
Reducing Supply Chain Management Risks in the Health Sector of Ghana: An Evaluation of the Central Level Supply Chain Management System of The Ghana Health Service
- Domie, Godswill.
- Gawu, Paul Senyo.
- Dodzi, Samuel
- 560-587
- May 7, 2024
- Business Management
Reducing Supply Chain Management Risks in the Health Sector of Ghana: An Evaluation of the Central Level Supply Chain Management System of The Ghana Health Service
Domie, Godswill.1, Gawu, Paul Senyo.1, Dodzi, Samuel.2
1PhD Student. Graduate School of Business Management, Philippine Christian University, Manila- Philippines.
2Supply Chain Practitioner. Ghana Health Service (GHS), Supply, Stores, & Drug Management (SSDM), Accra Ghana.
DOI: https://dx.doi.org/10.47772/IJRISS.2024.804044
Received: 14 March 2024; Revised: 23 March 2024; Accepted: 26 March 2024; Published: 02 May 2024
ABSTRACT
Supply Chain Management plays an indispensable role in any organization’s overall performance and success. The domain of Supply Chain Management has been of great research interest in recent years. In the ever-growing healthcare world, where most healthcare organizations are confronted with diverse SCM risks and growing customer demand trends, effective and efficient SCM has been identified as a tool to help them overcome this challenge. However, the main hurdle had been how to find innovative approaches to meet customer demands that will minimize operational costs. To address these concerns and deliver effective and efficient healthcare, the Government of Ghana represented by the Ministry of Health (MOH) and Ghana Health Service (GHS) in partnership with the Global Fund, GAVI, and the World Bank have deployed several interventions fundamentally founded on procurement and supply chain management to improve healthcare service delivery across the country. The interventions: Health commodity supply chain master plan (HCSCMP), the Last Mile Distribution (LMD), and the Ghana Integrated Logistics Management Information System (GhiLMIS), focus mainly on procurement, inventory, warehousing, and transportation of medical and non-medical products. The success and sustenance of these collaborative interventions in Supply Chain management within the health sector in Ghana hinges on key elements such as putting in place stringent procurement policies, ensuring availability of qualified personnel, transportation facilities to aid effective and efficient distribution, and paying attention to risk management practices. This study sought to examine the supply chain risk management practices at the central level of GHS and its regional and districts medical stores to identify the challenges of the existing SCM system and propose measures of addressing these challenges. The scope of the study was limited to the Ghana Health Service Supply Chain Practitioners (GHSSCP) at the central level and their collaborators at the regional levels (the Regional Health Directorates). Quantitative method was used in the study and the main research instrument used for the study was questionnaire administration. However, the study used convenience and purposive sampling techniques due to the sensitive nature of the subject matter. The target respondents were mainly Supply Chain Practitioners: supplies managers, procurement officers, general stores and pharmacy stores officers. The study relied on SPSS and used descriptive and inferential statistics to analyze data. The study found that notwithstanding the introduction of key interventions such as health commodity supply chain master plan (HCSCMP), the Last Mile Distribution (LMD) of health commodities from the Central level to Regional medical stores and to health facilities (Hospitals and the District Health Directorates), and the introduction of the Ghana Integrated Logistics Management Information System (GhiLMIS) as a technology tool for health commodity management at all levels across the public health sector SCM system which collective objective is to ensure the effectiveness and efficiency of the system through the minimization of SCM risks, interruptions, and vulnerabilities, there still exist a yawning underperforming gap due to the systems overly centralization and lack of priority for SCM risk reduction measures making the system still not performing at its full potential. The study concluded that there are basic weaknesses in almost all the supply chain dimensions covered: risk identification, risk assessment and mitigation, Supply Chain Risk Management Governance, impact of supply chain risk management, and employee supply chain risk routine activities because the much-needed attention is not given to SCM activities. The study recommended reforms including the establishment of a Supply Chain Risk Management Unit (SCRMU) at all levels (national, regional, and districts) under the direct supervision of Health Administration and Support services (HASS), the introduction of SCM performance contracts, and the implementation of a stronger but user-friendly technology driven SCM system including e-procurement, warehouse management tracking, supported by a robust feedback system to ensure risk free SCM
Keywords: Ghana, Supply chain Management, procurement, inventory, warehousing, transportation, Last Mile Distribution (LMD), Ghana Integrated Logistics Management Information System (GhiLMIS)
INTRODUCTION AND BACKGROUND
Supply Chain Management (SCM) in organizations has gained enormous attention in recent times due to the fact that it is considered one of the key lubricants of organizational operational excellence (Habib, Md. M. et al, 2022). Evidence suggest that healthcare organizations in most developing nations are confronted with numerous supply chain management challenges such as frustration of customers, unsuitable costs of health service, lack of service providers, medical implements, and modern technology (Al-Saa’da et al., 2022), compelling these nations to develop robust and resilient supply chain management systems to lessen the challenges and offer better service to society (Pervez et al., 2016). According to Lauer (2004), Supply Chain Management in Healthcare involves is the consistent movement of healthcare products (medical and non-medical) by stakeholders. Lauer maintained that the products must be delivered at the right time in the right quantities to preserve limited resources and minimize waste to meet the needs of healthcare providers and customers, as well as reducing waste and conserving resource. Schneller and Smeltzer (2006) explained that generally, supply chain management in most healthcare sectors has been largely disjointed and relatively unproductive. Schneller and Smeltzer (2006) noted that the independent functionality of elements within the healthcare supply chain management systems often produce contradictory objective and goals with skewed motivations which always inhibits the efficient and effective functionality of most healthcare supply chain management systems. Schneller and Smeltzer (2006) suggested a proper amalgamation of all components of the supply chain: government, healthcare agencies, manufacturers or producers, purchasers, providers, financial intermediaries and payers (banks) for an efficient execution of SCM policies, strategies, and practices. Aqlan et al. (2016) stated that Supply chain risk is a latent interruption of a supply chain system that affect its effectiveness and efficiency. They also maintained that Supply chain risk management (SCRM) involves a methodical approach of identifying, assessing, grading, and closely monitoring potential disruptions in supply chains so as to reduce them. Gurtu et al. (2021) also noted that Supply chain risk management involves the processes of implementing policies and plans targeted at continuous risk assessment to minimize shocks and vulnerabilities within supply chain networks to ensure supply chain resilience. Numerous Problems of Health Sector Supply Chain Management in Ghana had been documented ranging from lack of proper coordination, insufficient staff, lack of storage space especially at the regional and district levels, lack of transport for health commodity supplies, and lack of reliable data to support SCM activities (Atiga, O. et al., 2023). Osei-Assibey and Akweongo (2017) and Anvuur, A. et al. (2006) also mentioned insufficient procurement planning, wasteful expenditures, lack of capacity to pay suppliers, funding inadequacies, general low supplier delivery problems, and lack of qualified procurement staff as challenges of health sector SCM. Across the HSSCM system, there is a high speculation of very low attention to supply chain risks and their mitigation. Over the years, several efforts had been to address these challenges. Key among them include the introduction of Supply chain master plan (SCMP), Last Mile Distribution (LMD) of health commodities from the Central level to Regional medical stores and to health facilities in the Districts, and the introduction of the Ghana Integrated Logistics Management Information System (GhiLMIS) for health commodity management at all levels across the public health sector SCM system (MOH 2022; Atiga et al., 2023). Although the introduction and implementation of these health sector SCM interventions have yielded some positive results, there are still some inconsistencies making the SCM system in the public health sector in Ghana not realizing its full potentials. The continuous existence of challenges amid the introduction and implementation of these interventions constitute a great risk within the SCM system of health commodities and it is time research is conducted to assess the situation and proffer solutions. This study therefore seeks to examine the service delivery aspect of supply chain risk management practices at the central level of GHS to identify risks associated with the system in the midst of the introduction of Supply chain master plan (SCMP), Last Mile Distribution (LMD) of health commodities from the Central level to Regional medical stores and to health facilities in the Districts, and the introduction of the Ghana Integrated Logistics Management Information System (GhiLMIS) for health commodity management at all levels across the public health sector SCM system. The output of the study is expected to assist stakeholders of the health sector SCM system to improve its effectiveness and efficiency.
LITERATURE REVIEW
2.1 Concept of Supply Chain Management
The term “supply chain management” (SCM) was first introduced by Keith Oliver in 1982 who defined SCM as the process of planning, implementing, and controlling the operations of the supply chain with the movement and storage of raw materials, work-in-process inventory, and finished goods from point-of-origin to point-of-consumption purposely to satisfy customer requirements as efficiently as possible (Robert B. et al., 1999). In the mid-1990s, Mentzer, et al. (2001) popularized the term SCM by admitting that it was proper that the final consumer was included the early definition and added information flow and considered SCM as the interplay of supply chain activities through enhanced supply chain relationships to achieve a competitive advantage. To avoid the misconception in the domain of SCM, La Londe and Masters (1994) explained that supply chain management is different from ‘supply chain’ which is a collection of businesses who traffic materials, or a group of organizations, directly connected by one or more upstream and downstream flows of products, services, finances, or information from a source to a customer. La Londe and Masters maintained that supply chain management is the management of such a chain and that the chain must exist before it can be managed. Mentzer et al (2001) also make an additional distinction: supply chain management and supply chain orientation. According to them, supply chain orientation includes an acknowledgement that organizational strategy can only be achieved when upstream and downstream activities of customers are properly managed, while supply chain management involves the real execution of supply chain orientation.
