
Relationship between Quality of Life and Depressive Disorder among Women living with Breast Cancer in Nigeria
- Babatunde Suleiman
- Omodele Opadola
- Taiwo Alatishe
- Samson Ojedokun
- Folashade Dare
- Oluwafunbi Opadola
- 1161-1174
- Feb 17, 2023
- Psychiatry
Relationship between Quality of Life and Depressive Disorder among Women living with Breast Cancer in Nigeria
Babatunde Suleiman1, Omodele Opadola2, Taiwo Alatishe3, Samson Ojedokun4, Folashade Dare5, Oluwafunbi Opadola6*
1Department of Psychiatry, LAUTECH Teaching Hospital Ogbomoso, Oyo State Nigeria
2Department of Anesthesia, Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Osun State Nigeria
3Department of Psychiatry, LAUTECH Teaching Hospital Ogbomoso, Oyo State Nigeria
4Department of Chemical Pathology LAUTECH Teaching Hospital Ogbomoso Oyo State Nigeria
5Department of Medicine State Specialist Hospital, Asubiaro, Osun state
6Department of Psychiatry, LAUTECH Teaching Hospital Ogbomoso, Oyo State Nigeria
*Corresponding author
Abstract
Background: Quality of Life among women with breast cancer is an important parameter for monitoring disease progression in the early stage of the disease. A low/poor quality of life could increase their venerability to depression because of the stress that results in the course of diagnosis and treatment. This study aimed to assess the quality of life among women living with breast cancer and depressive disorder.
Methods: The study was a comparative cross-sectional design conduct among breast cancer patient with depressive disorder. 69 questionnaires were administered to the women test subject, and twice this number to the comparative control group (1:2), making a minimum sample size of 207. The instruments used for this study include; Socio-demographic and clinical variable questionnaire. Patients Health Questionnaire (PHQ-9). World Health Organization Quality of Life-BREF. Data were analyzed using SPSS version 21. The association between quality of life and depression were analyzed using an independent t-test and analysis of variance (ANOVA). The confidence level for all the tests will be set at 95%. A p-value of less than 0.05 was taken as statistically significant.
Results: The study observed that 34.3% of total respondents had major depression. From QoL, physical domain scores decreased significantly from no depression (64.7 ± 11.1) to major depression (50.5 ± 9.3), ρ-value = 0.001. Also, social domain scores were significantly higher among women with no depression (58.5 ± 16.0), those with major depression (43.0 ± 11.0), ρ-value = 0.003. These levels were statistically significant. Moreso, the mean score psychological and Environmental domains QoL were lower in the depressive subject compared to the control group however no statistically significant. (P-values 0.053 and 0.803 respectively)
Conclusions: The significant predictor for quality of life is the stress from the disease condition. Women with breast cancer who had Major Depressive Disorder had lower mean scores in all QoL domains compared to those without Major Depressive Disorder. Hence, the role of psychological assessment in the management of breast malignancies is hereby advocated to improve the quality of life and treatment outcomes.
Keywords: Quality of life, Breast cancer, depression, Ogbomoso, Nigeria
Introduction
One-third to half of the women with breast cancer have psychological distress. More often than not psychological distress is overlooked and this can impact negatively in how they cope with the disease.
Breast cancer risk is higher among women with depression because they are less likely to show concern for their health and thus forfeit the chance of early detection and treatment1.
Women with breast cancer could be more susceptible to depression because of the stress that results in the course of diagnosis and treatment2. Changes in the integrity of the body, physical symptoms stemming from cancer, the debilitating side effects of the treatment, financial burden, and social difficulty could make them vulnerable to depression.
The concept of quality of life (QoL) broadly encompasses how an individual measure the goodness of multiple aspects of their life3. It is the level of engagement in activities of daily living which has a significant effect on the feeling of being well, satisfaction, overall functioning, and control over the disease4. Health-related quality of life (HRQOL) on the other hand is the objective part of QOL. The domains of physical, psychological, and social, and spiritual well-being are often considered in the assessment of QOL of people with cancer5.
QOL among women with breast cancer is an important parameter for monitoring disease progression in the early stage of the disease6. There is a dearth of research on the association between depression and QOL among women with breast cancer locally and even in Africa as a continent. Begovic explored body image, physical attractiveness, and femininity and examined the effect of these variables on depression and QOL among 70 female breast cancer survivors in Cleveland, US. He concluded that being female, attractiveness, and dissatisfaction with body image has a positive correlation with depression and a negative one with the overall quality of life7. Furthermore, another study reported that although depression affects the overall QOL, it might not be significant in some domains/subscale8. Ardebil investigated the prevalence of depression to health-related QOL among 60 women with breast cancer in IMKH Hospital in Iran and found that depression does not affect the social/family subscale of the overall QOL.
