
Trend and Predictors of Non-Adherence among Tuberculosis Patients Treated on the Directly Observed Treatment in the Upper East Region of Ghana
- Elijah Atiyire
- N.K Oladejo
- Opoku Nicholas
- E. Mannu
- M. A Adjuik
- 155-168
- Mar 3, 2025
- Public Health
Trend and Predictors of Non-Adherence among Tuberculosis Patients Treated on the Directly Observed Treatment in the Upper East Region of Ghana
Elijah Atiyire1, N.K Oladejo*2, Opoku Nicholas3, E. Mannu4, M. A Adjuik5
1,3,4,5 School of Public Health, University of Health and Allied Sciences Ghana
2Department of Industrial Mathematics, C. K. Tedam University of Technology & Applied Sciences, Ghana
*Corresponding author
DOI: https://doi.org/10.51244/IJRSI.2025.121500014P
Received: 20 January 2025; Accepted: 30 January 2025; Published: 03 March 2025
ABSTRACT
This paper examines the trend and predictors of TB treatment default in patients treated with the DOTS strategy in Ghana’s Upper East Region. A matched case control study design was employed using record review and survey approaches in secondary data collection which includes sample size of 112 respondents, 56 cases of TB treatment non-adherent and 56 controls (TB treatment adherents. Multistage sampling technique was used in selecting the districts. The study collected primary and secondary data. Patients’ records were reviewed using data extraction sheets. The review gathered data on the trend of TB treatment default from 2016 to 2020. Primary data on factors predicting non-adherence to TB treatment were gathered from 2018 to 2020 using a structured questionnaire and analysed using STATA 16.0. The odds ratios were first calculated manually in excel and the values was confirmed using Mentel-Haenzel analyses at ˂0.05 level of significance and 95% confidence interval the results reveals the highest of 43.7% of TB defaulters among patients between ages 34-44 years in 2016 and 27.3% between the ages (44-45) as well as (27.3%) between the age (45-54) in 2017.While male defaulters increased from (2016 -2017) by 30.2% a Female defaulters increased from 10.7% to 25.0% in (2016 -2017) and maintained the prevalence of 25.0% in 2018. The highest prevalence (45.2%) of TB defaulters was from the Bolgatanga Municipality in 2017 and 35.7% in 2018. TB patients whose parents or family members were responsible for deciding where to seek healthcare were at increased risk of defaulting TB treatments [(ORMH=2.5, 95% CI: 1.04, 6.56), p=0.04].
Key words: Trend analysis, predator, Non-adherence, Tuberculosis, patients, direct observed treatment
INTRODUCTION
Tuberculosis (TB) is the leading cause of morbidity and mortality globally, particularly in Asia and Africa. In Ghana, the Ghana Health Service (GHS) has adopted the Directly Observed Therapy Short-Course (DOTS) to control and treat TB, however, there is still TB defaulters in the Upper East region. It a disease caused by bacteria (Mycobacterium tuberculosis) that most often affect the lungs, is the 13th leading cause of mortality worldwide as opined by [1] that the leading infectious disease killing more people globally. In 2021, about 1.6 million people died from TB with about 187,000 of these mortalities occurring among HIV/AIDS patients worldwide as studied by [2].
According to [2] over 10.6 million people fell ill with TB globally in the year 2021 and currently over six million men, 3.4 million women and 1.2 million children continue to fall sick from TB globally. TB is a global phenomenon. In 2021, the largest number of new TB cases occurred in the WHO South-East Asian Region, with 46% of new cases, followed by the WHO African Region, with 23% of new cases and the WHO Western Pacific with 18%. In 2020, 87% of new TB cases occurred in the 30 high TB burden countries. Eight countries accounted for more than two thirds of the global total: India, Indonesia, China, the Philippines, Pakistan, Nigeria, Bangladesh and the Democratic Republic of the Congo as disclosed by [2].
In Africa, Liberia, Nigeria, and Sierra Leone are the African countries experiencing the highest TB burdens (WHO, 2020). In 2020, the incidence of TB was 219, 298, and 314 per 100,000 people in Nigeria, Sierra Leone, and Liberia, respectively, while mortality rates for the same time were 62 percent, 51 percent, and 61.4 percent in Nigeria, Sierra Leone, and Liberia, respectively as revealed by [3].
In Ghana, according to [4]there were about 44, 000 TB cases in 2020 and the national survey in Ghana of 2019 reported estimated of the national prevalence of TB to be 290 per every 100,000 populations which is over three-times the acceptable prevalence of 92 per 100,000 by the WHO and the available data estimated the national prevalence of tuberculosis in the year 2020 through microscopy as 111 per 100,000 populations and bacteriologically confirmed TB was 356 per 100,000 populations as opined by [5]
In an effort to combat the TB epidemic in the country, stakeholders in Ghana in partnership with the WHO, introduced the Direct Observed Treatment Short-course (DOTS) in 1994 as a standard TB control method by Ghana Health Service with the aim of identify at least 70% of predicted TB infections and successfully treatment of 85% of them.
Since the introduction of the DOTS strategy, according to [6] TB case detection, and management rates have remarkably increased in Ghana However, despite the programme’s success, some challenges persist in managing and treating TB patients in the country. According to [7], financial constraints, shortage of TB drugs, healthcare inaccessibility and long distance to health facilities influenced TB treatment non-adherence and management in Ghana.
These challenges have been affirmed by [8] as treatment non-adherence has severe health consequences for patients. Failure to comply with treatment by TB patients increases the risk of TB-related death and the emergence of numerous drug-resistant strains of the TB bacteria as opined by [9]. Despite efforts to reach a 100 percent treatment compliance rate, the incidence of treatment defaulter cases among TB patients in the Upper East Region has increased in spite the introduction of the DOTS strategy in 2019. However, despite the challenge of treatment adherence among TB patients in the region, it seems less is known about TB treatment default trends and predictors among defaulters in the Upper East Region. This is because most studies on TB in the country largely focus on diagnostics with less attention on treatment as revealed by [10],[11],[12],[13] and [14]
According to [15],[16] and [17] Globally, there has been a rising trend of non-compliance to TB medication for instance, in China, an increasing trend of TB treatment non-adherence has been reported in pulmonary TB patients
According to [18] about 33.9% of patients with pulmonary TB missed taking their TB medications in China. Their findings disagree with related studies carried out in China by [19] which recorded a decreasing TB treatment defaulter rate among migrant pulmonary TB patients which recorded a 16% patient-defaulter rate.
