
The Voices of Recovery: Patient and Caregiver Perspectives on Psychosocial Interventions in Harare, Zimbabwe.
- Silindweyinkosi Chinoda
- Sam Takawira
- Joyce Machigere
- Elizabeth Tanyanyiwa
- Herbet Zirima
- 90-97
- Mar 19, 2025
- Health
The Voices of Recovery: Patient and Caregiver Perspectives on Psychosocial Interventions in Harare, Zimbabwe.
1Silindweyinkosi Chinoda, 2Sam Takawira, 3Joyce Machigere, 2Elizabeth Tanyanyiwa, 4Herbet Zirima
1Identity Consultancy Intern Counselling Psychologist
2Registered Counselling Psychologist
3Lecturer of Psychology, Women’s University in Africa
4School of Medical & Health Sciences, Great Zimbabwe University
DOI: https://dx.doi.org/10.47772/IJRISS.2025.917PSY0011
Received: 06 February 2025; Accepted: 17 February 2025; Published: 19 March 2025
ABSTRACT
This study investigated the perceptions of patients and caregivers towards psychosocial interventions at Tariro Halfway Home, a rehabilitation centre for mental health patients in Zimbabwe. The primary objective of this evaluation was to conduct a comprehensive assessment of psychosocial interventions at Tariro Halfway Home. This involved identifying and describing the current range of psychosocial interventions offered by caregivers, exploring the efficacy of these interventions in achieving desired patient outcomes, evaluating the level of community and family involvement in the delivery and support of these interventions, and ultimately, identifying key areas for improvement in the efficacy, delivery, and overall effectiveness of psychosocial interventions at the home. Using a qualitative case study approach, data were collected through focus group discussions with patients and individual interviews with caregivers. The findings revealed diverse psychosocial interventions, including practical skills training, self-management skills training, and social interaction activities. While participants reported positive outcomes such as improved mental health and enhanced quality of life, challenges such as resource constraints, patient engagement, and family involvement were identified. The study highlights the importance of a multi-faceted approach that addresses the individual needs of patients, fosters family involvement, and ensures adequate resources for effective intervention delivery.
Key Words: Psychosocial Interventions, Recovery, family involvement, mental health
INTRODUCTION
Psychosocial interventions hold significant promise in addressing the complex needs of forensic mental health patients, encompassing both mental health and criminogenic factors. However, a scarcity of rigorous evaluation studies limits our understanding of their effectiveness within this population. This study aims to investigate perceptions of psychosocial interventions towards psychiatric patients, utilizing Tariro Halfway Home as a case study.
Globally, an estimated 970 million individuals experience mental disorders at any given time. This includes 121 million with depression, 24 million with schizophrenia, and 37 million with dementia (WHO, 2020). In 2019, mental illness accounted for approximately 12.3% of the global burden of disease. By 2025, unipolar depressive disorders are projected to become the second leading cause of disability worldwide.
Africa, home to over one billion people, represents 14.8% of the world’s population. Despite its rich diversity in languages, religions, and cultures, Africa faces significant mental health challenges. While stressors are universal, specific patterns vary across time and place. African populations currently grapple with emotional distress arising from ethnic conflicts, wars, immigration, refugee crises, substance abuse, HIV/AIDS, and other socio-economic factors (Stein DJ, 2013).
Studies from Nigeria, a low-income country, report a 12-month prevalence of mental disorders of 4.7%, consistent with findings from other low-income nations (Benjet et al., 2016). In contrast, South Africa, a middle-income country, exhibits a higher lifetime prevalence of mental disorders at 30.3% (Olasoji et al., 2017). However, this figure remains lower than that observed in many high-income countries (Boen, Dalgard, and Bjertness, 2012).
