
Isolation, Identification and Detection of Campylobacter Fetus from Dairy & Poultry Products and Development of Pcr
- B. Bhavitha
- 931-939
- May 6, 2024
- Development Studies
Isolation, Identification and Detection of Campylobacter Fetus from Dairy & Poultry Products and Development of PCR
B. Bhavitha
M. G. R College, Hosur
DOI: https://dx.doi.org/10.47772/IJRISS.2024.804069
Received: 21 April 2024; Accepted: 03 April 2024; Published: 06 May 2024
ABSTRACT
Campylobacters spp. are mainly responsible for gastrointestinal infections. The main source of infection is the consumption of contaminated or undercooked meat (especially poultry products), unpasteurized dairy products and untreated water. It is a type of zoonotic disease where it spreads through feces and mouth. Campylobacter species are widespread among warm-blooded animals, so they are found in food animals such as poultry, cattle, pigs, sheep and ostriches. Therefore, animal samples were used in this study. The most common causes of this infection are Campylobacter jejuni (C.jejuni), Campylobacter coli (C.coli) and Campylobacter fetus (C. fetus). Molecular techniques such as multiplex polymerase chain reaction (mPCR) have been optimized to detect these species. Campylobacter fetus was initially divided into two subspecies to reconcile significant epidemiological, clinical, and biochemical differences between the two similar taxa, which were later shown to be highly related at the genomic level. Campylobacter fetus occurs mainly in the intestines of cattle and sheep and can cause spontaneous abortion in both animals.
Key words: Campylobacter coli, Campylobacter fetus and Campylobacter jejuni, PCR.
INTRODUCTION
Campylobacteriosis is the most commonly reported zoonosis in the European Union (EU) in the last decade, with more than 90% of infections caused by Campylobacter jejuni[1,2]. In tropical developing countries where Campylobacter infection was hyperendemic among young children [3]. The disease was initially identified by Theodor Escherich in 1886. He described the symptoms of intestinal Campylobacter infections in children as “cholera infantum” or “summer complaint” [4]. After this, Campylobacter was identified for the first time in 1906 when two British veterinarians reported the presence of “large numbers of a peculiar organism” in the uterine mucus of a pregnant sheep. Following that, the role of Campylobacter in sheep abortion was initially recognized when McFadyean and Stockman reported their isolation (named Vibrio at the time) from an aborted sheep Fetus in Britain in 1913 [5].
For many years, Campylobacters were commonly known as “Vibrio-like organisms” until 1963 when Sebald and Veron assigned the name “Campylobacter” to the genus. They made this decision based on the organisms’ shape and their need for microaerophilic growth [6]. Stern et al. measured seasonal changes in Campylobacter prevalence over the course of 1 year[7]. In 2006, New Zealand had one of the highest rates of campylobacteriosis among developed nations, recording 383.5 cases per 100,000 individuals [8].
The genus Campylobacter currently includes at least 28 validly described species and subspecies, based on DNA-DNA hybridization and 16S rRNA gene sequence analysis [9]. Campylobacter was not identified as a source of human enteritis until the mid-1970s, when specialized media for isolating the bacterium from human stool were developed[10].Most cases of Campylobacter-related illnesses in humans had symptoms like diarrhea, cramps, and possibly fever. Some severe cases required antibiotics, especially for immunocompromised patients[9]. Humans were typically infected through the consumption of undercooked or contaminated food, especially poultry meat, water, or milk, or through contact with animals or animal feces.[4]. However, the exact source remaining unclear in many cases[11].Person-to-person transmission is very rare[12].Recent studies suggested that C. jejuni infections were linked to the development of inflammatory bowel diseases such as Crohn’s Disease[7]. Also, severe neuropathological disorders Guillain–Barré syndrome (GBS) and Miller Fisher syndrome (MFS), along with reactive arthritis were associated with Campylobacter [4].