Aside from these conceptualizations of SCM, there are other generally acknowledged views of supply chain management. Nabil Abu el Ata and Rudolf Schmandt (2016) considered it as the management of upstream and downstream value-added flows of materials, final goods, and related information among suppliers, company, resellers, and final consumers. Mentzer, et al. (2001) said SCM is the systematic, strategic coordination of traditional business functions and tactics across all business functions within a particular company and across businesses within the supply chain, for the purposes of improving the long-term performance of the individual companies and the supply chain as a whole. Cooper et al (1997) defined SCM as the combination of key business processes across the supply chain for the purpose of creating value for customers and stakeholders. According to Kozlenkova et al (2015), the Council of Supply Chain Management Professionals (CSCMP) defines supply chain management as comprising the planning and management of all activities involved in sourcing, procurement, transformation, and logistics management which must include the harmonization and partnership with channel partners: suppliers, intermediaries, third-party service providers, and customers or consumers. Tang (2006) also define supply chain management as “the management of material, information and financial flows through a network of organizations (i.e., suppliers, manufacturers, logistics providers, wholesalers/distributors, retailers) that aims to produce and deliver products or services for the consumers”. Perhaps the most customer-focused definition of SCM is the one provided by Hines (2004: p.76) which state inter alia that supply chain management require a total system view of the links in the chain to ensure that they work together resourcefully to create customer satisfaction at the end point of delivery to the consumer. Hines further stated that such activities should be targeted at cost reduction through the elimination of unnecessary expenses associated with commodity movements and handling. Thus, the import of Hines conceptualization of SCM is to enhance effectiveness and efficiency through the removal of all bottlenecks to ensure customer or consumer value addition.
2.2 Theories Underpinning Supply Chain Management
Lavassani and Movahed (2010) identified some theories that laid the foundation of modern-day supply chain management. These are the Resource-based view Theory (RBV), the Stakeholder Theory (ST the Institutional Theory (IT), the Transaction cost theory (TCT), Network Theory, and the Resource dependence theory (RDT). Lavassani and Movahed admitted that these theoretical perspectives offered and explain and laid the foundation for various aspects of SCM. Shantanu Trivedi (2023) and Lavassani and Movahed (2010) all explained that the RBV theory focuses on the extent to which an organizations exceptional resources and capabilities can help them achieve competitive advantage in the supply chain. Shantanu Trivedi maintained that by optimally using resources firms can attain higher performance to differentiate themselves their competitors. Shantanu Trivedi stated that the concept of resource-based view forms the basis for firm’s agility, adaptability, and alignment regarding SCM. Another theory identified as shaping SCM is the Stakeholder Theory. This theory according to Shantanu Trivedi (2023) and Lavassani and Movahed (2010), is a model of organizational management and business ethics that deals with morals and values in managing an organization and enjoins organizations to critically premium the interests of all their stakeholders. They maintained that the stakeholder theory can be used to explain how firms can develop working relationships with their suppliers and customers to improve their supply chains. Shantanu Trivedi (2023) and Lavassani and Movahed (2010) further talked about institutional theory where firms within a particular industry are predisposed by the institutions in that environment which forms the basis of how individual firms adopt and adapt certain supply chain practices within their industry because they are norms in the industry or because they are legal requirements. Citing Ronald Coase (1937), Shantanu Trivedi (2023) maintained that transaction cost theory deals with cost considerations of doing business and explains why businesses chose to either internally manage or outsource their supply chain operations. Shantanu Trivedi (2023) also supported the Network theory of Bower (1981) and maintained that it is a concept that explains relationships and interactions between various entities within a supply chain as well as helping them to appreciate and understand how information flows, collaborations and partnerships among various players can shape the inclusive efficiency and pliability of the supply chain system as a whole. Shantanu Trivedi (2023) and Lavassani and Movahed (2010) pointed to the Resource Dependency Theory and stated that due to its ability to assist companies overcome their resource limitations, it has become the cornerstone for explaining why organizations depend on one another for resources and why it is important for companies to manage their relationships with their supply chain partners. Explaining the relevance of the systems theory to SCM, Shantanu Trivedi (2023) and Lavassani and Movahed (2010), posited that the systems theory brings together numerous components of a complex supply chain: human, capital, information, materials and financial resources, etc.) together to form a subsystem which is then part of a larger system of supply chains or networks. While we agree with the authors on these theories and their role in shaping supply chain, we are convinced that there is no all-embracing theory to chaperon supply chain management activities and that the choice of an ideal theory to use will and should be based on the specific context and situation.
2.3 Supply Chain (SC) Models
Anvyl (2022) enumerated six contemporary supply chain models that businesses can use to manage their SCM systems: The Continuous Flow SC Model, Agile SC Model, Fast Chain SC Model, Efficient Chain SC Model, Flexible SC Model, and Custom-Configured SC Model. According to Anvyl (2022), the Continuous Flow SC Model is applicable to businesses and that need to deliver stable and uninterrupted flow of products and resources to customers. Such companies the author noted should have strong supply chain networks and minimal variation between their purchase orders. Examples include beverage and pharmaceutical companies. Anvyl (2022) maintained that the agile SC model requires business to have four fundamental structures: virtual integration, process alignment, market sensitivity, and a network base. The presence of these fundamentals will deliver a combine effect that help companied to easily identify potential demand trends for the products and make or supply customized products that fit into the current market demand and customer trends. This is mostly the case of textiles and clothing industries. Some companies deal in products with short lifespans such as sports wears and seasonal products like Christmas toys etc. Anvyl (2022) noted that the Fast Chain SC Model is what is recommended for such companies, since it helps them to quickly vary their products types and do fast deliveries to the market before the product loses its relevance. Anvyl (2022) advocated the Efficient Supply Chain Model to businesses that have highly competitive markets seeking to be highly efficient within their supply chain environments. According to Anvyl, the efficient SC model lay emphasis on prudent inventory management and delivery of goods ensuring that all equipment and machines optimally operate to deliver goods without any unnecessary waste. Anvyl underscored that the flexible SC model is a type of supply chain model that accommodates peaks and dips in customer demand over time. Anvyl noted that to operate effectively and efficiently, supply chain systems should have segmentation, accurate stocking algorithms, and flexible planning. The model advocates for the establishment of depots and warehouses for commodity storage that would serve as shock absorber. For example, during low demands, commodities can be preserved and supplied when there are hikes or increased demand. In the opinion of Anvyl (2022), the custom-configured model, is a mixture of the agile and the continuous flow models. This model is good where firms are dealing with multiple product configurations during the production or assembly of different goods within the factory. It is also good for customers to get their products faster while permitting them to modify the product as needed.
2.4 Risk management
The International Organisation for Standardization (ISO) (ISO 31000:2009) defines risk management as a coordinated set of activities and methods that is used to direct an organization and to control the many risk that can affect its ability to achieve objectives (Purdy, G., 2010). Cheng et al. (2012) also considered risk management as the process where decisions are made to accept a known or assessed risk and the implementation of actions to reduce the effect or the probability of occurrence of an adverse event. Risk management was defined by Alhawari et al. (2012) as the implementation of strategies, methods, and the use of supporting tools to identify and control risk to an acceptable level. Fekete (2012a, 2021b) avers that risk management is a systematic process of identifying, evaluating, and addressing potential and actual risk. Thus, risk management is the process of first, accepting that business operations comes with uncertainties otherwise known as risks, and second, identifying the risks associated with the business operations, and third, implementing policies, strategies, plans, and procedures to reduce the risks to ensure effectiveness, efficiency, and value addition.