In contrast, a study in India found that women with breast cancer who had depression had lower QOL affecting not only in some domains but all.9 This implies that depression in breast cancer patients causes more impairment in the physical, psychological, social, and environmental domains. Hence, this study aimed to assess the quality of life among people living with breast cancer and depression in Ogbomoso Nigeria.
Methodology
Study Population
Participants were women with breast cancer attending the General Surgery Outpatient clinic and a comparison group of age-matched women without a history of breast cancer at LAUTECH Teaching Hospital, Ogbomosho Oyo State South West, Nigeria.
Study Design
The study was a comparative cross-sectional study
Sample Size
The sample size was calculated using the formula for comparing two groups by Wang et al10. The calculated minimum sample size was 62. The minimum size after correcting for attrition (non-response) when the anticipated response rate is 90% was approximately 69.
Therefore, 69 questionnaires were administered to the women with breast cancer, and twice this number to the comparative group (1:2), making a minimum sample size of 207.
Study Instruments
The instruments used for this study include;
- Socio-demographic and clinical variable questionnaire
- Patients Health Questionnaire (PHQ-9)
- World Health Organization Quality of Life-BREF
The socio-demographic and clinical variable questionnaire
This is a self-defined questionnaire that inquiries about socio-demographic variables. This includes; age, marital status, employment status, average income per month, educational status, amounts spent on medications/treatment per month. Clinical variables include; year of diagnosis, stage of the disease, treatment type, and duration of treatment, family history of breast cancer, alcohol, cigarette, use of contraceptives, previous history of depression, etc
Patients Health Questionnaire (PHQ-9)
The PHQ-9 is a self-reported questionnaire that consists of 9-items. Each question is scored 0-3 (0=not at all, 1=several days, 2=more than half the day, and 3=nearly every day). The least score is 0 while the highest is 27. The items reflect the DSM- IV criteria for major depressive disorder.
World Health Organization Quality of Life- BREF
Quality of life was assessed using the WHOQOL-Brief version, which was a 26-item self-administered questionnaire; a short version of the WHOQOL-100 scale.11 It has four domains and twenty-six items that are scored on a 5-point Likert scale. The four domains are; Physical health (7 items), Psychological health (6 items), social relationship (3 items), and Environment (8 items). Domain scores are scaled in a positive direction (i.e. higher scores denote a higher quality of life). The mean score of items within each domain is used to calculate the domain score. Mean scores are then multiplied by 4 to make domain scores comparable to the scores used in the WHOQOL-100, and subsequently transformed to a 0-100 scale, using the formula:
Transformed score = (SCORE – 4) x (100 16)
A method for the manual calculation of individual scores is below:
Physical domain = ((6-Q3) + (6-Q4) + Q10 + Q15 + Q16 + Q17 + Q18) x 4.
Psychological domain = (Q5 + Q6 + Q7 + Q11 + Q19 + (6-Q26)) x 4.
Social Relationships domain = (Q20 + Q21 + Q22) x 4.
Environment domain = (Q8 + Q9 + Q12 + Q13 + Q14 + Q23 + Q24 + Q25) x 4
The remaining two items assess individuals’ overall rating of the quality of Life (QOL) and subjective satisfaction with health and are not included in the domains but are used to form one facet of overall QOL and general health. Higher scores indicate better quality of life. Although the WHOQOL-BREF should be self-administered, interviewer-assisted, or interviewer-administered forms may be used if respondents have an insufficient reading ability.
Sampling
A systematic random sampling method was used in this study. From the record, the total population of women attending the outpatient clinic for breast cancer was 102. The sampling interval was 2.
The sampling frame for each clinic day was the total number of patients that presented in order of arrival. The first respondent was selected through random balloting of folded pieces of paper bearing the serial number of each patient in a jar. Subsequent respondents were recruited by an interval of 2.