In these cases, macrolides, primarily erythromycin, clarithromycinor azithromycin, and Fluoroquinolones, such as ciprofloxacin, are the drugs of choice for treatment of diarrheal illness. Tetracycline or doxycycline and select β-lactams also have been used for treating intestinal infections [13]. Detecting and identifying Campylobacter spp. was somewhat challenging due to its long incubation period and specific culture needs, including microaerobic conditions. However, various rapid and sensitive detection methods, such as immunological detection and PCR assays, were developed to address these challenges [14]. Conventional detection methods are difficult to perform and time consuming, causing disadvantages while handling large-scale samples or attempting to make a rapid diagnosis[15].
The PCR assay was used to detect Campylobacter infections in cattle and poultry products, including milk, water, and meat samples, as well as herd environments[16,2]. After enrichment and subculture on selective medium[16].Conventional cultural methods for diagnosing campylobacteriosis were laborious and time-consuming[17]. The global significance of Campylobacter as gastrointestinal human pathogens motivated numerous studies to characterize their population biology and evolution[4].The predominant Campylobacter species is Campylobacter jejuni, responsible for over 90% of infections, with Campylobacter coli causing the majority of the remaining cases[12].
Some studies report an association between dental disease or tooth extraction in combination with raw meat consumption leading to C. fetus infection[18].Campylobacter fetus subsp. fetus is transmitted orally and colonises the intestines of cattle and sheep inducing septic abortion, infertility, and diarrhea in cattle and sheep,C. jejuni and C. coli are also recognized as causal agents of abortions[19,10].Ovineabortion held significant importance in the economies of nations where lamb was the primary source of animal protein[20].Abortions could occur at any point, but were typically identified most frequently during the 4 to 6 months of gestation period. The condition generally resolved on its own in females, with most cows recovering and conceiving again within 3 to 6 months after being infected. Immunity lasted for several years, although some individuals might remain infected for extended periods. In contrast, bulls typically didn’t show any symptoms of the infection, and neither lesions nor protective immunity developed in them. The bacteria could inhabit the crypts of the preputial epithelium in bulls, and as they aged, the size and number of these crypts increased, allowing the infection to persist, leading to what was termed chronic carrier status. This made diagnosis and treatment more challenging [19]. The infection was often asymptomatic in males and was silently transmitted for long periods, allowing the pathogen to circulate within cattle herds [2].Detection of this important pathogen has frequently proven to be difficult under laboratory conditions[21]. The challenges associated with identifying campylobacters through phenotypic and genotypic tests were recently examined, with most issues related with theircomplextaxonomy, demanding growth conditions, and biochemical inactivity[22].
Campylobacter vaccination was globally employed to manage reproductive losses in sheep, yet this pathogen continued to be a primary cause of sheep abortions. The significant genetic and antigenic diversity among Campylobacter strains, along with inadequate cross-protection between the vaccine and wild-type bacteria, likely played a role in vaccine ineffectiveness[20].A recent Canadian study found about 145,000 cases of C. jejuni infection among 32.5 million people in 2006. This ranked C. jejuni as the third most common foodborne pathogen, following norovirus and Clostridium perfringens[23].
There is strong evidence that C. jejuni survives well in farm animal feces, in water, and in sand from the runs of chicken farms[21]. Poultry and ruminants were both major sources of human campylobacteriosis. From 2010 to 2015, the CDC reported 209 Campylobacter outbreaks in the US, with 72 linked to dairy and 33 to poultry. Infected cattle on farms could spread Campylobacter, raising infection risks through environmental contamination[24].It is also possible that manure-contaminated soil acts as a reservoir for C. jejuni in the field3.The disease can be economically important when present in cattle herds[19].Generallypoultry meats are known to be a primary cause of campylobacteriosis[3]. Other foods like ground beef, water, oysters, eggs, vegetables, and milk were also linked to Campylobacter illness[14]. Campylobacter, shed in the feces of dairy cattle, could have been easily transmitted to humans through dairy products like unpasteurized milk[24].Unpasteurized raw milk, in particular, was well-known for causing Campylobacter outbreaks[14].
