
Developmental Impact of Early Life Stress and Schizophrenia: An up to Date Review on the Psycho-Neurobiological Dysregulation
- Fredrick Otieno Oginga
- Kulimankudya Dominic Vasco
- Thabisile Mpofana
- 30-43
- Aug 30, 2024
- Public Health
Developmental Impact of Early Life Stress and Schizophrenia: An up to Date Review on the Psycho-Neurobiological Dysregulation
Fredrick Otieno Oginga1,2* Kulimankudya Dominic Vasco2 and Thabisile Mpofana3
1Department of Physiology, School of Laboratory Medicine and Medical Sciences, University of Kwa-Zulu Natal, Durban, South Africa
2Department of Clinical Medicine, School of Medical and Health Science, Kabarak University, Nakuru, Kenya.
3Department of Physiology, School of Medicine Nelson Mandela University Summerstrand, Gqeberha, South Africa
DOI: https://doi.org/10.51244/IJRSI.2024.1115003P
Received: 12 August 2024; Accepted: 17 August 2024; Published: 30 August 2024
ABSTRACT
Rationale; The study of the possible effects of early life stress (ELS) on later human behavior and neurobiology is a rapidly growing field. While epidemiological and neurobiological studies paint a grim picture of negative consequences, little attention has been paid to integrating the diverse evidence on possible cognitive and emotional deficits associated with ELS. Longitudinal studies examining the effects of perinatal mental disorders such as schizophrenia provide a new framework for understanding the mechanisms underlying ELS sequelae ranging from psychopathology to alterations in brain morphology.
Objective: The aim of this review was threefold. The first was to summarize the results of longitudinal data on the effects of perinatal stress on the development of mental illness in children. The second goal was to interpolate the effects of parental psychopathology on cognition. Third, to use this framework of normative brain development to interpret changes in developmental trajectories associated with deficits in cognitive and affective functioning after ELS.
Results: While ELS is associated with a variety of effects later in life, five normative principles of brain development were identified and used in this review to discuss the behavioral and neural consequences of ELS. Early adversity has been associated with deficits in a variety of cognitive (cognitive performance, memory, and executive functions) and affective (reward processing, processing of social and affective stimuli, and emotion regulation) functions.
Conclusion; we reached three general conclusions: (1) complex higher-order cognitive and affective functions associated with brain regions that have undergone prolonged postnatal development are particularly vulnerable to the deleterious effects of ELS (2) astrocytes in the hippocampus and orbital frontal cortices are particularly sensitive to early ELS; and (3) several deficits, particularly in the affective domain, appear to persist years after the end of ELS. However, there is no clear correlation between parental psychopathology during the perinatal period and the other two domains, cognitive and psychomotor, which may further explain the increased risk for later psychopathology.
Keywords: Early life Stress; Schizophrenia; Psychopathology; Anxiety; Parental Mental illness; children
INTRODUCTION
Stress is defined as the psychological response elicited when an individual perceives themselves to be under threat or challenge, and it is generally beneficial, eliciting a range of behavioural and physiological changes aimed at addressing the perceived threat. However, chronic and/or extreme stress causes these psychological, behavioural, and physiological stress response systems to be activated for an extended period, resulting in dysregulation and negative psychological and behavioural outcomes [1], [2].
Early life experiences have a significant impact on children’s neural, behavioural, and psychological development, with long-term consequences in a variety of domains [3], [4]. Throughout the lifespan, experience shapes neural plasticity and, as a result, behaviour and psychological processes. Infancy and early childhood have particularly high rates of synaptic regrowth and remodelling in the brain, and experiences can have long-term effects on development [5]. Prenatal and postnatal stress are some of the forms of early stressors that could have developmental effects on the fetuses. Prenatal stress (PS) in humans is associated with an increased vulnerability to developing a variety of psychosocial problems in both childhood and adulthood [6]. PS is linked to cognitive, behavioural, physical, and emotional problems in children, as well as autism spectrum disorder
(ASD) and attention deficit hyperactivity disorder (ADHD). In adults, PS is linked to depression and schizophrenia [7].
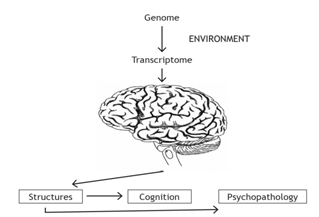
Fig 1; Pathophysiology of Mental Health: The environment interacts with the genome in the regulation of gene transcription. When these processes occur during development, the structure and function of the brain are changed, predisposing individuals to psychopathology.
Parental psychopathology has been identified as a risk factor for disruptive behaviour problems in children and adolescents, including the diagnoses of oppositional defiant disorder (ODD) and conduct disorder [8], [9].
Schizophrenia is a severe neuropsychiatric disorder that affects approximately 1% of the world’s population and is responsible for parental psychopathology. Schizophrenia is characterized by a variety of problems with thinking (cognitive), behaviour and emotions [10], [11]. Children of parents with schizophrenia have a higher risk of developing mental illness than children of parents who do not have mental illness [12], [13]. Schizophrenia is the most common mental illness in these children, with prevalence ranging from 15% to 40% in adulthood. In addition, children of schizophrenic parents are more likely to develop bipolar disorder or major depressive disorder, anxiety disorder, ADHD, and ASD. In children whose mother has a schizophrenic disorder, poor spelling at age 12 may be an increased indicator of later development of a psychotic disorder [14], [15].
