
Health Expenditure and Covid-19 Mortality Rate: The Role of Corruption
- Hussein Elkamel
- 284-296
- May 30, 2023
- Public Health
Health Expenditure and Covid-19 Mortality Rate: The Role of Corruption
Hussein Elkamel
Public Law Department at Sultan Qaboos University/ College of Law, Oman
DOI: https://doi.org/10.47772/IJRISS.2023.70524
Received: 21 April 2023; Accepted: 04 May 2023; Published: 30 May 2023
ABSTRACT
a sample consisting of 119 countries all around the world. The study uses three representations of corruption variables; utilizes a dataset from International Country Risk Guide ICRG. These representations are the country’s inherent corruption, the country’s ongoing corruption, and the country’s corruption and expenditure effects during Covid. The main finding is that corruption positively contributes to a higher Covid-19 fatality rate through inherent corruption, ongoing corrupt activities, and the collective role of corruption and government spending in Covid-19 mortality. Thus, countries pay the cost of their own corruption financially and physically.
Keywords: Covid-19; Corruption, Health, Expenditure; Mortality.
INTRODUCTION
The effectiveness of government health measurements is essential in determining the mortality rate due to Covid-19 (Khan, Awan, Islam, & Muurlink, 2020). Many covid-19 measures have required a financial budget that governments have to meet. The IMF is concerned about resources proposed to meet the emergency Covid needs of its members being misused by corrupt activities (IMF, 2021). Generally, corruption distorts the structure of government spending towards activities in that corrupt officials can extract higher bribe rates and thus leave fewer resources for health and education (Mauro, 1998). In addition, the average level of corruption before the Covid-19 outbreaks has put governments in different positions in the race to win over the pandemic. Developed countries with robust healthcare systems greatly suffer from Covid-19, while some developing countries with incompetent healthcare systems fail to defend against Covid-19 (Al-Zaman, 2020).
From a policy perspective, if the prevailing corruption level determines the effectiveness of the effort to prevent health shock, such as Covid-19, we pay the cost of corruption financially and physically. Reducing corrupt activities is not visible during a health shock, and countries aim to minimize their adverse effects on health service quality. Moreover, facing the needs and equipment required to deal with Covid-19 entitles the government to finance an emergency budget. Such government spending is a potential target for corrupt activities (Teremetskyi, Duliba, Kroitor, Korchak, & Makarenko, 2021), especially where government quality is low. Thus, corrupt officials may benefit from the simple auditing procedure many countries impose on getting supplies and equipment necessary for covid-19 patients on time (ACCA, 2020).
Corruption, as this study proposes, tends to trample our effort to defeat Covid-19 through three forces; the first is the initial magnitude and existence of corrupt activities that affected the quality of readiness before the covid-19. The second is corrupt activities ongoing during Covid-19. The last is the corrupt activities benefiting from the government spending with less restriction due to the urgently needed budgets during Covid-19. The statement that a low-corrupt government will perform better in defeating Covid-19 than a high-corrupt government is reasonably unquestionable and, to some extent, literature has proven ( (Farzanegan, 2021) (Eze, Ajah, Nwonovo, & Atama, 2021) (Alfano, Capasso, Ercolano, & Goel, 2022).
Nevertheless, this study intends to investigate the government’s level of corruption before Covid-19 affected health and well-being (i.e., exogenous effect) and whether the ongoing corrupt activities during the pandemic worsened the government’s performance against Covid-19 (i.e., endogenous development). Moreover, we intend to enrich the novel literature on this new phenomenon with a more updated and broader dataset, plus apply a multiple econometrics technique that better addresses the study’s questions.
The covid-19 was a crisis that was not expected, and countries had no time to adjust their capability to face it; in fact, they worked on their initial status with very little room to change their abilities. Countries with better health sectors had to work hard to face the tremendous demand for health services, while countries with poor health services had even worse situations. Covid-19 has put governments’ effectiveness to the test as the pandemic-defeating measures require efficient and transparent spending plans to face the urgent necessity of resources on a different level of their economies. Nevertheless, the corruption level that is prevailed in the government can be a real obstacle to such efforts. Thus, it is essential to investigate corruption’s role in determining the government’s effectiveness in defeating a health shock such as Covid. This study proposes the following: Section II relates to the Covid-19 death toll and other previous pandemics. The corruption and health linkages are in Section III. The data and methodology are presented in Section 4. The results are shown in Section 5. Then, the study concludes with the main findings in Section 6, and Section 7 contains the appendix.