The study was conducted on clinic days for women with breast cancer. Proper orientation and introduction about the study were given then the consent form was signed. Vital signs were taken with clinical assessments. The respondents were recruited from the GOPD of the same hospital. CDC symptoms of breast cancer were used to screen respondent. For each woman with breast cancer, 2 women without breast cancer were age-matched (+ or -3yrs) for control. Questionnaires were administered to capture the sociodemographic characteristic, PHQ and QoL. Participants were only identified by serial number on each questionnaire and utmost confidentiality was ensured.
Data Analysis
Data were analyzed using the statistical package for social sciences (SPSS version 21) computer software. The raw scores for each domain of WHOQOL-BREF were converted to transformed scores ranging from 0-100. The prevalence of depressive symptoms PHQ clinical interview were presented categorically using frequency figures, and percentages. The association between quality of life and depression were analyzed using an independent t-test and analysis of variance (ANOVA). The confidence level for all the tests will be set at 95%. A p-value of less than 0.05 was taken as statistically significant.
Ethical Approval
Ethical clearance was obtained from the Ethical Research Committee of LAUTECH Teaching Hospital, Ogbomoso Oyo State Nigeria.
Result
A total of 240 questionnaires were administered, 222 questionnaires were retrieved which yielded a response rate of 93%. Of the 222 respondents, 70 were women with breast cancer while 152 were age-matched women with no breast cancer. There were more respondents without breast cancer who were single (32.9%) compared to respondents with breast cancer (15.7%) while married respondents were more among respondents with breast cancer (70.0%) compared to the other group (61.2%), p-value = 0.022. There were more educated respondents among women without breast cancer. 60.5% of these respondents had a tertiary level of education compared to 42.9% among women with breast cancer, p-value = 0.014. There were more unemployed respondents among women without breast cancer (32.2%) than the other group (17.1%), p-value = 0.019. (Table I)
Table I: Socio-Demographic characteristics of subjects
| Variables | Control | Cases | X2 | Df | ρ-value |
| (n = 152) | (n = 70) | ||||
| Age (years) | |||||
| 20 – 29 | 34 (22.4) | 16 (22.8) | |||
| 30 – 39 | 43 (28.3) | 17 (24.3) | |||
| 40 – 49 | 35 (23.0) | 19 (27.1) | 0.8268 | 4 | 0.9348 |
| 50 – 59 | 22 (14.5) | 9 (12.9) | |||
| 60 – 69 | 18 (11.8) | 9 (12.9) | |||
| Mean ± SD | 38.3 ± 11.2 | 35.2 ± 8.6 | |||
| Marital status | |||||
| Single | 50 (32.9) | 11 (15.7) | |||
| Married | 92 (61.2) | 49 (70.0) | |||
| Divorced | 3 (2.0) | 2 (2.9) | 11.474 | 4 | 0.022* |
| Separated | 4 (2.6) | 3 (4.3) | |||
| Widow | 2 (1.3) | 5 (7.1) | |||
| Level of education | |||||
| No education | 8 (5.3) | 12 (17.1) | |||
| Primary | 19 (12.5) | 10 (14.3) | |||
| Secondary | 33 (21.7) | 18 (25.7) | 10.682 | 3 | 0.014* |
| Tertiary | 92 (60.5) | 27 (42.9) | |||
| Employment status | |||||
| Employed | 103 (67.8) | 57 (82.9) | 5.48 | 1 | 0.019* |
| Un-employed | 49 (32.2) | 12 (17.1) | |||
| Religion | |||||
| Christianity | 101 (67.3) | 55 (78.6) | |||
| Islam | 50 (32.9) | 15 (21.4) | 3.615 | 2 | 0.164 |
| Others | 1 (0.7) | 0 (0.0) | |||
| Average monthly income (naira) | |||||
| Below 50,000 | |||||
| 50,000 – 99,000 | 65 (42.8) | 28 (40.0) | |||
| 100,000 – 149,000 | 21 (13.8) | 9 (12.9) | |||
| 150,000 – 199,000 | 7 (4.6) | 7 (10.0) | 6.048 | 4 | 0.196 |
| 200,000 and above | 2 (1.3) | 0 (0.0) | |||
| No response | 6 (3.9) | 0 (0.0) | |||
| 51 (33.6) | 26 (37.1) |
X2: Chi-square statistics, df: the degree of freedom, p- value < 0.05 indicates significance
Using PHQ-9, 34.3% had major depression while 38.6% had minor depression and 27.1% were not depressed (Figure 1).
