
Effect of Comprehensive Sexuality Education on access to Sexual Reproductive health services among women with disabilities: A case of Bulawayo, Zimbabwe.
- Sindisiwe Silempa,
- 2808-2818
- Mar 12, 2025
- Education
Effect of Comprehensive Sexuality Education on Access to Sexual Reproductive Health Services among Women with Disabilities: A Case of Bulawayo, Zimbabwe.
Sindisiwe Silempa,
Midlands State University, Zimbabwe
DOI: https://dx.doi.org/10.47772/IJRISS.2025.9020216
Received: 12 November 2024; Accepted: 21 November 2024; Published: 12 March 2025
ABSTRACT
A lack in capturing the voice of women with disabilities on sexuality and reproductive health does not only constitute an inequality, but continues to marginalize those who by virtue of having impairments are already experiencing some forms of exclusion. This paper is an advocacy call intending to raise awareness on the importance of increasing knowledge among women with disabilities regarding sexuality and access to sexual reproductive health services in Zimbabwe, using Bulawayo as a case study. Lack of information about sexuality and reproductive health does not only make women with disabilities vulnerable, but also endangers the live of other people in society. The paper adopts a qualitative approach in capturing the views of women with disabilities regarding sexuality and access to reproductive heathy services. The study targeted women with disabilities under the following categories; the deaf, visually impaired and physical impairments. The research design adopted is a case study, focusing on Bulawayo. The sample comprised seven physically impaired, two hearing impaired and one visually impaired. Snowball sampling technique was applied within a purposive sample to identify participants. In depth interviews are the data collecting instruments. A sign language interpreter was engaged during the interviews with the deaf. Data is presented on tables and analyzed thematically. The study established that women with disabilities have limited knowledge on sexuality; are engaged in unhealthy and risky relationships which makes them vulnerable; information on sexuality and reproductive health is not only limited but is presented in inaccessible formats. The study also found out that the deaf are severely constrained in accessing information on sexuality due to language barriers. Therefore, the study recommends that government should strengthen laws that protect disability rights and autonomy. Service providers should avail information in accessible formats. Health care staff need to incorporate disability sensitivity on sexuality and reproductive health.
Key words: Sexuality; Sexual Reproductive Health and Women with disabilities.
INTRODUCTION
The lack in understanding of sexuality and access to reproductive health by women with disabilities does not only constitute an inequality, but continue to marginalize those who by virtue of having an impairment are already experiencing some form of exclusion. This study is an advocacy call to raise awareness on the importance of increasing knowledge among women with disabilities regarding sexuality and access to sexual reproductive health services in Zimbabwe. The study adopts a qualitative approach in order to establish the level of awareness among women with disabilities; the Deaf, visually impaired and those with physical impairments. The study site is Bulawayo Urban.
Background to the study
In many societies including Zimbabwe, sexuality and access to reproductive health for persons with disabilities has often been overlocked or ignored. Addlakha, Price and Heidar (2017), indicate that sexuality and access to reproductive health for persons with disabilities is not taken seriously. Morales, Edwards, Gauthier and Courtois (2016), also regard sexuality as taboo subject. The subject of sexuality is less talked about in the communities especially if it relates to persons with disabilities due to beliefs and norms. Further evidence from the same author reveals that women with disabilities are often misunderstood when they attempt to express themselves sexually. Lack of knowledge by any section of society is unhealthy. Marin, Ballon, Darabi, Karyeni, Soofi and Soltani (2021), describes sexuality as a broad concept encompassing physical, emotion, mental and social wellbeing in relation to sexuality. Genevey, Pachauri and Tubiana (2013), asserts that it leads to inequalities in society; Morales et al (2016), indicates that lack of knowledge force women with disabilities to put up with unhealthy relationships. Martin, Ballon, Darabi, Karyeni, Soofi and Soltani (2021), also note that it can result in sexuality offensive behaviors. While many societies may choose to ignore this subject, the lack in knowledge by women with disabilities can seriously undermine the attainment of Sustainable Development Goal 3 which focuses on Universal or equitable access to skilled and comprehensive sexual, reproductive and maternal health service (Ganle, Baati, Quansah, Dansa- Appiah 2020); as well as make the lives of women with disabilities to be more vulnerable.
