Bio accessibility, Health and Disease Effects. Trace Elements and Their Effects on Human Health and Diseases. [Pubmed | Google Scholar]
- Christopher E. Environmental Science Processes & Impacts, 2013; 15(10): 1785-1970). [PubMed | Google Scholar]
- Nieboer E, Gibson BL, Oxman AD, et al. Health effects of aluminum: A critical review with emphasis on aluminum in drinking water. Environ Rev. 1995; 3(1): 29-81). [PubMed | Google Scholar]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans, Cadmium and cadmium compounds, IARC Monogr. Eval. Carcinog. Risks Hum. 1993; 58:119-237). [PubMed | Google Scholar]
- Jomova K, Valko M. Advances in metal-induced oxidative stress and human disease. Toxicology 2011; 283(2-3): 65-87). [PubMed | Google Scholar]
- Kruszewski M. The role of labile iron pool in cardiovascular diseases. Acta Biochim Pol. 2004; 51(2): 471-480.). [PubMed | Google Scholar]
- CONTAM, Scientific opinion of the panel on contaminants in food chain on a request from European commission on Cadmium in food, The EFSA Journal, 2009; 980: 1-139). [PubMed | Google Scholar]
- Markowitz M. “Lead poisoning”. Pediatrics in Review, 2000; 21(10):327-332). [PubMed | Google Scholar]
- CDC (Centers for Disease Control and Prevention). Preventing lead poisoning in young children: A statement by the for Disease Control, October 1991, US Department of Health and Human Services, Atlanta, Ga, USA,1991). [PubMed | Google Scholar]
- Soliman MM, Baiomy AA, Yassin MH. Molecular and histopathological study on the ameliorative effects of curcumin against lead acetate-induced hepatotoxicity and nephrototoxicity in Wistar rats, Biol. Trace Elem. Res. 2015; 167:91-102, http://dx.doi.org/10.1007/s12011-015-0280-0). [PubMed | Google Scholar]
- Styner L, Smith R, Thun M, Schnorr T, Lemen RA. Dose-response and qualitative assessment of lung cancer risk and occupational cadmium exposure. Ann Epidemiol. 1992; 2: 177-194). [PubMed | Google Scholar]
- Shotyk W, Le Roux G. Biogeochemistry and cycling of lead. Met. Ions Biol. Syst. 2005; 43:239-275 (Accessed 25 April 2022 http://www.ncbi.nlm.nih.gov/pubmed/16370121). [PubMed | Google Scholar] [PubMed | Google Scholar]
- USEPA, 1994. Methods for Derivation of Lung Reference Concentrations and Application of Lung Dosimetery. Environmental Criteria and Assessment, Office of Health and Environmental and assessment, Office of Research and Development, USEPA Research Triangle Park, North Caroline EPA/600/8-90/066F). [PubMed | Google Scholar]
- Oberdorster G, Oberdorster E, Oberdorster J. Nanotoxicology: an emerging discipline evolving from studies of ultrafine particles. Environ Health Perspect, 2005; 113(7): 823-839). [PubMed | Google Scholar]
- WHO (World Health Organization), Environmntal Health Criteria 18: Arsenic, World Health Organization, Geneva, Switzerland, 1981; 43-102). [Pubmed | Google Scholar]
- International Agency for Research on Cancer (IARC) Monographs on the evaluation of carcinogenic risks to humans: (1993) vols. 1-58 IARC, Lyon, pp1971-1993). [PubMed | Google Scholar]
- Detail review paper on cell transformation assays for detection of chemical carcinogens. DRP No. 31. Fourth draft version). [Pubmed | Google Scholar]
- Brook RD, Fraklin B, Cascio W, Hong Y, Howard G, Lipsett M, et al. Air pollution and cardiovascular disease a statement for healthcare professionals from expert panel on population and prevention science of the America Heart Association. Circulation 2004; 109: 2655-2671). [PubMed | Google Scholar]
- Andujar, P., et al., Respiratory effects of manufactured nanoparticles. Rev Mal Respir, 2011; 28(8): p. e66–e75). [PubMed | Google Scholar]
- Mossman, B.T., et al., Pulmonary endpoints (lung carcinomas and asbestosis) following inhalation exposure to asbestos. J Toxicol Environ Health B Crit Rev, 2011; 14(1-4): 76-121). [PubMed | Google Scholar]
- Braakhuis HM, et al., Physicochemical characteristics of nanomaterials that affect pulmonary inflammation. Part. Fibre Toxicol, 2014; 11: 18). [PubMed | Google Scholar]
- Jud C, et al., Nanomaterials and the human lung: what is known and what must be deciphered to realise their potential advantages? Swiss Med. Weekly, 2013; 143: 13758). [PubMed | Google Scholar]
- Jones RM, Neef N. Interpretation and prediction of inhaled drug particle accumulation in the lung and its associated toxicity. Xenobiotica. 2012; 42:86-93). [PubMed | Google Scholar]
- Geiser M, Kreyling WG. Deposition and biokinetics of inhaled nanoparticles. Part Fibre Toxicol., 2010; 7: 2). [PubMed | Google Scholar]