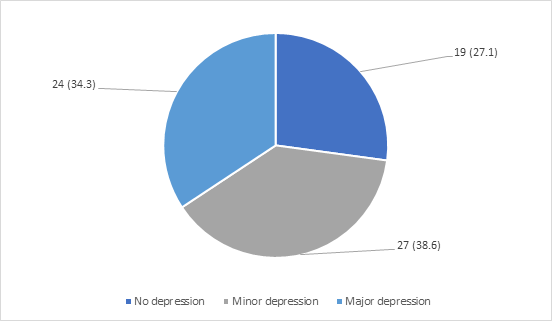
Figure I: Prevalence of Depressive Symptoms Among Women With Breast Cancer
The mean and standard deviation of the raw and transformed scores in each of the four domains (physical, psychological, social, and environmental) and the 2 facets; overall quality of life and general satisfaction with the health of the WHOQOL-BREF questionnaire are presented below.
Physical domain: The possible raw score range is 7-35. The mean raw score was 12.21±1.81 and the transformed was 57.7±12.2 when transformed to 0-100 scores.
Psychological domain: The possible raw score range is 6-30. The mean raw score was 12.66±1.96 and the transformed score was 56.9±13.9 when converted to 0-100 scores.
Social domain: The possible raw score range is 3-15. The mean raw score was 13.10±2.53 and the transformed score was 50.5±15.5 when transformed to 0-100.
Environmental domain: The possible raw score range is 8-40. The mean raw score was 12.54± 2.01 and the transformed score was 60.4±10.1 when converted to 0-100.
Overall Quality of Life: The possible raw score range is 1-5. The mean raw score was 3.47±0.75.
General satisfaction with health: The possible raw score range is 1-5. The mean raw score was 3.17±0.81.
Table II: Raw and Transformed Mean Scores in all the Four Domains and Two Facets of WHOQOL-BREF Among Respondents With Breast Cancer.
| Domains | Raw scores Mean±SD | Transformed scores (0-100) Mean±SD |
| Physical | 12.21±1.81 | 57.7±12.2 |
| Psychological | 12.66±1.96 | 56.9±13.9 |
| Social | 13.1±2.53 | 50.5±15.5 |
| Environmental | 12.54±2.01 | 60.4±10.1 |
| Overall QoL | 3.47±0.75 | |
| General Health | 3.17±0.81 |
Table III shows the QOL in respect to different levels of depressive symptoms among women with breast cancer. Quality of life scores across domains was compared among respondents who had no depression, minor, and major depression.
Physical domain scores decreased significantly from no depression (64.7 ± 11.1) to minor depression (58.9 ± 12.2) and major depression (50.5 ± 9.3), F = 9.062, ρ-value = 0.001.
Also, social domain scores were significantly higher among women with no depression (58.5 ± 16.0), compared to minor depression (51.7 ± 15.9) and major depression (43.0 ± 11.0), F = 6.176, ρ-value = 0.003.
Table III: Levels of Depression and Quality of Life Among Women with Breast Cancer
| Domain score | |||||
| Mean ± SD | No Depression | Minor depression | Major depression | F | p-value |
| Physical
Psychological Social Environmental |
64.7 ± 11.1
62.6 ± 12.7 58.5 ± 16.0 61.6 ± 10.3 |
58.9 ± 12.2
57.0 ± 14.8 51.7 ± 15.9 60.2 ± 10.3 |
50.5 ± 9.3
52.4 ± 12.4 43.0 ± 11.0 59.5 ± 10.1 |
9.062
3.070 6.176 0.221 |
0.001*
0.053 0.003* 0.803 |
F: F statistic, ρ-value < 0.05 indicates significance
Table IV shows the comparison of quality of life scores across domains among women with breast cancer with MDD and those without MDD. The mean scores for the physical domain were significantly lower among women with MDD compared (46.25 ± 7.12) to women without MDD (59.12 ± 12.01), t = -2.955, ρ-value = 0.004.
Table IV: Relationship between Quality of Life of Women With Breast Cancer by Major Depressive Disorder
| Domain score | Major Depressive Disorder | |||
| Mean ± SD | Yes (n = 8) | No (n = 62) | t-statistic | p-value |
| Physical
Psychological Social Environmental |
46.25 ± 7.12
50.75 ± 11.32 40.63 ± 10.11 57.13 ± 7.21 |
59.12 ± 12.01
57.75 ± 14.05 51.82 ± 15.71 60.77 ± 10.41 |
-2.955
-1.352 -1.975 -0.959 |
0.004*
0.181 0.055 0.341 |
t: t statistic, ρ-value < 0.05 indicates significance
From table VI, the physical domain scores were significantly higher among those that were employed (59.7 ± 11.3) compared to the unemployed (53.3 ± 11.9), F = 11.499, ρ-value = 0.001.