Numerous studies indicate that women with disabilities have had horrible experiences regarding sexuality and access to reproductive health. A study by Ganle et al (2020), indicate that women with disabilities experience poor treatment in health facilities. Mavuso and Maharaj (2015) indicate that health care personnel are surprised that women with disabilities also require family planning services and some suggest that they should undergo sterilization. Morales et al (2016), indicate that in Canada women with disabilities have their privacy violated and face sexual assault. In America, “rape culture” holds women accountable for being raped.
In Africa, the treatment has not been different from the rest of the world. In South Africa, Ubisi (2021), documents that from time immemorial sexuality of persons with disabilities have been misunderstood; this has led to sterilization laws which prohibit persons with disabilities from procreating. That period was followed by an era which made persons with disabilities to repress their sexuality and internalized societal disapproval of their sexuality. The study further adds that when persons with disabilities try to access reproductive health services, they often face institutional barriers such as shock, disbelief and attitudes from healthcare personnel.
A study by Neille, McEwen and Andrade (2024), also indicate that lack of information and poor access to health care have contributed to increased risk of HIV and Aids infections among the disabled population. This scenario has been aggravated by lack of sex education, which has seen women with disabilities having fewer opportunities to learn about sexuality. Hence women with disabilities have less experience with dating, intimacy and sexual interaction as compared to their peers.
In Zimbabwe, the experiences of women with disabilities are identical to the rest of the world. A study by Rugoho (2023), indicates that women with disabilities struggle to access sexual reproductive health services because they are excluded from platforms where they could acquire knowledge on sexual reproduction. Their challenge emanates from cultural beliefs held by many Zimbabweans that disability is associated with bad omen. Furthermore, some women with disabilities have been sterilized without their consent. There is great need to raise knowledge levels among women with disabilities so as to safeguard their lives.
The government of Zimbabwe and health care providers have implemented several initiatives to improve access to reproductive health services. Zimbabwe has increased by 67% access to modern contraceptives although disparities need to be addressed between urban and rural areas; adolescent friendly services coupled with confidential HIV testing and counselling; community based initiatives such as Sista2Sista program and policy reforms.
Statement of the Problem
The subject of sexuality is talked less about among Africans owing to cultural barriers and misconceptions. Sexuality in African communities is regarded as taboo. While debates on sexuality and reproductive health have gained momentum over the years, the same enthusiasm cannot be expressed for persons with disabilities. Women with disabilities constitute a fraction of society that is sidelined on issues of sexuality. Such lack in knowledge and awareness is not only detrimental to their lives but also endangers other people’s lives too. As part of empowerment initiatives, this study is an advocacy call to raise knowledge about sexuality and access to reproductive health for women with disabilities.
Research Major Question
- What is the level of understanding about sexuality and access to reproductive health among women with disabilities in Bulawayo?
Research Sub- questions
- How does access to information about sexuality and reproductive health among women with disabilities impact the attainment of SDGs in Zimbabwe?
- How does lack of information on sexuality impact the lives of women with disabilities?
- What support do women with disabilities require in order to access information on sexuality and reproductive health?
Research Objectives
The objective of study is to:
- Establish the extent to which women with disabilities understand sexuality and reproductive health.
- Identify the support required for/by women with disabilities to access information on sexuality and reproductive health.
Conceptual Framework
This study adopted the WHO’s Ecological Framework for Sexual Health. This framework recognizes that sexual health is shaped by multiple levels of influence, from individual biological and behavioral to relationship, community, societal and global factors. Through this interconnectedness, the framework offers a holistic perspective on promoting sexual health and thus preventing sexual ill- health.
