
Adherence to Dialysis Therapy and Associated Factors Among Insured Patients with End Stage Renal Disease Attending Dialysis Centers in Northern Zone of Tanzania
- Cesilia Charles
- Kajiru Kilonzo
- Florida Muro
- Baraka Moshi
- 157-170
- Jun 27, 2024
- Public Health
Adherence to Dialysis Therapy and Associated Factors Among Insured Patients with End Stage Renal Disease Attending Dialysis Centers in Northern Zone of Tanzania
*Cesilia Charles1,Baraka Moshi1,3, Kajiru Kilonzo1,2,3, Florida Muro1,2,3
Institute of Public Health, Kilimanjaro Christian Medical University College (KCMUCo), Kilimanjaro, Tanzania1
Internal Medicine Department Kilimanjaro Christian Medical Centre (KCMC), Kilimanjaro, Tanzania2
Kilimanjaro Clinical Research Institute, Moshi, Tanzania3
*Corresponding authors
DOI : https://dx.doi.org/10.47772/IJRISS.2024.806013
Received: 22 April 2024; Revised: 16 May 2024; Accepted: 21 May 2024; Published: 27 June 2024
ABSTRACT
The aim of the study was to determine adherence to dialysis therapy and associated factors among insured patients with end stage renal disease attending dialysis centers in the Northern zone of Tanzania. It was a hospital based cross-sectional study using both qualitative and quantitative methods of data collection via interviews.
Categorical variables were summarized by frequency and percentage while continuous variables were summarized by mean and standard deviation the factors associated with adherence to dialysis therapy were estimated by multivariable logistic regression and qualitative data were analyzed using thematic analysis, findings with p-value of less than or equal to 0.05 were considered statistically significant. The study revealed that adherence to dialysis therapy was 55% and significant factors associated with adherence were age above 60 years, higher education level, unemployment, more than five (5) years in dialysis, transport unavailability, and high frequency of receiving health information.
Thematic analysis revealed inaccessibility of dialysis services in terms of travel distance, poor roads and financial constraints were factors for non-adherence. While social support, awareness of disease and desire to prolong life were factors for good adherence. Collectively the results seem to indicate that more than half of insured patients with ESRD had good adherence status. Findings from this study recommend the need of strong social support relationship between patients, family members and HCWs in dialysis units.
In addition, health system should Prioritize transport access, road infrastructure, proximity to dialysis centers and ongoing patient education and counseling.
Keywords: Adherence, Dialysis therapy, insured patients, End Stage Renal Disease
INTRODUCTION
End-stage renal disease (ESRD) is a significant public health challenge with varying prevalence across different countries. There are nearly 700,000, 120,000 and 135,000 people with ESRD in the United States (US), United Kingdom (UK) and Europe respectively (Qazi et al., 2018).
Low- and middle-income countries including Sub Saharan Africa have higher rates of end-stage renal disease due to late-stage diagnoses and limited nephrology services, leading to a high demand for dialysis therapy (Mukakarangwa et al., 2018).
In the World Kidney Day platform, Sumaili et al. screened >15,000 adults in Kinshasa, Democratic Republic of Congo and reported that overall prevalence of Chronic Kidney Disease was 12.4% with 0.2% having stage ESRD (Swanepoel et al., 2013). In Tanzania, 7 % of the general population suffer from Chronic Kidney Disease by which 3.5% are ready in ESRD (Mohamedi & Mosha, 2022).
In Africa, only 9 to 16% of ESRD patients have access to dialysis therapy and estimated that this number could double to 5.4 million people by 2030 (Gupta et al., 2021). In contrast to higher- income countries, where around 40% of patients currently access renal replacement services including the dialysis services (Bikbov et al., 2020).
Adherence to dialysis therapy is important for positive clinical outcomes, around 50% of patients with long-term conditions including ESRD exhibit non-adherence to treatment (Kustimah et al., 2019). Adherence to dialysis varies across countries, for example in Japan and Italy adherence was 1% while in United states adherence was to 24 %(Al Salmi et al., 2018).
Also, Nepal reports high adherence (91.9%) may be due to free hemodialysis and social support. In Indonesia, adherence to dialysis therapy was estimated to be 60%, such results were linked with patient satisfaction, self- efficacy, and social support (Agustina et al., 2019; Sapkota et al., 2022).
Despite of not having overall reliable statistic on adherence to dialysis among African population, still patients with ESRD in African countries poorly adhere to dialysis therapy due to limited access to nephrology services and poverty. For example, in Nigeria only 30% of people with ESRD adhere to dialysis therapy while in Zimbabwe 97.3% had low adherence status, poor adherence was linked to socioeconomic status (Mukakarangwa et al., 2018; Timothy, 2022).
In Tanzania, dialysis therapy is becoming more of a concern due to cost in relation to necessity. The price for each dialysis session in Tanzania ranges from USD 120–150 (Furia et al., 2019). Funding for dialysis in Tanzania is through the National Health Insurance Fund (NHIF), initially established to cover public servants and now enrolling members from the private sector (Amu et al.,2018).
NHIF membership is 8% of Tanzania’s population and provides full reimbursement for dialysis services for its members (Durizzo et al., 2022). This signifies that members of this fund have guaranteed access to dialysis and other nephrology services. However, a study conducted at Muhimbili National Hospital (MNH) in Dar es Salaam revealed that only 69% of patients with NHIF had adhered to dialysis therapy (Mohamedi & Mosha, 2022).