There is now ample evidence that perinatal mental disorders are associated with an increase in a variety of psychological and developmental disorders in children. On the other hand, disorders are not inevitable, and effect sizes for these associations are usually moderate or small. Thus, it is critical to understand why there is an association between a particular parental disorder and child outcome and under what circumstances the risk is increased or mitigated [16]–[18].
Most researchers have attempted to answer this question by elucidating possible transmission mechanisms, i.e., the role of mediating variables underlying associations between parents’ psychopathology and outcomes in their children, and potential moderators that alter the strength of an association [16]. Children and adolescents acquire cognitive and social-emotional skills that shape their future early in life a period in which there’s robust neuroplasticity in the brains, this helps them in assuming adulthood and dealing with day-to-day stress in society [18]. The quality of the environment where children and adolescents grow up shapes their well-being and development. Early negative experiences in homes, schools, or digital spaces, such as exposure to violence, the mental illness of a parent or other caregiver, bullying and poverty, increase the risk of mental illness [19], [20].
Studies of people at high risk of mental illness have always focused on genetic factors in addition to environmental factors [21], [22]. Children of parents with a mental illness and/or addiction are more likely to develop mental illness due to both genetic and environmental factors. Offspring of parents with a severe mental illness (SMI), which is typically defined as schizophrenia, major depressive disorder, bipolar disorder, or severe borderline personality disorder (BPD), have a 50% chance of developing any mental illness and a 32% chance of developing a SMI. This is a 2.5-fold increase in risk when compared to children of parents who do not have mental illnesses [23]–[25].
The term impulse control disorder describes a person’s inability to avoid or refrain from doing things that could be harmful to themselves or others. It is not uncommon for people living with such a disorder to feel anxiety or tension before they begin to act or find relief in their behaviour – such as building up pressure or scratching an itch [26].
Even though the person knows how dangerous the action or behaviour is, and sometimes even given the negative consequences, they feel relieved, if not happy, after performing the behaviour [27], [28]. The taxon ‘impulse-control disorders not otherwise classified’ no longer exists. Instead, the above-mentioned disorders are classified as disruptive, impulse-control and conduct disorders. Attention deficit hyperactivity disorder (ADHD), trichotillomania, binge eating disorder, and pathologic gambling disorders were also removed and relegated to neurodevelopmental, obsessive-compulsive, feeding, and substance-related and addictive disorders, respectively [29], [30]. Furthermore, DSM 5 now allows ODD and CD to coexist phenomenologically and includes a severity scale for ODD. Compulsive shopping and internet addiction are now classified as ‘other specified disruptive, impulse control, and conduct disorder,’ whereas they were previously classified as disruptive behaviour disorder not otherwise specified (DBDNOS) [31], [32].
Oppositional Defiant Disorder
Oppositional defiant disorder (ODD), one of the most common clinical disorders in children and adolescents, is classified as a disruptive impulse control and conduct disorder (DICD). This occurs when children display oppositionality, vindictiveness, negativistic and hostile behaviour, and other forms of associated aggression (including verbal threats and physical acts) that cause a significant disruption in social, academic, or occupational functioning [33]. ODD is frequently associated with other psychiatric disorders, and it frequently precedes the development of conduct disorder (CD), substance abuse, and severely delinquent behaviour [34]. Management of ODD can be particularly difficult and often necessitates a multimodal approach that includes psychosocial and, on occasion, medication therapy [35].
Intermittent Explosive Disorder
Intermittent explosive disorder (IED) is a DSM-IV diagnosis characterized by repeated acts of impulsive aggression that are out of proportion to any provocation and can include verbal assault (e.g., screaming), destructive and nondestructive property assault, and/or physical attack [36], [37]. These aggressive outbursts cause a great deal of distress, as well as relationship problems and occupational difficulties. Initially thought to be uncommon, epidemiological research indicates that IED affects 4-6 per cent of the population, typically beginning in adolescence and lasting for the majority of an adult’s life. IED appears to be heritable and is likely associated with serotonin dysregulation. IED may be amenable to pharmacological and psychosocial interventions [37], [38].
Conduct Disorder
Conduct Disorder (CD) is a psychiatric diagnosis delineated by a repetitive and persistent pattern of behaviour that violates the basic rights of others as well as major age-appropriate social norms or rules [39], [40]. CD is one of the most common clinical conditions in child and adolescent mental health, with a slew of social, emotional, and behavioural issues that come at a high cost to the community. [41] conducted a systematic review that included 186,056 children and adolescents from 35 countries. The overall prevalence of conduct disorder was 8% (CI: 7-9%; I2: 99.77%), with females accounting for 7% (CI: 4-9%; I2: 99.56%) and males accounting for 11%. (CI: 7-15 percent; I2: 99.74%). The results of subgroup analysis revealed that measurement tools could explain total heterogeneity. The use of screening tools such as the Strengths and Difficulties Questionnaire (SDQ)-parent or teacher report and SDQ-self report, on the other hand, increased the pooled prevalence of conduct disorder to 10% and 16%, respectively.