2.5 Supply Chain Risk management
Tang (2006) defines Supply Chain Risk Management (SCRM) as “the management of supply chain risks through coordination or collaboration among the supply chain partners so as to ensure profitability and continuity”. Sun J. et al (2012) considered SCRM as a structured and synergetic process throughout the supply chain, which seeks to optimize the totality of strategies, processes, human resources, technology and knowledge. Tang (2006) identified two dimensions of supply chain management risks: operational and disruption risks. According to Tang, operational supply chain management risks include integral uncertainties like indeterminate customer demands, supply, and cost, while disruption supply chain management risks arise from major interruptions occasioned by natural and man-made disasters like earthquakes, floods, hurricanes, terrorist attacks, fire outbreaks, or economic crises such as currency evaluations, fluctuations, or strikes. Sun J. et al (2012) maintained that the process of risk mitigation is achieved through collaboration, co-ordination and application of risk management tools among the partners, to ensure continuity coupled with long term profitability of the supply chain. According to Harland et al (2003), there are nine classifications of SCMR, and these include Operations risks which affects a firm’s internal ability to produce and supply goods/services, Supply risks, which results in the unlikelihood of customer placing orders, Asset Impairment risks which reduces the utilization of an asset and can arise when the ability of the asset to generate income is reduced, and Competitive risks which result from an organizations inability to differentiate its products/services from its competitors. Others are Reputation risks which erode the value of the entire business due to loss of confidence, Financial risks which come out of a firms poor financial position and debt defaults and expose the firm to potential losses through changes in financial markets, Fiscal risks which come mainly from internal government policies such as taxation, Regulatory risks, situations that expose the firm with changes in regulations affecting the its business such as environmental regulation, and Legal risks coming from law suits against the business from customers, suppliers, shareholders or employees. We therefore proposed the following definition of Supply Chain Risk Management (SCRM): SCRM is a structured and synergic process which seeks to optimize the totality of strategies, processes, human resources, technology and knowledge throughout the supply chain system, with the aim to control, monitor and evaluate supply chain risk through coordination, collaboration, and cooperation to safeguard continuity and maximize profitability. Tang (2006) suggested four rudimentary procedures businesses can use through coordination and collaboration to mitigate supply chain management risks: supply management, demand management, product management, and information management. The diagram below adapted from Tang (2006) illustrates the processes of SCRM
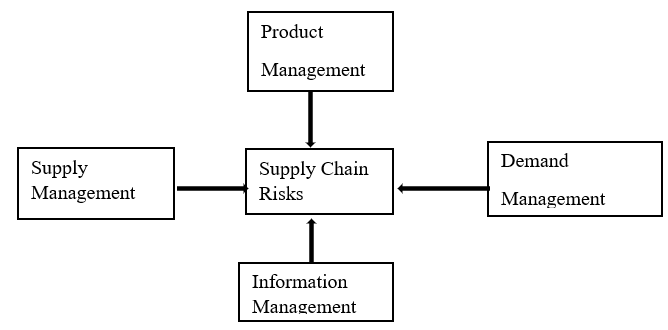
Figure 1. Four Basic Approaches for Managing Supply Chain Risks: Adopted from Tang (2006)
Tang (2006) explained that to effectively reduce SCR and enhance supply chain processes, businesses should first harmonize or cooperate with upstream partners to achieve efficiency in the supply of materials through the supply chain. Tang further advocated for firms to partner with downstream associates to impact demand in an advantageous way. He also advice firms to adjust their product or process designs to assist them meet customer demand. Tang called for effective and efficient information management within partners within supply chain management networks to advance their coordinated or efforts and better decision making. Based on the analysis of SCRM, we posit that SCMR can be mitigated if businesses implement their strategies, policies, and plans using the 3Cs: Collaboration, Cooperation, and Coordination
2.6 Public Sector Healthcare Procurement and Supply Chain System in Ghana
Public procurement in Ghana is regulated by the Public Procurement law, Act 663 of 2003, as amended, Act 914 of 2016, which also provides the framework for the health supply chain (Boakye., et al., 2021). In the public health sector of Ghana, health commodities are managed by a three-tier system: Central Medical Store (CMS), Regional Medical Stores (RMSs), and Service Delivery Points (SDPs) (USAID, 2009) and the Ministry of Health coordinates all public health sector procurement with the Ghana Health Service overseeing and administering the operations (service delivery aspect) of the supply chain system (Manso, et al., 2013). Central Medical Store is managed by the Ministry of Health while each regional medical store is managed by their individual Regional Health Directorates (RHDs) (Bossert., et al., 2014). Boakye., et al. (2021) noted that in exceptional instances, teaching and regional hospital after applying to the MOH are granted permission to directly procure from the CMS and also develop, arrange, and implement their own supply chains by independently dealing with private vendors. Following the review of the 2015 to 2020 Health Commodity Supply Chain Master Plan (HCSCMP) by the Ministry of Health in 2020 and the launch of the 2021 to 2025 version of the plan, the central level is responsible for the procurement and distribution of medical products to the region and facilities. However, Regional Health Directorates and facilities are allowed to stock three months medical products that falls outside the products distributed centrally based on Entity’s thresholds (MOH, 2022). From the afore discussions on Public Sector Healthcare Procurement and Supply Chain System in Ghana, we posit that the system revolves primarily around the Central Medical Stores acting as the Central unit of procurement and Supply Chain Management for the Ghana Health Services and other sister agencies and this overly centralization of supply and procurement activities at the central level can have some serious operational challenges for the performance health facilities.
2.7 Challenges and Weaknesses of SCM in the Health Sector
There is every reason to argue that apparently, there are weaknesses within the health sector supply chain system in Ghana that predispose or put procurement and supply chain management activities within the sector at risk and Adu-Poku et al (2011) referred to these risks as the vulnerability of supply chain. Laysons and Farrington (2006) also admitted that health sector procurement and supply chain is susceptible to a lot of risks due to some internal and external forces. Laysons and Farrington posited that the internal factors are frequently attributable to interactions between organizations in the supply chain due to growing complexity of supply networks while the external risks are connected to environmental, economic, and political and social causes, such as storms, earthquakes, terrorism, strikes, wars, fire outbreaks, embargoes, and computer viruses. According to Adu-Poku et al (2011), the weaknesses within the supply chain is due to five main factors: delays, disruptions, price increases, operations, and legislation and pointed out that ranking these factors against the occurrence, controls, and impact will help organizations identify the factors that mostly ignite the vulnerabilities. The authors further explained that delays in the supply chain have a direct impact on performance and cost and that supply chain disruptions are major source of risk and include unplanned and unanticipated events that disrupt the normal flow of goods, information and materials within a supply chain, and, as a consequence, expose firms within the supply chain to some degree of risk. It was also their case that disruption within the supply chain could also manifest in the form of erratic flow and availability of raw materials, poor transportation, poor disaster recovery, and lack of knowledge regarding the source of supply, rationalization of product ranges and inability to control theft. Adu-Poku et al suggested that organizations should keep a ‘risk register’ for keeping track of all supply chain risks so as to manage them effectively. The Public Procurement Authority reported in 2018 that inadequate procurement planning, delayed payments to suppliers, inconsistent commodity delivery especially to remote areas due to lack of adequate transportation, unnecessary interferences, and poor inventory management and control are the key challenges and weaknesses confronting the health sector supply chain management in Ghana (PPA, 2018).
2.7.1 Categorization of Challenges of SCM in the Health Sector
For better clarification and ease of comprehension, we summarize health sector SCM challenges into two main categories: internal and external, as shown in the following table
| Internal forces/ Challenges of HCSCM | Manifestations | External forces/ Challenges of HCSCM | Manifestations |
| Management and Leadership | Delays in operations
Poor rationalization of product ranges Inability to control theft Inadequate procurement planning Delayed in payments to suppliers Inconsistent commodity delivery Unnecessary interferences in SCM operations Poor inventory management and control |
Environmental | Storms, earthquakes, terrorism, fire outbreaks
Poor disaster recovery |
| Poor Stakeholder Management | Lack of knowledge regarding the source of supply
Erratic flow and availability of raw materials Poor transportation Legal battles |
Economic
|
Inability to control Price increases
Operational difficulties due to computer viruses |
| Political | Embargoes, legislations, Operational guidelines | ||
| Social | Strikes, industrial actions |
Figure 2: Categorization of Challenges of SCM in the Health Sector (Domie, Gawu, Dodzi, 2024)
2.8 Supply Chain Risk Mitigation (SCRM)
Several literatures abound to prove the fact that supply chain interruptions and vulnerabilities and their consequential glitches can have severe debilitating impacts on all supply chain systems and their overall performance (Chopra & Sodhi, 2004; Norrman & Jansson, 2004; Pettit., et al. 2013; Tang & Tomlin, 2008). To mitigate the impact of supply chain risk management, information sharing between stakeholders of supply chain systems had been identified asa viable tool for understanding the various SCM risks which could adversely impact on the supply chain systems (Faisal, et al., 2006), meanwhile, organizations ability to harness information to tackle SCRM has seen very little attention in literature (Fan, et al., 2016). As Fan, et al. (2017) and Zweig, et al. (2015) noted, an organization or any supply chain management system which processes SC risk (SCR) information stand a better chance to recognize, analyze and evaluate negative patterns to effectively and efficiently manage SC risks holistically and respond in a very timely manner. Supply Chain Risk Management is considered as a developing essential and multi-functional domain between Supply Chain Management (SCM), corporate strategic management and Enterprise Risk Management (ERM) (Hillman & Keltz, 2007; Zsidisin & Ritchie, 2009a, 2009b). However, Ho, et al. (2015) argued that suggested definitions of SCRM in the literature are not holistic and are only typically skewed towards some selected components of SCRM which failed to extend the SCRM processes completely or vary in their SCRM approaches and types of events. Agreeing with Ho, et al., Schlüter et al (2017) also define SCRM as: “an inter-organizational collaborative endeavor utilizing quantitative and qualitative risk management methodologies to identify, evaluate, mitigate and monitor unexpected macro and micro level events or conditions, which might adversely impact any part of a supply chain”. From the analysis, we considered Supply Chain Risk Mitigation as the process where organized efforts are initiated to identify, assess, mitigate, reduce disruptions and vulnerabilities within a supply chain system to create value for stakeholders, and in the context of healthcare supply chain management to create value for patients, visitors, staff and organizational assets as a whole. Digitalizing SCM processes had been identified as a mechanism that can aid in a faster management of supply chain risks. Relying on the works of Norrman and Lindroth (2004), Schlüter et al (2017) called the process of digitalizing SCM processes for faster supply chain risk reduction, Smart Supply Chain Risk Mitigation or “SCRM digitalization” and define it as “the integration of technology (sensors, actors, connectivity, analytics) along supply chain processes to improve supply chain risk identification, analysis, assessment, mitigation and monitoring through processing real time supply chain risk information – which comprises supply chain risk information sharing and analysis”.
2.8.1 Impact of Poor Supply Chain Risk Management on business operations
The object of any supply chain risk management is basically to recognize and examine the risks associated with SCM processes in supply chain networks, map out and implement strategies to mitigate the identified SCM vulnerabilities (Ganiyu, et. al., 2020). Wagner and Neshat (2012) admitted that poor supply chain risk management poses operational challenges to organizations including triggering losses of both short-term revenue and long-term profitability and market shares. There are several instances where organizations are on record to have suffered substantial losses due to their risk negligence or risk hostility. For example, a Bangladeshi multinational organization: Rana Plaza building, recorded huge losses following a collapse of their buildings (Koenig & Poncet, 2019). Pettit et al. (2013) noted that due to inappropriate handling of a natural disaster (earthquake), Toyota’s total production dipped by 40,000 automobiles in 2011, while uncontrolled floods in Thailand resulted in computer and automobile manufacturer’s incurring unimaginable loses (Chopra & Sodhi, 2014). Potentials for fire outbreaks and poor attention to such possibilities has also been identified as one of the key supply chain risks that when ignored can result in fatal losses. In Ghana for example fire had consumed the entire Central Medical Stores, the principal stores in 2015 and destroyed medicines and non-medical consumables valued at over GH₵237million beyond salvage (Owusu-Sekyere et al., 2017), a situation largely blamed on poor or total non-adherence to supply chain risk management principles and practices making it easy for suspected arsonists to set the national warehouse ablaze to cover up for huge an accounted for logistics. Pundits say the state or managers of the warehouse were grossly risk averse else they would have foreseen the danger and prevent its occurrence. Sadly, the huge investment made was also not insured against fire, theft or arson making Ghana lost all what was there (Joy FM, 2015).
