
Levels of Mental Health Literacy amongst University Students: Findings from a University in Masvingo Province, Zimbabwe
- Tonderai Masara
- Herbert Zirima
- 826-837
- Jul 3, 2024
- Mental health
Levels of Mental Health Literacy amongst University Students: Findings from a University in Masvingo Province, Zimbabwe
Tonderai Masara1, Herbert Zirima2
1Mental Balance Series
2Great Zimbabwe University
DOI: https://dx.doi.org/10.47772/IJRISS.2024.806065
Received: 14 May 2024; Revised: 29 May 2024; Accepted: 01 June 2024; Published: 03 July 2024
ABSTRACT
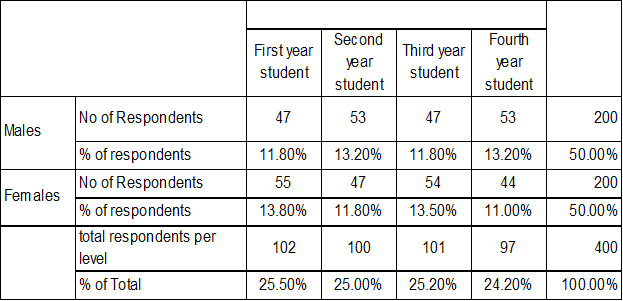
There is an increase in number of people roaming the streets with visibly clear mental health issues in every city and town in Zimbabwe. With the functional mental health legislations and policies in Zimbabwe, the researcher saw the need to use a quantitative approach, to investigate the level of knowledge on symptoms, accuracy on correct identification of mental health disorders, and level of mental health literacy of undergrad students at Great Zimbabwe University. The research made use of a population of 10,236 Great Zimbabwe university undergraduate students, and Cochran statistics was used to generate a sample size of 371 university undergrad students with an additional 19 more sample participants collected, making a total of 400 research sample participants. Representative and random sampling methods were used with closed-ended standardized questionnaires (Mental Health Literacy Assessment Inventory (MHLAI). The collected data was presented and analyzed using a descriptive research approach, precisely descriptive statistics. The information was presented in cross-tabulation tables that included gender and level of study. Results obtained showed that, the researcher failed to reject the null hypothesis of the study using the independent t test of -.135 and the Mann-Whitney U, Z score of -.129 and concluded that gender did not affect the level of mental health disorders’ symptom identification and mental health literacy levels. An overall total calculation of 50.51 percent responses of students are mental health literate, with 42.24 percent correctly displaying knowledge, 67.50 percent positive ways to prevent and 51.60 percent positive attitude. In terms of mental health disorder accuracy, 21.03 percent of male responses were 0.2 percent lower than 21.23 percent of female responses. The researcher concluded by outlining a model magazine strategy to increase mental health awareness in order to improve and make the world a better place. This study is of great significance as it highlights the level of mental health literacy amongst undergrad university students at Great Zimbabwe which can be used to project to the level of literacy in policy and legislation alignment. The study can be used to address the mismatch that exist with the number of unaccounted mental health people at government levels as a continuous alignment to benefit the populace.
Keywords: Levels, Mental health, literacy
INTRODUCTION
The kind and nature of interventions used in society are influenced by the degree of literacy that people have on mental health issues. This is a ground-breaking study that tracks mental health disorder literacy levels in Zimbabwe, despite the treatments already in place in the nation to make sure that people perform at their best. Such research is more crucial than ever because cultural, traditional, and Christian beliefs on mental diseases have overlapping and perplexing perceptions on the genesis of the illness, the illness itself, treatment, and prevention. According to one’s beliefs—which can range from spirituality to biology—there are numerous interpretations. The Great Zimbabwe University’s study will help Zimbabwe’s efforts to provide specialized interventions by further aligning and correcting the mismatch that currently with the number of mentally challenged people. According to earlier research, people with lower mental health literacy are less likely to actually seek mental healthcare, to intend to seek care, and to use psychotherapy and psychiatric medications afterward. These findings suggest that there is a higher level of unmet need for mental healthcare in this population, Waldmann T et.al (2020)
Statement of the Problem
The 2030 Sustainable Development Goals, notably SDG 3 on Good Health and Well-Being and SDG 4 on Quality Education, acknowledge the need to attain global good health. In essence, the SDGs promote knowledge about good health and the welfare of all people, including access to health facilities and the capacity to identify issues with one’s own and other people’s mental health. The Zimbabwe Mental Health Policy, which guarantees that every citizen has access to their fundamental human right to mental health without discrimination, is one of the many ways in which Zimbabwe has taken a stand on the issue of mental health. The government understands how critical it is to safeguard each citizen’s mental health, so it is necessary to address important issues like whether people are aware of and able to recognize mental health disorders, as well as whether the supply of mental health care facilities is adequate in comparison to demand.