Pathological Gambling
Many parts of the developing world have seen unprecedented increases in gambling availability, participation, and expenditure in recent years. In regions such as sub-Saharan Africa, this pattern of growth has become clear (SSA) [42]. Indeed, legal casinos are known to operate in several SSA countries. South Africa currently has the most casinos on the continent [43]. While the gambling industry is considered to have a beneficial impact on the economy through employment and taxation (Saunders & Doyle, 2021), unfortunately, gambling addiction is increasingly evolving into a public health concern in SSA, especially among young people (aged 10–24 years old). A biopsychosocial disorder characterized by a persistent and recurrent maladaptive pattern of gambling behaviour has been defined as a gambling addiction. This disorder has been linked to negative psychological, physical, economic, social, and legal outcomes [44], [45].
METHODS
We performed a search on July 23rd, 2022, using medical subject headings (MeSH) for articles relating to the effects of Early Life Stress and Schizophrenia On the Development of Impulse Control Disorder. We conducted computer-based searches in Medline(PubMed), EMBASE, and PsycINFO for articles published in English between inception and February 18th 2022, using the following keywords (or stems): (“early life stress” OR “early adversity” OR maltreatment OR “physical abuse” OR “sexual abuse” OR “emotional abuse” OR “psychological abuse” OR trauma OR neglect) AND (child OR childhood OR children OR infant OR adolescent OR adolescence) AND (Parental Psychopathology OR Parental stress OR Parental depression OR PTSD parents) AND (“Affective Disorder*” OR “Mood Disorder*” OR de-press* OR MDD). we also used forward and backwards searching to review bibliographies for additional studies. Finally, we sent emails describing our narrative review and its inclusion criteria to professional membership LISTSERVs of research organizations such as the American Psychological Association’s Society for a Science of Clinical Psychology, Association for Behavioral and Cognitive Therapies, and Society of Clinical Child and Adolescent Psychology. In addition, reference lists from select articles were manually reviewed for relevant studies not retrieved in searches. Articles were assessed for fit with inclusion and exclusion criteria. Inclusion criteria included studies: 1) Human studies on the relationship between effects of Early Life Stress and Schizophrenia on Development of Impulse Control Disorder. Exclusion criteria included studies: not written in English, not published in a peer reviewed journal, All Animal studies. Unpublished data sets, case studies, conference reports, non-refereed abstracts or observational studies. Multiple reports from the same data set.
In order to provide a comprehensive, up-to-date background on the effect of early life stress and schizophrenia on development of Impulse control disorder, we reviewed prominent meta-analyses as well as recent original studies that fit with the inclusion criteria described above. Meta-analyses were then used to synthesize the body of literature concerning the deferential effects prenatal and postnatal stress on development of impulse control disorder and complications of schizophrenia in Parental psychopathology. Included studies were used for a narrative review addressing the potential changes that occur in the brains that could lead to the development of the mental illness in children, effect of Parental psychopathology on cognition and alteration on biomarkers.
Search results
The search criteria yielded 1,657 articles (PubMed = 558, PsycInfo= 789, Cochrane Library = 310). After removal of duplicates, non-peer reviewed journal articles, and articles not written in English, 773 studies remained and were reviewed by title and abstract for fit with inclusion/ exclusion criteria. 47 articles underwent full-text review along with 12 others that were recovered in manual search of reference lists. Here, we have summarized findings from 59 studies that shed light on the effect of early life stress and schizophrenia on development of impulse control disorder and moreover the neurobiology relevant to the topics at hand.
Infant, Child and Adolescent Outcomes
Overview
Given the large number of studies that have examined associations between perinatal disorders and offspring outcomes, we organized this section by developmental domain, considering outcomes in the context of different disorders within each domain. Only recent studies from high-income countries (2005-2022) are included; however, because there are few studies from low- and middle-income countries (LMICs), all studies from these countries (2009-2022) were included.
Emotional (Internalizing) Difficulties and Social Development
Children’s emotional and behavioral problems are often categorized as internalizing or externalizing. Internalizing difficulties include depression and anxiety symptoms or diagnoses (e.g., separation anxiety and phobias) (J. et al., 2014; Meagher et al., 2009). A child’s social development is referred to as the development of social skills such as perspective taking, empathy, and cooperation. Prenatal depression has been reported to be associated with increased risk for emotional problems in children; self-reported symptoms and depressive disorders are associated with increased risk for clinical depression in late adolescence (Khoury et al., 2021). The increased risk for emotional problems in children of mothers who have postnatal depression has long been recognized. Infants of mothers suffering from postnatal depression are more likely to have problems with early emotion regulation and social behavior (Berthelot et al., 2020). Longitudinal studies show associations between postnatal depression and emotional outcomes across domains and ages, such as internalizing disorders, poor social skills in school, and increased risk for depression in adolescence. Although effect sizes are generally large for children of mothers with depressive disorders, risks are associated with both symptoms of depression and depressive disorder (Erickson et al., 2019; Khoury et al., 2021; Mokwena, 2021). Given the high degree of association between depression in the prenatal and postnatal periods, a large number of participants is needed to achieve sufficient power to determine whether the risks associated with prenatal and postnatal depression are independent (Pawlby⁎ et al., 2008; Pawlby et al., 2009; Pearson et al., 2013). Previous data show an independent association between prenatal and postnatal depression symptoms and offspring depression at age 18 (Field, 2010; Kersten-Alvarez et al., 2012; Madlala & Kassier, 2018). Maternal education level moderates the association between symptoms of postnatal depression and offspring depression, but not antenatal depression, implying that different mechanisms of risk are linked to antenatal and postnatal depression exposure. Fewer studies have examined the associations between prenatal and postnatal anxiety and infant emotional difficulties than perinatal depression. Because depression and anxiety are so closely related, associations attributed to one may include causes related to the other. Several studies have found that self-reported prenatal anxiety symptoms are associated with internalizing symptoms in childhood and adolescence. After antenatal and postnatal anxiety symptoms were taken into account, there was no independent effect of antenatal depression [46]–[48].
