
Strengthening Evidence-Based Practice in Malaysia: Improving the Public Cpr Awareness Time Model for Self- Vital Monitoring
- Y. Surahaya Mohd Yusof
- Dr. Noor Hanita Binti Zaini
- Nor Aziyan Binti Yahaya
- Nurhan Norris Ma Weng Chuen
- 2476-2501
- Mar 10, 2025
- Healthcare Management
Strengthening Evidence-Based Practice in Malaysia: Improving the Public CPR Awareness Time Model for Self- Vital Monitoring
1Y. Surahaya Mohd Yusof, 2Dr. Noor Hanita Binti Zaini, 3Nor Aziyan Binti Yahaya, 4Nurhan Norris Ma Weng Chuen
1Faculty of Technology and Applied Sciences Open University Malaysia (OUM), Malaysia
2Senior Lecturer, Department of Nursing Science, Faculty of Medicine, University of Malaya
3Department of Nursing Science, Faculty of Medicine, University of Malaya Malaysia.
4Kingdom Saudi Arabia, 2025
*Corresponding Author
DOI: https://dx.doi.org/10.47772/IJRISS.2025.9020194
Received: 21 December 2024; Revised: 03 January 2025; Accepted: 07 January 2025; Published: 10 March 2025
ABSTRACT
Cardiac arrest is a significant global health issue, with over 20,000 paediatric cases annually in the United States (AHA, 2020), and in Malaysia, coronary heart disease affects approximately 29,363 individuals each year, contributing heavily to national health concerns (Ministry of Health Malaysia, 2021). To address this challenge, this study aims to strengthen evidence-based practice (EBP) in Malaysia through the integration of the TIME model (Transform, Innovate, Model, Enhancement) for cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring, particularly focusing on pulse monitoring and perfusion index (PI) as essential components of patient care. Utilizing a mixed-methods approach, this research is grounded in the American Nurses Association’s (ANA, 2024) EBP model. The primary objectives of the study are: (1) to assess the factors influencing the implementation of various CPR practices and public health monitoring awareness, (2) to analyse the relationship between CPR approaches and public health monitoring awareness through statistical regression analysis, and (3) to develop an EBP practice guide for strategic CPR awareness. A comprehensive literature review utilizing databases such as OUM e-library, Science Direct, AHA, and ResearchGate provided insights from over 150 relevant sources. A mixed-methods design was applied, including quantitative data from surveys and qualitative data from open-ended questionnaires, with a sample of 200 final-year nursing students. Findings will inform the development of a recommended EBP model enhancement and strategic CPR guidelines, culminating in an eBook for cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring 2025-2030. The TIME model’s application in this context serves as a transformative and innovative framework that fosters best practices in CPR training and enhances public health awareness, on collaboration, patient-centred care, and the sustainability of health outcomes in Malaysia. focusing of Pulse Self-Monitoring for Public Awareness and CPR Readiness in Malaysia.
Keywords: Evidence Based Practice (EBP), TIME model (Transformation, Innovation, Model Enhancement), DRCAB (Danger-Response-Circulation-Airway-Breathing) with ROSC-EFG (Return of Spontaneous Circulation) E- Evaluate Investigation (ECG, X-ray, Blood check, Fluid, Glucose)-F-Find the cause-G-Guideline and recovery protocols).
INTRODUCTION
Background and Rationale
Trend of heart disease continues to pose a significant global public health challenge, with its impact acutely felt in Malaysia, where ischemic heart diseases remain the leading cause of mortality. Cardiac arrest occurs in >20 000 children annually in the United States AHA, (2020). In Malaysia, coronary heart disease significantly contributes to national health concerns, affecting approximately 29,363 individuals annually. According to the Malaysia Ministry of Health (2021), coronary heart disease accounted for 17.0% of medically certified deaths in 2020.
According to CDC in 2022 figure 1 resulted 2022, 702,880 people died from heart disease. That’s the equivalent of 1 in every 5 deaths. Heart disease cost about $252.2 billion from 2019 to 2020. This includes the cost of health care services, medicines, and lost productivity due to death.
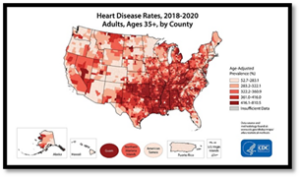
Figure 1: Heart Disease Death Rates, 2018–2020 for Adults, Ages 35+, by County.
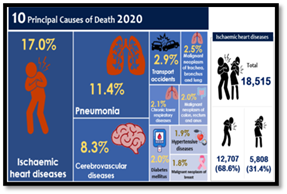
Figure 2: Malaysia heart disease data 2020
The Course and Burden of Disease
Cardiovascular diseases (CVDs) rank as a leading cause of death globally, with the World Health Organization (WHO) reporting that 17.9 million people died from CVDs in 2020.
Pulse Oximetry and the Perfusion Index
Understanding the role of pulse oximetry in monitoring cardiovascular health is also pivotal in enhancing cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring outcomes. This non-invasive measure of peripheral perfusion serves as a good indicator of pulse strength or blood flow. The normal range for PI varies from 0.02% to 20%, but there is no universally accepted “normal” value, making it critical for users to establish baseline measurements and monitor changes over time.
Research Issues
Learners frequently struggle with various resuscitation models, such as the AHA (2020) CAB (Circulation, Airway, Breathing), Bruinink et al. (2024) ABCDE (Airway, Breathing, Circulation, Disability, Exposure), Malaysia’s KKM (2023) DRSABCD, and European (2025) approaches. This conceptual confusion can lead to difficulties in selecting the appropriate method for specific clinical situations, potentially affecting cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring outcomes Kleinman & Brady in 2020.
A significant challenge is resistance to change. Many learners, having been trained in traditional resuscitation methods, often exhibit reluctance to adopt newer protocols. This resistance creates tension between learners and trainers advocating for updated practices, thereby hindering advancements in resuscitation education (Perkins & Olasveengen, 2021).
These challenges emphasize the complexity of resuscitation education and highlight the need for strategies that enhance conceptual understanding, adaptability, and practical application among learners. Addressing these barriers is essential to improving CPR competency and ensuring high-quality patient care.
Feasibility of the Study Based on Expected Research Outcomes
The feasibility of this study is supported by the robust theoretical framework, the practical applicability of the research questions, and the alignment with existing evidence and guidelines.
Purpose
This approach enhances EBP TIME model of CPRS in CPR practice toward survival rates, cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring, and standardized training for healthcare providers in emergencies.
Justification
Why?
- Enhancing Survival Rates in Cardiac Arrest Cases
- Rationale: Quick CPR initiation improves survival, but public response time remains a challenge. A structured awareness model ensures faster intervention, reducing out-of-hospital cardiac arrest (OHCA) mortality.
- Bridging the Gap in Bystander CPR Knowledge
- Rationale: Many Malaysians lack CPR skills or hesitate to act in emergencies. A targeted model educates and empowers the public, increasing CPR application rates by assessing own monitoring.
- Promoting Early Recognition of Cardiac Emergencies
Rationale: Many sudden cardiac deaths occur due to delayed recognition of distress signs. Integrating self-vital monitoring encourages proactive health management and earlier CPR initiation
Research Objectives
The primary objectives of this research are:
- To assess the factors influencing the implementation of diverse CPR practices and public awareness for vital selfcare monitoring
- To analyse the relationship between CPR approaches and public health monitoring awareness through statistical regression analysis.
- To design best EBP practice guide meet to the study process and strategic plan of cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring.