In this paper, patients treated with the DOTS technique in Ghana’s Upper East region were examined to determine the trend and predictors of TB treatment default thereby bridging the information gap on TB treatment and management in the region and the nation at large
Study Design
The paper use case study control and employ two data collection approaches which involves, review of TB records (cross sectional) to determine the trend of TB treatment default from 2016-2020 and a matched case-control approach (cases control) to determine the predictors of TB treatment default among TB patients in the Upper East region from 2018-2020.
The study was conducted in two phases: a review of TB treatment defaulters’ records 2016 -2020 to help determine the trend of TB treatment default in the region for the years under review and to identify potential participants (sample) for the primary data collection phase.
Following the secondary data collection, a structured questionnaire was used to obtain primary data from participants (TB treatment defaulters from January 2018 to December 2020) in order to learn more about the factors that influence TB treatment non-adherence among TB patients in the study region. To lessen recall bias, 2018-2020 was chosen as the key data gathering period.
The choice of 2018-2020 for the primary data collection was to help reduce recall bias[20]. In this research, respondents who had defaulted on their TB treatment were considered “cases” while those who had been cured were considered as “controls”. The advantage of using matched case control study design is that it allows evaluating multiple possible risk factors for a single outcome from relatively few participants as proposed by [21] and [22]
Study Setting and Research Methodology
The research took place in the Upper East Region of Ghana is located in the country’s north-eastern quadrant. It is bounded to the north by Burkina Faso, to the east by Togo, to the south by the North-East region and to the west by the Upper West region. The region covers 8,842 square kilometers and 2.7 percent of Ghana’s total land area. The land is relatively flat, with a few hills to the east and southeast. Most of the eastern and western parts of the region lie within River Volta’s basins and tributaries. The region lies within the “meningitis belt” (stretching from Senegal in the west to Ethiopia in the east of Africa, making it prone to periodic outbreaks of cerebrospinal meningitis [23]
The region has a population of 1,273,677 with 1,368 communities and a population density of 111/square kilometer according to [24] The annual population growth rate is 1.9%, with a total fertility rate of 3% (Community Water & Sanitation Agency [CWA], 2020). The region is divided into fifteen (15) administrative districts and one hundred (100) health sub-districts. It has 495 health facilities, and GHS operates about 90% of all health facilities in the region (GHS, 2017b). According to the [23] regional report, the Upper East region has a high record of TB treatment non-adherence (GHS, 2019). Although non-adherence to TB is gradually declining nationally, invariably non-adherence to TB treatment in the Upper East is still relatively higher. It is far above the accepted target of 5% by the WHO [23]. This, therefore, justifies the choice of the region for the proposed study. Figure 3.1 presents the location of the Upper East region in Ghana.

Figure 1: Map of Ghana showing the location of the Upper East Region (GSS, 2017)
Study Population
The study population for the cross-sectional study (Review of TB patients’ health records) constituted all confirmed pulmonary TB patients in the past five years (2016 to 2020) who were on TB medication under DOTS in the Upper East region. However, all confirmed pulmonary TB patients in the Upper East Region who were 18 years of age or older and taking TB treatment from 2018 -2020 made up the accessible group for the matched case control study.
Inclusion and Exclusion Criteria
Cases
Inclusion criteria for cases were all TB patients aged 18 years or above who had defaulted on their TB treatment within the survey period (2018-2020). TB treatment defaulters in this research comprised of patients who had experienced treatment interruption for at least two months during an intended treatment period and the years under review (2018-2020) were selected in order to minimize recall bias among participants. While the inclusion criteria for controls were all TB patients aged 18 years or above who had never defaulted on their TB treatment within the survey period (2018-2020) and had been declared cured or complete treatment at the end of the period.
Exclusion criteria for cases were any TB patients 18 years or above who interrupted their TB treatment within the years under review (2018 -2020), but were severely sick and unable to respond or participate or had moved out of the region at the time of data collection. While the exclusion criteria for controls were TB patients aged 18 years or above who adhered to their TB medication within the years under review but were severely sick or had moved out of the region at the time of conducting the study.
SAMPLE SIZE DETERMINATION
This research found out that 72.5% of TB clients who defaulted to TB treatment reported to have smoked cigarette compared with 28 % of TB clients who adhered to the TB treatment also smoked cigarette. The sample size was estimated with a desired power of 90%, precision at 95% confidence level, and a case-to-control ratio of 1:1. As a result, 72.5 percent proportion of cases were exposed Hence, using the difference in proportion formula by Kelsey, Whitmore and Thompson (1996), the sample size of this study was determined as follows:

Where: N cases = number of cases
![]() = standard normal deviation for two tailed-test based on alpha level = 1.96
= standard normal deviation for two tailed-test based on alpha level = 1.96
![]() = power of the study =90% = 1,282
= power of the study =90% = 1,282
![]() = ratio of controls to cases = 1
= ratio of controls to cases = 1
![]() = proportion of cases exposed =72.5% =0.725
= proportion of cases exposed =72.5% =0.725
![]() = proportion of controls exposed 36% = 0.28
= proportion of controls exposed 36% = 0.28
![]() = average proportion =
= average proportion = ![]() =
= ![]() =
= ![]() = 0.505
= 0.505
Substituting the above parameters into the formula:
N cases = ![]()
n cases = ![]() = ≈ 53
= ≈ 53
With the expected non-response rate of 5%, 5/100*53 =2.6 +53=55.6 = 56
Both cases+ controls were, thus, be 56+56 = 112
Hence, using a ratio of cases to controls as 1:1, a sample size of 112 participants were recruited for the study.
Sampling Procedure
Multi-stage sampling technique was used in the selection of the sub-regions and districts and a total of 112 respondents, made up of 56 cases and 56 controls, were interviewed. In selecting the cases and controls, the Upper East region was stratified into three zones: Western zone, Eastern zone and Central zone. The zones were further clustered into districts.
In selecting controls for the study, three districts were selected randomly from each cluster using simple random sampling technique (employing the lottery method). In the selected districts, proportional allocation of sample per the number of TB cases in the district relative to the total sample size. The participants were chosen using a simple random sampling procedure via balloting.
Data Management and Analysis
The data were recorded using EPI Data manager version (4.6.0). Data analysis was done using STATA version 16. To maintain safety and confidentiality, the data were properly stored, backed up and password protected. The data were presented in tables and figures and analyzed on TB treatment data review to examine and identify the trends in the distribution of defaulter among the TB patients’ overtime (2016-2020). Chi square test for trends was used to examine statistical significance of the observed trends in distributions in the data.