Therefore, from the policy point of view, the legislations and policies on mental health seems to have covered all necessary grounds. However, it remains a question to answer if the intended population is well versed with what the policies and legislation says. This also comes as a result of the number of mentally challenged people whom are increasingly roaming the streets in every city and town in Zimbabwe. The immediate question will be, is there knowledge on how to identify mental health issues and help one another if there is such need or the availability of institutions to deal with such services. This is the central focus area of this research paper, to find out the levels of mental health literacy amongst university students.
Although policies and proper legislations are in place to cater for mental health care, it remains a mystery in need to be addressed by finding out if people are knowledgeable of the mental health disorders. One cannot be able to exercise their right to health if they lack the information to recognize mental health problems. There is overwhelming evidence with global consensus on the advantages and disadvantages of high levels of mental health literacy available in literature. However, relatively few researches in Africa have examined the level of mental health literacy on the continent. Literature available shows that there is scarcity of literature researches exploring the level of mental health literacy in Zimbabwe.
Purpose of the Study
Through a quantitative research approach, the study aims to determine the level of mental health literacy among undergraduate students at Great Zimbabwe University. The researcher intended to fill a knowledge gap on mental health literacy in the country for policy and legislation alignment. The degree of mental health literacy in the nation was evaluated in this study using a sample of students from Great Zimbabwe University against the backdrop of an increase in the number of people with obvious mental health difficulties wandering the streets. According to earlier research, people with lower mental health literacy are less likely to actually seek mental healthcare, to intend to seek care, and to use psychotherapy and psychiatric medications afterward. These findings suggest that there is a higher level of unmet need for mental healthcare in this population, Waldmann et.al (2020).
Objectives
- To investigate students’ knowledge of symptoms of mental health disorders.
- To assess the extent of the accuracy of students’ knowledge of mental health disorders.
- To assess the level of mental health literacy amongst undergrad students at Great Zimbabwe University
- To compare the knowledge level of mental health disorders between male and female students.
- To use obtained data to propose an appropriate model for mental health literacy in the country as a whole.
Hypothesis
- Female undergraduate students do not have significantly different levels of knowledge about mental health disorders as compared to male students.
- There is no significant difference between male and female undergrad students’ mental health literacy at Great Zimbabwe University.
METHODOLOGY
Research Design
The descriptive research design was used by the researcher, which is a scientific method of describing and interpreting the current state of individuals, settings, conditions, or events without interfering with it. Mertler (2021). The researcher wished to describe, explain, and validate the levels of mental health literacy among Great Zimbabwe University undergraduate students.
According to Ji (2022), descriptions that come about as a result of creative exploration help to organize the findings so that they fit with explanations, which are subsequently evaluated or confirmed. The researcher refers to the method as creative since it frequently sheds light on information that is difficult to find or that individuals might not easily unearth, and this investigation required such expertise.
Sampling Strategy
In this study, representative and random sampling were both used. In order to rule out the possibility of biased samples, the researcher made sure that the three fundamental requirements of unbiased samples were met, resulting in more confidence conclusions about the general populace from the collected results. In order to lessen the degree of sampling error and increase the confidence in drawing statistical conclusions from the sample employed, this study used representative sampling and random sampling as two strategies. A representative sample represents important aspects and traits of the wider society being studied, Hugh C. (2024). For instance, in this study, the best respondents were chosen based on their gender and level of education. On the other hand, a random sample is a group that is selected at random from a larger population such that each person in the study’s larger group has an equal chance of being chosen, Hugh C. (2024). With the aid of the class representative, random selection was now done at the study level to choose participants from a list of numbers that had been prepared and randomly chosen. The next step was to send them a link to a survey via Facebook and WhatsApp. Participants responded 100% of the time thanks to the use of both platforms.