These study findings did not take into account factors associated with dialysis adherence among the insured population, also being involving a single institution and different geographical setting limits its generalizability.
Therefore, this study aimed at assessing adherence to dialysis therapy and its associated factors among the insured patients with ESRD attending dialysis centers in the Northern zone of Tanzania.
METHOD
Study area
The study was conducted in two regions in Northern zone of Tanzania, which are Kilimanjaro and Arusha. According to 2022 national census, the population size for Kilimanjaro region is 1,861,934 and that of Arusha is 2,356,255 (Administrative Units Population Distribution Report, n.d).
ESRD prevalence was reported to be 3.5% in the community setting in Northern Tanzania,where hypertension, diabetes and HIV were common diseases in ESRD patients (Stanifer et al., 2015). There are 4 dialysis centers in Kilimanjaro region, these are Kilimanjaro Christian Medical Center attend 60 insured ESRD patients per day, Reyna polyclinic attend 50 patients per day, St Joseph hospital attend 12 patients per day and Faraja hospital attend 6 patients per day.
In Arusha region, there are 5 dialysis centers which are Selian hospital which attend 15 insured ESRD patients per day, NSK hospital attend 50 patients, Orbit polyclinic and diagnostic center attend 10 patients, Moyo Medicare specialized clinic attend 36 and Mt Meru hospital attend 12 patients.
Study design
The study used a hospital based cross sectional study design, employing both quantitative and qualitative methods approaches with data collection conducted between 15th May 2023 to 15 June 2023.
Study population
Thestudyincluded251consentedhealthinsuredpatientsaged18yearsandabovediagnosedwith ESRD and attend dialysis therapy at dialysis centers with in the study area.
All eligible participants were invited to participate in the study and those participants who willingly spared their time for after filling up the questionnaire were purposely selected for qualitative data collection guided by saturation point.
Study Procedures
Before enrollment, the study purpose was explained to participants and those who agreed to participate in the study gave a written consent. Participants who were unable to write and read gave a thumb. Quantitative data was collected using closed-ended questions adopted from validated standard end-stage renal disease adherence questionnaire (ESRD- AQ) (Kim et al., 2010).
The qualitative data were collected using in depth interview directed by an interview guide developed from the literature focusing on social support, desire to prolong life and improved quality of life, transportation difficulties, awareness and knowledge of disease complications, and accessibility of dialysis centers.
Outcome variable
The primary outcome variable was adherence status, which was assessed by attendance of dialysis session without skipping, and the secondary outcome was staying in dialysis session without shortening the time to 10 minutes or more.
Independent variables
The independent variables were socio demographic characteristics such as age, sex, marital status, occupation, and religion, place of residence and level of education, social support, and duration of treatment, prescribed hours to dialysis, presence of other chronic illness, type of transportation used to go to dialysis center and convenient time for dialysis, distance to and from the dialysis unit, frequency of receiving health information, convenient time to dialysis session, difficulties on dialysis and shift of dialysis session.
Qualitative method
Data were collected from 27 participants using in-depth interview guide on their views and experiences regarding adherence to dialysis therapy. Saturation was reached when no new or emerging information was observed.
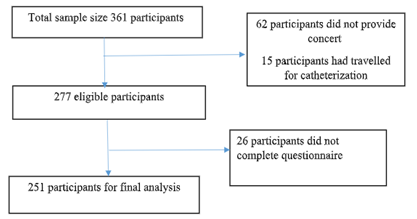
Figure 1: Recruitment outflow
Statistical analysis
Quantitative data analysis was carried out by using STATA version 15 software (StataCorp LP, College Station, USA). The categorical variables summarized and presented in frequency and percentages while for the continuous variables were summarized using Mean and standard deviation (SD) respectively.
The association between categorical variables was assessed using chi square test; the significance association was at P-value ≤ 0.05. In bivariate analysis, each independent variable fitted against response variable at a time, with significant association at P-value of ≤ 0.05. Variables with significant association, clinical importance and those reported in previous literature as factors associated with adherence to dialysis therapy was considered for multivariable binary logistic regression. In multivariable analysis, adjusted OR was reported with the significant association at P-value ≤ 0.05 and its corresponding 95%CI.
Qualitative data were analyzed using thematic analysis where familiarization, coding, interpretation of the findings and summarizing major themes from findings was done. Key themes are presented with using of paraphrase and/or direct quotes to elaborate more.
RESULTS
Of the 277 eligible participants selected to participate in the study between May 2023 to June 2023, 251 (90.6%) completed the questionnaire and were included in the final analysis. Majority were aged above 60, 48.6%, mostly male 169, 67.3%, with 106, 42.2% having primary education.
Moreover, 223, 88.8% being married. Around half lived in urban areas, 116, 53.8% were unemployed, and 123, 49% earned over 540,000 monthly and 121, 48.2% received dialysis for 1 to 5 years.