Recent reports indicated that multistress-tolerant strains of C. jejuni found in raw milk were capable of surviving high-temperature, short-time (HTST) pasteurization procedures. Consequently, understanding the prevalence of C. jejuni on dairy cattle farms was deemed crucial for disease management and prevention.C. jejuni strains had the ability to recombine and readily incorporate DNA from their surroundings, leading to significant genetic variability. Due to this genetic diversity, C. jejuni could express a broad range of toxins and pathogenic traits[24].The organism is cytochrome oxidase positive, microaerophilic, gram- negative, non- spore forming bacteria and possess a single or bipolar flagella at one or both ends[25].It is a curved shaped rods, ranging from0.2-0.8e and 0.5-6.0 long. When two or more bacterial cells are grouped together, they form an “S” or a “V” shape of gull wing.Themajority of Campylobacter species had a characteristic of corkscrew-like motion and is carried in the intestine of many wild and domestic animals.campylobacter is sensitive to high temperarture, low PH and osmoticstress.[14,26,27,28,25].The ideal environment for optimal growth of Campylobacter spp. requires an atmosphere containing approximately 5% O2, 10% CO2, and 85% N2[29].
MATERIALS AND METHODS
Our goal with this study was to create a polymerase chain reaction (PCR) assay for detecting and identifying Campylobacter spp. (particularly C. fetal) in dairy animals and poultry products. This technique used DNA templates extracted from cultured samples after enrichment on a selective medium.
2.1 Sample collection
These samples were collected from both organized and unorganized sheep and poultry farms in the Kashmir Valley. And samples were collected in sterile vials and transported to the laboratory with an ice pack in Cary Blair transport media. Isolated on Sterile cellulose acetate membranes of 0.45µ pore size placed on Muller Hinton Agar supplemented with 5% sheep blood and culture is incubated for 1-2 days at 37˚-42˚C in microaerophilic condition [30].
2.2. Sterilization and Incubation:
The Campylobacter broth base was weighed and added to distilled water in a sterile container. Agar was added into the medium, and the components were thoroughly mixed to dissolve completely. The media was sterilized by autoclaving at a temperature of 121℃ for 20 minutes. After autoclaving, the medium was brought to room temperature, and Campylobacter supplement III was aseptically added into the media. The medium was poured into sterile Petri dishes, and the medium was allowed to solidify. After solidification, a loop full of culture was taken, and the plates were streaked. The plates were positioned in an anaerobic jar and were incubated at 42℃ for 48 hours.

Figure 1. Cultures plates growing in anaerobic conditions
2.3. Gram’s staining
Gram staining is a differential staining technique that divides bacteria into two groups: Gram-positive and Gram-negative, depending on cell wall composition. The method begins with the staining of bacterial cells with crystal violet, followed by the addition of iodine, which forms a compound with the crystal violet within the cell. This is then washed with alcohol or acetone, which serves as a decolorizer and removes the stain from some bacterial cell walls. Gram-positive bacteria maintain the crystal violet-iodine complex due to their thicker peptidoglycan layer, making them seem purple, but Gram-negative bacteria lose the stain and are counterstained with safranin, making them appear pink under the microscope.
2.4. DNA Extraction
The bacterial culture was dispensed into individual 1.5 mL Eppendorf tubes using a sterile micropipette and tips at 1 mL per tube. The tubes were then centrifuged at 15,000 rpm for 2 min to pellet the bacterial cells, after which the supernatant was carefully removed with a micropipette. 200 µL of lysis buffer was added to each pellet and carefully resuspended. RNase (2 µl) and ProteinaseK (10 µl) were then added to the tubes, followed by vigorous vortexing to ensure complete dissolution of the cellular components. The tubes were then placed in a dry bath incubator at 56°C for 15 minutes to facilitate enzymatic reactions. After the incubation period, 350 µl of binding buffer and 50 µl of magnetic beads were added to each test tube. A full vortex was performed and the tubes were allowed to incubate for 5 minutes at room temperature. The next steps were automated with ROBAC (Robotic Biomolecule and Cell Separator), a semi-automated machine capable of processing 16 samples simultaneously. The machine’s nickel-plated sensors were sterilized with UV light for 10 minutes and placed in a holder attached to the ROBAC. An Eppendorf grid containing prepared tubes was then placed into the machine, beginning an automated process that took approximately 10 minutes. After automated extraction, the elution tubes containing the collected samples were mixed and further incubated in a dry bath to ensure. . efficient DNA elution. After another vigorous vortex, the tubes were centrifuged at 15,000 rpm for 2 minutes. The elution was then transferred to new Eppendorf tubes and stored at -20℃ until further steps in the procedure.
