
Towards the Exploration of Social Considerations against the Intention to Use the Modern Contraception among Women in Union in Burundi
- Jean François Régis Sindayihebura
- Franklin Bouba Djourdebbé
- Didier Nganawara
- Emmanuel Barankanira
- Désiré Manirakiza
- Willy-Marcel Ndayitwayeko
- Jean Nsabimana
- René Manirakiza
- 1265-1281
- Apr 9, 2024
- Social Media
Towards the Exploration of Social Considerations against the Intention to Use the Modern Contraception among Women in Union in Burundi
Jean François Régis Sindayihebura*1, Franklin Bouba Djourdebbé2, Didier Nganawara2, Emmanuel Barankanira3, Désiré Manirakiza4, Willy-Marcel Ndayitwayeko5, Jean Nsabimana1, René Manirakiza1
1Department of Geographic, Environment and Population Sciences – Faculty of Arts and Social Sciences – Center for Research and Studies on the Development of Societies in Reconstruction (Centre de Recherche et d’Etudes sur le Developpement des Sociétés en Reconstruction-CREDSR) – University of Burundi –Burundi
2Institute for Training and Demographic Research (Institut de Formation et de Recherche Démographiques – IFORD) – University of Yaounde 2 – Cameroun
3High Teachers’ Training School of Burundi (Ecole Normale Supérieure du Burundi – ENS) – Burundi
4Department of Socio-Anthropology – Faculty of Arts and Social Sciences – University of Burundi – Burundi
5Departmenr of Rural Economy – Faculty of Economics and Management – University Research Center for Economic and Social Development (Centre Universitaire de Recherche pour le Developpement Economique et Social – CURDES) – University of Burundi – Burundi
*Corresponding Author
DOI: https://dx.doi.org/10.47772/IJRISS.2024.803093
Received: 13 February 2024; Accepted: 06 March 2024; Published: 09 April 2024
ABSTRACT
Burundi, which intends to reduce its fertility from 5.5 to 3 children per woman, has seen the level of intention to use modern contraception decreasing from 66% to 53% between 2010 and 2016-2017. The aim of this study is therefore to explore the social considerations leading to non-intention to use modern contraception among women in union in Burundi. The study proceeds by thematic analysis of the content of the transcripts of 10 focus group discussions conducted in 5 provinces of the country. The results of the analysis show that these include side-effects experienced or feared, the absence of side-effect treatment services, the failure of some methods to prevent pregnancy, and religious opinions. In terms of social interactions, these include religious influences, myths and rumors, and the effects of social cohabitation. Women’s inability to self-determine their contraceptive decisions is also important. These results show that the socio-cultural influence of the community dominates women’s intention to use modern contraception, where the supply of family planning services does not attract users, due to a lack of side-effect treatment. To break down socio-cultural resistance, subsequent interventions would tend to reinsure potential clients of family planning services of the availability of the side-effect treatment package.
Keywords: social considerations, intention, modern contraception, women in union, Burundi
INTRODUCTION
Referring to the classification of countries according to the stage reached in their demographic transition (David, 2015), Burundi is classified among countries of uncompleted transition. With an average of 5.5 children per woman, Burundi counts among nations of highest fertility in Africa (Tabutin & Schoumaker, 2020). Given its rapid population growth since the independence or before, this high fertility makes it to be classified among the most densely populated countries. The consequences of this demographic growth are the socio-economic conditions that require birth planning. In a country where 90% of the population declare to live from traditional agriculture, the land no longer produces enough subsistence in a context of climate change, hence the deplorable health situations of malnutrition, anemia, etc. (Kamuragiye & Buruzingo, 2019; Sindayihebura, Manirakiza, et al., 2022; Sindayihebura & Nkunzimana, 2020). In basic social services such as education and health, data show that acceptable standards for quality services are exceeded (ISTEEBU, 2019; Kamuragiye & Buzingo, 2019).
To face these challenges of discrepancy between demographic data and the socio-economic situation, National Development Plan of Burundi consecrates the reduction of fertility to 3 children per woman and the reduction of the average annual population growth rate from 2.4% to 2% (République du Burundi, 2018). Despite this need and the ultimate goal of controlling fertility, family planning indicators are not promise of achieving these objectives. The rate of modern contraceptives use among women of childbearing age is just 23% (ISTEEBU & ICF International, 2017). The annual increase in this use is only 0.5% when the target is 1.5% (Kamuragiye & Buzingo, 2019). Furthermore, the intention to use modern contraception has fallen between 2010 and 2016-2017, from 66% to 53% (ISTEEBU & ICF International, 2017).
Facing these findings, previous studies that focused on understanding why women do not intend to use contraception in such a restrictive context. They explored the profile of women with no intention of using modern contraception (Sindayihebura et al., 2023) and studied the sources of the decline in the level of intention to use it (Sindayihebura, Ndayitwayeko, et al., 2022). In searching explanatory factors, the influence of household poverty (Sindayihebura, Nganawara, & Manirakiza, 2022b), that of the socio-economic weight of the community (Sindayihebura, Nganawara, & Manirakiza, 2022a), that of gender relationships (Sindayihebura et al., 2022) and that of the family planning services supply (Sindayihebura et al., 2022). However, the results of these studies have not sufficiently demonstrated the role of opinions and attitudes regarding contraception of the women whose non-intention to use is increasing in proportion. Although gender relationships have been analyzed, the role of social interrelations has also not been sufficiently elucidated. Also, when studying the influence of the family planning services supply, the analysis was limited to the influence of knowledge and awareness, without involving that of the methods offered and the treatment of their effects.
The studies conducted in other contexts found that the social considerations against the intention to use modern contraceptives are made of negatives opinions and attitudes like the fear of side-effects (Agha, 2010; Gebremariam & Addissie, 2014; Negewo, 2010), the myths and rumors (Babalola et al., 2015; Meskele & Mekonnen, 2014; Rutenberg & Watkins, 1997) and religion mistrusts (Ahuja et al., 2020; Tiruneh et al., 2016). The social interactions referring to important referents like the sexual partners, friends, relatives or doctors are also mentioned among the social considerations against the intention of contraception use (Bosompra, 2001; Rutenberg & Watkins, 1997). In addition, the lack of self-efficacity is indexed as the social factor that is against the use of modern contraception (Agha, 2010; Wuni et al., 2018). These studies, made in different contexts show that the social constructions around a phenomenon like contraception use may harm its effectiveness. Thus, they give the reason of being of this study in the Burundian context and constitute for it the important references.
