
Factors Associated with Exclusive Breastfeeding Practices in the First Six Months: A Case of Mulungushi Rural Health Centre, Mumbwa District.
- Banda Mathews Spider
- Choongo Mulungu
- 360-375
- May 30, 2024
- Public Health
Factors Associated with Exclusive Breastfeeding Practices in the First Six Months: A Case of Mulungushi Rural Health Centre, Mumbwa District.
Banda Mathews Spider1, Choongo Mulungu2*
*Corresponding Author
1University of Zambia/Ministry of Health – Mumbwa District Health Office
2University of Lusaka/Ministry of Health – Lusaka District Health Office
DOI: https://dx.doi.org/10.47772/IJRISS.2024.805026
Received: 31 March 2024; Revised: 22 April 2024; Accepted: 01 May 2024; Published: 29 May 2024
ABSTRACT
Exclusive Breast Feeding (EBF), the best feeding practice for infants from birth to six (6) months, has faced challenges of adherence, exposing infants to infections such as diarrhea, despite information on its importance being given to mothers. The main objective of this study was to assess factors associated with inadequate exclusive breastfeeding practices towards children in the first 6 months, particularly at Mulungushi Rural Health Centre in Mumbwa District. A descriptive cross-sectional study involving 192 breast-feeding mothers selected using systematic sampling method was conducted in Mumbwa. The respondents were interviewed using a structured questionnaire at study sites. The study found that the prevalence of exclusive breast-feeding practice was at 47%. The factors that were found to be statistically significant to exclusive breastfeeding were age of infant, educational level, parity, occupation of the mother, number of meals mothers ate per day, child spacing and support breastfeeding mothers received. The study revealed that mothers found it difficult to practice Exclusive Breastfeeding because of the amount of work at home, some feared to transmit the HIV to their babies, some because of the business trips, those in employment stated that the conditions at work were not very conducive for breastfeeding and spouses found it difficult to help with house chores because culturally it was a woman’s work. Despite the respondents having adequate knowledge about the importance of EBF, the practice was still below what WHO recommendation of (60%), thus there was still need to strengthen the practice in the study area through education of spouses, family and the community on infant feeding for them to support breastfeeding mothers. Government to develop a policy to allow for time for working breastfeeding mothers to be given time to breastfeed their babies in the first 6 months at work.
Key Terms: Exclusive Breastfeeding, Mothers, Rural, Practices, First 6 Months
BACKGROUND
Exclusive Breastfeeding has been defined by the World Health Organization as a practice where the infant has to receive only breast milk from his/her mother or expressed breast milk, and no other liquids or solids, except drops or syrups of vitamins, mineral supplements or medicines (WHO, 2015). Milk is the primary source of nutrition for newborns before being able to digest other foods other than milk (WHO, 2001). Breastfeeding offers health benefits to mother and child, birth spacing through lactation amenorrhea and motor and cognitive development in childhood of the child (Black, et al., 2013). Breast milk is the ideal food for infants, providing essential nutrients, antibodies, and hormones necessary for their growth and immune system development. It adapts to meet the changing needs of the growing baby. UNICEF recommended exclusive breastfeeding for 6 months of life and continued breastfeeding up to two years of age or beyond (UNICEF, 2016).Thereafter, infants and young children should be given nutritionally and adequate, safe, complementary foods from the age of 6 months to meet the evolving needs of their growing bodies. Mothers should continue breastfeeding up to the age of 2 years or beyond as this has numerous benefits for both infant and maternal health.
An appropriate feeding practice is important in survival, growth and development (WHO, 2013). For example, breast milk is important as it helps decrease the risk of infectious and chronic diseases, including diarrhea and respiratory tract infections, especially during infancy (Ijumba2014). Exclusive breastfeeding can further provide numerous health benefits for infants, including protection against infections such as diarrhea and pneumonia, reduced risk of allergies and chronic diseases, and optimal nutrition for healthy growth and development. Furthermore, mothers with shorter breastfeeding duration have an increased risk of breast and ovarian cancer, type 2 diabetes and hypertension.Withdrawing the process of breastfeeding before the time recommended to children pauses a high risk of infections to infants and causes mortality (Victora, et al., 2016).
Withdrawing breastfeeding before the time gave birth to The Infant & Young Child Nutrition (IYCN) Project, as the flagship project on infant and young child nutrition of the US Agency for International Development (USAID) which aims to improve nutrition for mothers, infants, and young children, and promote HIV-free survival of infants and children. Today, health workers and Community Health Volunteers are instructed and mandated to counsel HIV-positive mothers to exclusively breastfeed their infants for six months unless replacement feeding is affordable, feasible, acceptable, sustainable, and safe, for an HIV-positive woman to breastfeed (USAID, 2010).
IYCN is supporting training of health providers in infant and young child feeding within the context of HIV, providing technical assistance to improve the national infant and young child feeding curriculum, strengthening training sessions, designing a supportive supervision system, and training providers. Additionally, IYCN supports nutrition counseling and clinical referrals for HIV-positive mothers, their children, and other orphans and vulnerable children through activities at the community level that exclusive breastfeeding practice is now a leading intervention in promoting Child Health Survival and a single most effective intervention that could prevent 13 – 15% of infant’s deaths. The practice is recommended by the World Health Organization and United Nations Children’s Funds (World Health Organization, 2012). Globally, it is estimated that less than 39% of infants are exclusively breastfed for the first four months of life. Stunting prevalence worldwide is about 21-33%, and indicated as one of the factors caused by inadequate exclusive breastfeeding for the six months of life (Victora, et al., 2016). Non–exclusive breastfeeding additionally has future impact, including poor school performance, reduced productivity, and impaired intellectual and social development. It can also increase the danger of dying as a result of diarrhea and pneumonia during the first five months of age by more than twofold (Gawhara, Gad, Soliman, Ebrahem1, & et.al, 2019).
In Sub-Saharan African countries, exclusive breastfeeding rate for six months is about 30% (UNICEF 2016), 47% in Ethiopia, 13% in Kenya (Kiboi & Patrick, 2017) and 50% in Tanzania (Leshabari, Blystad, de Paoli, & Moland, 2007). Although the CDC reported that, breastfeeding is rising by 2% (CDC, 2007). One of the studies indicated that, the race, maternal age, maternal occupation, parent’s educational level, social-economic status, insufficient milk supply, infant health problems, maternal obesity, smoking, parity, method of delivery, maternal interest, social culture, and lack of knowledge were factors that caused inadequate exclusive breastfeeding (Roudbari, 2015).