Table V: Association Between Physical Domain Scores and Socio-Demographic Characteristics of Respondents With Breast Cancer
| Variables | Mean ± SD | F | p-value |
| Age (years) | |||
| 30 – 39 | 59.7 ± 7.2 | ||
| 40 – 49 | 56.3 ± 13.0 | 1.621 | 0.18 |
| 50 – 59 | 62.1 ± 13.2 | ||
| 60 – 69 | 47.6 ± 12.3 | ||
| Marital status | |||
| Single | 56.8 ± 7.6 | ||
| Married | 58.4 ± 13.7 | 1.046 | 0.391 |
| Divorced | 69.0 ± 3.7 | ||
| Separated | 54.0 ± 3.5 | ||
| Widow | 50.0 ± 6.0 | ||
| Level of education | |||
| No education | 55.2 ± 10.1 | ||
| Primary | 50.7 ± 12.2 | 1.823 | 0.151 |
| Secondary | 58.8 ± 14.8 | ||
| Tertiary | 60.3 ± 10.6 | ||
| Employment status | |||
| Employed | 59.7 ± 11.3 | 11.499 | 0.001* |
| Un-employed | 47.5 ± 11.9 | ||
| Religion | |||
| Christianity | 58.8 ± 12.4 | 2.434 | 0.123 |
| Islam | 53.3 ± 10.8 | ||
| Average monthly income (naira) | |||
| Below 50,000 | 57.2 ± 9.1 | ||
| 50,000 – 99,000 | 64.1 ± 14.6 | 1.402 | 0.25 |
| 100,000 – 149,000 | 60.7 ± 7.1 |
F: F statistics, p-value < 0.05 indicates significance
From table VI, the psychological domain scores among women with breast cancer was significantly higher among those that were employed (58.7 ± 13.2) compared to the unemployed (48.5 ± 14.4), F = 5.748, ρ-value = 0.019.
Table VI: Association Between Psychological Domain Scores and Socio-Demographic Characteristics of Respondents
| Variables | Mean ± SD | F | p-value |
| Age (years) | |||
| 30 – 39 | 53.8 ± 8.4 | ||
| 40 – 49 | 59.1 ± 14.6 | 1.135 | 0.348 |
| 50 – 59 | 58.9 ± 16.7 | ||
| 60 – 69 | 47.4 ± 10.4 | ||
| Marital status | |||
| Single | 54.6 ± 15.4 | ||
| Married | 57.6 ± 13.8 | 0.839 | 0.505 |
| Divorced | 62.5 ± 9.2 | ||
| Separated | 64.7 ± 9.6 | ||
| Widow | 48.8 ± 14.3 | ||
| Level of education | |||
| No education | 53.1 ± 11.5 | ||
| Primary | 50.1 ± 12.8 | 2.251 | 0.091 |
| Secondary | 56.0 ± 14.4 | ||
| Tertiary | 61.3 ± 13.9 | ||
| Employment status | |||
| Employed | 58.7 ± 13.2 | 5.748 | 0.019* |
| Un-employed | 48.5 ± 14.4 | ||
| Religion | |||
| Christianity | 57.2 ± 14.7 | 0.103 | 0.75 |
| Islam | 55.9 ± 10.5 | ||
| Average monthly income (naira) | |||
| Below 50,000 | 57.8 ± 10.1 | ||
| 50,000 – 99,000 | 58.8 ± 17.6 | 1.402 | 0.25 |
| 100,000 – 149,000 | 63.4 ± 12.2 |
F: F statistics, ρ-value < 0.05 indicates significance
Table VII shows a statistical difference in social domain scores across marital status with a higher quality of life scores among married (52.6 ± 14.9), divorced (72.0 ± 4.2) and separated respondents (58.3 ± 9.7) compared to single respondents (38.0 ± 12.3), F = 3.844, ρ-value = 0.007.
