
Impact of Magnesium on In-Hospital Ami Outcomes in Bangladesh.
- Barua Sushanta
- Roy Haripada
- Roy Nikhil
- Hasan Abu Reza Hasibul
- Barua Rita Rani
- Barua Prashanta
- Ansari MA Jalil
- Barua Hena Rani
- 739-748
- May 25, 2024
- Health Education
Impact of Magnesium on In-Hospital Ami Outcomes in Bangladesh.
Barua Sushanta1*, Roy Haripada2, Roy Nikhil3, Hasan Abu Reza Hasibul4, Barua Rita Rani5, Barua Prashanta6, Ansari MA Jalil7, Barua Hena Rani8
1Department of Cardiology, Dhaka Medical College Hospital, Dhaka, Bangladesh.
2Upazila Health Complex, Gopalgonj, Dhaka,
3Assistant Professor, BIHS, General Hospital, Dhaka, Bangladesh.
4Department of Cardiology, Dhaka Medical College Hospital, Dhaka, Bangladesh.
5Professor Department of Pathology, Dr. Sirajul Islam Medical College, Dhaka, Bangladesh.
6Dhaka Medical College Hospital, Dhaka, Bangladesh.
7Professor of Endocrinology, Principal, MH Samorita Medical College, Tejgoan, Dhaka, Bangladesh.
8Department of Gynae & Obs, Rangamati Medical College Hospital.
*Corresponding Address
DOI: https://dx.doi.org/10.47772/IJRISS.2024.803048S
Received: 24 March 2024; Revised: 13 April 2024; Accepted: 24 April 2024; Published: 25 May 2024
ABSTRACT
Background: Coronary artery disease (CAD) is a major cause of death globally. Bangladesh has a high prevalence of CAD, especially in urban areas. Acute myocardial infarction (AMI) is a serious condition that occurs when there’s a blockage in the coronary arteries. Electrolyte imbalances, such as magnesium deficiency, can worsen AMI.
Objectives: To evaluate the association between serums magnesium level on in-hospital acute myocardial infarction outcomes.
Study Design and Methods: This prospective study recruited 110 patients diagnosed with AMI in Dhaka, Bangladesh. Researchers measured serum magnesium levels, monitored patients, and recorded clinical outcomes.
Results: The study found that patients with lower magnesium levels were more likely to experience complications such as arrhythmias, cardiogenic shock, and left ventricular dysfunction.
Conclusion: The study highlights the importance of monitoring magnesium levels in AMI patients. However, more research is needed to determine the optimal magnesium level and its impact on patient outcomes.
Key Words: Acute Myocardial infarction, Major adverse cardiac events, Serum Magnesium.
INTRODUCTION
The burden of cardiovascular disease (CVD) is increasing in developing countries, especially in low- and middle-income countries (LMICs) like Bangladesh. Bangladesh is highly prevalent for cardiovascular disease particularly in urban areas. While population aging may be a factor, urbanization seems to impact improvements in eating habits and physical activity. [19] Acute coronary syndrome (ACS) encompasses various clinical manifestations of myocardial ischemia, including unstable angina (UA), non-ST segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI). Diagnosis of ST-segment elevation myocardial infarction is suspected when a patient has ST-segment elevation in two or more anatomically adjacent ECG leads and a compatible medical history. [2] Acute ST-segment elevation myocardial infarction is caused by occlusion of one or more coronary arteries. Coronary arteries supply blood to the heart. Immediate disruption of blood flow, usually caused by plaque rupture, erosion, or detachment, results in the formation of an occlusive thrombus. Correct diagnosis and treatment of these patients must be based on information available at time initial diagnosis.ST-segment elevation myocardial infarction occurs when a large epicardial coronary artery is completely occluded, usually due to thrombosis. Myocardial ischemia causes changes in metabolism and ion exchange. This cellular process prolongs repolarization and increases action potentials in the ischemic region of the myocardium. [3] Differences between long-term tissue potentials and ischemic potentials may lead to increased dispersion of Tran’s mural repolarization due to the influence of electrophysiological heterogeneity in the ventricular myocardium and long-term unresponsiveness. These processes may be contributing factors to the development of recurrent arrhythmias. This arrhythmia is the most common cause of death in patients with STEMI. [4, 5] Electrolyte imbalances affect not only