In countries like Ethiopia, exclusive breastfeeding was recorded to be 47% in 2012, while in Nigeria the rate was 20% (Setegn, 2012). The major factors causing inadequate/poor EBF in Tanzania for example were inadequate advice and support on how to feed their child (Mahesh Sarki & et.al, 2018). A study conducted in Mexico to assess the association between working mothers and breastfeeding using secondary data source from three national health surveys (1999, 2006 & 2012), the findings of the study suggest that maternal full-time employment was negatively associated with breastfeeding mothers with a child under age one year. The study elaborated that full time employed mothers were 20% less likely to breastfeed compared to part-time employed mothers. While, full time employed mothers were 27% less likely to breastfeed compared to non-employed mothers (WHO, 2011).
Economic factors, mother’s age, perception of mothers on sufficiency of breast milk and social cultural influence has been associated with inadequate breastfeeding in Tanzania (Leshabari, Blystad, de Paoli, & Moland, 2007). Data from Tanzania Demographic Health Survey indicated that an exclusive breastfeeding practice for the six months of an infant’s life is not widely practiced. The National rate of exclusive breastfeeding in Tanzania being 50% regardless of mother’s HIV status, only 49% of children breastfed within an hour of birth.
A study done at Morogoro, Kilimanjaro, and Igunga district, shows that EBF is not widely practiced, only 9% of nursing mother practiced exclusive breastfeeding in Dar-es-salaam regional (Shirima, Greiner, Kylberg, & Gebre-Medhim, 2011) whereby EBF practices in HIV positive mothers is high from birth to 2 months (80%), decreasing rapidly at age 3 to 4 months 34% and lowest among infants of six months 13.3% (Shirima, Greiner, Kylberg, & Gebre-Medhim, 2011). The percentage is below the National prevalence of 41% (Shirima, Greiner, Kylberg, & Gebre-Medhim, 2011). Most factors identified were cultural beliefs which hinder exclusive breastfeeding, whereby more than half of infants are supplemented early and the majority of mothers have inadequate knowledge on exclusive breastfeeding (Shirima, Greiner, Kylberg, & Gebre-Medhim, 2011)
Another study conducted in South Africa the neighboring country to Zambia revealed that although the initiation of breastfeeding was immediate and prevalent, with 79% of children fed with colostrum, exclusive breastfeeding for the 6 months of life was rarely practiced; only 36% of the children were exclusively breastfed for the 6 months of life, with substitute (49%) being common although mixed feeding was practiced (Gamuchirai, 2020; Chakona, 2020).
Zambia adopted exclusive breastfeeding as a method of infant feeding from birth to six months and unless replacement feeding was Acceptable, Feasible, Affordable, Sustainable and Safe (Tembo & Ngoma, 2015). In Zambia, the 2018 ZDHS reported that mortality during the first month (neonatal mortality), is higher than post neonatal mortality (27 deaths per 1,000 births versus 14 deaths per 1,000 births) and accounts for 64% of the overall infant mortality and the common cause of death was poor breastfeeding practices especially among first time mothers.
The target of Zambia for Exclusive breastfeeding for the six months of life is 60%, however, the prevalence of EBF in Zambia is at 61% (Tembo & Ngoma, 2015), (ZamStat, 2019). Despite the great advances in health services in Zambia, the 2018 ZDHS report states that the practice of EBF dropped from 65% at 2 – 3 months to 35% at 4 – 5 months of age. A study in Luangwa which considered breastfeeding practices in the area concluded that despite exclusive breastfeeding practice having improved in the district, there was still a need to strengthen the practice in the district through education of spouses, family and the community on infant feeding for them to support breastfeeding mothers. 62% of children aged 4-5 months are receiving food supplements to breast milk (ZamStat, Zambia Demographic and Health Survey, 2019). Another research which was carried out in Chadiza district area, under the program of PMTCT, reported that nursing mothers who had received adequate counseling on exclusive breastfeeding had a higher rate of practicing exclusive breastfeeding than those who do not, 56% to 70 % (Kiboi & Patrick, 2017).
Despite the benefits of exclusive breastfeeding, there are challenges in promoting and practicing it effectively. These challenges may include inadequate support for breastfeeding mothers, lack of knowledge about breastfeeding benefits, misinformation, stigma surrounding breastfeeding in public spaces, and barriers to accessing maternal healthcare services.
Efforts have been made by the Zambian Government, Donors, NGO and other stakeholder to protect, support and promote and meet the target for exclusive breastfeeding for the first six months of life which stands at 60% (ZamStat, 2019). Some of the efforts and initiatives include and not limited to breastfeeding education campaigns, training for healthcare providers, establishing breastfeeding-friendly workplaces and public spaces, and providing support to mothers through community programs and healthcare services.
Efforts to promote exclusive breastfeeding have led to increased awareness among Zambian mothers about its importance for infant health and nutrition. However, further efforts are needed to address remaining barriers and ensure widespread adoption of exclusive breastfeeding practices across all communities. However, the ZDHS, 2018 hypothesized that in Zambia, 35% of children under five are stunted, 4% wasted, or thin for their height, 12% of children under five are underweight, or too thin for their age, while 5% are overweight (Zambia Statistics Agency, 2019).
In this context, increasing breastfeeding rates is a strategic priority in Zambia. However, understanding the determinants of breastfeeding behavior as well as IYCF practices are a critical step towards the prevention of undernutrition in young children and decreasing the risk of infant morbidity and mortality within vulnerable settings in the country. Maternal characteristics such as age and education, household demographic such as household size and household head and socioeconomic factors such as income and employment status, have been implicated in driving poor IYCF practices. Furthermore, cultural beliefs such as food taboos and perceptions by mothers, households and communities also influence breastfeeding behavior and complementary feeding, including the types of foods young children are given. Grandmothers’ knowledge and their decisions were also regarded as critical for early child feeding practices in other communities (Zambia Statistics Agency, 2019).
Generally, in some parts of Zambia’s communities, various socioeconomic factors influenced breastfeeding practices, these may include cultural beliefs, traditional feeding practices, maternal education, employment status, access to healthcare services, and support from family and communities.
Therefore, this study intended to add knowledge on determining factors associated with inadequate exclusive breastfeeding practices in the first 6 months in the Mulungushi area of Mumbwa District.