Although research on other disorders is limited, one study found that children of mothers admitted to mother-baby facilities with severe postnatal disorders have a higher risk of developing a psychiatric (mainly emotional) disorder in adulthood than siblings who were not exposed to a postnatal episode [49]–[51].
Behavioural (externalizing) Difficulties
Attention-deficit/hyperactivity disorder, oppositional defiant disorder, and conduct disorder or symptoms of any of these disorders are examples of externalizing difficulties. Several studies have found an association between prenatal depression and externalizing behavior in a child, even if the child was adopted [52], [53]. A small study found a link between antenatal depression and antisocial behavior in adolescence that was unrelated to postnatal depression. Several large longitudinal studies, including those from low- and middle-income countries, have found that symptoms and disorders of postnatal depression are linked to a child’s externalizing behavior, particularly symptoms of attention deficit hyperactivity disorder, up to the age of 16 years [54]–[57].
The association between prenatal symptoms and persistent childhood symptoms of attention deficit hyperactivity disorder was lower after accounting for postnatal symptoms in a large study of prenatal and postnatal maternal depression symptoms [58]. Self-reported maternal anxiety symptoms, both prenatal and postnatal, are associated with externalizing disorders in childhood. We found no studies using clinical diagnostic interviews, so the associations between specific anxiety disorders and children’s externalizing difficulties remain unknown [59]–[61].
Few studies have addressed the differential effects of other perinatal psychopathologies on behavioral outcomes. According to the results of one small study, infants born to mothers in whom postnatal depression and a personality disorder coincided showed dysregulated behaviors [62].
Parental Attachment
Attachment occurs when a young child uses a caregiver as a secure base from which to explore and to serve as a safe haven and source of comfort when needed. This attachment is based on early experiences with the responsiveness of the child’s caregivers [63].
Independent of postnatal depression, prenatal depression has been associated with disorganized attachment (a type of insecure attachment) [64]. Postnatal depression has been associated with increased risk of insecure (especially disorganized) mother-infant attachment in two meta-analyzes. This association is weak or not significant in community samples compared with clinical samples, and when depression is measured by self-report rather than diagnostic interviews. Infants of mothers with unipolar depression but not manic disorder were more likely to have insecure attachment at 12 months than infants of mothers without perinatal disorder in a small sample of mothers with severe psychopathology who were hospitalized postnatally. [65]–[67]. Even with paucity of papers in low- and middle-income countries, one in four and one in five mothers, respectively, are depressed after childbirth. The causes of depression could be explained by social, maternal, and psychological constructs. A high risk of adverse infant health outcomes is associated with PND [68].
Cognitive Development
Prenatal depression (both self-reported symptoms and illness) is associated with poor overall cognitive development, including low IQ scores in childhood [55], [69]–[71]. However, effect sizes are usually small, and not all studies found a significant association. Postnatal depression has been associated with a range of cognitive outcomes in early childhood, including child learning ability, achievement of developmental milestones, and language and general cognitive development (including studies from LMICs) [72]–[75]. The persistence of postnatal depression appears to be especially important in terms of cognitive development.
The long-term effects of postnatal depression on cognitive function have been studied, but the results were inconclusive. One large study found an association between postnatal depression symptoms and a very small decrease in IQ scores at 8 years of age that was no longer significant after controlling for maternal depressive symptoms after birth. Another large study found no association between postnatal depression and poor performance in mathematics at age 11, while a small British study found an association between postnatal depression and academic performance in adolescence [76], [77].
Several studies have examined perinatal depression and anxiety using self-report measures. Associations with poor infant cognitive performance were specific for depression symptoms; these studies included prenatal and postnatal symptoms. Other studies have found that prenatal anxiety symptoms, not depression, are associated with poor test performance at age 11 [78]. An association was found between prenatal anxiety symptoms and impaired executive skills. We found no studies linking other disorders in mothers during pregnancy to their child’s cognitive development [79].
Paternal Psychopathology
Traditionally, most attention is paid to the mental health of the mother. However, the importance of fathers’ mental health is increasingly being recognized. Fathers may have a direct influence on their children through the quality of their interactions or through genetic influences, or they may have an indirect influence through their support of the mother and family environment [80], [81]. A large Chinese population study found an association between symptoms of prenatal depression in the father and poor socioemotional and behavioral development of children in the first month of life; postnatal symptoms were not studied. [82]. In contrast, another study found no evidence that paternal symptoms of prenatal depression were associated with child depression at age 18, but only an association with paternal symptoms of postnatal depression [83].