Table 1: Distribution of the study patients by their sociodemographic characteristics (N = 251)
| Characteristics | Frequency | Percentage |
| Age in years | ||
| Mean (SD) | 59.8 (±11.6) | |
| 18 – 30 | 6 | 2.40% |
| 31 – 40 | 9 | 3.60% |
| 41-50 | 37 | 14.70% |
| 51-60 | 77 | 30.70% |
| Above 60 | 122 | 48.60% |
| Sex | ||
| Male | 169 | 67.30% |
| Female | 82 | 32.70% |
| Marital Status | ||
| Unmarried | 28 | 11.20% |
| Married | 223 | 88.80% |
| Religion | ||
| Christian | 225 | 89.60% |
| Muslim | 24 | 9.60% |
| Others | 2 | 0.80% |
| Education level | ||
| Completed Primary | 106 | 42.20% |
| Completed Secondary | 68 | 27.10% |
| Completed Higher level | 77 | 30.70% |
| Occupation | ||
| Employed | 116 | 46.20% |
| Unemployed/retired | 135 | 53.80% |
| Monthly income level (TZS) | ||
| Less than 135,000 | 47 | 18.70% |
| 135,000 – 270,000 | 29 | 11.60% |
| 270,000 – 540,000 | 52 | 20.70% |
| More than 540,000 | 123 | 49.00% |
| Years in Dialysis | ||
| 3 months -1 year | 88 | 35.60% |
| More than 1 year – 5 years | 121 | 48.20% |
| More than 5 years | 42 | 16.70% |
Of 251 insured patients with ESRD who participated in this study, prevalence of adherence to dialysis therapy was 55% and non-adherence was 45%. In sub analysis, 195 (77.7%) reported to have never missed dialysis session purposely even once in a month while 181(72.1%) never shortened dialysis session on their own initiatives even once in a month (figure 1).
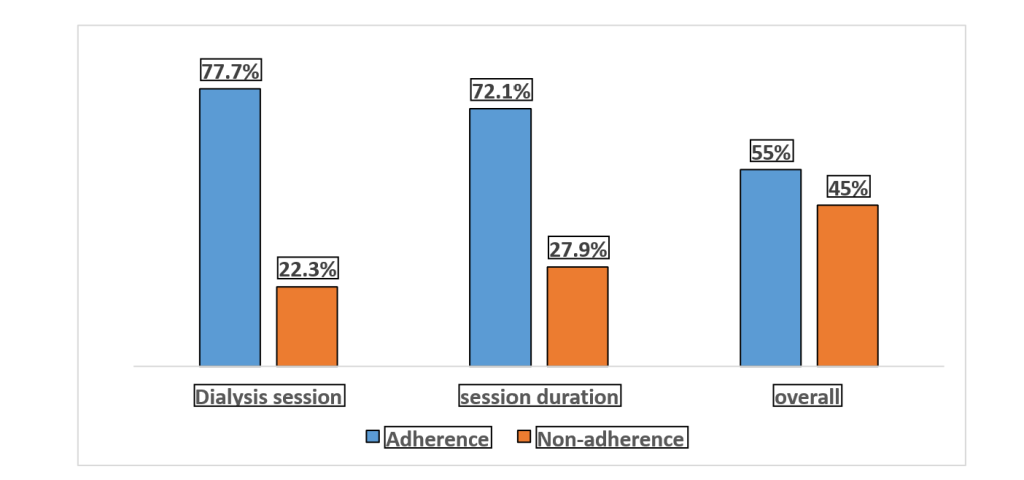
Figure 3. Proportional of insured patients with ESRD adhering to dialysis therapy in Northern zone of Tanzania from May 2023 to June 2023.actor associated with adherence to dialysis session among the insured patients with ESRD
In univariate analysis, the factors associated with adherence to dialysis therapy were age, unemployment; months in dialysis treatment, and frequency of receiving health information were significantly associated with adherence to dialysis therapy.
Participants aged above 60 years had significantly 6 times higher odds of adherence to dialysis session duration compared to those aged between 18 to 30 years (OR: 6.41; 95% CI:1.17, 36.82). Unemployed participants had significantly 2 times higher odds of adherence to dialysis session duration than employed ones (OR: 2.17; 95% CI: 1.24, 3.81). Dialysis treatment for more than 60 years was statistically associated with 4 times higher odds of adherence to dialysis session than that between 3months to 1 year (OR :3.77; 95% CI:1.22, 11.67). In addition, irregular receiving health information was significantly associated with four times higher odds of adherence to dialysis session duration than never receiving health information (OR: 4.35; 95% CI: 1.13, 16.74).
In adjusted analysis, age, education level, occupation, treatment duration, frequency of receiving health information, transport availability and difficulties in dialysis were significantly associated with adherence to dialysis therapy.