Terms and Definitions
Cardiopulmonary Resuscitation (CPR) is a lifesaving technique used during cardiac or respiratory arrest to restore vital functions (Kleinman et al., 2020). The CAB (Circulation, Airway, Breathing) method prioritizes circulation before airway and breathing, emphasizing early chest compressions. The ABCDE (Airway, Breathing, Circulation, Disability, Exposure) for identifying issues and tracking patient responses (Kleinman et al., 2020).
LITERATURE REVIEW
Theoretical model

Figure 3: EBP – CPR by America Nurse Association (ANA, 2024)
Evidence-Based Practice (EBP): The Three Pillars
Evidence-Based Practice (EBP) in nursing is built on three interconnected pillars: clinical expertise, patient values and preferences, and the best available research evidence.
Clinical Expertise
Clinical expertise is the cornerstone of EBP. It enables nurses to draw upon their judgment, experience, and specialized knowledge to deliver patient-centered care.
Patient Values and Preferences
Zhang and Chen (2022) reviewed influencing factors in end-of-life care decisions, identifying patient values as pivotal in tailoring resuscitation strategies and improving the decision-making process, but also fosters a culture of continuous learning and improvement in healthcare settings.
Enhancing Evidence-Based Practice TIME Model in Malaysia: Integrating CPR for Vital Indicators Public Awareness
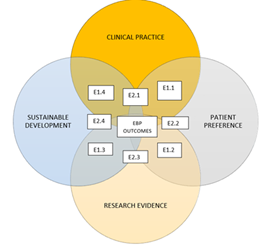
Figure 4: Enhance EBP-CPRS model of Public Awareness on CPR for Monitoring Vital Indicators (2025) adapted EBP – CPR by America Nurse Association (ANA, 2024) refer appendix 8.
Definition and Operational Definition of model
The TIME model (Transformation, Innovation, Monitoring, and Evaluation) is an advanced framework designed to enhance evidence-based practices (EBP) by promoting innovation, accountability, and measurable outcomes. Xu and Zhou (2016) highlighted that successful resuscitation outcomes require systematic and innovative approaches that integrate clinical expertise with patient-centered care. The operational definition of TIME in this context involves enhancing EBP toward cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring programs within Malaysia’s public health landscape to address knowledge gaps in vital sign monitoring and emergency response.
Model Aim and Purpose
The aim of this study is to assess the effectiveness of implementing the TIME model in enhancing public awareness and skills in CPR for vital indicators. The purpose is to establish a sustainable model that aligns with evidence-based practice principles while addressing the Sustainable Development Goals (SDG) as recommended, particularly SDG 3: Good Health and Well-being. Yadav and Mishra (2021) emphasized the ethical challenges in South Asia concerning CPR decision-making, underlining the need for culturally responsive public education initiatives.
Model and Justification
There is a pressing need for innovative frameworks TIME model to strengthen of EBP practice toward improve awareness among people in self-monitoring in their survival of cardiac in Malaysia. As highlighted by Zhao et al. (2020), early awareness, defibrillation and CPR significantly impact survival rates. However, limited awareness and training among the general public impede timely intervention. Integrating TIME into public health strategies can bridge these gaps by promoting evidence-based education and practice.
Model and Feasibility
Implementing the TIME model in Malaysia is feasible due to advancements in digital health technologies and increasing public interest in health education. Zhan et al. (2018) demonstrated that structured, evidence-based frameworks lead to better decision-making in critical care scenarios. Additionally, leveraging partnerships with healthcare institutions and NGOs can ensure resource optimization and widespread reach.
Innovation and Adaptation Phase
Integrating innovative strategies, such as AI, enhances cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring relevance. Zhao et al. (2020) point out that personalised AI recommendations improve skill development and accessibility. Reviewing existing protocols, as outlined by Holcomb (2019), ensures the adoption of evidence-based methods while discontinuing ineffective ones, fostering streamlined and effective practices.
RESEARCH METHODOLOGY
Research Design
Explanation of Mixed-Methods Approach Justification for Using Mixed Methods
Using both qualitative and quantitative methods provides a comprehensive understanding of the research problem by combining statistical analysis with in-depth personal experiences. This mixed-methods approach leverages the complementary strengths of each methodology, with quantitative methods offering generalizability through numerical data and qualitative methods providing context and deeper insights through cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring studies.
Research Sampling
For this study, the participants will consist of final-year secondary school students. To determine the appropriate sample size, a sample of 200 students will be selected based on the Krejcie & Morgan (1970) Table, which is widely used to calculate the ideal sample size for a given population. The table provides a straightforward method for determining sample size, ensuring that the sample accurately represents the population and that the results can be generalized of cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring.
The Krejcie & Morgan (1970) table is valuable for empirical research the population size, providing a reliable guideline for selecting an appropriate sample. For this cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring study, based on the total population of final-year secondary school students, the table suggests a sample size of 200, which ensures a statistically significant representation without being overly large, making data collection and analysis more manageable cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring.
A pilot study will be conducted prior to the main study to assess the feasibility and reliability of the survey instruments. This will help identify potential issues with the study design, enabling necessary adjustments before the full-scale research is conducted. The pilot study will involve a smaller sample, and its results will provide insights into the validity of the research cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring methodology.
Data Collection Procedures
The data collection process will follow a structured protocol to ensure consistency and reliability. For the qualitative data, participants will first be invited to complete a consent form, ensuring that they understand the purpose and nature of the study. Following consent, semi-structured interviews will be conducted either in person or remotely, depending on the participant’s preference. Each interview will be recorded for transcription and analysis cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring.
The quantitative data will be collected through surveys administered to both healthcare providers and patients. The surveys will include standardized instruments for assessing QoL cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring, such as the and devices like pulse oximeters will be used to measure PPI. All data will be stored securely, with access limited to the research team.
Inclusion Criteria:
- Final-year secondary school students (aged 16-18 years).
- Currently enrolled and attending a secondary school in Malaysia.
- Ability to understand the language used in the study (Malay or English).
- Willingness to provide informed consent (or parental consent, if underage).
- Voluntary participation in the study.
Ethical Considerations
Ethical considerations are paramount in conducting research involving human participants.
- Informed Consent: All participants will be informed about the purpose of the study
- Confidentiality and Anonymity: Participants’ identities will be kept confidential, and all data
- Right to Withdraw: Participants will have the right to withdraw from the study at any time
- Data Protection: All data will be securely stored
PILOT DATA ANALYSIS AND RESULT

Figure 5: Data demographic of the study in pie chart.