2.9 Case studies of supply chain in healthcare
Several case studies have been conducted into supply chain management within healthcare settings. We present highlights of two of the recent case studies to throw more insight into supply chain management in healthcare. A study conducted by Asamoah et al. (2023) on Supply chain visibility in Kumasi Metro Health Directorate in Ghana found that technology limitations, absence of collaborations between computerized and physical operations, discrepancies in data among key supply chain stakeholders, poor reverse communication, haphazard planning, and budget constrictions are the bane of ineffective supply chain management and recommended that to ensure a robust and resilience SCM system these bottlenecks must be addressed.
Domie and Dodzi (2023) in their study of Medicine Procurement Framework for Public Hospitals in the Western Region under the Ministry of Health in Ghana found that the supply chain systems for medicines to hospitals was challenged by centralization and non-involvement of stakeholders at the lower levels of the chain. The study noted that, due to the disconnect between key stakeholders, the had been serious SCM disruptions resulting in prolong shortages of essential medicines. The study further noted that challenges facing the medicine supply chain within the Ghanaian health sector were mainly from three domains. First, from policy dimension which includes non-transparent contract and selection process of Suppliers, poor tracking of commodity (Medicines) Delivery process, lack of access to framework policy, suppliers and supplier contract management process by lower level stakeholders. Second, lack of proper coordination between Regional Medical Stores and suppliers resulting in non -response to call offs by suppliers, low supplier delivery capacity (SDC), delay in meeting delivery timelines, delivery of substandard medicines, general non -adherence to specified packaging standards, and transportation difficulties in the SCM process. Third, lack of proper monitoring and supervision of SCM stakeholders which also culminated into inadequate supply of medicines from RMSs to service delivery points (SDPs), supply of near expiry or completely expired medicines from suppliers and RMSs, inadequate stock of medicines at facilities, and to a large extent corruption secondary to moral hazards. The study recommended the need for a wider and a more comprehensive stakeholder engagement and decentralization of the SCM process to ensure effective and efficient SCM system within the health sector
2.10 Conceptual Frameworks: Health Supply Chain Management and Health Supply Chain Risk Management
2.10.1 Conceptual Frameworks for Health Supply Chain Management (HSCM)
The study adopted the Kwon and Kin (2018) Supply Chain Implementation Conceptual Framework with. Figure 2 below illustrates the adopted Kwon and Kin (2018) framework.
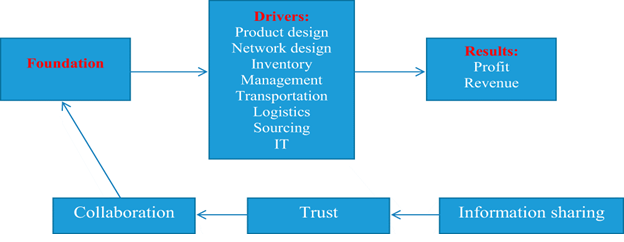
Figure 3: Original Conceptual Framework for SCM Implementation. Kwon and Kim (2018)
In their conceptual framework for SCM implementation, Kwon and Kim (2018) argued that supply chain processes from start to finish rest on three main building blocks of processes or goals: foundation, drivers and outcomes. According to kwon and Kin, outcomes from supply chain implementation is contingent upon the perfection to which the supply chain drivers are connected to each other and implemented. They further argued that each driver needs significant capital investment outlays to achieve projected meaningful outcomes. They warned that any disconnection between the drivers has a bid tendency to derail anticipated gains. Critical to Kwon and Kin’s framework is how well players or stakeholders in each driver connects, collaborates, or cooperate with one another. Kwon and Kin maintained that for example, should there arise any disconnection between inventory managers and transportation decision-makers, the supply chain will suffer shortage or excess inventory depending on how the disconnection unfold and between manufacturers and health-care providers, due to information inadequacy or mismanagement providers can produce more or less than requested and or in some instances, commodities not requested for at all, a situation that will compromise quality of care. The authors believed that Kwon and Kin’s conceptual framework typifies the Ghanaian situation however, added other variables including DATA SECURITY as an additional driver not included by Kwon and Kim (2018) and used the modified conceptual framework to undergird the study on it.
2.10.2 Modified Conceptual Framework for SCM Implementation
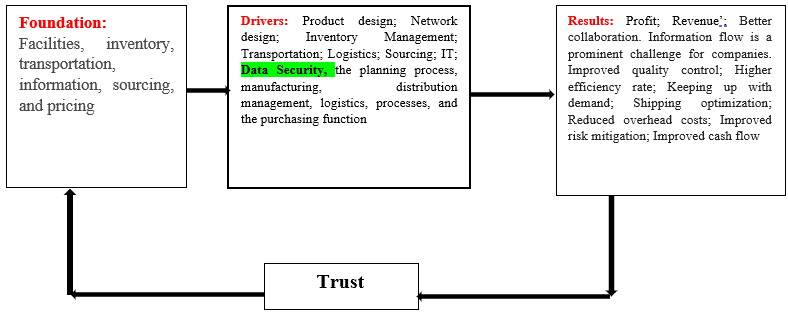
Figure 4: Author’s Modified Conceptual Framework for SCM Implementation
In our new model we assumed that the Conceptual Framework for SCM Implementation advanced by Kwon and Kim (2018) is not elaborative and informative enough. So, we expanded it the concepts. For example, Kwon and Kim did not mention any indicator under the foundation but we assumed that the foundations of any effective SCM system should include: Facilities, inventory, transportation, information, sourcing, and pricing. We also expanded the Drivers further to comprise: Data Security, the planning process, manufacturing, distribution management, logistics, processes, and the purchasing functions. Our model assumed that the results of any good SCM system is not only profit and revenue go beyond that to embrace other indicators such as Better collaboration and information flow, improved quality control; higher efficiency rate; keeping up with demand; shipping optimization; reduced overhead costs and improved risk mitigation. We also assumed in our model that Information Sharing and collaboration form part of the benefits or the results of good SCMs and should be a stand alone and so combine it with the results. We finally are of the opinion that, the results will build the needed trust which will inform the foundations of the system on next actions.
2.10.3 Conceptual Frameworks for Health Supply Chain Risk Management (HSCRM)
The conceptual framework for SCRM for this study is guided by the Smart Supply Chain Risk Management or “SCRM digitalization framework proposed by Norrman and Lindroth (2004) and its subsequent refinements. Norrman and Lindroth (2004) advanced a five-unit framework in SCRM: single logistical activity within a company (single logistics); logistical activities of the whole company (company logistics); logistical activities between two companies (dyads logistics); logistical activities between companies linked to a chain (supply chain logistics) and logistical activities between companies linked to a network (supply chain network). Norrman and Lindroth thereafter offered another dimension of SCRM based on the types of risk: operational, tactical and strategic. The work of Norrman and Lindroth has been improved by Ponis and Ntalla (2016) in their description of models and frameworks of SCRM. Further modifications were made to the SCRM framework of Norrman and Lindroth (2004) by scholars who conducted series of publication reviews for SCRM steps and match them with the ISO 31000-SCRM procedure (de Oliveira, et al.,2017; Curkovic et al., 2013). Based on these extensive works on SCRM, this study proposes the following five component SCRM framework dubbed ‘the cyclical SCRM Framework’, a slight deviation from that of Norrman and Lindroth (2004). The figure 3 below illustrates the authors proposed Cyclical Supply Chain Risk Management (CSCRM) Conceptual Framework for the study.
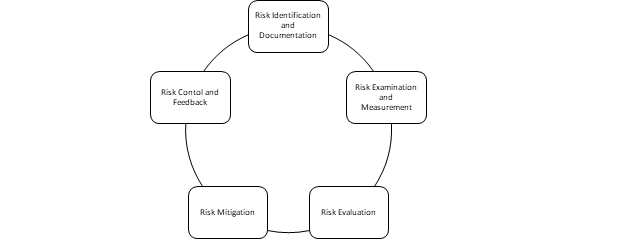
Figure 5. Cyclical Supply Chain Risk Management (CSCRM) Conceptual Framework. Authors’ Construct, (2024)
The framework proposes that to effectively and efficiently manage supply chain risks, organizations and their supply chain systems must first conduct system scanning to identify and document all SCM risks. They must critically examine and measure the risks to know if they pose an immediate potential threat or not. They must also assess the potential impact of the risks on the operations of the organization or the SCM system in the short, medium, and long terms. The framework further proposes that after assessing the probable consequences of the risks, SCM systems should develop and implement strategies and plans to mitigate the impacts and thereafter assess the results and use the feedback to consolidate gains or improve the operations of the system for value creation and addition.
2.11 Research Hypotheses
Based on the literature and the Conceptual Frameworks, the following hypotheses were developed.
Ho_1: There is no significant relationship between Risk Identification and Supply Chain Risk Reduction.
Ho_2: Risk Assessment and Mitigation does not influence Supply Chain Risk Reduction.