Theoretical Framework
The paper adopted social inclusion theory to circumvent the marginalization of women with disability on sexuality issues. According to Rawal (2008) social inclusion is both a process and a goal of increasing participation in society, particularly for people who are disadvantaged, through enhancing opportunities, access to resources, voices and respect for rights. The Social Inclusion theory is fundamental, particularly in the context of sexuality and reproductive health, because it emphasizes the importance of creating least restrictive environments where diversity is valued and respected. The theory challenges systemic marginalization and fosters a culture of acceptance, reducing stigma and discrimination. This inclusive approach ensures equitable access to resources and services allowing individual to thrive and contribute fully to society. Furthermore, Social Inclusion theory dismantles harmful norms, policies and practices that promote exclusion. Ultimately, the incorporation of Social Learning Theory in sexuality and reproductive health promotes an inclusive and vibrant society for all.
METHODOLOGY
This study adopted a qualitative research approach to establish knowledge and awareness on sexuality and reproductive health. According to Yin (2016) qualitative research involves studying the meaning of people’s lives and experiences under real world conditions. This approach provides a nuanced and contextualized understanding of the experiences of women with disabilities; thus allowing the study to capture the challenging dominant narratives that often marginalize women with disabilities. The qualitative approach enabled the participants to share their insights and meanings about sexuality; thus uncovering the intricacies of their sexual lives, which inform program developers and inclusive policies and practices.
Research Design
In an endeavor to capture nuanced experiences on sexuality, the study adopted the case study design to provide rich insights into factors influencing sexual experiences of women with disabilities. Yin (2016), describe a case study as an in-depth examination of a single case to gain deeper understands about the phenomenon. In this study the phenomenon of sexuality is explored within disability context.
Research Instruments
The study adopted in-depth interviews to explore complex, intersections of disability, intimacy and overlooked perspectives of women with disabilities. The use of Interviews allowed the creation of empathetic space for women with disabilities to share the feelings and experiences about sexuality. Pandey (2015), observes that interviews are useful when seeking views and opinions of people with a specific perspective.
Population
The population of interest for this study consists of fifty women with physical and sensory impairments excluding those with intellectual impairments. Brierley (2017), describes population as a group of people or items the researcher wants to make a conclusion about. Only women with disabilities are the targeted population
Sample
Ramanujan, Bhattacharjea and Alcott (2022) describe sampling as a process of systematically selecting units of analysis within a given population. According to Noderifar, Ghaljaei and Goli (2017), this is a process of choosing a part of the population to represent the whole. The study applied snowball sampling technique to purposefully select a sample comprising women with disabilities. The target sample of the study consists of women with disabilities. In order to obtain information on sexuality and reproductive health, seven women with physical impairment, two with hearing impairment and one with visual impairment were selected as key informants.
Sampling technique
The study applied snowball sampling technique which is both purposeful and convenient. According to Noderifar et al (2017), snowball sampling is a method of gathering data that target specific groups of people. Use of snowball sampling technique allowed the researcher to identify specific participants based on disability criteria. The identified participant in turn identified other participants. Although Parker, Scott and Geddes (2019), criticizes it for its failure to meet criteria of random samples; however, its cost effectiveness cannot be ignored (Dragan and Maniu,2013).
Exclusion Criteria
This study has confined its self to focusing only on three categories of impairments; that is visual impairment, hearing impairment and physical impairment. Women with intellectual impairments were excluded from the study due to cognitive limitations and communication barriers. It was feared that the interviews could be overwhelming for them.
RESULTS AND FINDINGS
Demographic Information
Age Distribution
| Participant | Age of participant | Marital Status | Income Level |
| Participant 1 | 37 | single | Self- employed |
| Participant 2 | 41 | single | Self –employed |
| Participant 3 | 43 | single | Self- employed |
| Participant 4 | 46 | Married | Employed |
| Participant 5 | 42 | single | Self- employed |
| Participant 6 | 35 | single | Self –employed |
| Participant 7 | 67 | Married | Employed |
| Participant 8 | 41 | single | Self –employed |
| Participant 9 | 44 | single | Employed |
| Participant 10 | 43 | Married | Self – employed |
Mean of the participants = 43.90
Median = 42.50
Table 1 above shows age distribution among participants. The participants within the age range 37-67 were identified for participation in the study. A mean of 43.90 indicate that participants are middle aged, although there are no participants are within the age of twenty. Participant 7 is an elderly woman who may shy away from openly discussing issues of sexuality. The absence of participants within the range of twenties indicate that their views are not represented in the study.