Covid-19 Deaths
As of Sept 2022, the World Health Organization (WHO) has announced that around 6.5 million deaths globally resulted from Covid-19 (WHO, 2022). It is the most significant number of deaths due to a pandemic compared to what the world has experienced since the Spanish Flu (1918-1920). Where the last pandemic has claimed to cause 40-50 million deaths (MEDICOVER, 2020), the tremendous development in health and research centers internationally should make the 6.5 million Covid-19 deaths a concern. In addition, HIV/AIDS, since discovered in 1981, has caused around 35 million deaths to roll and probably less than a million per year as average growth, and still lower compared to Covid-19 deaths on average.
TABLE I: Pandemics and deaths toll
| Pandemic | Periods | Death’s toll |
| Spanish Flu | 1918-1920 | 40-50 million |
| Asian Flu | 1957-1958 | 1-2 million |
| Hong Kong Flu | 1968-1970 | 1-4 million |
| Ebola | 2014-2016 | 11,300 thousand |
| HIV/AIDS | 1980- ongoing | 35 million |
| Covid-19 | 2019- ongoing | 6.5 million |
Source: MEDICOVER, URL: https://www.medicover.pl/en/coronavirus/world-pandemics-history-sars-cov-2-coronavirus/
Covid-19 has created many challenges for healthcare providers and the health sector. There has been an enormous number of covid-19 patients beyond the capacity of health facilities, and countries vary in this matter. However, all countries generally experience a massive demand for medical supplies and physicians. The phenomenon of the global chain that production operations are scattered in several countries to gain the possible lower cost has led to interdependence among countries in supplying medical goods. Thus, no countries were ready to meet the sudden colossal demand for such goods, even with less sophisticated supplies such as personal protective equipment products (face masks, surgical gloves, sanitizers, etc.). One country locking down within the production chain of medical supplies would cause an interruption of the production supply of that medical good. Many hospitals had been forced to turn patients away as they ran out of space and supplies.
Moreover, hospitals’ access to enough Oxygen was limited and, in some cases, missing entirely. Oxygen is the most critical medicine for Covid-19 patients with severe conditions, and the lack of it may kill covid-19 patients with extreme conditions ((MSF), 2021). Other factors contributing to covid-19 deaths are the lack of physicians and emergency room spaces, which significantly increases when the Covid-19 infection rate.
The death toll among countries varies, and several determinants contribute to these variations. Medical supplies and personnel capacity are among the most significant factors contributing to the size death toll of Covid-19. The government’s ability to enforce social distancing to prevent the diffusion of coronavirus is a fundamental factor in reducing the death toll. It is a real challenge when defatting a pandemic requires people to change their social and cultural practices. All these factors are interdependent, and the government must enhance these factors collectively. Nevertheless, corruption is known to hinder the government’s ability to provide better service and cause its administration levels to act with inefficiency. Corruption also utilizes government procurement as a source of private payments leading to poor equipment that more corrupt governments will encounter compared to a less corrupt government.
Corruption and health linkages
Corruption is a significant obstacle to development and may affect the quality of services that government provides its citizens. Corruption involving the health sector can damage the quality of services, which in turn falls on citizens’ health. For instance, in OECD countries, more than 6% of health expenditure loss is attributed to fraud and error, whereas it is even worse globally, corresponding to 45% ((OECD), 2017). It is more serious when the services are direct to a pandemic such as covid-19, which can potentially cause people’s death. Corruption has been claimed to cause a cost that most literature is interested in its financial form; however, corruption in times of pandemic can cost lives, and the scale can be significant, as Covid-19 has already shown us. Health services are critical in terms of time and supply needed. Corruption causes bureaucrats to delay services provided as a tool to demand bribes and causes a shortage in supply due to fraudulent activities in countries where corruption is prevalent. Thus, a dominant corruption environment leads to poor health services even before covid-19; however, the latter impose more time pressure on corrupt government dealing with covid-19 needs, which could limit the government’s ability to save lives.