2.5. Primers
Nucleotide sequence data for all three was species taken from (accession; OV754562.1 (C.jejuni), CP038868.1 (C.coli) andC. fetus (CP042162.1) ). Two sets of specific primers were designed using software, primers were selected based on the brightest band appearance. Multiplex PCR (mPCR) was carried out with the combination of two specific pairs of primers in one reaction.
2.6. PCR amplification
The species were amplified using monoplex PCR with genes MapA, ceuE and CarbSpC. fetus specific to Campylobacter jejuni, Campylobacter coli and Campylobacter fetus respectively. The monoplex PCR assay was optimized to function in a final reaction volume of 25 μl with these primers and under these conditions: 10X PCR buffer with MgCl2(2.5µl); dNTPs(2µl)(; Forward and reverse primers (0.5µl each); DNA template(1 µl); Taq DNA polymerase (0.15 µl) and remaining adjusted with Nuclease free water. The assay was performed using Applied Biosystems(Thermal cycler) under the following cycling conditions: initialization denaturation at 94°C for 5 min, followed by 35 cycles of 94°C for 1 min, 52°C for 60 s, 72°C for 60 s, followed by a final extension at 72°C for 10 min[31].
2.7. Multiplex PCR
A multiplex PCR test was performed with conservative genes: Campylobacter spp. with a typical IAC (16SrRNA) gene. The membrane lipoprotein gene (MapA) for C. jejuni, the lipoprotein component of the enterochelin gene (CeuE) for C. coli, and the carbon starvation protein gene for C. fetus . The sequence used for the primers is shown in Table 1. The multiplex PCR assay was optimized to run in a final reaction volume of 25 μl with these primers and conditions Taq DNA Polymerase Master Mix RED 2x and 1.5 mM MgCl2 ( 10 µl); Forward and reverse primers (3 µl each) ;DNA template (1.5 µl) and the rest adjusted with nuclease-free water. Analysis was performed using Applied Biosystems (Thermocycler) under the following cycling conditions: denaturation at 94 °C for 5 min followed by 35 cycles of 94 °C for 1 min, 52 °C for 60 s, 72 °C: 60 s followed by final extension at 72°C for 10 min[31].
Table 1. The primers were used for the assay.
PCR primers used for Campylobacter speciation
| Target gene | Product size(bp) |
| 16S rRNA (genus specific) | 201 |
| MapA (C. jejuni) | 340 |
| CeuE (C. coli) | 582 |
| CarbSP (C. fetus subsp. fetus) | 749 |
2.8. Sensitivity and Specificity of the multiplex PCR assay
The sensitivity of the multiplex PCR assay was tested by changing DNA concentration, Where the DNA of each species in multiplex PCR was tested and 0.5µl DNA was the limit of detection of all three species.
The specificity of the multiplex PCR assay was tested by using primers of one species cross-reacted with all three species’ genomic DNA. Where DNA was extracted from an overnight culture with the SN Bacterial DNA isolation kit (Bengaluru, India).
RESULTS AND DISCUSSION
Campylobacter spp. stands out as a major contributor to foodborne illness, mainly through campylobacteriosis. The consequences of this bacterial infection can range from mild diarrhea to serious complications such as fever, miscarriage, and even Guillain-Barre syndrome. These symptoms highlight the importance of early detection and intervention. One of the main routes of infection is the consumption of undercooked meat, especially poultry such as chicken, lamb and beef. Recognizing the importance of this threat, researchers have developed a multiplex PCR assay designed to rapidly detect three prominent species: C. jejuni, C. coli, and C. fetus.
The design of the multiplex PCR assay is carefully tailored for specificity . and efficiency. Specific primers targeting specific genes were designed for each Campylobacter species: the membrane lipoprotein gene (MapA) for C . jejuni, the lipoprotein component of the enterochelin gene (CeuE) for C. coli and the carbon starvation protein gene for C. fetus.