Participation by Disability Category
| Value | Frequency | Percentage |
| Physical impairment | 7 | 70 |
| Hearing Impairment | 2 | 20 |
| Visual Impairment | 1 | 10 |
The table above shows participating disability categories. Three disability categories who participated are; physical impairment (70%), hearing (20%) and visual impairment (10%). The result indicates that most of the views captured are from women with physical impairment, followed by hearing impairment and lastly visual impairment. The low participation levels of women who are hearing impaired could be attributed to communication and language barriers. As for the visually impaired, accessibility to print is a barrier. Four are married, while six are not. The nature and severity of impairment sometimes impact relationships. Only a few women are gainfully employed whereas the rest are self- employed. Most of them are vendors.
Thematic Analysis
Several themes emerged from the qualitative responses gathered from the participants. Emerging themes from the study include; sex, intimacy and sexual behaviors;
| Theme | Data collected |
| Sex, Intimacy& Sexual behaviors | Participant 1; intimacy, sex
Participant 2: intimacy, organs Participant 3; intimacy Participant 4; natural changes of a person’s life, gender Participant 7&8; desire to indulge Participant 9; intimacy and affection for my lover Participant 10; sexual feelings, attraction & behavior towards it |
relationships; safety; workshops; hospitals, clinics &pharmacy; attitudes; support and access.
Thematic Area 1: Sex, Intimacy & Sexual Behaviors
The table above shows participants’ understanding of sexuality. Most (60%) of the participants understand sexuality as referring to intimacy, sexual feelings, attraction and behaviors towards it. Sex and intimacy featured the most. The result indicates a limited understanding of the concept, but suffice to say they are aware of some of the elements embedded within the concept. Of the remaining percentage, 10% expressed that sexuality refer to male and female while 30% had no idea at all. This is evidenced by far-fetched responses like “to wide”, self- control’. The response from one deaf participant, indicated that she has no knowledge about sexuality. Due to language barrier, the