Corruption also led to citizens mistrusting institutional government entities and reduced the ability of the government to fight against Covid-19 (Eze, Ajah, Nwonovo, & Atama, 2021). Using a qualitative methodology, the latter study proposed to investigate the health sector corruption during Covid-19 in two Nigerian states (Anambra & Enugu). The authors utilized a questionnaire of 36 respondents that were drawn from these two mentioned states. The respondent referred to the vast and deep inherent corruption that exists not only in the health sector but almost everywhere in Nigeria. (Farzanegan, 2021) though utilizing cross-section data of 64 countries investigates the role of corruption causing Covid-19 fatality while controlling for some variables that may contribute to the Covid-19 mortality rate, such as demographic population structure and tourism arrivals to the country. The author finds that corruption is associated with a higher rate of Covid-19 mortality. In addition, the findings are consistent with the literature view that better governance reforms will enhance the government budget allocation of public goods, including health sectors.
(Gupta, Davoodi, & Tiongson, 2001) One of the earliest studies on the adverse effect on infant health utilized a dataset covering 1985-97. In highly corrupt countries, the infant mortality rate tends to be 30% higher than in low corrupt countries, and the difference is higher when considering low-birthweight babies. Several policy suggestions, the authors stated that improving health services are not only about increasing spending but more about transparency and accountability of that spending. In addition, the private sector’s higher participation in health services may reduce the monopoly power of corrupt officials that they rely on when embezzling bribes. Finally, people’s participation in public resource allocation would reduce corruption in the health sector. However, one should admit that the time window that Covid-19 provides is much shorter, and the pandemic is a shock requiring immediate action. (Alfano, Capasso, Ercolano, & Goel, 2022) We have found that where the government is percept as more corrupt, the number of Covid cases is higher with controlling for other related variables to covid-19. The channel can be a weak institution that corruption spreads among society and contributes to individuals’ compliance and rejection of covid-19 measures.
DATA AND METHODOLOGY
Our objective is to associate the death rate due to Covid-19 with corruption levels, individually and conjunctionally, with government spending. The sample consists of 119 countries all around the world. The country set varies from developed and developing countries; poor and rich countries contain all world regions. The data is a cross-country set, and below is the definition of all variables based on their representation in the analysis:
The dependent variable
The number of deaths of Covid-19 in 2021 per 1 million population. From Table 1, we notice a significant variation across countries in the rate of deaths due to covid-19, which our study intends to explain. Several studies use the number of deaths as a dependent variable for the research question where the interest is in the variations of people’s health due to corruption ( (Farzanegan, 2021) (Gupta, Davoodi, & Tiongson, 2001) (Bosancianu, et al., 2020)).
The Independent variables
Corruption
Corruption is the leading indicator we utilize to explain the variation in fatality rates across countries. The corruption variable is the International Country Risk Guide ICRG which measures corruption within the political system. The corrupt practices may take different forms, such as bribes, excessive patronage, nepotism, job reservation, or favor-for-favor. The variable assesses the corrupt activity on a scale of 6, where the highest value refers to minor corruption and the lower value to the highest corruption. However, for convenience, we rescaled the variable that the higher values indicate higher corruption levels, and the lower value indicates value lower corruption. Thus, the coefficient on the corruption variables is assumed to be positive that corruption positively contributes to covid-19 mortality.
The corruption in our analysis has three representations. The first is the initial corruption of each country before covid-19, which averaged the corruption levels in three years (2017-2019). This representation tests the claim that countries with higher corruption (better governance) tend to respond less effectively (more effectively) to Covid-19 shock and thus cause a more significant mortality rate. The second representation of the corruption variable is to investigate the effect of the same year’s corruption level on the number of covid fatalities in our country-set data. The effectiveness of the government responding to urgent needs may depend on the ongoing corrupt activities which hinder the health capacity to save lives. The last representation is the interaction of corrupt activities with government expenditure to investigate the effectiveness of government spending, which is vital to prevent covid-19 mortality incidence.