The different sizes of these primers – 340 bp, 582 bp and 749 bp – help to accurately identify each species. In addition, the addition of an internal positive control of 16S rRNA ensures the reliability of the results by validating the PCR conditions. This internal control serves as an important reference point that minimizes the risk of false negative results, especially in cases where the copy number difference between the control locus and the diagnostic loci is not critical.
The simplicity and sensitivity of the multiplex PCR method make it very good value for the detection of Campylobacter. The smooth process, together with the fact that the stock does not require further processing apart from the spin method, emphasizes its practicality and efficiency. The potential impact of the analysis on clinical diagnosis is profound, providing a fast and accurate way to detect Campylobacter spp. infections in their nascent stage.
Early detection is key to controlling the spread of these pathogens and reducing associated health risks, making the mPCR test a valuable tool in public health initiatives aimed at combating foodborne illnesses. In addition, the versatility of the multiplex PCR method extends beyond the clinical settings Its usefulness extends to many fields, including food safety and epidemiological surveillance. Rapidly identifying Campylobacter spp. preventive measures can be taken in animal populations and foodstuffs to prevent diseases and protect public health.
In addition, the adaptability of the assay facilitates its integration into routine screening protocols, which improves overall surveillance capability and enables rapid response to new threats. Continuous improvement and optimization of molecular diagnostic techniques such as multiplex PCR emphasizes a proactive approach to the assay. audience health problems As microbial threats evolve, so must our diagnostic capabilities.
The multiplex PCR analysis is a significant advance in this regard and is an effective tool for the early detection and control of Campylobacter infections. Its continued development and deployment promises to strengthen our defenses against foodborne illness and promote a safer, healthier future for all..

Fig. 3.1. monoplex PCR: Lane 1. C. coli(C1); 2. C. coli(C2); 3. C. jejuni(J1); 4. C. jejuni(J2); 5. C. jejuni(J3); 6. C. jejuni(J4); 7. C. jejuni(J5); 8. C. jejuni(J6); 9. C. jejuni(J7); 10. C. jejuni(J8); 11. C. fetus subsp. fetus(F1)
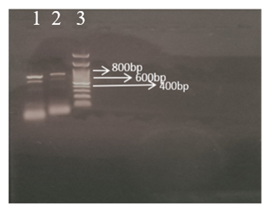
Fig. 3.2 Multiplex PCR: lane 1: C. jejuni; C. coli, and C. fetus. Lane 2: C.jejuni; C.coli, and C.fetus. Lane 3:100bp
CONCLUSION
In our study, we developed and validated a new multiplex PCR-based assay for the rapid detection of three prominent Campylobacter species that cause campylobacteriosis, a common foodborne illness. This innovation holds significant promise for clinical diagnostics, providing healthcare professionals with a rapid and reliable means to rapidly diagnose Campylobacter infections. Unlike traditional methods, which often require time-consuming culture techniques, our PCR-based multiplex assay streamlines the diagnostic process and provides results with greater speed and accuracy. In addition, the simplicity of the method facilitates its application in a variety of clinical settings, which can reduce diagnostic delays and improve patient outcomes. coli, this innovative approach can improve early detection and facilitate rapid intervention strategies in epidemic situations. Its efficiency in detecting multiple species simultaneously saves time and resources, as well as reduces the risk of false negative results, improving the overall reliability of Campylobacter surveillance systems. Overall, our study highlights the transformative potential of multiplex PCR-based analysis to advance clinical and public health initiatives to combat Campylobacter infections and reduce their burden on global health systems.
REFERENCE
- Sigita Ramonaite, Egle Tamuleviciene, Thomas Alter, Neringa Kasnauskyte and Mindaugas Malakauska. MLST genotypes of Campylobacter jejuni in Lithuania Ramonaite et al. BMC Infectious Diseases (2017).
- Coral Polo , Teresa García-Seco , Marta Hernandez, Víctor Fernandez, David Rodríguez-Lazaro , Joaquín Goyache , Lucas Domínguez , Marta Perez-Sancho; Evaluation of PCR assays for Campylobacter fetus, 14 July 2021.