Table 1. Showing Gender and Level of Study Cross-tabulation
Instrument
In order to conduct this study, the researcher developed the Mental Health Literacy Assessment Inventory (MHLAI) instrument with the use of the Diagnostic and statistical manual of mental disorders (5th ed., text rev) DSM V TR, American Psychiatric Association. (2022) and the mental health literacy scale. The African cultural background and environment were taken into account when O’Connor, M., and Casey, L. (2015) designed the Mental Health Literacy Scale. The created tool was a closed-ended, standardized questionnaire with sections that closely connected or joined the research’s goals and conceptual framework. The respondent’s biographical information was gathered in Section A, which was sorted. To determine the respondent’s aptitude for accurately identifying or recognising the illnesses, Section B was sorted.
Section C of the questionnaire, which probes the respondent’s health-seeking behavior, and Section D, which inquiries about one’s familiarity with some self-help strategies and ways of maintaining good mental health. In keeping with the researcher’s choice of quantitative research design of objectivity, standardized questions were used because they promote the gathering of responses objectively. This was consistent with Barker, Pistrang, and Elliott’s (2015) claim that standardized questionnaires allow practitioners to independently verify the measurement statements of other practitioners. Standardization allows for more accurate scientific reporting and statistical analysis than subjective conclusions.
Research Procedure and Ethical Considerations
The Great Zimbabwe University’s Study and Postgraduate offices were consulted for approval, and all research procedures and ethical issues were made clear to them. In order to quickly acquire contact information for participants from all levels and programs from where they originated, the researcher sought out all contact information for class reps from each program and level. The participants were told why their information was being collected and how it would be used, and all ethical procedures were followed. Relationships that were personal or private were not permitted since they could manipulate participants. As a result, the goal of this study was to exclude any type of bias or manipulation and to portray the genuine results of the individuals.
Data Analysis
After testing the hypothesis stated above, one can only make an assumption or validate whether or not undergrad students at Great Zimbabwe University are mental health literate. The data gathered was then entered into SPSS to test the hypothesis. An independent t test was also used as a parametric test to compute a hypothesis.
RESULTS
The study assessed students’ ability to correctly identify mental health disorders. The section consisted of ten questions with descriptions of symptoms of various mental health disorders, and the combined responses of level 1 to 4 students showed that 22.10 percent (884 responses) responded with “extremely unlikely,” and 35.26 percent (1426 responses) responded with “unlikely.” As a result, 57.76 percent (2310) of total student responses failed to correctly identify symptoms of mental health disorders. In comparison, 23.13 percent (925) of responses were marked as likely, and 19.13 percent (765) were marked as extremely likely. As a result, 42.24 percent (1690) of student responses correctly identified the symptoms being asked.
The study evaluated the students’ help-seeking behavior, and the findings revealed that 50.37 percent of the students’ responses failed to correctly identify with positive or good health-seeking behaviors. Of the 50.37 percent (1210) responses, 22.79 percent (547) were classified as extremely unlikely, while 27.63 percent (663) were classified as unlikely. When we add these two figures together, we get (547+663=1210), or 50.37 percent. In comparison, 49.53% of responses were correctly identified as positive or good health-seeking behaviors. According to this figure, 29.79 percent (715) of responses were deemed likely, while 19.79 percent (475) were deemed extremely likely. Combining these two figures yields 475 and 715 responses, for a total of 1190 responses, or 49.53 percent.
When asked how to prevent some mental health disorders, 32.5 percent of students said it was unlikely or extremely unlikely, while 67.5 percent said it was likely or extremely likely. Third-year students recorded the most likely and extremely likely responses, accounting for 70.9 percent of all responses, followed by second-year students with 69.8 percent. Overall, 32.5 percent of students answered extremely unlikely or unlikely, while 67.5 percent answered extremely likely or likely.
According to the findings on student attitudes toward people with mental health disorders, 51.60 percent of student responses are willing and have a positive attitude toward mentally challenged people. The total of 51.60 percent (619) responses is comprised of 31.80 percent (381) responses indicating willingness and 19.80 percent (238) responses indicating extreme willingness.