participant could have suspected that the researcher was digging into her privacy. This finding resonates with that of Morales et al (2016), who argue that women with disabilities have little knowledge or experience and often have negative feelings about sexuality. A similar opinion is expressed by Rugoho (2023), who reiterate that sexual discrimination is prevalent at family level where they are left out in sexuality and reproductive health issues. Their lack of knowledge can make them to be susceptible to a lot of dangers and mistreatment.
Relationships
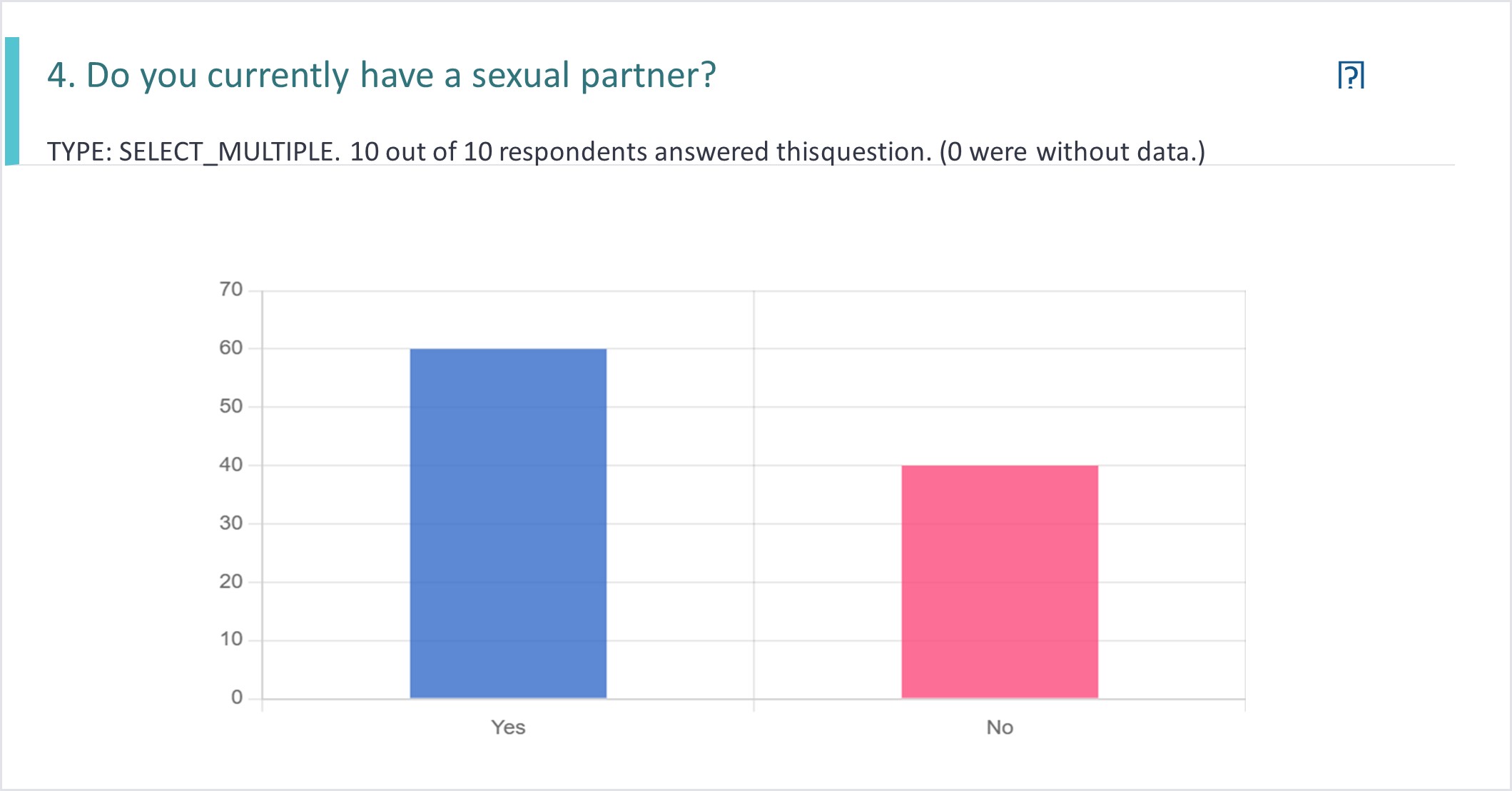
The histogram above shows that 70% of women with disabilities are in relationships while 30% are not. The results seem to confirm that women with disabilities have sexual partners. The 70% is testimony that women with disabilities, like other women require information on sexuality and reproductive health for their own safety and survival. The remaining 30% of women who do not have sexual partners for now also need information for their own safety in-case they develop relationships in the future. Lack of knowledge on sexuality and reproductive health is risky as it may expose women with disabilities to unhealthy relationships. The findings above are relatable to results by Morales et al, 2016), which indicate that one woman with disability had been sexually abused by family members during adolescence and had never known any kind of sexual relationship that did not involve force against her. Without adequate information women with disabilities shall continuously be exposed to all forms of abuse. Another dimension in relationships relates to health personnel. A study by Mavuso and Maharaj (2015), established that women with disabilities have poor relationships with health personnel as they are often scolded for asking for contraceptives; nurses ask too many questions and always suggest that they undergo sterilization. There is need for awareness for both the health personnel and women with disabilities in order to facilitate health relationships
Safety
Safety concerns in sexuality and reproductive health is of outmost importance to every individual. Women with disabilities also need to ensure they are safe in all aspects of their lives.
