
The Impact of Stigma and Discrimination, on Adherence Levels in HIV-Positive Patients: Evidence from Ondo State Clinics
- Fashanu A. J
- Akinniyi R. O
- Ogunbadejo J
- 4448-4455
- Mar 24, 2025
- Public Health
The Impact of Stigma and Discrimination, on Adherence Levels in HIV-Positive Patients: Evidence from Ondo State Clinics
Fashanu A. J1, Akinniyi R. O2, Ogunbadejo J3
1,2,3Department Of Public Health, Faculty Public and Allied Health, Babcock University, Ilishan-Remo, Ogun State Nigeria
DOI: https://dx.doi.org/10.47772/IJRISS.2025.9020350
Received: 13 February 2025; Accepted: 18 February 2025; Published: 24 March 2025
ABSTRACT
Target 6A, which sought to stop the transmission of HIV by 2015 and start to reverse it, was one of the Millennium Development Goals’ achievements. The number of AIDS-related fatalities and new HIV infections has decreased by 42% and 40%, respectively, as of 2014. Low risk perception, concurrent sexual relationships, and insufficient access to high-quality healthcare treatments are the primary causes of the infection in Nigeria. The main obstacle impeding the country’s response to the epidemic is HIV stigma and prejudice, which is at the heart of this problem. This study aimed to assess the level of effect that stigma and discrimination has on enrolment status and drug adherence among HIV positive individuals in Ondo State. This study made use of a cross-sectional descriptive design involving 432 HIV patients selected across four facilities in Ondo State. Results showed that there was a high level of adherence to treatment by PLWA, and there is a significant association between stigma, discrimination and adherence. This study concluded that PLWHA show a high level of adherence to treatment due to the low stigma they experienced
Keywords: Adherence, HIV, Impact, Discrimination, Stigma
INTRODUCTION
One of the Millennium Development Goals’ achievements was objective 6A, which sought to stop the transmission of HIV by 2015 and start to reverse it. New HIV infections and fatalities from AIDS have decreased by 40% and 42%, respectively, as of 2014 [1]. Although the region is home to 70.0% of people living with HIV worldwide, Sub-Saharan Africa was left behind in this accomplishment [2]. Approximately 46% of the 36.7 million people living with HIV as of the end of 2015 have access to treatment, according to latest figures. With 3.8 million and an adult incidence of 3.1%, Nigeria has the second-highest number of these [3]. According to ref [4], poor risk perception, concurrent sexual engagements, and limited access to high-quality healthcare facilities are among of the primary reasons contributing to the infection in Nigeria. At the core of these concerns is the problem of HIV stigma and discrimination, which poses a significant obstacle to good healthcare, particularly for those with HIV, as well as to the country’s response to the pandemic.
Discrimination occurs when any kind of distinction, exclusion, or restriction is applied to an individual due to a personal characteristic or attribute. Stigma is the term used to describe beliefs and/or attitudes that mark or discredit a person or group of people. Sociocultural, political, and economic issues all have an impact on how stigma is manifested or expressed, and this leads to disparities in access to HIV care, treatment, and support [5]. HIV-stigma operates at the individual, family, community, and institutional levels as a result of these multi-level influences. Many of these causes also differed throughout cultures, therefore addressing the phenomenon requires context-specific approaches. Nigeria, one of the nations with the highest number of PLHIV, has worked to reduce HIV stigma and prejudice in an effort to slow the pandemic, according to ref [6]. Confronting blame and HIV stereotypes; managing the disclosure of a stigmatized status; renegotiating social relationships; and self-acceptance, or one’s degree of comfort with one’s HIV diagnosis, are the four components of internalized HIV stigma [7]. Sometimes stigma keeps families from receiving or providing help. To hide the fact that they are HIV positive, people may not always take their medications as prescribed or at the appropriate times. Consequently, stigma and prejudice fuel the spread of HIV and undermine AIDS responses [8]. This problem is especially important in places like Ondo State, Nigeria, where there are few resources and poor healthcare facilities, and where PLHIV stigma is still widely accepted.
