
Postpartum Depression: Risk Factors and Prevalence in Adolescent Girls and Young Women (AGYWs) in Gwanda, Zimbabwe
- Honest Tshuma
- Bhekisisa I. Madololo
- Sheron Gomera
- 4019-4026
- Feb 20, 2025
- Psychology
Postpartum Depression: Risk Factors and Prevalence in Adolescent Girls and Young Women (AGYWs) in Gwanda, Zimbabwe
Honest Tshuma, Bhekisisa I. Madololo, Sheron Gomera
Great Zimbabwe University
DOI: https://dx.doi.org/10.47772/IJRISS.2025.9010311
Received: 12 January 2025; Accepted: 16 January 2025; Published: 20 February 2025
ABSTRACT
The study sought to assess risk factors and prevalence of postpartum depression in adolescent girls and young women in Gwanda. The research objectives included identifying the level of postpartum depression, outlining risk factors leading to postpartum depression, establishing ways of early detection of postpartum depression and assessing possible ways of reducing postpartum depression in adolescent girls and young women. Relevant literature to the study was reviewed, with relevant theories like the biological, psychosocial and evolutionary theories and conceptual framework on the hierarchical model of risk factors. The methodology for the study was a quantitative approach using the Edinburg Postnatal Depression Scale tool for screening for postpartum depression and questionnaires for responses. The researcher collected data from the postnatal mothers up to 8 weeks. From the major findings, it was discovered that the prevalence of postpartum depression of the selected group in Gwanda was 74%. It was noted that the possible risk factors of postpartum depression are lack of support from partner/husband, constant sickness of the baby and depression, stress and anxiety. In conclusion, there was lack of knowledge from the postnatal mothers concerning postpartum depression issues and lack of communication between hospitals and postnatal mothers on the issue. As part of recommendations, the researcher recommended screening of postpartum depression, awareness campaigns and counseling. Future researchers are recommended to broaden this research in Zimbabwean outskirts to attempt mitigating postpartum depression.
Key terms: Prevalence, Postpartum, Depression, Intervention,
AGYWs – Adolescent girls and young women
CMD – Common mental disorders
EPDS – Edinburgh Postnatal Depression
PND – Postnatal depression
PPD – Postpartum depression
INTRODUCTION
Postpartum depression is associated with mother-infant bonding impairment, child abuse, child neglect, maternal substance abuse, and self-harm [10]. Globally, the prevalence of depression in pregnant and postpartum adolescents varies. According to O’Hara et al (2014) postpartum depression has a prevalence range from 0.5 to 60.8%, affecting approximately 1 in 5 women globally, either during pregnancy and/or in the postnatal period. As a significant psychological disorder, although its risk can increase throughout the first 90 days, the postnatal period is mostly defined to be the first 6 weeks after delivery but depressive symptoms have been noted to extend even up to 16 weeks after delivery [13]. However, Alsayed et al. (2021), asserts that the risk may even last up to almost two years, thus creating a burden on society, with the greatest burden in lower and-middle-income countries compared to high-income countries, largely due to the limited accessibility to mental health professionals and resources, as well as factors such as social stigma and reduced societal awareness. In low and middle-income countries, the prevalence of PPD is higher than in developed countries and is estimated around 19.8% [4]. Narrowing down to Africa, the PPD seems to be the most prevalent psychological disorder with a prevalence of around 18%, showing how much Africa is struggling with such a mental issue. Although in urban Zimbabwe, high prevalence of PPD has been reported, the situation in rural settings is largely unknown [6]. This reflects how there is little research concerning PPD in Zimbabwe in general. However, reports state that within Zimbabwe, PPD ranged from 16.0% to 34.2% across different settings between 1995 and 2015, which indicates a research gap till to date [6]
Objectives
The specific objectives of the study were
- To identify the level of postpartum depression in AGYWs who are 24 years and below and have children who are not more than 8 weeks old.
- To outline the risk factors leading AGYWs who are 24 years and below and have children who are not more than 8 weeks old to postpartum depression.
- To establish ways of early detection of postpartum depression in AGYWs who are 24 years and below and have children who are not more than 8 weeks old.
- To assess possible ways of reducing postpartum depression in AGYWs who are 24 years and below and have children who are not more than 8 weeks old.
