
Causes and Sites of Intra-Abdominal Abscesses at Moi Teaching and Referral Hospital.
- Michelle Nyawira Clay
- Loice Sitienei
- Cornelius Kipchirchir
- 2344-2355
- Mar 8, 2025
- Education
Causes and Sites of Intra-Abdominal Abscesses at Moi Teaching and Referral Hospital.
Michelle Nyawira Clay*, Loice Sitienei, Cornelius Kipchirchir
Department of Radiology and Imaging. Moi University School of Medicine, Eldoret, Kenya.
*Corresponding Author
DOI: https://dx.doi.org/10.47772/IJRISS.2025.9020184
Received: 12 March 2023; Accepted: 20 March 2023; Published: 10 March 2025
ABSTRACT
Background: Intra-abdominal abscesses are a major contributor to morbidity and mortality around the world. More so in developing countries like Kenya where diagnosis and management are usually carried out late due to factors that include gender, level of education and long waiting time for specialized treatment. In the past and even currently, most of the Intra-abdominal abscesses (IAA) are treated via open surgery. However, with the age of Interventional Radiology, IAA are managed faster, and with better clinical and radiological outcomes. It is for these reasons that the role of Interventional Radiology needs to be assessed to see how better we can assist these patients.
Objective: To determine the causative mechanisms of intra-abdominal abscesses at Moi Teaching and Referral Hospital.
Methods: This was a census, a prospective study conducted among 39 patients scheduled for percutaneous catheter drainage from January 2020 to December 2020. The study population was all patients who had confirmed intra-abdominal abscess in the outpatient department and in the medical and surgical wards, referred to the Interventional Radiology section of the Radiology & Imaging Department. A data collection form was used to record the demographics, causative mechanisms, radiological findings, microbiological features, clinical features and complication findings. The IAA were drained by the consultant radiologist under ultrasound guidance using a 3.5-5MHZ curvilinear transducer of Mindray M7. Data was extracted from the patients’ records and there after presented in form of tables, diagrams and prose.
Results: The median age of patients was 40 (IQR 25, 48) years. The proportion of males was slightly higher (56.4%) compared to females (43.6%). Most (38.5%) of the IAA were complications following surgery; followed by trauma (25.6%) and cancer (23.1%). Majority (30.8%) of these IAA were in the right lower quadrant, sub-phrenic constituted 17.9% and psoas represented 12.8% of the sites. Out of the 39 patients included in the study, 28(71.8%) reported to have procedural complications. Of these 28, 26(92.9%) had minor complications that requires no therapy(Level A), 1(3.6%) had complications that resulted in hospitalization (Level C and D) while another 1(3.6%) had major complications that resulted in permanent change of the percutaneous catheter(Level E). Majority (88.5%) of those who had minor complication complained of pain, 1(3.8%) had a leak requiring no intervention while another 1 (3.8%) had fever post procedural.
Conclusions: The most common causative mechanism of IAA was as complications following surgery. Clinically most of the patients complained of abdominal pains. Radiologically, majority of the IAA contained purely fluid material. Only 1 of the patients had a major complication.
Keywords: Intra-abdominal abscesses: MTRH
INTRODUCTION
Intra-abdominal abscess (IAA) is an intra-abdominal collection of pus or infected material usually due to a localized infection inside the peritoneal cavity. It is usually surrounded by inflamed tissue. It can involve any intra-abdominal organ or can be located freely within the abdominal or pelvic cavities. The eight functional compartments in the peritoneal cavity where an IAA abscess may develop include: the pelvis, right paracolic gutter, left paracolic gutter, right infra diaphragmatic space, left infra diaphragmatic space, lesser sac, hepatorenal space (Morrison space) and the interloop spaces between small intestine loops. (Saber, Alan A, 2018). In relation to intra-abdominal collections, intra-abdominal spaces are separate compartments within the peritoneal cavity, compartmentalized by various peritoneal ligaments and their attachments.
Most abscesses are postoperative, because of acute inflammatory abdominal condition like cholecystitis, appendicitis, diverticulitis with or without perforation, due to associated inflammatory bowel disease, due to trauma, or due to tuberculosis.
Intra-abdominal sepsis most frequently follows penetrating or blunt abdominal trauma or perforated appendicitis or diverticulitis. The initial leakage of the endogenous gastrointestinal microflora into the peritoneal cavity results in peritonitis and secondary septicemia, which is frequently followed by localized intra-abdominal abscess. These infections are most frequently polymicrobial and relate directly to the unique endogenous microflora at the various levels of the gastrointestinal tract. The treatment of intra-abdominal sepsis is primarily centered around prompt, appropriate surgical intervention. Parenterally administered antibiotics are also required to decrease the chance of local bacterial infection or septicemia (Nichols, 1986).
Patient presenting symptoms are an important aspect in diagnosis and treatment of an IAA. The most common presenting symptoms for IAA have been shown to be pyrexia in 39 (97%), abdominal tenderness in 32 (80%), guarding in 1 (2.5%) and abdominal mass in 3 (7.5%). (Saber, Alan A, 2018). However, the clinical presentation can be quite variable.
Abscesses occurred most commonly in the subphrenic space, pelvis, or subhepatic space. (Fry et al., 1980). A study done on the improved localization and survival of patients with IAA showed that of 100 patients analyzed in regards to etiology, abscesses developed in 71% of these patients as a result of spontaneous intraabdominal disease, and in 29% as a complication of operation or procedures.(Saini et al., 1983). Intra-abdominal infections differ from other infections through the broad variety in causes and severity of the infection, the etiology of which is often polymicrobial, the microbiological results that are difficult to interpret.(Blot & De Waele, 2005). With the age of laparoscopic surgery, IAA have become more common with studies showing that there is a significant increase in the incidence of postoperative intra-abdominal abscess with perforated appendicitis after laparoscopic compared with open appendectomy in pediatric patients (Krisher et al., 2001). Laparoscopic appendectomy for perforated appendicitis is associated with a higher rate of postoperative intra-abdominal abscess formation without the benefit of a shortened hospital stay (Paik et al., 1997).