METHODS AND MATERIALS
This was a mixed methods study employing a descriptive cross-sectional survey approach. It involved non-experimental procedures for the mothers and healthcare workers in study. This design was aimed at determining the current status of the population with regard to one or more variables. The design was suitable for study because data was intended to describe the existing conditions. A standardized questionnaire covering demographic information; socio-economic, knowledge and attitude and service related information with regards to breastfeeding practices among the 192breast feeding mothers of Mulungushi Rural Health Centre, Mumbwa district was used for data collection purposes.
Participants
This study was conducted from Mulungushi Rural Health Center catchment area, Mumbwa district. The facility has a total population of 7,805 and attends to not less than 700 patients per week. The site was purposely selected because it was easy for the researcher to reach respondents. Expenses such as transport were reduced because all respondents were confined within the area. The main activities performed are clinical service, clinical support, mother and child services and diagnostic activities, (ZDHS, 2019).
The sample size was composed of one ninety-four (192) breastfeeding mothers. This was due to the approximated number of thebreastfeeding mothers as per population size of 372 possible expected breastfeeding mothers at the time the research was being conducted. The sample size was calculated using Yamane’s (1973) formula: n=N/1+N(e)2
A systematic random sampling method was used to select the participants. The majority of the respondents (n=117, p=60.9%) were in the age group 20 – 30 years, followed by those between ages 31 – 40 years (n=41, p=21.4%), while (n=22, p=11.5%) were < 20 years and the least being those aged > 40 years were in the minority (n=12, p=6.3%). Further, the mean age of the sample population was 27.51 years with a standard deviation (SD) of 6.730 years with the age range of 14 years to 48 years.
The majority of the participants were married or had a partner (n=121, p=63%); (n=39, p=20.3%) were single; and another (n=17, p=8.9%) were either divorced or separated; 9(4.7%) were cohabiting and the minority group 6(3.1%) were widowed. Of the 192 participants, (n=114, p=59.4%) were primiparous and the least fraction (n=78, p=40.6%) were multiparous.
On the education level, the majority of participants (n=101, p=52.6%) attained primary education; whilst 51(26.6%) had attained secondary education; with (n=28, p=14.6%) without any formal education. Those with tertiary education were only (n=12, p=6.3%).
The majority of the participants (n=161, p=83.9%) were not in formal employment; 20(10.4%) were in employment and whilst (n=11, p=5.7%) were in self-employment and businesses. On the actual type of work the participants were doing, (n=98, p=58%) of the participants were farmers; (n=39, p=20.3%) were business-oriented participants; (n=18, p=9.4%) were in some employment whereas (n=37, p=19.3%) represented those that were homemakers.
Instruments
This study used two instruments for data collection namely; a questionnaire for quantitative and qualitative data from breastfeeding mothers and an interview guide for qualitative data from Key Informants that included health workers and community health workers.
Questionnaires increased the chances of getting honest responses since they ensured anonymity of the respondent. The questionnaire used both open-ended and closed ended questions. The use of open-ended questions offered flexibility for the respondents to provide more details. Closed ended questions allowed for quantitative analysis. This balance was useful for a comprehensive analysis.
An interview is a purposeful conversation in which one person asks prepared questions and another answers them. This is so to gain information on a particular topic or a particular area to be researched. The use of the interview approach is flexible, providing a large amount of detail.
Data Analysis
Descriptive analysis was used in the study and it provided the researcher with profiles of the study population such as their size, composition, efficiency, preferences and so on. In this case, data quality control and cleaning commenced in the field by the researchers ensuring that all the information on the questionnaires had been properly collected, recorded and checked for completeness of data and internal consistency. Data analysis was done after all data captured was entered. Closed-ended questions were analyzed using nominal scales into mutually exclusive categories and frequencies by employing descriptive statistics using the Statistical Package for Social Sciences version (v 22) and MS Excel. Open-ended questions were analyzed using conceptual content analysis. Analysis involved the production and interpretation of frequencies, counts, tables and graphs that described and summarized the data. To examine the relation between independent variables of the respondents, an independent sample t-test, one-way analysis of variance test of significance, and multiple linear regressions was used. The correlation coefficient was used to determine the type of relationship that existed between the independent variables and the p-value indicated if the relationship was significant or not. We further triangulated the responses from key informants to analyze and determine common themes emerging from their responses, looking at the number of key informants, the themes that were held by more than two informants were considered for a frequency count and further presented as verbatims in this study.
Data Collection Procedure
Once the proposal was approved by the University Public Health Department Faculty and the UNZA Biomedical Research Ethics Committee (REF. NO. 3500-2022), the researchers started the data collection processby seeking permission from the Mumbwa District Health Office and the management team of Mulungushi RHC catchment area.
This study sought help from the community health workers as the research assistants; they were trained on the tools and issued with the questionnaires to administer to the breastfeeding mothers during an under five session. Being aware of the challenges involved in interviews, the researchers made adequate preparations to maximize the chances of successful interviews. This was accomplished by informing the service providers about the study and requesting interviews with them.
RESULTS
The findings for both quantitative and qualitative inquiry conducted on the exclusive breastfeeding in Mumbwa are presented under themes that were derived from the research objectives. The themes were subdivided to provide relevant data, as contained in the questionnaire and interview schedules. A total of 192 breastfeeding mothers were enrolled in the study and the data were collected between January 2023 and April 2023.
Place of Delivery
The figure 1 below shows that the majority of the respondents (n=152, p=79.2%) delivered from the Hospital whilst only (n=2, p=1%) respondents had deliveries assisted by the traditional birth attendants. On the other hand, (n=2, p=1%) were home deliveries.
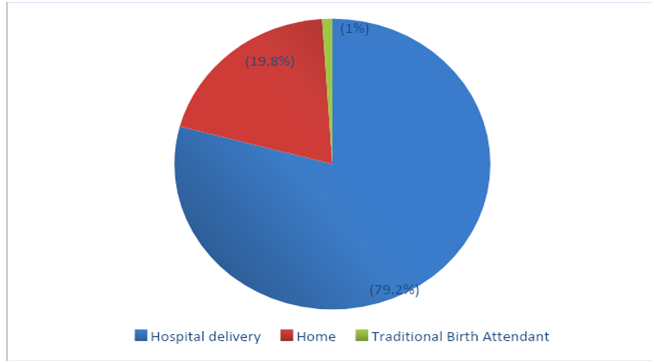
Figure 1: Respondents Place of Delivery
We sought to understand what influenced the place of delivery among mothers in the catchment area despite the emphasis placed on it as mothers attended antenatal clinics. We interviewed key informants and women provided their responses through open ended questionnaire sections and the following are commonly held positions.