Symptoms of paternal postnatal mental disorders have been linked to an increased risk of emotional and behavioral disorders in young children, as well as difficulties with language development and depression at age 18. In the postnatal period, paternal and maternal depression appear to have similar effects on behavioral outcomes, whereas maternal depression is associated with higher risk for emotional difficulties. A meta-analysis of associations between maternal and paternal disorders and the child’s internalizing or externalizing difficulties in childhood found that the younger the child was at the time of the study, the larger the effect sizes for associations with maternal depression, whereas the opposite was found for paternal depression. [83]–[86].
Mechanism & Future Perspectives
Overview
The figure describes a model that summarizes the potential mechanisms underlying the links between parental psychiatric disorders and child development. Biologically mediated effects of prenatal disorders (via effects in utero) would occur only in mothers, whereas postnatal effects and genetic effects could occur when both parents are affected by a disorder.
Genetic Factor
Common genetic risk factors are most likely responsible for part of the association between parental mental disorders at any time point (including the perinatal period) and child vulnerability. However, there is evidence that the environment plays an important role in the development of mental disorders [87]. Through genetic confounding, correlations (both passive and evocative) between genetic and environmental factors could explain some of the variance in associations between parental interference and child outcomes. Our understanding of this genetic contribution is still limited.
Individual differences in susceptibility to environmental factors may also be determined by the inherited genotype of the child. The possibility that gene polymorphisms may mitigate the effects of many early childhood adversities, including maternal mental disorders, on child development has piqued the interest of researchers [88]. Although there are some anecdotal reports of the effects of gene-environment interactions when applied to both prenatal and postnatal environments, the results are often not replicated, and the effects of individual genetic variations on environmental exposure change are likely to be very small, and genetic susceptibility to the environment is defined by many interactive variations in the genome. [89], [90].
Epigenetics
Epigenetic changes (alteration of gene expression without alteration of genetic sequence, e.g., by methylation) are one mechanism proposed to explain the long-term effects of early life experiences, including the perinatal environment, on biological and behavioral phenotypes. Most of the research comes from animal studies; however, preliminary studies in humans show that prenatal stress and anxiety increase methylation (i.e., silencing) of glucocorticoid receptors (involved in stress responses) in children. Maternal psychological distress may alter maternal caregiving after birth, leading to epigenetic changes in offspring in animal studies. Although this hypothesis has not been formally tested, epigenetic pathways may mediate the link between maternal disorders and child outcomes. [91]–[93].
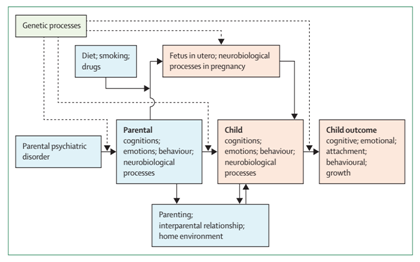
Figure 2: Possible mechanisms underlying the association of parental psychiatric disorders and child outcomes Dotted lines show genetic processes. Solid lines show interactions. Orange colors refer to the child. Blue colors refer to the parents. Green represents genetic processes. Figure is based on figure 1 from Stein and Harold.
Astrocytes Density in the Hippocampus and Pre-fontal cortices
The hippocampus is a key limbic structure involved in the formation and retrieval of memories, including autobiographical memories. Place cells, together with grid cells in the intervening entorhinal cortex, form an internal positioning system for the spatiotemporal representation of places, ways, and related experiences in the hippocampus. Several psychiatric disorders, including post-traumatic stress disorder, major depression, schizophrenia, bipolar disorder, and borderline personality disorder, have been associated with abnormalities in the hippocampus. [94], [95].
The hippocampus is also the brain’s most obvious target when reflecting on the possible effects of childhood maltreatment [96], [97]. It is highly susceptible to damage from high levels of glucocorticoids such as cortisol because it is densely populated with glucocorticoid receptors. In addition, preclinical studies have shown that chronic glucocorticoid exposure leads to reversible atrophy of dendritic processes on pyramidal cells in the cornu ammonis as well as suppression of neurogenesis in the dentate gyrus (DG) [98], [99].
Overall, there is compelling evidence that adults with histories of maltreatment have smaller hippocampuses than non-maltreated comparison subjects. We found 37 papers reporting hippocampal findings in adults with childhood maltreatment histories at the time of writing, and 30 of these papers reported one or more significant differences between groups with and without maltreatment histories or an inverse correlation between maltreatment severity and hippocampal volume. Three papers that reported non-significant effects found near-significant reductions or correlations (in the nonabusive sample). Another study found no differences in a geriatric sample (mean age 70.93.7 years) and may have been confounded by aging effects. All three remaining studies that found no significant changes in hippocampus examined only female participants and had small sample sizes [100]–[103].
DISCUSSION AND CONCLUSION
From a policy perspective, identifying both parents and children at increased risk for adverse outcomes due to perinatal mental disorders is an important first step in providing early treatment and prevention. Children have needs that cannot always be met by treating the parental disorder alone. Although much progress has been made in understanding the mechanisms and pathways that lead to both healthy and disordered child development, much remains to be done. For example, most mental disorders or symptoms in pregnancy often persist after birth, giving rise to questions about the contribution of prenatal and postnatal stress and the extent to which their contributions differ, influence each other, or accumulate. Whether prenatal effects are caused by a direct impact on fetal development or because prenatal symptoms persist after birth is still a gray area to which we intend to provide answers. Understanding the mechanisms, especially the modifiable pathways, is critical
REFFERENCES
[1] B. S. McEwen, “The resilient brain: Epigenetics, stress and the lifecourse,” Psychoneuroendocrinology, 2017, doi: 10.1016/j.psyneuen.2017.07.442.