cardiac repolarization but also outcomes after AMI. In addition to general risk factors, blood magnesium concentration is also suggested to be a determinant of AMI. [6] In acute myocardial infarction, hypomagnesaemia occurs, causing magnesium to be converted to extracellular potassium and depolarized, leading to cardiac arrhythmias. Magnesium is an important intracellular ion responsible for the activity of sodium and potassium adenosine triphosphate and is considered important in regulating the passage of potassium across cell membranes. As magnesium concentration decreases, membrane stability decreases, cells become more excitable, and arrhythmias occur. Additionally, reduced magnesium levels may affect magnesium inhibited calcium influx, leading to physical and pulmonary dysfunction, i.e. afterload impairment, an important factor in determining pump performance. [ 7] Previous studies have shown that serum Mg and K concentrations are reduced in patients with AMI and CHD and that the two are closely related. In a recent study, [8] Choudhury et al. (2011) showed that low serum magnesium levels are associated with inflammation and dysregulation of vascular tone and endothelial function. This process is thought to contribute to the development and progression of atherosclerosis, which may lead to the development of coronary heart disease (CHD). [9] Magnesium is also known for its role in electrical stability and energy balance of cardiomyocytes. [10] Because hypomagnesaemia is associated with atrial and ventricular arrhythmias, low serum magnesium levels may increase the risk of sudden cardiac death (SCD). The lack of association between serum magnesium concentrations and QTc interval or sudden death in a retrospective study was unexpected. However, a serum magnesium level of 2.4 mg/dl is an indicator of improved clinical practice in patients with OAC. [11] Hypomagnesaemia is important in the development of ventricular fibrillation, the most common cause of sudden death in coronary heart disease. Coronary artery spasm due to hypomagnesaemia is considered an important cause of sudden death from coronary artery disease. Magnesium deficiency causes the development of atherosclerotic plaques due to hyperlipidemia. Myocardial infarction is one of the most common causes of death, and its occurrence depends on many factors [12]. Therefore, in this study, we sought to measure blood magnesium concentration in patients with myocardial infarction.
MATERIAL AND METHODS
Study Design and Setting
This prospective study was conducted from July 2022 to June 2023at the Department of Cardiology, Dhaka Medical College & Hospital, Dhaka, Bangladesh.
Patients
Inclusion criteria:
Duration 12 hours from onset of chest pain.
The following criteria has been used to diagnose acute myocardial infarction. The presence of any of the two criteria has been considered:
- History of typical chest pain.
- Changes in the ECG suggestive of acute myocardial infarction
- Increase level of biochemical marker e.g. troponin-I, Ck-MB
- Echocardiographic findings
Exclusion criteria:
Liver disease, Renal insufficiency (serum creatinine >1.4mg/dL), Current use of medications affecting electrolytes (diuretics, glucocorticoids), Recent surgery or trauma (within 48 hours), Active infectious or inflammatory disease, Use of magnesium-containing supplements or medications affecting magnesium metabolism, Pregnancy and Prior administration of thrombolytic therapy (STK) outside the hospital
Ethical Considerations:
Ethical clearance was obtained from the institutional ethical review committee of Dhaka Medical College, Dhaka.
Sample Size: 110
Sample size calculation: The sample size is determined by following formula:
n= ((P1 (100-P1) + P2 (100-P2)) / (P1-P2 )2)×(Zα+Zβ )2 (Kumari1 & Prasad, 2020)
Where,
n =sample size
P1 =16 [Proportion of exposed group]
P2=37 [Proportion of unexposed group]
Zα = Z value at a define level of significance (1.96 at 5% level of significance)
Zβ =Z value at a define power of test (1.64 at 95% power of test)
n=((16(100-16)+37(100-37))/(16-37)2 )×(1.96+1.64)2
n=((1344+2331) / 441) ×12.96
n= 108
As this is a hospital based study, therefore 110 cases were taken. Considering inclusion and exclusion criteria at least 110 STEMI & Non- STEMI patients of both sexes were included in the study.