Despite the significant burden of mental illness, treatment access remains limited across Africa. In Nigeria, only 8% of individuals with severely disabling disorders received treatment in the preceding 12 months (Olasoji et al., 2017). South Africa fares slightly better, with 25.5% of those with mental disorders accessing treatment (Inge et al., 2009). Overall, a substantial treatment gap persists, with 76.3% to 85.4% of individuals with serious mental disorders in developing countries lacking access to treatment compared to 35.5% to 50.3% in developed countries (Boen, Dalgard, and Bjertness, 2012). Moreover, even when treatment is sought, evidence-based interventions are often unavailable in low- and middle-income countries.
The mental health needs of marginalized populations, particularly the poor, are often underserved. Poverty exacerbates mental health issues, and inequalities in service delivery further marginalize these communities (Ngui et al., 2010).
Stigma associated with mental illness poses significant challenges for both patients and their families. Research indicates that stigma can erode the morale of caregivers, leading to withdrawal from support networks (Becker et al., 2010). This is particularly relevant in contexts like Zimbabwe, where families often conceal mental illness to avoid social discrimination.
Zimbabwe, like many developing countries, faces significant underfunding and undertreatment of mental health issues. 1 The scarcity of public mental health facilities is a major concern. While provincial hospitals have psychiatric units, many lack adequately trained staff. For instance, Ingutsheni Central Hospital, one of the largest psychiatric hospitals in Southern Africa, has only one trained clinical psychologist (Sithole, 2010). This severe shortage of mental health professionals exacerbates the treatment gap, particularly for the most vulnerable populations. 2
Recognizing the limitations of traditional approaches, there is a growing emphasis on developing and implementing effective psychosocial interventions. These interventions aim to address the multifaceted needs of individuals with mental illness, including emotional, social, and behavioral challenges. However, robust evidence on the efficacy of these interventions in the Zimbabwean context is lacking. This study seeks to address this gap by assessing perceptions of psychosocial interventions towards psychiatric patients at Tariro Halfway Home.
This study underscores the critical need for further research and development of effective psychosocial interventions for psychiatric mental health patients. By understanding the perceptions of these interventions and evaluating their impact, we can work towards improving mental health outcomes for this vulnerable population.
Aim
The study aimed to assess patients’ and caregivers’ perceptions of the psychosocial interventions provided at Tariro Halfway Home.
Objectives
- Identify the psychosocial interventions provided by caregivers to patients at Tariro Halfway Home.
- Explore the efficacy of the psychosocial interventions at Tariro Halfway Home.
- Evaluate the involvement of the community and families in the psychosocial interventions at Tariro Halfway Home.
- Identify ways of improving the efficacy of psychosocial interventions at Tariro Halfway Home.
Research Questions
- What psychosocial interventions are being provided by caregivers to patients at Tariro Halfway Home?
- How effective are the psychosocial interventions at Tariro Halfway Home?
- To what extent are the community and families involved in psychosocial interventions at Tariro Halfway Home?
- How can the psychosocial interventions at Tariro Halfway Home be improved to enhance their effectiveness?
Assumption
- Psychosocial interventions have an impact on the mental health of patients and may assist them in re-entering society.