| Participant | Data collected |
| Participant 1 | Yes, I can negotiate |
| Participant 2 | Yes, I can. They tend to take advantage |
| Participant 4 | Yes, with a deaf guy, he agrees to use condoms |
| 5 | Yes, I am |
| 6 | Yes, I do |
| 7 | Yes, I am |
| 8 | Yes, I am |
| 10 | Yes |
Eight (80%) of participants expressed that they are capable of negotiating for safe sex. The remaining 20% had a different opinion regarding the subject. From the 20%, ten percentage expressed that they no longer want to engage anymore. The sentiments reflect resentment or bitterness. The last 10%, said “not always because at times the partner asks if I do not trust him and we end up quarrelling and he ends up forcing himself on me”. Although the percentage is small, evidence shows that some women with disabilities indicate that there is need to raise awareness for negotiating for safer sex. By virtue of having a disability and being women makes them susceptible to unpleasant sexual contacts. This result tallies with evidence from Opsahl and Pick (2017), which indicate that deaf women experience higher rates of life time sexual assault as compared to other hearing counterparts. Similarly, Ganle et al (2020), note that lack of information about sexuality and reproductive health increases vulnerability to STIs and HIV & Aids. Another observation from Neille et al (2024), indicates that lack of information and poor access to health care have been identified as barriers contributing to increased risk of HIV and Aids infections among the disabled. Lack of information in accessible formats may continuously increase the vulnerability of women with disabilities.
Workshops
Access to knowledge and information on a particular phenomenon is vital for human survival. Without adequate information people can risk their health and make uninformed decisions and choices.
| Participant | Data Collected |
| Participant 1 | Me, get from workshops |
| Participant 2 | Workshops, media, television |
| Participant 6 | Workshops, nurses, from OI clinic |
| Participant 7 | Through workshops |
| Participant 8 | Education, workshops |
| Participant 9 | Access information through media, workshops. |
The table above shows results on access to information on sexuality and reproductive health. Six (60%) of participants expressed that they access information through workshops. The evidence reflects efforts made by Government and Non – Governmental Organizations in ensuring that people with disabilities have access to information. The remaining 40% indicate that information is sought from media, social media, friends, radio, neighbors and clinics. It is pleasing to note that at least information is availed through various channels. While workshops occupy largest space, there is need to mainstream all disability categories and also resort to new modalities of communication such as online. However, information is restricted and is not availed in accessible formats (Rugoho and Maposa 2017). Due to limited information, some communities think that there is something wrong with man who have sex with disabled women (Thabethe 2022). The above observation indicates that knowledge is not only lacking for persons with disabilities but also to able- bodied in societies.
Hospitals, Clinics and Pharmacy
| Participant | Data collected |
| Participant 1 | Hospitals, buy |
| Participant 2 | Clinics & family planning services |
| Participant 3 | Hospitals & pharmacy |
| Participant 6 | Pharmacy |
| Participant 7 | Clinic |
| Participant 9 | Hospitals like Mpilo & MAC and NAC |
| Participant 10 | Pharmacy |
The table above shows facilities /centers which provide contraceptives to women with disabilities. The majority (70%) of participant’s access reproductive health services from hospitals, clinics and pharmacies. The 30% not reflected on the table could be resorting to other means or they do not access contraceptives at all. From the thirty percent, 10% said, “Zero, nowhere” and another 10% said, “prior I had my long term contraceptive, my family, Aunty chose for me tubalisation”. The statement suggests that family members could be infringing on the rights of persons with disability by making choices for them. This finding is buttressed by Ubisi (2021), who indicate that the rights of women with disabilities are often ignored. Women with disabilities need to be empowered through knowledge so that they make their own choices and prevent other people from taking advantage of their impairments.
Attitudes
Understanding and having knowledge about attitudes is fundamental is designing programs and dispatching services. The result indicate that the majority of participants tend to hold un authenticated perspectives regarding the sexuality of persons with disability. The responses reflect negative perceptions regarding women with disabilities. The following statements were supplied by participants, “ women with disabilities are not capable of having multiple sexual partners and therefore are safe to have unprotected sex with ; having sex with a disabled women is a favor ; women with disabilities should be protected from sexual contact; it’s a burden ( participant 2&10); feel pity ( participant ( participant 10& 9; it’s shameful ; women with disabilities are viewed as asexual ( participant 9); it’s a taboo( participant 3; some people are wondering how they do it ; some think women with disabilities are desperate and some think its abuse.