The hypotheses tests used was as follows:
H0: There is no association between marital status and depression
H1: There is an association between marital status and depression
Specifically for Table 4.6, the decision and conclusion were as follows;
Since the p-value is less than our chosen significance level (α=0.05), we reject the null hypothesis. We conclude there is enough evidence to suggest an association between marital status and depression (stress and anxiety): χ2 (1)=10.909.p=0.001.
Likewise, the same applied to all the other variables.
METHOD
Population
The population used was women in Gwanda who are of child bearing age, which according to zhuji world statistics is approximately 8208, with approximately 4611 in the childbearing age range [21].
Sample and sampling techniques
The target population for the study was 461 women who were of child bearing age receiving post-natal care at the hospital. The data size was determined through a good maximum size of 10% as recommended by tools4dev (2021). The calculations were done as follows
The study utilized purposive sampling as it dealt with a predefined population of 461 post-natal mothers up to 8 weeks from the age of 24 years and below receiving care at Gwanda hospital [10].
Data gathering instrument
Primary data was through two tools, the Edinburg Postnatal Depression Scale tool (EPDS) and a questionnaire.
The EPDS is a screening tool most widely used to screen for PPD [16]. On the other hand, the questionnaire collected information concerning demographic and general social background of participants, for secondary data, the researcher made use of the Neonatal department in Gwanda Hospital, for records of postnatal information.
Procedure
Permission to collect data was obtained from Gwanda hospital. Nurses at the hospital were responsible for the distribution of the questionnaire and any incomplete EPDS and questionnaires were disregarded. All participants were made to sign the consent forms before the administering of the questionnaires and EPDS indicating they understood and consented with the study.
The researcher made us of clinicians at the hospital who were administering the tests to the willing mothers during their post-natal visits to the hospital. The EPDS was used to test and screen for mothers with PPD in order to give statistics on PPD prevalence among Gwanda AGYWs. On the other hand, the questionnaire attached to the EPDS collected demographic information and possible risk factors that may be associated with PPD.
Design
For this study, the research framework used was cross-sectional design. As an observational study design, the researcher measured the outcome of PPD and the exposures in the study respondents at the same time [3] .This was useful in assessing prevalence of PPD in AGYWs in Gwanda, while understanding the exposure and the outcomes due to giving birth
Data analysis
The data collected in the study was analyzed using the Statistical package for social sciences (SPSS-21) to obtain descriptive statistics and make use of chi-square test. This assisted in statistical significance and to understand the relationship between prevalence of PPD and its risk factors.
FINDINGS OF THE STUDY
Findings
The questionnaire captured participants’ demographic data of note; age, marital status, level of education and employment status, mode of delivery, and number of children. These informed the risky factors which were; lack of support from husband and/or family, being abused emotionally 34or physically, having the baby constantl4y ill, and having a terminal illness as a mother. The response rate was 96%, which for researchers was sufficient. The target population was AGYWs (18-25 years). The majority were married, with ordinary level as their highest attained education, unemployed, had a normal delivery, and had 2 children.
Table I Participants’ Statistics on Number of Children and Delivery.
| Highest Education Level | Number of Children | Delivery mode | ||||||
| Level | Frequency | Percent (%) | Children | Frequency | Percent (%) | Mode | Frequency | Percent (%) |
| Primary | 52 | 11.8 | 1 | 299 | 67.6 | Normal | 390 | 88.2 |
| O’level | 325 | 73.5 | 2 | 104 | 23.5 | Operation | 39 | 8.8 |
| A’level | 13 | 2.9 | Missing | 39 | 8.8 | Missing | 13 | 2.9 |
| Tertiary | 39 | 8.8 | ||||||
| Missing | 13 | 2.9 | ||||||
Risk factors
The participants’ questionnaire, had six questions stemming from the risk factors to be assessed for prevalence of PPD.These included; support offered (from husband, family & friends), any kind of abuse faced, constant sickness of both the baby and mother as well as any signs of depression, anxiety, and stress. On receiving support from their partners, the marital and employment status statistics; 364(82.4%) married, and 65(14.7%) single. The other 2.9% did not indicate their marital status. The larger proportion 273(91%) of those who are married were unemployed but received support from their husbands, with slightly above half 78(55%) of the unemployed married ones not receiving support. On these two variables, the marital and employment status, the single mother participants receive support from their partners and the majority are unemployed, however, the bulk 61 (93.85%) of those single mothers that didn’t receive support from partner responded they did receive support from family and friends. The health of a baby can be stressful to postnatal mothers, especially first-time mothers as they don’t know what to do or to read the intensity of the pain the baby is having. From the responses, we can note that the majority 260(59%) did not have problems with their babies’ health. At times it’s not the baby that’s constantly not feeling well even the mother, whose body is still trying to recover from pregnancy and giving birth. This can also be a risk factor for PPD. However, in the study, the responses indicated that only 91(20.6%), had terminal sickness they suffered from.