Conceptual Framework
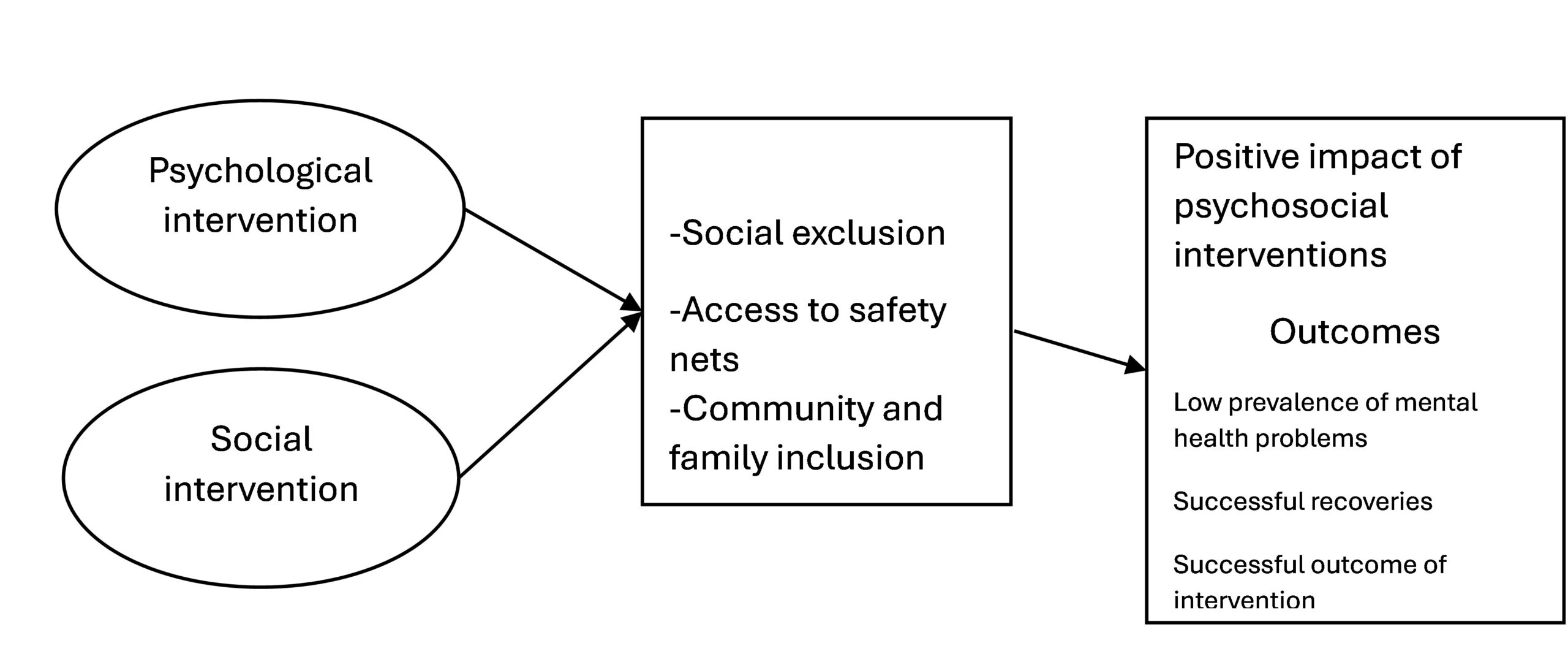
Figure 1: Conceptual model. Source: Chinoda, 2024
The conceptual framework emphasizes the interconnectedness of psychological and social interventions in successful patient outcomes. It highlights the influence of social factors, such as social exclusion and access to safety nets, on the effectiveness of interventions. The model posits that successful interventions should lead to improved mental health outcomes, reduced prevalence of mental health problems, and successful reintegration into society.
METHODOLOGY
Research Approach
This study employed a qualitative case study approach to gain an in-depth understanding of the perceptions and experiences of patients and caregivers at Tariro Halfway Home.
Research Design
This study employs an exploratory case study research design. As Saunders et al. (2012) outlined, a case study involves an empirical investigation of a specific phenomenon using multiple sources of evidence. In this research, the focus is on understanding the perceptions of patients and caregivers towards psychosocial interventions at Tariro Halfway Home, a mental health rehabilitation center. While acknowledging the generalizability limitations inherent in case studies, Aaker et al. (2011) emphasize the valuable insights they provide into the characteristics and relationships within the studied unit. A case study design was deemed appropriate as it allows for an in-depth exploration of a specific phenomenon within its real-world context (Yin, 2014), given the emphasis on eliciting patients’ subjective experiences.
Population and Sampling
The study targeted two populations: (a) psychiatric inpatients at Tariro Halfway Home and (b) their caregivers. A combination of purposive and convenience sampling was employed to select participants. Ten psychiatric inpatients and three caregivers who were available at the institution were selected. The patients were discharged from the psychiatric hospital at varying timelines and were being rehabilitated at the home.