Table VII: Association Between Social Domain Scores and Socio-Demographic Characteristics of Respondents
| Variables | Mean ± SD | F | p-value |
| Age (years) | |||
| 30 – 39 | 49.1 ± 12.1 | ||
| 40 – 49 | 52.2 ± 16.9 | 0.492 | 0.742 |
| 50 – 59 | 51.2 ± 17.8 | ||
| 60 – 69 | 42.6 ± 7.0 | ||
| Marital status | |||
| Single | 38.0 ± 12.3 | ||
| Married | 52.6 ± 14.9 | 3.844 | 0.007* |
| Divorced | 72.0 ± 4.2 | ||
| Separated | 58.3 ± 9.7 | ||
| Widow | 45.0 ± 15.7 | ||
| Level of education | |||
| No education | 50.4 ± 14.1 | ||
| Primary | 48.8 ± 19.1 | 0.08 | 0.971 |
| Secondary | 50.1 ± 14.8 | ||
| Tertiary | 51.4 ± 15.9 | ||
| Employment status | |||
| Employed | 51.6 ± 16.2 | 1.159 | 0.212 |
| Un-employed | 45.4 ± 10.7 | ||
| Religion | |||
| Christianity | 49.7 ± 16.3 | 0.836 | 0.364 |
| Islam | 53.8 ± 12.0 | ||
| Average monthly income (naira) | |||
| Below 50,000 | 50.0 ± 15.4 | ||
| 50,000 – 99,000 | 58.3 ± 17.8 | 1.17 | 0.328 |
| 100,000 – 149,000 | 53.6 ± 8.0 |
F: F statistics, ρ-value < 0.05 indicates significance
Table VIII shows that environmental domain scores were significantly higher among respondents with a higher level of education compared to those that had a lower level of education, 2.274, ρ-value = 0.048.
Table VIII: Association Between Environmental Domain Scores and Socio-Demographic Characteristics of Respondents
| Variables | Mean ± SD | F | ρ-value |
| Age (years) | |||
| 30 – 39 | 64.8 ± 10.4 | ||
| 40 – 49 | 60.3 ± 9.5 | 1.901 | 0.121 |
| 50 – 59 | 58.8 ± 10.3 | ||
| 60 – 69 | 51.4 ± 9.2 | ||
| Marital status | |||
| Single | 59.2 ± 7.8 | ||
| Married | 60.3 ± 11.0 | 0.595 | 0.668 |
| Divorced | 66.0 ± 4.2 | ||
| Separated | 67.0 ± 3.5 | ||
| Widow | 57.6 ± 8.3 | ||
| Level of education | |||
| No education | 56.3 ± 11.9 | ||
| Primary | 54.4 ± 6.0 | 2.774 | 0.048* |
| Secondary | 62.7 ± 10.5 | ||
| Tertiary | 62.6 ± 9.3 | ||
| Employment status | |||
| Employed | 60.9 ± 10.1 | 1.226 | 0.272 |
| Un-employed | 57.4 ± 9.9 | ||
| Religion | |||
| Christianity | 60.6 ± 10.6 | 0.193 | 0.662 |
| Islam | 59.3 ± 8.3 | ||
| Average monthly income (naira) | |||
| Below 50,000 | 58.8 ± 10.3 | ||
| 50,000 – 99,000 | 65.4 ± 7.7 | 2.422 | 0.074 |
| 100,000 – 149,000 | 67.0 ± 10.7 |
F: F statistics, ρ-value < 0.05 indicates significance
Discussion
This study compared Major Depressive Disorder and QOL in respondents with breast cancer and age-matched women without breast cancer. In this study, the age range of women with breast cancer was 29-65 years and the majority of the respondents with breast cancer were married.
In this study, women with breast cancer had significantly lower mean scores in all the domains of quality of life (WHOQOL-BREF) except for the environmental domain. This is consistent with the study by Kluthiovsky et al. Using WHOQOL-BREF, the study assessed the quality of life among 202 breast cancer survivors and compared it with age-matched women with no cancer history attending a primary care centre12. He found that survivors of breast cancer experienced a poorer quality of life in the physical, psychological and social domains than the comparison group. No significant difference was observed in the environmental domain.
This finding was similar to findings by De Ligt et al and Lee ES et al13,14. Both studies assessed the health-related quality of life of breast cancer survivors using EORTIC instrument and compared to a healthy population. Respondents with breast cancer had lower mean scores. De Ligt et al reported significantly lower mean scores for the role, cognitive, emotional, and social functioning than the control. Whereas Ahn et al in a similar study found a significant difference in areas of cognitive and social functioning15.