[2] R. M. Sapolsky, “Stress and the brain: Individual variability and the inverted-U,” Nature Neuroscience. 2015, doi: 10.1038/nn.4109.
[3] M. Bischoff et al., “Save the children by treating their mothers (PriVileG-M-study) – Study protocol: A sequentially randomized controlled trial of individualized psychotherapy and telemedicine to reduce mental stress in pregnant women and young mothers and to improve Child’s,” BMC Psychiatry, 2019, doi: 10.1186/s12888-019-2279-0.
[4] T. Mpofana, W. M. U. Daniels, and M. V. Mabandla, “Exposure to Early Life Stress Results in Epigenetic Changes in Neurotrophic Factor Gene Expression in a Parkinsonian Rat Model,” Parkinsons. Dis., 2016, doi: 10.1155/2016/6438783.
[5] D. Cicchetti, “Resilience under conditions of extreme stress: A multilevel perspective,” World Psychiatry. 2010, doi: 10.1002/j.2051-5545.2010.tb00297.x.
[6] L. M. Laifer, D. Dilillo, and R. L. Brock, “Prenatal negative affectivity and trauma-related distress predict mindful parenting during toddler age: Examining parent-infant bonding as a mechanism,” Dev. Psychopathol., 2021, doi: 10.1017/S0954579421000894.
[7] E. Lipner, S. K. Murphy, and L. M. Ellman, “Prenatal Maternal Stress and the Cascade of Risk to Schizophrenia Spectrum Disorders in Offspring,” Current Psychiatry Reports. 2019, doi: 10.1007/s11920-019-1085-1.
[8] A. M. Chronis, B. B. Lahey, W. E. Pelham, H. L. Kipp, B. L. Baumann, and S. S. Lee, “Psychopathology and substance abuse in parents of young children with attention-deficit/hyperactivity disorder,” J. Am. Acad. Child Adolesc. Psychiatry, 2003, doi: 10.1097/00004583-200312000-00009.
[9] A. Fernandez-Quintana, K. W. Nilsson, and S. Olofsdotter, “P.044 Mental Health in children of parents with ADHD: current knowledge and future research opportunities,” Eur. Neuropsychopharmacol., 2020, doi: 10.1016/j.euroneuro.2020.09.044.
[10] G. Ayano, G. Tesfaw, and S. Shumet, “The prevalence of schizophrenia and other psychotic disorders among homeless people: A systematic review and meta-analysis,” BMC Psychiatry. 2019, doi: 10.1186/s12888-019-2361-7.
[11] G. Blackman and J. H. MacCabe, “Schizophrenia,” Medicine (United Kingdom). 2020, doi: 10.1016/j.mpmed.2020.08.004.
[12] D. Rasic, T. Hajek, M. Alda, and R. Uher, “Risk of mental illness in offspring of parents with schizophrenia, bipolar disorder, and major depressive disorder: A meta-analysis of family high-risk studies,” Schizophr. Bull., 2014, doi: 10.1093/schbul/sbt114.
[13] D. Rasic, T. Hajek, M. Alda, and R. Uher, “Risk of mental illness in offspring of parents with schizophrenia, bipolar disorder and major depressive disorder: a meta-analysis of family high-risk studies,” Compr. Psychiatry, 2013, doi: 10.1016/j.comppsych.2013.07.057.
[14] S. L. Matheson et al., “Effects of maltreatment and parental schizophrenia spectrum disorders on early childhood social-emotional functioning: A population record linkage study,” Epidemiol. Psychiatr. Sci., 2017, doi: 10.1017/S204579601600055X.
[15] N. Sadeghi, F. Etedali, M. F. Moghadam, and A. Shamsi, “Comparison of behavioral problems between the children with one schizophrenic parent and children with healthy parents,” Psychiatria, 2021, doi: 10.5603/psych.2020.0023.
[16] D. A. Winiarski, M. L. Engel, N. S. Karnik, and P. A. Brennan, “Early Life Stress and Childhood Aggression: Mediating and Moderating Effects of Child Callousness and Stress Reactivity,” Child Psychiatry Hum. Dev., 2018, doi: 10.1007/s10578-018-0785-9.
[17] N. M. Morelli et al., “Reward-related neural correlates of early life stress in school-aged children,” Dev. Cogn. Neurosci., 2021, doi: 10.1016/j.dcn.2021.100963.
[18] J. L. Hanson, A. V. Williams, D. A. Bangasser, and C. J. Peña, “Impact of Early Life Stress on Reward Circuit Function and Regulation,” Frontiers in Psychiatry. 2021, doi: 10.3389/fpsyt.2021.744690.
[19] J. P. Shonkoff et al., “The lifelong effects of early childhood adversity and toxic stress,” Pediatrics, 2012, doi: 10.1542/peds.2011-2663.
[20] Prenatal Stress and Child Development. 2021.
[21] C. Murgatroyd and D. Spengler, “Epigenetics of early child development,” Frontiers in Psychiatry. 2011, doi: 10.3389/fpsyt.2011.00016.