Ho_3: Poor supply chain risk management does not impact Supply Chain Risk Reduction
Ho_4: There is no significant association between Employee involvement in supply chain risk routine activities and Supply Chain Risk Reduction
Ho_5: There is no significant relationship between Supply Chain Risk Management Governance and Supply Chain Risk Reduction
METHODOLOGY
The study was conducted in Ghana and the scope was limited to key officers of the Ministry of Health and Ghana Health Service Supply Chain Practitioners (GHSSCP) at the central level and their collaborators at the regional levels (the Regional Health Directorates). The target population were Supply Chain Practitioners: Regional medical stores managers, supplies managers, procurement officers, general and pharmacy stores officers. Due to the nature and the objectives of the study, it employed convenience and purposive sampling techniques to select 36 participants from the Stores, Supplies, and Drug Management (SSDM) and Health Administration and Support Services (HASS) units at national level and 4 officers each from the 16 regions making a total of 100 participants. A 10% margin was added to the sample to account for withdrawals and non-participation making the total sample 110. Quantitative method was used for primary data collection. The main research instrument used for the study was questionnaire administration. The instrument consists of questions with four-point Likert Scale responses: Strongly Agree, Agree, Disagree, and Strongly Disagree. Five (5) main categories of questions were included in the research instruments: risk identification, risk assessment and mitigation, Supply Chain Risk Management Governance, impact of supply chain risk management, and employee supply chain risk routine activities. The research instrument was subjected to Cronbach Alpha test (Cronbach, 1951) to ensure validity and reliability. SPSS was used to analyze data with descriptive statistics. Appendix 1 presents details of individual elements in the research instrument.
Table 3.1: Results of One-Sample Statistics
| One-Sample Statistics | ||||
| N | Mean | Std. Deviation | Std. Error Mean | |
| There is no significant relationship between Risk Identification and Supply Chain Risk Reduction | 110 | 2.95 | .913 | .087 |
| Risk Assessment and Mitigation does not influence Supply Chain Risk Reduction | 110 | 3.11 | .971 | .093 |
| Poor supply chain risk management does not impact Supply Chain Risk Reduction | 110 | 2.95 | .913 | .087 |
| There is no significant association between Employee involvement in supply chain risk routine activities and | 110 | 2.28 | .879 | .084 |
| There is no significant relationship between Supply Chain Risk Management Governance and Supply Chain Risk Reduction | 110 | 2.22 | .932 | .089 |
The results of the One-sample statistics indicate that the Mean sample scores (2.95 ± 0.933), (3.11 ± 0.971), (2.95 ± 0.913), (2.28 ± 0.879), (2.22 ± 0.932), are all lower than but closer to the population normal mean score of 5.0. This implies that the sample mean of the population is not too different from the population mean at 95% confidence. The standard deviations close to 1 or lower as indicated in the results suggest that the data points are closer to the mean, representative of a low variance. This considered good in the framework of consistency or predictability
Table 3.2: Results of One-Sample Test
| One-Sample Test | ||||||
| Test Value = 5.0 | ||||||
| t | df | Sig. (2-tailed) | Mean Difference | 95% Confidence Interval of the Difference | ||
| Lower | Upper | |||||
| There is no significant relationship between Risk Identification and Supply Chain Risk Reduction | -23.474 | 110 | .000 | -2.036 | -2.21 | -1.86 |
| Risk Assessment and Mitigation does not influence Supply Chain Risk Reduction | -20.453 | 110 | .000 | -1.883 | -2.07 | -1.70 |
| Poor supply chain risk management does not impact Supply Chain Risk Reduction | -23.474 | 110 | .000 | -2.036 | -2.21 | -1.86 |
| There is no significant association between Employee involvement in supply chain risk routine activities and | -32.735 | 110 | .000 | -2.721 | -2.89 | -2.56 |
| There is no significant relationship between Supply Chain Risk Management Governance and Supply Chain Risk Reduction | -31.591 | 110 | .000 | -2.784 | -2.96 | -2.61 |
The results of the One-Sample Test indicated that the influence of Risk Identification on Supply Chain Risk Reduction was statistically significantly lower than the population’s normal Supply Chain Risk Reduction score, t (110) = -23.474, p = .000. The effect of Risk Assessment and Mitigation on Supply Chain Risk Reduction was also statistically significantly lower than the population’s normal Supply Chain Risk Reduction score, t (110) = -20.453, p = .000. That of Poor supply chain risk management on Supply Chain Risk Reduction yielded a statistically significantly lower outcome that the population’s normal Supply Chain Risk Reduction score, t (110) = -23.474, p = .000. The influence of Employee involvement in supply chain risk routine activities on Supply Chain Risk Reduction was also statistically significantly lower than the population’s normal Supply Chain Risk Reduction score, t (110) = -32.735, p = .000, while the effect of Supply Chain Risk Management Governance on Supply Chain Risk Reduction also recorded a statistically significantly lower outcome than the population’s normal Supply Chain Risk Reduction score, t (110) = -31.591, p = .000. The Supply Chain Risk Reduction scores were normally distributed, as assessed by Bloom’s fractional ranked estimation method (SPSS, v.21) (p < 0 .05) and there were no outliers in the data, as assessed by inspection of a boxplot. The results indicate further that there is a statistically significant difference between the sample and all defined means (p < .05). Therefore, all the null hypotheses were rejected, and the alternative hypotheses accepted. The import of the Sig. (2-tailed)) values .000 (reported as p <. 001) which are less than 0.05 suggests that there is significant evidence to reject the null hypothesis. Therefore, the null hypotheses (Hos) were rejected and the alternative hypotheses (Has) were accepted.
Table 3.3: Results of Instrument Reliability Test
| S/N | Research Instrument (Scale) | Number of Items | Cronbach Alpha Coefficient |
| 1 | Risk identification | 11 | .838 |
| 2 | Risk assessment and mitigation | 4 | .724 |
| 3 | Supply Chain Risk Management Governance | 3 | .769 |
| 4 | Impact of supply chain risk management | 8 | .799 |
| 5 | Employee supply chain risk routine activities | 10 | .889 |
| Overall | 33 | .863 |
The Cronbach Alpha results of all the individual elements of the instrument were above 0.70 which imply they are reliable for measuring the various objectives set for the study. The Cronbach Alpha result for the overall instrument is also 0.863 which indicates that the various elements in the instrument collectively are reliable for measuring the indicators to achieve the set objectives of the study.
RESULTS AND FINDINGS
Table 4.1: Demographic Profile of Respondents
| Index | Category | Number | Percentages | Mean | SD | Counts/sum |
| Gender | Male | 76 | 69.1 | 1.31 | .464 | 144 |
| Female | 34 | 30.9 | ||||
| Total (N) | 110 | 100 | ||||
| Staff category | Junior staff | 31 | 28.2 | 1.88 | .660 | 207 |
| Middle level staff | 61 | 55.4 | ||||
| Senior level staff | 18 | 16.4 | ||||
| Total (N) | 110 | 100.0 | ||||
| Age | 21-30 | 16 | 14.5 | 40.64 | 1.090 | 290 |
| 31-40 | 44 | 40.0 | ||||
| 41-50 | 14 | 12.7 | ||||
| 51-60 | 36 | 32.7 | ||||
| Total (N) | 110 | 100.0 |
For Gender, the sample of consisted of 76 males (69.1%) and female 34 (30.9%), mean of 1.31 (SD= .464) at (N = 110). For Staff Category, the sample consisted of 31 (28.2%) junior, 61 (55.4%) middle, and 18 (16.4%) senior level staff, a mean of 1.88 (SD = .660) at (N=110). Average age of respondents was 40.64 (SD = 1.090) at (N= 110).
Regression Analysis
SPSS V.21 was used to run multiple linear regression to determine the effect of the independent (predictor) variables on the dependent (outcome) variable.
Table 4.2: Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | .893a | .797 | .789 | .463 |
| a. Predictors: (Constant), Employee supply chain risk routine activities, Supply Chain Risk Management Governance, Risk Assessment and Mitigation, Impact of poor supply chain risk management on organizational operations | ||||
The R-value represents the correlation between the dependent and independent variable. A value greater than 0.4 is taken for further analysis. In this case, the value is .893, which is good. The R-square shows the total variation for the dependent variable that could be explained by the independent variables. A value greater than 0.5 shows that the model is effective enough to determine the relationship. In this case, the value is .797, which is good. The Adjusted R-square shows the generalization of the results, thus, the variation of the sample results from the population in multiple regression. It is required to have a difference between R-square and Adjusted R-square minimum. In this case, the value is .789, which is not far off from .797, so it is good. This R-square result indicates that 78.9% of the variance in the dependent/outcome/response variable, Supply Chain Risk Reduction (SCRR) is explained by the independent/ predictor variables:), Employee supply chain risk routine activities, Supply Chain Risk Management Governance, Risk Assessment and Mitigation, Impact of poor supply chain risk management on organizational operations
Table 4.3: ANOVAa
| Model | Sum of Squares | df | Mean Square | F | Sig. | |
| 1 | Regression | 87.692 | 4 | 21.923 | 102.206 | .000b |
| Residual | 22.308 | 104 | .214 | |||
| Total | 110.000 | 108 | ||||
| a. Dependent Variable: Supply Chain Risk Reduction | ||||||
| b. Predictors: (Constant), Employee supply chain risk routine activities, Supply Chain Risk Management Governance, Risk Assessment and Mitigation, Impact of poor supply chain risk management on organizational operations | ||||||
From the ANOVA table, the sig value is .000b (p < .01). This means that within the general SCM system of the GHS, there are statistically significant differences among the groups in Supply Chain Risk Reduction (SCRR) across the different organizations or facilities. Base on this evidence the null hypothesis, which assumes no significant differences was rejected. Because the used a 95% confidence interval or 5% level of the significance level, it implies that the p-value should be less than 0.05. In the above table, it is .000. Therefore, the result is considered significant. The study however did not run post-hoc analysis to determine how each predictor differs from another. The study thus relied on the general assumption derived from the ANOVA table.