Data Collection
Patients who fulfilled including criteria were selected as study subject. Study subjects were informed about risk and benefit about research work. Patients were subjected to undergo investigations like complete blood count, urine examination, blood sugar, blood urea, serum creatinine, fasting lipid profile, cardiac enzymes and ECG was done in all cases. Estimation of serum magnesium level was done on day 1 and day 5. Then data were collected in a predesigned data collection form through a detailed medical history, including demographics, symptom onset, duration, co-morbidities and potential complications. Comprehensive physical examination was performed and laboratory findings are included.
Serum Magnesium Measurement:
Blood samples were collected within 48 hours of admission following aseptic precautions. Five milliliters of venous blood were drawn and transferred to a sterile tube to prevent hemolysis. Samples were centrifuged, serum separated, and stored at -20°C before transport to the Biochemistry Department.
Method of estimation serum magnesium
The method used was colorimetric end point test with Xylidyl blue as the reagent. Magnesium standard: 2.5 mg/dL.
Principle:
Magnesium reacts with xylidyl blue at alkaline pH resulting in the formation of a chelating red colored compound. The increase in the red color (or) the decrease in blue color are proportionate to the concentration of magnesium in the serum.
Specimen
Analysis of non-hemolyzed serum or lithium heparin plasma may be done since the concentration of magnesium inside the red cells is 10 times greater than that in the ECF. Separation of serum from the cell should be done as early as possible and hemolysis should be avoided.
Interpretation of findings was correlated with AMI patients. Then patients were be kept under close monitoring and management continued according to hospital protocol. Sample were collected within 48 hours and notice for any clinical parameters like arrhythmia e.g. VF, AF, long QTc Interval , Torsade’s De pointes ,cardiogenic shock, LVF, Conduction block within the total admission period of the patient.
Normal Magnesium level: 1.6- 2.4 gm/dl
Data Analysis
Patients were divided into two groups: unexposed (normal serum magnesium) and exposed (low serum magnesium).Patient data, clinical findings, laboratory results, and outcomes were collected and analyzed using SPSS 23 software (Chicago, USA).Chi-square and t-tests were used for statistical analysis. P-values less than 0.05 were considered statistically significant.
RESULT
There were a total of 200 respondents involved in this study and the overall response rate was 110(55%). All these respondents had an acute myocardial infarction and had registered at the Department of Cardiology, Dhaka Medical College Hospital, Dhaka, after fulfilling inclusion and exclusion criteria 110 STEMI patients were selected for the study. Figure I indicates that most of the patients were in the age range of 51-60 years in the unexposed group & 41-50 years in the exposed group of the study population.
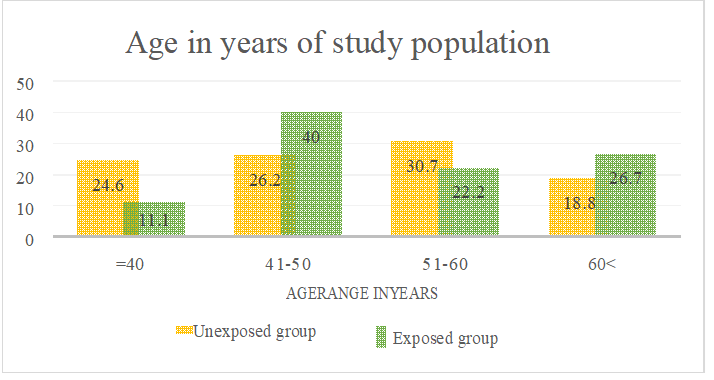
Figure: I Distribution of age among the study population.
Patients in the exposed group were generally older than the patients in the Unexposed group (54.18±10.11 vs. 51.54±10.12, p=0.43).