Understanding opinions and attitudes involves beliefs as well as social interrelationships, and requires the expression of those who live the social and cultural context in which the phenomenon under study prevails (De Loenzien, 2006). Thus, this study uses a qualitative approach to analyze the social considerations that goes against the intention to practice modern contraception. Its aim is to explore the social considerations at the basis of resistance to contraception, in a context that nevertheless requires it. The following section covers methodological aspects, presentation and discussion of the results, and ends with a conclusion.
METHODOLOGY
- Data collection
In order to explore the social considerations reported by the women who experience them, this study adopted a qualitative approach. Qualitative data were collected from women in union, aged between 15 and 49, who were visited in five provinces of Burundi. These were the provinces of Kirundo (North region), Karusi (Centre region) and Ruyigi (East region), Makamba (South region) and Bubanza (West region). In each province, one commune was chosen, resulting in five communes being targeted. These were Gisuru in the East, Musigati in the West, Shombo in the Center, Kirundo in the North and Mabanda in the South (Figure 1). The choice of these provinces and communes was a reasoned one, based on the principal of regional diversity. The choice of participants also took into account their place of residence. In each commune, the focus groups were held in the urban center and in a rural area a little further away (Figure 1). A total of ten (10) focus groups were conducted. The women who took part in the interview were chosen at random, while avoiding family ties that could compromise the accuracy of the statements. Thus, a woman and her mother-in-law, a mother and her daughter, or a woman and her sister-in-law could not participate in the same activity.
The data collection approach used was that of focus groups. This is a technique that enables us to obtain a wide range of ideas on a given subject, to gain a complete understanding of the topic under study, and to provide an accurate picture of reality as it is experienced (ROCARE & ADEA, 2006). This method was therefore suited to the needs of this study, whose aim was to understand opinions, attitudes and social interactions that previous studies had failed to capture.
The interview guides were structured to capture opinions, attitudes and social interactions against contraceptive intentions in Burundi. Thus, the interview questions were structured around the components of the theories of reasoned action and planned behavior, and the four dimensions of ideation. It was necessary to look for data that serve to show how the dimensions and attitudes of ideation are linked to contraceptive non-intention beyond the socio-economic, cultural and demographic factors that were already explored (Babalola et al., 2015). The interview guide was structured around four main themes: (1) knowledge of contraception, (2) opinions and attitudes towards contraception, (3) the influence of social interactions and (4) contraceptive self-efficacy coupled with control of perceived behavior.
Data collection took place from September 12 to 16, 2022 and over a period of 5 days. Prior to the main data collection, a pre-test of the interview guides was carried out in the city of Bujumbura. The information gathered during the pre-test was transcribed, coded, analyzed and criticized. The interview guides were then redesigned on the basis of the comments made.
- Analysis methods
The data collected was analyzed using the technique of thematic content analysis (Andreani & Conchon, 2005; Krippendorff, 2004). Thus, data transcription was carried out at the same time as pre-coding according to the four themes-dimensions of ideation (Auerbach & Silverstein, 2003; Larivière & Corbière, 2014; Paillé & Mucchielli, 2021). Analysis of the transcribed data consisted in identifying the main ideas by theme, with explanations provided (Andreani & Conchon, 2005). This analysis of opinions, attitudes and social interactions was mainly manual, to mean without statistical processing using analysis software (Andreani & Conchon, 2005). However, Microsoft Word was the essential tool for transcription, thematic classification and highlighting during content analysis.
- Ethical research
In order to conform to the obligation of research ethics, the fieldwork was endorsed by a research attestation issued by the Research Office of the University of Burundi, and a mission order issued by the Faculty of Arts and Social Sciences. At the time of the country inside visit, the above-mentioned documents were presented to the local authorities. The latter endorsed the mission order, which gave legitimacy to the collection at local level. In each case, the head of the hill or quarter was involved as the first-level local authority and as the mobilizer of participants in the focus groups. Before starting the group discussion, the consent form was read and approved by the participants. As is customary in data collection and analysis, the consent form stipulated the voluntary participation of the respondents, their freedom to leave if the need arose, the recording of discussions, the non-disclosure of the respondents’ identities, the admissibility of all answers and the recovery of travel expenses.
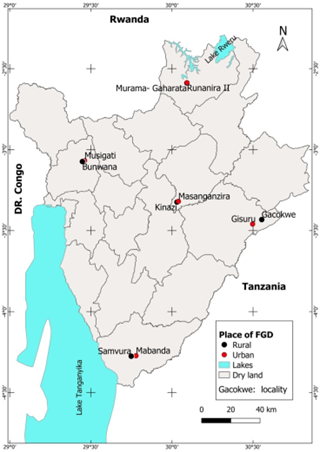
Figure 1: Places of qualitative data collection in 2022
Source: Authors, using places of focus group coordinates
RESULTS
Transcription and analysis were carried out according to a thematic classification of the factors evoked by the focus group participants. The results were also presented according to the four themes corresponding to the dimensions of ideation.
- Influence of knowledge of modern contraception methods
The results show that all the women interviewed are aware of these methods. In responding, they mentioned sources of information, supply channels and the importance accorded to these methods. Some also mentioned certain aspects of contraceptive availability and the likelihood of using them.
With regard to sources of information, N.A.M., 40, Gisuru, mentions the awareness-raising sessions that take place every morning before the start of services in health facilities, or the community animations carried out by Community Health Workers. In her view, as human beings are likely to fall ill, and most seek treatment in health centers, everyone needs to be aware of the methods taught there. She goes on to say:
No one is immune to disease, just as no one can escape being kept in hospital; and it is in the health centers that awareness-raising takes place; moreover, that’s why the Community Health Workers are there….. That’s why I wouldn’t say there’s anyone who doesn’t know about modern contraception.
For N.V., 30, Shombo, there may be women who haven’t yet used these methods, but there can’t be those who haven’t yet heard about them. N.S., 35, Gisuru, mentions secondary schoolbooks to show that sources of knowledge about contraceptive methods are various and that everyone has to be aware of their existence.
Thus, knowledge of contraception does not appear to be a factor in non-intention to use modern contraception in the Burundian context, where over 97% of women declare having heard of at least one modern contraceptive method (ISTEEBU & ICF International, 2017). This conclusion is supported by the quantitative analysis of the previous study, the results of which show that knowledge of modern contraception makes no significant difference between women who intend to use contraception and those who do not at the 5% threshold (Sindayihebura, Nganawara, & Manirakiza, 2022b).