- David A. Alfredson & Victoria Korolik, St John of God Pathology, Australia; and Microbial Glycobiology, Institute for Glycomics Australia. Antibiotic resistance and resistance mechanisms in Campylobacter, 19 October 2007.
- Andrea Margarita Olvera-Ramírez , Neil Ross McEwan, Karen Stanley , Remedios Nava-Diaz and Gabriela Aguilar-Tipacamú; 13 April 2023; Role of Wildlife as Carriers and Spreaders of Campylobacter spp; ani13081334.
- Orhan Sahin, Michael Yaeger, Zuowei Wu, and Qijing Zhang: Campylobacter-Associated Diseases in Animals. Department of Veterinary Diagnostic ,Pathology, Microbiology and Production Animal Medicine. November 9, 2016.
- Smith and Tylor 1919 and Sebald and veron 1963; campylobacter fetus.
- S.M. Horrocks , R.C. Anderson , D.J. Nisbet , S.C. Ricke United States Department of Agriculture, Agricultural Research Service, Incidence and ecology of Campylobacter jejuni ; AR 72704, USA, 15 (2009).
- B. J. Gilpin, P. Scholes, B. Robson and M. G. Savill Institute of Environmental Science and Research Ltd., Christchurch, New Zealand; The Transmission of Thermotolerant Campylobacter spp. to People Working on Dairy Farms ; December 4, 2007.
- Orhan Sahin, Michael Yaeger, Zuowei Wu, and Qijing Zhang: Campylobacter-Associated Diseases in Animals. Department of Veterinary Diagnostic ,Pathology, Microbiology and Production Animal Medicine. November 9, 2016.
- K. Sato, P. C. Bartlett, J. B. Kaneene, and F. P. Downes. College of Veterinary Medicine and Department of Community Health, Michigan 48909. Vol. 70, No. 3 Comparison of Prevalence and Antimicrobial Susceptibilities of Campylobacter. 2 December 2003.
- B. WEGMULLER, J. LUTHY, AND U. CANDRIAN Laboratory of Food Chemistry, Institute of Biochemistry, 4 May 1993; Direct Polymerase Chain Reaction Detection of Campylobacter in Raw Milk and Dairy Products, Vol. 59, No. 7.
- Amera Gibreel and Diane E. Taylor; Journal of Antimicrobial Chemotherapy (2006) ; 30 May 2006, Macrolide resistance in Campylobacter jejuni, Department of Medical Microbiology and Immunology, University of Alberta, Edmonton, Alberta, Canada.
- Chris A. Whitehouse, Shaohua Zhao, Heather Tate; U.S. Food and Drug Administration, Laurel; Volume 103, ISSN 0065-2164. Antimicrobial Resistance in Campylobacter Species (2018.01.001).
- Jung-Whan Chon , Kun-Ho Seo1, Binn Kim , Dongkwan Jeong , and Kwang-Young Song, 1KU Center for Food Safety and Dept. of Public Health, Korea. : September 21, 2020.
- İlhan, Z., Ekin, İ.H. and Gülaydın, O; Department of Microbiology Turkey,; Determination of Campylobacter fetus subsp. fetus and Campylobacter jejuni in Aborted Sheep Fetuses by Multiplex PCR Assay; Vol. 76 (4) December 2021.
- Andrew D. Sails, Andrew J. Fox, Frederick J. Bolton, David R. A. Wareing, Preston Public Health Laboratory and Department of Biological Sciences, United Kingdom ,A Real-Time PCR Assay for the Detection of Campylobacter jejuni in Food . 11 December 2002, Vol. 69, No. 3.
- Atif Elbrissi & Y. A. Sabeil & Khalda A. Khalifa & Khalid Enan1& Osama M. Khair & A. M. El Hussein.: 4 February 2017; Isolation, identification and differentiation of Campylobacter spp. using multiplex PCR assay from goats. DOI 10.1007/s11250-017-1231-x.