Keeping constant other factors, participants aged above 60 years had significantly 8 times higher odds of adherence to dialysis session duration compared to those aged between 18 to 30 years (AOR: 8.32; 95% CI: 1.41, 49.15). Unemployed participants had significantly 2 times higher odds of adherence to dialysis session duration than employed ones (AOR: 2.26; 95% CI: 1.28, 4.00). Treatment duration of more than 60 months had significantly 4 times higher odds of adherence to dialysis session than between 3 months to 12 months (AOR: 4.08; 95% CI: 1.28, 13.06). In addition, participants who received health information significantly had significantly 5 times higher odds of adherence to dialysis session duration than those who never received health information (AOR: 5.22; 95% CI: 1.33, 20.54). Although in crude analysis education level and transport availability indicated a non-statistically significant association, after adjustment of confounders participants attained higher level of education had significantly 3 times higher odds of adherence to dialysis session than those attained primary education (AOR: 2.68; 95% CI: 1.13, 6.35). Also, participants who had available transport had significantly 2 times higher odds of adherence to dialysis session than those with unavailability of transport (AOR: 2.43; 95% CI: 1.12, 5.28). (Table 3a &3b)
Table 3a: Factors associated with adherence to dialysis session among insured patients with ESRD
| Variable | COR (95%CI) | p-value | AOR (95%CI) | p-value |
| Age (years) | ||||
| 18 – 30 | 1 | 1 | ||
| 31 – 40 | 3.50 (0 .37 ,32.97) | 0.274 | 3.45 (0.37, 32.59) | 0.279 |
| 41-50 | 2.70 (0.47, 15.65) | 0.268 | 2.71 (0.47, 15.69) | 0.267 |
| 51-60 | 5.41 (0.98, 30.09 | 0.053 | 5.42 (0.98, 30.14) | 0.053 |
| Above 60 | 3.21 (0.61,16.76) | 0.167 | 3.22 (0.61, 16.84) | 0.166 |
| Sex | ||||
| Male | 1 | 1 | ||
| Female | 1.15 (0.60, 2.18) | 0.676 | 1.14 (0.60, 2.19) | 0.690 |
| Marital Status | ||||
| Unmarried | 1 | 1 | ||
| Married | 1.18 (0.48, 2.95) | 0.717 | 1.24 (0.49, 3.14) | 0.652 |
| Education level | ||||
| Primary | 1 | 1 | ||
| Secondary | 0.78(0.39, 1.55) | 0.477 | 0.88(0.43, 1.78) | 0.723 |
| Higher level | 2.2 (0.98, 4.84) | 0.056 | 2.68 (1.13, 6.35) | 0.025 |
| Months in Dialysis | ||||
| 3 -12 | 1 | 1 | ||
| > 12 -60 | 1.38(0.74, 2.60) | 0.315 | 1.40(0.73, 2.65) | 0.310 |
| > 60 | 3.77(1.22, 11.67) | 0.021 | 4.08(1.28, 13.06) | 0.018 |
| Transport availability | ||||
| Not easily available | 1 | 1 | ||
| Easily available | 2.055814 | 0.059 | 2.43(1.12, 5.28) | 0.025 |
Table 3b: Factors associated with adherence duration of dialysis session among insured patients with ESRD (N=251)
| Factors | COR (95% CI) | p-value | AOR (95% CI) | p-value |
| Age (years) | ||||
| 18 – 30 | 1 | 1 | ||
| 31 – 40 | 4 (0.45, 35.79) | 0.215 | 5.39 (0.58, 49.67) | 0.139 |
| 41-50 | 2.93 (0.47, 18.10) | 0.246 | 3.40 (0.54, 21.32) | 0.192 |
| 51-60 | 6.11 (1.04, 36.01) | 0.046 | 7.67 (1.26, 46.47) | 0.027 |
| Above 60 | 6.41 (1.17, 36.82) | 0.037 | 8.32 (1.41, 49.15) | 0.02 |
| Sex | ||||
| Male | 1 | 1 | ||
| Female | 0.76 (0.42, 1.35) | 0.348 | 0.81 (0.45, 1.47) | 0.491 |
| Education level | ||||
| Completed primary | 1 | 1 | ||
| Completed secondary | 0.26 (0.13, 0.52) | <0.001 | 0.29 (0.14, 0.58) | <0.001 |
| Completed higher level | 0.72 (0.35, 1.49) | 0.377 | 0.76 (0.36, 1.61) | 0.472 |
| Occupation | ||||
| Employed | 1 | 1 | ||
| Unemployed | 2.17 (1.24, 3.81) | 0.007 | 2.26 (1.28, 4.00) | 0.005 |
| Frequency of receiving health information | ||||
| Never | 1 | |||
| Irregular | 4.35 (1.13, 16.74) | 0.032 | 5.22 (1.33, 20.54) | 0.018 |
| Regular | 2.13 (0.59, 7.69) | 0.251 | 2.6 (0.70, 9.54) | 0.154 |
| 4o |
QUALITATIVE STUDY RESULTS
The qualitative data allowed for a deeper insight of the patient towards factors associated with adherence to dialysis therapy.
Factors for adherence to dialysis therapy among the insured patients with ESRD attending dialysis therapy in Kilimanjaro and Arusha regions.
The most common factors for adherence to dialysis therapy that emerged from the interview were divided into six sub- themes, which were awareness and knowledge of disease complications, social support, desire to prolong life and improved quality of life, transport difficulties and accessibility of dialysis centers.
Social support
Majority of the study participants expressed the importance of the family in their course of disease and treatment as illustrated in a quote below.
“As I have told you, my wife passed away but my children especially the ladies really love their fathers, God bless them, they are many like 5 of them and I just have one boy. They do well, for example the moment I was getting here they said Daddy you can’t board a bus and they had to organize for a flight, then I got the treatment then flew back without any tiredness, they are very committed and am Very impressed by their efforts” (R 147).
In some dialysis centers, patients organize themselves and support one who has failed to go on with dialysis due to financial difficulties or health insurance derangements as one participant explained:
“Because you find that one is married and when her husband notice that she can’t conceive, he decides to divorce and take the insurance and she stops attending for treatment, so we who knew her, have to organize and contribute something. We too not well financially, our menu is different from others, getting something for me to eat and at the same time, doing an effort to assist another patient is really pity because you see her dying. We are like 60 people here, if we give 3000Tshs each we get 180,000Tshs, and if she adds a little then we get at least one patient per week whom we can support, but there are more than 8 patients I know in our unit” (R161).