Table 4.4. Coefficientsa
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | ||
| B | Std. Error | Beta | ||||
| 1 | (Constant) | .346 | .196 | 1.770 | .080 | |
| Risk Assessment and Mitigation | .984 | .055 | .947 | 17.959 | .000 | |
| Supply Chain Risk Management Governance | -.051 | .052 | -.046 | -.968 | .335 | |
| Impact of poor supply chain risk management on organizational operations | -.041 | .195 | -.036 | -.212 | .832 | |
| Employee supply chain risk routine activities | -.070 | .182 | -.064 | -.384 | .702 | |
| a. Dependent Variable: Supply Chain Risk Reduction | ||||||
Table 4.5: Excluded Variablesa
| Model | Beta In | t | Sig. | Partial Correlation | Collinearity Statistics | |
| Tolerance | ||||||
| 1 | Risk Identification | .b | . | . | . | .000 |
| a. Dependent Variable: Supply Chain Risk Reduction | ||||||
| b. Predictors in the Model: (Constant), Employee supply chain risk routine activities, Supply Chain Risk Management Governance, Risk Assessment and Mitigation, Impact of poor supply chain risk management on organizational operations | ||||||
The results indicate that except for Risk Identification, all the other independent variables: Risk Assessment and Mitigation, Supply Chain Risk Management Governance, Impact of poor supply chain risk management on organizational operations, and Employee supply chain risk routine activities collectively immense negative effects on Supply Chain Risk Reduction in a manner (F (4, 79) = 102.206; R2 = 0. 797; P <0.05). Overall, the study found that these variables contributed to 78.9% of the variance in the dependent/outcome/response variable, Supply Chain Risk Reduction (SCRR). The results specifically indicated that Supply Chain Risk Management Governance β= -.051; t = -.968; P>0.05), Impact of poor supply chain risk management on organizational operations (β= -.041; t = -.212; P>0.05), and Employee supply chain risk routine activities (β= -.070; t = -.384; P>0.05) have a negative effect on Supply Chain Risk Reduction, while Risk Assessment and Mitigation (β = .984; t= 17.959; P< 0.05) is an independent predictor of Supply Chain Risk Reduction. These results established that while Supply Chain Risk Reduction is undeniably influenced by Supply Chain Risk Management Governance, Impact of poor supply chain risk management on organizational operations, and Employee supply chain risk routine activities negatively, Risk Assessment and Mitigation can influence it positively depending on how it is implemented. The results showing both negative and positive correlations between the independent variables and the dependent variable are adequate and statistically significant at P>0.05. Consequently, the hypotheses tested were presumed to be valid. Generally, these results amply demonstrated that Supply Chain Risk Management Governance, Impact of poor supply chain risk management on organizational operations, the level of employee involvement in supply chain risk routine activities, and the extent to which risk assessment and mitigation is conducted, contribute effectively to predicting the level and impact of Supply Chain Risk Reduction in the facilities.
DISCUSSIONS, CONCLUSION, AND RECOMMENDATIONS
5.1 Discussions of Findings
The results of the study generally revealed fundamental weaknesses in almost all the supply chain dimensions covered: risk identification, risk assessment and mitigation, Supply Chain Risk Management Governance, impact of supply chain risk management, and employee supply chain risk routine activities. These discoveries agreed with findings in previous studies (Adu-Poku et al., 2011; Laysons & Farrington., 2006; PPA, 2018). The general implication of these weaknesses on the SCM system is their higher tendency to expose the system to aggravated SCM deficiencies leading to the occurrence of high level SCM risks that will have dare consequences for healthcare delivery and by extension health outcomes. Of great concern is the fact that supply chain interruptions and vulnerabilities such as the nonexistence of risk registers, accident books, and reference manual for SCM risk activities, irregular SCM Risk Identification Exercise of facilities, lack of mapping and collection of information on SCM risks, lack of quantification and calculation of risk exposure toward specific SCM activities, and irregularly conduct of business interruption risk audit on existing SCM activities are the drivers of the high SCM risks within the system, something that can easily be controlled. These findings resonate with those of (Chopra and Sodhi, 2004; Norrman and Jansson, 2004; Pettit, Crocton & Fiksel, 2013; Tang & Tomlin, 2008; Faisal, et al., 2006, 2008; Fan, et al., 2016, 2017; Zweig, et al., 2015; Joy FM, 2015; Owusu-Sekyere et al., 2017) when they variously found in their studies that the supply chain systems they studied are surrounded with myriad of interruptions and vulnerabilities that militate against the systems performance. The proof that the SCM system of the GHS is fraught with poor Risk Assessment and Mitigation measures across the chain manifesting in non-reliance on internal Safety Stocks, usage of single sourcing strategies, and non-implementation of supplier development programs or suppliers’ protection measures as SCM risk mitigation measures as evidenced in the study should be of great concern to all stakeholders within the system. The huge SCM leadership and governance gaps exemplified by lack of Senior management’s concern for and commitment to Supply chain risk management issues is not only a worry but a syndrome if not checked and nipped in the bud will have debilitating consequences for the system as most facilities were found not to have any supply chain risk management framework and do not involve external partners and stakeholders in supply chain risk management processes. The high level of non-adherence to supply chain risk management practices by almost all facilities within the GHS which has resulted and is still resulting in huge financial and material losses through theft and corruption, unnecessary shortage of medicines and non-medical consumables, low productivity, low staff morale and poor performance, customer dissatisfaction, low level of donor confidence, and to poor health outcomes and loss of lives in the health sector must serve as an epicenter for policy review on SCM. The low level of employee involvement in supply chain risk management routine activities across the chain at all levels serve as a great disincentive and will compel people to sabotage the system if nothing is immediately done to reverse the trend. The manifestations of staff not working with any clear facility level written SCM instructions or guidelines although there is a national guideline to be relied upon, neither do they work effectively as a SCM teams should not be overemphasized. Channels of communication on SCM issues were also found to be lacking, because there are no serious tracking and most departments /units do not take supply chain risk management seriously. Breakdown of communication is a serious gap which can destroy the system. The world is changing and technologies on SCM are fast evolving so if training in SCRM for staff especially at the middle and lower levels (regions and districts) are ignored, the consequences will be very severe because more than 70 to 80% of the SCM activities happened downstream. Goods and services in any SCM system must reach the final consumer to be deemed as complete, therefore, the ineffective transportation system will increase turnaround time for delivery delays and this defeats the purpose of the introduction of the LMD. As Ganiyu, et. al. (2020), Wagner and Neshat (2012), Koenig and Poncet, (2019), Pettit et al. (2013), Chopra and Sodhi, (2014), Owusu-Sekyere et al. (2017), and Joy FM, (2015) variously indicated, it is unequivocal to state that the collective consequence of the gaps identified in the study are capable of destroying the marginal gains made by the introduction and execution of key interventions such as Supply chain master plan (SCMP), the Last Mile Distribution (LMD) of health commodities from the Central level to Regional medical stores and to health facilities in the Districts, and the introduction of the Ghana Integrated Logistics Management Information System (GhiLMIS) for health commodity management at all levels across the public health sector SCM system. We believe that if the overarching objective of these interventions is to ensure the effectiveness and efficiency of the system through the minimization of SCM risks, interruptions, and vulnerabilities, then at their current state, the system is still subject to ineffectiveness and inefficiencies of existing Supply Chain Technical Working Groups (SCTWGs) in the system which only largely exist on paper but their collective functionality grossly overridden by the centralization of the system at all the levels consequently exposing the system to high level SCM interruptions, vulnerabilities, and risks which when not tackled will break down the entire SCM system in the future.
5.2 Conclusions
This study examined the supply chain and its risk management practices among key stakeholders (the central level, regional and districts) of GHS to identify the challenges of the existing SCM system risk management and propose measures of addressing these challenges. The main focus of the study was to answer the research question: The introduction of Supply chain management interventions across the public health sector in Ghana do not lead to supply chain risk reduction within the health sector as envisaged. The study exposed basic weaknesses in almost all the supply chain dimensions covered: risk identification, risk assessment and mitigation, Supply Chain Risk Management Governance, impact of supply chain risk management, and employee supply chain risk routine activities and indicated that that 78.9% of the variance in the dependent/outcome/response variable, Supply Chain Risk Reduction (SCRR) is explained by the independent/ predictor variables:), Employee supply chain risk routine activities, Supply Chain Risk Management Governance, Risk Assessment and Mitigation, Impact of poor supply chain risk management on organizational operations. We therefore conclude that although the intension of introducing supply chain management interventions into the public health sector in Ghana is to ensure that the system works to value for money by enhancing financial performance, customer satisfaction, reduce delivery times, build trust, confidence and commitment among suppliers, there is however lack of proper attention of integration of supply chains activities to achieve expected benefits evidenced by the existence of key challenges notwithstanding the implementation of the interventions due to managements’ poor attitude to risk, overly centralization of SCM activities, and non-involvement of the grassroot professionals in SCM decisions.
5.3 Recommendations
Based on the findings, we recommend that the GHS should establish alongside the existing Supply Chain Technical Working Groups (SCTWGs), a Supply Chain Risk Management Unit (SCRMU) at all levels (national, regional, and districts) under the supervision of Health Administration and Support Services and charged with define SCM leadership and governance roles and responsibilities including proper monitoring and supervision mechanisms to ensure timely risk identification, risk assessment, prioritization, and management, with the involvement of all stakeholders in the process to achieve the intended SCM operations and its risk mitigation and reduction. We also recommend the introduction of the signing of SCM performance contracts with incentives (punishments and rewards) at all levels across the SCM system of the service to inspire stakeholders to live up to their expected roles and responsibilities. We are also proposing that Supply Chain Risk Management (SCRM) should form part of the orientation and appraisal of managers and all supply chain staff for the purpose of implanting and nurturing strong risk management principles and culture in the Service. We further endorse a stronger and enhanced but user-friendly GhiLMIS technology driven SCM supported by a robust feedback system to ensure proper accountability.