Previous studies have suggested that stigmatization can lead to decreased treatment engagement, as many of these patients may be scared of disclosing their status or attending regular clinic visits, which may further aggravate the impact of the disease on their health and wellbeing [9], [10]. It is important then, to understand the relationship between stigma, discrimination, and adherence to treatment in order to further improve HIV outcomes. Adherence to Antiretroviral therapy (ART) is essential for the suppression of viral load, reduction of transmission risks, and enhancement of overall quality of life for HIV-positive individuals [11]. Stigmatization and discrimination can significantly hamper this adherence by preventing patients from attending appointments and following prescribed treatment regimen. Hence, this study investigates the extent to which stigma and discrimination affects adherence levels among HIV-positive individuals in ART clinics in Ondo State. The study aims to provide evidence that can inform policies, decisions and interventions, by focusing on patient experiences, to mitigate these problems and improve the quality of care for HIV positive individuals.
Research Questions
- What is the stigma and discrimination and human right violation experiences among HIV positive individuals enrolled in ART clinics in Ondo State?
- What is the level of drug adherence among HIV positive individuals attend ART Clinics in Ondo State
- Does any relationship exist between stigmatization and drug adherence among HIV positive individuals attending ART clinics in Ondo State?
Research Hypothesis
H0 = There is no significant association between stigma and discrimination of HIV positive individuals attending ART clinics in Ondo state and their level of drug adherence
LITERATURE REVIEW
Persistently held misconceptions and anxieties about HIV/AIDS have a detrimental impact on the disease’s prevention and treatment. In relation to HIV/AIDS, the use of metaphors such as “death,” “horror,” “punishment,” “shame,” “guilt,” and “otherness” has made matters worse and strengthened stigmatization and discrimination [12]. Moral judgment is another factor that fuels stigma. People believe that participating in “bad” behaviors like adultery, male-to-male intercourse, and injecting drugs is a personal decision made by PLWHA. To put it another way, they should feel embarrassed of themselves because they caused it. This embarrassment affects not just the individuals but also their families. Others might interpret it as God punishing PLWHA for their disobedience or abnormal conduct. As a result, people with HIV might not always take their medications as prescribed in order to hide the fact that, they are positive. Consequently, stigma and discrimination fuel the spread of HIV and undermine AIDS responses. [13] reaffirmed this, stating that stigma and discrimination have a detrimental impact on the transmission of HIV AIDS. In a similar vein, Nyblade et al. [14] emphasized stigma reduction as a crucial component of their HIV-AIDS project, which aims to eradicate AIDS by 2030.
METHODOLOGY
The research was conducted in Ondo State, Nigeria, which is situated in the country’s south-west geopolitical zone. With 18 Local Government Areas, Ondo State was established in 1976 from the former Western State. It is predominantly occupied by the Yorubas who speak various dialects of the Language such As Akoko, Akure, Apori, Idanre, Ijaro, Ikale, Ilaje, Ondo and Owo, Ondo State, which is indeed a microcosm of the Nigerian Nation [15]. The study utilized a cross-sectional descriptive study design. The population includes HIV positive individuals enrolled into supported ART and PMTCT sites in Ondo State.
Sample size was determined to be 432 using Cochran formular [16] as it is a standard method of randomization and identifies the limits of errors considered as the most essential items in the survey.
For this study, a multistage sampling technique was used.
First stage: The list of all facilities where HIV positive clients are supported on treatment (doing ART and PMTCT) within Ondo State was obtained. 4 facilities were selected by simple random sampling. The four facilities selected with estimated clients per clinic visitation on monthly basis are listed in table 1 below:
TABLE I
| S/No | Name of facilities | Average number of clients |
| 1 | HIV/AIDS Antiretroviral Therapy Centre, State Hospital, Ondo | 400 |
| 2 | University of Medical Science Teaching Hospital, Ondo | 320 |
| 3 | Comprehensive Health Centre, Moferere, Ondo | 240 |
| 4 | State Hospital, Ile-Oluji, Ondo | 200 |
| Total | 1160 |
Fig. 1 A sample line graph using colors which contrast well both on screen and on a black-and-white hardcopy
Second stage: The desired sample size was selected using stratified random sampling with proportional allocation of respondents from the selected facilities.
For HIV/AIDS Antiretroviral Therapy Center, State Hospital, Ondo
Number of clients in facility (400) x 422 = 146
Total number in 4 facilities (1160)
For University of Medical Science Teaching Hospital, Ondo = 116
For Comprehensive Health Center, Moferere, Ondo = 87
For State Hospital, Ile-Oluji, Ondo = 73
Third Stage: Then, using the facility register, the respondents were chosen using systematic sampling, with the sample percentage being established by the number of clients in the facility and the number of respondents to be chosen. First respondent was selected by simple random technique and subsequent respondents were selected using sampling fraction.