A cross tabulation of the results extracted using the gender of students shows that 57.75 percent (2310) of both male and female responses failed to accurately identify the mental health disorders being asked for, with 28.98 percent (1159) male responses and 28.78 percent (1151) female responses failing to accurately identify the symptoms asked for. A total of 28.98 percent (1159) is derived from 10.80 percent (432) of male responses that failed to correctly identify MHDS and responded on extremely likely, and 18.18 percent (727) from male responses that responded on unlikely. Furthermore, 28.78 percent (1151) of female responses failed to correctly identify the MHDS asked, with 11.30 percent (452) scoring extremely unlikely and 17.48 percent (699) scoring unlikely.
Ho: Female undergrad students do not have significant different level of knowledge on mental health disorders to male students
The Mann-Whitney U-test was used to test the hypothesis and test statistics yields a Z value of -.129 and a P value of.897. As a result, p > 0.05 indicates that there is less disagreement between our data and the null hypothesis and that the groups under study are likely to be aware of the same mental health disorders. In this scenario, we fail to reject the null hypothesis that there is no significant difference in the knowledge of mental health disorders between female and male undergrad students. The researcher then concludes that the gender of the students has no bearing on their understanding of mental health disorders.
Table 2 Disorders Test Statistics
| Mann-Whitney U | 19851.000 |
| Wilcoxon W | 39951.000 |
| Z | -.129 |
| Asymp. Sig. (2-tailed) | .897 |
a. Grouping Variable: 1. Gender
An overall computation of results shows that Great Zimbabwe University students have mental health literacy with 50.51 percent responses cases, compared to 49.49 percent of the time. A total of 50.51 percent (4849) of respondents have mental health literacy, which is made up of 30.20 percent (2899) who responded likely / willing on attitude and 20.31 percent (1950) who responded extremely likely or extremely willing. Calculating the two parts yields a total of 50.51 percent responses, indicating that Great Zimbabwe University students are mentally healthy. In comparison, a total of 49.49 percent (4751) responses indicate a figure with no mental health literacy. These total figures are derived from a total of 19.08 percent (1832) responses directed at extremely unlikely or extremely unwilling people, and a total of 30.41 percent (2919) responses directed at extremely unlikely or extremely unwilling people.
Ho: There is no significant difference between male and female undergrad students’ mental health literacy at Great Zimbabwe University
The independent t test yields f value of .397 and a p value of.893 (p > 0.05), resulting in a t value of -.135. As a result of the results presented, the p value is greater than 0.05, and the researcher fails to reject the null hypothesis, noting that there is no significant difference in mental health literacy between male and female undergrad students.
DISCUSSION
Findings from this objective’s assessment of the levels of mental health literacy among Great Zimbabwe University undergraduate students reveal that 50.51 percent of students are mental health literate. The researcher believes that undergrad students at Great Zimbabwe University have a pretty decent mental health literacy level as demonstrated by findings that are just above 50%, whereas 49.49 percent of responses show that students do not have mental health literacy. This data, given that it is one of the first studies to research such an issue to date, leaves much to be desired and needs further exploration to understand and arrive at a better understanding of why there is a fairly good result of literacy on university students. Research is required to gain a deeper understanding of the relationship between knowledge, beliefs, and attitudes in diverse cultural contexts, as well as the relationship between particular stigma types and proactive help-seeking.
There is great strides on mental health research in Africa as a whole. Health Literacy Among Young People in Africa, Evidence Synthesis a study by Amanu A, et.al (2023). The research showed that low health literacy was common among young people, and there was a significant association between low health literacy and negative health outcomes among this group. Health literacy among young people was impacted by a wide range of socio-demographic factors. On this research subtle mental health concerns can cause people to put off getting help. For the public to be protected against mental diseases, it is crucial to recognize mental signs and symptoms very away. Data on the identification of symptoms of mental health issues showed that, while 42.24 percent (1690) of student responses correctly identified the symptoms being asked, 57.76 percent (2310) of student responses could not. The Social Development School of thought holds that a kid should progressively learn about mental health, however the findings indicate that students of various ages and educational levels have not succeeded in gradually learning about mental health literacy. Additionally, the Social Construct school of thought maintains that the community should build a child, and the results indicate that the community lacks or has a mental health disorders identification gap because their end products, the students, failed to correctly identify the mental health disorders symptoms being asked.