There are many factors that lead to delivery outside the facility but the most common reason among mothers in our catchment is beliefs passed on by elderly community women. However, the number dwindled because the Headmen and their committees had adopted the system of making mothers pay during postnatal visits if they happen to deliver away from the health facilities (KI -Clinic).
These days, are there women that want to deliver from home? Only a few that believe in traditional cleansing and what older women say do that although it is not common (KI – Woman).
Mode of Delivery
Figure 2 shows the mode of delivery that the respondents in the study underwent as they were giving birth to the baby they were breastfeeding at the time of data collection. The study found that (n=169, p=88%) of the total respondents delivered normally (normal vaginal delivery), (n=15, p=8%) had caesarean section and the lowest fraction was that of the assisted deliver (n=8, p=4%).
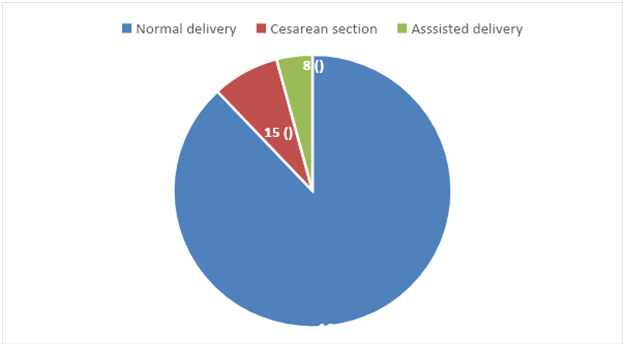
Figure 2: Respondents Mode of Delivery
Time of Introduction of the Supplementary Food to the Child
The Pie chart below shows the time in months when the supplementary food was introduced to the child. Of the 192 respondents, (n=91, n=47%) introduced food at 6 months, (n=64, p=33%) introduced food between 4 to 5 months, (n=34, p=18%) respondents introduced food to the child between 1 to 3 months and (n=3, p=2%) introduced food the time the child was less than 1 month old.
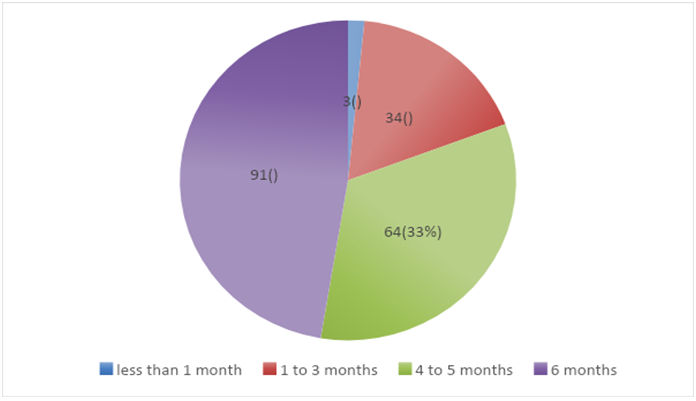
Figure 3: Time of Introduction of the Supplementary Food to the Child
Based on a big number of women (33%) introducing supplementary foods for their infants around the fourth month, we sought to understand the associated factors. The majority of the women that introduced supplementary foods were from the working class.
Well for me I started a month after I reported back to work. We are only given three months of leave at work so after observing that pumping milk was not that helpful I decided to start using formula (KI – Mother).
Most of us mothers due to pressure at the farm, mostly during the rainy season, we resort into giving extra food stuffs to our babies because we stay long hours working at the farm (KI – Mother).
Time of Initiating Breastfeeding after Delivery.
Figure 4 shows the time when breastfeeding was initiated to the baby after delivery. The study found that (n=79, p=41%) of respondents had initiated breastfeeding within 1 hour after delivery, (n=52, p=27%) respondents only initiated breastfeeding between 2-3 hours after delivery while (n=44, p=23%) of the respondents initiated breastfeeding immediately after delivery and (n=17, p=9%) respondents only initiated breastfeeding after a day or more.
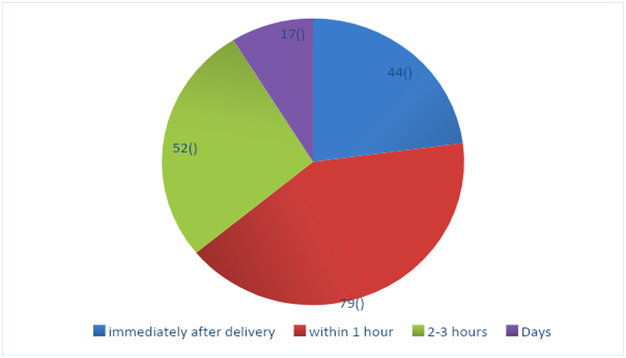
Figure 4: Initiation of Breastfeeding after Delivery
Exclusive Breastfeeding and Age of the Mother
Table 1 below illustrates the relationship between exclusive breastfeeding and age of the mother. The Chi–square test conducted at 95% confidence level showed that it was 2.216 and the p–value was 0.529. This indicated that there was no statistical significance or association between age of the mother and exclusive breastfeeding practice. It therefore means that the age of the mother does not influence the decision to practice exclusive breastfeeding or not.
Table 1: Relation between Exclusive Breastfeeding and Age of the Mother
| Exclusive Breastfeeding Practice | Age of the mother |
P – value |
||||
| <20 years | 20-30 years | 31-40 years | >40 years | Total | ||
| Exclusive Breastfeeding | 13 | 56 | 21 | 8 | 98 | 0.529
(Chi – Square) x2=2.216 |
| Non-Exclusive Breastfeeding | 9 | 61 | 20 | 4 | 94 | |
| Total | 22 | 117 | 41 | 12 | 192 | |
Exclusive Breastfeeding and Parity
Table 2 below shows the relationship between exclusive breastfeeding practices and parity of the breastfeeding mother interviewed. The Chi – square test conducted at 95% confidence level showed that it was 4.464 with a p–value of 0.035. This result indicated that there was a statistical significance or association between exclusive breastfeeding practices and parity. The number of pregnancies had an influence on the exclusive breastfeeding practice among mothers with primiparous less likely to breastfeed exclusively compared with multiparous.
