
The Role of Courtyard to Improve the Physical Environment of Inpatient Wards: A Case Study of Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh
- Md. Monjur Kader Sarker
- Jasmin Ara Begum
- Mallik Akram Hossain
- 503-513
- May 11, 2024
- Architecture
The Role of Courtyard to Improve the Physical Environment of Inpatient Wards: A Case Study of Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh
Md. Monjur Kader Sarker1*, Jasmin Ara Begum2, Mallik Akram Hossain3
1Department of Architecture, Ahsanullah University of Science and Technology, Bangladesh.
2Faculty of Architecture and Planning, Ahsanullah University of Science and Technology, Bangladesh.
3Faculty of Life and Earth Science, Jagannath University, Bangladesh.
*Corresponding Author
DOI: https://doi.org/10.51244/IJRSI.2024.1104036
Received: 28 March 2024; Accepted: 09 April 2024; Published: 11 May 2024
ABSTRACT
This research investigates the role of a courtyard to improve the physical environment of inpatient wards at Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh. The objective is to investigate the luminous, thermal and acoustic conditions and identify if courtyard has improved the ward’s physical environment. Both qualitative and quantitative survey have been conducted to measure the light, temperature, humidity, ventilation and sound among experimental group (wards beside courtyard) and control group (wards away from courtyard); and interviews from patients to get their experiences. The findings demonstrate that the presence of the courtyard positively influences wards’ physical environment. Patients also express higher levels of satisfaction with the courtyard. The wards beside courtyards have a higher level of light, ventilation rate and lower level of sound rate and the wards away from courtyard have a lower level of light, ventilation rate and higher level of sound rate. The outcome underscores the importance of incorporating nature into healthcare facilities and provide valuable insights for healthcare authorities to create patient-centered and sustainable healing environments in hospitals in context of Bangladesh.
Keywords— Courtyard, Hospital, Inpatient Wards, Physical Environment, Light, Temperature, Humidity, Ventilation, Sound, Shaheed Suhrawardy Medical College Hospital, Dhaka.
INTRODUCTION
Background of the Study
In recent years, the integration of nature and green spaces within healthcare settings has gained significant attention. These green spaces, such as gardens, courtyards, and indoor plants, have shown to have a positive impact on patients’ psychological and physiological states, leading to improved health outcomes and satisfaction levels (Makram & Razek, 2019). Research has demonstrated that exposure to natural environments and greenery can have a calming effect, reducing stress, anxiety, and depressive symptoms among patients (Yao et al., 2021). The presence of vegetation and access to outdoor green areas have been linked to improved lighting levels, air quality, reduced noise levels, and enhanced social interactions, all of which contribute to a more conducive healing environment (Van den Berg, 2005; Collado et al., 2016).
Problem Statement and Rationale of the Study
In Bangladesh, particularly in urban areas like Dhaka, healthcare facilities face numerous challenges in providing optimal care for patients due to limited resources, high patient load and congested environments. It is also difficult for a govt. hospital to provide a better environment for patients as there is high demand. The hospital inside area is often a trapped zone and it lacks of light, ventilation and better environment. The Shaheed Suhrawardy Medical College Hospital (ShSMCH) in Dhaka serves as a prominent healthcare institution and faces similar challenges. The problem statement of the research is, the inpatient wards of ShSMCH often face poor thermal, luminous and acoustic conditions and in spite of having a courtyard inside the hospital, the utilization of the courtyard to improve the physical environment of the inpatient wards is rarely found. By examining the role of the courtyard to improve the luminous, thermal and acoustic environment, this study aims to provide evidence-based insights for enhancing the healing environment in hospital ward settings.
Research Questions
a) What is the impact of courtyard on the inpatient physical ward environment?
b) What is the relationship of courtyard with the luminous, thermal, and acoustic conditions of in-patient ward environment?
c) How does it improve the luminous, thermal, and acoustic environment of inpatient wards?
d) What are the perceptions of patients on the existence of a courtyard to improve the physical ward environment?