Mohd et al in a comparative study of quality of life among women with breast cancer and healthy women in Malaysia using EORTIC instrument reported a contrasting finding16. He found out that quality of life was comparable between the 2 groups. This was seen especially in women with breast cancer who had survived more than 5 years. Similarly, Lena et al in a study of long-term breast cancer survivors found that general health and overall quality of life were comparable to the general population17.
One possible explanation for the similarity in the quality of life between women with breast cancer and the comparison group without a history of breast cancer might be that breast cancer is a chronic disease and therefore women over time might develop the coping skill to alleviate its impact in different areas of life. In Lena et al study, respondents with breast cancer had survived the disease for 10 years and thus the effects might not be as such as seen in the early years of the disease. In this study, however, the majority of breast cancer respondents were still within the first 5 years of the disease and thus would not have developed the resilience to minimize the impact of the disease on their lives, hence the lower quality of life compared to healthy women.
Moreover, this study found that depressive symptoms and major depressive disorder were commoner in women with breast cancer compared to age-matched women without a history of breast cancer. 11.42% of respondents with breast cancer had major depressive disorder compared to 1.97% in age-matched control.
This finding is in line with reports by Hartung et al in a study on depression among breast cancer patients and the general population using PHQ instrument18. He found that the risk of being depressed among cancer patients was more than 5 times higher than in the general population. This is also consistent with previous studies by Nicholas et al and Fafouti et al19,20. Nicholas et al who reported that the prevalence of depressive symptoms was higher among breast cancer respondents than among the general female population.
This study also assessed the relationship between Major Depressive Disorder and Quality of life. Respondents with breast cancer who had Major Depressive Disorder had lower mean scores in physical, psychological, social, and environmental domains compared to those without Major Depressive Disorder. It was significantly lower for the physical domain. Women with breast cancer experience debilitating physical symptoms such as loss of appetite, nausea, bone pain, loss of libido, hair loss, weight loss, etc. This could stem from either the disease condition or side effects of the treatment (chemotherapy and radiotherapy). The aftermath of this on their functioning in daily activities might add more to their emotional burden.
This is consistent with a similar study by Debasweta et al who found that women with breast cancer who had depression experienced poorer quality of life in all domains than those without depression using WHOQOL-BREF and PHQ-9 for assessment of the quality of life and depression respectively21. Also, Francisco et al in a study of depression and QOL among 45 women with breast cancer receiving chemotherapy and monoclonal antibodies using HADS and EORTIC questionnaires reported that patients with breast cancer and depressive symptoms receiving these treatments had an appreciably lower Qol compared to patients without depression22.
Moreso, women with breast cancer who have depression might develop apathy to the disease and the treatment and in the light of hopelessness could decide not to comply with the treatments and other precautions or advice. This might worsen the disease condition and further compromise their quality of life, thus running a vicious cycle. Yen et al23 reported that although depression was significantly associated with QOL in both groups, the malignant group had poorer physical and psychological QOL.
Conclusion
This study showed that for the malignant group, the significant predictor for QOL is the stress from the disease condition. Breast malignancy is more virulent than benign breast lesions in that it has a propensity of spreading to other organs of the body causing higher physical and psychological distress. Women with breast cancer had significantly lower mean scores in all the domains of quality of life except for the environmental domain. Also, respondents with breast cancer who had Major Depressive Disorder had lower mean scores in QoL domains compared to those without Major Depressive Disorder. The role of psychological assessment in the management of breast malignancies is hereby advocated to improve the quality of life and treatment outcomes.
Conflict of Interest
The authors declared no conflict of interest
Funding
This work was solely funded by the authors
Acknowledgement
My profound gratitude to God almighty for making this work a successful one. I thank all my co-authors for their tireless efforts and meaningful contributions. To all staff members of the departments of surgery and psychiatry LAUTECH Ogbomoso, I say thank you all.
References
- Ell K, Sanchez K, Vourlekis B, Lee PJ, Dwight-Johnson M, Lagomasino I, et al. Depression, correlates of depression, and receipt of depression care among low-income women with breast or gynecologic cancer. Vol. 23, Journal of Clinical Oncology. 2005. p. 3052–60.
- Jafari A, Goudarzian AH, Nesami MB. Depression in women with breast cancer: A systematic review of cross-sectional studies in Iran. Asian Pacific Journal of Cancer Prevention. 2018;19(1):1–7.
- Theofilou P. Quality of life: Definition and measurement. Eur J Psychol. 2013;9(1):150–62.
