
Evaluation of the Millennium Development Goal 4 (Reduce Child Mortality) and the Impact of Government Expenditure on Health in Nigeria
- Oru Patricia Oghenekevwe
- Sodeeq Opeyemi ADESOYE
- 2254-2261
- Aug 2, 2024
- Education
Evaluation of the Millennium Development Goal 4 (Reduce Child Mortality) and the Impact of Government Expenditure on Health in Nigeria
Oru Patricia Oghenekevwe1, Sodeeq Opeyemi ADESOYE2
1Department of Economics, School of Secondary Education (Business), Federal College of Education (Technical), Asaba, Delta State, Nigeria
2Policy Innovation Center, Nigerian Economic Summit Group Abuja, Nigeria
DOI: https://dx.doi.org/10.47772/IJRISS.2024.803164S
Received: 13 June 2024; Accepted: 27 June 2024; Published: 02 August 2024
ABSTRACT
This study assesses millennium developmental goal MDG 4 (Reduce Child mortality) and role of government expenditure on health 2000-2015. The statistical tool employed for analysis was the ARDL, given data obtained from the Statistical Bulletin of the Central Bank of Nigeria and the World Bank Development Index. The authors have addressed issues such as government health expenditure, under-five mortality, and also MDG 4 trend analysis in Nigeria. In line with the theoretical prediction, the empirical findings show that government recurrent expenditure on health has the expected positive but however is statistically insignificant with Under-five mortality rate in Nigeria. However, it gives emphasis to the fact that there is a strong need to intensify immunization activities to generate long term strategic outcome. To ensure reduction in under-five mortality, the government need to invest in effective health programmes, and also have to work to remove inefficiencies that have been identified and focus on achieving the Sustainable Development Goal 3. Primarily, realizing value of available resources and exploiting early start is critical.
Keywords: Under-Five mortality, Millieum Development Goals, Sustainable Development Goals, Government Expenditures, Health
INTRODUCTION
There is a need to reduce the rate of child mortality to retain and conserve the future capacity of nations and their economic systems. Child deaths are associated with health problems like poor sanitation, diarrhoea, malnutrition, and environmental conditions. The leading causes of neonatal deaths are birth asphyxia, severe infections, and preterm birth while the main causes of child mortality and morbidity are diarrhoea, acute respiratory tract infections, measles and malaria [1].
In the year 2000, Nigeria was one of the countries which supported the United Nations Millennium Declaration which resulted in the adoption of eight Millennium Development Goals (MDGs) which include reducing child mortality (MDG 4). Nigeria adopted a variety of policies and programmes to achieve MDG goals by 2015 using part of the savings from the Paris Club Debt Relief deal [2][3]. Despite the overall success, the MDGs have been criticized for not paying adequate attention to inequalities within countries and directing resources to specific goals by crowding out broader investments in health systems [4].
Despite several reforms and policies, the estimation of the rate of increase in child survival indices has been very low in Nigeria one of the worst in Sub-Saharan Africa [1]. As an illustration, Nigeria incurs roughly 9% of all neonatal mortality in the world [5], also the MDG Goal 5, regarding to under-five mortality, was not achieved as at 2015 [6]. Much of the past research on determinants of under-5 mortality has focused less on the effect of government expenditure on health [7]. However, the high infant and child mortality rates in Nigeria are persisting despite the growing health expenditure, which implies the necessity of investigating the influence of government expenditure volatility in attaining MDG 4. Thus, the purpose of this study is to analyse the trend of the nature of MDG Goal 4 in Nigeria and determine the correlation between the under-five mortality rate and government spending on health.
After the introduction, the rest sections of the paper are organized as follows: Section 2 summarizes the relevant primary and secondary literature review on under-five mortality and government expenditure on health. The next section (3) discusses the estimation method, and the data used in the study. Section 4 presents the empirical key findings, while Section 5 discusses the study’s conclusions and policy recommendations.
LITERATURE REVIEW
The first five years of life are the most crucial to the physical and intellectual development of children and can determine their potential to learn and thrive for a lifetime. That is why it is specifically stated as one of the goals of the MDGs to reduce infant mortality by two thirds by 2015. Between 2000 and 2007, an average of 2.1% to 5.8% of total government expenditure was spent on health, in 2018, 4% of the total budget of 8.612 trillion was allocated for healthcare expenditure, which was far below April 2001 [8]. The Millennium Development Goals (MDGs) were 8 goals set in September 2000 by 189 United Nations member countries with a promise to work passionately until 2015 to reduce extreme poverty and other human development-related issues. The MDGs recognised the complexity of development and poverty reduction that could not be achieved simply by rising incomes. Child mortality is a very worrying demographic phenomenon, especially in developing countries, which has attracted the attention of various scholars and researchers.