2. Influence of opinions and attitudes against modern contraception
During the survey, a number of opinions and attitudes were found to be at the basis of non-intention to use modern contraception. Among other facts and opinions, the answers given reveal experienced or feared side-effects, fear of experienced side-effects, the absence of mechanisms for treating side-effects, religious opinions and the proven limitations of contraceptives in preventing additional pregnancy.
a. Experienced side effects and the fear of experiencing them
Experienced side-effects and the fear of experiencing them are among the most important determinants of negative attitudes towards the intention to use contraception. Among the side effects cited are vaginal bleeding, sterility, oedemas, anaemia and so on. Here are a few comments from women who have experienced side effects.
N.C., 32, Musigati, mentions that after trying three methods, she only experienced vaginal bleeding and had to give up. She expresses herself as follows:
I’ve already tried three unsuccessful methods: the implant didn’t work very well, nor did the injectable, and when I tried the IUD, it hurt with non-stop menstruation. Now I’ve given up on everything, because my stomach always hurts, my belly is always swollen; I’ve been all over the healthcare facilities, but with no results. Then I became anaemic and had to stop. After a year, I got conceived and now I’m pregnant.
Bleeding has also been reported in Gisuru, where the fear of suffering the same misfortune as one’s peers nourishes a feeling of mistrust towards modern contraception. N.S., 40, Gisuru, reacting to the case of a participant who had experienced bleeding, put it this way:
If you have the chance to see the effects these methods have brought to your friend before you’ve even gone to get them, it seems you wouldn’t go there. Moreover, she’s not the only one; I myself had to be hospitalized in Ruyigi for practicing a contraceptive method.
In addition to the bleeding, M.Y., 38, Musigati, mentions the fear of infertility:
I used modern contraception, but I had to stop it, because I had used the implant, but when I went to have it removed to conceive another baby, the Doctor failed to remove it entirely; a piece remained. This doctor has always told me it’s okay, but I haven’t conceived yet.
These side effects, that are sometimes terrifying, make attitudes towards contraception are strongly negative. Asked whether they felt any regret at having an anti-contraceptive attitude in an environment that requires rigorous fertility control, the women showed little concern, comforted by the feeling that they had escaped the harmful effects suffered by their fellow women as a result of contraception. N.V., 39, Shombo, puts it this way:
I regret, but if I were to take them for side effects that would cost the sale of the plot where those already born would build, I wouldn’t have gained anything. I’m losing out because I give birth all the time, but if I go, I risk endangering my health and that of the children.
In summary, it is remarkable that the side-effects experienced by victims nourish their fear of reliving them, and discourage the intentions of those who would like to adopt modern contraception. They are afraid of suffering the same misfortune as those who have already used them.
b. Cost and lack of side-effect treatment services
For most respondents, it was difficult to talk about side effects without adding the absence of services to treat them. In rural areas, respondents were quick to complain that contraceptive methods were often offered free of charge, and that there was no services to treat the side-effects of using them. In this regard, M.M., 32, Kirundo, points to this truncated offer of family planning services in the following terms:
These methods are offered to us free of charge, but sometimes they don’t work properly and the user falls ill. In that case, you’re not welcome and you’re made to pay. So many prefer to give up these methods because they can’t find the money.
N.M., 35, Kirundo, describes how she and her friend were denied the service they had hoped to find at the health center that had offered an implant. She explains:
…I was the victim of a case; I was accompanying a widow; she was not received because we were asked for a colossal sum of money.
All these facts show how the provision of family planning services that are limited to the supply of methods presents a limit to their use. Respondents wanted free or affordable services to assist them in treating side-effects when they happen.
c. Religious opinions
Among the reasons for not intending to use modern contraception, religious opinions stand out. Most respondents mention that using contraceptives is murder, that it’s breaking God’s 5th commandment, forbidding to kill. For some women, contraceptive use prevents them from receiving the graces of God’s intercessions and blessings from heaven.
N.C., 48, Musigati, Catholic, argues that the use of contraception is a sin and that prayers made on behalf of a contraceptive user cannot be answered. She puts it this way:
…. But also its use is a sin. If you use it, you kill! Don’t you understand that walking around with an implant in your body is similar to wearing an amulet?
K.L., 20, Shombo, Pentecostal, relying on her religious convictions finds that using contraception would be against divine will and chooses not to intend to use it. She expresses herself as follows:
…. Considering again the way I perceive the things of God, I understand that I would be at fault, and that’s why I don’t intend to resort to it.
K.A., 22, Shombo, Catholic, considering the smell of a contraceptive user’s menstruation, compares this use to abortion, an act strongly opposed by her religious confession. She says:
…. Even the church forbids it, because it’s infanticide; besides, a user’s menstruation smells as if it contains the elements of a decomposing child’s body.
All these opinions show that the religious beliefs held by women of childbearing age can prevent them from embracing the use of modern contraception. Combined with the fear of side-effects and related testimonials, these religious opinions are not likely to encourage adherence to contraception in a context where almost the entire population claims to belong to a religious group.
d. Failure of contraceptives to prevent pregnancy
A certain mistrust of the effectiveness of the methods already used or used by their relatives emerged. Finding that there’s no benefit in using a method that doesn’t prevent you from getting pregnant, I.J., 22, Gisuru, would prefer to leave everything to keep things on good terms with her husband, because conceiving in this case might seem like infidelity. She expresses herself as follows:
It’s necessary, but what disconcerts us is that you can get pregnant while holding an implant in your body. How does this happen? …. If those who go to get them get pregnant, is it really important for the rest of us to go? We don’t! Even in the home, it can cause a misunderstanding: people will ask you where this pregnancy came from when you’re on a contraceptive method?
N.J., 28, Mabanda, who has in fact used contraception, would intend to use it again, but her intention seems to be fading because of the one barrier of failure she has experienced. She said:
I’d like to continue using them in the future, even though there are plenty of barriers; personally, even though I’ve used them, it hasn’t prevented me from conceiving. Later, I had to stop.
3. Influence of social interactions on non-intention to use modern contraception
Social interactions have always been indexed as factors attributable to contraceptive non-intention. Thus, respondents were asked what people around them said about contraception, whether these statements were likely to discourage contraceptive practice, and whose influence might prevent contraceptive use. Influences can be divided into three categories: firstly, myths and rumors, which are sometimes the reality experienced by women. Then there are religious influences and social cohabitation.
a. Myths and rumors. Or reality?
Myths and rumors are popular beliefs and truths that are transmitted orally and end up imposing themselves as true (Babalola et al., 2015). In this study, we consider the beliefs that are often put forward to discourage the use of modern contraception and that have ended up imposing their influential power in society.