EPDS Scores
Coupled with the questionnaire, was the EPDS, a PPD screening tool. The scale consists of 10 short questions and the total score of responses ranges from 0 to 30, with an outcome of at least 10 showing that one might be suffering from PPD. From Table 4.3, the EPDS scores ranged from 0 to 29, with an average score of 13.76 and the most frequent score being 14, meaning there is a high prevalence of PPD among the adolescent postnatal mother respondents. Moreover, the number of those who scored at least 10 is 325(74%), which is quite a lot, indicative of how most young postnatal mothers have PPD. The Chi-square test of independence was performed to assist in statistical significance and understanding of the relationships between the prevalence of PPD and associated risk factors. All the associated risk factors were tested and part of the results are presented in Fig 1, 2 & 3. The reason for showing part is that they all gave the same decision and conclusion.

Fig.1 EPDS Statistics
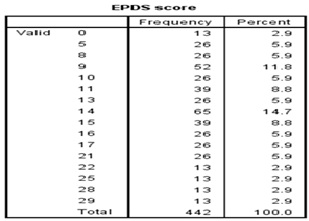
Fig.2 EPDS scores
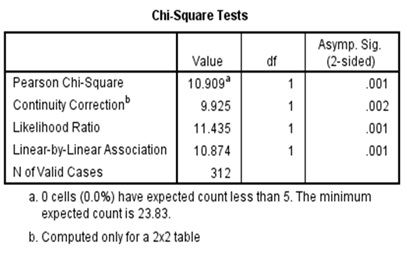
Fig.3 Sample of chi-square tests
The hypotheses tests used was as follows:
H0: There is no association between marital status and depression
H1: There is an association between marital status and depression
Specifically for Table 4.6, the decision and conclusion were as follows;
Since the p-value is less than our chosen significance level (α=0.05), we reject the null hypothesis. We conclude there is enough evidence to suggest an association between marital status and depression (stress and anxiety): ![]()
Likewise, the same applied to all the other variables.
During data collection, as the researchers were debriefing the participants about the study, they noted that postnatal mothers were not aware of PPD at all. There was little or no knowledge at all concerning the matter.
DISCUSSION, CONCLUSION & RECOMMENDATIONS
Discussion of findings
According to the findings of the study, firstly, the demographics suited the type of participants required, which were postnatal AGYWs in Gwanda. Most of the postnatal mothers had 1 child, delivered normally, with the highest education level attained being O’level, implying that they were literate enough to participate in the study. Many of the participants were unemployed, Wang. K., et al. (2020) [18] postulate that some demographics like occupation status, among others, indirectly affect postnatal mothers’ health. Support from a partner and/or family is a psychosocial and behavioral characteristic that affects the general living condition of the postnatal mother. This is similar to the findings of Xie, R.H, et al. (2010 [19], who indicated in their research that lack of support was an important risk factor for PPD, whilst Mbawa, et al. (2018) [9] said bad and negative relationships within families were found to be among the factors causing PPD. Given the study conducted by January, J., & Chimbari, M.J. (2018) [6] the issue of having a child with a birth weight under 2500g was among the prevalence of PPD, and baby underweight is normally associated with constant sickness. Abuse being in different forms like physical, emotional, or verbal was required as one of the responses from the participants. Results from Shamu, et al. (2016) [15] research, highlight issues of partner violence among women and discover it to be prevalence of PPD. During the lifespan of women, at periods like the hormonal changes of pregnancy and giving birth, the likelihood of depression, stress, and anxiety is high Rapkin, A. (2003). [14]. In this view, the participants had to indicate if they experienced such feelings. The question on signs or feelings of depression, stress, and anxiety indicated that almost half of the postnatal mother participants were experiencing those feelings. Normally, it is a result of environmental, psychological, or even physiological changes. According to the conceptual framework by Ahmad, N. et al., (2018) [1], all three levels of distal, intermediate, and proximal determinants within the hierarchical model of risk factors contribute to depression, stress, and anxiety. Thus, every possible risk factor has a chance of creating that feeling or experience. In agreement with this author like Halbreich, U. (2005) [5] also emphasize how much stress is a risk factor for depression after giving birth, especially when paired with other psychological social, and biological vulnerabilities. This relates to the research findings as can be noted from the responses that the stress and depression emanating from other paired psychological social and biological vulnerabilities like unemployment, lack of support, and sickness of either baby or mother.