Among the traditional risk factors for CAD, smoking, diabetes mellitus, hypertension, family history of CAD and obesity, presented in the table -I were not differ significantly between the two groups. Only dyslipidemia was found significantly higher in the exposed group than in the unexposed group.
Table I Sample characteristics
| Total (N) | 110 | ||
| Unexposed Group | Exposed Group | P-Value | |
| Age (Mean Age)
Gender N (%) Male Female Male/Female(ratio) |
51.54±12.60 yr.
(50)76.9 23.1 3.33 : 1 |
54.18±10.11yr
(30)66.7 33.3 2 :1 |
0.43ns
0.76ns |
| Risk Factors ((%) | |||
| Smoking | 55.4 | 55.6 | 0.64ns |
| Hypertension | 61.5 | 53.3 | 0.088ns |
| Diabetes mellitus | 43.07 | 33.33 | 0.06ns |
| Family h/o CAD | 41.5 | 37.80 | 0.215ns |
| Dyslipidemia | 58.46 | 71.11 | 0.013s |
| Obesity | 14.1 | 17.77 | 0.74ns |
Family h/o CAD=Family h/o Coronary Artery Disease. P<0.05.
Different type of Myocardial Infarction
In the present study of 110 patients, NSTEMI 26 (43.34%) more in unexposed group than exposed group. had anterior wall MI, 14 (23.33%) vs 12(24%), patients had inferior wall MI 6(12%) vs 9(15%) and 7 (14%) vs 8(13.33%) patients had anteroseptal MI and2(4%) vs 3 (5%) patients had anterolateral MI.
Table II types of Myocardial infarction of study subject (N=110)
| Types of MI | Exposed
(N=50)% |
Group | Unexposed
(N=60)% |
Group |
| Anterior MI | 12 | 24% | 14 | 23.33% |
| Inferior MI | 6 | 12% | 9 | 15% |
| Anteroseptal MI | 7 | 14% | 8 | 13.33% |
| Anterolateral MI | 2 | 4% | 3 | 5% |
| NSTEMI | 23 | 43.1% | 26 | 43.34% |
MI = myocardial infarction, NSTEMI=Non ST elevated myocardial infarction.
Table III Mean Serum magnesium level in mg/dl in study subject in first &fifth days. (N=110)
| Name of day | Exposed(n=50) | Unexposed(n=60) | P value |
| First day | 1.54±0.27 | 2.20±0.38 | < 0.05s |
| Fifth day | 2.12±0.27 | 2.32±0.16 |
Mean Serum magnesium significantly low in patients in exposed group which was statistically significant.
Table IV Association of serum magnesium level between STEMI and NSTEMI patients (N=110)
| Types MI | Unexposed Group (N=60) (%) | Exposed Group (N=50)(%) | p-value |
| STEMI | 34(56.66%) | 27(56.9%) | |
| NSTEMI | 26(43.34%) | 23(43.1%) | <0.005s |
| Total | 60(100.0) | 50(100.0) |
Unexposed= (S. Mg 1.6-2.4 mg/dl) Exposed = S. Mg <1.6mg/dl)
STEMI=ST segment elevated myocardial infarction, NSTEMI=Non ST segment elevated myocardial infarction p= <0.005
Serum magnesium significantly low in both STEMI and NSTEMI patients in exposed group which was statistically significant
Table V: Association of MACE with exposed and unexposed group (N=110)
| MACE | Unexposed Group
(N=85) (%) |
Exposed Group
(N=65) (%) |
p-value |
| Arrhythmia | 7(8.3%) | 31(63.1%) | <0.001s |
| LVF | 2(2.4%) | 9(13.8%) | <0.007s |
| Cardiogenic shock | 2(2.4%) | 7(10.8) | <0.031s |
| Death | 2(2.4) | 3 (4.8%) | <0.444ns |
Table V also shows the association of MACE with exposed and unexposed groups. Where Arrhythmia, LVF and Cardiogenic shock were statistically significant. The table shows that AMI patients with MACE are significantly higher in the exposed group.