Table 2: Relation between Exclusive Breastfeeding and Parity
| Exclusive Breastfeeding Status | Parity | |||
| Primiparous | Multiparous | Total | P – value | |
| Exclusive Breastfeeding | 51 | 47 | 98 | 0.035
(Chi – Square) X2 = 4.464 |
| Non-Exclusive Breastfeeding | 63 | 31 | 94 | |
| Total | 114 | 78 | 192 | |
Exclusive Breastfeeding and Education Level
Table 3 below illustrates the relationship between exclusive breastfeeding practices and level of education. The Chi – square test conducted at 95% confidence level showed that it was 21.497 with a P – value of 0.000. This result indicated that there was a statistical significance or association between exclusive breastfeeding practices and education level.
We observed that some mothers with tertiary education had poor exclusive breastfeeding practices. However, with the explanation we got regarding working women, an association was connected to their level of education.
Table 3: Relationship between EBF and Education Level
| Exclusive Breastfeeding Status | Education Level | P – value | ||||
| No Formal Education | Primary Education | Secondary Education | College education | Total | ||
| Exclusive Breastfeeding | 7 | 45 | 37 | 9 | 98 | 0.000(Chi – Square)
x2=21.497 |
| Non-Exclusive Breastfeeding | 21 | 56 | 14 | 3 | 94 | |
| Total | 28 | 101 | 51 | 12 | 192 | |
Exclusive Breastfeeding and Occupation
Table 4 illustrates the relationship between exclusive breastfeeding practices and occupation. The Chi – square test conducted at 95% confidence level showed that it was 12.882 with a P – value of 0.005. This result indicated that there was a statistical significance or association between exclusive breastfeeding practices and the mother occupation
Table 4: Relation between Exclusive Breastfeeding and Occupation
| Exclusive Breastfeeding Status | Occupation |
P – value |
||||
| Employed | Farmer | Business | None | Total | ||
| Exclusive Breastfeeding | 12 | 58 | 11 | 17 | 98 | 0.005
(Chi-Square) X2 = 12.882 |
| Non-Exclusive Breastfeeding | 6 | 40 | 28 | 20 | 94 | |
| Total | 18 | 98 | 39 | 37 | 192 | |
Exclusive Breastfeeding and Initiation of Breastfeeding after Delivery
Table 5 below illustrates the relationship between exclusive breastfeeding practices and Initiation of breastfeeding after delivery. The Chi – square test conducted at 95% confidence level showed that it was 13.690 with a P – value of 0.003. This result indicates that there was a statistical significance or association between exclusive breastfeeding practices and time breastfeeding was initiated after delivery.
Table 5: Relationship between EBF and Initiation of Breastfeeding after Delivery
| Exclusive Breastfeeding Status | Initiation of breastfeeding after delivery | P – value | ||||
| Immediately after delivery | Within 1 hour | 2-3 hours | Days | Total | ||
| Exclusive Breastfeeding | 31 | 41 | 17 | 9 | 98 | 0.003
(Chi – Square) x2=13.690 |
| Non-Exclusive Breastfeeding | 13 | 38 | 35 | 8 | 94 | |
| Total | 44 | 79 | 52 | 17 | 192 | |
Exclusive Breastfeeding and Introduction of Supplementary Feeding
Table 6 below, illustrates the relationship between exclusive breastfeeding practices and Introduction of Supplementary Feeding. The Chi – square test conducted at 95% confidence levels showed that it was 15.595 with a P – value of 0.001. This result indicated that there was a statistical significance or association between exclusive breastfeeding practices and introduction of supplementary feeding.
Table 6: Relationship between EBF and Introduction of Supplementary Feeding
| Exclusive Breastfeeding Status | Introduction of Supplementary Feeding | P – value | ||||
| < 1 Months | 1-3 Months | 4-5 Months | At 6 Months | Total | ||
| Exclusive Breastfeeding | 2 | 10 | 27 | 59 | 98 | 0.001
(Chi – Square) x2=15.595 |
| Non-Exclusive Breastfeeding | 1 | 24 | 37 | 32 | 94 | |
| Total | 3 | 34 | 64 | 91 | 192 | |
Exclusive Breastfeeding and Mothers Number of Meals
Table 7 below illustrates the relationship between exclusive breastfeeding practices and Number of Meals mothers have per day. The Chi – square test conducted at 95% confidence levels shows that it was 15.397 with a P – value of 0.002. This result indicated that there was a statistical significance or association between exclusive breastfeeding practices and Number of Meals mothers have per day.
Table 7: Relationship between EBF and Number of Meals mothers had per day
| Exclusive Breastfeeding Status | Number of Meals mothers have per day |
P – value |
||||
| < 3 times per day | At least 3 times per day | > 3 times per days | On demand | Total | ||
| Exclusive Breastfeeding | 22 | 55 | 17 | 4 | 98 | 0.002
(Chi – Square) x2=15.397 |
| Non-Exclusive Breast feeding | 41 | 33 | 20 | 0 | 94 | |
| Total | 63 | 88 | 37 | 4 | 192 | |
Exclusive Breastfeeding and Child Spacing
Table 8 below illustrates the relationship between exclusive breastfeeding practices and child spacing. The Chi – square test conducted at 95% confidence levels shows that it was 28.252 with a P – value of 0.000. This result indicated that there was a statistical significance or association between exclusive breastfeeding practices and child spacing.
Table 8: Relationship between EBF and Child Spacing
| Exclusive Breastfeeding Status | Child Spacing | |||||
| 0-1 Year | 2 Years | 3 Years | Other | Total | P – value | |
| Exclusive Breastfeeding | 18 | 27 | 25 | 28 | 98 | 0.00
(Chi – Square) x2=28.252 |
| Non-Exclusive Breast feeding | 26 | 49 | 15 | 4 | 94 | |
| Total | 44 | 76 | 40 | 32 | 192 | |
Exclusive Breastfeeding and HIV Status
Table 9 below illustrates the relationship between exclusive breastfeeding practices and HIV status. The Chi – square test conducted showed that at 95% confidence level it was 1.362 and the P – value was 0.243. This indicated that there was no statistical significance or association between exclusive breast feeding and HIV status.