Numerous empirical studies have investigated factors influencing child mortality rates across different countries and contexts using primary data collected through surveys. The work of [9] in Nigeria, [10] in Katsina State, and [7] analysing the 2016/2017 Multiple Indicator Cluster Survey employed methods like ordinary least squares regression, correlation analysis, and multilevel modelling. These studies examined the effects of factors like government health expenditure, maternal literacy, household income, and access to services on child mortality indicators.
[9] This study explores Health spendings, child mortality and economic growth in Nigeria using time series data ranging within the period 1980 to 2020. In this work, the method applied in analysing the data was the Ordinary Least Square (OLS) method. The regression analysis shows a negative and statistically insignificant effect of government expenditure on health for under-five child mortality. This by extension mean that capital funds by the government is a negative and insignificant predictor of under-five mortality while recurrent spendings has a negative but significant predictor of under-five mortality.
The paperwork [10] titled “Mothers” literacy, Public Health Expenditure and under-five mortality rate in Funtua Local Government Area of Katsina State” used a Two-stage clustered sampling method to select the study units, 100 questionnaires were given to the chosen adult female participants. This study used data on the spending on health and under-five mortality in Funtua Local Government. From the PCC it was realized that there exists a high degree of relationship between public health expenditure and mortality rate of children below the age of five. It also came to a conclusion that increasing female literacy rate best reduce the under-five’s mortality rate in Funtua Local Government.
[11] analysed the effects on the association between health expenses and three proxies of health in West African Countries, of governance. This was done by using two least square estimation method on a panel of fifteen (15) West African Countries etc Nigeria, Chad, and Guinea-Bissau of period 2000-2018. The health proxies for the current study are infant mortality rate, probability of dying between birth and age five, and life expectancy which would be examined at same time as six governance effectiveness proxies which are government effectiveness, rule of law, voice and accountability, regulatory quality, political stability and absence of violence(terrorism), and control of corruption. On this study also, it was premised that though health expenditure has negative effect on infant mortality and under-five mortality, it has positive impact on life expectancy.
[12] In his paper, titled “Whose child is dying? Household characteristics and under-5 mortality in Nigeria,” examined the predictors of Under-5 mortality focusing on household–level variables Data for the study were obtained from the 2008 Nigeria Demographic and Health Survey The sample of the study involved 36 800 households that were selected from across the country. Household surveys were conducted on 33,385 women aged 15 – 49 years who have given birth to at least one live-born infant in the five years preceding the survey. According to him, with the result he got from the analysis of the data which was done using a multilevel-model approach, he was able to infer that under-5 mortality rate is still high in Nigeria. This will not be resolved until household level interventions are performed using a framework which is specific to families and the issue of the necessity of raising the maternal education level in the country is solved.
On secondary data usage, [13] in their work titled “Health care expenditure and child mortality in Nigeria” They used Vector auto regression model techniques, unit root tests and cointegration test were carried out using time series date for the period between 1986 and 2016, the outcome has revealed that expenditure on healthcare possesses a negative correlation with the mortality of infants and neonates. The study discovers that if the Nigerian government raises and maintains health expenditure specifically on activities focused on minimizing infant mortality, it will translate to reduction in infant mortality in Nigeria.
In the work of [14], titled “Malawi and Millennium Development Goal 4: a Countdown to 2015 Country Case Study” aimed mainly at explaining the country’s success in improving child survival. They estimated child and neonatal mortality for the years 2000–14 using five district-representative household surveys. The study included recalculation of coverage indicators for that period, and used the Lives Saved Tool to attribute the child lives saved in the years from 2000 to 2013 to various interventions. They documented the adoption and implementation of policies and programmes affecting the health of women and children and developed estimates of financing. This case study confirmed that Malawi had achieved MDG 4 for child survival by 2013. This was achieved through interventions that were effective against the major causes of child deaths (malaria, pneumonia, and diarrhoea), programmes to reduce child undernutrition and mother-to-child transmission of HIV, and some improvements in the quality of care provided around birth.