Data Collection
Data were collected through focus group discussions with patients and individual in-depth interviews with caregivers. Semi-structured interview guides were developed to elicit detailed information about their experiences with psychosocial interventions.
Research procedure
The researcher sought to understand the perceptions towards psychosocial interventions from the view of patients and caregivers, hence10 psychiatric in-patients were physically involved in a focused group discussion at the home. This has the advantage that, participants are observed in a completely natural and unchanged environment so as not to affect them. These assist in finding out if they are fully prepared to accept their condition through psycho-education. 3 caregivers had a one-on-one interview in trying to find out their perceptions of the psychosocial interventions that are offered to patients.
Data Analysis
Thematic analysis was used to identify key themes and patterns within the qualitative data. This involved careful reading, coding, and interpretation of the data to understand the underlying meanings and perspectives (Braun & Clarke, 2006).
Ethical considerations
This data involves key informants who are psychiatric in-patients as well as their caregivers. As such some ethical considerations were adhered to.
- The research aimed at maximizing the benefit of psychiatric patients and society and minimizing risk and harm.
- The rights and dignity of patients and caregivers were respected.
- Participation was voluntary and respondents were appropriately informed.
- The research was conducted with integrity and transparency.
- The research respected the confidentiality and anonymity of the patients and caregivers.
- Independence and impartiality of the research were highlighted and maintained, and where conflicts of interest could not be avoided, they were made explicit.
KEY FINDINGS AND ANALYSIS
Diverse Range of Psychosocial Interventions:
A variety of interventions were observed, including practical skills training (gardening, crafts), self-management skills training, and social interaction activities. This aligns with best practices in psychosocial rehabilitation, which emphasize holistic approaches that address not only mental health symptoms but also functional limitations and social integration needs (World Health Organization, 2010).
Patient A highlighted that “these mattresses sell like hotcakes at the market”
Further responses indicated that several discharged patients relocated to different areas of the country. One example was of a patient running a bed-making business, while the majority had established themselves at a furniture complex. Patient H commented that,
“How can I sleep on the floor whilst I can make a bed”.
One of the caregivers (caregiver A) at the home concurred with the patient during FGD, by saying
“We try to keep them busy with work therapies such as mattress covering, poultry, and gardening, not only as jobs but also as healing therapies.”
The rich soils and the availability of borehole water present an opportunity for the centre to train patients on how to grow different crops and market them. In this regard, patient F claims to have bought the jeans he was wearing with the money he got from selling produce from his garden portion,
“I bought these jean trousers with the money I got from selling vegetables in my garden”.
In this regard, though productivity can be viewed as an important component, the patient is made into an important and meaningful contributor to the community. Patient G remarked that,
“these kinds of jobs are making us be recognized in the community”.
Perceived Benefits of Interventions:
1. Improved mental health: Patients reported reduced symptoms of depression and anxiety.
A blend of assertiveness training and exercise can effectively reduce anxiety and depression. The improvements in mood result from exercise boosting blood circulation, which helps alleviate psychological stress. Patient B concurred with the statement;
“When you are running, gardening, or taking care of the chickens, your focus is entirely on the task at hand. This concentration helps take your mind off stress, allowing you to feel more relaxed and grounded”.
Enhanced quality of life: Interventions provided a sense of purpose and improved daily living skills. Interventions provided a sense of purpose and improved daily living skills. This supports the emphasis on improving quality of life as a key outcome of psychosocial rehabilitation (World Health Organization, 2010).
However, caregiver C remarked that self-management and assertiveness training was rather a challenge for some patients; in initial sessions were difficult to work with and was asked to elaborate the caregiver said,
“some come to the home in a filthy state and refuse to bath and we learn to be perseverant with such a person until he/she learns to do it by him/herself”
After training, caregivers are taught to be perseverant, which assists them in coping with the patients’ general weaknesses.