In other hand, some participants declared that the majority of the doctors and nurses were caring, supportive and knowledgeable to support them attending their scheduled dialysis. As one respondent reported that:
“…Doctors tell us not to do this and counsel not to skip dialysis until the Investigation show normal progress, also the nurses can tell you not to drink a lot of water or stop something, so they really warn us and encourage us well to go on with dialysis schedule” (R147).
Desire to prolong life and improved quality of life
Majority of participants highlighted the need to adhere to dialysis for the purpose of prolonging their lives and improving quality of life. Dialysis therapy was considered as very helpful, where ESRD participants were expecting life and improvement of their quality of their life as well, as one participant said that:
“I don’t come here by will or choice but am forced to come, otherwise am shortening my life, so all the time I make sure I don’t miss. And this makes a person with no decision at all in your life, you must make sure you wake up and come whether you like or not, and if you can’t they pick you up” (R149).
Some participants reported to have fear of death and wish live at peace, such desire push them to adhere to scheduled dialysis as one participant stated that: “First of all am scared of death, I want to live at peace and also changing the environment, just coming from home to here, I just become happy when I see new environment” (R 145)
Transportation difficulties
The lack of transport among participants was a factor that was increasing the chances to do not attend hemodialysis treatment and this was related to financial issues, traveling a long distance or coming from a place where taxis or buses are few and don’t work every day. Majority of the participants mentioned the problem of transport.
“… You can wake up early but transport is a problem because I have to take series of vehicles…. a motorbike to the road then a car from the road to here. So, it’s hard to get here early because it often stands to pick people.” (R147). Another participant said: “…everyday spending 5000Tshs,10000Tshs,3000Tshs,6000Tshs, the money is lost so much on bus fare…During rainy season there is much more trouble because from home to the bus stop there is a lot of muds, also cold and rain falling on me, If the umbrella is small rain will fall on me a little, so these are just minor things but also waiting for a bus might take about half an hour till an hour so when it is still raining, I get wet more….”(R43).
Awareness and knowledge of disease complications
Awareness and knowledge about ESRD complications and its treatment caused patients to undergo the treatment recommended by the nephrologist. Majority of the patients are aware of the disease complications as they are frequently reminded by their care providers and at some point, at least a patient had ever encounter either of the disease complication in normal or severe form especially when missed any of the session, therefore this made decision to stick in his dialysis schedule as per prescribed, as one participant explained that:
“Knowing that I have problems in the kidneys is the great motivation for my attendance in the clinic. I thought that, if I have kidney problems, I have to be treated. Then, the doctors decided that I have to attend dialysis” (R02). Another participant also reported: “…. this makes a person with no decision at all in your life, you must make sure you wake up and come whether you like or not, and if you can’t they pick you up …Just Based on your health condition, because if you don’t come there are complications you see in the body. And that will make you really come …” (R149)
Additionally, people with positive attitude toward disease may perceive health information in a way that prompts them to act appropriately to protect their health, as one participant explained:
“First I have already acknowledged that I have a problem, so my problem is upon me tackling it, also the doctor told me if you miss a dialysis, it might cost you than you think, that’s why am coming all the time” (R148).
Accessibility of dialysis centers
There are few dialysis centers in Northern zone of Tanzania, which makes limited availability of dialysis therapy, with consequences of low adherence to dialysis therapy. Majority of the participants explained to have traveled a long distance and spend many hours to reach the dialysis centers, described in the quote below:
“I was living in Singida, and I had to go for dialysis in Manyara at Hydom Hospital, It’s about 300 kilometers. and when we get there the car don’t wait for us, it departs with other passenger who are going in other regions now you find when we are done with dialysis at 4:00PM or 5PM we have to board a last bus to take us home which is very loaded and we travel more than 3 hours while standing to Kateshi to take the other bust to Singida….with such challenge many have dispersed to other places like in Dodoma to their relatives, some in Dar es salaam and others in Arusha and others at Moshi.…. Staying to someone is a big burden because you find that a place you go there are also having their own life challenges, like renting houses or other needs and within time you become a burden and decide to move.” (R 158).
However, some patients explained that shortage of health care provider in the dialysis unit makes difficulty handling of the machine and emergences whenever happened therefore such incidence rise worry and anxiety and therefore fail to attend the dialysis therapy as required, as explained by one participant that:
“The shortage of nurses is big challenge, because they are also people and sometimes get tired, if they are many they will usually have shifts and that is better….it might happen the patient might be in need but there is a delay in attending the patients, then a patient die, it is very simple to lose life for a dialysis patient, because if the pressure falls down, and sugar decrease suddenly and the nurse fails to notice, a patient dies and that has ever happened.”[R02]
DISCUSSION
Our study results showed that overall prevalence of adherence to dialysis therapy was 55%. In sub analysis, 77.7% of participants did not miss dialysis sessions even once in the month on their own initiative. Additionally, 72.1% of the participants never shortened their dialysis sessions by more than 10 min in a month. Adherence to dialysis therapy was significantly associated with age, education level, and occupation, and treatment duration, convenient time to dialysis, copying strategy, and frequency of receiving health information, transport availability and difficulties in dialysis.