This research demonstrated that first-year students outperformed fourth-year students by 11.15 percent in their ability to correctly identify the symptoms of mental health disorders. These findings indicate that by fourth year, a student may have suffered a loss or decrease in their mental health disorder symptom identification by 2.48 percent. The general assumption is that university is the highest level of learning and knowledge acquisition, implying that individuals should be more valuable in all aspects of life. In contrast, the university appears to lack the motivation to empower students in the area of mental health. Aging is associated with two areas of change that may increase the importance of knowledge in later life. First, aging is associated with declines in the efficiency of cognitive processes Salthouse & Miles, (2002). Secondly, knowledge, representing the long-term products of processing, is relatively well-preserved in later life as reflected in stable levels of crystallized ability e.g., Salthouse, 2000; Schaie, (1993). With the results gained above, it seems age and level of education is slowly wearing away the early life knowledge of mental health as older people who should be full of wisdom tend to be mental health bankrupt.
Another study contacted in Swiden on how gender and low mental health literacy are related to unmet need for mental healthcare: a cross-sectional population-based, Blom (2024). The study unveiled that men and women who are linked with low mental health literacy were most likely to not perceive a need for mental healthcare, education, poor mental health and to refrain from seeking mental healthcare, Blom (2024). This study on Great Zimbabwe students is constant agreement with such results as the findings of the research showed that, the researcher failed to reject the null hypothesis and concluded that gender itself does not affect mental health literacy.
A significant comparative study on students was carried out in the United States on evaluating mental health literacy amongst US college students: a cross sectional study, Ariel K. T et.al (2024). The United States study shows that individuals who had a previous mental disorder diagnosis had significantly higher scores than those with no previous diagnosis hence a significant positive relationship was found between mental health literacy and self-compassion. On this Great Zimbabwe University study 42.24 percent of students who correctly identified the mental health symptoms described in this study closely resemble results from a developing country. According to the findings, social constructionism theory suggests that higher-scoring individuals, live in a better-equipped community. This can as well sum that, the environment and educational materials includes and involves more accessible to mental health materials hence the more they progress with their lives the more mental health information is availed to them.
When discussing mental health issues in an African environment, it is challenging to overlook cultural and traditional beliefs of the people. It is believed that certain aspects of mental health have definitions, meanings, and western connotations that are distinct from those in Africa. Richter, D et.al, (2023) state that there are various approaches to describe and understand mental illnesses. Research spanning cultures shows that developed countries have greater levels of mental health literacy, notably the ability to identify mental illnesses. We can therefore draw the conclusion that, as demonstrated by the published statistics comparing regional African research, Africans are making progress in terms of acceptability because it is an established approach of promoting mental health wellbeing. Zimbabwe is also part of the African progress with 50.51% mental health literacy rate on undergrad students from Great Zimbabwe University.
A similar study was conducted on Mental health literacy among primary healthcare workers in South Africa and Zambia Korhonen J (2022). The results shows that on closer inspection of individual items, it was discovered that the respondents found knowledge-related questions more difficult. With this in mind, the results highlight the need for standardized mental health education by demonstrating heterogeneous MHLs among PHC workers Korhonen J et.al (2022). By contrast, this Great Zimbabwe research revealed that only 42.24 percent undergrad students were able to display knowledge on identification of mental health disorders symptoms. This however reflects a deeper problem as when one is unable to correctly identify a mental health their attitude and health seeking behavior for themselves and others will be questionable as well. There is need to put all hands on the deck so that everyone jump on the mental health awareness train and start educating one another about it.
The fact that gender has no bearing on comparative performance is an intriguing benefit of the government of Zimbabwe’s programs for gender inclusion. The results suggest that there is just a 0.2 percent difference between male and female students failing to accurately identify, leading to this statement about the accuracy of information on mental health disorders symptoms recognition. To arrive at this number, 28.78 percent of female responses were subtracted from 28.98 percent of male responses. The accuracy of female responses was higher than male responses by a particular percentage of 0.2 percent. Comparatively to the United States study by Ariel K.T et.al (2024), it shows that women scored significantly higher than men (p < .01) on mental health literacy. The same results can be said to have been observed on Great Zimbabwe University study as women scored more than .02 than men. A lot can be said on the reasons why this results and one of it being women visits the hospitals in African setups than males. There is more mental health educational visuals in hospitals than any other places in Zimbabwe.