Table-VI: Association of exposed and unexposed group between MACE present or absent (N=110)
| MACE | Unexposed
(N=60)(%) |
Exposed
(N=50)(%) |
p-value |
| Present | 13(15.3%) | 60(92.3%) | <0.05s |
| Absent | 72(84.7%) | 5(7.7%) | |
| Total | 85(100.0) | 65(100.0) |
Data were expressed as frequency and percentage, Chi-square test was done, s= significant MACE= Major adverse cardiac events
The above table shows that AMI patients with MACE is significantly higher in exposed group.
DISCUSSION
In this study, baseline characteristics of risk factors between the two groups were similar except for dyslipidemia. Regarding age distribution, the mean age of patients in the exposed group was more than that of the unexposed group and it was not statistically significant. Most of the patients were in the age range of 51-60 years in the unexposed group & 41-50 years in the exposed group of the study population. This observation was supported by Dwijanako. [13] Regarding gender, male patients were 50 (76.90%) and 30(67.70%) in the unexposed &exposed group respectively and the male: female ratio was; in the unexposed group 3.33:1 and exposed group 2:1. Male predominance was observed in both groups without significant difference (p=0.76). Similar results were found by Lopes, Ahmed and Zaid et al. [14, 16, 17] The present study showed less number of women than men in both the groups, only 23.1% and 33.3% of women in the unexposed group and exposed group respectively. This gender disparity is multi-factorial: less predisposition to CAD in reproductive age, overall less health care seeking attitude of female patients and less attention by male counterparts of their family. Regarding CAD risk factors in this study, smoking, diabetes mellitus, hypertension, family history of CAD and obesity, did not differ significantly between patients with exposed and unexposed group. Only dyslipidemia was found significantly higher in the exposed group than in unexposed group A (p=0.013). Dyslipidemia is a well-known risk factor for the development of coronary artery disease. In their study, Abd alamir [2] showed that dyslipidemia is associated with multivessel coronary artery disease and increased coronary artery calcium score. These factors may indicate the presence of severe CAD. Smoking rates were high in both groups, highlighting the need for stronger preventative measures against cardiovascular disease. Interestingly, the smoking rate was slightly lower in the exposed group compared to the unexposed group, which requires further investigation. This number is very large, thus requiring special attention in cardiovascular disease prevention programs. The present study found NSTEMI 26 (43.34%) more in unexposed group than exposed group. had anterior wall MI, 14 (23.33%) vs 12(24%), patients had inferior wall MI 6(12%) vs 9(15%) and 7 (14%) vs8 (13.33%) patients had anteroseptal MI and2 (4%) vs 3 (5%) patients had anterolateral MI. Similar observations were made by Mhatre MA et al & Rajhans Ret al. [15, 19]
Magnesium and Acute Myocardial Infarction
Magnesium, the fourth most abundant intracellular cation, plays a key role in a wide range of cellular functions. It has numerous critically important roles in maintaining the body’s normal homeostasis. One major role is in cardiac homeostasis. Magnesium is essential for ATP activation, which is necessary for the proper function of the sodium-potassium pump. It has also been implicated in the pathogenesis of acute myocardial infarction and its complications, such as arrhythmias. Low serum magnesium levels have been associated with inflammation and disturbances in the regulation of vascular tone and endothelial function. Additionally, magnesium is known for its role in maintaining electrical stability and energy balance within cardiomyocytes. Hypomagnesaemia (low magnesium levels in the blood) has been linked to atrial and ventricular arrhythmias, suggesting that low serum magnesium could also be a risk factor for sudden cardiac death. Table III shows mean serum magnesium level in two groups. It was significantly low