For this study, a semi-structured questionnaire which was pre-tested among HIV positive individuals in a facility in Osun State used as the survey instrument.
Ethical Consideration: An informed consent form was utilized where respondents had the liberty to participate or refrain from participation in the study. Those who agreed to participate were assured of the highest level of confidentiality and their data protected.
RESULTS
Of the 432 respondents, 272 (63%) are women, 226 (52.3%) are between the ages of 26 and 36, 194 (44.9%) are married and currently living with their spouse, 228 (52.8%) have a tertiary education, 226 (52.3%) are employed full-time, 322 (74.5%) are Christians, 307 (71.1%) are Yoruba, and 235 (54.4%) have had HIV/AIDS for 1 to 5 years, according to Table 2.
Table 2: Socio-demographics (N=432)
| Variable | Frequency | % |
| Sex | ||
| Male | 159 | 36.8 |
| Female | 272 | 63 |
| Transgender | 1 | 0.2 |
| Age in Categories | ||
| 15 – 25 | 44 | 10.2 |
| 26 – 36 | 226 | 52.3 |
| 37 – 47 | 123 | 28.5 |
| 48 – 58 | 26 | 6 |
| 59 – 69 | 8 | 1.9 |
| 70 – 80 | 2 | 0.5 |
| 81 – 91 | 3 | 0.7 |
| Marital status | ||
| Single | 144 | 33.3 |
| Married and spouse is currently living in house hold | 194 | 44.9 |
| Married and spouse is working away from the household | 37 | 8.6 |
| In a relationship but not living together | 26 | 6 |
| Divorced /separated | 25 | 5.8 |
| Widow / widower | 6 | 1.4 |
| Educational level | ||
| No formal education | 44 | 10.2 |
| Primary school | 82 | 19 |
| Secondary school | 78 | 18.1 |
| Technical college / university | 228 | 52.8 |
| Employment status | ||
| In full time employment | 226 | 52.3 |
| In part time employment | 11 | 2.5 |
| Self-employed (full time) | 90 | 20.8 |
| Self-employed (part time) | 62 | 14.4 |
| Not working at all | 43 | 10 |
| Religion | ||
| Christian | 322 | 74.5 |
| Moslem | 90 | 20.8 |
| Traditional | 20 | 4.6 |
| Ethnicity | ||
| Yoruba | 307 | 71.1 |
| Hausa | 35 | 8.1 |
| Igbo | 85 | 19.7 |
| Others Edo, Ijaw | 5 | 1.2 |
| Years of living with HIV/AIDS | ||
| 1-5 years | 235 | 54.4 |
| 6-10 years | 172 | 39.8 |
| Greater than 10 years | 25 | 5.8 |
Respondents Experience on stigma and discrimination
Table 3 above shows that , 10(2.3%) very often excluded from social gatherings due to HIV/AIDS, 7(1.6%) often excluded from religious activities or places of worship based on your HIV/AIDS status , 7(1.6%) often excluded from family activities or places, 15(3.5%) often physically assaulted or threatened, 15(3.5%) sometimes experienced sexual rejection as a result of positive HIV status, 18( 4.2%) often discriminated against by other people living with HIV/AIDS while 18(4.2%) had wife/husband had been discriminated by household due to HIV status.