Current study shows that the majority of the respondents (77.7%) adhered to dialysis session. This proportion is above the finding reported from Muhimbili National Hospital which found adherence was 69% (Mohamedi & Mosha, 2022). Difference in findings could be explained by the fact that it was a single center study report involving a mixed population (insured and non-insured patients) as well as being a national hospital level, a standard of health services provision varies with other hospital levels like standing alone dialysis units and regional hospital. Also, could be explained by improved dialysis services provided in the health facilities in Arusha and Kilimanjaro regions. However, our study findings are lower than reported from UK, Europe, Japan, and Germany where dialysis adherence rate was more than 90% (Al Salmi et al., 2018). This could be due social disparities between countries. Regardless of these differences, the fact remains that adherence to dialysis therapy is of concern to patients with ESRD. There is a need of health care providers and government in general to improve access to dialysis services so as to improve adherence.
Our study findings showed that 72.1 % of the participants did not shorten dialysis session for more than 10 min at least once in a month. This finding is nearly similar to 75.5% reported by American Kidney Fund (Sapkota et al., 2022). However, our findings are higher than 50.1% reported in Brazil (Dantas et al., 2019), and lower than 92.1% reported by (Mohamedi & Mosha, 2022). Factors like inclusion criteria, setting, and the pandemic (as in Brazil) may explain differences. These findings emphasize the need for society and policy-level efforts to raise awareness about the importance of adhering to prescribed dialysis sessions
Participants aged 60 years and above showed higher odds of adherence to dialysis therapy compared to those aged between 18 and 30 years. This may be due to the fact that majority (49.8%) of study participants were > 60 years. Similarly, (Al Salmi et al., 2018) found that elder age had higher adherence compared to younger ones. Contrary, (Alzahrani & Al-Khattabi, 2021; Clark et al., 2014; Mukakarangwa et al., 2018) found dialysis withdraw in elder patients of >70 years (29.83%) compared to young ones. ESRD in young age reflect the equilibrium shift of disease, therefore policy makers should increase advocacy in disease prevention and control across all age groups.
Our findings revealed that; unemployed participants had two times higher odds of adherence to dialysis therapy compared to employed ones. The higher adherence could be attributed to the fact that a considerable number of participants were retirees who received pensions or financial support, in contrast to employed participants with demanding work schedules. This finding is parallel to (Chenitz et al., 2014; Mohamedi & Mosha, 2022; Mukakarangwa et al., 2018; Sapkota et al., 2022) which suggested that demographic factors like age and employment status are not significantly associated with adherence to HD. Difference could be due to different in sample size and data collection tool. This highlights the necessity of employees to recognize the patients with ESRD in working areas, reminding them and spare sometimes for them to attend their scheduled dialysis session. For example, use of hotline call system in reminding patients to go for dialysis showed 75% improvement in adherence and patient’s satisfaction (Som et al., 2017).
Participants with more than 60 months in dialysis highly adhered to dialysis session compared to those who were in dialysis between 3 months and 12 months, which was consistent with previous studies in Muhimbili national hospital (Mohamedi & Mosha, 2022). Could be because patients evaluate the effects of dialysis on their body and learn to cope with complications by talking to other patients and the healthcare staff as times goes. In contrast to our findings, (Chenitz et al., 2014) reported that many years in dialysis was associated with decreased adherence. As the disease get advanced there is increase in sense of loneliness and dependency therefore lack of adequate support may lead to non- adherence.
The availability of transport to an area was associated with higher odds of adherence to dialysis session, may be due to the reason that more than 50% of participants resided in urban areas. These findings are in line with other findings in developed countries like Japan and Belgium (Al Salmi et al., 2018) where transportation to HD facilities located near public transportation lines. This rise the cue that, there is a need of health insurance agencies to consider universal coverage of transportation to HD facilities to shorten time for a patient reach a dialysis unit either introduction of special cars like ambulances to take patients for dialysis.
Additionally, our study findings found that participants who received health information frequently had higher odds of adherence to dialysis therapy compared to those who never which was similar to (Alzahrani & Al-Khattabi, 2021). This signify that patients’ education and counselling are important in formulating general perception toward various treatment aspects which in turn increase adherence to HD. Contrary, (Naalweh et al., 2017) showed that adherence was higher (more than 50%) despite majority (58%) of participant being never counseled regarding completing HD sessions .Continuous education and counselling sessions are important in maintaining patient in hemodialysis session.
Qualitative method revealed social support from the family and community, awareness of the disease consequences and desire to prolong life were factors influencing adhere to dialysis therapy among insured patients with ESRD. These results are consistent with other studies (Claire Mukakarangwa et al., 2020; Sciberras et al., 2016). Contrarily to our findings other literatures (Chironda & Bhengu, 2019; Claire Mukakarangwa et al., 2020; Tataradze et al., 2016) which reported social support was from HCWs in terms of caring and counselling. This finding highlights the need of continuous mentoring and support patients with ESRD. Since patients in chronic illness like ESRD tend to develop a sense of loneliness and dependency as time goes by, therefore lack of support draw them back to non-adherence to hemodialysis despite of positive attitude.
Furthermore, inaccessibility of dialysis services in terms of transportation difficulties, distance to travel, poor quality of the roads, financial constraints were barriers to dialysis adherence. Macielet al reported similar findings (Maciel et al., 2015). Contrarily, (Chironda & Bhengu, 2019) reported transport difficulties was not an issue in patients who were going to dialysis unit using a transportation van and driving over 17 min to get to the dialysis center. For effective adherence, health system should consider availability of transport means, road infrastructure and bring near dialysis services to the patients with ESRD.