CONCLUSION
- Results from first-year students reveal that primary and secondary school curriculums in Zimbabwe lacks knowledge about mental health conditions. This is demonstrated by the noticeable decline of knowledge figures displayed by forth year students and first year students. A further indication that tertiary education falls short in imparting and upholding students’ knowledge of mental health is the decline in knowledge figures as they go up to fourth year students.
- The researcher concludes that the university environment is a challenging place in all aspects of life that requires a strong mental health support system to educate and keep students’ wellbeing in check. The decline of mental health knowledge and ability to identify symptoms reflects a gap in the education environment that needs a close consideration to empower students with proper and expected knowledge for wellbeing.
- The researcher can confidently conclude that the knowledge accuracy level is very low and requires extensive education efforts, based on the 57.75 percent figure obtained on mental health disorder symptoms identification, where participants failed to correctly identify symptoms being asked. There is need for more knowledge to be made accessible to the students.
- Based on the two hypotheses tested in this study, it is possible to conclude that gender has no bearing on one’s level of mental health literacy. And knowledge is a personal process that cannot be hampered or influenced by gender.
- Furthermore, the researcher can conclude that a figure of 50.51 percent indicates that there is mental health literacy amongst undergrad students at Great Zimbabwe University.
- There is a need for extensive work on mental health disorder awareness in order to increase the population’s mental health literacy.
RECOMMENDATIONS
This research has opened the door to a greater comprehension of how and where to act, in line with the mission of the World Health Organization to uphold and protect everyone’s mental health. The following recommendations is given in this regard:
- The country should launch a comprehensive mental health education and awareness campaign. While the Ministry of Health and Child Care, in collaboration with the Ministry of Information, Publicity, and Broadcasting Services, should take the lead in this regard, other stakeholders, including civil society organizations, are encouraged to get involved. Psychologists and other mental health professionals are being challenged to stop being keyboard “warriors” and instead organize mental health awareness campaigns to bring mental health to the people. Newspapers, magazines, social media platforms, radio, and television will be useful in advancing this cause.
- The government, through the Ministry of Primary and Secondary Education and the Ministry of Higher and Tertiary Education, Innovation, Science and Technology Development, should incorporate mental health into the country’s educational curriculum. This should see schools and tertiary education facilities teaching about mental health on the HIV and Aids teaching model, for instance. Additionally, the Ministry of Higher and Tertiary Education, Innovation, Science and Technology Development, in conjunction with the Ministry of Health and Child Care, should introduce short-to-medium-term courses on mental health to equip trainees to identify illness and perform first aid, amongst other critical issues. Lessons should be drawn from countries such as Australia and the United Kingdom’s First Aid Program. While this should be open to everyone, including pastors, traditional leaders, and individuals, the program should target village health workers who already play a key role in the promotion of community health, especially in rural areas.
- The government, through the Ministry of Health and Child Care, should ensure the availability of suitably qualified mental health professionals in adequate numbers at all health facilities in the country to promote easy access to mental health services. Among other key duties, these professionals should conduct mental health awareness campaigns at the community level.
- The government, through the Ministry of Health and Child Care, should ensure the availability of suitably qualified mental health professionals in adequate numbers at all medical facilities in the country to promote easy access to mental health services. Among other key duties, these professionals should conduct mental health awareness campaigns at the community level.
- In view of the prevalence of mental health challenges in the country and in line with international trends, the government should recognize the role played by psychology professionals in promoting citizens’ health. To this end, the government should enact a policy to ensure that all educational institutions and corporates, amongst other institutions, recruit a psychologist to provide mental health information and counseling services to the usually large number of people who frequent these spaces. Lessons can be drawn from the United Arab Emirates, where all schools are manned by psychologists and social workers.
- The Ministry of Health and Child Care should, as a matter of urgency, introduce and publicize a 24-hour toll-free mobile/telephone service facility to cater for mental health issues.
- The Parliament of Zimbabwe should review the Mental Health Act [Chapter 15:12] of 1996 in line with developments and to amplify the role of Psychology professionals in the country.
- The Ministry of Health and Child Care will lead World Mental Health Celebrations at a national level. In essence, the Ministry should organize a visible platform to sensitize people on mental health issues to be widely covered by the media.