An efficient government can better deal with circumstances caused by the covid when the level of good governance is higher.
Government expenditure
The government expenditure is the government’s final consumption expenditure as a percentage of GDP in 2021 extracted from WDI. We favor this variable representation over the government expenditure as annual growth as most of the annual growth of most governments’ spending has shrunk due to covid. Government expenditure as a share of the country’s GDP can be the best spending measurement associated with Covid-19 as common goods and services the government spent on has decreased, and more spending on Covid related goods and services has increased. In countries where corruption is high, government spending during the pandemic can be a target for corrupt activities, especially with the urgency of this spending that caused less auditing process. Regarding our sample, Table 2 shows that the variable is free of outliners as the mean and median are very close.
Control variables
This set of variables serves the purpose of reducing the risk of omitted variables; such variables’ choice is built on either theoretical justification or other studies’ use of them.
Initial health expenditure
This variable intends to measure the country’s capacity for health services readiness. The covid-19 pandemic tests countries’ health sector quality and the level that these countries had been spending in the sector before the pandemic. Thus, we use the averaged 3-year health expenditure as a share of the country’s GDP before the pandemic to control countries’ different positions in health sector services. Table 1 indicates that the variable does not contain outliers as the difference between mean and median is small; however, the variable has considerable variations that should account for covid-19 fatality across countries.
GDP per capita
We use GDP per capita to control for economic development differences as our large country sample contains a variety of countries that differ in income acquisition per capita. The latter variation can be seen from the summary statistics in Table 1, where Malawi is the most negligible GDP per capita at around 392$ per price in 2015 compared to Luxembourg’s GDP per capita at around 107,637$ evaluated at 2015 prices. In such a case, we should represent this variable in log value to smooth striking differences among our sample.
Population 65 and above
Demographic age structure is claimed to affect the fatality rate as the Covid-19 known to severely endangers 65 years and older people more than younger ones (Yanez, Weiss, Romand, & Treggiari, 2020). Many studies have found a positive relationship between the Covid-19 fatality rate and the share of the higher-age population (Dowd, et al., 2020) (Caramelo, Ferreira, & Oliveiros, 2020). The variable is represented as an averaged percentage of the total population of those aged 65 or above from 2017 to 2019.
Physicians
This variable represents the number of physicians per 1,000 in the population. The summary statistics of this variable in Table 1 do not indicate the existence of outliers.
Those physicians can be generalists or specialist physicians. Including this variable refers to the necessity of doctors for those whose covid infection is critical and could cause death. However, using a number of physicians as an indication of health services performance implicitly indicates that all physicians are with similar levels of skills and education across our countries’ sample which is a strong assumption.
Tourism
There is no doubt that travelers were the vehicle that spread the covid-19 among worldwide, and tourism destination countries are expected to have a higher rate of covid infection than other countries. We are expecting that non-attracted tourist country can expiated that quarantined and closing border measurement than tourist destination countries. The variable is the number of international visitors who arrive in the country.
Urban Population
One challenge that countries encounter is the enforcement of physical distancing among the population to stop the infection from spreading, and challenges are higher in over-populated areas. Covid-19 infection is a chain that can develop very fast in crowded living areas and cause a higher rate of covid mortality. Thus, we include this variable as a percentage of the country’s urban population over the total population. The variable validity is affected by the country’s practical quarantined measurements, and different law enforcement across countries may change the credibility of this variable.
TABLE II: Summary statistics
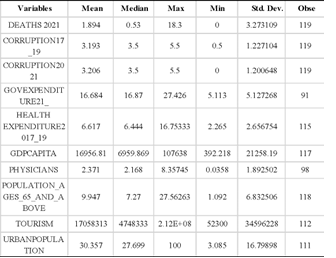
Data definitions and sources are in the appendix.
Speaking of the methodology, our main analysis relies on cross-sectional regression of 119 countries. There will be six models of regressions that investigate the role of corruption in Covid-19 deaths across our sample. These models differ in corruption variable representations besides two models of the short and extended forms of control variables. The corruption alternative representations are the initial corruption level before covid, the ongoing corruption during covid, and the interaction effect of corruption and government spending on Covid-19 deaths.