Strength and limitation of the study
To our knowledge, this is the first multicenter hospital-based study that has assessed for adherence to dialysis therapy and associated factors among the insured patients with ESRD in Northern zone of Tanzania. Thus, the results can act as baseline information on dialysis adherence among insured patients with ESRD in our area. Moreover, we examined the factors for adherence to dialysis therapy in different contexts as the study used both quantitative and qualitative methods of data collection, thus revealed several important findings that requires further investigations using a larger sample size and a stronger research design like longitudinal study.
Despite these strengths, given the cross-sectional design, causal relationships between measured factors and adherence to dialysis therapy cannot be drawn. In addition, only two dialysis adherence indicators were considered in the study, which limit generalization therefore future studies should focus on addressing adherence while taking into consideration more adherence indicators as delineated in the ESRD-AQ.
CONCLUSION
More than a half of the insured patients with ESRD our study area adhered to their prescribed dialysis therapy. Older age, higher education level, unemployment, many years in dialysis, frequency of receiving health information and availability of transport are factors associated with adherence to dialysis therapy. Social support, desire to prolong life, awareness of disease complications were factors for good adherence while transportation difficulties and inaccessibility of dialysis centers were factors for poor adherence. Therefore, results of this study recommend the need of health care workers and family members to develop strong support relationships with the patient in order to help patients improve adherence. In addition, ministry of health and dialysis units should establish proper strategies that allow continuous education and counselling of patients regarding disease treatment and self-care. Furthermore, insurance agencies should go extra mile
In addition, consider coverage of transportation via ambulances to take the patients who fail attend dialysis therapy due to transportation issues.
Contributors: CC, BM, KK, and FM at initial draft, revisions and data analysis. In addition, CC had the original idea for the research work, initiated the collaborative and monitored data collection. CC BM, KK, and FM designed the study, revised the paper and worked on entire research components.
Funding no: external funding.
Competing Interests: None declared.
Data sharing statement: All data generated or analyzed during this study are available from the Kilimanjaro Christian Medical University College upon reasonable request from the corresponding author.
Ethical consideration
Permission to conduct this study was granted Kilimanjaro Christian Medical University College and Research Ethics Review Committee with No PG 08/2023.Also, written informed consent was obtained from all participants.
Acknowledgments: We are grateful to all participants who participated in this work and the data collection team
REFERENCES
- Administrative Units Population Distribution Report. (n.d.).
- Agustina, , Yetti, K., & Sukmarini, L. (2019). Contributing factors to hemodialysis adherence in Aceh, Indonesia. Enfermeria Clinica, 29, 238–242. https://doi.org/10.1016/j.enfcli.2019.04.028
- Al Salmi, I., Larkina, M., Wang, M., Subramanian, L., Morgenstern, H., Jacobson, S. H., Hakim, R., Tentori, F., Saran, R., Akiba, T., Tomilina, N. A., Port, F. K., Robinson, B. M., & Pisoni, R. L. (2018). Missed Hemodialysis Treatments: International Variation, Predictors, and Outcomes in the Dialysis Outcomes and Practice Patterns Study (DOPPS). American Journal of Kidney Diseases, 72(5), 634–643. https://doi.org/10.1053/j.ajkd.2018.04.019
- Alzahrani, A. M. A., & Al-Khattabi, G. H. (2021). Factors Influencing Adherence to Hemodialysis Sessions among Patients with End-Stage Renal Disease in Makkah Saudi Journal of Kidney Diseases and Transplantation, 32(3), 763–773. https://doi.org/10.4103/1319-2442.336772
- Amu, H., Dickson, K. , Kumi-Kyereme, A., & Maafo Darteh, E. K. (2018). Understanding variations in health insurance coverage in Ghana, Kenya, Nigeria, and Tanzania: Evidence from demographic and health surveys. PLoS ONE, 13(8), 1–14. https://doi.org/10.1371/journal.pone.0201833
- Bikbov, B., Purcell, C. A., Levey, A. S., Smith, M., Abdoli, A., Abebe, M., Adebayo, O. M., Afarideh, M., Agarwal, K., Agudelo-Botero, M., Ahmadian, E., Al-Aly, Z., Alipour, V., Almasi-Hashiani, A., Al-Raddadi, R. M., Alvis-Guzman, N., Amini, S., Andrei, T., Andrei, C. L., … Murray, C. J. L. (2020). Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet, 395(10225), 709–733. https://doi.org/10.1016/S0140-6736(20)30045-3
- Chenitz, K. B., Fernando, M., & Shea, J. A. (2014). In-center hemodialysis attendance: Patient perceptions of risks, barriers, and Hemodialysis International, 18(2), 364–373. https://doi.org/10.1111/hdi.12139