FURTHER RESEARCH
Future research may explore the correlation between the components of mental health and their contribution to mental health literacy. Another study needs to be done to explore the correlation between attitude and literacy levels and mental health. In addition, cultural values can be explored as well to ascertain how they affect mental health literacy. Furthermore, studies can be conducted to examine the literacy level in relation to different mental health disorders.
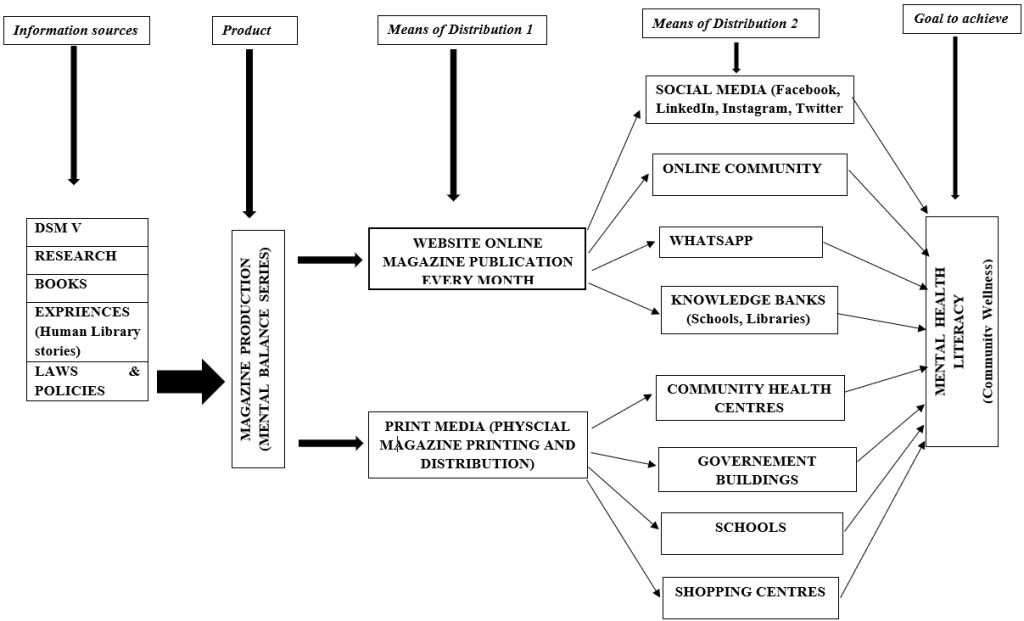
MODEL
This research will give birth to a Magazine model which stands to have its services freely accessible and named the Mental Balance Series. This model can be accessed through the website and print media platforms with the aim of promoting mental health awareness to the community. The publications will be made sure to comprise of always updated verified correct mental health awareness information. The magazine will be produced on a monthly basis, and made available on the website for sharing on different online platforms and also in print form. The network’s services will be available on WhatsApp (a tool that makes it simple to transmit content to individuals) and social media platforms, which need having up-to-date Facebook, LinkedIn, Twitter, and Instagram pages. Other online and offline communities can gain from this because it will also be printed and distributed in key locations. As a result, there will be a step taken to fill the information gap about the availability of mental health literature, which will benefit the knowledge bank of the community and educational institutions. Due to the requirement for proper information dissemination and the possibility of diagrammatic illustration, this model is best suited to be operated by qualified experts as shown below.
REFERENCE
- Amanu A A, Birhanu Z, Godesso A. Health Literacy Among Young People in Africa: Evidence Synthesis. Risk Manag Healthc Policy. 2023;16:425-437 https://doi.org/10.2147/RMHP.S399196
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
- Barker, C., Pistrang, N., & Elliott, R. (2015). Research methods in clinical psychology: An introduction for students and practitioners. John Wiley & Sons.
- Blom, S., Lindh, F., Lundin, A. et al. How gender and low mental health literacy are related to unmet need for mental healthcare: a cross-sectional population-based study in Sweden. Arch Public Health 82, 12 (2024). https://doi.org/10.1186/s13690-023-01228-7
- Hanurawan, F. (2012). Qualitative research in psychology. Journal of Educational, Health and Community Psychology, 1(2), 120-132.
- Hugh C. (2024) Research Methods and Statistics in Psychology 8th Edition. Routledge London. https://doi.org/10.4324/9781003215967
- Ji, J. , Zhao, N. and Liu, G. (2022) Research on the Application of Krathwohl Classification in Ideological and Political Education of Professional Courses. Creative Education, 13, 1554-1563. doi: 10.4236/ce.2022.135097.