Research Objectives
The general objective of this research is to investigate the role of a courtyard to improve the luminous, thermal, and acoustic conditions of hospital ward environment.
The specific objectives are:
a) To review the luminous, thermal and acoustic conditions (i.e. light, ventilation, temperature, humidity, sound etc.) of in-patient wards from experimental group and control group of the selected hospital; and
b) To evaluate the patients’ perception on ward environment from experimental group and control group of that hospital.
MATERIALS AND METHOD
Both qualitative and quantitative research design are employed to investigate the impact of a courtyard on inpatient ward environments at ShSMCH, Dhaka, Bangladesh. The case study approach focuses on this specific hospital due to its prominent healthcare status, featuring an existing green courtyard. Combining survey, physical observation, and interviews, primary data are collected on luminous, thermal, and acoustic aspects. Secondary data are sourced from academic databases. Using purposive or simple random sampling, 5 wards and 50 patients near the courtyard (experimental group) and 5 wards and 50 patients away from the courtyard (control group); thus, a total of 10 wards and 100 patients are surveyed, aiming to understand the physical environment and patients’ perceptions. Instruments include Lux Meter to measure light intensity, Anemometer to measure air velocity, Thermo Hygrometer to measure temperature and relative humidity, Sound Level Meter to measure sound intensity, and structured questionnaires for patients’ perceptions. Environmental measurements and questionnaire data analysis are conducted to compare parameters in wards with and without courtyards, providing a comprehensive understanding.
Table 1. Instruments Used for Measurements (Author, 2023)
| Lux Meter | Thermo Hygrometer | Anemometer | Sound Level Meter |
| Model no.: LX1330B | Model no.: DT – 618 | Model no.: KT – 905 | Model no.: DT – 8850 |
 |
 |
 |
RESULT
Hospital Overview
Shaheed Suhrawardy Medical College (ShSMC), established in 2006, is the 14th government medical college in Bangladesh and holds the third position in the government medical college ranking. Located in Dhaka, near the National Parliament House, it is recognized globally and situated within the medical zone, surrounded by various medical institutes. The hospital, initially Ayub Central Hospital, was developed into a medical college in 2006, operating with 850 beds and 36 departments. Designed by architect Louis I Kahn in 1963, the campus features a thoughtfully crafted central courtyard with lush greenery, water features, and landscaping, providing a calming environment for patients, visitors, and medical staffs (ShSMCH, 2023). There are wards situated both beside the courtyard buffering by corridors and wards away from the central courtyard.
Table 2. Hospital Images (Author, 2023)
| Legend | Images |
| ShSMC Hospital Courtyard and Corridor |  |
| Wards beside Courtyard (Experimental Group) |  |
| Wards away from Courtyard (Control Group) | 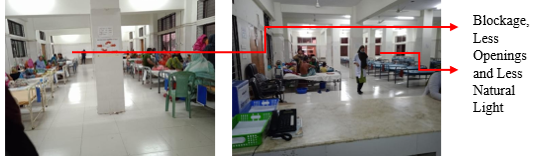 |
Environmental Data Analysis
1) Measurement of Luminous Environment:
Table 2. Measurement of Light (Author, 2023)
| Serial No. | Floor No. | Experimental Group | Control Group | ||||||
| Ward no. | Avg. Light Intensity | Optimum Light Intensity | Percentage Needed for Optimum Light Intensity | Ward no. | Avg. Light Intensity | Optimum Light Intensity | Percentage Needed for Optimum Light Intensity | ||
| 1 | 3rd | 420 A | 290 lux | 500 lux | 42% | 420 B | 72.5 lux | 500 lux | 85.50% |
| 2 | 4th | 526 | 335 lux | 500 lux | 33% | 525 | 65 lux | 500 lux | 87% |
| 3 | 4th | 527 A | 470 lux | 500 lux | 6% | 527 B | 95 lux | 500 lux | 81% |
| 4 | 5th | 633 | 390 lux | 500 lux | 22% | 632 | 82.5 lux | 500 lux | 83.50% |
| 5 | 5th | 635 | 530 lux | 500 lux | -6% | 634 | 125 lux | 500 lux | 75% |
From table 2, in experimental group 3rd and 4th-floor wards, light intensity require a 42% and 33% increase, respectively, to reach the recommended 500 lux. 4th-floor ward no. 527A has sufficient light, needing only a 6% increase. 5th-floor ward no. 633 needs a 22% boost, while ward no. 635 surpasses the recommended level by 6%. Notably, wards no. 527A and 635 are the most suitable, with light intensity increasing with floor height.