Table 9: Relationship between EBF and HIV status
| Exclusive Breastfeeding Status | HIV status | |||
| Negative result | Positive result | Total | P – value | |
| Exclusive Breast feeding | 77 | 21 | 98 | (Chi – Square) = 0.243
x2=1.362 |
| Non-Exclusive Breastfeeding | 67 | 27 | 94 | |
| Total | 114 | 48 | 192 | |
Regression Analysis Outcome
A one-way ANOVA was conducted to determine the effect of parity, age of the mother, age of the child and number of meals mothers eat per day. The table below shows the output of the ANOVA analysis and whether there was a statistical significance among the variables
Table 10: ANOVA
| Model | Sum of Squares | Df | Mean Square | F | Sig. | |
| Regression | 2.960 | 4 | .740 | 3.074 | .018b | |
| Residual | 45.019 | 187 | .241 | |||
| Total | 47.979 | 191 | ||||
- Predictors: (Constant), age of the child, number of meals mother eats, parity, and age of mother
- Dependent Variable: Exclusive breastfeeding practice
A one-way ANOVA test was performed to predict the influence age of the child, number of meals mother eat, parity, and age of the mother as predictors of exclusive breastfeeding practice among 192 breastfeeding mothers. The outcome showed that the one-way ANOVA model was statistically significant (p < 0.05). A one-way ANOVA revealed that there was a statistically significant difference among the predictor variables on exclusive breastfeeding practice F (4, 187) = 3.074, p = 0.018, df = 4.
Table 12: Model Summar
| R | R Square | Adjusted R Square | Std. Error of the Estimate | Change Statistics | ||||
| R Square Change | F Change | df1 | df2 | Sig. F Change | ||||
| .230a | .053 | .043 | .490 | .053 | 5.290 | 2 | 189 | .006 |
- Predictors: (Constant), age of the child, number of meals mother eat, parity, and segment age
- Dependent Variable: Exclusive breastfeeding practice
The model summary above, revealed that the R = 0. 230, R square of 0.053 And Adjusted R square of .043 which indicated a relationship between prediction and grouping. This means that some of the variables were statistically significant to the prediction, P – value = 0.006. These variables are parity and number of meals the mother was taking.
DISCUSSION AND IMPLICATIONS
Exclusive Breastfeeding in Mulungushi, Mumbwa
The findings of this study showed that the proportion of respondents who knew what exclusive breastfeeding was 45.8% despite the majority 79.2% acknowledging that health education on EBF was being provided by health workers. Only 53.3% of the respondents stated that all babies should be exclusively breastfed during the first six months of life. This finding could be attributed to the respondents’ inadequate knowledge on the subject of exclusive breastfeeding. This was likely to be the factor affecting the adoption of exclusive breastfeeding practices at Mulungushi RHC. Infants are expected to be exclusively breast fed from birth to six months because breast milk is a natural food that supplies all the vital nutrients an infant requires during this period (Fraser, Cooper, & Nolte, 2015). The study revealed that the prevalence of exclusive breastfeeding practice was at 47%, a finding which was below the national target of 80% (NFNC, 2022). The results of Mulungushi were slightly lower than the findings in Mazabuka where 68.8% of infants were exclusively breast fed and those of Kafue where 53% of infants were exclusively breast fed (Tembo & Ngoma, 2015). The variations could have been due to the different social context of the three settings where the researches were conducted from. Other fluids and foods were given to some infants and reasons given for the practice were insufficient breast milk.
Exclusive Breastfeeding and Level of Education
The study showed that there was an association between exclusive breastfeeding practice and educational level of the mother (p=0.000). However, it was observed that the twelve (12) mothers who had attained college education exclusively breast fed their infants and that may point to an influence of occupation status of the mother on feeding practice owing to their level of education. This finding is contrary to other studies in Spain, Ghana and other countries which revealed that mothers’ levels of education are not associated with breastfeeding although higher education levels were related to positive trends of feeding (Ordenana, Colodro, & Tornero, 2011).
In this study, marital status was not related with the respondent’s level of knowledge on EBF (P-value = 0.415). These findings agreed with the study Musonda Chilufya (2018), who also reported that marital status was not related with the respondent’s level of knowledge on EBF. It should be noted that two findings were not in line with a study conducted by the American Academy of Paediatrics (2017) which stated that single mothers have great difficulty supporting themselves and caring for the baby especially if they are young. These findings also argue with another study which concluded that without husbands’ support, activities outside the home such as having to work might prevent EBF practices(American Pediatrics Academy, 2017).
Exclusive Breastfeeding and Occupation
Occupation of the mother in this study was found to have an effect on the level of knowledge on EBF (P value = 0.005). The participants involved in the study were either formally employed farmers or they were into business or some farming and others were just homemakers who had exhibited less or no knowledge on EBF practices at all. Those that were in formal employment, some found it difficult to breastfeed due to tight work schedules more especially among those working from the mines where women work long hours in non-conducive environments for carrying babies to work or breastfeeding. This finding was in line with the study conducted by Musonda (2018) who stated that other women found it hard to maintain their milk supply when separated from their babies and were forced to stop breastfeeding. Another scholar also agrees with this finding by stating that maternal employment outside the home is often cited as a major factor in short- term breastfeeding patterns seen throughout the world (Perry, 2003)
Exclusive Breastfeeding and Parity
It is believed that multiparas are more likely to initiate breastfeeding and have longer breastfeeding duration (Zafar et al. 2021; Hackman et al. 2015). Consistent with this our study also found statistical significance or association between exclusive breastfeeding practices and parity (P – value of 0.035). It was noted that participants who had many children, practiced breastfeeding more than those who had 1, 2 and or 3 children. This could have been due to the fact that as the number of children increased, the more knowledgeable the mother could become on the importance of breast milk to the baby. On the contrary, Mohamed et al. (2018) found that there were no differences in the early infant feeding practices between primiparous and multiparous mothers.
In our study we observed that the older the child, mothers introduced other foods before reaching the age of six months. At the age of 6 months, only 91 (47%) of infants were exclusively breast fed. The findings showed some significant relationship between Exclusive breastfeeding and age of an infant (P-value=0.001). These results were higher than the findings of the study which was conducted in Luangwa which had 10% of infants who were exclusively breast fed at the same age (Tembo & Ngoma, 2015).