N.S., 26, Karusi, showing that her negative attitude towards contraception makes her regret nothing, points to the way rumors attribute women’s infertility to contraceptive methods as an element of contraceptive non-intention. She puts it this way:
No, we don’t lose anything because most fear them, because they would become sterile, to be satisfied with those they gave birth to before this use.
N.J., 26, Gisuru, speaking about the way social opinion makes people believe that the use of some methods leads to permanent menstruation (bleeding), finds that this is a rumor that may be at the root of the non-intention to use them. She puts it this way:
They say it degrades your health … There would be some who use them and would have bleeding every week.
Other myths and rumors concern the illnesses that would be caused by the use of certain contraceptive methods. In her reaction, M. J., 37, Kirundo, mentions abdominal tumors. She indicated:
It is said that the person who uses these methods may have the tumors in his belly.
These results, which refer to “hearsay”, show that popular beliefs have a negative influence on the intention to use modern contraception. However, given that some of the effects conveyed seem to have been experienced by some women, are we still going to say that these are rumors?
b. Religious influences
Religious influences have also been indexed among the social influences that negatively affect the intention to use contraception. For M.N., 38, Shombo, Pentecostal, contraception is contrary to her faith because the Bible says to multiply like the sand of the sea. She says:
Our faith doesn’t allow us to use contraception; God says we must multiply like the sand! No one has ever achieved this greatness in their descendants.
Most of the interviewees converge on the fact that religious confessions regard the use of contraceptive methods as a transgression of God’s 5th commandment, which constitutes a major obstacle to the adoption of contraceptive methods. K. L., 48, Kirundo, Catholic, states:
Religious confessions also prevent people from using these methods; their followers say they would not resort to these methods because they would have committed murder.
N.S., 35, Gisuru, adds that the way religious leaders regard the use of modern contraception as an unforgivable sin is a dissuading factor for those intending to use it. She said:
In Christian confessions, for example, it is said that users kill, that it is a sin that is never forgiven. This makes it difficult to decide whether to adopt these methods.
Faced with these positions taken by religious confessions, most women resolve to reject any idea of modern contraception in order to remain in line with their religious confessions. This is the case, for example, of N.D., 28, Shombo, who declares:
It’s faith that can prevent me because we are passing on this earth; because, in that case, I would have made my body a property to be exploited.
These data show how the positions taken by religious confessions with regard to contraception remain preponderant in adherence to the latter. If these are added to individual opinions and attitudes that are not favorable, because of the side effects mentioned that are not taken into account, the chances of intending to use contraception are further reduced.
c. Social cohabitation
According to respondents’ answers, the influence of some close personalities can be at the basis of contraceptive non-intention. The husband’s position, or that of the woman’s parents or in-laws, may prevent her from intending to use contraception.
Reacting to the question of who can negatively influence her contraceptive intentions, N.D., 28, Shombo, shows that her husband’s position can be decisive while refuting the influence of her mother-in-law. She states:
The only person who can stop me from going is my husband and the person who has already experienced the negative effects of them. Otherwise, my mother-in-law can’t stop me because she has no responsibility for managing my life.
Reinforcing the idea of the primacy of the husband’s position, M. J., 37, Kirundo, points out that a woman cannot use contraception when her husband still wants children, because doing so in secret will lead to discord in the treatment of side effects.
Although the latter seem to refute the part played by in-laws’ opinions in the intention to use contraception, others don’t seem to deny their influence. N.S., 40, Gisuru, shows that the influence of in-laws can support the antagonism between contraception and traditional natalism. She points out that in-laws can inspire their son to chase away a woman who wants to use contraception, retorting:
You’ve only got two children, and you want to stop there? My son, repudiate her and take another who will give you more children to enlarge our family!
Alongside a parent who advises his son to force his wife to conceive, K. D., 33, Kirundo, asserts that mothers can encourage their daughters in marriage to prefer childbirth to minimize any side effects. She puts it this way:
For example me, my mother told me that the reason I give birth by caesarean section is because I use contraceptive methods, that I’m stupid, that I shouldn’t do it while I’m still fertile; that we still have the strength to work to maintain the family, and so we must procreate to the last egg.
4. Self-efficacy and control of perceived behavior
Questions were asked to understand whether women could initiate the use of modern contraception themselves, or influence decision-making despite the refusal of those around them.
For some women, they could easily choose contraception for the well-being of their families. This is the case of N.Y, 29, Karusi, who reassures us:
Neither faith nor traditions, nothing can stop me from using birth planning methods because it doesn’t cause any worries. Instead of giving birth to those who will go stealing (for lack of livelihood), I would use these methods.
Some of her friends (in the focus group) also seem self-confident in asserting that they would be able to adhere to contraception for the sake of suitability between offspring and available resources. They would benefit from the discretion assured in the administration of these methods in health care facilities. This discretion also enables some women to deny using them publicly, even though they do use them.
However, other answers seem to be ambivalent, varying between the will to influence one’s destiny and the limit that characterizes a woman who cannot manage the side effects of contraception herself. Others understand that the result can never be better without the consensus of those closest to her.
This is the case of N.J., 33, Mabanda, who asserts that she could decide on her own to use contraception, as she has done in the past. However, she doesn’t forget to mention that she has 8 children and that the couple’s relationship must have been troubled. Contraception helped her to space out the births, but she couldn’t stop if she needed to, because she was on her own.
For other women interviewed, contraception is not an option for women on their own, for reasons of managing side-effects when they happen. N.J., 26, Gisuru, reacts as follows:
Could you take the money to go and buy these things without your husband’s consent? Nooo! And if there are side effects that often happen without your husband knowing …!?!
The other aspect of self-efficacy that came up was the ability to engage in a discussion about family planning. The responses revealed that women remain limited in their freedom of action. Indeed, while M.Y., 38, Musigati, confirms that a woman can initiate a discussion concerning family planning within the couple, others find that it is not easy to do so, and that even if a woman manages to initiate such a discussion, the result can easily be fruitless. N.G., 37, Mabanda, puts it this way:
…. A woman can’t have the last word in decision-making; you make a decision together, but because of the husband’s state of drunkenness, as a result of the drinks that stimulate their bodies, the decision made together doesn’t hold water.
I.J., 22, Gisuru, agrees, saying:
It’s not possible. You can’t tell a drunk person to leave. He can even tell you that you’re going to give birth as much as he wants, but not according to your own will. If a husband tells you: I’ll have a child according to my will, that’s the way it is.