In control group wards, light intensity is insufficient. 3rd-floor ward no. 420B needs 85.5% more light, 4th-floor ward no. 525 requires an 87% increase, and 4th-floor ward no. 527B needs 81% more light. 5th-floor ward no. 632 needs 83.5%, and ward no. 634 requires a 75% boost to meet the recommended 500 lux. Among control group wards, ward no. 634 shows relatively better luminous conditions, and light intensity increases with floor height.
A comparison of light intensity in lux for experimental group and control group is shown in chart 1.
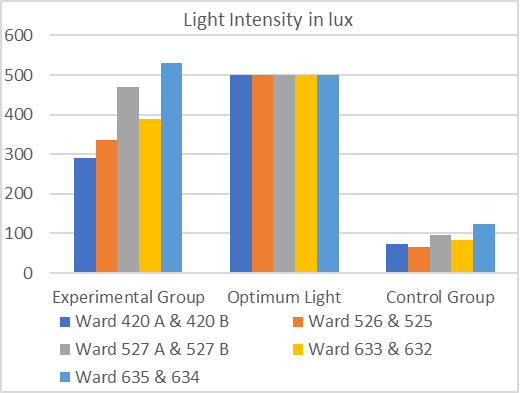
Chart 1. Comparison of Light Intensity for Experimental Group and Control Group (Author, 2023)
From the comparison, it is noticed that the experimental group has much more higher light intensity than the control group.
2) Measurement of Thermal Environment:
Table 3. Measurement of Temperature and Humidity (Author, 2023)
| Serial No. | Floor No. | Experimental Group | Control Group | ||||||||
| Ward no. | Indoor Temp. | Optimum Indoor Temp. | Relative Humidity (RH) | Optimum RH | Ward No. | Indoor Temp. | Optimum Indoor Temp. | Relative Humidity (RH) | Optimum RH | ||
| 01 | 3rd | 420 A | 25.9 oC | 24 oC | 38 % | 40% – 60% | 420 B | 26.9 oC | 24 oC | 30 % | 40% – 60% |
| 02 | 4th | 526 | 26.2 oC | 24 oC | 38 % | 40% – 60% | 525 | 26.2 oC | 24 oC | 35 % | 40% – 60% |
| 03 | 4th | 527 A | 26.3 oC | 24 oC | 35 % | 40% – 60% | 527 B | 26.5 oC | 24 oC | 33 % | 40% – 60% |
| 04 | 5th | 633 | 26.3 oC | 24 oC | 34 % | 40% – 60% | 632 | 26.5 oC | 24 oC | 33 % | 40% – 60% |
| 05 | 5th | 635 | 26.5 oC | 24 oC | 29 % | 40% – 60% | 634 | 26.6 oC | 24 oC | 30 % | 40% – 60% |
Wards at SShMCH fall short of optimal indoor conditions in November month. From table 3, in experimental group, the 3rd-floor ward no. 420A has 25.9°C, 38% humidity; 4th-floor ward no. 526 has 26.2°C, 38% humidity; 4th-floor ward no. 527A has 26.3°C, 35% humidity; 5th-floor ward no. 633 has 26.3°C, 34% humidity, and ward no. 635 has 26.5°C, 29% humidity. The recommended ASHRAE standards for hospital wards are 24°C and 40%-60% humidity (Health Care Facilities, 2019). The dry season in November contributes to the observed low humidity.