While the statements reflect negative attitudes, there is also evidence of lack of knowledge. Some statements reflect emotions harbored by society concerning sexuality. Such misconceptions are detrimental on human development.
Support
This thematic area identifies various forms of support required by women with disabilities. The views expressed by women with disabilities indicate varied needs depending on disability category. Forty percent of participants indicate that they require support in Sign language. The need for sign language is two -fold, information that need to be put in sign language; secondly personnel in health care centers need to communicate in sign language. Twenty percent of respondents require government assistance on contraceptives. Another twenty percent need information on sexuality and reproductive health timeously in accessible formats and also through workshops and campaigns. Ten percent of participants require government assistance in form of school fees for their children. The remaining ten percentage require information on disease transmission and counselling services so that patients do not default in taking their medication.
Access
Access to sexuality and reproductive health differs with each disability category. The deaf require information in sign language; visually impaired in braille, physically impaired require accessible clinics and adjustable hospital beds. This study reveals that although 60% of participants have an idea about sexuality and reproductive health; a lot more information is required so that women with disabilities are safe and make informed decisions. Women with physical disabilities who constitute 70% expressed that there is need to increase access for the deaf due to language barrier. The visually impaired who constitute 10% expressed that they need information in audio and braille. Access to information is critical in the prevention of various forms of abuse. The study revealed that women with disabilities have partners who are forceful in soliciting for sexual intercourse and yet some have procedures done on them without their consent. The study revealed that “tubalisation” and administration of Depo are some procedures done without the consent of women with disabilities. Awareness is necessary in ensuring that women with disabilities are protected from all forms of abuse and sexually transmitted infections. This result tallies with the observation by Ganle et al (2020), who lament that information is not availed in accessible formats.
CONCLUSIONS
The purpose of this study is to raise awareness about sexuality and access to reproductive health services in Bulawayo Metropolitan Province for women with disabilities. To accomplish this goal, women with disabilities were interrogated using thematic analysis to establish the extent to which they understood sexuality and access to reproductive health services. In a bid to find out how much women with disabilities understood the concept “sexuality”, the study found out that participants have limited understanding of the concept. Most of the participants zeroed in on “sex and intimacy”, leaving out broader and fundamental aspects such as gender, body consciousness and rights. The study concludes that while most of the women have limited understanding, the deaf are further limited by language barrier. The study also established that women with disabilities are engaged in relationships like all women. However, lack of understanding about sexuality makes them vulnerable and susceptible to unhealthy and toxic relationships. Furthermore, the study noted that the majority of women with disabilities are capable of negotiating for safe sex. Although information about sexuality is conveyed through workshops, not all people get to attend hence the government needs to do more in ensuring that information is passed through social media platforms. The study concludes that government and service providers need to mainstream disability categories. Furthermore, the study established that some family members of disabled persons make choices and decisions on behalf of persons with disabilities regarding contraceptives without their consent. Negative attitudes continue to be a barrier for women with disabilities especially when accessing reproductive health services. Government as well as other stakeholders need to provide support, more so, to the deaf. It was also noted that information need to be put in accessible formats for the disability categories. Women with disabilities need support on contraceptives, they need to access them for free. Conclusively, government and program designers need to collaborate and ensure knowledge levels are raised as well as increase reproductive health services for women with disabilities. Knowledge levels need to be increased for the care givers and or parents of women / girls with disabilities.
RECOMMENDATIONS
In view of the findings above, this study recommends a multi-faceted approach to address the critical gaps in sexuality and reproductive health knowledge and marginalization of women with disabilities;
- Policy makers need to develop inclusive policies ensuring access to comprehensive sexuality education and reproductive healthcare for women with disabilities.