in exposed group than unexposed group 1.54±0.27 vs2.20±0.38 on first day. This observation was supported by laxmi Mohananani 2019, Rasmussen HS et al and Shechter M et al. [21, 22, 23] Current research work showed that Serum magnesium significantly low in both STEMI and NSTEMI patients in exposed group which was statistically significant. In table IV it showed STEMI & NSTEMI 27(56.9%) VS 23(43.1%) in exposed group. Same observation was supported by Akila, A 2017 and Hasan MZ et al.2023. [5, 24] Table V also shows the association of MACE with exposed and unexposed groups. Where Arrhythmia, LVF and Cardiogenic shock were statistically significant. The table shows that AMI patients with MACE are significantly higher in the exposed group. Laxmi Mohananani 2019 showed Serum magnesium level (1.6402 vs 2.2833) was significantly low among the patients who were having arrhythmia as compared to those who were not having arrhythmia (p<0.001). Similarly mean QTc was prolonged (546.88 vs 404.33) among those having arrhythmia as compared to those who were having no arrhythmia (p<0.001). [21] All observed reduced magnesium levels in patients with acute myocardial infarction (AMI) compared to healthy controls. These findings suggest a potential link between magnesium deficiency and arrhythmias, a complication of AMI. In the present study, the serum magnesium level on day-1 was significant lower in patients with arrhythmias than those without arrhythmia (p<0.001). There was an increase in serum magnesium from Day-1 to Day-5 in both those with arrhythmias and those without arrhythmias. This study also highlighted the association between low magnesium levels and arrhythmias. Overall, this study supports the routine monitoring of magnesium levels in cardiovascular patients. However, it highlights the need for further research to clarify the optimal magnesium level and its impact on patient outcomes.
CONCLUSION
The key takeaway is the importance of monitoring magnesium levels in AMI patients, but the benefit of correcting deficiencies remains unclear.
RECOMMENDATION
- Every AMI patient should do Serum Magnesium level during admission period to have close supervision monitoring whether the complication is associated with low serum
- Scrum magnesium levels were apparently lower in patients with complications as compared in who had uneventful recovery.
- Overall, this section highlights the need for further research on the role of magnesium in cardiovascular health.
Conflict of interest: None
REFERENCES
- Abraham, A.S., Eylath, U., Weinstein, M. and Czaczkes, E., 1977. Serum magnesium levels in patients with acute myocardial infarction. New England Journal of Medicine, 296(15), pp.862-863.
- Abd alamir M, Goyfman, M, Chaus A, Dabbous F, Tamura L, Sandfort V, Brown A, Budoff M,2018, ‛The Correlation of dyslipidemia with the extent of coronary artery disease in the multiethnic study of atherosclerosis,’ Journal of Lipids.2018:13, 1–9.
- Ahmed M, Rubaiyat KA, Saleh MA D, Chowdhury AW, Khuda C K E, Ferdous KA F, Hasan N, Hoque ATM, Islam KN, Amin MG, 2018, Clinical characteristics and angiographic profile of acute coronary syndrome patients in a tertiary hospital of Bangladesh, Bangladesh Heart Journal. 33: 1, 10– 15.
- Akar, JG & Akar, FG 2007 ‛ Regulation of ion channels and arrhythmias in the ischemic heart,‘ J Electrocardiol. 40: S37-S41.
- Akila, A., Anandaraj, J., Karthikeyan, S. 2017. Serum Magnesium Levels in Acute Myocardial Infarction. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS), 16(5), pp.35-40.
- Burton, FL& Cobbe, SM 2001,‛ Dispersion of ventricular repolarization and refractory period,’ Cardiovascular Res, 50: 10-23.
- Carmeliet, E 1999, ‛Cardiac ionic currents and acute ischemia: from channels to arrhythmias,’ Physiol Rev. 79: 917-1017.
- Choudhury, M.B.K., Rahman, M.S., Hassan, M.M., Begum, R., Hoque, N., Akhtaruzzaman, M. and Chowdhury, A.N., 2011. Comparison of Serum Magnesium and Potassium in Acute Myocardial Infarction and Chronic Ischemic Heart Disease. Journal of Dhaka National Medical College & Hospital, 17(1), pp.33-36.