Being well-informed about the illness was seen as a major benefit by the patients. Patient J remarked,
“we are taught that if you fail to take your drugs or if you stress too much it affects your healing process”
2. Reduced reliance on medication: In some cases, patients reported decreased medication dependence. While medication is often essential, Leff et al., 2014 express that psychosocial interventions can help individuals develop coping mechanisms and self-management skills that reduce reliance on medication over time.
Patient D promoted that,
“we are taught to take care of ourselves so that the illness cannot worsen”
Assertiveness interventions on psychiatric patients were designed to improve one’s assertive beliefs and behaviors which can help one change how they view themselves and establish self-confidence. Patient A was asked to explain how he benefited from this training and the response was;
“you have to change your perception that you are crazy as they say in the community, this is just a disease like BP or diabetes”
Thus, one develops a positive attitude towards the illness such as that one is not affected by what the society is saying about mental health illness.
Challenges and Considerations:
- Resource constraints: Limited funding and staff shortages were significant challenges. Limited funding and staff shortages are significant challenges, echoing common challenges faced by mental health services in resource-limited settings (World Health Organization, 2010).
- Patient engagement: Maintaining patient motivation and engagement in interventions was crucial.
- Family involvement: While family involvement can be beneficial, inconsistent family support can impact patient outcomes. This emphasizes the critical role of family involvement in mental health recovery (Lebowitz & Weissman, 2005).
Patient B, a 33-year-old woman, had a poignant story to share. She was quiet and struggled to open up during the session, only speaking about her family’s involvement. Despite being admitted to the home two years ago, she has not had a single visitor. She shared,
“No one has visited me since my admission. I left my child behind, and I do not even know how much she has grown”
Hence, it was noticed with greater concern that, patients who were visited regularly showed jovial mood and contributed more to the discussion whilst those who had not had any relative visit them sounded withdrawn and contributed less.
Efficacy of Interventions
The effectiveness of interventions varied depending on factors such as patient engagement, caregiver support, and the quality of intervention delivery. Maintaining patient motivation and engagement in interventions is crucial. This aligns with research highlighting the importance of patient engagement in the success of any treatment program (Dunn et al., 2010).
Caregiver 2 remarked that,
“the success rate of these interventions was 50-50”.
Thus, success depends on all parties involved. Both patients and families must play their part accordingly for the learned skills to be effective and rewarding. Major evaluators are follow-ups which are a must, and these are done to see if both the patient and the family were utilizing the skills acquired at the home. The observation that follow-up is crucial for evaluating long-term outcomes aligns with existing evidence on the importance of ongoing support and maintenance strategies after discharge from treatment (Bond et al., 2001). The caregiver highlighted that due to the lack of transport at the centre, it was a challenge to visit all discharged patients, hence those close to the centre enjoyed the benefit.
The major objective deducted from the patients about self-management is that they play a major role in the process of managing themselves. Patient I added and said,
“if you do not follow the teachings, you are the one who gets affected, the healing process also lies with us”.
Perceptions of Caregivers
Caregivers emphasized the importance of family involvement and highlighted the need for ongoing training and support. Involving family members in psychosocial treatment was to assist both the patient and the family in gaining insight into the illness such that when the patient is discharged, the therapy also continues at home. Caregivers emphasized the importance of family involvement, aligning with research highlighting the crucial role of family support in mental health recovery (Lebowitz & Weissman, 2005). Caregiver 3 pointed out that,
“It helps those families that attend family intervention days that are done after every 3 months, you can see that this family has sound social support towards their ill relative”
CONCLUSIONS
The findings suggest that psychosocial interventions have the potential to improve the mental health and well-being of psychiatric mental health patients. However, several challenges remain, including resource constraints, ensuring patient engagement, and optimizing family involvement.
RECOMMENDATIONS
Strengthening Interventions:
- Implement individualized treatment plans based on individual patient needs.
- Enhance family involvement through family therapy and support groups.