Intra-abdominal sepsis most frequently follows penetrating or blunt abdominal trauma or perforated appendicitis or diverticulitis. The initial leakage of the endogenous gastrointestinal microflora into the peritoneal cavity results in peritonitis and secondary septicemia, which is frequently followed by localized intra-abdominal abscess. These infections are most frequently polymicrobial and relate directly to the unique endogenous microflora at the various levels of the gastrointestinal tract. The treatment of intra-abdominal sepsis is primarily centered around prompt, appropriate surgical intervention. Parenterally administered antibiotics are also required to decrease the chance of local bacterial infection or septicemia (Nichols, 1986).
Diagnosis is made majorly using ultrasound, but CT has also been used effectively in the diagnosis and management of IAA. Ultrasonic scanning was used to examine 102 patients suspected of having a postoperative intra-abdominal abscess. An intra-abdominal fluid collect ion was demonstrated in 16 patients; in all 16 the diagnosis was confirmed by operation or necropsy (Maklad et al., 1974).
Percutaneous catheter drainage of intra-abdominal abscesses currently is a well-established technique. Adequate drainage documented by pelvic computerized tomography scans and follow-up confirmed satisfactory long-term results.(Dov et al., 1986). Percutaneous CT-guided abscess drainage is an effective method for treating intra-abdominal abscess and should be considered as the treatment of choice in patients with localized intra-abdominal abscess without signs of generalized peritonitis (Khurrum Baig et al., 2002)..
Subphrenic and other upper abdominal abscesses continue to be associated with high mortality, even in today’s era of broad-spectrum antibiotics and sophisticated surgical techniques. Conventional radiography also remains an effective method in the initial detection of upper abdominal abscesses (Connell et al., 1980).
(Krisher et al., 2001)(Paik et al., 1997)In IAA after penetrating abdominal injury, over 80 percent of penetrating wounds leading to abscesses occurred in the upper quadrants, and common risk factors included multiple intra-abdominal solid organ injuries requiring open drainage, coupled with gastrointestinal tract perforation.
Table 1: Location of Abscess on Diagnostic Imaging Study
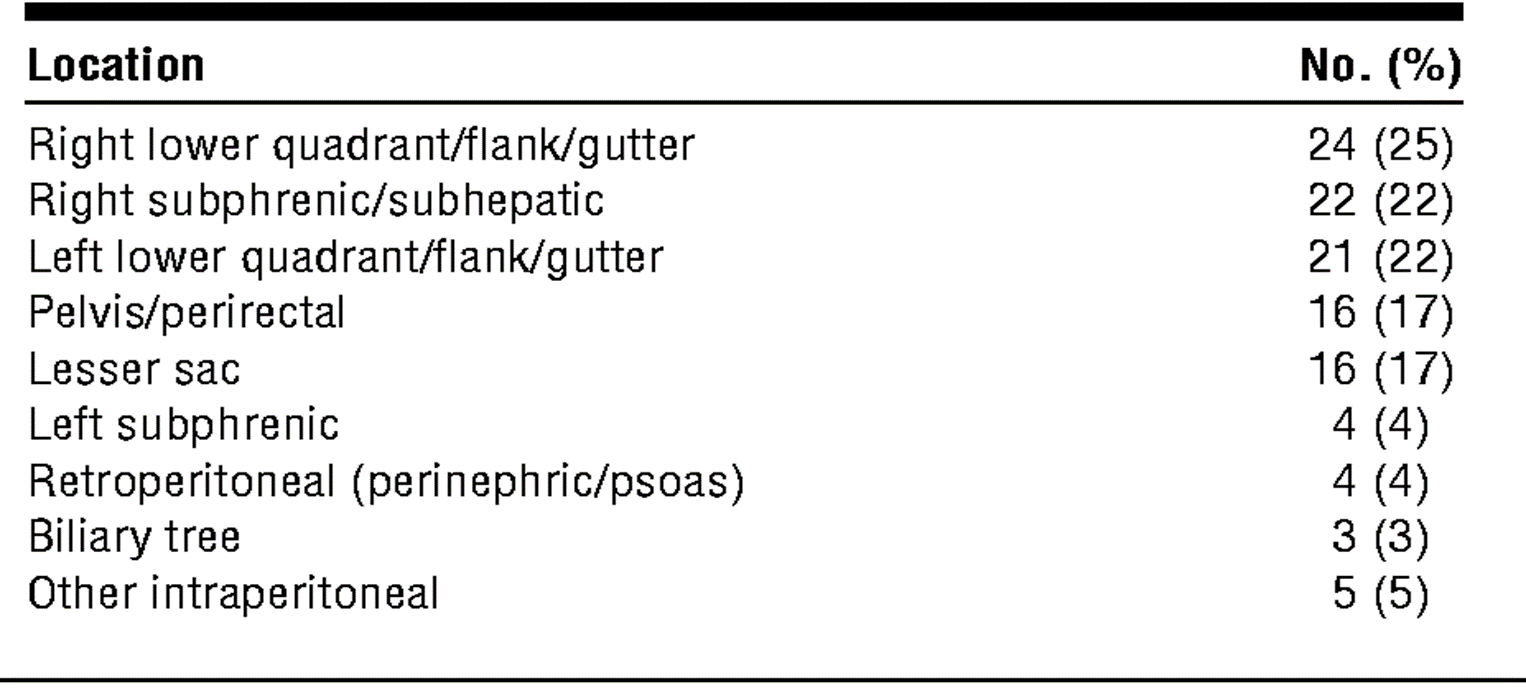
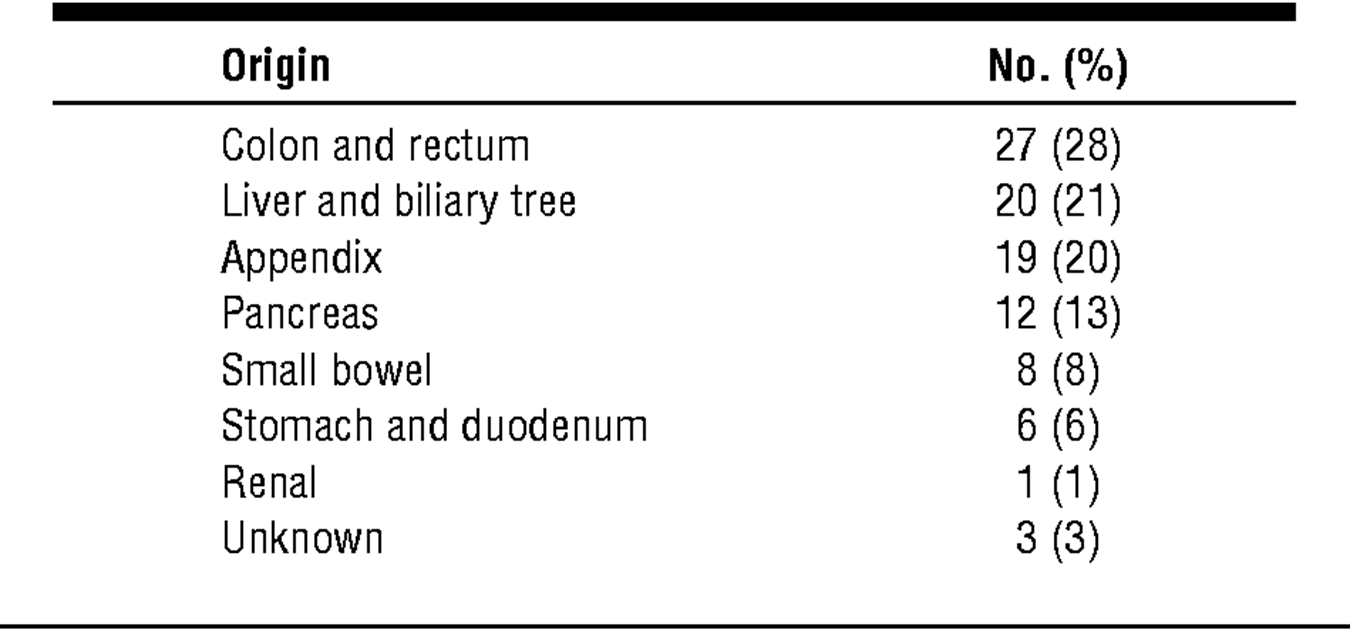
Table 2: Origin of Intra-abdominal Abscesses
(Cinat et al., 2002)