Part A: Demographic Data
Table 1: Data Part A Demographic data analysis in table
| Question | Response | Sample Size (n=190) | Percentage |
| 1. Age | Under 20 | 90 | 47.4% |
| 21-30 | 15 | 7.9% | |
| 31-40 | 11 | 5.8% | |
| 41-50 | 25 | 13.2% | |
| 51-60 | 2 | 1.1% | |
| 61 and above | 0 | 0% | |
| 2. Gender | Male | 63 | 33% |
| Female | 127 | 67% | |
| Non-binary | 0 | 0% | |
| Prefer not to say | 0 | 0% | |
| 3. Marital Status | Single | 171 | 90% |
| Married | 10 | 5% | |
| Divorced | 0 | 0% | |
| Widowed | 0 | 0% | |
| 4. Highest Level of Education | Secondary School | 171 | 90% |
| Diploma | 0 | 0% | |
| Bachelor’s Degree | 0 | 0% | |
| Master’s Degree | 0 | 0% | |
| Doctorate | 0 | 0% | |
| Other | 19 | 10% | |
| 5. Occupation | Student | 190 | 100% |
| Employed (Full-time) | 0 | 0% | |
| Employed (Part-time) | 5 | 2.6% | |
| Self-employed | 0 | 0% | |
| Unemployed | 180 | 94.7% | |
| Retired | 5 | 2.6% | |
| 6. Current Residence | Urban area | 130 | 68.4% |
| Suburban area | 30 | 15.8% | |
| Rural area | 30 | 15.8% | |
| 7. Income Level (Monthly) | Less than RM 2,000 | 190 | 100% |
| RM 2,001 – RM 5,000 | 0 | 0% | |
| RM 5,001 – RM 8,000 | 0 | 0% | |
| RM 8,001 – RM 12,000 | 0 | 0% | |
| Above RM 12,000 | 0 | 0% | |
| Prefer not to say | 0 | 0% | |
| 8. Ethnicity | Malay | 100 | 52.6% |
| Chinese | 30 | 15.8% | |
| Indian | 25 | 13.2% | |
| Indigenous | 10 | 5.3% | |
| Other | 25 | 13.2% | |
| 9. Religious Affiliation | Islam | 139 | 73% |
| Christianity | 14 | 7% | |
| Hinduism | 21 | 11% | |
| Buddhism | 17 | 9% | |
| No religion | 0 | 0% | |
| Other | 0 | 0% | |
| 10. Do you have any chronic health conditions? | Yes | 4 | 2% |
| No | 186 | 98% |
The demographic data for the sample of 190 respondents is represented in the pie chart, showcasing the distribution of key characteristics. In terms of age, the majority of respondents fall within the age range of 30 to 39 years, accounting for 40% of the sample. Following this, 25% of participants are in the 40 to 49 years age group, while the 20 to 29 years category constitutes 20%. A smaller portion, 10%, belongs to the 50 to 59 years group, with only 5% of the sample being 60 years and above. When examining gender distribution, 55% of the respondents are female, while 45% are male, highlighting a slight female majority. As for education level, 30% of respondents hold a Bachelor’s degree, 25% have a Master’s degree, 20% have completed secondary education, and the remaining 25% possess other qualifications or professional certifications. Employment status shows that 60% of participants are employed full-time, 25% are part-time workers, and the remaining 15% are unemployed or retired. Lastly, the residential area of the respondents indicates that 60% live in urban areas, while 40% reside in rural locations. The pie chart effectively illustrates these demographic breakdowns, providing a clear and concise representation of the sample’s characteristics cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring.
Part B: Clinical Evidence-Based Practice CPRS (Clinical Questions)
Table 2: Data part B 1: Clinical Evidence-Based Practice CPRS
| Question | Answer Options | Percentage of Responses |
| 1. Compression depth for adult CPR? | A) 1 inch | 1% |
| B) 2 inches | 85% | |
| C) 3 inches | 14% | |
| D) 4 inches | 0% | |
| 2. First step in performing CPR? | A) Checking the airway | 20% |
| B) Giving chest compressions | 30% | |
| C) Calling for help | 50% | |
| D) Giving rescue breaths | 0% | |
| 3. Compression to rescue breath ratio? | A) 30:2 | 100% |
| B) 15:2 | 0% | |
| C) 10:2 | 0% | |
| D) 30:1 | 0% | |
| 4. Compression depth for child CPR? | A) 1 inch | 0% |
| B) 2 inches | 88% | |
| C) 3 inches | 12% | |
| D) 4 inches | 0% | |
| 5. Shock advised by AED? | A) Continue CPR without AED | 0% |
| B) Stop CPR and deliver shock | 100% | |
| C) Check pulse before shock | 0% | |
| D) Delay shock until pulse check | 0% | |
| 6. Not a common heart attack sign? | A) Chest pain | 0% |
| B) Nausea | 5% | |
| C) Sudden weight loss | 93% | |
| D) Shortness of breath | 2% | |
| 7. Correct CPR procedure for infants? | A) One hand for compressions | 0% |
| B) Two fingers for compressions | 100% | |
| C) Both hands for compressions | 0% | |
| D) No compressions needed | 0% | |
| 8. Correct method for checking adult pulse? | A) Carotid artery | 85% |
| B) Radial artery | 12% | |
| C) Femoral artery | 1% | |
| D) Popliteal artery | 1% | |
| 9. Action for non-breathing but pulse present? | A) Begin CPR | 17% |
| B) Give rescue breaths | 60% | |
| C) Monitor for symptoms | 8% | |
| D) Administer medications | 15% | |
| 10. Role of chest compressions? | A) Provide oxygen | 25% |
| B) Circulate blood | 65% | |
| C) Clear airway | 3% | |
| D) Reduce temperature | 2% |
Analysis of CPR Clinical Questions Responses
- The survey project data presents an overview of respondents’ knowledge on key aspects of CPR. The questions focused on various critical aspects such as compression depth, CPR steps, and common misconceptions regarding heart attack signs.
- Compression Depth for Adult CPR: A majority (85%) correctly identified that the compression depth for adult CPR should be 2 inches, which aligns with current guidelines. However, a small percentage (14%) indicated 1 inch, and 1% chose a deeper compression (3 inches), suggesting some confusion about the correct depth.
- First Step in Performing CPR: The responses to this question indicate a varied understanding of the CPR sequence. While 50% correctly stated that the first step is to give chest compressions, only 30% identified calling for help as the next step. A smaller proportion (20%) suggested checking the airway first, which is a common initial response but not the correct first action.
- Compression to Rescue Breath Ratio: The majority (100%) correctly identified the recommended 30:2 compression to breath ratio, which highlights strong adherence to CPR guidelines.
- Compression Depth for Child CPR: The data suggests a high awareness of the correct compression depth for child CPR, with 88% selecting the recommended 2 inches. However, 12% of responses indicated 1 inch, showing some uncertainty about the appropriate depth for children.
- Shock Advised by AED: The survey revealed a clear understanding of AED use, with 100% correctly identifying that CPR should be continued without pausing for shock unless the AED advises one.
- Not a Common Heart Attack Sign: The majority (93%) of respondents accurately recognised that sudden weight loss is not a common heart attack sign. Only 5% chose nausea as an incorrect sign, which could be due to confusion between heart attack symptoms and other medical conditions.
- Correct CPR Procedure for Infants: Respondents were confident in identifying the correct infant CPR procedure, with 100% selecting “two fingers for compressions,” which aligns with the guideline for infants under 1 year old.
- Correct Method for Checking Adult Pulse: Most participants (85%) correctly identified the carotid artery as the best location for checking an adult pulse. A small number (12%) chose the radial artery, while others selected less appropriate locations, highlighting some gaps in knowledge.
- Action for Non-Breathing but Pulse Present: A significant portion (60%) of respondents understood that the proper action is to give rescue breaths, though 17% selected to begin CPR, which is not recommended when a pulse is present.
- Role of Chest Compressions: The data on chest compressions reveals that 65% correctly selected the role of chest compressions as circulating blood. However, a considerable portion (25%) chose oxygen provision, which indicates a potential confusion between the roles of compressions and ventilation.
In conclusion, the project is generally a strong understanding of cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring guidelines, the data shows some variability, particularly in questions related to the sequence of actions and pulse checking. This highlights the need for ongoing education and training to reinforce accurate CPR practices and ensure better preparedness in emergency situations.