To sum up, we can see that women still have this limitation of being able to self-determine in the use of contraception. Reasons for this may include side-effect management. Reasons of accessibility were not often mentioned because, in the environments visited, contraceptives are offered free of charge in health centers. However, most of the women who responded did not believe that a woman could decide to commit the financial means without her partner’s consent.
So, from the information provided by the women who took part in the focus groups, we can see the reasons behind the evident unwillingness to use modern contraception. In the following paragraphs, these will be discussed with the results of previous studies.
DISCUSSION
The aim of this study was to identify the opinions, attitudes and social influences that influence people’s unwillingness to use contraception. In the following paragraphs, the results are compared with those of previous studies.
- Influence of opinions and attitudes related to experienced or feared side-effects and the poor quality of services offered to manage them
Experienced or feared side-effects reported include menstrual cycle abnormalities such as vaginal bleeding for shorter or longer periods, menstrual delays, absence of menstruation after stopping the method, and abdominal tumors. These side-effects experienced by former users make them unwilling to use the method again. They also frighten those who would like to adopt them, and reinforce those who have no intention of using them at all. In this way, the latter are comforted by the feeling that they have escaped the harms suffered by those who have used them.
As far as previous use is concerned, these results are the opposite of those found in almost all the studies reviewed for this study. With the exception of women who had experienced abortion in the town of Ambo in Ethiopia (Negewo, 2010), the results of the other studies show that having used a contraceptive method would increase the likelihood of intending to use it in the future. These include the study conducted in rural Bangladesh (Callahan & Becker, 2013), Ghana (Eliason et al., 2013; Wuni et al., 2018), Morocco, Nigeria (Babalola et al., 2015), Pakistan (Campo et al., 2012).
In all these studies, women who had used a modern contraceptive method were the most likely to intend to use it in the future. In rural Bangladesh, women who had used contraception in the past were around 2.5 times more likely to intend to use it than those who had not (Callahan& Becker, 2013). In rural Ghana, where women who had previously used the oral pill, injectables and emergency contraception were around 2, 4 and 1.5 times more likely to intend to use these methods than those who had not (Eliason et al., 2013). In urban areas in Ghana, among women attending childhood clinics, those who had previously used contraception were 1.15 times more likely to intend to use it again than those who had never done so (Wuni et al., 2018). In Morocco, women who had experience of using contraception were 3.3 times more likely to intend to use it in the future than those who had not (Curtis & Westoff, 1996). In Nigeria’s main cities, women who had already used modern contraceptives were 2.05 times more likely to intend to use them than those who had not (Babalola et al., 2015).
Visibly, these results testify to use without adverse effects by women who had practised contraception. Successful use was the basis of a good attitude towards contraception. In addition, the health care services on offer would have been those that assisted contraceptive users through to the treatment of side-effects. Moreover, these studies, which sometimes took place in exclusively urban settings, targeted women who had access to full care, including administration and side-effect treatment (Babalola et al., 2015; Wuni et al., 2018). Isn’t it also in urban settings that accessibility to methods of choice and purchasing power are high?
The results of this study, in which experienced or feared side effects were at the basis of negative attitudes towards modern contraception, converge with studies carried out in Oromia (Negewo, 2010), Tigray (Gebremariam & Addissie, 2014) and Wolaita (Meskele & Mekonnen, 2014) in Ethiopia, Pakistan (Agha, 2010) and Senegal (Machiyama & Cleland, 2013). In these studies, women with negative side-effect-related attitudes towards contraception were the most likely not to intend to use modern contraception. In Ambo, women with a good attitude towards long-acting and permanent methods (LAPMs) were around 9 times more likely to use them than those with a poor attitude (Negewo, 2010). In Tigray, women who believed that LAPMs destroy the womb were 74% less likely to intend to use them than those who didn’t (Gebremariam &Addissie, 2014). In the Wolaita zone of Ethiopia, women with a positive attitude towards LAPMs were around 2.5 times more likely to intend to use them than those with a negative attitude. In Pakistan, women who believed that contraceptive methods can destroy the womb were 25% and 30% less likely to intend to use the IUD and sterilization, respectively (Meskele&Mekonnen, 2014).
The reasons behind these negative attitudes to modern contraception are similar to those cited by the women interviewed. These include the belief that long-acting methods such as the IUD can destroy the womb and lead to infertility (Gebremariam&Addissie, 2014; Meskele&Mekonnen, 2014). In Kenya’s Nyanza Province, women believed that pills could accumulate unhealthy masses in the stomach and cause the user to give birth to a child with two heads (Rutenberg & Watkins, 1997). In addition, abdominal tumors, delayed menstruation and pregnancy after discontinuation of the method, prolonged bleeding or menstruation, etc. reinforce negative attitudes in the context of the study.
Although we have no references concerning the effect of the cost or lack of availability of side-effect treatment services, we can believe that these attitudes are due to the fact that women are still afraid for their health. This is all the more true if we note that these studies were conducted in a context not dissimilar to that of this study. These are poor countries where the provision of family planning services does not guarantee the handling of side effects (Gebremariam&Addissie, 2014; Machiyama& Cleland, 2013; Meskele&Mekonnen, 2014; Negewo, 2010).
In addition to the high cost and lack of side-effect treatment services on offer, we can also add the deficiency of the available services, which do not guarantee the success of an adopted method. It’s true that in this case, the ability of the user to ensure regular follow-up in order to effectively avoid an unwanted pregnancy must be taken into account before judging the services offered, but if these women already list such failures among the factors contributing to negative attitudes, the offer must be reviewed or reorganized at the community awareness level. This would be helpful in a context where results already show that awareness-raising mechanisms such as home visits by family planning agents bring a benefit to the intention to use contraception (Sindayihebura et al., 2022).
- Religious influences sustained by myths, rumors and misconceptions
The results of this study show that religious opinions and beliefs influence non-intention to use modern contraception. In all the regions visited, women used religion to justify their non-intention to use modern contraception.
These findings seem to converge with studies in rural Bangladesh (Callahan& Becker, 2013), Ethiopia (Tiruneh et al., 2016), Ghana (Ahuja et al., 2020), Kenya and Nigeria (Babalola et al., 2015). In rural Bangladesh, Muslim women were more likely than Hindu women to have no contraceptive intention (Callahan& Becker, 2013). In Ghana, Muslim women were still more likely than Pentecostal/Charismatic women to have no intention (Ahuja et al., 2020). In Nigeria and Ethiopia, it was still Muslim women who were more likely than non-Muslims to have this intention (Babalola et al., 2015; Tiruneh et al., 2016). Only in Kenya are Muslim women more likely to have no such intention than non-Muslims.