Intra-abdominal abscesses are a major contributor to morbidity and mortality around the world. Mortality rate in cases of untreated IAA may be as high as 80% to 100%. (Ferrucci Jr & vanSonnenberg, 1981) Early diagnosis and management is therefore crucial in the survival of these patients. Percutaneous Catheter Drainage is a mode of management of IAAs where contents of infected collections are syphoned out under either ultrasonography, computed tomography or fluoroscopic guidance; using tubes and catheters. Successful cure rates of up to 86% have been documented (Grainger & Allison’s Diagnostic Radiology 5th Ed 2008). There exists little information on the causes and complications of percutaneous drainage of IAA in Africa and therefore this study will be crucial in bridging this gap. In the past and even currently, most of the IAA are treated via open surgery. Utilization of PCD is low. We aim to shift our mode of management from open surgery to PCD especially for stable patients. Successful abscess resolution after percutaneous drainage has been shown to be as high as 79 percent even in older patients (Malangoni et al., 1990).with a different study showing success rates of as high as 90.8%. (vanSonnenberg et al., 1984a) with an average of about 70-93% success rate. (Schechter et al., 1994a)However, with improvement in our health systems and training, advancement in imaging and interventional radiology modalities, IAA can now be managed effectively with less invasive techniques.
Study Objective: To assess the causative mechanisms and locations of intra-abdominal abscesses of patients at Moi Teaching and Referral Hospital.
METHODOLOGY
Study Site: The study was conducted at the Moi Teaching and Referral hospital, radiology and imaging department, in the interventional radiology room.
Study design: This was a census, a prospective study and was carried out for a period of one year.
Study Population: The study ran for a period of 12 months and included all patients with intra-abdominal abscesses in surgery, medical and interventional radiology department.
Sampling Method: Census method was used as the number of patients with intra-abdominal abscesses who undergo percutaneous drainage in MTRH yearly is approximately 50. Therefore, all patients who underwent percutaneous drainage due to IAA between Jan to Dec 2020 were included in the study to describe their indication and outcomes.
Sampling technique: Consecutive sampling was used to recruit participants into the study.