- Government need to strengthen laws protecting disability rights, autonomy and decision making.
- Health care provides need to engage in disability sensitivity training on sexuality and reproductive health
- Health care providers should provide confidential and individualised counselling services.
- Education sector should develop inclusive educational materials on sexuality and reproductive health in formats that are accessible to persons with disabilities.
- Care givers of persons with disabilities should be trained on sexuality and reproductive health for persons with disabilities
- Program planners should amplify the voice of women with disabilities through advocacy and participatory research.
REFERENCES
- Addlakha, R.; Price, J. and Heidari, S. 2017. Disability and Sexuality: Claiming sexual and Reproductive rights. An international Journal on sexual and reproductive health and rights. Vol.25, 2017. Issue 50. https://doi.org.10.1080/ 09688080.2017.
- Brierley, J. A. 2017. The role of a pragmatist Paradigm when adopting mixed methods in behavioral accounting research. International Journal of Behavioral Accounting and Finance 6 (2) pp 140-15. ISSN 1753-1969. White Rose.
- Ganle, J.K.; Baati, R.; Ema, L. Quansah, R. and Danso, A A. 2020. Barriers facing persons with disability in accessing sexual and reproductive health services in sub –Saharan Africa: A systematic Review. Open Access. Doi. 10.1371. /journal 0238585.15 (10) e 0238585.
- Genevey, R.; Pachauri, R.K. and Tubiana, L 2013. Reducing inequalities: A substance Development Challenge. Afd. IDDRI.
- Mavuso, S.S and Maharaj, P 2015. Access to Sexual and Reproductive health services: Experiences and perspectives of people with disabilities in Durban, South Africa.
- Martin, B.K.; Ballon, M.; Darabi, F.; Karyani, A.K. Soofi, M. and Soltani, S. 2021. Sexual health concerns in women with Intellectual disabilities: A systematic review in qualitative studies. BMC Public Health.21: 1965.htttps://doi. Org/10.1186/s 12889-021- 12027=6. Open Access.
- Morales,E.; Edwards,G.; Gauthier, V and Courtois,F 2016. Women with Disabilities’ Perceptions of Sexuality, Sexual Abuse and Masturbation Sex. Bisabil.Doi.10.1007/s11195-016-9440-1. Springer
- Neille, J.; McEwen, H. and Andrade, V de. 2024. An Exploration into People with Disabilities Access to sex , sexuality and sex education in South Africa. Sexuality and Disability. https://doi.org/10.1007/s11195-023-09827-6. Springer.
- Noderifar, M.; Ghaljaei, F. and Goli, H. 2017. Snowball sampling: A purposeful method of sampling in Qualitative Research. Strides Dev Med. https://www.researchgate,net.Doi 10. 5812/scime.67670.
- Pandey, P. 2015.Research Methodology: Tools and techniques. Bridge Center. Romania.
- Parker, C.; Scott, S. and Geddes, A. 2019. Snowball sampling: Research Methods Foundations. Sage. University of Gloucestershire. UK.
- Rawal, N. 2008. Social Inclusion and Exclusion: A review. Dhaulagiri Journal of Sociology and Anthropology. Vol. 2. Academia Edu.
- Rugoho, T and Maphosa, F. 2017. Challenges faced by women with disabilities in accessing sexual and reproductive health in Zimbabwe: The case of Chitungwiza town. A OSIS. African journal of Disability. ISSN(Online)2226-7220. Print 2223-9170.https://doi.org/10.4102.
- Opsahl, N. and Pick, L.H.2017.Undersanding The Sexual Assault Disclosure Experiences of Deaf Women. Jadara.Volu. 51/1553/ No 3.44-67. https://repository.wcsu.edu.jadara
- Ubisi, L. 2021.The sexuality of Disabled Bodies and Individuals with Disability in South Africa’s Comprehensive Sexuality Education Scripted Lesson Plans. University of Pretoria
- Yin, R.K. 2016. 2ND E. Qualitative Research. From Start to Finish. Guilford Press.