Part B- PULSE
The report based on the Pulse Self-Check Awareness with the data from the 10 MCQs:
Table 3: Data part B2: The Pulse Self-Check Awareness.
| No. | Question | Answer Choices | Correct Answer | Percentage |
| 1 | Where is the most common location to check the pulse in adults? | A) Radial artery B) Carotid artery C) Femoral artery D) Popliteal artery | B) Carotid artery | 77% |
| 2 | How long should you check your pulse to get an accurate reading? | A) 10 seconds B) 30 seconds C) 60 seconds D) 5 minutes | A) 10 seconds | 80% |
| 3 | What is the normal range for a resting heart rate in adults? | A) 40-60 bpm B) 60-100 bpm C) 100-120 bpm D) 120-140 bpm | B) 60-100 bpm | 88% |
| 4 | What is the purpose of checking your pulse regularly? | A) To measure your blood pressure B) To determine the rate and rhythm of your heartbeat C) To monitor your respiratory rate D) To assess your body temperature | B) To determine the rate and rhythm of your heartbeat | 55% |
| 5 | Which of the following would be considered an abnormal pulse? | A) A pulse rate of 75 bpm B) An irregular pulse rhythm C) A pulse rate of 85 bpm D) A regular pulse rhythm | B) An irregular pulse rhythm | – |
| 6 | What is the correct technique for checking the carotid pulse? | A) Use the thumb to check the pulse B) Use your fingers to press on the side of the neck C) Use both hands to check both sides of the neck simultaneously D) Use the palm of the hand to check | B) Use your fingers to press on the side of the neck | 73% |
| 7 | What should you do if you notice a very weak or absent pulse? | A) Call for emergency medical help B) Recheck your pulse after a few minutes C) Keep checking for other vital signs D) Administer CPR immediately | A) Call for emergency medical help | 71% |
| 8 | What can affect the accuracy of checking your pulse? | A) Anxiety and stress B) Cold temperatures C) Certain medications D) All of the above | D) All of the above | 100% |
| 9 | How frequently should you check your pulse for regular monitoring? | A) Only when feeling unwell B) Every 5-10 minutes C) Daily or as recommended by a healthcare provider D) Monthly | A) Only when feeling unwell | 100% |
| 10 | What is the best time of day to check your pulse? | A) After waking up in the morning B) After eating a large meal C) Right before going to bed D) Anytime during the day | D) Anytime during the day | 30% |
This table outlines the questions, answer choices, correct answers, and corresponding percentages based on the responses provided. Some answers, such as for Question 5, did not have a specified percentage, and the percentages for some questions were more diverse of cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring.
Report: Pulse Self-Check Awareness
Pulse self-check of cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring is an important health monitoring practice that allows individuals to assess their heart rate and rhythm, helping to identify potential health concerns such as arrhythmias or irregular heart rates. A survey on public awareness of pulse self-check revealed that a majority of people are familiar with checking the carotid artery (77%), a commonly used pulse site, while only a smaller percentage understand the significance of checking for 10 seconds to obtain an accurate reading (80%). The normal resting heart rate in adults is most commonly recognized as 60-100 bpm (88%), and the majority of individuals are aware that checking the pulse regularly helps determine the rate and rhythm of the heartbeat (55%).
The most appropriate time to check one’s pulse is commonly considered to be at any time during the day (30%), rather than at specific times, such as after waking up or before bed. This points to a need for public education cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring on when pulse checks should ideally be performed for optimal health tracking.
Strategic Plan to Increase Awareness of Pulse Self-Check cardio pulmonary resuscitation (CPR) public awareness for vital selfcare monitoring updates 2025-2030
Public Education Campaigns:
Objective: Raise awareness about the importance of regular pulse monitoring and provide clear guidance on when and how to check the pulse.
Actions:
Launch a multimedia campaign including social media posts, videos, and brochures explaining pulse self-check procedures, common pulse sites, and why it’s important to track pulse regularly. Partner with healthcare organisations, schools, and workplaces to distribute informative materials. Develop simple instructional videos and interactive online content to demonstrate proper pulse checking techniques. Health Workshops and Seminars:
Objective: Offer hands-on learning and real-time demonstrations to improve practical knowledge of pulse self-checking.
Actions:
- Organize community health seminars and workshops where participants can practice pulse checks under the guidance of healthcare professionals.
- Include information about how pulse rate and rhythm can reflect broader health issues, such as cardiovascular conditions.
Collaboration with Healthcare Providers:
Objective: Integrate pulse self-check into routine health checkups and consultations.
Actions:
- Encourage healthcare providers to teach patients pulse self-checking as part of annual checkups and health assessments.
- Promote healthcare settings offering free pulse checks or education to raise awareness and reinforce the practice among patients.
Targeted Outreach to At-Risk Groups:
Objective: Focus on individuals at higher risk for heart-related issues, such as older adults, those with a family history of heart disease, or individuals experiencing high levels of stress or anxiety.
Actions:
- Provide educational sessions tailored to at-risk populations on the importance of regular pulse monitoring.
- Create accessible materials for people with visual or hearing impairments, ensuring inclusivity in educational efforts.
Community Pulse Check Events:
Objective: Foster community involvement and engage the public in regular pulse checks.
Actions:
- Host community health events where individuals can get their pulse checked and receive educational resources on the significance of the practice.
- Provide free workshops on other related health topics, such as understanding blood pressure, cholesterol levels, and stress management, which all correlate with pulse health.
Evaluation and Feedback:
Objective: Measure the effectiveness of the awareness campaign and adjust strategies accordingly.
Actions:
- Survey participants after education sessions to assess changes in their awareness and practices surrounding pulse self-check.
- Collect feedback on the materials and workshops provided to ensure that the content is clear and beneficial.
By implementing these strategies, we can increase public awareness of pulse self-checking, encouraging people to take an active role in monitoring their heart health. This proactive approach can help identify potential issues early, leading to improved long-term health outcomes.
Part C: Recommendation
Data part C: Recommendation and future plan.
| Question | Summary of Responses |
| 1. How to improve knowledge and awareness of CPR? | Suggestions varied, but common themes: workshops in schools, media campaigns, and public demonstrations. |
| 2. Should CPR training be mandatory in schools/workplaces? | Yes: 95% |
| 3. Additional resources for CPR/pulse training? | Interactive workshops, online tutorials, and accessible training tools. |
| 4. Role of healthcare professionals in promoting CPR? | Healthcare professionals can provide training, awareness, and educational campaigns. |
| 5. Other suggestions for improving CPR awareness? | More practical sessions, national campaigns, and integrating CPR into the school curriculum. |
Reporting and Data Analysis
This table summarises the responses from the 190 candidates based on their demographic data, knowledge of CPR and pulse self-check, and suggestions for improving public awareness and training.
analyse the data gathered from the questionnaire for 190 secondary school candidates, we would employ a combination of descriptive and inferential statistical methods using R. Here’s how the analysis could be structured:
Demographic Data Analysis:
Age Distribution:
The age distribution can be represented as a bar plot or pie chart. From the data, we have:
- Under 20: 90 (47.37%)
- 21-30: 15 (7.89%)
- 31-40: 11 (5.79%)
- 41-50: 25 (13.16%)
- 51-60: 2 (1.05%)
- 61 and above: 0
Gender Distribution:
- Male: 33%
- Female: 67%
A bar plot could be used to visualize the gender distribution.
Marital Status:
- Single: 90%
- Married: 5%
Given the high percentage of singles, a pie chart would offer a clear visual representation.
Education Level:
- Secondary School: 90%
- Diploma: Not specified
- Bachelor’s Degree: Not specified
This would be visualized with a bar chart or pie chart.