However, if the explanations given in Ghana are to be believed, Muslim women’s non-intention to use modern contraception is not due to faith. It is a socio-cultural effect of the view in some Muslim societies that women who use contraception want to avoid pregnancy in their infidelity (Ahuja et al., 2020). Findings to the contrary in Kenya would suggest a society with little regard for such matters. The same is true of cases where Catholics and Pentecostals/charismatics are presented as the least likely to have no intention of using modern contraception. These religions are never in favor of modern contraception; it is only their followers who choose to practice it for personal reasons (Nkunzimana et al., 2021; Schwarz et al., 2021; Sindayihebura, Nganawara, & Manirakiza, 2022a). The only results that would be consistent with the faith defended by religious confessions would be those of the Orthodox and Anglicans, where the use of modern contraception is tolerated for reasons of the economic health of their followers’ households.
It is therefore important to transfer the reasoning to the level of religiosity. It is at this level that the influence of religion is externalized in the consciousness of the individual and, consequently, on contraceptive intentions. This is shown by the study carried out in the main cities of Nigeria, where women of high religiosity are the most likely not to have the intention studied than others (Babalola et al., 2015). This position is supported by the earlier study, which suggests not relying solely on the findings that Protestant women are more likely than Catholics to lack contraceptive intention in Burundi (Sindayihebura, Nganawara, &Manirakiza, 2022a). During our focus group discussions, the women who expressed their opposition to modern contraception came from a variety of religious confessions, both Catholic and Protestant, hence the interest in considering religiosity rather than religion.
All these religious confessions do not accept modern contraception, which they see as a cession to sexual libertinage at the expense of chastity and abstinence. Thus, their followers would like to remain in union with God by avoiding the “sin” of contraception. Besides those who would prefer to procreate in order to fulfill the will of God, who told Abraham, the ancestor of believers, to multiply like the sand of the seas, it should be noted that this non-intention is supported by extreme beliefs that the use of contraception is a sin for which one never receives forgiveness. Some go so far as to assert that the use of contraception is like abortion, and therefore murder. Others assert that intercessions for users of modern contraception cannot be granted.
These beliefs prevail in a context where women who use modern contraception encounter problems of untreated side-effects, and combine with a context where misconceptions, myths and rumors reduce individual initiative. In this regard, the findings agree with those of studies conducted in Nigeria and Ethiopia, where women exposed to misconceptions, myths and rumors are most likely to be non-intentional users of modern contraception (Meskele & Mekonnen, 2014; Babalola et al., 2015).
- Influence of other social interactions
Alongside religious influences and misconceptions, myths and rumors, women mentioned social interactions that may be at the basis of non-intention to use modern contraception. Among all the social cohabitations mentioned, it was mainly the position of the husband/sexual partner that influenced the intention to use modern contraception among the women surveyed. There is also the influence of the mother-in-law. Given the importance of the influence of religious opinions, we can also consider the influence of religious leaders, from whom women find their convictions regarding modern contraception.
These findings are similar to studies carried out in universities in Ghana (Bosompra, 2001), rural Ghana (Eliason et al., 2013), Kenya and Nigeria (Babalola et al., 2015) and Pakistan (Agha, 2010). In Ghanaian universities, both students who intended to use condoms consistently and those who had no such intentions conformed to the wishes of their significant referents (sexual partners, close friends, relatives and doctors) (Bosompra, 2001). It was certainly because of fear of referents that few women claimed they could introduce a family planning topic in front of a chief or his wife, a teacher or his wife and a man of the clergy in Nyanza, Kenya (Rutenberg & Watkins, 1997). In Nigeria, women not subject to social interaction were 1.32 times more likely to intend to use modern contraception than those subject to it (Babalola et al., 2015). In rural Ghana, women whose mothers-in-law approved of family planning methods were 3.06 times more likely to intend to use them than those whose mothers-in-law did not. Those whose mothers approved of family planning were 1.60 times more likely to intend to use contraception than those whose mothers did not. Women whose fathers-in-law approved of family planning were 44% less likely to intend to use contraception than those whose fathers-in-law did not (Eliason et al., 2013). In Pakistan, women whose in-laws approved of family planning were more than 2 times more likely to intend to use, hormonal methods, the IUD and female sterilization (Agha, 2010).
These studies agree with our study in showing that there are important people in the environment of the people studied whose opinion on contraception can be decisive for contraceptive intentions. Bosompra (2001) mentions important referents such as sexual partners, close friends, relatives and doctors among university students in Ghana. These referents are logically comparable to husbands, mothers and mothers-in-law of women in union, to whom we can add religious leaders.
The husband’s influence is indisputable in a patriarchal society where household management is in the hands of the spouses. For this reason, the woman’s level of education and occupation are of little significance in explaining contraceptive non-intention. On the other hand, the husband’s desire for a smaller number of children than the wife’s desire reduces contraceptive non-intention among women in union in Burundi. In addition, negative sexual behavior (wife beating if sexual relations are refused) increases this non-intention (Sindayihebura et al., 2022).
The role of the mother’s position, like that of the mother-in-law, is part of the traditional natalism of societies in the first phase of demographic transition (David, 2015; Gendreau, 1993). The perpetuity of the bloodline has always been the basis for encouraging the procreation of advanced generations compared with younger generations in Burundi (Kamuragiye & Buzingo, 2019). In the case of this study, the influence of the father-in-law was not reported. If we follow the logic of the study carried out in rural Ghana, where the approval of contraception discouraged contraceptive intention, we might think that these are the reasons for the fear of being accused of infidelity (Eliason et al., 2013). In traditional societies, distance has always been created between the woman and her father-in-law to avoid such cases. In Burundi, this distance means that the parent-in-law’s opinion has no influence.
- Influence of women’s self-efficacy
With regard to self-efficacy in the area of modern contraception, the responses show that, despite the desire to take control of family destiny and influence procreation, women cannot substantially engage in a discussion about family planning. Clauses can be unilaterally flouted by the husband, and the desired results cannot be achieved.
These findings are in line with studies carried out in Ghana (Wuni et al., 2018) and Pakistan (Agha, 2010). In Ghana, women who had the latitude to discuss family planning with their partners were about 1.5 times more likely to intend to use contraception than those who did not (Wuni et al., 2018). In Pakistan, women who did not have the latitude to discuss family planning with their husbands were 27% less likely to use female sterilization than those who could conduct this discussion.