- Heyder J, Svarten, MU. Basic principles of particle behavior in the human respiratory tract, In: Bisgaard H, O’Callaghan C, Smaldone GC, Eds. Drug Delivery to the Lungs. Lung Biology in Health and Disease, Marcel Dekker; New York: 2002. p. 21-45). [PubMed | Google Scholar]
- Kagi JHR, Kogima Y., eds. Chemistry and Biochemistry of metallothionein. Boston: Birkhäuser, 1987; 25-61). [PubMed | Google Scholar]
- Slater TF. Free-radical mechanisms in tissue injury, Biochem Journal 1984; 222: 1-15,). [PubMed | Google Scholar]
- Joesten MD, Johnson DO, Netterville JT, Wood JL. World of Chemistry, Brooks/cole. Pacific Grove, CA, USA, 1ST Edition, 1990). [PubMed | Google Scholar]
- Vako M, Morris H, Cronin MT. Metals, toxicity and oxidative stress, Current Medicinal Chemistry, 2005; 12 (10): 1161-1208). [PubMed | Google Scholar]
- Kagi JHR, Kogima Y. Chemistry and biochemistry of metallothionein. Boston: Birkhäuser, eds. 1987. pp. 25-61). [PubMed | Google Scholar]
- Halliwell B, Gutterridge, JMC. Free radical and antioxidant protection: Mechanism and significant in toxicity and diseases. Human Toxicity, 1988; 7: 7-13.). [PubMed | Google Scholar]
- Aust SD, Morehouse LA, Thomas CE. The role of metals in oxygen radical reactions, J. Free Rad. Biol. Med. 1985; 1: 3-25). [PubMed | Google Scholar]
- Eichhorn GL, Butzow JJ, Shin YA. Some effects of metal ions on DNA structure and genetic information transfer. Proc. Int. Symp. Biomol., Struct., Interactions, Suppl. J. Biosci. 1985; 8 (3&4): 527-535.). [PubMed | Google Scholar]
- Morris DL. DNA-bound metal ions: recent developments. BioMol Concepts 2014; 5(5): 397-407). [PubMed | Google Scholar]
- Eichhorn, GL. In advances in Inorganic Biochemistry (eds Eichhorn, GL and Marzilli) (New York, Elsevier) Vol. 3. P2). [PubMed | Google Scholar]
- Ruby MV, Schoof R, Brattin W, Goldade M, Post G, Harnois M, Mosby DE, Casteel SW, Berti W, Carpenter M, et al. Advances in evaluating the oral bioavailability of inorganics in soil for use in human health risk assessment. Environ. Sci. Technol., 1999; 33: 3697-3705.). [Pubed. |Cross Ref Full Text | Google Scholar]
- Ng JC, Juhasz A, Smith E, Naidu R. Assessing the bioavailability and bio accessibility of metals and metalloids, Environ. Sci. Pollut. Res. 2015; 22: 8802-8825). [Pubmed. |Cross Ref Full Text | Google Scholar]
- Huang X, Betha R, Tan LY, Balasubramanian R. Risk assessment of bio accessible trace elements in smoke haze aerosols versus urban aerosols using simulated lung fluids. Atmos. Environ. 2016; 125: 505-5111.). [PubMed | Google Scholar]
- Cui X, Xiang P, He R, Juhasz A, Ma L. Advances in in vitro methods to evaluate oral bio accessibility of PAHs and PBDEs in environmental matrices. Chemosphere 2016; 150, 378-3891.). [PubMed. |CrossRef Full Text | Google Scholar]
- Guo CH, Liu P, Hsia S, Chuang C, Chen P. Role of certain trace minerals in oxidative stress, imflammation, CD4/CD8 lymphocyte ratios and lung function in asthmatic patients. Ann. Clin. Biochem. 2011; 48: 344-351). [PubMed. |Cross Ref Full Text | Google Scholar]
- Ermis B, Armutcu F, Gurel A, Kar L, Demircan N, Altin R, Daemirel E. Trace elements status in children with bronchial asthma. Eur. J Gen Med. 2004; 1(1): 4-8.). [PubMed | Google Scholar]
- Niu J, Liberda EN, Qu S, Guo X, Li X, Zhang J, et al. The role of metal components in the cardiovascular effects of PM5, PLoS One, 2013; 8(12): e83782.). [PubMed | Google Scholar]
- Ewona, I. O. Osang, J. E. Obi, E. O. (2013). Air Quality and Environmental Health in Calabar, Cross River State, Nigeria. International Journal of Engineering and Science Invention (IJESI) Vol.6(6) 55-65. [ Cross Ref] [Google Scholar]
- Sunday O. Udo and Igwe O. Ewona (2016). Preliminary Findings on Air Quality Characterisation in the Niger Delta Area of Nigeria. Proc. of the Fourth International Conference on Advances in Civil, Structural and Environmental Engineering – ACSEE 2016. ISBN: 978-1-63248-114-6 doi: 10.15224/ 978-1-63248-114-6-13. [ Cross Ref] [Google Scholar]
- Sunday O. Udo, Mfon D. Umoh, Igwe O. Ewona, and Chinelo T. Okpalaonwuka (2020). An Assessment of Particulate Matter Pollution in Calabar, Nigeria ASJ: International Journal of Health, Safety and Environment (IJHSE) Vol. 6 (07) 618 – 626 www.academiascholarlyjournal.org/ijhse/index_ijhse.htm ISSN: 2360-9311©Academia Scholarly Journals Indexed In: Directory of Research Journals Indexing – http://www.drji.org Also Available@: Archive.org/Udo et al. Open access. [ Cross Ref] [Google Scholar].