Study procedure
Patients who showed signs and symptoms of IAA and who required drainage from the interventional radiology room were screened using ultrasonography by the principal investigator. Confirmation on presence of the abscess with correlation of the history provided by the patient was done by the interventional radiologist the probable etiology identified with the help of the history provided for by the patient. The diagnosis made was used for classification. All those with confirmed IAA were recruited into the study and consent sought. All these patients with confirmed IAAs were booked and billed prior to recruitment into the study as per the hospital protocol for the charges of the procedure including waiving for inpatients. Information on the age and sex at the time of procedure was also obtained. All the patients’ files were also reviewed. For those who had a CT scan done as a mode of investigation prior to diagnosis of the procedure, their reports were assessed by the principal investigator and the interventional radiologist and reviewed to confirm the diagnosis and to classify the location of the abscesses. Patients were assessed for any contraindications which included uncorrected coagulopathy, clinical instability and lack of safe access to a collection. All PCD fixation were done by the interventional radiologist assisted by the principal investigator. Treatment was then instilled via percutaneous drainage in accordance to the guidelines after complete diagnostic evaluation by the interventional radiologist that included confirmation via the clinical symptoms and imaging confirmation via ultrasonography.(Radiology, n.d.) and criteria for consideration included, a well-defined abscess cavity, a safe percutaneous route, concurring surgical consultation and immediate operative capability.(Gerzof et al., 1981).The principal investigator assisted in all the patients who had PCD fixation for IAAs recruited in the study. Under local anesthesia and discretionary premedication, a 4 mm incision was made and then widened by (Gerzof et al., 1981)Technique for PCD was either done via the tandem trochar method (One step technique) or the Seldinger technique (Two step) for deep IAAs. One step technique was done for superficial collections and small-sized drains while the seldinger technique was used following diagnostic aspiration performed under US guidance; (Radiology, n.d.) however the trocar technique has been advocated for endocavitary drain placement to avoid the risk of loss of access during the process of serial dilation.(Lorenz & Thomas, 2006a)The exact cutaneous entry site and proposed catheter route were meticulously planned prior to needling and were based on the size, location, and anatomic relation of the abscess to surrounding structures as shown by ultrasound scan. The depth for needle aspiration was the shortest distance from the entry site to the near wall of the abscess to avoid perforation of the far wall.(Gerzof et al., 1981)A sample of the aspirate from each patient was collected, in a sample bottle, labelled and taken to the lab together with a lab request form for gram stain and culturefor evaluation. A successful procedure was defined as one that resulted in a comfortable patient leaving the interventional radiology department with a drained abscess and the drain catheter still connected (Radiology, n.d.)and that there was improvement of clinical wellbeing of the patient, and reduction of the size of the cavity on repeat imaging. (John A. Kaufman, n.d.)A successful percutaneous drainage was defined as one that resulted in the complete resolution of both symptoms and the abscess collection. Postoperative hospital stay was calculated using the dates of the PCD and the date of discharge. As per the department protocol all patients were required to present to the department the following day for review and similarly on day 3. In-hospital follow-up was essential after catheter placement, as adjustments in catheter position and catheter number are occasionally required to ensure clinical improvement in the patient’s condition. The timing of catheter removal was based on the clinical condition of the patient and the daily output from the catheter.(Maher et al., 2002). The catheter was removed when there was improvement in clinical well-being of the patient and resumption of appetite; when there was defervescence and normalization of white cell count’ when the catheter drainage was <15 mL per day and when there was disappearance or reduction in size of collection on repeat imaging.
Patient Preparation
Prior to percutaneous drainage, all patients were prepared by carrying out a coagulation profile, a triple serology and a full hemogram. In the wake of Covid 19 a Covid 19 PCR test was included as screening tool for all patients prior to the procedure. These are part of the requirements for all patients prior to carrying out PCD.
The coagulation screen included prothrombin time and INR. PT had to be more than four seconds and the International Normalized Ratio had to be less than 1.5. This was done to avoid or anticipate any complications that may occur during the procedure. Any patient with deranged factors was deferred until stable depending on the lab findings.
It was recommended that broad- spectrum antibiotics be administered to the patients at least one hour prior to the drainage.
If the patient required sedation mostly children, the patient was asked to fast for at least eight hours prior to the procedure. However, sedation was not carried out for majority of the patients in the study. The procedure was done under local anesthesia (2% lignocaine) for all patients including the patients who were sedated to assist with pain relief after the procedure.
After the procedure, four hours of observation was recommended to assess for complications. Immediate complications were assessed at this stage. The patients were then required to be reviewed after 24 hours and on day 3 for possible discharge. Follow up for complications was however done by the principal investigator for up to a week via phone consultation. The cost of this was incurred by the principal investigator.
Technique
Two techniques were used.
Tandem Trochar Method (commonest)
Seldinger Technique
For the Tandem trochar method, it relied on the placement of a catheter containing a hollow stiffener and a diamond pointed stylet, parallel to a guide needle into a collection. Trochar catheters are available from 8 to 16Fr in size and this range of sized catheters were what was used to drain the IAAs. The interventional radiologist used a hydrophilic coated ultra-thane catheter with a locking loop for image-guided drainage. The distance from the skin surface to the abscess was measured and a 18G guide needle of appropriate length chosen. The portion of the needle outside the skin needed to be long enough to guide the trajectory of the catheter. Following cleansing and local anesthetic administration, the catheter was placed through the skin into the collection and a sample obtained for culture. This sample also allowed assessment of the viscosity of the collection, but the collection was not aspirated further until the catheter was placed appropriately. A 10–12Fr catheter was usually necessary if the contents were frank pus; an 8–10Fr catheter was adequate for less viscous fluid. The distance from the skin to the contents of the collection was marked on the catheter. Following a skin incision and tissue separation adjacent to the guide needle, the catheter was introduced parallel to the guide needle, to the level of the mark on the catheter. The catheter was then advanced over the stiffener or the stiffener withdrawn, and the retention pigtail formed.
Once adequate catheter position was confirmed, the contents of the collection were evacuated, the catheter was secured to the skin with an adhesive device and a drainage bag was attached. Catheter irrigation at the time of abscess drainage using normal saline was done to increase drainage yield, disrupt adhesions and improve healing time. However, the volume of normal saline injected didn’t exceed that of the fluid drained from the collection to prevent cavity distension and reduce the risk of bacteremia. (Grainger & Allison’s Diagnostic Radiology 5th Ed 2008, n.d.-b). The mean duration of catheter drainage was about three days (vanSonnenberg et al., 1982).