Similarly, in control group, 3rd-floor ward no. 420B has 26.9°C, 30% humidity; 4th-floor ward no. 525 has 26.2°C, 35% humidity; 4th-floor ward no. 527B has 26.5°C, 33% humidity; 5th-floor ward no. 632 has 26.5°C, 33% humidity, and ward no. 634 has 26.6°C, 30% humidity. These conditions do not align with ASHRAE recommendations for hospital wards, and the dry November season exacerbates low humidity levels.
A comparison of temperature in degree celsius for experimental group and control group is shown in chart 2 and RH in percentage in chart 3.
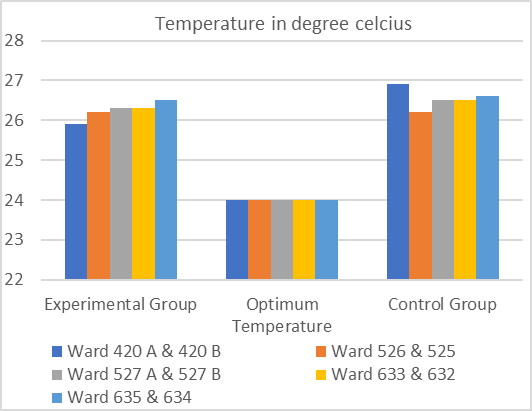
Chart 2. Comparison of Temperature for Experimental Group and Control Group (Author, 2023)
The temperature is around 26 oC for both conditions. However, the experimental group has nearer values to optimum temperature than the control group.
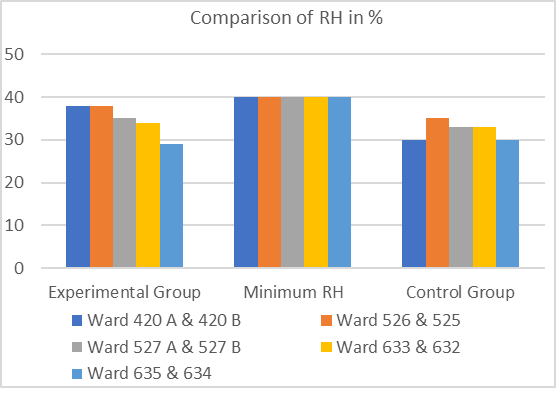
Chart 3. Comparison of RH for Experimental Group and Control Group (Author, 2023)
The survey is conducted in dry season and the RH is below optimum minimum level for both condition. However, the experimental group has nearer values to optimum minimum RH than the control group.
Table 4. Measurement of Air Velocity (Author, 2023)
| Serial No. | Floor No. | Experimental Group | Control Group | ||||||
| Ward no. | Min. Air Velocity | Max. Air Velocity | Avg. Air Velocity | Ward No. | Min. Air Velocity | Max. Air Velocity | Avg. Air Velocity | ||
| 01 | 3rd | 420 A | 0.4 m/s | 1.4 m/s | 0.9 m/s | 420 B | 0.3 m/s | 0.9 m/s | 0.6 m/s |
| 02 | 4th | 526 | 0.6 m/s | 2.8 m/s | 1.7 m/s | 525 | 0.1 m/s | 0.4 m/s | 0.25 m/s |
| 03 | 4th | 527 A | 0.6 m/s | 1.6 m/s | 1.1 m/s | 527 B | 0.3 m/s | 1.0 m/s | 0.65 m/s |
| 04 | 5th | 633 | 0.7 m/s | 2.8 m/s | 1.75 m/s | 632 | 0.1 m/s | 0.5 m/s | 0.3 m/s |
| 05 | 5th | 635 | 0.7 m/s | 1.8 m/s | 1.25 m/s | 634 | 0.4 m/s | 1.0 m/s | 0.7 m/s |
From table 4, in experimental group, the 3rd floor, ward no. 420A has a range of 0.4-1.4 m/s and an average of 0.9 m/s. The 5th floor ward no. 633 records the highest air velocity with a range of 0.7-2.8 m/s and an average of 1.75 m/s, showing an increase with floor height.