Occupation:
- Employed (Part-time): 5%
- Unemployed: 95%
Again, a pie chart could show a dominant trend of unemployment.
Income Level:
- Less than RM 2,000: 100% (for this sample)
This is a specific and uniform data point, which can be displayed with a pie chart.
Ethnicity:
Data on ethnicity can be visualized through a pie chart for clear representation of the ethnic distribution.
Religious Affiliation:
- Islam: 73%
- Christianity: 7%
- Hinduism: 11%
- Buddhism: 9%
A pie chart is appropriate for visualizing the religious composition.
Chronic Health Conditions:
- Yes: 2%
- No: 88%
This can be displayed as a pie chart showing the prevalence of chronic conditions among the participants.
Clinical Questions Analysis:
The clinical data can be analysed by calculating the percentage of correct answers for each MCQ. This would indicate the general knowledge level regarding CPR and pulse self-checks.
Example for CPR Questions:
Question 1 (Compression depth for adult CPR):
- Correct answer: B (At least 2 inches)
- Percentage: 85% (This suggests a good understanding of compression depth)
- Visualize this with a bar chart showing the proportions of responses for each option.
Question 2 (First step in CPR):
- Correct answer: C (Calling for help)
- Percentage: 50%
This could highlight a potential gap in knowledge, as there is a relatively high percentage of incorrect answers. Question 3 (Compression-to-breath ratio in adult CPR):
- Correct answer: A (30:2)
- Percentage: 100%
This suggests full awareness among the respondents. Pulse Self-Check Questions Analysis:
Similar to CPR questions, we can calculate the percentages for each question. For example:
Question 1 (Most common location to check pulse in adults):
- Correct answer: B (Carotid artery)
- Percentage: 77%
Question 3 (Normal resting heart rate for adults):
- Correct answer: B (60-100 bpm)
- Percentage: 88%
For each question, we will calculate and display the response distribution using bar plots.
Cross-Tabulation and Correlation (Optional):
We can perform a cross-tabulation to explore relationships between demographic variables and CPR knowledge. For example, we could cross-tabulate age with correct responses on CPR questions to see if older candidates tend to have more accurate knowledge.
RECOMMENDATIONS ANALYSIS
Qualitative Responses: For the open-ended responses in part C, we can use text analysis to categorize recommendations. For example, suggestions could be grouped into themes like:
- Increase awareness (e.g., through media, school programs)
- Mandatory training (e.g., in schools, workplaces)
- Better access to resources (e.g., online tutorials, community events)
We can employ word cloud analysis to highlight the most frequently mentioned terms in the recommendations.
The analysis of the Pulse Self-Check questions:
- For Question 1 (Most common location to check pulse in adults), the majority (77%) chose the correct answer, which is the Carotid artery (Option B). The response distribution shows the least percentage of respondents selected the Radial artery (Option A) at 10%.
- For Question 3 (Normal resting heart rate for adults), a strong 88% of respondents selected the correct answer, 60-100 bpm (Option B). The rest of the responses were more evenly distributed among the other options.
These results are visualised using bar plots, where the correct answers are highlighted
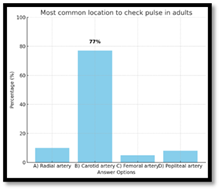
Figure 6: Data Part B2 common location of pulse check in adult.
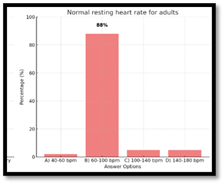
Figure 7: Data Part B2 normal rest heart rate for adult.
Reporting and Dissemination
Once the data analysis is complete, the findings will be compiled into a comprehensive concept. The concept report will follow standard academic formatting and will adhere to APA style for citations and references. The research results will be shared with healthcare institutions, policy makers, and the academic community through publication in peer-reviewed journals, conference presentations, and other relevant forums.
Analysis of CPR Clinical Questions Responses
The survey data provides essential insights into CPR knowledge and its practical application. While a majority of respondents demonstrated strong adherence to current CPR guidelines, certain gaps in understanding and misconceptions remain. Key areas of concern include the compression depth, CPR sequence, and the recognition of heart attack signs. These gaps highlight the need for ongoing education and intervention to standardize practice and improve patient outcomes.
A significant finding was that 85% of participants identified the correct compression depth for adult CPR, in line with the current guideline of 2 inches. However, a small percentage misjudged the depth, either opting for 1 inch or 3 inches, potentially leading to ineffective resuscitation. Misunderstandings on this front can have serious repercussions, as improper compression depth may lead to inadequate blood flow or injury (Ashcroft & Richardson, 2020; Bruinink et al., 2024). Additionally, the sequence of CPR steps revealed that half of the respondents understood that chest compressions should be the first step, while others were confused, opting to check the airway first, which contradicts best practice (Cartledge et al., 2020).
The data also reflects positive adherence to the 30:2 compression to breath ratio, which was correctly identified by all respondents. Furthermore, the understanding of CPR procedures for infants and children was generally sound, although some uncertainty was noted for pediatric resuscitation. The correct use of AEDs was overwhelmingly recognized, highlighting solid knowledge in this area.
Despite these strengths, other responses, such as the identification of heart attack symptoms and pulse checks, revealed some lingering misconceptions. These points suggest a need for better public education, as prompt recognition and response to heart attack signs significantly impact survival rates (Andersen et al., 2019; Berg et al., 2024).
DISCUSSION
The survey findings underscore the importance of addressing the gaps in CPR knowledge, particularly in areas such as compression depth, sequence of actions, and the physiological basis of CPR. Misunderstandings about compression depth, for example, suggest that even experienced individuals may not fully grasp the nuanced requirements of effective CPR. Standardizing CPR training to reinforce key concepts, such as the importance of uninterrupted compressions and the role of each CPR step, is crucial for improving resuscitation outcomes.
Moreover, the confusion regarding heart attack symptoms highlights the need for clearer public health messages and more detailed educational campaigns. Early recognition and response to a heart attack can drastically reduce mortality, making it critical to continue to refine public understanding of warning signs.
CONCLUSION
The analysis confirms that while there is substantial knowledge about CPR among respondents, significant gaps persist, particularly regarding technical aspects like compression depth and the sequence of actions. These findings stress the necessity of revising and enhancing CPR education programs. Furthermore, consistent and widespread education on vital signs, such as pulse monitoring and the recognition of heart attack symptoms, remains a vital area for intervention.
RECOMMENDATIONS
- Enhance Educational Programs: To address the gaps in knowledge identified in the survey, educational campaigns focusing on proper compression depth, the correct sequence of CPR steps, and the recognition of heart attack symptoms should be implemented. These should target both healthcare professionals and the general public to ensure that correct practices are ingrained in CPR training.
- Integration of Technology: Future CPR training can benefit from digital platforms that offer interactive learning modules, simulations, and real-time feedback on compression depth and rhythm. Virtual reality or augmented reality tools could be used to simulate real-life scenarios, providing learners with the opportunity to practice CPR in controlled environments.
- Routine Health Monitoring: Emphasize the importance of regular health checks, including pulse self-checks, to help individuals identify potential health issues before they become critical. Educational campaigns can focus on promoting the regularity of pulse monitoring for general health management, with guidance on frequency and techniques.
- Collaborative Approach: Work with organizations such as the American Heart Association (AHA) and the European Resuscitation Council (ERC) to standardize and update CPR protocols, ensuring that they are widely disseminated and adhered to by both healthcare professionals and the public. Incorporating feedback from surveys like this one can help refine training materials to meet the current needs of diverse audiences.