A discordant pair analysis (Mantel-Haenszel) was done to determine the predictors of TB treatment default with location and sex as matched variables. However, in analyzing Mantel-Haenszel test results, the raw data from Epi data was exported to excel for cleaning.
The Mantel-Haenszel matched pair analysis was performed using Microsoft excel 2016 and odds ratio calculated using STATA version 21. Concordant and discordant pairs were identified manually in excel while STATA was used to calculate the odds ratios. Matched pairs were identified by response type ID assigned to respondents. All variables that were initially non-dichotomous were re-defined and categorized as dichotomous in order to identify concordant and discordant pairs.
Ethical Consideration
Ethical approval for this study was obtained from the University of Health and Allied Sciences (UHAS) Research Ethics Committee (UHAS-REC A.8 [1] 20-21). Permission was obtained from the Upper East Regional Health Directorate, and subsequently, from the selected districts. Copies of clearance letters and approval to proceed with the study from the University of Health and Allied Sciences were made available to appropriate authorities prior to the start of the study.
RESULTS AND DISCUSSION
Distribution of TB treatment defaulters in Upper East region by age groups
The fig.1 below depicts the trend of TB defaulters recorded by age groups from (2016 -2020) shows the highest number of 43.7% of TB defaulters recorded among patients between the ages of (34-44) in the year 2016 ; 27.3% between the ages(34-44) and 27.3% between the ages of (45-54), in the year 2017. The observe trend of TB defaulters by the various age groups compared across the years (2016 – 2020) was not statistically significant as (Ptrend =0.645).
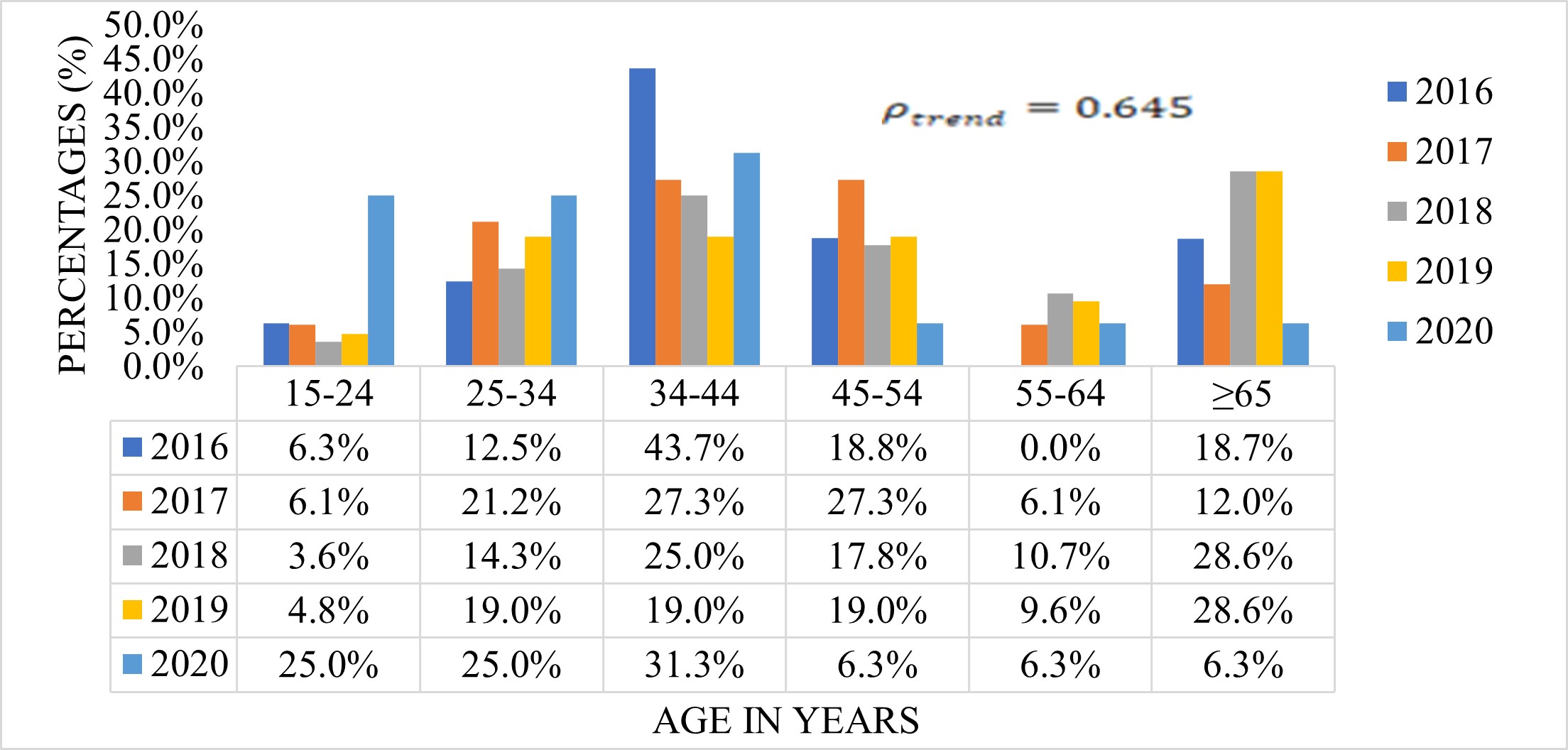
Fig. 1 shows distribution of TB defaulters by age groups, from (2016-2020)
Distribution of TB treatment defaulters in Upper East region by gender
The fig.2 below shows the trend of TB defaulters recorded by gender from (2016-2020). Over the five years (from 2016-2020) the number of male defaulters were more than the female. Moreover, as the number of male defaulters increased from (2016-2017) by 30.2%, and has since been declining steeply, female defaulters increased from 10.7% in 2016 to 25.0% in 2017 and maintained the prevalence of 25.0% in 2018. However, the number of male TB defaulters decreased from the year (2018- 2020). Thus the observe trend of TB defaulters by the various age groups was not statically different in the year (2016-2020) as (Ptrend =0.306).