On the other hand, in control group, ward no. 420B on the 3rd floor, the air velocity ranges from 0.3 to 0.9 m/s, averaging 0.6 m/s. The 4th floor ward no. 525 has the lowest air velocity with a range of 0.1-0.4 m/s and an average of 0.25 m/s. Meanwhile, the 5th floor ward no. 634 exhibits the highest air velocity, ranging from 0.4 to 1.0 m/s and averaging 0.7 m/s. Overall, air velocity increases with floor height.
Table 5. Measurement of Air Changes Rate (Author, 2023)
| Experimental Group | Control Group | ||||||||||||||
| Serial No. | Floor No. | Ward No. | Air Velocity (v) | Cross- Sectional Area of Inlet (A) | Volumetric Flow Rate (Q = Av) | Room Volume (V) | Air Changes Per Hour (ACH= 3600Q/V) | Min. ACH | Ward No. | Air Velocity (v) | Cross- Sectional Area of Inlet (A) | Volumetric Flow Rate (Q = Av) | Room Volume (V) | Air Changes Per Hour (ACH= 3600Q/V) | Min. ACH |
| 1 | 3rd | 420 A | 0.9 m/s | 6.3 m2 | 5.67 m3/s | 3567.5m3 | 5.72 | 4 | 420 B | 0.6 m/s | 6.3 m2 | 3.78 m3/s | 2782.63m3 | 4.89 | 4 |
| 2 | 4th | 526 | 1.7 m/s | 4.08 m2 | 6.93 m3/s | 4994.45m3 | 4.99 | 4 | 525 | 0.25 m/s | 14.49 m2 | 3.62 m3/s | 4682.31m3 | 2.78 | 4 |
| 3 | 4th | 527 A | 1.1 m/s | 6.3 m2 | 6.93 m3/s | 3567.5m3 | 6.99 | 4 | 527 B | 0.65 m/s | 6.3 m2 | 4.09 m3/s | 2782.63m3 | 5.29 | 4 |
| 4 | 5th | 633 | 1.75 m/s | 4.08 m2 | 7.14 m3/s | 4994.45m3 | 5.14 | 4 | 632 | 0.3 m/s | 14.49 m2 | 4.34 m3/s | 4682.31m3 | 3.34 | 4 |
| 5 | 5th | 635 | 1.25 m/s | 6.3 m2 | 7.87 m3/s | 3567.5m3 | 7.94 | 4 | 634 | 0.7 m/s | 6.3 m2 | 4.41 m3/s | 2782.63m3 | 5.7 | 4 |
From table 5, in the experimental group, all surveyed wards exceed the minimum Air Changes per Hour (ACH) requirement of 4 for hospital wards, as per ASHRAE (2020) standards. Ward no. 635 exhibits the highest ventilation rate, indicating an improvement with floor height.
Contrastingly, in the control group, some wards fall below the recommended minimum ACH, with ward no. 525 having the lowest ventilation rate. The ventilation rate tends to increase with floor height in the control group.
A comparison of ACH for experimental group and control group is shown in chart 4.