For the Seldinger technique, this allowed more controlled catheter placement, especially if there was high risk of catheter transgression of the posterior wall of a collection and facilitated better drainage of large multiloculated collections by placement of a multi-sidehole catheter.
A 19G ultrathin needle containing a stylet or a sheathed needle was initially placed into the collection. An 0.035-inch guidewire was advanced through the needle or sheath and, once adequate positioning was confirmed, the tract was serially dilated. Ultrasound-guided catheter insertion was performed under direct guidance following skin preparation. A guide needle was not necessary unless one wished to sample contents of the collection to assess consistency before choosing the catheter size. (Grainger & Allison’s Diagnostic Radiology 5th Ed 2008, n.d.-a)
For both techniques the trochar and Seldinger techniques, drainage catheters were flushed with normal saline every 8–12 h to maintain catheter patency and optimize drainage. A flush volume of 5 millimeters towards the patient and 5 millimeters towards the drainage bag via a three-way stopcock is normally sufficient unless a collection is very small or very large. Daily catheter outputs were monitored, and the contents of the drainage bag noted. Catheter removal was considered in a well patient when daily outputs were low, normally on the order of 10 millimeters or less per day or when any if present associated fistulas had closed. Before catheter removal it was necessary to confirm complete drainage of the collection by CT or ultrasound imaging and confirm that the cavity had collapsed around the catheter and that there was no fistula present by fluoroscopic-guided injection. Catheter removal at this stage was followed by complete collapse of the cavity. (Grainger & Allison’s Diagnostic Radiology 5th Ed 2008, n.d.-a). Follow up was done, abscess features and the clinical status were recorded for the patients before and after the procedure
Ethical Considerations
The study proposal was sent to Moi University/ MTRH Institutional Research and Ethics Committee (IREC) for review and approval. Permission was sought from the management of MTRH for the study to be carried out at the facility. Informed consent was sought directly from the respondents undergoing the procedure.
Consent: Written consent was sought from patients above 18 years undergoing the procedure while for those below 18 years of age, consent was sought from their parents or guardian or legally accepted representative. Participation in the study was voluntary and the participants were free to withdraw at any time. Confidentiality of the respondents’ information was maintained, and codes were used instead of the respondents’ names to protect their identity.
Confidentiality: The information provided by the respondents and that obtained from their medical records was kept confidential and was stored in a lockable cabinet. The data was entered into a password protected computer and using codes in place of individual names.
Benefits: There was no direct monetary benefits in the participation of the study. Respondents could withdraw from the study at any time with no need to seek prior authorization or consequences for doing so.
Risks: No major risks existed as a result of participating in the study except the time spent in participation of the study.
RESULTS
Patients’ demographic characteristics
Table 1: Patients’ demographic characteristics.
| Variable | Category | Frequency | Percentage |
| Age | Median (IQR) | 40 (25-48) | |
| Gender | Male | 22 | 56.4 |
| Female | 17 | 43.6 | |
| County of residence | Uasin Gishu | 21 | 53.8 |
| Siaya | 3 | 7.7 | |
| Nandi | 2 | 5.1 | |
| Trans Nzoia | 2 | 5.1 | |
| Turkana | 2 | 5.1 | |
| Others | 9 | 23.1 |
The age of patients ranged from 4 to 83 years with a median age of 40 (IQR 25, 48) years. Where the proportion of males was slightly higher (56.4%) compared to females (43.6%). Slightly above half (53.8%) of the patients were residents of Uasin Gishu county while the bordering counties (Elgeyo Marakwet, Nandi, Kakamega and Trans Nzoia Counties contributed 6(15.4%) of the respondents.
Table 2: Causative mechanisms
| Variable | Category | Frequency | Percentage |
| Etiology | Postoperative | 15 | 38.5 |
| Trauma | 10 | 25.6 | |
| Cancer | 9 | 23.1 | |
| Gangrenous cholecystitis | 2 | 5.1 | |
| Pancreatitis | 2 | 5.1 | |
| TB | 2 | 5.1 | |
| Perforation of small bowel | 1 | 2.6 | |
| Perforated appendicitis | 1 | 2.6 | |
| Mesenteric ischemia | 1 | 2.6 |
Most (38.5%) of the patients with IAA had them as complications following surgery. followed by trauma (25.6%) and cancer (23.1%); these three etiologies contributing to 87.2% of the total (n=39) cases of IAA included in the study.
Table 3: Radiological features
| Variable | Category | Frequency | Percentage |
| Location | Right lower quadrant | 12 | 30.8 |
| Sub-phrenic | 7 | 17.9 | |
| Psoas | 5 | 12.8 | |
| Peri splenic | 5 | 12.8 | |
| Left iliac fossa | 2 | 5.1 | |
| Anterior abdominal wall | 1 | 2.6 | |
| Supravesical | 1 | 2.6 | |
| Hepatorenal | 1 | 2.6 | |
| Inguinal | 1 | 2.6 | |
| Lesser sac | 1 | 2.6 | |
| Para-vertebral | 1 | 2.6 | |
| Peri-pancreatic | 1 | 2.6 | |
| Prevesicle | 1 | 2.6 |
Majority (30.8%) of these IAA were located in the right lower quadrant, sub-phrenic constituted 17.9% and psoas represented 12.8% of the sites.
DISCUSSION
Introduction
Intra-abdominal abscesses are a major contributor to morbidity and mortality around the world. More so in developing countries like Kenya where diagnosis and management are usually carried out late due to factors that include gender, level of education and long waiting time for specialized treatment. In the past and even currently, most of the Intra-abdominal abscesses (IAA) are treated via open surgery. However, with the age of Interventional Radiology, IAA are managed faster, and with better clinical and radiological outcomes.