REGRESSION RESULTS
First, we estimate the correlation matrix along with t statistics as shown in Table 5 in the appendix. The deaths due to covid did not show the expected sign of corruption. The sign was negative but insignificant. We point out some issues in the limitation section that corrupt governments may have an interest in reporting a lower number of deaths due to covid to reduce society’s outrage. Worth mentioning, in our regression, the corruption coefficient turned positive and significant on covid-19 deaths only when a population of 65 and more are included in the models. GDP per capita indicates a positive association with covid deaths but the coefficient is insignificant. The coefficient on government spending indicates a positive association with the number of deaths which refers to the idea that the country’s higher spending is the one with a larger public sector and in turn one with higher corrupt activities and thus associated with a higher death rate. This result explains the significance of the interaction coefficient of corruption and government spending in our regression models. The coefficient for population 65 and above has the expected sign and is very significant that the country with a higher population of 65 and above tends to have a higher rate of covid-19 deaths. Also, the coefficient on tourism has shown the expected correlation with deaths that countries that are tourism destinations tend to encounter a higher rate of covid-19 deaths. The urban population coefficient is not significant, nor it has the expected sign. The physician’s coefficient has a positive sign indicating that the higher the number of physicians the higher the death rate, which is contradictory. Such a result may indicate the great variations within physicians’ skills and professions that a higher number of physicians may not indicate a better health service.
Our sample contains a variety of countries in their perceived level of corruption. Thus, we split our sample into two groups: the above-average group and the average group. The average is, as indicated in Table II, 3.2 points. Surprisingly, the below-average corruption group has the expected sign between corruption and covid-19 deaths; that is as the country perceived higher corrupt activities as the covid-19 death rate is higher. On contrary, the above-average corrupt group correlation matrix was similar in its results to all countries’ correlation matrices in Table III. One possible explanation is that the above-average corruption group may suffer from false reporting of covid-19 deaths. The government that perceived a higher level of corruption lacks accountability and transparency thus government reporting of deaths may deliberately be underestimated the number of deaths and thus we fail in catching the positive correlation between corruption and covid deaths in highly corrupt countries. However, regression control variables in our regression models hopefully will control for these issues.
Cross-sectional Regression
All regression models indicate that the country’s level of corruption contributes to the death rate due to covid. The role of corruption affecting covid mortality takes three trajectories; one is through the inherent corruption level that the government had before covid-19 outbreaks. The second is through the ongoing corrupt activities within the same year of covid fatality; the last is conjunctional with government spending that should mitigate the negative impact of covid-19. The following table summarizes all six models’ results that investigate one or more corruption indices and other control variables contributing to covid-19 mortality. The sample size varies across model specifications.
In the first model test for the effect of the initial corruption on covid-19 mortality, the coefficient indicates a positive effect of the corruption level that the country possesses before covid-19 on the death rate. The initial health capacity reduces the fatality rate due to covid-19 indicating that countries with higher health spending seem to be in a better position than countries spending less on health before Covid-19 outbreaks. The population above 65 variable has the expected sign that countries with a higher ratio of the population of 65 tend to have higher deaths due to covid-19 increase. GDP per capita turns insignificant, and the case is the same for government spending. The model explains 47% of the covid-19 deaths variation.
The second model investigates the role of current corruption in the same year of covid-19 deaths. The model shows that countries with higher ongoing corruption tend to increase the fatality rate of Covid-19. The other control variables produce almost the same results concerning value and significance compared to Model 1. Model 3 serves the same purpose as model 1, which tests the role of inherent corruption before the Covid-19 shock with the addition of extended control variables. These are physicians, tourism, and urban population; however, they all show insignificant coefficients. In model 4, we test for the role of the interaction effect between the initial level of corruption and the government’s ongoing expenditure.