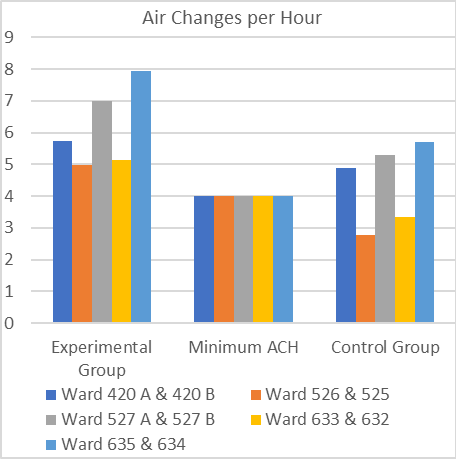
Chart 4. Comparison of ACH for Experimental Group and Control Group (Author, 2023)
From the comparison, it is noticed that the experimental group has much higher ventilation rate than the control group.
3) Measurement of Acoustic Environment:
Table 6. Measurement of Sound (Author, 2023)
| Serial No. | Floor No. | Experimental Group | Control Group | ||||||
| Ward No. | Max. Sound Intensity | Boundary Level | Percentage Exceeded | Ward No. | Max. Sound Intensity | Boundary Level | Percentage Exceeded | ||
| 01 | 3rd | 420 A | 47 dB | 40 dB | 17.5 % | 420 B | 60 dB | 40 dB | 50 % |
| 02 | 4th | 526 | 56 dB | 40 dB | 40 % | 525 | 72 dB | 40 dB | 80 % |
| 03 | 4th | 527 A | 50 dB | 40 dB | 25 % | 527 B | 58 dB | 40 dB | 45 % |
| 04 | 5th | 633 | 59.4 dB | 40 dB | 48.5 % | 632 | 70.9 dB | 40 dB | 77.25 % |
| 05 | 5th | 635 | 50.8 dB | 40 dB | 27 % | 634 | 55 dB | 40 dB | 37.5 % |
From table 6, in experimental group all wards exceed the WHO-recommended maximum daytime sound level of 40 dB for hospital wards. Ward no. 420A on the 3rd floor performs relatively better, exceeding the limit by 17.5%, while ward no. 633 on the 5th floor surpasses it by 48.5%. In comparison, ward no. 635 exceeds the limit by 27%.
All control group wards also significantly surpass the WHO recommended maximum sound level. Ward no. 525 on the 4th floor stands out as the worst performer, exceeding the limit by 80%. Notably, ward no. 634 on the 5th floor performs relatively better, exceeding the limit by 37.5%.
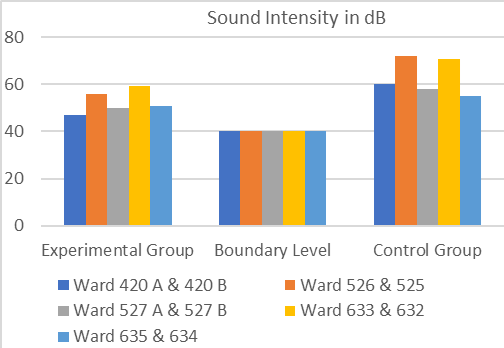
Chart 5. Comparison of Sound Intensity in dB for Experimental Group and Control Group (Author, 2023)
From the comparison, it is noticed that the control group has much higher noise level than the experimental group.
Questionnaire survey
Patients are asked questions based on the luminous, thermal and acoustic conditions of their ward settings. In the experimental group, the majority of patients reported ample light in their rooms, while in the control group, most indicated insufficient light. Regarding thermal conditions, patients in the experimental group generally expressed satisfaction with air circulation and thermal comfort, whereas those in the control group tended to report poor conditions. As for noise levels, patients in the experimental group commonly agreed that the environment was not noisy, while those in the control group often perceived it as noisy. The questionnaire result is shown below:
a) How would you describe the natural light in your room?