[22] J. C. Gomez-Verjan, O. S. Barrera-Vázquez, L. García-Velázquez, R. Samper-Ternent, and P. Arroyo, “Epigenetic variations due to nutritional status in early-life and its later impact on aging and disease,” Clin. Genet., 2020, doi: 10.1111/cge.13748.
[23] Y. Everett, C. G. Martin, and M. Zalewski, “A Systematic Review Focusing on Psychotherapeutic Interventions that Impact Parental Psychopathology, Child Psychopathology and Parenting Behavior,” Clinical Child and Family Psychology Review. 2021, doi: 10.1007/s10567-021-00355-3.
[24] E. H. Steele and C. McKinney, “Relationships Among Emerging Adult Psychological Problems, Maltreatment, and Parental Psychopathology: Moderation by Parent–Child Relationship Quality,” Fam. Process, 2020, doi: 10.1111/famp.12407.
[25] J. L. Silberg, H. Maes, and L. J. Eaves, “Genetic and environmental influences on the transmission of parental depression to children’s depression and conduct disturbance: An extended Children of Twins study,” J. Child Psychol. Psychiatry Allied Discip., 2010, doi: 10.1111/j.1469-7610.2010.02205.x.
[26] K. Lieb, M. C. Zanarini, C. Schmahl, P. M. M. Linehan, and P. M. Bohus, “Borderline personality disorder,” in Lancet, 2004, doi: 10.1016/S0140-6736(04)16770-6.
[27] &NA;, “DSM V,” J. Dev. Behav. Pediatr., 2013, doi: 10.1097/dbp.0b013e3182978a90.
[28] V. Del Barrio, “Diagnostic and statistical manual of mental disorders,” in The Curated Reference Collection in Neuroscience and Biobehavioral Psychology, 2016.
[29] H. Van Marle, “Impulse-control disorders and behavioural and personality disorders in DSM-5: No more age-limits or rigid category boundaries,” Tijdschr. Psychiatr., 2014.
[30] P. N. Dannon, “The 21st century and reevaluation of impulse control disorders,” Frontiers in Psychiatry. 2010, doi: 10.3389/fpsyt.2010.00008.
[31] C. C. Probst and T. van Eimeren, “The functional anatomy of impulse control disorders.,” Current neurology and neuroscience reports. 2013, doi: 10.1007/s11910-013-0386-8.
[32] M. E. Yuksel et al., “9th International Congress on Psychopharmacology & 5th International Symposium on Child and Adolescent Psychopharmacology,” Psychiatry Clin. Psychopharmacol., 2017, doi: 10.1080/24750573.2017.1314599.
[33] M. R. Mohammadi et al., “Lifetime prevalence, sociodemographic predictors, and comorbidities of oppositional defiant disorder: The national epidemiology of iranian child and adolescent psychiatric disorders (IRCAP),” Brazilian J. Psychiatry, 2020, doi: 10.1590/1516-4446-2019-0416.
[34] J. Schoorl, S. van Rijn, M. de Wied, S. van Goozen, and H. Swaab, “Boys with Oppositional Defiant Disorder/Conduct Disorder Show Impaired Adaptation During Stress: An Executive Functioning Study,” Child Psychiatry Hum. Dev., 2018, doi: 10.1007/s10578-017-0749-5.
[35] “Practice parameter for the assessment and treatment of children and adolescents with oppositional defiant disorder,” J. Am. Acad. Child Adolesc. Psychiatry, 2007, doi: 10.1097/01.chi.0000246060.62706.af.
[36] M. K. Fahlgren, A. A. Puhalla, K. M. Sorgi, and M. S. McCloskey, “Emotion processing in intermittent explosive disorder,” Psychiatry Res., 2019, doi: 10.1016/j.psychres.2019.01.046.
[37] E. F. Coccaro, “A family history study of intermittent explosive disorder,” J. Psychiatr. Res., 2010, doi: 10.1016/j.jpsychires.2010.04.006.
[38] M. S. McCloskey, K. Kleabir, M. E. Berman, E. Y. Chen, and E. F. Coccaro, “Unhealthy Aggression: Intermittent Explosive Disorder and Adverse Physical Health Outcomes,” Heal. Psychol., 2010, doi: 10.1037/a0019072.
[39] A. Junewicz and S. B. Billick, “Conduct Disorder: Biology and Developmental Trajectories,” Psychiatric Quarterly. 2020, doi: 10.1007/s11126-019-09678-5.
[40] P. J. Frick and E. C. Kemp, “Conduct Disorders and Empathy Development,” Annual Review of Clinical Psychology. 2021, doi: 10.1146/annurev-clinpsy-081219-105809.
[41] M. R. Mohammadi, M. Salmanian, and Z. Keshavarzi, “The global prevalence of conduct disorder: A systematic review and meta-analysis,” Iran. J. Psychiatry, 2021, doi: 10.18502/ijps.v16i2.5822.
[42] H. Sinclair, S. Pasche, A. Pretorius, and D. J. Stein, “Clinical profile and psychiatric comorbidity of treatment-seeking individuals with pathological gambling in South-Africa,” J. Gambl. Stud., 2014, doi: 10.1007/s10899-014-9516-8.