The 74% results obtained indicated a high prevalence as compared to other studies done in Zimbabwe by researchers like [9], and [6] among others. This is a cause of concern and to worsen it having had random discussions with the AGYWs postnatal mothers, the researcher discovered that they had zero knowledge of the issues of PPD. Their worry was more about the baby’s health, with less concern for theirs. Thus, the mothers go for baby checkups and nothing more. The researcher also realized that at the hospital, there is no awareness of PPD and the medical staff does not screen or talk about it to the postnatal mothers during hospital visits. This also confirms the discovery of non-PPD screening in most Zimbabwean hospitals January, J., & Chimbari, M.J. (2018) [6].
Limitations of the study
The limitations of the study included the following;
5.2.1 The sample was limited to a single center, Gwanda Hospital, however, results may be applicable to other centers as well with similar characteristics.
5.2.2 The sample size with missing data might not give conclusive results, however, the missing data was catered for in the analysis.
Conclusions
According to the main findings, the prevalence of PPD in Gwanda among AGYWs is 74%, which is very high. In this research, the difference between other studies is that the EPDS screening was not selective of factors like Ahmad, N. et al., (2018) [1] who sought prevalence for different factors. Moreover, other researchers like Moya, E., Mzembe, G., Mwambinga, M. et al. (2023 [11] sought the prevalence of PPD in stages; from moderate to severe, with different cut-off EPDS scores, whereas this research sought the prevalence through mere screening for the possible PPD postnatal mother participants with any cutoff score.
Recommendations
Considering the research findings, the following recommendations could be implemented;
- Hospitals: Conduct PPD screening through the EDPS as early as the prenatal stage up to the postnatal stage, while being consistent throughout the whole process. Have awareness campaigns and programs in hospitals teaching pregnant women and postnatal mothers on issues of PPD. Creating counseling sessions for pregnant and postnatal mothers so that they get to talk to someone on issues that may be of concern for better health.
- The Community: Empowering the girl child on handy skills as a source of income, instead of waiting on employment. Teaching the community the importance of showering love, care, and support to postnatal mothers.
- The mothers: Assistance of mothers in fighting PPD through screening at hospitals and getting counseling and support after the discovery of PPD.
- Future researchers: To broaden the research to more rural areas and outskirts and assess the prevalence of PPD, to attempt to mitigate it.
REFERENCES
- Ahmad, N. et al., (2018). Postnatal depression and intimate partner violence: A nationwide clinic-based cross-sectional study In Malaysia. DOI: 10.1136/bmjopen-2017-020649.
- Alsayed, N.A., Altayyeb, J.F., Althuniyyan, L.S., Alzubaidi, S.K., & Farahat, F. (2021). Prevalence of postpartum depression and associated risk factors among women in Jeddah, Western Saudi Arabia. https://doi.org/10.7759%2Fcureus.14603.
- Dermatol, I.J. (2016). Methodology series module 3: Cross-sectional studies. May-Jun; 61(3): 261–264. doi: 10.4103/0019-5154.182410.
- Fisher, J., Mello, M. C. D., Patel, V., Rahman, A., Tran, T., Holton, S., & Holmes, W. (2012). Prevalence and determinants of common perinatal mental disorders in women in low-and lower-middle-income countries: a systematic review. Bulletin of the World Health Organization, 90, 139-149.