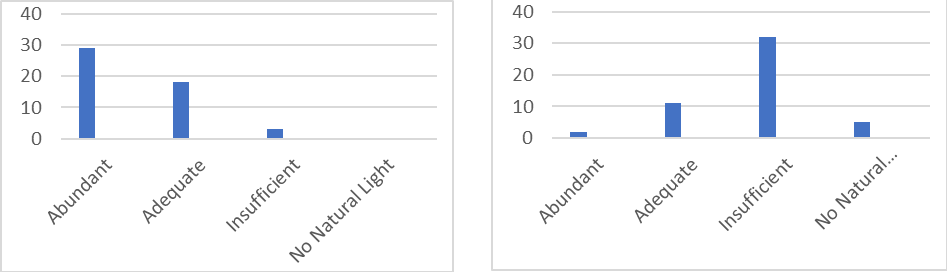
Chart 6. Natural Light in Experimental Group (Left) and Control Group (Right) (Author, 2023)
b) How would you describe the air circulation and thermal comfort in your room?
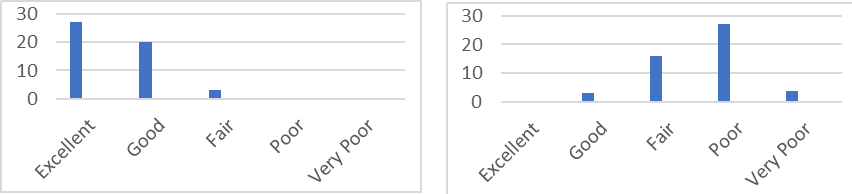
Chart 7. Air Circulation and Thermal Comfort in Experimental Group (Left) and Control Group (Right) (Author, 2023)
c) Is the place noisy?
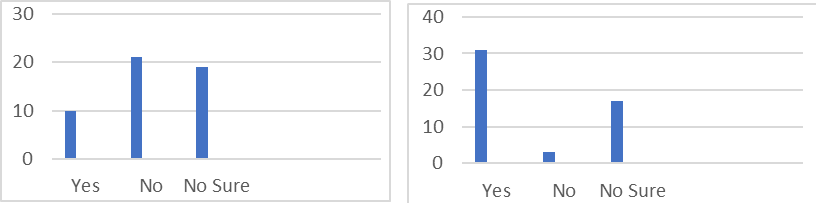
Chart 8. Noise in Experimental Group (Left) and Control Group (Right) (Author, 2023)
From the questionnaire survey, it is also noticed that the patients from the experimental group has experienced a higher level of light, ventilation, thermal comfort and lower noise level than the patients of control group. The patients from the experimental group has more positive answers regarding the luminous, thermal and acoustic conditions of their physical environment than the control group.
Physical observation
From the physical observation it is noticed that, wards adjacent to the courtyard experienced enhanced luminous conditions with ample natural light, improved thermal comfort due to better air circulation, and reduced noise levels, providing a conducive atmosphere for patient healing and well-being. In contrast, wards distant from the courtyard faced challenges with insufficient natural light, poor air circulation, and higher noise levels, resulting in discomfort for patients. These findings underscore the importance of integrating green spaces like courtyards into healthcare facilities to create patient-centered healing environments.
DISCUSSIONS
The results of this study demonstrate that the experimental group, which is beside the courtyard, exhibited significantly better physical environment compared to the control group without such provision. The wards beside the courtyard had better luminous, thermal and acoustic conditions compared to those away from the courtyard. Patients in the experimental group reported a higher light, ventilation and thermal comfort, and lower noise level during their hospital stay. The green courtyard provided a calming and soothing environment, fostering a connection with nature that positively influenced the patients’ overall well-being. In contrast, the control group, lacking exposure to the green space, experienced comparatively lower light, ventilation rate and thermal comfort, and higher noise. These findings highlight the therapeutic benefits of integrating green spaces within healthcare settings, promoting patient-centered care and supporting the notion that nature-based interventions can effectively contribute to improving patient outcomes in hospital environments.