The coefficient on the interaction term indicates that initial corruption through government spending increases the rate of Covid-19 fatality. This is a sign that a government with a high rate of corruption seems to ineffectively spend resources where government spending initiatives are critical to deal with Covid-19 response plans. The addition of the interaction term has made the personal corruption variable insignificant; however, that is the cost one needs to sacrifice to include the interaction term in general. Both initial health and population >65 variables remain with expected signs and are statistically significant like the previous models. The goodness of fit has slightly increased compared to the previous models. Model 5 utilizes the interaction term as model 4 to investigate the connection between corruption and government spending, where we use ongoing corruption (Corruption 2021).
The interaction term is significant and has the expected sign that as government possesses more corrupt levels, government spending tends to be ineffective, and the mortality rate of Covid-19 increases. The other control variables are consistent with other previous models. However, this model has the highest R squared value among all models. Model 6 is the same as Model 2, with only more control variables. The model is consistent with results obtained in Model 2 and other models in general.
To sum up, all individual corruption variables possess the expected sign and are significant when the interaction term is not in use. When the interaction term is used, it turns to absorb the effect of the individual corrupt variables, but it did not affect the other variables of the models. The initial health variable is with the expected sign and significant through all models. Likewise, the population >=65 variable is consistent through all models regarding sign and significance. Even though our sample contains 119 countries, the sample size ranges between 68 and 87 due to some variables missing observations.
TABLE III: Covid mortality, corruption, and government expenditure: cross-section regressions
(1) (2) (3) (4) (5) (6)

Note: T statistics are in parenthesis. The constant is included in all models but are not reported. (***,**,*) refer to statistical significance at 99%, 95% and 90% confidence intervals; respectively.
Finally, we move to a basic robustness test by splitting our country sample into two groups; one is a set of the country above average corruption levels, and the other is below average. We run the three regression tests for each group of countries. Three regression models are differentiated in the corruption variable representations similar to our primary analysis but with the same control variables. The results are presented in Table VII in the appendix. The results for the countries with average corruption (more corrupt countries) showed insignificant coefficients in variables of corruption through all models. In more corrupt countries, the death toll due to covid can be intentionally misreported as the corrupt government aims to reduce the societal pressure on health services failure. More about this potential claim is in Section 7, which introduces the study’s limitations. Concerning the below-average group set countries (less corrupt), the initial corruption and ongoing corruption variable model turned out to be insignificant on the main variables, and the only significant coefficient through models is the population 65 and above. However, when introducing the interaction term of corruption and government spending, the corruption and the interaction term are significant and have the correct sign. The more corruption, the higher the death toll due to Covid-19. Moreover, corruption activities benefit from government spending during the time of Covid-19, and collectively they cause higher Covid-19 deaths.
CONCLUSION
There has been growing interest in corruption’s effects on multiple aspects of our lives. Interestingly, covid-19 brings a new extension of corruption effects that countries with higher corruption may suffer from higher fatality rates of covid-19. The preexisting corruption could effectively reduce the country’s readiness to deal with health shocks such as covid-19. The short time window that covid-19 has imposed on the government to deal with increasingly new covid-19 cases allowed no room for enhanced governance and countries have to work on their initial status. In addition, ongoing corruption may crumble the country’s measures to prevent covid, thus higher death results. Lastly, corruption can target government spending during covid-19; these spendings are crucial to fight covid-19, and failure to prevent from corrupt activities could cause a higher fatality rate.
This study utilizes a large sample of countries, including 119 countries worldwide. Moreover, collecting a variety of variables contribute to the covid-19 death rate. The study uses the death rate extracted in December for a week on average. Countries have experienced a peak death rate and, at other times, a period of a lower rate, depending on the date recorded. We assume that picking this month as a random point time will smooth these differences across the country and should not affect the results. Corruption level has three representations: one is as averaged three years prior to covid-19; the second is the ongoing corrupt activities during the year; the last representation of corruption variable is its interaction role with government spending. Besides, we include a set of control variables to control for omitted variables effect: health initial, GDP per capita, population 65 years and above, physician, tourism, and urban population.
The study uses regression analysis of cross-section and adopts six models to test the central claim that corruption contributes positively to a higher death rate due to covid. The models examine the three corruption representations mentioned above and two models of extended control variables to improve the goodness of fit of our claim. The results indicate that corruption increases the death rate in our country sample through three mechanisms: preexisting corruption before the pandemic, ongoing corrupt activities in the same year, and conjunctionally with the current government expenditure. These results inform us that corruption does not only cause a financial cost, but it also causes a life cost.