- Chironda, G., & Bhengu, B. R. (2019). Motivators of adherence to integrated management among patients with chronic kidney disease: A qualitative Nursing and Health Sciences, 21(1), 63–70. https://doi.org/10.1111/nhs.12556
- Claire Mukakarangwa, , Chironda, G., Nkurunziza, A., Ngendahayo, F., & Bhengu, B. (2020). Motivators and barriers of adherence to hemodialysis among patients with end stage renal disease (ESRD) in Rwanda: A qualitative study. International Journal of Africa Nursing Sciences, 13(March), 100221. https://doi.org/10.1016/j.ijans.2020.100221
- Clark, S., Farrington, K., & Chilcot, J. (2014). Nonadherence in dialysis patients: prevalence, measurement, outcome, and psychological Seminars in Dialysis, 27(1), 42–49. https://doi.org/10.1111/sdi.12159
- Dantas, L. G. G., De Seixas Rocha, M., Junior, J. A. M., Paschoalin, E. L., Paschoalin, S. R. K. P., & Sampaio Cruz, C. M. (2019). Non-adherence to Haemodialysis, Interdialytic weight gain and cardiovascular mortality: A cohort BMC Nephrology, 20(1). https://doi.org/10.1186/s12882- 019-1573-x
- Durizzo, K., Harttgen, K., Tediosi, F., Sahu, M., Kuwawenaruwa, A., Salari, P., & Günther, I. (2022). Toward mandatory health insurance in low-income countries? An analysis of claims data in Tanzania. Health Economics (United Kingdom), 31(10), 2187–2207. https://doi.org/10.1002/hec.4568
- Furia, F. F., Shoo, J., Ruggajo, P. J., Kilonzo, K., Basu, G., Yeates, K., Varughese, S., Svarstad, E., & Kisanga, O. (2019). Developing nephrology services in low income countries: A case of Tanzania. BMC Nephrology, 20(1), 1–9. https://doi.org/10.1186/s12882-019-1568-7
- Gupta, R., Woo, K., & Yi, J. A. (2021). Epidemiology of end-stage kidney disease. Seminars in Vascular Surgery, 34(1), 71–78. https://doi.org/10.1053/j.semvascsurg.2021.02.010
- Kustimah, K., Siswadi, A. G. P., Djunaidi, A., & Iskandarsyah, A. (2019). Factors Affecting Non- Adherence to Treatment in End Stage Renal Disease (ESRD) Patients Undergoing Hemodialysis in Indonesia. The Open Psychology Journal, 12(1), 141–146. https://doi.org/10.2174/1874350101912010141
- Maciel, C. D. G., Ferraz, R. N., França, V. V., Frazão, S., & Oliveira, A. K. De. (2015). Adherence to Hemodialysis Treatment: The Perception of Chronic Renal Patients. Cogitare Enferm, 20(3), 538– 546.
- Mohamedi, S., & Mosha, I. H. (2022). Hemodialysis Therapy Adherence and Contributing Factors among End-Stage Renal Disease Patients at Muhimbili National Hospital, Dar es Salaam, Tanzania. Kidney and Dialysis, 2(1), 123–130. https://doi.org/10.3390/kidneydial2010014
- Mukakarangwa, M. C., Chironda, G., Bhengu, B., & Katende, G. (2018). Adherence to Hemodialysis and Associated Factors among End Stage Renal Disease Patients at Selected Nephrology Units in Rwanda: A Descriptive Cross-Sectional Study. Nursing Research and Practice, 2018, 1–8. https://doi.org/10.1155/2018/4372716
- Naalweh, K. S., Barakat, M. A., Sweileh, M. W., Al-Jabi, S. W., Sweileh, W. M., & Zyoud, S. H. (2017). Treatment adherence and perception in patients on maintenance hemodialysis: A cross – Sectional study from Palestine. BMC Nephrology, 18(1), 1–9. https://doi.org/10.1186/s12882-017-0598-2
- Qazi, H. A., Chen, H., & Zhu, M. (2018). Factors influencing dialysis withdrawal: A scoping review. BMC Nephrology, 19(1), 1–11. https://doi.org/10.1186/s12882-018-0894-5
- Sapkota, A., Sedhain, A., Kc, T., Sigdel, S., & Subedi, S. (2022). Adherence to Treatment among Patients With End-Stage Renal Disease Undergoing Hemodialysis In Selected Centers In Nepal. Journal of Nepal Health Research Council, 20(1), 72–78. https://doi.org/10.33314/jnhrc.v20i01.3828
- Sciberras, A., Senior, M. S., Clinical, R., & Nott, J. S. (2016). Facilitators and barriers to treatment with haemodialysis among persons in mid-adulthood : an interpretative phenomenological analysis. 8. https://doi.org/10.1111/scs.12381
- Som, A., Groenendyk, J., An, T., Patel, K., Peters, R., Polites, G., & Ross, W. R. (2017). Improving Dialysis Adherence for High Risk Patients Using Automated Messaging: Proof of Concept. Scientific Reports, 7(1), 1–7. https://doi.org/10.1038/s41598-017-03184-z
- Stanifer, J. W., Maro, V., Egger, J., Karia, F., Thielman, N., Turner, E. L., Shimbi, D., Kilaweh, H., Matemu, O., & Patel, U. D. (2015). The epidemiology of chronic kidney disease in Northern Tanzania: A population-based survey. PLoS ONE, 10(4), 1–12. https://doi.org/10.1371/journal.pone.0124506
- Swanepoel, C. R., Wearne, N., & Okpechi, I. G. (2013). Nephrology in Africa – Not yet uhuru. Nature Reviews Nephrology, 9(10), 610–622. https://doi.org/10.1038/nrneph.2013.168
- Tataradze, A., Managadze, G., Beglarashvili, L., Kipshidze, N., Managadze, L., & Chkhotua, A. (2016). Comparative Costs of Different Renal Replacement Therapies in Lower Middle Income Countries on the Example of Georgia. International Journal of Clinical Medicine, 07(07), 437–444. https://doi.org/10.4236/ijcm.2016.77046
- Timothy, E. A. (2022). Adherence to Haemodialysis Among Chronic Renal Failure Patients of a Tertiary Health Facility , Benin City , Edo State . Borno medical Journal 2021 Vol Adherence to Haemodialysis Among Chronic Renal Failure Patients of a Tertiary Health Facility , Benin C. 18(December 2021), 1–10.