Exclusive Breastfeeding and Place of Delivery
In this study, place of delivery was statistically significant on the EBF practices among respondents. Those that delivered their babies from the health facilities exhibited more knowledge on breastfeeding than the ones who delivered either from home or were attended to by the birth attendants. The findings in this study agreed with the study which was carried out in Chadiza district area, under the program of PMTCT, reported that nursing mother who had received adequate counseling on exclusive breastfeeding from the health facilities mostly before and during labor had high rate of practicing exclusive breastfeeding than those who do not, 56% to 70 % (Kiboi & Patrick, 2017)
Some hospital policies in this study proved to have an effect on breastfeeding practices, such as delay of skin-to-skin contact, separation of mothers and newborns, and supplementation of breast milk with infant formula (P – value of 0.003). Some respondents lamented that they could not initiate breastfeeding immediately due to some medical conditions suffered before and or during labor phases such as Covid-19. Thrower & Peoples in 2015, lamented that routine hospital activity may delay breastfeeding. This could be due to maternal cesarean section or hospital policies that may make a separation between mothers and infants to give mothers a period to rest after delivery (Gardner, Green, & Gardner, 2015).
Most of the respondents in this study reported that they received support from health professionals which was in a form of education on infant feeding. Despite education being given, 52.6% of respondents practiced mixed feeding and by the age of 4-5 months, only 10(16%) of infants were exclusively breast fed which is low. Furthermore, some mothers reported receiving support from other people for example spouses, grandmothers and mothers. It was interesting to note that the mothers who received support from their grandmothers, were able to exclusively breast feed their infants.
CONCLUSION
The purpose of the study was to assess factors associated with inadequate exclusive breastfeeding practices at Mulungushi RHC, Mumbwa District. The prevalence of exclusive breastfeeding in this study was lower at 47% below the National target of 80%. There was still a need to strengthen the practice because mixed feeding was still being practiced in infants below six months of age. The factors that were significant to exclusive breastfeeding were age of infant and support. Mothers received support from health professionals but probably they were not able to comprehend information due to low levels of education. Support received from spouses, mothers, and grandmothers may have had gaps due to insufficient knowledge on exclusive breastfeeding among them. Focus group discussions revealed that mixed feeding was a common practice by mothers in the community which probably meant that there was influence from the community. The other factors were age of the mother, HIV status of the mother and support from spouse which were found not to be statistically significant to exclusive breastfeeding. We recommended that the family and community must be educated on the importance of exclusive breastfeeding for them to effectively support breastfeeding mothers. There is a need to continue encouraging mothers who may be willing to go back to school to further their education. We also recommend the government to develop a policy to allow for time for working breastfeeding mothers to be given time to breastfeed their babies in the first 6 months at work.
REFERENCES
- Abdulmalek. (2008). Factors Affecting Exclusive Breastfeeding Practices in Benghazi, Libya. Libyan Journal of Science and Technology, 7(1), 36-38.
- Allen, L., & Haskell, M. (2001). Vitamin A Requirements of Infants Under Six Months. Food and Nutrition Bulletin, 22(3) :(P)214-234.
- Alyousefi, N., Alharbi, A., Almugheerah, B., & et.al. (2017). ‘Factors influencing Saudi mothers’ success in exclusive breastfeeding for the first six months of infant life: a cross-sectional observational study’. Int J Med Res Health Sci., 6, pp. 68–78 [6].
- Alzaheb, R. A. (2016). Factors Associated with The Early Introduction of Complementary Feeding in Saudi Arabia. Int J Environ Res Public Health. 2016 Jul, 13(7): 702.
- American Pediatrics Academy. (2017). Breastfeeding and the use of human milk. Pediatrics., 129(3), e827-e841. Doi:10.1542/peds.2011-3552.
- Batal, M., Boulghourjian, C., Abdallah, A., & Afifi, R. (2005). Breast-Feeding and Feeding Practices of Infants in a Developing Country, National Survey in Lebanon. Public Health Nutrition, 9; (P) 13-319.
- Bezner Kerr, R., Dakishoni, L., Shumba, L., Msachi, R., & Chirwa, M. (2008). ‘We Grandmothers Know Plenty’: Breastfeeding, Complementary Feeding and The Multifaceted Role of Grandmothers in Malawi. Soc Sci Med., 662008;66:1095–10.
- Black, R. E., Victora, C., Walker, S., Bhutta, Z. A., Christian, P., M, O., & et.al. (2013). Maternal and Child Under Nutrition and Overweight in Low-income and Middle-income Countries. Lancet, 382(9890) :(p)427–51.
- Burns, N., & Groove, S. (1993). The Practice of Nursing Research. Philadelphia. Randomized Trial. Journal of Human Lactation, (15) 125-130.
- CDC. (2007). Breastfeeding Report, United States 2012. Retrieved from http://www.cdc.gov/breastfeeding/pdf/2012Breastfeeding
- Dop, M. C. (2002). Breastfeeding in Africa:Will Positive Trends Be Challenged by The AIDS Epidemic? Sante, African Journal 12(1): 64-72.
- Elizabeth, W., Kimani-Murage, & et.al. (2014). Factors Affecting Actualization of The WHO Breastfeeding Recommendations in Urban Poor Settings in Kenya. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal and Child Nutrition, 11, pp. 314–332.
- Fraser, D., Cooper, M., & Nolte, A. (2015). Myles Textbook for Midwives. Elsevier: Churchill.
- Gamuchirai, C. (2020). Social Circumstances and Cultural Beliefs Influence Maternal Nutrition, Breastfeeding and Child Feeding Practices in South Africa; Chakona Nutrition Journal (2020), 19:47.
- Gardner, H., Green, K., & Gardner, A. (2015). Infant Feeding Practices of Emirati Women in The Rapidly Developing City of Abu Dhabi, United Arab Emirates. Int. J Environ. Res. Public Health.12, 10923–10940.
- Gawhara, Gad, Soliman, Ebrahem1, & et.al. (2019). Factors Contributing to Inadequate Exclusive Breast Feeding among Infants Aged 0-6 Months. IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-ISSN: 2320–1959.p- ISSN: 2320–1940 Volume 8.
- Hackman NM, Schaefer EW, Beiler JS, Rose CM, Paul IM. (2015). Breastfeeding outcome comparison by parity. Breastfeed Med. (3):156-62. doi: 10.1089/bfm.2014.0119. Epub PMID: 25549051; PMCID: PMC4378341.
- Karmacharya, C., Cunningham, K., Choufani, J., & Kadiyala, S. (2017). Grandmothers’ Knowledge Positively Influences Maternal Knowledge and Infant and Young Child Feeding Practices. Public Health Nutrition., 2017; 20(12): p (2114–23).