Policymakers can reduce the cost of corruption through tight auditing of government spending, but it will be challenging to meet society’s needs in time. There is still an effort to prevent corruption from causing more death by reducing the level of ongoing corruption and educating on the societal level that corruption contributes to a higher mortality rate. It can be an excellent opportunity to impose a profound message to society about the cost of corruption, which helps with efforts in fighting it in the medium and long term.
Limitation
other social, economic, and institutional variables and these associations are the main practical negativity that corruption possesses. But also, create estimation problems with regression models. The number of deaths due to covid-19 may not be exogenous to the level of corruption. The Covid-19 death reporting may depend on the level of government quality as reporting of deaths will come from different sources and regions in the country. In addition, reporting Covid-19 deaths has a political aspect that may lead corrupt officials to intentionally understate the number of deaths in order to mitigate public outrage. Looking for an instrument variable that can account for this difference across countries and at the same time exogenous to countries corruption level may solve the problem. Thus, the country where corruption level high tends to have lower deaths’ reporting than the real deaths numbers. Time limitation is an obstacle, and we intend to leave it for near future to address this limitation.
APPENDIX
List of countries:
Albania, Algeria, Angola, Argentina, Armenia, Australia, Austria, Azerbaijan, Bahamas, Bahrain, Bangladesh, Belarus, Belgium, Bolivia, Botswana, Brazil, Bulgaria, Burkina Faso, Cameroon, Canada, Chile, China, Colombia, Costa Rica, Cote d’Ivoire, Croatia, Cuba, Denmark, Ecuador, Egypt, El Salvador, Estonia, Ethiopia, Finland, France, Gabon, Germany, Ghana, Greece, Guatemala, Guinea, Guinea-Bissau, Guyana, Haiti, Honduras, Hong Kong, Hungary, Iceland, India, Indonesia, Iran, Iraq, Ireland, Italy, Jamaica, Japan, Jordan, Kazakhstan, Kenya, Kuwait, Latvia, Lebanon, Libya, Lithuania, Luxembourg, Madagascar, Malawi, Malaysia, Mali, Malta, Mexico, Moldova, Mongolia, Morocco, Mozambique, Myanmar, Namibia, Netherlands, New Zealand, Nicaragua, Niger, Nigeria, Norway, Oman, Pakistan, Papua New Guinea, Paraguay, Peru, Philippines, Poland, Portugal, Qatar, Romania, Russia, Saudi Arabia, Senegal, Serbia, Sierra Leone, Singapore, Slovakia, Slovenia, South Korea, Spain, Sri Lanka, Sudan, Sweden, Switzerland, Syria, Tunisia, Turkey, Uganda, Ukraine, United Arab Emirates, United Kingdom, United States, Uruguay, Venezuela, Zambia, Zimbabwe.
TABLE IV: Variables definitions and sources

TABLE V: Correlation and t-statistics
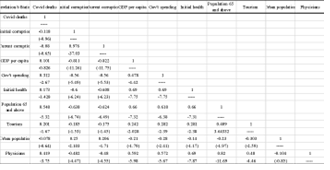
TABLE VI: Correlation and t-statistics of above-average corruption country-sample
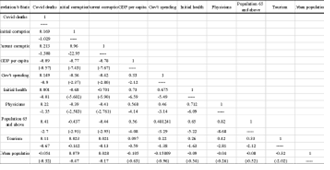
TABLE VII: Correlation and t-statistics of below-average corruption country-sample
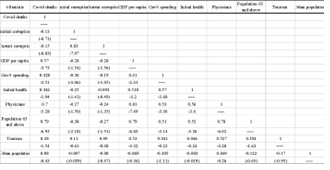
TABLE VIII: Above and below average corruption country-group (cross-section regressions)
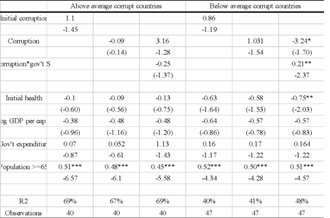
Note: T statistics are in parenthesis. Constant is included in all models but are not reported. (***,**,*) refer to statistical significance at 99%, 95% and 90% confidence intervals; respectively.