Table 3: Respondents Experience on stigma and discrimination
| Variable | Not at all | Rarely | Often | Very often |
| Excluded from social gatherings or activities in the last 12 months | 357(82.6%) | 11(2.5%) | 54(12.5%) | 10(2.3%) |
| Exclusion from religious activities or places of worship | 409(94.7%) | 11(2.5%) | 5(1.2%) | 7(1.6%) |
| Exclusion from family activities or places of worship | 409(94.7%) | 12(2.8%) | 4(0.9%) | 7(1.6%) |
| Been gossip by others due to HIV/AIDS infection | 383(88.7%) | 14(3.2%) | 15(3.5%) | 20(4.6%) |
| In the last 12 months, how long were you verbally insulted /harassed. | 385(89.1%) | 18(4.2%) | 26(6.0%) | 10(2.3%) |
| In the last 12 months, how often were you physically assaulted? | 373(86.3%) | 18(4.2%) | 26(6.0%) | 15(3.5%) |
| In the last 12 months, how often did you experience sexual rejection? | 395 91.4%) | 18(4.2%) | 15(3.5%) | 4(0.9%) |
| In the last 12 months, how often were you discriminated against by PLW HIV? | 389(90.0%) | 11(2.5%) | 14(3.2%) | 18(4.2%) |
| In the last 12 months, how often did your spouse experience discrimination as a result of your HIV status? | 386 89.4%) | 8(1.9%) | 20(4.6%) | 18(4.2%) |
Adherence among respondents
Table 4: Self-reported adherence among respondents
| Variable | Yes | No |
| Have you been on ART? | 422(97.7%) | 10 (2.3%) |
| Do you sometimes forget to take your medicine? | 39(9%) | 393(91%) |
| Thinking back over the two weeks, have you missed any of your doses? | 31(7.2%) | 01(92.8%) |
| Sometimes when you feel poorly after you take your medicine, do you stop | 33(7.6%) | 99(92.4%) |
| Do you always take your medication at the appropriate time? | 389(90%) | 43(10%) |
| When you feel like your symptoms are under control, do you sometime stop taking your medication? | 31(7.2%) | 401(92.8%) |
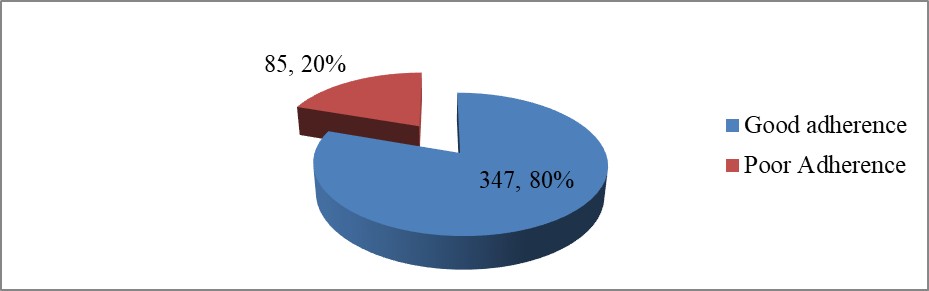
Fig. 1: summarized adherence among respondents
Summarily, out of 432 respondents, 85(20%) had poor adherence while 347 (80%) had good adherence as shown in Figure 1.
Association between Stigma, discrimination and adherence
Table 5: Association between Strigma, discrimination and adherence
| Correlations | |||
| Stigma Discrimination | Adherence | ||
| Stigma Discrimination | Pearson Correlation | 1 | .538 |
| Sig. (2-tailed) | .010 | ||
| N | 432 | 432 | |
Table 5 above shows that there is a significant association between Stigma and discrimination, and adherence ( P< 0.05) among HIV patients attending ART clinics in Ondo state. This shows that stigma and discrimination influenced the adherence of the patients to their drug regimen.
DISCUSSION
According to this study, adherence rate was 80%. This was similar to studies by [17] having reported adherence rates of 76-93%. Forgetting to take the prescription, drug toxicity, lack of availability, fear of losing the treatment’s benefits, and avoiding side effects were the main causes of non-adherence, according to this study. According to some additional research, the main causes of non-adherence in the African context were forgetting to take the medication and not having the funds to travel to an ART clinic ([18]. Additionally, education has affected adherence in a number of ways, such as by making it easier to communicate with medical professionals. The majority of patients with poor adherence in our study were illiterate, meaning they had a lower level of education.
This study also showed that there was a low level (25%) of stigma and discrimination among the patients. This low level of stigma and discrimination has in turn translated into a high rate of adherence among the patients. Since the test for hypothesis showed clearly a significant association between stigma and adherence. Hence it is safe to say that the low levels of stigma and adherence have led to a high level of adherence among the patients. Since the patients did not face high rate of stigma, they had no reason not to adhere to their treatment regimen. The study showed that the 20% low adherence was as a result of other reasons already discussed in the first paragraph.
CONCLUSION
This study has been able to provide evidence from some ART clinics in Ondo State that stigma and discrimination among HIV patients has a significant effect on patients’ adherence to their treatment regimen. The low levels of stigma experienced by the patients have yielded in a good level of adherence by those patients. Also, the level of education of patients can impact their adherence to treatment.