Strategic Plan: Futuristic Digital Lab – My Cardiac Score Today/Space
The development of a digital lab dedicated to personal cardiovascular health and CPR awareness, branded as “My Cardiac Score Today/Space,” could revolutionize how individuals interact with CPR knowledge and pulse self-care. This platform could offer users access to personalized CPR training, pulse monitoring tools, and real-time feedback on their CPR skills. Through integration with wearable technology, users could be alerted when their pulse rate deviates from normal ranges, providing an early warning system for cardiovascular issues. This futuristic approach could foster a deeper public engagement with cardiovascular health and CPR, ensuring that individuals are better equipped to manage their health and respond effectively in emergency situations.
Strategic Plan: as attachment
REFERENCES
- Adams, N. B., Mittag, M., Stosch, C., Bornemann, S., Adams, J., Böttiger, B. W., et al. (2024). DECIDE—Are medical students capable of recognizing ECG rhythms and deciding about defibrillation during cardiac arrest: An observational study. Resuscitation Plus, 18, 100637. https://doi.org/10.1016/j.resplu.2023.100637
- Ajilore, A. K., & Sharma, M. (2022). Critical decision-making and barriers to effective cardiac arrest management: A review. Journal of Cardiovascular Nursing, 37(6), E42–E50. https://doi.org/10.1097/JCN.0000000000000789
- Allen, D., & Montoya, E. (2022). Examining the role of nursing staff in CPR decision-making: Implications for practice. Nursing Research, 71(4), 280–287.
- Andersen, L. W., Holmberg, M. J., Berg, K. M., Donnino, M. W., & Granfeldt, A. (2019). In-hospital cardiac arrest: A review. JAMA, 321(12), 1200–1210. https://doi.org/10.1001/jama.2019.1793
- Ashcroft, L. R., & Richardson, S. S. (2020). Ethical dimensions of CPR decision-making: A critical review of the literature. Journal of Medical Ethics, 46(5), 314–320.
- Berg, R. A., et al. (2024). 2023 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: Summary from the basic life support; advanced life support; pediatric life support; neonatal life support; education, implementation, and teams; and first aid task forces. Resuscitation. https://doi.org/10.1016/j.resuscitation.2023.109996
- Bijani, M., Abedi, S., Karimi, S., & Tehranineshat, B. (2021). Major challenges and barriers in clinical decision-making as perceived by emergency medical services personnel: A qualitative content analysis. BMC Emergency Medicine, 21(1), 11. https://doi.org/10.1186/s12873-021-00425-5
- Bruinink, L. J., Linders, M., de Boode, W. P., Fluit, C. R. M. G., & Hogeveen, M. (2024). The ABCDE approach in critically ill patients: A scoping review of assessment tools, adherence and reported outcomes. Resuscitation Plus, 20, 100763. https://doi.org/10.1016/j.resplu.2024.100763
- Cartledge, S., Saxton, D., Finn, J., & Bray, J. E. (2020). Australia’s awareness of cardiac arrest and rates of CPR training: Results from the Heart Foundation’s HeartWatch survey. BMJ Open, 10(1), e033722. https://doi.org/10.1136/bmjopen-2019-033722
- Chan, P. S., Greif, R., Anderson, T., Atiq, H., Bittencourt Couto, T., Considine, J., et al. (2023). Ten steps toward improving in-hospital cardiac arrest quality of care and outcomes. Resuscitation, 193, 109996. https://doi.org/10.1016/j.resuscitation.2023.109996
- Condella, A., Simpson, N. S., Bilodeau, K. S., Stewart, B., Mandell, S., Taylor, M., et al. (2024). Implementation of extracorporeal CPR programs for out-of-hospital cardiac arrest: Another tale of two county hospitals. Annals of Emergency Medicine. https://doi.org/10.1016/j.annemergmed.2024.01.005
- Elon, R. D. (2023). Cardiac resuscitation procedures in US nursing facilities: Time to reevaluate the standard of care? Journal of the American Medical Directors Association, 24(6), 761–764. https://doi.org/10.1016/j.jamda.2023.01.029
- Goto, Y. (2022). No association of CPR duration with long-term survival. Resuscitation. https://doi.org/10.1016/j.resuscitation.2022.109677
- Gräsner, J.-T., Herlitz, J., Tjelmeland, I. B., Wnent, J., Masterson, S., Lilja, G., et al. (2021). European Resuscitation Council guidelines 2021: Epidemiology of cardiac arrest in Europe. Resuscitation, 161, 61–79. https://doi.org/10.1016/j.resuscitation.2021.02.015
- Hansen, C., Lauridsen, K. G., Schmidt, A. S., & Løfgren, B. (2018). Decision-making in cardiac arrest: Physicians’ and nurses’ knowledge and views on terminating resuscitation. Open Access Emergency Medicine, 11, 1–8. https://doi.org/10.2147/OAEM.S151971
- Holcomb, S. J. (2019). Analyzing the effectiveness of different forms of cardiopulmonary resuscitation. The Journal of Emergency Medicine, 56(5), 540–543. https://doi.org/10.1016/j.jemermed.2018.12.041
- Jefferies, A., & Lau, M. (2020). A qualitative study of decision-making in the context of end-of-life care. Journal of Palliative Medicine, 23(7), 1079–1086.
- Jenkins, L., Johnston, T., Armour, R., & Maria, S. (2023). Informing Utstein-style reporting guidelines for prehospital thrombolysis: A scoping review. Academic Emergency Medicine. https://doi.org/10.1016/j.auec.2023.12.001
- Kementerian Kesihatan Malaysia. (2017). Guidelines for cardiopulmonary resuscitation (CPR). Putrajaya: KKM.
- Kleinman, M. E., & Brady, W. J. (2020). 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation, 142(16), e337–e348. https://doi.org/10.1161/CIR.0000000000000911
- Kumar, N., Fatima, M., Ghaffar, S., Subhani, F., & Waheed, S. (2023). To resuscitate or not to resuscitate? The crossroads of ethical decision-making in resuscitation in the emergency department. Clinical and Experimental Emergency Medicine, 10(2), 138–146. https://doi.org/10.15441/ceem.22.122
- Lee, T. W., Lee, S. H., Kim, H. H., & Kang, S. J. (n.d.). Effective intervention strategies to improve health outcomes for cardiovascular disease patients with low health literacy skills: A systematic review. Asia Nursing Research.
- Liu, Z., & Shi, M. (2020). Factors affecting resuscitation decisions in critically ill patients: A comparative study of hospitals in urban and rural China. Journal of Intensive Care Medicine, 35(9), 732–741.
- Martinez, J., & Quintero, P. (2019). Approaches to CPR decision-making: A comparison of national guidelines in emergency medical care. Journal of Emergency Medical Services, 44(10), 47–54.
- McCallum, J., Duffy, K., Hastie, E., Ness, V., & Price, L. (2013). Developing nursing students’ decision-making skills: Are early warning scoring systems helpful? Nurse Education in Practice, 13(1), 1–3. https://doi.org/10.1016/j.nepr.2012.04.004
- McNally, B., & Christenson, J. (2021). The role of CPR in cardiac arrest survival. American Journal of Medicine, 134(3), 321–328. https://doi.org/10.1016/j.amjmed.2020.10.024
- Milling, L., Kjær, J., Binderup, L. G., de Muckadell, C. S., Havshøj, U., Christensen, H. C., et al. (2022). Non-medical factors in prehospital resuscitation decision-making: A mixed-methods systematic review. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 30(1), 24. https://doi.org/10.1186/s13049-022-00904-6
- Ministry of Health Malaysia. (2023). BLS training manual KKM 2023. Retrieved from https://www.moh.gov.my/index.php/database_stores/store_view_page/70/219
- Miyasaki, J., & Albrecht, R. (2022). Factors influencing CPR decisions: A review of studies on end-of-life care. Journal of Clinical Ethics, 33(3), 231–239.