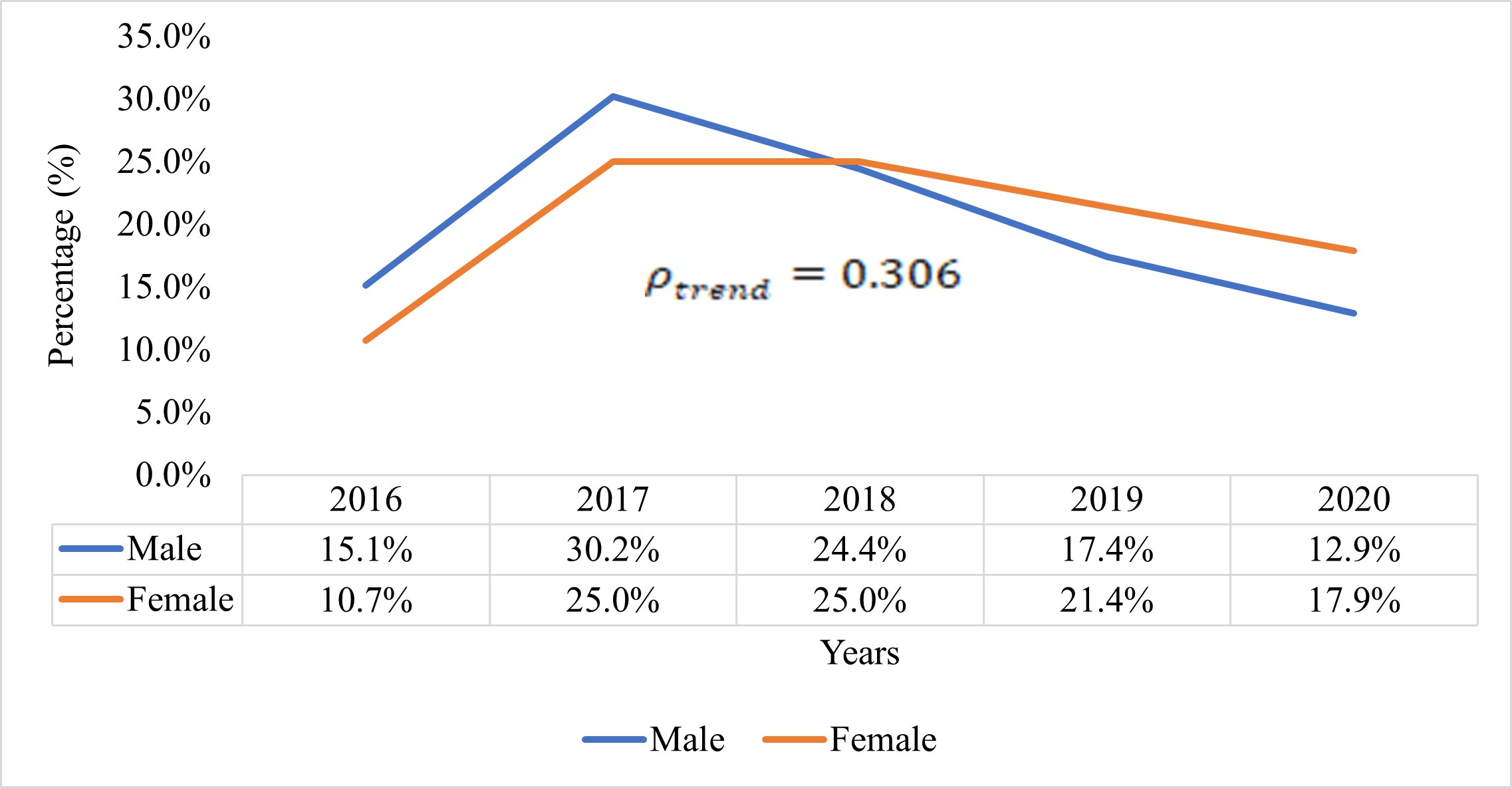
Fig 2 shows distribution of TB defaulters by gender, from 2016 – 2020
Distribution of TB treatment defaulter in Upper East by district
Deducing from fig3, the trend of TB defaulters by the various districts compared across the years (2016-2020) was not statistically significant. The highest number, 15(45.2%) of the TB defaulters were from Bolgatanga Municipal, followed by both Builsa North, 7(21.2%), and Kasena Nankana Municipality, 7(21.2%), Talensi and Bawku Municipal also recorded as low as 2(6.2%) defaulters in the year 2017. Again, Bolgatanga Municipal recorded the highest number 10(35.7%) TB defaulters in 2018, followed by Kasena Nankana Municipal and Bongo District recording 7(25.0%) and 4(14.3%) respectively. However, Bawku Municipal also recorded the highest of 7(33.2%) TB defaulters in 2019, followed by Bolgantanga Municipal, Talensi district and Kasena Nankana Municipality recording 3(14.3%) respectively. Also, Builsa North district recorded the highest number of 5(31.2%) TB defaulters in the Upper East Region in 2020, followed by Bawku Municipality, recording 4(25.0%) defaulters and Pusiga recording 3(18.0%). The rest of districts recorded either 1(6.2%) or zero cases.