Causative mechanisms and locations of intra-abdominal abscesses.
Most (38.5%) of the patients with IAA had them as complications following surgery followed by trauma (25.6%) and cancer (23.1%); these three etiologies contributing to 87.2% of the total (n=39) cases of IAA included in the study.
This corresponded well to a study by Stephen G. Gerzof et al that found majority (67%) of the patients had IAA formation due to surgery (Gerzof et al., 1981). Other studies also showed that most of the IAA were due to surgery including Cinat et al (Cinat et al., 2002)(Yamaguchi et al., 2004) and (Connell et al., 1980). Cinat et. al., demonstrated post-surgical as the most causative mechanism with a mean SD of 22-29 days after operation with majority of the patients showing the abscess on the initialpost-surgical scans and the rest developing the abscesses after the initial scans. Yamaguchi et. al., in his study on patients with Crohn’s disease demonstrated majority of their patients had a positive history of having had surgery prior and the most common reason as to which his patients required surgery prior was stenosis which is common in Crohn’s disease.
One study demonstrated trauma as the commonest cause (Nichols, 1986). Nichole et. al., observed that more than 80% of the abscesses occurred after penetrating abdominal trauma and they therefore demonstrated the major importance of gastrointestinal perforation to postoperative infection. They additionally reported the results of a prospective study of 145 patients who presented with penetrating abdominal trauma & intestinal perforationand they also demonstrated the risk of abscess formation being greater with increasing age, injury to the left colon necessitating colostomy, greater requirements for blood or blood products during surgery and increasing number of organs injured. The difference in this study can be attributed to the fact that the study was geared towards treatment of intraabdominal sepsis as opposed to IAA specifically.
Majority (30.8%) of these IAAs were located in the right lower quadrant, sub-phrenic constituted 17.9% and psoas represented 12.8% of the sites. This corresponded well with a study by W. A. Altemeier which showed majority of the IAA located in the right lower quadrant in the peritoneal cavity. (Altemeier et al., 1973). Altemeier et al., more than half of the abscesses were located in the right lower quadrant followed by the left lower quadrant, pelvis and subphrenic areas. They additionally stated that understanding of these anatomic considerations was important for the recognition and drainage of the abscesse
CONCLUSIONS
Most of the patients with IAA had them as complications following surgery. Clinically most of the patients complained of abdominal pains. Radiologically, only 30% of the IAA were visualized by ultrasound to be hyper vascular. Mild pain was the commonest post procedural complication. Only 1 of the patients had a major complication. Overall success rate of PCD was 96.7%.
RECOMMENDATIONS
Clinical assessment of patients early; especially post-surgical patients to enable early detection of the IAA. Adequate post procedural analgesia with counselling on the expected complications. Percutaneous drainage be considered as one of the first line treatment options for patients with IAAs owing to its high success rate.
CONFLICT OF INTEREST
The authors declare no conflict of interest in this study
REFERENCES
- Abdominal Abscess | Radiology Key. (n.d.). Retrieved April 19, 2022, from https://radiologykey.com/abdominal-abscess-4/
- Altemeier, W. A., Culbertson, W. R., Fullen, W. D., & Shook, C. D. (1973). Intra-abdominal abscesses. The American Journal of Surgery, 125(1), 70–79. https://doi.org/https://doi.org/10.1016/0002-9610(73)90010-X
- Blot, S., & De Waele, J. J. (2005). Critical Issues in the Clinical Management of Complicated Intra-Abdominal Infections. Drugs, 65(12), 1611–1620. https://doi.org/10.2165/00003495-200565120-00002
- Cinat, M. E., Wilson, S. E., & Din, A. M. (2002). Determinants for Successful Percutaneous Image-Guided Drainage of Intra-abdominal Abscess. JAMA Surgery, 137(7), 845–849. https://doi.org/10.1001/archsurg.137.7.845
- Civardi, G., Di Candio, G., Giorgio, A., Goletti, O., Ceragioli, T., Filice, C., Caremani, M., & Buscarini, L. (1998). Ultrasound guided percutaneous drainage of abdominal abscesses in the hands of the clinician: a multicenter Italian study. European Journal of Ultrasound, 8(2), 91–99. https://doi.org/10.1016/S0929-8266(98)00059-7
- Connell, T. R., Stephens, D. H., Carlson, H. C., & Brown, M. L. (1980). Upper abdominal abscess: a continuing and deadly problem. American Journal of Roentgenology, 134(4), 759–765. https://doi.org/10.2214/ajr.134.4.759
- Dov, K., David, L., & K.T., L. J. (1986). Percutaneous Drainage of Prostatic Abscesses. Journal of Urology, 135(6), 1259–1260. https://doi.org/10.1016/S0022-5347(17)46064-2
- Dr Craig Hacking and Dr Prashant Mudgal et al. (n.d.). Peritoneal Spaces.
- Dr. Vladimir, V. F. (1967). 済無No Title No Title No Title. In Gastronomía ecuatoriana y turismo local. (Vol. 1, Issue 69).