Limitations
Although the study relied exclusively on quantitative data and used descriptive and inferential statistics generated by SPSS v.21 in analyzing data, it uses non-probability sampling due to the uniqueness of the subject matter. A mixed method with random sampling for quantitative data and non-random sampling for qualitative data would have triangulated the findings and give a more reflection of the issues considered.
Further Research
Future research should consider employing mixed method to ensure the use of multiple statistical tools and analysis to triangulate data and ensure a more acceptable generalizability of findings.
ACKNOWLEDGMENT
We are most grateful to God and all collaborators who has inspired us to conduct this study. We also appreciated the practical insights we had from officers of the Stores, Supply, and Drug Management (SSDM) division of the GHS. Our gratefulness also goes to the faculty of Business Management at Philippine Christian University, Manila Philippines where some of the authors are currently studying for Ph.D. in Business Management (International Healthcare Systems. We also acknowledge the health facilities and professionals who were involved and contributed to the study.
Conflicts of Interest
The authors declare no conflicts of interest concerning the publication of this paper
REFERENCES
- Adu-Poku S, Asamoah D., Aseweh Abor P. (2011). Users’ Perspective of Medical Logistics Supply Chain System in Ghana: The case of Adansi South District Health Directorate. SAGE Journal of Medical Marketing Vol. 11, 2, 176–190.
- Alhawari S., Karadsheh L., Talet A.N., Mansour E., (2012). Knowledge-Based Risk Management framework for Information Technology project, International Journal of Information Management (32), 50–65.
- Al-Saa’da, R., Taleb, Y., Abdallat, M., Al-Mahasneh, R., Nimer, N., & Al-Weshah, G. (2022). Supply Chain Management and Its Effect on Health Care Service Quality: Quantitative Evidence from Jordanian Private Hospitals. Journal of Management and Strategy, 4, 42-51.
- Anvuur, A., Kumaraswamy, M., & Male, S. (2006). Taking forward Public Procurement Reforms in Ghana. In A. Serpell (Ed.), Proceedings of CIB W107 International Symposium on Construction in Developing Economies (Paper No. 1.4). CIB.
- Anvyl (2022, September 2). Evaluating the 6 Supply Chain Models Powering Businesses Around the World. Supply Chain Models. https://anvyl.com/blog/supply-chain-model/
- Asamoah, K. , Asare-Bediako, E. and Jacqueline, A. (2023) Effects of Supply Chain Visibility on Supply Chain Performance in Ghana Health Service: The Case of Kumasi Metro Health Directorate. Open Journal of Business and Management, 11, 437-463. doi: 10.4236/ojbm.2023.112024
- Atiga, O., Walters, J. & Pisa, N. (2023). Challenges of medical commodity availability in public and private health care facilities in the Upper East Region of Ghana: a patient-centered perspective. BMC Health Serv Res 23, 719. https://doi.org/10.1186/s12913-023-09717-9
- Aqlan, Faisal, and Sarah S. Lam. 2016. Supply chain optimization under risk and uncertainty: A case study for high-end server manufacturing. Computers & Industrial Engineering 93: 78–87
- Boakye, G., Gyedu, A., Stewart, M. et al. (2021). Assessment of local supply chains and stock management practices for trauma care resources in Ghana: a comparative small sample cross-sectional study. BMC Health Serv Res 21, 66. https://doi.org/10.1186/s12913-021-06063-6
- Bossert T, Bowser D, Amenyah J. (2014). Ghana: Decentralization and the Health Logistics Systems.
- Cheng T.C.E., Yip F.K., Yeung A.C.L., (2012). Supply risk management via guanxi in the, Chinese business context: The buyer’s perspective, International Journal of Production Economics (139), 3–13.
- Chopra, S. and M. S. Sodhi (2004). “Managing Risk To Avoid Supply-Chain Breakdown”. In: MIT Sloan Management Review 46.1, pp. 53–61.
- Chopr S & Sodhi M. (2014). Reducing the risk of supply chain disruptions. MIT Sloan Manag Rev. 55:72–80.
- Cooper, M.C., Lambert, D.M., & Pagh, J. (1997) Supply Chain Management: More Than a New Name for Logistics. The International Journal of Logistics Management Vol 8, Iss 1, pp 1–14
- Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika, 16, 297–334.
- Curkovic, S., T. Scannel, and B. Wagner (2013). “ISO 31000:2009 – Enterprise and Supply Chain Risk Management: A Longitudinal Study”. In: American Journal of Industrial and Business Management 3, pp. 614–630.
- de Oliveira, U. R., F. A. S. Marins, H. M. Rocha, and V. A. P. Salomon (2017). “The ISO 31000 standard in supply chain risk management”. In: Journal of Cleaner Production 151, pp. 616–633.
- Domie, G. and Dodzi, S. (2023) Medicine Procurement Framework for Public Hospitals under the Ministry of Health in Ghana: A Case of the Western Region. Open Journal of Business and Management, 11, 2084-2103. doi: 10.4236/ojbm.2023.115115.
- Faisal, M. N., D. K. Banwet, and R. Shankar (2006). “Supply chain risk mitigation: modeling the enablers”. In: Business Process Management 12.4, pp. 535–552
- Fan, H., T. C. E. Cheng, G. Li, and P. K. C. Lee (2016). “The Effectiveness of Supply Chain Risk Information Processing Capability: An Information Processing Perspective”. In: IEEE Transactions on Engineering Management 63.4, pp. 414–425.
- Fan, H., G. Li, H. Sun, and T. Cheng (2017). “An information processing perspective on supply chain risk management: Antecedents, mechanism, and consequences”. In: International Journal of Production Economics 185, pp. 63–75.
- Fekete, A. 2012a. Spatial disaster vulnerability and risk assessments: Challenges in their quality and acceptance. Natural Hazards 61(3): 1161–1178.
- Fekete, A. 2012b. Safety and security target levels: Opportunities and challenges for risk management and risk communication. International Journal of Disaster Risk Reduction 2: 67–76.
- Ganiyu, S., Yu, D., Xu, C. and Providence, A. (2020) The Impact of Supply Chain Risks and Supply Chain Risk Management Strategies on Enterprise Performance in Ghana. Open Journal of Business and Management, 8, 1491-1507. doi: 10.4236/ojbm.2020.84095.
- Gurtu, Amulya, and Jestin Johny. (2021). “Supply Chain Risk Management: Literature Review” Risks 9, no. 1: 16. https://doi.org/10.3390/risks9010016
- Habib, Md. M., Chowdhury, F., Sabah, S., & Debnath, D. (2022). A Study on Hospital Supply Chain Management. American Journal of Industrial and Business Management, 12, 806-823. https://doi.org/10.4236/ajibm.2022.125042
- Harland C., Brenchley R., Walker H., (2003). Risk in supply networks, Journal of Purchasing and Supply Management (9), 51–62.
- Hillman, M. and H. Keltz (2007). Managing Risk in the Supply Chain – A Quantitative Study. Ed. by AMR Research.
- Hines, Tony. (2014). Supply Chain Strategies: Demand Driven and Customer Focused. Taylor & Francis. ISBN 978-1-136-70396-6
- Ho, W., T. Zheng, H. Yildiz, and S. Talluri (2015). “Supply chain risk management: a literature review”. In: International Journal of Production Research 53.16, pp. 5031–5069
- Joy 99.7 FM (January 14, 2015). Fire ravaged Central Medical Stores: Not insured. https://web.facebook.com/joy997fm/posts/fire-ravaged-central-medical-store-was-not-insured-ministry-it-has-emerged-that-/10152984182991894/? rdc=1& rdr
- Koenig P, Poncet S (2019) Social responsibility scandals and trade. World Dev 124:104640
- Kozlenkova, Irina V.; Hult, G. Tomas M.; Lund, Donald J.; Mena, Jeannette A.; Kekec, Pinar (2015). “The Role of Marketing Channels in Supply Chain Management”. Journal of Retailing. 91 (4): 586–609. doi:10.1016/j.jretai.2015.03.003. ISSN 0022-4359
- Kwon, I.-W. and Kim, S.-H. (2018), “Framework for successful supply chain implementation in healthcare area from provider’s prospective”, Asia Pacific Journal of Innovation and Entrepreneurship, Vol. 12 No. 2, pp. 135-145. https://doi.org/10.1108/APJIE-04-2018-0024
- Lauer, C. (2004). Excellence in supply chain management. Modern Healthcare. 34(50): 29-32
- La Londe, B. and Masters, J. M. (1994). Emerging Logistics Strategies: Blueprints for the Next Century, International Journal of Physical Distribution & Logistics Management, Vol. 24 No. 7, pp. 35-47. doi:10.1108/09600039410070975
- Lavassani, K.M., & Movahedi, B. (2010). Critical Analysis of the Supply Chain Management Theories: Toward the Stakeholder Theory.
- Laysons , K . & Farrington , B . (2006) Purchasing and Supply Chain Management, 7th edn. London; New York: Financial Times/Prentice.
- Manso JF, Annan J, Anane SS. (2013). Assessment of Logistics Management in Ghana Health Service. Int J Bus Soc Res. 3(8):75–87.
- Mentzer, J.T.; et al. (2001). “Defining Supply Chain Management”. Journal of Business Logistics. 22 (2): 1–25. doi:10.1002/j.2158-1592.2001.tb00001.x.
- Ministry of Health, Ghana (2022). Health Commodity Supply Chain Master Plan (HCSCMP). https://www.moh.gov.gh/wp-content/uploads/2022/06/Ghana-Final-Final.pdf
- Ministry of Health, Ghana (2022). Health Commodity Supply Chain Master Plan (HCSCMP) 2021-2025. https://www.moh.gov.gh/wp-content/uploads/2022/06/Ghana-Final-Final.pdf
- Nabil Abu el Ata, Rudolf Schmandt (2016), The Tyranny of Uncertainty, Springer, ISBN 978-3662491041
- Norrman, A. and U. Jansson (2004). “Ericsson’s proactive supply chain risk management approach after a serious sub-supplier accident”. In: International Journal of Physical Distribution & Logistics Management 34.5, pp. 434–456
- Norrman, A. and R. Lindroth (2004). “Categorization of Supply Chain Risk and Risk Management”. In: Supply chain risk. Ed. by C. Brindley. Hanpshire, Burlington: Ashgate Publishing Ltd., pp. 14– 27.