- Halbreich, U. (2005). The association between pregnancy processes, preterm delivery, low birth weight, and postpartum depressions—the need for interdisciplinary integration. American journal of obstetrics and gynaecology, 193(4), 1312-1322.
- January, J., & Chimbari, M.J. (2018). Prevalence and factors associated with postnatal depression among women in two rural districts of Manicaland, Zimbabwe. S Afr J Psychiat. 2018;24(0), a1176. https://doi.org/10.4102/sajpsychiatry.v24i0.1176.
- January, J., Burns, J., & Chimbari, M. (2017). Primary care screening and risk factors for postnatal depression in Zimbabwe: A scoping review of literature. J Psychol Afr. 2017; 27(3):294-298. https://doi.org/10.1080/14330237.2017.1321866.
- January, J., Chivanhu, H., Chiwara, J., Denga, T., Dera, K., Dube, T., Chikwasha, V., & Chikwanha, T. M. (2015). Prevalence and the correlates of postnatal depression in an urban high-density suburb of Harare. The central African Journal of medicine. Vol. 61, Nos. 1/4.
- Mbawa, M., Vidmar, J., Chingwaru, C., & Chingwaru, W. (2018). Understanding postpartum depression in adolescent mothers in Mashonaland Central and Bulawayo Provinces of Zimbabwe. Asian journal of psychiatry. Volume 32. https://doi.org/10.1016/j.ajp.2017.11.013.
- McCombs, S. (2019). Sampling methods | Types, techniques & examples. Retrieved from https://www.scribbr.com/methodology/sampling-methods/.
- Moya, E., Mzembe, G., Mwambinga, M. et al. (2023). Prevalence of early postpartum depression and associated risk factors among selected women in southern Malawi: a nested observational study. BMC Pregnancy Childbirth 23, 229. https://doi.org/10.1186/s12884-023-05501-z.
- Naidoo, S., & Taylor, M. (2020). Antenatal and postpartum depression: Prevalence and associated risk factors among adolescents’ in Kwazulu-Natal, South Africa. Depression Research and Treatment. Volume 2020. https://doi.org/10.1155/2020/5364521.
- O’Hara, M.W., Wisner, K. L., Asher N, et al. (2014). Perinatal mental illness: Definition, description and etiology. Best Pract Res Clin Obstet Gynaecol. 2014;28(1):3–12. https://doi.org/10.1016/j.bpobgyn.2013.09.002.
- Rapkin, A. (2003). A review of treatment of premenstrual syndrome & premenstrual dysphoric disorder. Psych neuroendocrinology, 28, 39-53.
- Shamu, S., Zarowsky, C., Roelens, K., Temmerman, M., & Abrahams, N. (2016). High-frequency intimate partner violence during pregnancy, postnatal depression and suicidal tendencies in Harare, Zimbabwe. General hospital psychiatry, 38, 109-114.
- Tsai, A. C., Scott, J. A., Hung, K. J., Zhu, J. Q., Matthews, L. T., Psaros, C., & Tomlinson, M. (2013). Reliability and validity of instruments for assessing perinatal depression in African settings: systematic review and meta-analysis. PloS one, 8(12), e82521.
- Tools4dev (2021). How to choose sample size. https://tools4dev.org/resources/how-to-choose-a-sample-size/
- Wang. K., et al. (2020). Proximal social determinants of adolescents’ health: The importance of everydaylife circumstances. Sage journals. Volume 53, Issue 6. https://doi.org/10.1177/0044118X20918436.
- Xie, R.H, Yang J, Liao S, et al. (2010). Prenatal family support, postnatal family support and postpartum depression. Aust N Z J Obstet Gynaecol 2010; 50:340–5.
- Yim, I.S., Stapleton, L.T., Guardino, C.M., Hahn-Holbrook, J., & Schetter, C. D. (2015). Biological and psychosocial predictors of postpartum depression: Systematic review and call for integration. Annual review of clinical psychology. Vol. 11:99-137 https://doi.org/10.1146/annurev-clinpsy-101414-020426.
- Zhujiworld (2021). Gwanda, Zimbabwe-statistics https://zhujiworld.com/zw/496855-gwanda/