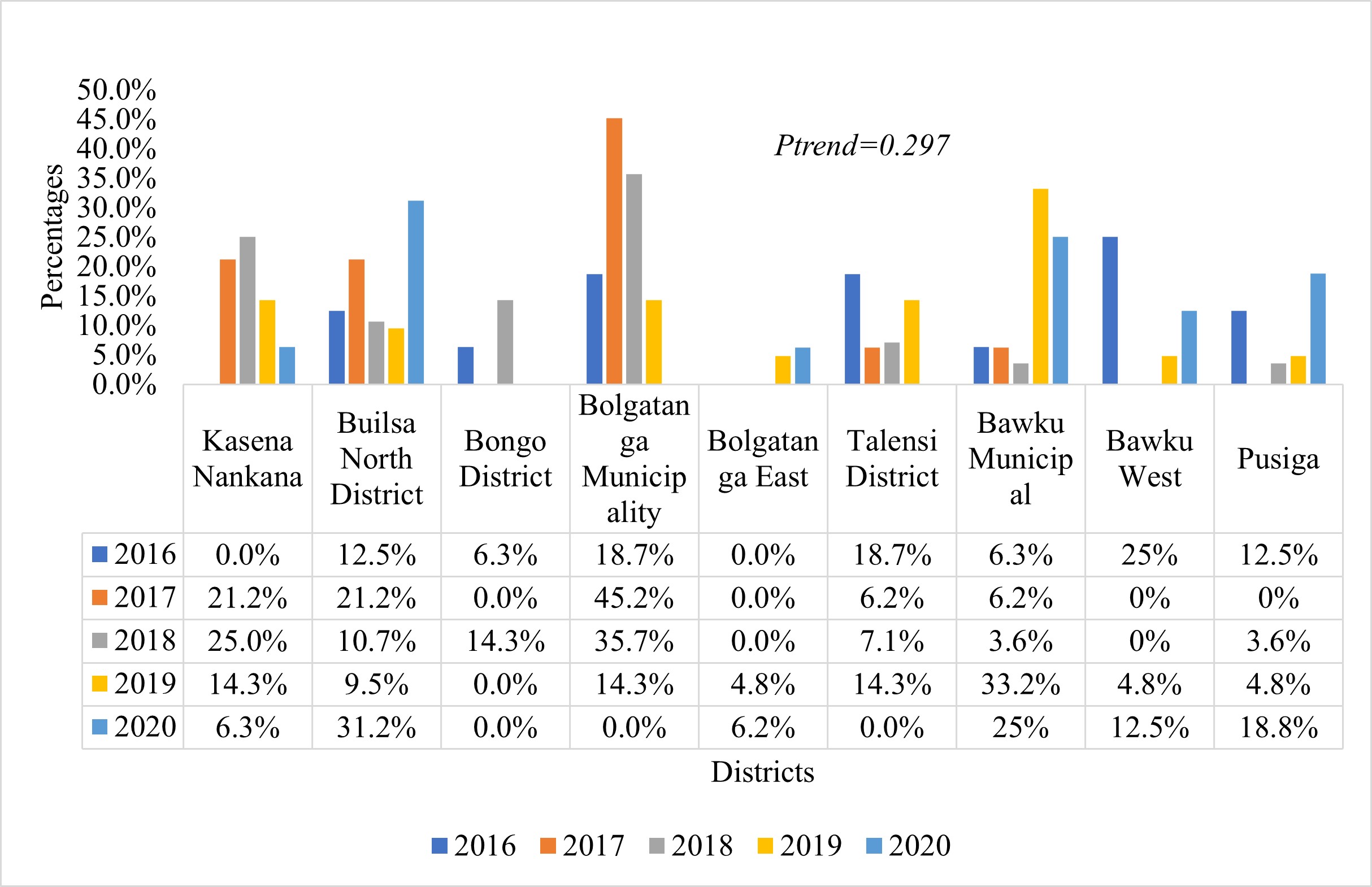
Fig.3 show distribution of TB defaulters by districts from January 2016 -2020
Distribution of TB treatment defaulters in Upper East region by TB infection classification
The fig.4 below depicts the trend of TB defaults recorded by the classification of the TB case from (2016-20200. The trend observed among the TB defaulters recorded by the TB class compared across the five (2016-2020) was not significant as
(![]() ).
).
Throughout the five years, number of Pulmonary TB cases that defaulted treatment increased in the first two years (2016 -2017). While the number from 2017 has been declining.
For the extra pulmonary cases, 1(12.5%) defaulted in 2016, increased to 2(25.0%) in 2017, which had been maintained in number until 2020. The number of extra pulmonary cases who defaulted treatment decreased from 2(25.0%) in 2019 to 1(12.5%) in 2020.
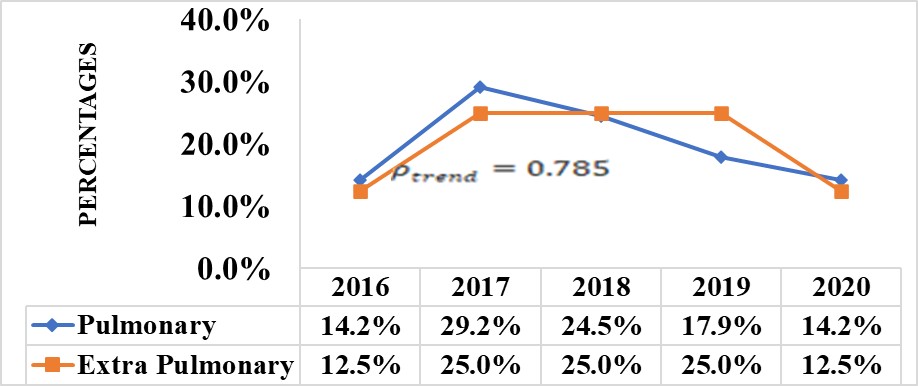
Fig.4 show distribution of TB defaulters by TB class, from (2016- 2020)
Predictors of TB treatment non-adherence among patients treated with the DOTS strategy
A discordant pair analysis (Mantel-Haenszel) was used to assess the predictors of TB therapy using location and gender as matched variables. The Mantel-Haenszel odds ratio (ORMH) refers to the ratio of the sum of the discordant pairs in which the case is exposed over the sum of the discordant pairs in which the control is not exposed. Concordant pairs (in which the case and the control are either both exposed or both unexposed) do not contribute to the numerator nor to the denominator of the ORMH.
Socio-demographic predictors of TB treatment default among respondents
Those whose decision to attend TB clinic was taken by other family members were 2.5 times more likely to default during treatment as compared to those who took the decision by themselves to attend TB clinic [(ORMH=2.5 (95% CI: 1.04, 6.56), p=0.04]. Also, though not statistically significant, those who were unemployed were 3 times more likely to default during TB treatment as compared to those who were employed [(ORMH=3.0 (95% CI: 0.54, 30.39), p=0.15].