The study have some limitations too that are needed to be addressed. It is a single case study, limiting the applicability of the findings to other healthcare settings. The sample size was relatively small, which may affect the statistical power and the ability to detect more subtle effects. Moreover, data represent the November month and can be changed in different seasons of the year. In case of air inlet measurements, the negligible inlets were not accounted. The self-report measures can be susceptible to response bias. Future research with larger and more diverse samples, multi-site studies and objective measures would help overcome these limitations and provide a more comprehensive understanding of the role of courtyards on the physical environment of hospital wards.
There are plenty of future possibilities for this research. This analysis can explore factors such as the role of natural light in promoting healing, the impact of greenery on air quality, the impact of sound on patient health and wellbeing, the psychological benefits of connecting with nature etc. A focus group interview with patients, healthcare providers and hospital staffs can gain insights into the design of patient-centered environment. Future studies can explore the specific needs and preferences of different patient groups (e.g., age, medical condition, length of stay etc.) regarding the courtyard environment. For example, older adults or patients with chronic conditions may have different perceptions and experiences compared to younger, healthier patients. By addressing these suggestions, future research can strengthen the evidence base on the role of courtyards in healthcare settings and contribute to the development of more effective interventions to improve patient outcomes and satisfaction.
CONCLUSION
The study provides compelling evidence of the positive impact of a courtyard on hospital wards at Shaheed Suhrawardy Medical College Hospital in Dhaka, Bangladesh. In a populated country like Bangladesh where it is difficult for the govt. hospitals to provide a better environment for the patients, there hospitals can be arranged with courtyards beside the inpatients wards, so that the inpatients can get sufficient natural light, suitable temperature, humidity and higher ventilation rate; and lower level of noise. The courtyard improves the physical environment of a ward that can significantly create a healing environment for the inpatients. In this study, patients also expressed higher levels of satisfaction with their overall hospital experience. The conclusion highlights the importance of patient-centered care and the potential benefits of integrating nature into healthcare settings.
ACKNOWLEDGEMENT
The authors greatly share thankfulness to Prof. Dr. M.A Muktadir, Prof. Dr. Rumana Rashid and Asst. Prof. Ar. Rana Das, Department of Architecture, Ahsanullah University of Science and Technology for their guidance and providing necessary instruments.
REFERENCES
- ASHRAE. (2020). Retrieved December 20, 2023, from. https://www.ashrae.org/file%20library/technical%20resources/standards%20and%20guidelines/ standards%20errata/standards/170_2017_a_20200901.pdf
- Collado, S., Staats, H., Corraliza, J. A., & Hartig, T. (2016). Restorative Environments and Health. Handbook of Environmental Psychology and Quality of Life Research, 127–148. https://doi.org/10.1007/978-3-319-31416-7_7
- Health Care Facilities. (2019). Retrieved December 20, 2023, from https://www.ashrae.org/file%20library/technical%20resources/covid-19/si_a19_ch09healthcarefacilities.pdf
- How to Light a Hospital. (2018, February 23). Lighting Equipment Sales. https://lightingequipmentsales.com/how-to-light-a-hospital.html
- Makram, A., & Razek, S. A. A. (2019). Design indicators based on nature and social interactions to enhance wellness for patients in healthcare facilities. International Journal of the Academic Research Community Publication, 1, 1-12.
- Schweitzer, M., Gilpin, L., & Frampton, S. B. (2004). Healing Spaces: elements of environmental design that make an impact on Journal of Alternative and Complementary Medicine, 10(supplement 1), S-83. https://doi.org/10.1089/acm.2004.10.s-71
- ShSMCH. (2023). ShSMCH. Retrieved December 20, 2023, from https://shsmch.gov.bd/about-us/
- Van den Berg, A. E. (2005). Health impacts of healing environments; a review of evidence for benefits of nature, daylight, fresh air, and quiet in healthcare settings. UMCG.
- Yao, W., Zhang, X., & Gong, Q. (2021). The effect of exposure to the natural environment on stress reduction: A meta-analysis. Urban Forestry & Urban Greening, 57, 126932. https://doi.org/10.1016/j.ufug.2020.126932