[15] analysed trends and social differentials in neonatal and under-five mortality in a Nicaraguan community from 1970 to 2005 in their article “Tracking progress towards equitable child survival in a Nicaraguan community: neonatal mortality challenges to meet the MDG 4” Two linked community-based reproductive surveys in 1993 and 2002 followed by a health and demographic surveillance system providing information on all births and child deaths in urban and rural areas of León municipality, Nicaragua. A total of 49,972 live births were registered. According to their results, a rapid reduction in under-five mortality was observed during the late 1970s (from 103 deaths/1000 live births) and the 1980s, followed by a gradual decline to the level of 23 deaths/1000 live births in 2005. This community is on track for the Millennium Development Goal 4 for improved child survival.
Collectively these bodies of empirical work highlight the multiple aspect of child health outcomes and the importance of all-encompassing strategies that address both proximate as well as socioeconomic factors to improve child health and decrease the burden of preventable deaths in children and accelerate the realization of development goals in the context of maternal and child health.
DATA AND METHODOLOGY
Data Source
The secondary data employed for this research, specifically the annual time series type of data from 2000-2015 (quarterly data) was sourced from the publications of the Central Bank of Nigeria (CBN) and the World Bank Index (WBI).
Theoretical Framework
[16] This analytical framework for study of child mortality was adopted. The theory is often used implicitly or explicitly for empirical studies on child mortality and, it distinguishes between proximate and socio-economic determinants of child mortality, proximate determinants (or intermediate variables) directly affect child mortality risk, such as maternal factors (age, parity, and birth interval), environmental contamination (hygienic factors, water, and sanitation), nutrition, injuries, and personal illness control
Model Specification
The framework of Eboh, Aduku and Onwugalu (2022) was adopted, and the functional model is specified as:
CM = f (GFCF, RCEXP, CEXP, GHEXP) ………………………………..(1)
Where, CM is the under-five child mortality rate, GFCF is gross fixed capital formation, RCEXP is a recurrent expenditure, CEXP is capital expenditure, and GHEXP is government health.
The adaption of [9] study was re-modified, dependent and independent variables to be the indicators of MDG 4 and Government recurrent expenditure on health to fit the study respectively:
U5MR= f (PIAM, INMR, GREXH) ………………………… (2)
Where:
U5MR= Under-five Mortality rate (Dependent variable)
PIAM= Proportion of 1 year old Immunized against Measles (Independent variable)
INMR =Infant Mortality Rate (Independent variable)
GREXH=Government Recurrent expenditure on Health (Independent variable)
It is presented in linear function as follows;
![]()
The factors omitted in the model are considered by introducing an error term (disturbance term; ), in the model to capture all kinds of disturbances that might distort the structure of the model.
The above model is transformed into log linear model as specified below:
![]()
This is done in other to satisfy the statistical condition of a model.
DATA PRESENTATION AND DISCUSSION
Unit Root
Unit root test was conducted using Phillips-Perron test equation with constant & trend for all variables in this study to determine the stationarity of the variables at the level and at first difference as presented in table 1 below. The under-five mortality (LU5MR) and Infant Mortality rate (LINMR) were significant with constant and trend where the probability 0.0062 and 0.0097 are less than 0.05 respectively, we reject the null hypothesis and the variables are stationary at level I(0).
The proportion of years old immunized against measles (LPIAM) and Government recurrent expenditure on health (LGREXH) was not significant at the level so we subject it to further differencing, the variables became significant at first their difference both with the trend and without trend at 5%, we reject the null hypothesis and the variable is stationary at the first difference I(1). Thus, the results indicate all series possessing integrated a mixed-order
Table 1: Phillips-Perron Unit Root Test
| Phillips-Perron Unit Root Test | |||||
| At Level | |||||
| LU5MR | LPIAM | LINMR | LGREXH | ||
| With Constant & Trend | t-Statistic | -4.2822 | -1.1404 | -4.1196 | -1.8441 |
| Prob. | 0.0062 | 0.9135 | 0.0097 | 0.6713 | |
| Sig. | *** | No | *** | No | |
| At First Difference | |||||
| d(LU5MR) | d(LPIAM) | d(LINMR) | d(LGREXH) | ||
| With Constant & Trend | t-Statistic | – | -3.6225 | – | -4.2156 |
| Prob. | – | 0.0359 | – | 0.0075 | |
| Sig. | – | ** | – | *** | |
Notes: (*) significant at 10 %,(**) significant at 5% and (***) significant at 1%, (No) Not Significant.