Table3.1 Discordant pair analysis of Socio-demographic predictors of TB treatment defaulting (N=112, matched pairs=56)
| Variable | Controls (N=5 6) | ORMH (95% CI) | p-value | |||
| Age | 40yrs+ | <40yrs | Total | |||
| Cases | 40yrs+ | 24 | 12 | 36 | ||
| <40yrs | 15 | 5 | 20 | 0.8(0.34,1.83) | 0.70 | |
| Total | 39 | 17 | 56 | |||
| Marital status | Married | Single | Total | |||
| Cases | Married | 39 | 9 | 48 | ||
| Single | 7 | 1 | 8 | 1.29(0.43,4.06) | 0.80 | |
| Total | 46 | 10 | 56 | |||
| Educational status | No formal Education | Formal Education | Total | |||
| Cases | No formal Education | 29 | 14 | 43 | ||
| Formal Education | 8 | 5 | 13 | 1.75(0.69,4.81) | 0.20 | |
| Total | 37 | 19 | 56 | |||
| Occupational Status | Unemployed | Employed | Total | |||
| Cases | Unemployed | 47 | 6 | 53 | ||
| Employed | 2 | 1 | 3 | 3.0(0.54,30.39) | 0.15 | |
| Total | 49 | 7 | 56 | |||
| Income Level | ≤₵500 | >₵500 | Total | |||
| Cases | ≤₵500 | 34 | 12 | 46 | ||
| >₵500 | 8 | 2 | 10 | 1.5(0.56,4.23) | 0.37 | |
| Total | 42 | 14 | 56 | |||
| Transport to TB Clinic | Public | Private | Total | |||
| Cases | Public | 3 | 2 | 5 | ||
| Private | 7 | 44 | 51 | 0.29(0.03,1.50) | 0.10 | |
| Total | 10 | 46 | 56 | |||
| Cost of Transport to TB Clinic | ≤₵10 | >₵10 | Total | |||
| Cases | ≤₵10 | 37 | 6 | 43 | ||
| >₵10 | 6 | 7 | 13 | 1.00(0.27,3.74) | 1.00 | |
| Total | 43 | 13 | 56 | |||
| TB Clinic Attendance Decision | Not Self | Self | Total | |||
| Cases | Not Self | 11 | 20 | 31 | ||
| Self | 8 | 17 | 25 | 2.5(1.05,6.56) | 0.04* | |
| Total | 19 | 37 | 56 | |||
Source: Field Data (2021)
Health System predictors of TB treatment defaulting
Even though the association of patient waiting time at health facility for TB care and defaulting during TB treatment was statistically insignificant, those who waited for 60 minutes or more were 6 times more likely to default during TB treatment as compared to those who waited for less than 60 minutes [(ORMH=6.0 (95% CI: 0.73, 75.99), p=0.13]
Table 3. 2 Discordant pair analysis of health system predictors of TB treatment defaulting (N=112, matched pairs=56)
| Variable | Controls (N=56) | ORMH (95% CI) | p-<0.05value | |||
| Distance (Km) to TB Clinic | <10Km | ≥10Km | Total | |||
| Cases | <10Km | 29 | 6 | 35 | ||
| ≥10Km | 10 | 11 | 21 | 0.6(0.18,1.82) | 0.45 | |
| Total | 39 | 17 | 56 | |||
| Ever paid money for Medication | Yes | No | Total | |||
| Cases | Yes | 0 | 2 | 2 | ||
| No | 3 | 51 | 54 | 0.67(0.06,5.82) | 1.00 | |
| Total | 3 | 53 | 56 | |||
| Side effect of TB drug | Yes | No | Total | |||
| Cases | Yes | 3 | 12 | 15 | ||
| No | 6 | 35 | 41 | 2(0.69,6.49) | 0.24 | |
| Total | 9 | 47 | 56 | |||
| Reminder on next visit | Yes | No | Total | |||
| Cases | Yes | 53 | 2 | 55 | ||
| No | 1 | 0 | 1 | 2(0.10,117.99) | 1.00 | |
| Total | 54 | 2 | 56 | |||
| Privacy at TB Clinic | Yes | No | Total | |||
| Cases | Yes | 52 | 1 | 53 | ||
| No | 3 | 0 | 3 | 0.33(0.01,4.15) | 0.63 | |
| Total | 55 | 1 | 56 | |||
| Assigned TB Supporter | Yes | No | Total | |||
| Cases | Yes | 41 | 9 | 50 | ||
| No | 4 | 2 | 6 | 2.25 (0.63,9.99) | 0.27 | |
| Total | 45 | 11 | 56 | |||
| Stigma at TB Clinic | Yes | No | Total | |||
| Cases | Yes | 2 | 9 | 11 | ||
| No | 5 | 40 | 45 | 2.25 (0.63,9.99) | 0.27 | |
| Total | 7 | 49 | 56 | |||
| Counselling on TB drugs | Yes | No | Total | |||
| Cases | Yes | 54 | 1 | 55 | ||
| No | 1 | 0 | 1 | 1.00(0.01,78.50) | 1.00 | |
| Total | 55 | 1 | 56 | |||
| Patient’s waiting times | 60 mins++ | <60 mins | Total | |||
| Cases | 60 mins++ | 11 | 6 | 17 | ||
| <60 mins | 1 | 38 | 39 | 6.0(0.73,75.99) | 0.13 | |
| Total | 12 | 44 | 56 | |||
| Ever visited a herbalist | Yes | No | Total | |||
| Cases | Yes | 4 | 11 | 15 | ||
| No | 9 | 32 | 41 | 1.22(0.46,3.33) | 0.82 | |
| Total | 13 | 43 | 56 | |||
| Health seeking facility | Private | Public | Total | |||
| Cases | Private | 4 | 1 | 5 | ||
| Public | 3 | 48 | 51 | 0.33(0.01,4.15) | 0.63 | |
| Total | 7 | 49 | 56 | |||
Source: Field Data (2021)
DISCUSSION OF FINDING AND RESULTS
- Trend of non-adherence to TB treatment among patients treated with the DOTS strategy
This paper found the highest (43.7%) TB defaulters was recorded among patients aged (34-44) years in 2016, followed by patients 34-44 (27.3%) and 45-54 (27.3%) years in 2017. This trend shows a decline in the number of TB defaulters with age. The findings of this study are in line with the findings of a similar study carried out in South Africa [25]. The South African study reported a decline in TB defaulter rate of 9.1% among those between the ages of 25 and 34, 8.7%; 35–44 years: 7.0%; 45–54 years: 5.2%; 55–64 years: 4.4%; >64 years.
Moreover, their study demonstrates a decline in TB defaulter rate with age. However, a study in Nigeria contrasts the current findings where TB defaulter rate increased with old age in the study [26]. Also, this study found increased in TB treatment defaulters among older adults 65 years and above in 2018. This finding is consistent with that of a cohort study conducted in South Korea, where older persons aged over 65years defaulted on their TB treatment in 2017 and 2018, compared to those under 65 [27]
Additionally, in agreement with the findings of this study, a study done in Brazil with 745 TB patients discovered a percentage of 41.5 percent TB treatment non-adherence in patients above the age of 60 (Reis-Santos et al., 2015). Other studies also found higher TB treatment defaulter rate among older (60 years and above) TB patients [28],[29],[30].and [26]
According to the Pakistan Bureau of Statistics Labour Force 2013–14 Survey report, those over 60 are more likely to have negative medication reactions when receiving TB therapy (Pakistan Bureau of Statistics, 2015). Low treatment adherence in the elderly in the current study may be due to the adverse reaction to TB therapy and the higher risk of multi-morbidity and subsequent routine use of five or more medications [31].[32].
Furthermore, this study found that, over the five years’ period from (2016 -2020), the number of male TB treatment defaulters were consistently more than female TB treatment defaulters. Moreover, the number of male defaulters increased from the year 2016 to 2017 by half (30.2%), and declined steeply. For the female defaulters, they increased from 10.7% in 2016 to 25.0% in 2017, and maintained the prevalence of 25.0% in 2018 whiles the number of male TB defaulters decreased from the year (2018 -2020).