- PENSON RT, WENZEL LB, VERGOTE I, CELLA D. Quality of Life Considerations in Gynecologic Cancer. Vol. 95, International Journal of Gynecology and Obstetrics. 2006.
- Ferrell BR, Hassey Dow K. Quality of life among long-term cancer survivors. Vol. 11, Oncology. 1997. p. 565–8.
- Velikova G, Awad N, Coles-Gale R, EP W, JM B, PJ S. The clinical value of quality of life assessment in oncology practice–a qualitative study of patient and physician views. Vol. 17, Psycho-Oncology. 2008. p. 690-698 9p.
- Begovic-Juhant A, Chmielewski A, Iwuagwu S, Chapman L. Impact Of Body Image on Depression and Quality of Life Among Women with Breast Cancer. Vol. 30, Journal of Psychosocial Oncology. 2012.
- Ardebil MD, Bouzari Z, Shenas MH, Keighobadi M. Depression and health related quality of life in breast cancer patients. J Pak Med Assoc. 2013;63(1):69–71.
- Purkayastha D, Venkateswaran C, Nayar K, Unnikrishnan UG. Prevalence of Depression in Breast Cancer Patients and its Association with their Quality of Life: A Cross-sectional Observational Study. Indian J Palliat Care. 2017;23(3):268–73.
- Wang H, Chow SC. Sample Size Calculation for Comparing Proportions. In: Wiley Encyclopedia of Clinical Trials. 2007.
- Skevington SM, Lotfy M, O’Connell KA. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. Vol. 38, European Science Editing. 2012. p. 35–7.
- Kluthcovsky ACGC, Urbanetz AA. Fatigue and quality of life in breast cancer survivors: a comparative study. Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(3):119–26.
- de Ligt KM, Heins M, Verloop J, Ezendam NPM, Smorenburg CH, Korevaar JC, et al. The impact of health symptoms on health-related quality of life in early-stage breast cancer survivors. Breast Cancer Res Treat. 2019;178(3):703–11.
- Lee ES, Lee MK, Kim SH, Ro JS, Kang HS, Kim SW, et al. Health-related quality of life in survivors with breast cancer 1 year after diagnosis compared with the general population: A prospective cohort study. Ann Surg. 2011;253(1):101–8.
- Ahn SH, Park BW, Noh DY, Nam SJ, Lee ES, Lee MK, et al. Health-related quality of life in disease-free survivors of breast cancer with the general population. Annals of Oncology. 2007;18(1):173–82.
- Hashim HSM, Lim C, Junazli NI, Choo SL, Low KY, Munisamy M. Is the Quality of Life in Breast Cancer Survivors the Same as Healthy Women? A Case Control Study Among Women in Klang Valley, Malaysia. J Glob Oncol. 2018;4(Supplement 2):103s–103s.
- Koch L, Jansen L, Herrmann A, Stegmaier C, Holleczek B, Singer S, et al. Quality of life in long-term breast cancer survivors-a 10-year longitudinal population-based study. Acta Oncol (Madr). 2013;52(6):1119–28.
- Hartung TJ, Fried EI, Mehnert A, Hinz A, Vehling S. Frequency and network analysis of depressive symptoms in patients with cancer compared to the general population. J Affect Disord. 2019;256:295–301.
- Maass SWMC, Roorda C, Berendsen AJ, Verhaak PFM, De Bock GH. The prevalence of long-term symptoms of depression and anxiety after breast cancer treatment: A systematic review. Vol. 82, Maturitas. 2015. p. 100–8.
- Fafouti M, Paparrigopoulos T, Zervas Y, Rabavilas A, Malamos N, Liappas I, et al. Depression, anxiety and general psychopathology in breast cancer patients: A cross-sectional control study. In Vivo (Brooklyn). 2010;24(5):803–10.
- Purkayastha D, Venkateswaran C, Nayar K, Unnikrishnan U. Prevalence of Depression in Breast Cancer Patients and its Association with. Indian J Palliat Care. 2017;23(3):268–73.
- Trinca F, Infante P, Dinis R, Inácio M, Bravo E, Caravana J, et al. Depression and quality of life in patients with breast cancer undergoing chemotherapy and monoclonal antibodies. Ecancermedicalscience. 2019;13.
- Yen JY, Ko CH, Yen CF, Yang MJ, Wu CY, Juan CH, et al. Quality of life, depression, and stress in breast cancer women outpatients receiving active therapy in Taiwan. Psychiatry Clin Neurosci. 2006;60(2):147–53.