Long-Run and Short-Run MDG Goal 4 And Target
In the short run, one variable was found to be significant LINMR at level, the variable is significant at 1%. A percentage increase in the dependent variable will increase LINMR by about 44 percent. In other words, a percentage increase in the under-five mortality rate will increase infant mortality rate by about 44 percent, this finding is significant at for confidence interval of 99 percent. Also, the proportion of 1-year-olds immunized against Measles has a significant impact on reducing the child mortality rate within a short period. The LPIAM is 10 per cent significant and inversely influences the under-five mortality rate in the first lag period. This depicts immunization programs should be encouraged more often. However, there exists a long-run relationship and the coefficient is significantly negative, implying that about 22 per cent of disequilibrium is being corrected at a subsequent period, which means, the adjustment parameter is given by the coefficient of error term at lag 1, ECM (-1), and shows the speed of adjusting to long-run equilibrium has the value of (-0.21802). (See table 2 below)
Table 2: short run analysis for MDG goal 4 and target
| Variable | Coefficient | Std. Error | t-Statistic | Prob. |
| D(LU5MR(-1)) | 0.684801 | 0.07979 | 8.582511 | 0.0000 |
| D(LPIAM) | 0.000965 | 0.000873 | 1.105528 | 0.2740 |
| D(LPIAM(-1)) | -0.0016 | 0.0008 | -2.00422 | 0.0500 |
| D(LINMR) | 0.445037 | 0.106651 | 4.172842 | 0.0001 |
| D(LGREXH) | 0.002922 | 0.001981 | 1.474942 | 0.1463 |
| CointEq(-1) | -0.21802 | 0.057757 | -3.77474 | 0.0004 |
In the long run, the proportion of one-year-olds immunized against measles has a positive relationship with the under-five mortality rate (U5MR). However, this relationship is not statistically significant (p-value = 0.1175 > 0.05), indicating that changes in the immunization rate do not significantly affect the under-five mortality rate in the long run. The infant mortality rate has a significant and positive relationship with the under-five mortality rate (U5MR) in the long run. This relationship is statistically significant (p-value = 0.0000 < 0.05).
On the other hand, government recurrent expenditure on health has a negative but statistically insignificant relationship with the under-five mortality rate (U5MR) in the long run (p-value = 0.7391 > 0.05). This indicates that changes in health expenditure do not have a significant impact on reducing the under-five mortality rate. The constant term is statistically significant (p-value = 0.0000 < 0.05), indicating that other factors not included in the model also play a significant role in determining the under-five mortality rate.
| Table 3: Long-Run Analysis of MDG Goal 4 And Targets | ||||
| Variable | Coefficient | Std. Error | t-Statistic | Prob. |
| LPIAM | 0.001464 | 0.00092 | 1.591925 | 0.1175 |
| LINMR | 1.132752 | 0.001152 | 983.0553 | 0.0000 |
| LGREXH | -0.00108 | 0.003226 | -0.3348 | 0.7391 |
| C | -0.11627 | 0.008209 | -14.1643 | 0.0000 |
Source: Authors computations
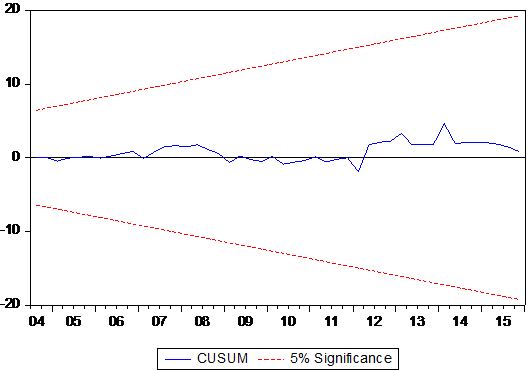
Figure 1: CUSUM test
Stability Test (Post-Estimation diagnostic)
The CUSUM test is based on the cumulative sum of the recursive residuals. Movement of cusum within the 5% critical lines is suggestive of coefficient stability, the test clearly indicates stability in the equation during the sample period as depicted in figure above:
CONCLUSION AND RECOMMENDATION
Nigeria’s efforts aimed at reducing avoidable child deaths have been met with gradual and sustained progress. The under-five mortality rate (U5MR) has improved remarkably looking at the trend analysis, Nigeria falls short of the 2015 target. The proportion of one-year-old children immunized against measles increased according to the study.