All taken together, these data show how, in these patriarchal societies, women cannot take the initiative for contraception and carry it out without the decisive involvement of their husbands. In Burundi, this is a context where the need is actually felt. Women would like to influence the procreation of their households, but their will struggles to be externally expressed. Even in cases where women have the latitude to express it, they lack the strength to influence its realization. Spouses have so much power of influence that they can undermine the family planning initiatives their wives have initiated. The mere fact of having had one too many can torpedo birth control clauses.
CONCLUSION
The aim of this study was to investigate the opinions, attitudes and social interactions that sustain the non-intention to use modern contraception in a context where it is most needed. For this reason, qualitative data collection was organized and carried out in ten locations in the provinces of Bubanza, Karusi, Kirundo, Makamba and Ruyigi. The data collected was analyzed using thematic content analysis.
The results of the analysis show that the main opinions, attitudes and social interactions that have a negative influence on the intention to use modern contraception are the side effects experienced by former users. Besides former users, those who have not yet had to use modern contraception fear the same fate. The cost and unavailability of side-effect treatment services, and the failure of methods used to avoid pregnancy, also discourage those who are free from the pressure of social interactions. Indexed social interactions include religious beliefs and the influence of important family members such as husbands, mothers and mothers-in-law. With all these influences, a woman’s individual ambition for contraception fades.
These results show that social pressure takes advantage of a loophole in the provision of family planning services to annihilate the individual initiatives of women who harbor ambitions to use modern contraception. Thus, the provision of family planning services deserves to be rethought in this context of poverty, where rural households are not financially able to cope with the side effects.
Such findings add significant value to previous studies carried out in Burundi that, based on quantitative data from the Demographic and Health Surveys, had not been able to sufficiently bring out the influence of opinions, attitudes and social interactions, which deserved to be studied. By adopting a qualitative approach, it has the merit of questioning in depth the factors behind contraceptive non-intention, by identifying them as well as discovering their mechanisms of influence, as told by those who experience them, rather than quantifying them. However, although the results are comparable to those of previous studies and in other contexts, the limitation of this work may lie in the very fact of enumerating factors without statistically measuring the significance of each one. In addition, although the results implicitly show that respondents referred mainly to long-acting methods, the use of modern contraception was mentioned without specifying the method. Therefore, future studies could focus on specific methods in order to highlight those that are much likelier to be the subject of controversy.
ACKNOWLEDGEMENT
Our acknowledgements are addressed to the Research Office of the University of Burundi, which provided us with funding for data collection, as well as administrative support during data collection.
REFERENCES
- Agha, S. (2010). Intentions to use contraceptives in Pakistan : Implications for behavior change campaigns. BMC Public Health, 10(1), 450. https://doi.org/10.1186/1471-2458-10-450
- Ahuja, M., Frimpong, E., Okoro, J., Wani, R., & Armel, S. (2020). Risk and protective factors for intention of contraception use among women in Ghana. Health Psychology Open, 7(2), 205510292097597. https://doi.org/10.1177/2055102920975975
- Andreani, J.-C., & Conchon, F. (2005). Méthodes d’analyse et d’interprétation des études qualitatives : État de l’art en marketing. Cahier de recherche ESCP-EAP, 1‑26.
- Auerbach, C. F., & Silverstein, L. B. (2003). Qualitative data : An introduction to coding and analysis. New York University Press.
- Babalola, S., John, N., Ajao, B., & Speizer, I. (2015). Ideation and intention to use contraceptives in Kenya and Nigeria. Demographic Research, 33, 211‑238. https://doi.org/10.4054/DemRes.2015.33.8
- Bosompra, K. (2001). Determinants of condom use intentions of university students in Ghana : An application of the theory of reasoned action. Social Science & Medicine, 52(7), 1057‑1069. https://doi.org/10.1016/S0277-9536(00)00213-6
- Callahan, R., & Becker, S. (2013). Contraceptive Intentions and Use in Rural Bangladesh. Annual Meeting of the Population Association of America. https://paa2013.princeton.edu/papers/130056
- Campo, S., Askelson, N. M., Spies, E. L., & Losch, M. (2012). Ambivalence, communication and past use : Understanding what influences women’s intentions to use contraceptives. Psychology, Health & Medicine, 17(3), 356‑365. https://doi.org/10.1080/13548506.2011.608432
- Curtis, S. L., & Westoff, C. F. (1996). Intention to Use Contraceptives and Subsequent Contraceptive Behavior in Morocco. Studies in Family Planning, 27(5), 239. https://doi.org/10.2307/2137996
- David, O. (2015). La population mondiale : Répartition, dynamique et mobilité (3e éd). Armand Colin.
- De Loenzien, M. (2006). Fondement des approches qualitatives dans les études de population. In M. De Loenzien & S.-D. Yana (Éds.), Les approches qualitatives dans les études de population : Théorie et pratique (p. 11‑45). Agence universitaire de la francophonie Éditions des Archives contemporaines, eac.
- Eliason, S., Baiden, F., Quansah-Asare, G., Graham-Hayfron, Y., Bonsu, D., Phillips, J., & Awusabo-Asare, K. (2013). Factors influencing the intention of women in rural Ghana to adopt postpartum family planning. Reproductive Health, 10(1), 34. https://doi.org/10.1186/1742-4755-10-34
- Gebremariam, A., & Addissie, A. (2014). Intention to use long acting and permanent contraceptive methods and factors affecting it among married women in Adigrat town, Tigray, Northern Ethiopia. Reproductive Health, 11(1), 24. https://doi.org/10.1186/1742-4755-11-24
- Gendreau, F. (1993). La population de l’Afrique : Manuel de démographie. CEPED : Karthala. https://horizon.documentation.ird.fr/exl-doc/pleins_textes/pleins_textes_7/carton07/35169.pdf
- ISTEEBU. (2019). Tableau de bord social du Burundi : Edition 2018 (p. 46). https://www.isteebu.bi/wp-content/uploads/2020/05/TBS-DECEMBRE-2019-Edition-2018.pdf
- ISTEEBU, & ICF International. (2017). Troisième Enquête Démographique et de Santé 2016-2017. https://www.isteebu.bi/wp-content/uploads/2020/10/EDS-III.pdf
- Kamuragiye, A., & Buzingo, D. (2019). Maitriser la croissance de la population pour profiter du dividende demographique en Afrique subsaharienne : La cas du Burundi. Les Editions l’Empreinte du Passant. https://lempreintedupassant.com/index.php/product/maitriser-la-croissance-de-la-population-pour-profiter-du-dividende-demographique-en-afrique-subsaharienne-le-cas-du-burundi/
- Krippendorff, K. (2004). Content analysis : An introduction to its methodology (2nd ed).