- Jaap A. Wagenaar, Marcel A. P. van Bergen, Martin J. Blaser, Robert V. Tauxe, Diane G. Newell, and Jos P. M. van Putten, 18 February 2014. Campylobacter fetus Infections in Humans. Department of Medicine, New York University School of Medicine, New York. DOI: 10.1093/Cid/ciu085.
- Isabelle Truyers, Tim Luke , David Wilson and Neil Sargison. Diagnosis and management of venereal campylobacteriosis in beef cattle. Truyers et al. BMC Veterinary Research 2014.
- María Andrea Fiorentino , Micaela Stazionati , Yanina Hecker , Claudia Morsella , Germán Cantón , Hernán Romero Harry , Alejandra V. Velilla , Lucía Gallo Vaulet , Marcelo Rodríguez Fermepin, Daniel O. Bedotti , November 2017. Campylobacter fetus subsp. fetus ovine abortion outbreak in Argentina, REDVET – – ISSN 1695-7504.
- H.M. NAM, V. SRINIVASAN, S.E. MURINDA, and S.P. OLIVER, FOODBORNE PATHOGENS AND DISEASE Volume 2, Number 2, 2005, Detection of Campylobacter jejuni Using SYBR Green Real-Time Polymerase Chain Reaction.
- S HUM, K QUINN, J BRUNNER and SLW ON; Aust Vet J 1997;75:827-831; Evaluation of a PCR assay for identification and differentiation of Campylobacter; Aust Vet J Vol 75, No 11, November 1997.
- Evelyne Gue´ vremont,1 Lisyanne Lamoureux,1 Catherine B. Loubier,1,2 Se´ bastien Villeneuve,1 and Jocelyn Dubuc FOODBORNE PATHOGENS AND DISEASE Volume 11, Number 5, 2014, Detection and Characterization of Campylobacter spp. From Cattle Herds in Quebec, Canada.
- Jae-UK An, Hungwui Ho, Jonghyun Kim, Woo-Hyun Kim, Junhyung Kim , Soomin Lee, Seung-Hyun Mun, Jae-Ho Guk, Sahyun Hong and Seongbeom cho..Epidemiological and molecular characterization of campylobacter jejuni.18 December 2018.
- Jaap A. Wagenaar, Marcel A. P. van Bergen, Martin J. Blaser, Robert V. Tauxe, Diane G. Newell, and Jos P. M. van Putten, 18 February 2014. Campylobacter fetus Infections in Humans. Department of Medicine, New York University School of Medicine, New York. DOI: 10.1093/Cid/ciu085.
- Jones et.al;1931,Veron and Chatelain ,1973 ;Campylobacter jejuni.
- Anna-Delia Knipper, Carolina Plaza-Rodríguez, Matthias Filter, Imke F. Wulsten, Kerstin Sting , Tasja Crease; Modeling the survival of Campylobacter jejuni in raw milk:18 June 2023.
- Honsheng Huang and Manuel Mariano Garcia, Isolation of Campylobacter from Food and Food-Related Environment; Microbiology and Food Safety, Ottawa, Canada, National Academy of Science and Technology, Manila, Philippines.
- S. M. Lutful Kabir, Most. Mostary Lubna, Md. Mehedul Islam, A. K. M. Ziaul Haque, Sucharit Basu Neogi, Shinji Yamasaki,: Department of Microbiology and Hygiene, Bangladesh Agricultural University, Japan. , molecular identification and antimicrobial resistance patterns of Campylobacter; Veterinary Science Development 2018; volume 8:7838.
- Generunner.net. 2022. Gene Runner. [online] Available at: <http://www.generunner.net/> [Accessed 16 May 2022].
- Bisma, G., Sabia, Q., Amin, K., Ahmad, W., Nabi, M., Ahmad, M., Isfaqul, H., Aasim, H., Ali, R., Shafkat Majeed, K., Rafia, M. and Shafi, S., 2018. RFLP analysis of flagellin (<i>Fla</i>) gene of <i>Campylobacter jejuni</i> from ovines of Kashmir, India. Journal of Food Safety, 38(5), p.e12509.doi: 10.1111/jfs.12509.