- Provide ongoing training and supervision for caregivers.
Improving Resource Allocation:
- Advocate for increased funding to support the implementation and sustainability of psychosocial interventions.
- Utilize technology to enhance access to mental health services.
Promoting Community Engagement:
- Foster community partnerships to provide support and resources for patients after discharge.
Conducting Rigorous Evaluation:
- Implement a robust system for monitoring and evaluating the effectiveness of interventions.
This study provides valuable insights into the perceptions and experiences of patients and caregivers regarding psychosocial interventions. The findings can inform the development and improvement of mental health services for psychiatric mental health patients in Zimbabwe and other similar settings.
REFERENCES
- Aaker, D. A., Kumar, V., & Day, G. S. (2011). Marketing research. John Wiley & Sons
- Araya, R., Rojas, G., & Fritsh, C. (2013). Task shifting for mental health care in low- and middle-income countries: A review. World Psychiatry, 12(1), 10-17.
- Auerbach, R., et al. (2016). The epidemiology of mental disorders in Nigeria: Results from the WHO World Mental Health Survey Initiative. Journal of Affective Disorders, 190, 107-114.
- Becker, A. E., Greenberg, J. P., & Boyd, J. (2010). Stigma, depressive symptoms, and coping among family caregivers of individuals with severe mental illness. Community Mental Health Journal, 46(3), 255-264.
- Benjet, C., et al. (2016). Prevalence, severity, and treatment of DSM-IV mental disorders in Nigeria: Results from the WHO World Mental Health Survey Initiative. Journal of Affective Disorders, 190, 107-114.
- Boen, F., Dalgard, O. S., & Bjertness, E. (2012). Treatment gaps in mental health care in low- and middle-income countries: A systematic review. BMC Psychiatry, 12(1), 1-12.
- Bond, G. R., Drake, R. E., Mueser, K. T., & Swartz, M. S. (2001). Psychosocial rehabilitation for severe mental illness. New England Journal of Medicine, 345(25), 1810-1818.
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101.
- Creswell, J. W. (2010). Research design: Qualitative, quantitative, and mixed methods approaches. Sage.
- Dunn, L. L., Nowack, K., & Andersen, R. N. (2010). Patient engagement: A framework for action. Milbank Quarterly, 88(4), 483-518.
- Inge, K. E., et al. (2009). Prevalence, correlates, and service utilization for mental disorders in South Africa: Results from the South African Stress and Health Study. Social Psychiatry and Psychiatric Epidemiology, 44(10), 790-800.
- Lebowitz, B. D., & Weissman, M. M. (2005). The role of family in the course of depressive disorders. Journal of Clinical Psychiatry, 66(Suppl 10), 2-7.
- Leff, J., Kuipers, L., Berkowitz, R., Eberlein-Fries, R., & Sturgeon, D. (2014). Family interventions for schizophrenia: A randomised controlled trial. British Journal of Psychiatry, 164(2), 145-153.
- Ngui, E. M., et al. (2010). Mental health and poverty: Conceptual and methodological issues. International Journal of Mental Health Systems, 4(1), 1-10.
- Olasoji, H. A., et al. (2017). The epidemiology of mental disorders in Nigeria: Results from the WHO World Mental Health Surveys. World Psychiatry, 16(2), 128-136.
- Saunders, M., Lewis, P., & Thornhill, A. (2012). Research methods for business students. Pearson Education.
- Sithole, N. (2010). Mental health care in Zimbabwe: Challenges and opportunities. African Journal of Psychiatry, 13(4), 230-235.
- Stein, D. J. (2013). Mental health in Africa: Challenges and opportunities. World Psychiatry, 12(2), 104-109.
- World Health Organization (WHO). (2020). Mental disorders. [Online]. Available: https://www.who.int/health-topics/mental-health
- World Health Organization. (2010). Mental Health Action Plan 2013-2020. [Online]. Available: https://www.who.int/publications/i/item/9789241506021