The study reveals that there is a mixed insignificant relationship between under 5 mortality rate and government expenditure on health in Nigeria, an increase in government recurrent expenditure on health has no significance on the under-five mortality this could be a result of the inadequate funding and resources in Nigeria’s health sector. However, the evidence encourages the immunization program to continue at an acceleration pace to have a significant impact in the long run
In order to develop an effective solution strategy for prevention of under-five mortality rate in Nigeria, the government should allocate more funds to targeted health intervention such as immunization and infant health programs. Focusing on the budget allocation and dealing with fundamental issues of health expenditure are important for building changes in the long term. Furthermore, the targets and activities should now shift their priority towards the accomplishment of the Sustainable Development Goals (SDGs), especially the third goal that seeks to reduce neo-natal and under-5 mortality by the year 2030. To fill the existing gaps, Nigeria requires the application of existing tools and knowledge for the achievement of SDGs; putting the early priorities into practice and utilizing SDG funding from various sources including the private sector.
REFERENCES
- Ojewumi Titus, K., & Ojewumi Johnson. (2015). ‘Trends in Infant and Child Mortality in Nigeria: a wake-up call assessment for intervention towards achieving the 2015 MDGs.’ Science Journal of Sociology & Anthropology ISSN: 2276-6359.
- Oshewolo, S. (2011). ‘Poverty Reduction and the Attainment of the MDGs in Nigeria: Problems and Prospects’.
- MDGs. (2015). MDG 4: Reduce Child Mortality. 91, 143-148.
- WHO. (2015). ‘Health in 2015 from MDGs to SDGs’. https://www.who.int/data/gho/publications/mdgs-sdgs
- Ogbuoji and Yamey. (2019). ‘How many child deaths can be averted in Nigeria? Assessing state-level prospects of achieving 2030 sustainable development goals for neonatal and under-five mortality [version 1; peer review: awaiting peer review]’. Osondu Ogbuoji. May, 1-15.
- Bello, A.M. and Danasabe, A.A. (2022). ‘Nigeria and Sustainable Development Goal 3: Impediments to Realistic Implementation’. International Journal of Intellectual Discourse, 5(1), pp.121-128.
- Adeyinka, D.A., Muhajarine, N., Petrucka, P. and Isaac, E.W. (2020). ‘Inequities in child survival in Nigerian communities during the Sustainable Development Goal era: Insights from analysis of 2016/2017 Multiple Indicator Cluster Survey’. BMC Public Health, 20, pp.1-18.
- Pate, M. (2017), The future of health and promise of primary health care in Nigeria. Premium Times Opinion. Available at: https://opinion.premiumtimesng.com/2017/10/21/the-future-of-health-and-promise-of-primary-health-care-in-nigeria-by-muhammad-pate/
- Eboh, I. A., Aduku, E. B., & Onwughalu, U. B. (2022). ‘Health Expenditure, Child Mortality and Economic Growth in Nigeria’. 3(3), 198-216.
- Faruk, B.U. (2020). ‘Mothers’ Literacy, Public Health Expenditure and under-five Mortality rate in Funtua Local Government Area of Katsina State’. Gusau International Journal of Management and Social Sciences, 3(1), pp.18-18.
- Ibukun, C.O., 2021. The role of governance in the health expenditure–health outcomes nexus: insights from West Africa. International Journal of Social Economics, 48(4), pp.557-570.
- Izugbara, C. (2014). ‘Whose child is dying? Household characteristics and under-5 mortality in Nigeria’. South African Journal of Child Health, 8(1), pp.16-22.
- Adeosun, O.T. and Faboya, O.M. (2020). ‘Health care expenditure and child mortality in Nigeria’. International Journal of Health Care Quality Assurance, 33(3), pp.261-275.
- Kanyuka, M., Ndawala, J., Mleme, T., Chisesa, L., Makwemba, M., Amouzou, A., Borghi, J., Daire, J., Ferrabee, R., Hazel, E. and Heidkamp, R. (2016). ‘Malawi and Millennium Development Goal 4: a Countdown to 2015 country case study’. The Lancet Global Health, 4(3), pp.e201-e214.
- Pérez, W., Peña, R., Persson, L.Å. and Källestål, C. (2011). ‘Tracking progress towards equitable child survival in a Nicaraguan community: neonatal mortality challenges to meet the MDG 4.’ BMC public health, 11, pp.1-7.
- Mosley, W.H. and Chen, L.C. (1984). ‘An analytical framework for the study of child survival in developing countries.’ Population and development review, 10, pp.25-45.