- Larivière, N., & Corbière, M. (Éds.). (2014). Méthodes qualitatives, quantitatives et mixtes : Dans la recherche en sciences humaines, sociales et de la santé. Presses de l’Université du Québec.
- Machiyama, K., & Cleland, J. C. (2013). Analyse des besoins non satisfaits au Sénégal. London School of Hygiene & Tropical Medicine. https://knowledgecommons.popcouncil.org/cgi/viewcontent.cgi?article=1275&context=departments _sbsr-rh
- Meskele, M., & Mekonnen, W. (2014). Factors affecting women’s intention to use long acting and permanent contraceptive methods in Wolaita Zone, Southern Ethiopia : A cross-sectional study. BMC Women’s Health, 14(1), 109. https://doi.org/10.1186/1472-6874-14-109
- Negewo, D. (2010). Assessment of factors affecting women’s intention to use long acting and permanent contraceptive methods among family planning clients of public health facilities in Ambo town, Oromia National Regional state, Ethiopia. https://doi.org/10.20372/NADRE/12810
- Nkunzimana, E., Babale, M. S., Ndoreraho, A., & Nyandwi, J. (2021). Uptake of Modern Contraceptive Methods among Burundian Women and Associated Factors : Analysis of Demographic and Health Survey Data, Burundi 2016–2017. East African Health Research Journal, 5(1), 75‑81. https://doi: 10.24248/eahrj.v5i1.654
- Paillé, P., & Mucchielli, A. (2021). L’analyse qualitative en sciences humaines et sociales (5e éd). Armand Colin.
- République du Burundi. (2018). Plan National de Développement du Burundi (PNDB 2018-2027). http://www.presidence.gov.bi/wp-content/uploads/2018/08/PND-Burundi-2018-2027-Version-Finale.pdf
- ROCARE, R. O. et C. A. de R. en E., & ADEA, A. pour le D. de l’Education an A. (2006). Extraits de Guides pour la Recherche Qualitative. www.rocare.org/PetitesSubventions_GuideRechercheQuali.pdf.
- Rutenberg, N., & Watkins, S. C. (1997). The Buzz Outside the Clinics : Conversations and Contraception in Nyanza Province, Kenya. Studies in Family Planning, 28(4), 290‑307. https://doi.org/10.2307/2137860
- Schwarz, J., Manirakiza, R., & Merten, S. (2021). Reproductive Governance in a Fragile and Population-Dense Context : Family Planning Policies, Discourses, and Practices in Burundi. The European Journal of Development Research. https://doi.org/10.1057/s41287-021-00482-1
- Sindayihebura, J. F. R., Barankanira, E., Manirakiza, D., Nganawara, D., Manirakiza, R., & Bouba Djourdebbé, F. (2022). Influence of gender relationships on the non-intention to use modern contraception among women aged 15 to 49 in union in Burundi. Applied Mathematical Sciences, 16(8), 387‑396. https://doi.org/10.12988/ams.2022.916836
- Sindayihebura, J. F. R., Bouba Djourdebbe, F., Nganawara, D., Manirakiza, D., Ndayitwayeko, W.-M., Barankanira, E., & Manirakiza, R. (2023). Qui Sont les Femmes en Union Sans Intention d’Utilisation de la Contraception Moderne au Burundi ? Etude du Profil Socio-Démographique à Partir des Données de 2010 et 2016-2017. European Scientific Journal ESJ, 19(14), 123‑144. https://doi.org/Doi:10.19044/esj.2023.v19n14p123
- Sindayihebura, J. F. R., Manirakiza, R., & Nganawara, D. (2022). Profil des Femmes à Haut Risque d’Anémie : Influence des Mutations Rurales. Les annales de l’IFORD, 22(1), 109‑126.
- Sindayihebura, J. F. R., Ndayitwayeko, W.-M., Manirakiza, R., & Nganawara, D. (2022). Sources of decline in the level of intention to use modern contraception among women of childbearing age between 2010 and 2017 in Burundi. Applied Mathematical Sciences, 16(7), 329‑338. https://doi.org/10.12988/ams.2022.916798
- Sindayihebura, J. F. R., Nganawara, D., Bouba Djourdebbé, F., & Manirakiza, R. (2022). Family Planning Services Supply and Non-Intention to Use the Modern Contraception among Women of Childbearing Age in Union in Burundi. Internation Journal of Mathematical Analysis, 16(2), 81‑88. https://doi.org/10.12988/ijma.2022.912423
- Sindayihebura, J. F. R., Nganawara, D., & Manirakiza, R. (2022a). Community socio-cultural pressure in explanation of the non-intention to use modern contraception among the women aged 15-49 in Union in Burundi. Application of the multi-level analysis. International Journal of Mathematical Analysis, 16(4), 149‑157. https://doi.org/10.12988/ijma.2022.912431
- Sindayihebura, J. F. R., Nganawara, D., & Manirakiza, R. (2022b). Household Poverty and Contraceptive Non-Intention Among Women of Childbearing Age in Union in Burundi : Validity of the Theory of Intergenerational Flows of Wealth. Journal of Population and Social Studies, 31, 80‑94. https://doi.org/10.25133/JPSSv312023.005
- Sindayihebura, J. F. R., & Nkunzimana, A. (2020). Changement climatique et anémie chez les femmes en âge de procréer au Burundi : Approche par la région de résidence. Revue de l’Université du Burundi : Séries Sciences Humaines et Sociales, 18(1), 160‑173. http://revue.ub.edu.bi/JUB/article/view/84
- Tabutin, D., & Schoumaker, B. (2020). La démographie de l’Afrique subsaharienne au XXIe siècle : Bilan des changements de 2000 à 2020, perspectives et défis d’ici 2050. Population, 75(2), 169. https://doi.org/10.3917/popu.2002.0169
- Tiruneh, F. N., Chuang, K.-Y., Ntenda, P. A. M., & Chuang, Y.-C. (2016). Factors associated with contraceptive use and intention to use contraceptives among married women in Ethiopia. Women & Health, 56(1), 1‑22. https://doi.org/10.1080/03630242.2015.1074640
- Wuni, C., Turpin, C. A., & Dassah, E. T. (2018). Determinants of contraceptive use and future contraceptive intentions of women attending child welfare clinics in urban Ghana. BMC Public Health, 18(1), 79. https://doi.org/10.1186/s12889-017-4641-9