2 Socio-demographic predictors of TB treatment non-adherence among patients treated with the DOTS strategy
Considering patient non-adherence to TB therapy as predicted by demographic factors, this study found decision to seek healthcare to be the main predictor of TB treatment default. Besides, this study found that TB patients were 2.5 times more likely to stop taking their medication throughout treatment if their family members made the decision to go to the TB clinic than if they made the decision themselves [(ORMH=2.5 (95% CI: 1.04, 6.56), p=0.04]. This finding is in line with what Ryan and Deci (2017) propounded in their self-determination theory which postulates that when people do not make decision out of their own will or interest (i.e., when one’s autonomy is violated), they are more likely to default a health intervention.
This research indicates that TB patients are more likely to discontinue their TB treatment when they do not take responsibility for the decision to seek TB therapy. Consistent with the current findings,[31] recorded more TB treatment defaulters among patients whose decision to attend TB treatment was influenced by their family members. According to [31], when the family members who influenced the decision to seek TB treatment are unavailable, patients tend to feel reluctant to comply with TB treatment. Contrary to the current findings,[32] found that parental or family influence on decision to undertake TB treatment by TB patients reduced TB defaulter rate in Kumasi. He further revealed that, these TB patients receive adequate support from their family in their TB treatment routine.
The difference in the findings may be attributed to the methodical differences in the two study. Whiles the current study employed a quantitative approach, He used a mixed method approach in soliciting information from participants. Perhaps, respondents in his were able to elaborate on the contribution of family members in their treatment regime contrary to the current study.
3 Healthcare system predictors of non-adherence to TB treatment among patients treated with the DOTS strategy
Even though the association of patient waiting time at health facility for TB care and defaulting during TB treatment was statistically insignificant, comparing individuals who waited for less than 60 minutes to those who waited for 60 minutes or more, the likelihood of defaulting on TB treatment increased by 6 times [(ORMH=6.0 (95% CI: 0.73, 75.99), p=0.13].
Contrary to the current findings, patient waiting time at health facility was associated with TB defaulter rate in Ethiopia [33]. Besides, a cross-sectional study in Sudan found increased TB defaulter rates among patients who wait longer at the medical institution, which is in contrast to the findings of [34]. Other studies have also confirmed the association between patients waiting time and TB defaulter rate [35];[36],[37] These findings call for a more drastic measures to be put in place to reduce TB patients waiting time at the various TB treatment centers in the Upper East region of Ghana.
CONCLUSIONS
This paper found the number of TB defaulters to be higher among males than females from 2016 to 2020. This implies that more males are prone to die from TB due to their poor adherence to TB treatment but males defaulters was found to have declined progressively from (2017-2020). Furthermore, the number of TB defaulters were highest in the Bolgatanga municipality which implies that high defaulter rate implies a potential spread of the TB disease in the Bolgatanga municipality if adequate measures are not put in place. It was also realised that, the higher number of TB defaulters in the Bolgatanga municipal was recorded in 2019 and experienced a further increase in 2020.
This may mean that the outbreak of the Covid-19 disease influenced TB control program negatively. This possible failure on the part of the TB control program may put the public in danger through their exposure to the defaulted TB patients in the Bolgatanga municipality and hereby recommend that TB patients whose parents or family member/s decide on when and where to seek TB treatment intervention were more likely to default their TB treatment. Therefore, a more drastic measures should be put in place to counter the predictor of TB treatment default identified in this study.
In order to control the predictors influencing TB defaulter rate in the Upper East Regional TB control programme should gear their efforts towards educating TB patients on TB treatment to enable TB patients to make their own decision to seek TB treatment an makes policy on TB treatment in the Upper East region should be geared towards ensuring TB patients autonomy in the TB treatment process
REFERENCES
- World Health Organisation (2022a). Tuberculosis: Key facts. Retrieved from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- World Health Organisation (2022b). Tuberculosis: Key facts. Retrieved from https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- Teferi, M. Y., El-Khatib, Z., Boltena, M. T., Andualem, A. T., Asamoah, B. O., Biru, M., & Adane, H. T. (2021). Tuberculosis treatment outcome and predictors in africa: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 18(20), 10678.
- Dogah, E., Aviisah, M., Kuatewo, D. A. M., Kpene, G. E., Lokpo, S. Y., & Edziah, F. S. (2021). Factors Influencing Adherence to Tuberculosis Treatment in the Ketu North District of the Volta Region, Ghana. Tuberculosis Research and Treatment, 2021, 1-6.
- Osei, E., Oppong, S., & Der, J. (2020). Trends of tuberculosis case detection, mortality and co-infection with HIV in Ghana: A retrospective cohort study. Plos One, 15(6), e0234878
- Danso, E., Addo, I. Y., & Ampomah, I. G. (2015). Patients’ compliance with tuberculosis medication in Ghana: evidence from a periurban community. Advances in Public Health, 2015, 1-12.
- Salifu, Y., & Eliason, C. (2017). Tuberculosis treatment adherence in Ghana: Patients’ perspectives of barriers and enablers to treatment. NUMID, 7, 6-23.
- Tesfahuneygn, G., Medhin, G., & Legesse, M. (2015). Adherence to Anti-tuberculosis treatment and treatment outcomes among tuberculosis patients in Alamata District, northeast Ethiopia. BMC Research Notes, 8(1), 503.
- Addo, K. K., Yeboah-Manu, D., Dan-Dzide, M., Owusu-Darko, K., Caulley, P., Mensah, G. I., and Ofori-Adjei, D. (2010). Diagnosis of tuberculosis in Ghana: the role of laboratory training. Ghana Medical Journal, 44(1).
- [10]. Bjerrum, S., Kenu, E., Lartey, M., Newman, M. J., Addo, K. K., Andersen, A. B., & Johansen, I. S. (2015). Diagnostic accuracy of the rapid urine lipoarabinomannan test for pulmonary tuberculosis among HIV-infected adults in Ghana–findings from the DETECT HIV-TB study. BMC infectious diseases, 15(1), 407.
- Der, J.B., Grint, D. Narh, C. T., Bonsu, F., & Grant, A.D. (2020). Where are patients missed in the tuberculosis diagnostic cascade? Prospective cohort study in Ghana. PloS One, 15(3), e0230604.
- Kuupiel, D., Adu, K. M., Apiribu, F., Bawontuo, V., Adogboba, D. A., Ali, K. T., & Mashamba-Thompson, T. P. (2019). Geographic accessibility to public health facilities providing tuberculosis testing services at point-of-care in the upper east region, Ghana. BMC Public Health, 19(1), 718.