- Chowdhury, A.W., Alam, N., Khan, H.L.R., Sabah, K.M.N. and Amin, M.G., 2015. The pattern of cardiac disease at the coronary care unit of Dhaka Medical College Hospital. Cardiovascular Journal, 7(2), pp.119-122.
- Coronary Artery Disease – STEMI Topic Review. Downloaded from: https://www.healio.com/cardiology. Retrieved on March 2020
- Dwijanarko W, Maharani, E & Anggrahini, D 2017, ‛T Peak–T End Interval Alteration as Parameter of Successful Fibrinolysis in Patients with ST Segment Elevation Acute Myocardial Infarction,’ Acta Cardiologia Indonesian a. 3: 1. 14-22
- Fatema K, Zwar N, Milton A, Ali L, Rahman B, 2016, ‛Prevalence of Risk Factors for Cardiovascular Diseases in Bangladesh: A Systematic Review and Meta-Analysis,’ PLoS ONE.11 (8): 1-14.
- Kieboom, B., Niemeijer, M., Leening, M., Marten, E. (2016). Serum Magnesium and the Risk of Death From Coronary Heart Disease and Sudden Cardiac Death. J Am Heart Assoc, 5(1): e002707
- Lopes NH, Grupi C, Dina CH, De Gois AF, Hajjar LA, Ayub B, 2006, ‛QT interval dispersion analysis in acute myocardial infarction patients: coronary reperfusion effect,’ Arq Bras Cardiol. 87: 91-8.
- Mhatre MA, Sirur FM, Rajpal DR, Shah MR. A clinical study of arrhythmias associated with acute myocardial infarction and thrombolysis.Int J Res Med Sci. 2017 Jan;5(1):335.
- Mohan, G., Jain, V., 1994. Serum magnesium: A prognostic tool of acute MI. Indian J Physiol Pharmacol, 38(4), pp.294-296.
- Naksuk, N., Hu, T., Krittanawong, C., Thongprayoon, C., Sharma, S., Park, J. (2017). Association of Serum Magnesium on Mortality in Patients Admitted to the Intensive Cardiac Care Unit. The American Journal of Medicine, 130, pp.221-229.
- Parikka, H., Toivonen, L., Naukkarinen, V., Tierala, I., Pohjola-Sintonen, S., Heikkilä, J. and Nieminen, M.S., 1999. Decreases by magnesium of QT dispersion and ventricular arrhythmias in patients with acute myocardial infarction. European Heart Journal, 20(2), pp.111-120.
- Rajhans R, Narayanan M. Assessment of arrhythmias in 50 patients of ST-elevation myocardial infarction after thrombolysis: a 24 hour Holter study. Int J Adv Med. 2017;4(3):734-40.
- Roth, G, Mensah, G, Johnson, C. et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J Am Coll Cardiol. 2020 Dec, 76 (25) 2982– 3021. https://doi.org/10.1016/j.jacc.2020.11.010
- Laxmi Mohanani, Kuldeep Deopujari , Raghvendra Singh Meena, T. N. Dubey . Serum magnesium level and QTc interval prolongation in acute myocardial infarction patients and its correlation with arrhythmias. Int J Res Med Sci. 2019 Nov;7(11)
- Rasmussen HS, Norregard P, Lindeneg O, McNair P, Backer V, Balslev S. Intravenous magnesium in acute myocardial infarction. The Lancet. 1986 Feb 1;327(8475):234-6.
- Shechter M, Hod H, Marks N, Behar S, Kaplinsky E, Rabinowitz B. Beneficial effect of magnesium sulfate in acute myocardial infarction. The American J Cardiol. 1990 Aug 1;66(3):271-4.
- Hasan MZ, Nahar K , Sharif JU , Paul SC , hakur AK , Mahmud A , Siddique NA , Islam MR , Paul GK. Serum Magnesium Level and It’s Relation in Predicting Adverse In-Hospital Outcome in Patients with First Attack of Myocardial Infarction.MMJ, 01 Jan 2023, 32(1):65-72
PMID: 36594303