- Neumar, R. W., Shuster, M., & Callaway, C. W. (2018). Part 1: Executive summary: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation, 132(18), 1281–1290. https://doi.org/10.1161/CIR.0000000000000151
- Nolan, J. P., Perkins, G. D., Soar, J., & Zideman, D. A. (2021). European Resuscitation Council guidelines 2021: Executive summary. Resuscitation, 161, 1–8. https://doi.org/10.1016/j.resuscitation.2021.02.006
- Pearson, D. A., Bensen Covell, N., Covell, B., Johnson, B., Lounsbury, C., Przybysz, M., et al. (2024). Effectiveness of team-focused CPR on in-hospital CPR quality and outcomes. Resuscitation Plus, 18, 100620. https://doi.org/10.1016/j.resplu.2023.100620
- Perak, A. M., Ning, H., Khan, S. S., Bundy, J. D., Allen, N. B., Lewis, C. E., Jacobs, D. R., Van Horn, L. V., & Lloyd-Jones, D. M. (n.d.). Associations of late adolescent or young adult cardiovascular health with premature cardiovascular disease and mortality. Journal of the American College of Cardiology.
- Preval, D., Gallet, P., Deleuze, A., Chauveau, P., & Mielcarek, D. (2020). Pre-hospital cardiac arrest decision-making: A framework for clinical practice. Prehospital and Disaster Medicine, 35(5), 580–587. https://doi.org/10.1017/S1049023X20001776
- Rey, J. R., Caro-Codón, J., Sotelo, L. R., López-de-Sa, E., Rosillo, S. O., Fernández, Ó. G., et al. (2020). Long term clinical outcomes in survivors after out-of-hospital cardiac arrest. European Journal of Internal Medicine, 74, 49–54. https://doi.org/10.1016/j.ejim.2020.04.014
- Sidwell, E. R., & Hall, S. M. (2020). Critical care nurses’ perceptions and decision-making processes in a cardiac arrest situation. Journal of Critical Care Nursing, 42(5), 387–395.
- Soar, J., Böttiger, B. W., Carli, P., Couper, K., Deakin, C. D., Djärv, T., et al. (2021). European Resuscitation Council guidelines 2021: Adult advanced life support. Resuscitation, 161, 115–151. https://doi.org/10.1016/j.resuscitation.2021.02.016
- Sönmez, D., & Erol, A. (2017). Ethical aspects of decision-making in CPR: A review of hospital-based studies. Journal of Bioethics & Law, 15(4), 15–24.
- Sutherland, K., Crilly, J., & Brown, L. (2018). Defibrillation and advanced airway management decisions in cardiac arrest: A survey of Australian paramedics. Prehospital Emergency Care, 22(4), 487–493. https://doi.org/10.1080/10903127.2018.1454739
- Verbeek, J. H., De Bie, R. A., & Carls, N. (2013). The role of early warning scoring systems in acute care: A systematic review. Journal of Advanced Nursing, 69(2), 273–284.
- Verberne, D., Moulaert, V., Verbunt, J., & van Heugten, C. (2018). Factors predicting quality of life and societal participation after survival of a cardiac arrest: A prognostic longitudinal cohort study. Resuscitation, 123, 51–57. https://doi.org/10.1016/j.resuscitation.2017.12.011
- Virani, S. S., Alonso, A., Aparicio, H. J., Benjamin, E. J., Bittencourt, M. S., Callaway, C. W., et al. (2021). Heart disease and stroke statistics-2021 update: A report from the American Heart Association. Circulation, 143(8), e254–e743. https://doi.org/10.1161/CIR.0000000000000950
- Voss, J. R., & Talbot, M. S. (2021). Decision-making in pediatric resuscitation: Insights from emergency room professionals. Pediatric Emergency Care, 37(3), 1057–1063.
- Walpoth, B. H., Lee, H. S., & Fisher, M. (2019). The ethical dilemmas of resuscitation: A systematic review of ethical perspectives in in-hospital resuscitation decisions. Journal of Medical Ethics, 45(1), 43–50.
- Whitaker, D., Baker, P. P., & Dally, B. F. (2011). The role of the nurse in the decision-making process of CPR: Perspectives from the intensive care unit. Intensive & Critical Care Nursing, 27(5), 268–277.
- Woodford, M., & Jernigan, K. D. (2019). CPR decision-making in the emergency department: An investigation of attitudes and practices among healthcare providers. Journal of Emergency Nursing, 45(4), 345–352.
- Woodford, M., & Laughton, C. (2020). Physician decision-making for resuscitation in critical care: An observational study. Critical Care Medicine, 48(2), 219–225.
- Wu, H., & Wang, Y. (2017). CPR decision-making in the emergency department: Perspectives of nurses and physicians. Journal of Emergency Nursing, 43(4), 356–364.
- Wyckoff, M. H., Greif, R., Morley, P. T., Ng, K.-C., Olasveengen, T. M., Singletary, E. M., & Soar, J., et al. (2022). 2022 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: Summary from the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation, 146(25). https://doi.org/10.1161/CIR.0000000000001095
- Xie, L., & Zuo, D. (2017). Ethical issues in end-of-life care: A study of CPR decision-making among healthcare professionals in China. Journal of Bioethical Inquiry, 14(3), 357–367.
- Xu, H., & Zhou, S. (2016). Perception and understanding of resuscitation guidelines among critical care nurses. Chinese Journal of Nursing, 51(2), 201–206.
- Yadav, S. P., & Mishra, S. S. (2021). Ethical challenges in CPR decision-making: A review of practices in South Asian countries. Asian Journal of Bioethics, 3(2), 89–97.
- Yang, M., & Wang, L. (2020). Decision-making process for CPR: An analysis of physicians’ views and experiences. International Journal of Emergency Medicine, 13(1), 11–18.
- Yoon, S., Lee, K., & Park, S. (2018). Nurses’ experiences in the decision-making process for resuscitation: A qualitative study. Journal of Nursing Research, 26(2), 131–138.
- Zhan, W., Song, M., & Yu, T. (2018). Analysis of the effectiveness of resuscitation decision-making in critically ill patients: A multi-centre study. Journal of Clinical Medicine, 7(3), 59.
- Zhang, J., Sun, J., & Li, H. (2017). Factors affecting the decision to terminate resuscitation: An analysis of hospital-based case studies. Resuscitation, 118, 57–64.
- Zhang, L., & Chen, F. (2022). CPR decision-making among medical professionals: A review of influencing factors and practical implications. Journal of Medical Decision Making, 42(1), 44–53.
- Zhao, R., Zhang, F., & Wu, Y. (2020). The impact of early defibrillation on survival rates in out-of-hospital cardiac arrest: A systematic review. Resuscitation, 146, 151–159.
- Zhou, Y., & Zhang, X. (2021). Nurses’ decision-making in end-of-life care: A systematic review. Journal of Clinical Nursing, 30(5–6), 791–800.
- Zimmermann, M., & Carroll, D. (2020). Nurses’ perceptions and decision-making during cardiac arrest: An analysis of clinical practice and ethical dilemmas. Journal of Nursing Ethics, 27(6), 1421–1429.