- Osei, E., Akweongo, P. & Binka, F. (2015). Factors associated with delay in diagnosis among tuberculosis patients in Hohoe Municipality, Ghana. BMC Public Health, 15, 721-732.https://doi.org/10.1186/s12889-015-1922-z
- Ajao, K. O., Ogundun, A. O., Afolabi, O. T., Ojo, T. O., Atiba, B. P., & Oguntunase, D. O. (2014). Treatment compliance and challenges among tuberculosis patients across selected health facilities in Osun State Nigeria. Afr J Med Med Sci, 43(5), 21-9.
- AlSahafi, A. J., Shah, H. B. U., AlSayali, M. M., Mandoura, N., Assiri, M., Almohammadi, E. L., and AlGarni, F. (2019). High non-compliance rate with anti-tuberculosis treatment: a need to shift facility-based directly observed therapy short course (DOTS) to community mobile outreach team supervision in Saudi Arabia. BMC Public Health, 19(1), 1-10.
- .Mekonnen, H. S., & Azagew, A. W. (2018). Non-adherence to anti-tuberculosis treatment, reasons and associated factors among TB patients attending at Gondar town health centers, Northwest Ethiopia. BMC Research Notes, 11(1), 1-8.
- Fang, X. H., Shen, H. H., Hu, W. Q., Xu, Q. Q., Jun, L., Zhang, Z. P., … & Wu, G. C. (2019). Prevalence of and Factors Influencing Anti-Tuberculosis Treatment Non-Adherence Among Patients with Pulmonary Tuberculosis: A Cross-Sectional Study in Anhui Province, Eastern China. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 25, 1928.
- Zhou, C., Chu, J., Liu, J., Tobe, R. G., Gen, H., Wang, X., … & Xu, L. (2012). Adherence to tuberculosis treatment among migrant pulmonary tuberculosis patients in Shandong, China: a quantitative survey study. PloS One, 7(12), e52334.
- Windle, P. E. (2010). Secondary data analysis: is it useful and valid. Journal of PeriAnesthesia Nursing, 25(5), 322-324.
- Gebremedhin, D., Berhe, H., & Gebrekirstos, K. (2016). Risk factors for neonatal sepsis in public hospitals of Mekelle City, North Ethiopia, 2015: unmatched case control study. PloS One, 11(5), e0154798.
- Weldearegawi, G. G., Teklehaimanot, B. F., Gebru, H. T., Gebrezgi, Z. A., Tekola, K. B., & Baraki, M. F. (2019). Determinants of late antenatal care follow up among pregnant women in Easter zone Tigray, Northern Ethiopia, 2018: an unmatched case-control study. BMC Research Notes, 12(1), 752.
- Gumma, M. K., & Pavelic, P. (2013). Mapping of groundwater potential zones across Ghana using remote sensing, geographic information systems, and spatial modelling. Environmental Monitoring and Assessment, 185(4), 3561-3579.
- Ghana Statistical Service (2019). Population by regions: Upper East. https://statsghana.gov.gh/regionalpopulation.php?population=MTQ3NzkxOTU0MS4wODQ=&&Upper%20East®id=8.
- Kigozi, G., Heunis, C., Chikobvu, P., Botha, S., & Van Rensburg, D. (2017). Factors influencing treatment default among tuberculosis patients in a high burden province of South Africa. International Journal of Infectious Diseases, 54, 95-102
- Ifebunandu, N. A., & Ukwaja, K. N. (2012). Tuberculosis treatment default in a large tertiary care hospital in urban Nigeria: prevalence, trend, timing and predictors. Journal of Infection and Public Health, 5(5), 340-345.
- Bea, S., Lee, H., Kim, J. H., Jang, S. H., Son, H., Kwon, J. W., & Shin, J. Y. (2021). Adherence and Associated Factors of Treatment Regimen in Drug-Susceptible Tuberculosis Patients. Frontiers in pharmacology, 12, 625078. https://doi.org/10.3389/fphar.2021.625078
- Gust, D. A., Mosimaneotsile, B., Mathebula, U., Chingapane, B., Gaul, Z., Pals, S. L., & Samandari, T. (2011). Risk factors for non-adherence and loss to follow-up in a three-year clinical trial in Botswana. PLoS One, 6(4), e18435.
- Kulkarni, P. Y., Akarte, S. V., Mankeshwar, R. M., Bhawalkar, J. S., Banerjee, A., & Kulkarni, A. D. (2013). Non. Adherence of new pulmonary tuberculosis patients to anti. Tuberculosis treatment. Annals of Medical and Health Sciences Research, 3(1), 67-74.
- Naidoo P, Peltzer K, Louw J, Matseke G, Mchunu G, Tutshana B (2013). Predictors of tuberculosis (TB) and antiretroviral (ARV) medication non-adherence in public primary care patients in South Africa: a cross-sectional study. BMC Public Health, 2(13) 396-406.
- Freire I. L. S., Santos F. R., Lcc M. (2019). Adherence of elderly people to tuberculosis treatment. Rev. Fund Care Online 11 (3), 555–559.
- Adu, P. M. (2016). Non-adherence to tuberculosis treatment and determinant factors among patients with tuberculosis in Kumasi, Ghana. PloS one, 5(12), e76793.
- Nezenega, Z. S., Gacho, Y. H., & Tafere, T. E. (2013). Patient satisfaction on tuberculosis treatment service and adherence to treatment in public health facilities of Sidama zone, South Ethiopia. BMC Health Services Research, 13(1), 1-8.
- OAA, A., & Martin, H. P. (2014). Barriers leading to treatment default among tuberculosis patients in Khartoum State, Sudan: a qualitative study. Clin Med Invest 3(1): 1-8
- Nour El Din, M., Elhoseeny, T., & Mohsen, A. M. M. A. (2013). Factors affecting defaulting from DOTS therapy under the national programme of tuberculosis control in Alexandria, Egypt. EMHJ-Eastern Mediterranean Health Journal, 19 (2), 107-113, 2013
- Suliman, Q., Lim, P. Y., & Tan, K. A. (2022). Risk factors for early TB treatment interruption among newly diagnosed patients in Malaysia. Scientific Reports, 12(1), 1-9.
- Bulage, L., Sekandi, J., Kigenyi, O., & Mupere, E. (2014). The quality of tuberculosis services in health care Centres in a rural district in Uganda: the providers’ and clients’ perspective. Tuberculosis Research and Treatment, 2014, 1-11.