ACKNOWLEDGMENT
The authors declare that there is no potential conflict of interest or any personal or other relationships with other people or organisations that could influence this work.
REFERENCES
- De Cock, K. M., Jaffe, H. W., & Curran, J. W. (2021). Reflections on 40 Years of AIDS. Advances in Clinical Immunology, Medical Microbiology, COVID-19, and Big Data, 231-245.
- WHO, Health in 2015: From MDG to SDG, World Health Organization, Geneva, Switzerland, (2015)
- Obeagu, E. I., & Obeagu, G. U. (2023). A Review of knowledge, attitudes and socio-demographic factors associated with non-adherence to antiretroviral therapy among people living with HIV/AIDS. Int. J. Adv. Res. Biol. Sci, 10(9), 135-142.
- Oludayo, F. A. (2022). Analysis of factors influencing stis transmission and access to stis-related services among youths in southwest nigeria.
- Hempel, S., Ferguson, L., Bolshakova, M., Yagyu, S., Fu, N., Motala, A., & Gruskin, S. (2021). Frameworks, measures, and interventions for HIV-related internalized stigma and stigma in healthcare and laws and policies: systematic review protocol. BMJ open, 11(12), e053608.
- Bwosh, S. D. (2022). HIV and AIDS and the stigmatization of woman by men in Nigeria: a pastoral care intervention strategy (Doctoral dissertation, Stellenbosch: Stellenbosch University).
- Snow, S. (2022). Therapy & HIV positive clients: exploring aspects that promote psychosocial adjustment using constructivist grounded theory (Doctoral dissertation, London Metropolitan University).
- Yu, C. H., Huang, C. Y., Ko, N. Y., Tung, H. H., Huang, H. M., & Cheng, S. F. (2021). The lived experiences of stigmatization in the process of HIV status disclosure among people living with HIV in Taiwan. International journal of environmental research and public health, 18(10), 5089.
- Hack, S. M., Muralidharan, A., Brown, C. H., Drapalski, A. L., & Lucksted, A. A. (2020). Stigma and discrimination as correlates of mental health treatment engagement among adults with serious mental illness. Psychiatric Rehabilitation Journal, 43(2), 106.
- Crawford, T. N., Silverstein, S., Spaulding, T., Cheribin, D., Murray, T., Rivera, J., & Wilcher, K. (2023). Exploring the impact of experiences with every day and major discrimination and HIV-related stigma on engagement in HIV care among older African Americans living with HIV. Journal of Racial and Ethnic Health Disparities, 10(4), 1910-1917.
- Bomfim, I. G. D. O., Santos, S. D. S., & Napoleão, A. A. (2022). Adherence to antiretroviral therapy in people living with HIV/AIDS: A cross-sectional study. AIDS patient care and STDs, 36(7), 278-284.
- Dumoulin, J. (2023). Stigma isn’t all bad: How storytelling and monster metaphors in Anita Blake challenge existing notions of health-related stigma and generate productive stigma outcomes (Doctoral dissertation, Université d’Ottawa/University of Ottawa).
- Kumar, V. (2023). Stigma and Discrimination Related HIV-AIDS. Journal of Research in Social Science and Humanities, 2(9), 20-28
- Nyblade, L., Mingkwan, P., & Stockton, M. A. (2021). Stigma reduction: an essential ingredient to ending AIDS by 2030. The lancet HIV, 8(2), e106-e113.
- Omotosho, O. F., ologbenla, d. K., alex, o. O., & omotosho, o. F. (2020). The people of ondo kingdom and their culture: a historical survey and political underpinning. Ijasos-international e-journal of advances in social sciences, 6(17), 688-694.
- Cochran, W. G. (1977). Sampling techniques. Johan Wiley & Sons Inc.
- Vincent, C. C. N., Obeagu, E. I., Agu, I. S., Ukeagu, N. C., & Onyekachi-Chigbu, A. C. (2021). Adherence to Antiretroviral Therapy among HIV/AIDS in Federal Medical Centre, Owerri. Journal of Pharmaceutical Research International, 33(57A), 360-368.
- Peter, M. (2022). Factors contributing to non adherence to antiretroviral therapy among hiv clients attending art clinic at ndejje health centre iv kampala district.