- Kiboi, W., & Patrick, K. (2017). Factors Associated with Exclusive Breastfeeding in Kenya: A Systematic Review. International Journal of Community Medicine and Public Health Mututho LN et al. Int J Community Med Public Health. Dec; 4, (12):4358-4362.
- Leshabari, S., Blystad, A., de Paoli, M., &Moland, M. (2007). HIV And Infant Feeding Counseling: Challenges Faced by Nurse-Counselors in Northern Tanzania. Human Resources for Health, Pg 5(18): 5-9.
- Mahesh Sarki, & et.al. (2018). Comparison of National Cross-sectional Breast-feeding Surveys by Maternal Education in Europe (2006–2016. Public Health Nutrition: 22(5), 848–861.
- Mamabolo, R., M, A., Mbenyane, G., Steyn, N., Nthangeni, N., De, D.-v., & Waal, H. e. (2004).
- MC, D. (2002). Breastfeeding in Africa: will positive trends be challenged by the AIDS epidemic? Sante, African Journal, 64-72.
- MC, D. (n.d.). Breastfeeding in Africa: will positive trends be challenged by the AIDS pandemic? Sante, African Journal !12(1), 64-72.
- MDHO. (2018). Mumbwa District Data Review Meeting. Mumbwa: MDHO.
- MDHO. (2018). Mumbwa District Health Information. Mumbwa: Mumbwa DHO.
- Mohamed, M.J., Ochola, S. & Owino, V.O. (2018). Comparison of knowledge, attitudes and practices on exclusive breastfeeding between primiparous and multiparous mothers attending Wajir District hospital, Wajir County, Kenya: a cross-sectional analytical study. Int Breastfeed J 13, 11 (2018). https:// doi. org/10.1186/s13006-018-0151-3
- Mugenda, A., & Mugenda, O. (2010, January 23). Research Methods: Quantitative and Qualitative Population Reference Bureau. Retrieved from World Population Data Sheet.: http://www.prb.org/Publications/Datasheets/19/04/2021-worldpopulation-data-sheet/data
- NFNC. (2022, August 1-7th). World Breatfeeding-Week-Press-Release. Lusaka: NFNC. Retrieved from https://www.nfnc.org.zm
- Ordenana, J., Colodro, L., & Tornero. (2011). Relationship Between Level of Education and Breastfeeding Duration Depends on Social Context. Journal of Human Lactation, 27(3), 272-278.
- Polit, D., & Hungler, B. (1995). Research in Nursing: Principles and Methods. Lippincott: Philadelphia.
- Ross, & Wilson. (2014). Anatomy & Physiology in Health and Illness: 12th Edition, Elsevier: Churchill.
- Roudbari, M. (2015). Exclusive Breastfeeding Duration (EBFD) and Breastfeeding Duration Factors Related (BFD). Oman Medical Journal (2015), Pg(342- 348).
- Setegn, T. (2012). Factors Associated with Exclusive Breastfeeding Practices among Mothers in Goba District, South Africa, Ethiopia. A College of Public Health and Medical Sciences, Department of Population and Family Health, Jim University Ethiopia.
- Sherriff, N., Hall, V., & Panton, C. (2014). Engaging and Supporting Fathers to Promote Breastfeeding: a concept analysis Midwifery 30 (6), 667–677.
- Shirima, R., Greiner, T., Kylberg, E., & Gebre-Medhim, M. (2011). Exclusive Breastfeeding Is Rarely Practiced in Rural and Urban Morogoro, Tanzania. Public Health Nutrition, 4(2):148-151.
- Sonko, A., & Worku, A. (2015.). Prevalence and predictors of exclusive breastfeeding for the first six months of life among women in Halaba Special Woreda, Southern Nations, Nationalities and Peoples ’Region/SNNPR/, Ethiopia. a community based cross-sectional study 73, (1), (p)1–11.
- Tembo, C., & Ngoma, M. (2015). Exclusive Breastfeeding Practice in Zambia. Medical Journal of Zambia, Vol.42, No.3, (p)124-129.
- Treece, E. W., & Treece, J. W. (1986). Elements of Research in Nursing. St. Louis.: Mosby.
- UNICEF. (2007). Preventing Disease and Saving Resources, Increase of Breastfeeding In the UK. UK: UNICEF.
- UNICEF. (2016). The Initiation of Breastfeeding Within One Hour of Birth, the Tanzania National Road map strategic plan. New York: UNICEF.
- Victora, C., Bahl, R., Baros, A., Franca, G., Horton, S. K., & et.al. (2016). Breastfeeding in the 21st century. Lancent North Am.ed, 475-490.
- WHO. (2001, 03 16). WHO int. Retrieved from WHO web: htt;//who.int/nutrition/topics/infantfeeding/en/
- WHO. (2002). Effect of Breastfeeding on Infant and Child Mortality Due to Infectious Diseases in Less Developed Countries: A Pooled Analysis. WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality Lancet 2000, 355(9202):451-5.
- WHO. (2011). Exclusive Breastfeeding for Six Months Best for Babies Everywhere. World Health Organization, 120.
- WHO. (2013). Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and Nutrition. Geneva: WHO.
- WHO. (2013, March 31). p (10). Retrieved from WHO: http://whqlibdoc.who.int/hq/2012/who_DCO_WHD_2012_g.p
- WHO. (2015). WHO Exclusive Breastfeeding. Retrieved from http://www.who. in/nutrition/topics/exclusive breastfeeding/en/.
- World Health Organization. (2012). Good health adds life to years. Global brief for World Health Day 2012. Geneva: WHO.
- Zafar S, Shamim K, Mehwish S, Arshad M, Barkat R. (2022) Comparison of Challenges and Problems Encountered in the Practice of Exclusive Breast Feeding by Primiparous and Multiparous Women in Rural Areas of Sindh, Pakistan: A Cross-Sectional Study. Cureus. 2021 May 12;13(5): e14976. doi: 10.7759/cureus.14976. Retraction in: Cureus. 17;14(3): r48. PMID: 34123672; PMCID: PMC8193157.
- Zambia Statistics Agency, (2019). 2019-2018 Zambia Demographic Health Survey Summary Report. Lusaka, Zambia: Zambia Statistics Agency, MOH, and ICF.
- ZamStats. (2019). Zambia Demographic and Health Survey. Lusaka: Central Statistical Office.