- Jorm A. (2000) Mental health literacy; public knowledge and beliefs about mental disorders. British Journal of Psychiatry. 2000; 177:396-401.
- Jorm, A. (2015), Why We Need the Concept of “Mental Health Literacy, Health Communication, volume 30, pages1166 – 1168
- Korhonen J, Axelin A, Stein DJ, Seedat S, Mwape L, Jansen R, Groen G, Grobler G, Jörns-Presentati A, Katajisto J, Lahti M; MEGA Consortium/Research Team. Mental health literacy among primary healthcare workers in South Africa and Zambia. Brain Behav. 2022 Dec;12(12):e2807. doi: 10.1002/brb3.2807. Epub 2022 Nov 3. PMID: 36326480; PMCID: PMC9759138.
- Krathwohl, D. R. (1993). Methods of educational and social science research: An integrated approach. Longman/Addison Wesley Longman.
- Kristina, S. A., Mardea, N. A., Ramadhani, F., & Aliyah, H. (2020). Mental health literacy among university students in Yogyakarta. Mental Health, 25(04).
- Kutcher, S,Wei Y, Coniglio C. (2016). Mental Health Literacy: Past, Present, and Future. Can J Psychiatry. 2016 Mar;61(3):154-8. doi: 10.1177/0706743715616609. PMID: 27254090; PMCID: PMC4813415.
- Mertler, C.A., Vannatta, R.A., & LaVenia, K.N. (2021). Advanced and Multivariate Statistical Methods: Practical Application and Interpretation (7th ed.). Routledge. https://doi.org/10.4324/9781003047223
- Mwambwa-Johnson, E. Y. (2021). Mental Health Literacy Among Rural and Urban Young Adults in Zambia (Doctoral dissertation, Walden University).
- NHS England. (2019). The NHS Long Term Plan https://www.longtermplan.nhs.uk/wp-content/uploads/2019/01/nhs-long-term-plan-june-2019.pdf
- Nightingale, D. J., & Cromby, J. (2002). Social constructionism as ontology: Exposition and example. Theory & Psychology, 12(5), 701-713.
- O’Connor, M., & Casey, L. (2015). The Mental Health Literacy Scale (MHLS): A new scale-based measure of mental health literacy. Psychiatry research, 229(1-2), 511-516.
- Richter, D., & Dixon, J. (2023). Models of mental health problems: a quasi-systematic review of theoretical approaches. Journal of Mental Health, 32(2), 396–406. https://doi.org/10.1080/09638237.2021.2022638
- Rickwood, D., & Thomas, K. (2012). Conceptual measurement framework for help-seeking for mental health problems. Psychology research and behavior management, 5, 173.
- Shotter, J., & Gergen, K. J. (1994). Social construction: Knowledge, self, others, and continuing the conversation. Annals of the international communication association, 17(1), 3-33.
- Sibindi, C., Mushambwe, T., Mageza, A., & Socci, A. (2021). Population characteristics, outcomes, and center wide insights of the Zimbabwe national experience with the SIGN intramedullary nail (2013–2020). International Orthopedics, 1-8.
- The Sustainability Development Goals of the United Nations (UN) for the advancement of good health worldwide are Good Health and Well-Being (SDG-3), and (SDG-4) Quality Education. https://www.undp.org/sustainable-development-goals?utm_source=EN&utm_medium=GSR&utm_
- Vygotsky, L. S., & Cole, M. (1978). Mind in society: Development of higher psychological processes. Harvard university press.
- Waldmann T, Staiger T, Oexle N, Rüsch N. Mental health literacy and help-seeking among unemployed people with mental health problems. J Mental Health. 2020;29(3):270–6. https://doi.org/10.1080/09638237.2019.1581342.
- World Health Organization, (WHO), (1998), Life in the 21st century A vision for all, Report of the Director-General, World Health Organization 1211 Geneva 27, Switzerland
- Yarahmadi, F. (2020). Multistage Sampling Technique and Estimating Sample Size for a Descriptive Study on Viewers’ Perception of TV Commercials. SAGE Publications Ltd.
- Zimbabwe Mental Health Policy http://zdhr.uz.ac.zw:808/