- Ferrucci Jr, J. T., & vanSonnenberg, E. (1981). Intra-abdominal Abscess: Radiological Diagnosis and Treatment. JAMA, 246(23), 2728–2733. https://doi.org/10.1001/jama.1981.03320230052028
- Ferrucci, J. T., & vanSonnenberg, E. (1981). Intra-abdominal Abscess: Radiological Diagnosis and Treatment. JAMA, 246(23), 2728–2733. https://doi.org/10.1001/JAMA.1981.03320230052028
- Friday, R. O., Barriga, P., & Crummy, A. B. (1975). Detection and Localization of Intra-abdominal Abscesses by Diagnostic Ultrasound. Archives of Surgery, 110(3), 335–337. https://doi.org/10.1001/ARCHSURG.1975.01360090105022
- Fry, D. E., Garrison, R. N., Heitsch, R. C., Calhoun, K., & Polk Jr., H. C. (1980). Determinants of death in patients with intraabdominal abscess. Surgery, 88(4), 517–523. https://doi.org/10.5555/uri:pii:0039606080901269
- Gerzof, S. G., Robbins, A. H., Johnson, W. C., Birkett, D. H., & Nabseth, D. C. (1981). Percutaneous Catheter Drainage of Abdominal Abscesses. New England Journal of Medicine, 305(12), 653–657. https://doi.org/10.1056/NEJM198109173051201
- Global Guidelines for the Prevention of Surgical Site Infection. (2016).
- Goletti, O., Lippolis, P. V, Chiarugi, M., Ghiselli, G., De Negri2, F., Conte, M., Ceragioli, T., & Cavina, E. (2005). Percutaneous ultrasound-guided drainage of intra-abdominal abscesses. British Journal of Surgery, 80(3), 336–339. https://doi.org/10.1002/bjs.1800800323
- Grainger & Allison’s Diagnostic Radiology 5th ed 2008. (n.d.-a).
- Grainger & Allison’s Diagnostic Radiology 5th ed 2008. (n.d.-b).
- Hemming, A., Davis, N. L., & Robins, R. E. (1991). Surgical versus percutaneous drainage of intra-abdominal abscesses. The American Journal of Surgery, 161(5), 593–595. https://doi.org/https://doi.org/10.1016/0002-9610(91)90907-U
- Khurrum Baig, M., Hua Zhao, R., Batista, O., Uriburu, J. P., Singh, J. J., Weiss, E. G., Nogueras, J. J., & Wexner, S. D. (2002). Percutaneous postoperative intra-abdominal abscess drainage after elective colorectal surgery. Techniques in Coloproctology, 6(3), 159–164. https://doi.org/10.1007/s101510200036
- Koetser, I. C. J., de Vries, E. N., van Delden, O. M., Smorenburg, S. M., Boermeester, M. A., & van Lienden, K. P. (2013). A Checklist to Improve Patient Safety in Interventional Radiology. CardioVascular and Interventional Radiology, 36(2), 312–319. https://doi.org/10.1007/s00270-012-0395-z
- Krisher, S. L., Browne, A., Dibbins, A., Tkacz, N., & Curci, M. (2001). Intra-abdominal Abscess After Laparoscopic Appendectomy for Perforated Appendicitis. JAMA Surgery, 136(4), 438–441. https://doi.org/10.1001/archsurg.136.4.438
- Kusel, K., & Hameed, A. (2013). Ultrasound guided percutaneous drainage. Radiopaedia.Org. https://doi.org/10.53347/RID-21172
- Lambiase, R. E., Deyoe, L., Cronan, J. J., & Dorfman, G. S. (1992). Percutaneous drainage of 335 consecutive abscesses: results of primary drainage with 1-year follow-up. Radiology, 184(1), 167–179. https://doi.org/10.1148/radiology.184.1.1376932
- Levin, D. C., Eschelman, D., Parker, L., & Rao, V. M. (2015). Trends in Use of Percutaneous Versus Open Surgical Drainage of Abdominal Abscesses. Journal of the American College of Radiology, 12(12, Part A), 1247–1250. https://doi.org/https://doi.org/10.1016/j.jacr.2015.06.015
- Lorenz, J., & Thomas, J. L. (2006a). Complications of percutaneous fluid drainage. Seminars in Interventional Radiology, 23(2), 194–204. https://doi.org/10.1055/s-2006-941450
- Lorenz, J., & Thomas, J. L. (2006b). Complications of percutaneous fluid drainage. Seminars in Interventional Radiology, 23(2), 194–204. https://doi.org/10.1055/s-2006-941450
- Maher, M. M., Kealey, S., McNamara, A., O’Laoide, R., Gibney, R. G., & Malone, D. E. (2002). Management of Visceral Interventional Radiology Catheters: A Troubleshooting Guide for Interventional Radiologists. RadioGraphics, 22(2), 305–322. https://doi.org/10.1148/radiographics.22.2.g02mr20305
- Maklad, N. F., Doust, B. D., & Baum, J. K. (1974). Ultrasonic Diagnosis of Postoperative Intra-Abdominal Abscess. Radiology, 113(2), 417–422. https://doi.org/10.1148/113.2.417
- Malangoni, M. A., Shumate, C. R., Thomas, H. A., & Richardson, J. D. (1990a). Factors influencing the treatment of intra-abdominal abscesses. The American Journal of Surgery, 159(1), 167–171. https://doi.org/https://doi.org/10.1016/S0002-9610(05)80623-3
- Malangoni, M. A., Shumate, C. R., Thomas, H. A., & Richardson, J. D. (1990b). Factors influencing the treatment of intra-abdominal abscesses. The American Journal of Surgery, 159(1), 167–171. https://doi.org/https://doi.org/10.1016/S0002-9610(05)80623-3
- mtrh. (n.d.). MTRH.
- Nichols, R. L. (1986). Management of intra-abdominal sepsis. The American Journal of Medicine, 80(6, Supplement 2), 204–209. https://doi.org/https://doi.org/10.1016/0002-9343(86)90502-4
- Nisarg Y. Mehta; Eddie L. Copelin II. (n.d.). Abdominal Abscess. Mehta NY, Copelin II EL. Abdominal Abscess. . In: StatPearls [Internet]. Treasure Island (FL): . Available from: Https://Www.Ncbi.Nlm.Nih.Gov/Books/NBK519573/.