- Osei-Assibey, A., & Akweongo, P. (2017). Assessment of Availability of Essential Medicines in Sekondi-Takoradi Metropolis. Journal of Biomedical and Pharmaceutical Research, 6, 100-111.
- Owusu-Sekyere, Ebenezer & Yakubu Adjuik, Robert & Wedam, Emmanuel. (2017). The Central Medical Store Fire Disaster: A Test for Institutional Compliance in Disaster Prevention in Ghana. SAGE Open. 7. 215824401769952. 10.1177/2158244017699528.
- Pervez, M. N., Mahmud, J., & Bachar, S. C. (2016). Supply Chain Management of Pharmaceutical Products in Hospitals: A Case Study in A Privately-Owned Tertiary Level Hospital. Journal of Research in Business and Management, 4, 14-23.
- Pettit, T. J., K. L. Crocton, and J. Fiksel (2013). “Ensuring Supply Chain Resilience: Development and Implementation of an Assessment Tool”. In: Journal of Business Logistics 34.1, pp. 46–76.
- Ponis, S. T. and A. C. Ntalla (2016). “Supply Chain Risk Management Frameworks and Models: A Review”. In: International Journal of Supply Chain Management 5.4, pp. 1–11. Proceedings of 2015 International Conference on Intelligent Computing and Internet of Things: ICIT 2015 : January 17-18, 2015, Harbin, China (2015). Piscataway, NJ: IEEE.
- Public Procurement Authority, PPA (2018). HEALTH SECTOR PROCUREMENT IN GHANA: WEAKNESSES AND OPPORTUNITIES. https://ppa.gov.gh/health-sector-procurement-in-ghana-weaknesses-and-opportunities/
- Purdy, G (2010). “ISO 31000:2009–Setting a New Standard for Risk Management”. Risk Analysis. 30 (6): 881–886.
- Robert B. Handfield; Ernest L. Nichols (1999). Introduction to Supply Chain Management. New York: Prentice-Hall. p. 2. ISBN 0-13-621616-1
- Schneller, S. Eugene S., Larry R. Smeltzer. (2006). Strategic Management of the Healthcare Supply Chain. Jossey-Bass.
- Schlüter, Florian; Henke, Michael (2017) : Smart supply chain risk management – a conceptual framework, In: Kersten, Wolfgang Blecker, Thorsten Ringle, Christian M. (Ed.): Digitalization in Supply Chain Management and Logistics: Smart and Digital Solutions for an Industry 4.0 Environment. Proceedings of the Hamburg International Conference of Logistics (HICL), Vol. 23, ISBN 978-3-7450-4328-0, epubli GmbH, Berlin, pp. 361-380, https://doi.org/10.15480/882.1466
- Shantanu Trivedi (2023). Some Contemporary Theories in Supply Chain Management. https://managemententhusiast.com/some-contemporary-theories-in-supply-chain-management/
- Sun J., Matsui M., Yin Y., (2012). Supplier risk management: An economic model of P-chart considered due-date and quality risks, International Journal of Production Economics (139), 58–64.
- Tang, C. S. (2006). Perspectives in Supply Chain Risk Management. International Journal of Production Economics, 103, 451-488. http://dx.doi.org/10.1016/j.ijpe.2005.12.006
- Tang, C. and B. Tomlin (2008). “The power of flexibility for mitigating supply chain risks”. In: International Journal of Production Economics 116.1, pp. 12–27
- USAID, (2009). DELIVER PROJECT TO, editor. Logistics System Assessment Tool (LSAT). Arlington: USAID | DELIVER PROJECT, Task Order 1.
- Wagner, S. M., & Neshat, N. (2012). A Comparison of Supply Chain Vulnerability Indices for Different Categories of Firms. International Journal of Production Research, 50, 2877-2891.
https://doi.org/10.1080/00207543.2011.561540 - Zsidisin, G. A. and B. Ritchie (2009a). “Chapter 1: Supply Chain Risk Management – Developments, Issues and Challenges”. In: Supply Chain Risk. Ed. by G. A. Zsidisin and B. Ritchie. Vol. 124. International Series in Operations Research & Management Science. Boston MA: SpringerVerlag US, pp. 1–12.
- Zsidisin, G. A. and B. Ritchie, eds. (2009b). Supply Chain Risk: A Handbook of Assessment, Management, and Performance. Vol. 124. International Series in Operations Research & Management Science. Boston MA: Springer-Verlag US.
- Zweig, M., A. Agawal, B. Stall, C. Bremer, P. Mangers, A. Beifus, and M. Chauhan (2015). Globalize or customise: finding the right balance: Global steel 2015-2016. Ed. by EY.
APPENDIX A:
Research Instrument: Questionnaire
This study REDUCING SUPPLY CHAIN MANAGEMENT RISKS IN THE HEALTH SECTOR OF GHANA: AN EVALUATION OF THE CENTRAL LEVEL SUPPLY CHAIN MANAGEMENT SYSTEM OF THE GHANA HEALTH SERVICE is set to examine supply chain risk management practices at the central level of GHS, identify the challenges of the existing SCM system and propose measures of addressing these challenges. Please tick (√) in the appropriate column that represents your candid opinion in each statement
Risk Identification (RI)
| Codes | Items | Strongly Agree | Agree | Disagree | Strongly Disagree |
| RI.1 | We have risk register to documenting SCM risks | ||||
| RI.2 | We use risk register to document SCM risks | ||||
| RI.3 | We have reference manual for SCM risk activities | ||||
| RI.4 | We use reference manual for SCM risk activities | ||||
| RI.5 | We have alternative plans for SC risk management | ||||
| RI.6 | We have SCM accident book | ||||
| RI.7 | We use SCM accident book for registering SCM accidents | ||||
| RI.8 | We conduct Regular SCM Risk Identification Exercise | ||||
| RI.9 | My facility/organization map and collect information on SCM risks | ||||
| RI.10 | My facility/organization quantify/calculate its risk exposure toward any specific SCM activity | ||||
| RI.11 | My facility/organization regularly conducts a business interruption risk audit on existing SCM activities |
Risk Assessment and Mitigation (RAM)
| Codes | Items | Strongly Agree | Agree | Disagree | Strongly Disagree |
| RAM.1 | My facility/organization relies on its internal Safety Stock to mitigate supply Business Interruption | ||||
| RAM.2 | My facility/organization adopts dual sourcing strategy (i.e., buying the same item from two different suppliers) as risk mitigation measure | ||||
| RAM.3 | My facility/organization has pre-qualified back-up suppliers (i.e., a secondary supplier that is used only when a primary supply is disrupted as risk mitigation measure | ||||
| RAM.4 | My facility/organization implements supplier development programs or suppliers’ protection measures (i.e., measures to fortify suppliers in order to strengthen their reliability and resilience during disruptions and in turbulent environments as a risk mitigation measure |
Supply Chain Risk Management Governance (SCRMG)
| Codes | Items | Strongly Agree | Agree | Disagree | Strongly Disagree |
| SCRMG.1 | My facility/organization has a defined Senior management for Supply chain risk management | ||||
| SCRMG.2 | My facility/organization has a supply chain risk management framework | ||||
| SCRMG.3 | My facility/organization involves external partners and stakeholders in its supply chain risk management |
Impact of poor supply chain risk management on organizational operations (IPSCRM)
| Codes | Items | Strongly Agree | Agree | Disagree | Strongly Disagree |
| IPSCRM.1 | Non-adherence to SCM Risk associated with my job can result into serious financial lost | ||||
| IPSCRM.2 | Poor SCM risk management can result low productivity | ||||
| IPSCRM.3 | Poor Supply Chain risk management can result in customer dissatisfaction | ||||
| IPSCRM.4 | Non- insurance of warehouses and stocks is a serious SCM risk breech | ||||
| IPSCRM.5 | Poor Supply chain risk management can cause shortage of medicines and non-medical consumables | ||||
| IPSCRM.6 | Poor SCRM can lead to poor health outcomes and loss of lives in the health sector | ||||
| IPSCRM.7 | Risk free SCM environment can lead to theft and corruption | ||||
| IPSCRM.8 | Poor SCRM can lead to low level of donor confidence | ||||
| IPSCRM.8 | Poor SCRM can lead to low staff morale and poor performance |
Employee supply chain risk routine activities (ESCMRA)
| Codes | ITEMS | Strongly Agree | Agree | Disagree | Strongly Disagree |
| ESCMRA.1 | In my facility, I work with a clear written SCM instruction | ||||
| ESCMRA.2 | In my facility, we work effectively as a SCM team | ||||
| ESCMRA.3 | In my facility, there are existing clear channels of communication on SCM issues | ||||
| ESCMRA.4 | In my facility, my department /unit takes risk management seriously | ||||
| ESCMRA.5 | In my facility, the last time I had training in SCRM in relation to my job is over a year | ||||
| ESCMRA.6 | In my facility, there is little or no risk associated to my job as a SCM professional | ||||
| ESCMRA.7 | In my facility, availability and use of Risk Guide will make my work easier | ||||
| ESCMRA.8 | In my facility, my work is full of Supply chain risk or uncertainty but there is no guideline of dealing with them | ||||
| ESCMRA.9 | In my facility, a am allowed to develop a good SCRM work plan | ||||
| ESCMRA.10 | In my facility, good transportation system exists to reduce SCMR of delivery delays |