BIBLIOGRAPHY
- Khan, J. R., Awan, N., Islam, M., & Muurlink, O. (2020, July). Healthcare Capacity, Health Expenditure, and Civil Society as Predictors of COVID-19 Case Fatalities: A Global Analysis. Frontiers in Public Health, 8.
- Al-Zaman, M. S. (2020). Healthcare Crisis in Bangladesh during the COVID-19 Pandemic. The American Society of Tropical Medicine and Hygiene, 103(4), 1357–1359.
- Mauro, P. (1998). Corruption and the composition of government expenditure . Journal of Public Economics, 69(2), 263-279.
- ACCA. (2020). The impact of Covid-19 on Audit and Assurance – challenges and considerations. the Association of Chartered Certified Accountants.
- Yanez, N. D., Weiss, N., Romand, J.-A., & Treggiari, M. (2020). COVID-19 mortality risk for older men and women. BMC Public Health, 20(1742).
- Dowd, J. B., Andriano, L., Brazel, D., Rotondi, V., Block, P., & Ding, X. (2020). Demographic science aids in understanding the spread and fatality rates of COVID-19. Proceedings of the National Academy of Sciences, 117, 9696-9698.
- Caramelo, F., Ferreira, N., & Oliveiros, B. (2020, February 25). Estimation of risk factors for COVID-19 mortality.
- IMF. (2021, 2 17). How the IMF is Promoting Transparent and Accountable Use of COVID-19 Financial Assistance. Retrieved September 2022, from International Monetary Fund: https://www.imf.org/en/About/Factsheets/Sheets/2020/04/30/how-imf-covid19-financial-help-is-used
- (OECD), T. O.-o. (2017). Tackling Wasteful Spending on Health. Retrieved 9 2022, from https://www.oecd.org/els/health-systems/Tackling-Wasteful-Spending-on-Health-Highlights-revised.pdf
- Teremetskyi, V., Duliba, Y., Kroitor, V., Korchak, N., & Makarenko, O. (2021). Corruption and strengthening anti-corruption efforts in healthcare during the pandemic of Covid-19. Medico-Legal Journal, 89(1), 25-28.
- Eze, O. J., Ajah, B., Nwonovo, O., & Atama , C. (2021). Health sector corruption and COVID-19 outbreak: evidence from Anambra and Enugu States, Nigeria. Journal of Contemporary African Studies, 40(1), 34-46.
- Farzanegan, M. R. (2021). The Effect of Public Corruption on Covid-19 Fatality Rate: A Cross-Country Examination. CESifo Working Paper, No. 8938, Center for Economic Studies and Ifo Institute (CESifo).
- Gupta, S., Davoodi, H., & Tiongson, E. (2001). Corruption and the provision of health care and education services. In The Political Economy of Corruption (p. 31). Routledge.
- Alfano, V., Capasso, S., Ercolano, S., & Goel, R. (2022). Death takes no bribes: Impact of perceived corruption on the effectiveness of non-pharmaceutical interventions at combating COVID-19. Social Science & Medicine, 301.
- Bosancianu, C. M., Hilbig, H., Humphreys, M., KC, S., Lieber, N., & Scacco, A. (2020). Political and Social Correlates of Covid-19 Mortality.
- WHO, W. H. (2022, Sept 30). WHO Coronavirus (COVID-19) Dashboard. Retrieved from https://covid19.who.int/?mapFilter=deaths
- MEDICOVER. (2020, May). World pandemics history – SARS-CoV-2 coronavirus compared to other pandemics. Retrieved from https://www.medicover.pl/en/coronavirus/world-pandemics-history-sars-cov-2-coronavirus/
- (MSF), M. S. (2021, May). More oxygen supplies needed to avoid COVID-19 patients “gasping for air”. Retrieved from https://www.msf.org/oxygen-supplies-must-be-scaled-coronavirus-covid-19-response