- Vascular and interventional radiology: the requisites by John A. Kaufman, Prof Michael J. Lee. Second edition
- Nuernberg, D. (n.d.). Diagnostic and Therapeutic Paracentesis of Free Abdominal Fluid. https://radiologykey.com/diagnostic-and-therapeutic-paracentesis-of-free-abdominal-fluid/#b2a651a880_1
- Paik, P. S., Towson, J. A., Anthone, G. J., Ortega, A. E., Simons, A. J., & Beart, R. W. (1997). Intra-abdominal abscesses following laparoscopic and open appendectomies. Journal of Gastrointestinal Surgery, 1(2), 188–193. https://doi.org/10.1016/S1091-255X(97)80108-4
- Park, J., & Charles, H. W. (2012). Intra-abdominal abscess drainage: interval to surgery. Seminars in Interventional Radiology, 29(4), 311–313. https://doi.org/10.1055/s-0032-1330065
- Radiology, I. (n.d.).
- Ripollés, T., Martínez-Pérez, M. J., Paredes, J. M., Vizuete, J., García-Martínez, E., & Jiménez-Restrepo, D. H. (2013). Contrast-enhanced ultrasound in the differentiation between phlegmon and abscess in crohn’s disease and other abdominal conditions. European Journal of Radiology, 82(10). https://doi.org/10.1016/j.ejrad.2013.05.043
- Saber, Alan A, R. D. L. (2018). Abdominal abscess.
- Saini, S., Kelium, J. M., O’Leary, M. P., O’Donnell, T. F., Tally, F. P., Carter, B., Deterling, R. A., & Curtis, L. E. (1983). Improved localization and survival in patients with intraabdominal abscesses. The American Journal of Surgery, 145(1), 136–142. https://doi.org/https://doi.org/10.1016/0002-9610(83)90180-0
- Sartelli, M., Catena, F., Ansaloni, L., Coccolini, F., Corbella, D., Moore, E. E., Malangoni, M., Velmahos, G., Coimbra, R., Koike, K., Leppaniemi, A., Biffl, W., Balogh, Z., Bendinelli, C., Gupta, S., Kluger, Y., Agresta, F., Saverio, S. Di, Tugnoli, G., … Barnabé, R. (2014). Complicated intra-abdominal infections worldwide: the definitive data of the CIAOW Study. World Journal of Emergency Surgery, 9(1), 37. https://doi.org/10.1186/1749-7922-9-37
- Schechter, S., Eisenstat, T. E., Oliver, G. C., Rubin, R. J., & Salvati, E. P. (1994a). Computerized tomographic scan-guided drainage of intra-abdominal abscesses. Diseases of the Colon & Rectum, 37(10), 984–988. https://doi.org/10.1007/BF02049309
- Schechter, S., Eisenstat, T. E., Oliver, G. C., Rubin, R. J., & Salvati, E. P. (1994b). Computerized tomographic scan-guided drainage of intra-abdominal abscesses. Diseases of the Colon & Rectum, 37(10), 984–988. https://doi.org/10.1007/BF02049309
- The Peritoneum | Boundless Anatomy and Physiology. (n.d.). Retrieved November 26, 2019, from https://courses.lumenlearning.com/boundless-ap/chapter/the-peritoneum/
- The Peritoneum – Visceral – Parietal – TeachMeAnatomy. (n.d.). Retrieved November 26, 2019, from https://teachmeanatomy.info/abdomen/areas/peritoneum/
- Ultrasound for Diverticulitis? | Emory School of Medicine. (n.d.). Retrieved April 25, 2022, from https://med.emory.edu/departments/emergency-medicine/sections/ultrasound/case-of-the-month/abdominal/ultrasound_for_diverticulitis.html
- vanSonnenberg Eric, M. D., Wittich Gerhard R., M. D., Goodacre Brian W., M. D., Casola Giovanna, M. D., & D’Agostino Horacio B., M. D. (2001). Percutaneous Abscess Drainage: Update. World Journal of Surgery, 25(3), 362–369. https://doi.org/10.1007/s002680020386
- vanSonnenberg, E., Ferrucci, J. T., Mueller, P. R., Wittenberg, J., & Simeone, J. F. (1982). Percutaneous drainage of abscesses and fluid collections: technique, results, and applications. Radiology, 142(1), 1–10. https://doi.org/10.1148/radiology.142.1.7053517
- vanSonnenberg, E., Mueller, P. R., & Ferrucci, J. T. (1984a). Percutaneous drainage of 250 abdominal abscesses and fluid collections. Part I: Results, failures, and complications. Radiology, 151(2), 337–341. https://doi.org/10.1148/radiology.151.2.6709901
- vanSonnenberg, E., Mueller, P. R., & Ferrucci, J. T. (1984b). Percutaneous drainage of 250 abdominal abscesses and fluid collections. Part I: Results, failures, and complications. Radiology, 151(2), 337–341. https://doi.org/10.1148/radiology.151.2.6709901
- Wall1, S. D., Fisher, M. R., Amparo, E. G., Hricak, H., & Higgins, C. B. (1985). Magnetic Resonance Imaging in the Evaluation of Abscesses. www.ajronline.org
- What is the Difference Between Intraperitoneal and Retroperitoneal – Pediaa.Com. (n.d.). Retrieved November 26, 2019, from https://pediaa.com/what-is-the-difference-between-intraperitoneal-and-retroperitoneal/
- Yamaguchi, A., Matsui, T., Sakurai, T., Ueki, T., Nakabayashi, S., Yao, T., Futami, K., Arima, S., & Ono, H. (2004). The clinical characteristics and outcome of intraabdominal abscess in Crohn’s disease. Journal of Gastroenterology 2004 39:5, 39(5), 441–448. https://doi.org/10.1007/S00535-003-1317-2