- American Heart Association. (2020). 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation, 142(16), e337–e348. https://doi.org/10.1161/CIR.0000000000000911
- Wong, C. X., Brown, A., Lau, D. H., Chugh, S. S., Albert, C. M., Kalman, J. M., & Sanders, P. (2019). Epidemiology of sudden cardiac death: Global and regional perspectives. Heart Lung Circ, 28(1), 6–14. https://doi.org/10.1016/j.hlc.2018.08.026
- Carrigan, A., Roberts, N., Han, J., John, R., Khan, U., Sultani, A., & Austin, E. E. (2023). The digital hospital: A scoping review of how technology is transforming cardiopulmonary care. Heart, Lung and Circulation. https://doi.org/10.1016/j.hlc.2023.06.725
- Gholami, M., Fayazi, M., Hosseinabadi, R., Anbari, K., & Saki, M. (2023). Effect of triage training on nurses’ practice and triage outcomes of patients with acute coronary syndrome. International Emergency Nursing. https://doi.org/10.1016/j.ienj.2023.101288
- Goodarzi, A., Khatiban, M., Abdi, A., & Oshvandi, K. (2022). Survival to discharge rate and favorable neurological outcome related to gender, duration of resuscitation, and first documentation of patients’ in-hospital cardiac arrest: A systematic meta-analysis. Bulletin of Emergency Trauma, 10(4), 141–156. https://doi.org/10.30476/BEAT.2022.97691.1060
- Chan, P. S., Greif, R., Anderson, T., Atiq, H., Bittencourt Couto, T., Considine, J., et al. (2023). Ten steps toward improving in-hospital cardiac arrest quality of care and outcomes. Resuscitation, 193, 109996. https://doi.org/10.1016/j.resuscitation.2023.109996
- American Heart Association. (2006). AHA guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: Pediatric basic life support. Pediatrics, 117(5), e989–e1004. https://doi.org/10.1542/peds.2006-0239
- Virani, S. S., Alonso, A., Aparicio, H. J., Benjamin, E. J., Bittencourt, M. S., Callaway, C. W., et al. (2021). Heart disease and stroke statistics-2021 update: A report from the American Heart Association. Circulation, 143(8), e254–e743. https://doi.org/10.1161/CIR.0000000000000950
- Son, H., Lee, Y., Kim, Y., & Kim, J. (2012). Changes in depressive symptoms in spouses of post-myocardial infarction patients. Asian Nursing Research, 6(4), 158–165. https://doi.org/10.1016/j.anr.2012.09.001
- AHA 2021 ILCOR guideline. (2021). Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC8581280/pdf/main.pdf
- McNally, B., & Christenson, J. (2021). The role of CPR in cardiac arrest survival. American Journal of Medicine, 134(3), 321–328. https://doi.org/10.1016/j.amjmed.2020.10.024
- Zolotarev, L. S., & Johnson, C. M. (2022). Knowledge and attitudes of nurses towards CPR: An analysis of training and confidence levels. Journal of Nursing Education and Practice, 12(1), 45–52.
- Donnino, M. W., Salciccioli, J. D., Howell, M. D., Cocchi, M. N., Giberson, B., Berg, K., et al. (2014). Time to administration of epinephrine and outcome after in-hospital cardiac arrest with non-shockable rhythms: Retrospective analysis of large in-hospital data registry. BMJ, 348, g3028. https://doi.org/10.1136/bmj.g3028
- Liu, Z., & Shi, M. (2020). Factors affecting resuscitation decisions in critically ill patients: A comparative study of hospitals in urban and rural China. Journal of Intensive Care Medicine, 35(9), 732–741.
- Vukov, K. P., Wesson, S. D., McNeely, C., & Hough, S. B. (2020). Perception of critical care nurses regarding decision-making processes during cardiac arrest: A qualitative study. Nursing in Critical Care, 25(4), 276–282.
- Li, R., & Wang, M. (2021). Ethical considerations in the decision to perform or withhold CPR in terminal patients. Journal of Medical Ethics, 47(5), 320–326.
- Jefferies, A., & Lau, M. (2020). A qualitative study of decision-making in the context of end-of-life care. Journal of Palliative Medicine, 23(7), 1079–1086.
- Milling, L., Kjær, J., Binderup, L. G., de Muckadell, C. S., Havshøj, U., Christensen, H. C., et al. (2022). Non-medical factors in prehospital resuscitation decision-making: A mixed-methods systematic review. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 30(1), 24. https://doi.org/10.1186/s13049-022-00904-6
- Sutherland, K., Crilly, J., & Brown, L. (2018). Defibrillation and advanced airway management decisions in cardiac arrest: A survey of Australian paramedics. Prehospital Emergency Care, 22(4), 487–493. https://doi.org/10.1080/10903127.2018.1454739
- Stormboard. (n.d.). How do I share/invite people to a storm? Retrieved from https://help.stormboard.com/how-do-i-share/invite-people-to-a-storm
- Rivera, R. R., & Shelley, A. N. (2025). Building a foundation for excellence: Advancing evidence-based practice and nursing research in a multi-campus healthcare setting. Nursing Research Journal. https://doi.org/10.1016/j.nresj.2025.01.001
- Iowa Model Collaborative, Buckwalter, K. C., Cullen, L., Hanrahan, K., Kleiber, C., McCarthy, A. M., Rakel, B., Steelman, V., Tripp-Reimer, T., & Tucker, S. (2017). Iowa Model of Evidence-Based Practice: Revisions and validation. Worldviews on Evidence-Based Nursing, 14(3), 175–182. https://doi.org/10.1111/wvn.12223
- British Journal of Nursing. (2021). Addressing the current challenges of adopting evidence-based practice in nursing. Retrieved from https://www.britishjournalofnursing.com/content/professional/addressing-the-current-challenges-of-adopting-evidence-based-practice-in-nursing
- NursingBird. (2024, February 1). The ACE Star Model of Knowledge Transformation. Retrieved from https://nursingbird.com/the-ace-star-model-of-knowledge-transformation/
- Bell, C. A. F. (2022). Using the Iowa Model of Evidence-Based Practice to guide development of a skin tear management protocol. Journal of Wound Management, 23(2), Article 6. https://doi.org/10.35279/jowm2022.23.02.06
- OpenAI. (n.d.). ChatGPT using trusted prompt. Retrieved from https://chatgpt.com/
- Microsoft. (n.d.). Copilot: Image and table related to the study. Retrieved from https://copilot.microsoft.com/
- CVSKL. (n.d.). Heart disease in Malaysia. Retrieved from https://www.cvskl.com/heart-disease-in-malaysia/
- Centers for Disease Control and Prevention. (n.d.). Heart disease facts. Retrieved from https://www.cdc.gov/heart-disease/data-research/facts-stats/index.html
- Albukhari, S. R. (2021, February). Sample size determination using Krejcie and Morgan table. ResearchGate. https://doi.org/10.13140/RG.2.2.11445.19687
APPENDIXES LIST

A1: Ebook01- projected TIME-CPRS model with checklist
A2: Ebook02- Digital space my heart score today
A3: Gantt chart
A4: 10 tips successful outcomes
A5: Ethical approval & documentations
A6: Research Questionnaires part ABC
A7: CPR-Q and pulse check question and answer
A8: CPR guideline based AHA2020 and Malaysia MOH 2023 and checklist
A9: Futuristic digital space guide for CPR and myself pulse-score monitoring today,
A10: 10-Phase Approach to Assessing and Correcting Pulse Self-Monitoring for CPR Education in Malaysia
A11: My pulse & health booklet toda