[43] G. N. Stein, A. Pretorius, D. J. Stein, and H. Sinclair, “The association between pathological gambling and suicidality in treatment-seeking pathological gamblers in South Africa,” Ann. Clin. Psychiatry, 2016.
[44] K. Vaddiparti and L. B. Cottler, “Personality disorders and pathological gambling,” Current Opinion in Psychiatry. 2017, doi: 10.1097/YCO.0000000000000300.
[45] L. L. Ashley and K. K. Boehlke, “Pathological gambling: A general overview,” J. Psychoactive Drugs, 2012, doi: 10.1080/02791072.2012.662078.
[46] M. Hernandez-Reif, T. Field, M. Diego, Y. Vera, and J. Pickens, “Happy faces are habituated more slowly by infants of depressed mothers,” Infant Behav. Dev., 2006, doi: 10.1016/j.infbeh.2005.07.003.
[47] W. Nilsen, J. Dion, E. B. Karevold, and A. Skipstein, “Maternal Psychological Distress and Offspring Psychological Adjustment in Emerging Adulthood: Findings from over 18 Years,” J. Dev. Behav. Pediatr., 2016, doi: 10.1097/DBP.0000000000000365.
[48] R. M. Pearson et al., “Maternal depression during pregnancy and the postnatal period risks and possible mechanisms for offspring depression at age 18 years,” JAMA Psychiatry, 2013, doi: 10.1001/jamapsychiatry.2013.2163.
[49] R. Abbott, V. J. Dunn, S. A. Robling, and E. S. Paykel, “Long-term outcome of offspring after maternal severe puerperal disorder,” Acta Psychiatr. Scand., 2004, doi: 10.1111/j.1600-0447.2004.00406.x.
[50] S. A. et al., “Effects of perinatal mental disorders on the fetus and child,” The Lancet. 2014.
[51] M. S. Tavaragi, “Postpartum depression – its prevalence and correlation with family dynamics, at a tertiary care hospital,” Indian J. Psychiatry, 2019.
[52] F. P. Velders et al., “Prenatal and postnatal psychological symptoms of parents and family functioning: The impact on child emotional and behavioural problems,” Eur. Child Adolesc. Psychiatry, 2011, doi: 10.1007/s00787-011-0178-0.
[53] M. M. Al-Amin et al., “Predictors of postnatal mother-infant bonding: The role of antenatal bonding, maternal substance use and mental health.,” Arch. Womens. Ment. Health, 2016.
[54] A. S. et al., “Behaviour problems in children-a longitudinal study of genetic and environmental factors,” Eur. Child Adolesc. Psychiatry, 2015.
[55] E. D. Barker, S. R. Jaffee, R. Uher, and B. Maughan, “The contribution of prenatal and postnatal maternal anxiety and depression to child maladjustment,” Depress. Anxiety, 2011, doi: 10.1002/da.20856.
[56] C. Winsper, D. Wolke, and T. Lereya, “Prospective associations between prenatal adversities and borderline personality disorder at 11-12 years,” Psychol. Med., 2015, doi: 10.1017/S0033291714002128.
[57] M. Korhonen, I. Luoma, R. Salmelin, and T. Tamminen, “Maternal depressive symptoms: Associations with adolescents’ internalizing and externalizing problems and social competence,” Nord. J. Psychiatry, 2014, doi: 10.3109/08039488.2013.838804.
[58] H. Huhdanpää et al., “Prenatal and Postnatal Predictive Factors for Children’s Inattentive and Hyperactive Symptoms at 5 Years of Age: The Role of Early Family-related Factors,” Child Psychiatry Hum. Dev., 2021, doi: 10.1007/s10578-020-01057-7.
[59] E. Norén Selinus et al., “Subthreshold and threshold attention deficit hyperactivity disorder symptoms in childhood: psychosocial outcomes in adolescence in boys and girls,” Acta Psychiatr. Scand., 2016, doi: 10.1111/acps.12655.
[60] R. P. Breaux, H. R. Brown, and E. A. Harvey, “Mediators and Moderators of the Relation between Parental ADHD Symptomatology and the Early Development of Child ADHD and ODD Symptoms,” J. Abnorm. Child Psychol., 2017, doi: 10.1007/s10802-016-0213-1.
[61] L. W. Wesseldijk et al., “Risk factors for parental psychopathology: a study in families with children or adolescents with psychopathology,” Eur. Child Adolesc. Psychiatry, 2018, doi: 10.1007/s00787-018-1156-6.
[62] J. Fritz, A. M. de Graaff, H. Caisley, A. L. van Harmelen, and P. O. Wilkinson, “A Systematic Review of Amenable Resilience Factors That Moderate and/or Mediate the Relationship Between Childhood Adversity and Mental Health in Young People,” Frontiers in Psychiatry. 2018, doi: 10.3389/fpsyt.2018.00230.
[63] C. Cookman, “Attachment in older adulthood: Concept clarification,” J. Adv. Nurs., 2005, doi: 10.1111/j.1365-2648.2005.03435.x.
[64] S. L. Toth, F. A. Rogosch, M. Sturge-Apple, and D. Cicchetti, “Maternal depression, children’s attachment security, and representational development: An organizational perspective,” Child Dev., 2009, doi: 10.1111/j.1467-8624.2008.01254.x.
[65] L. J. Hayes, S. H. Goodman, and E. Carlson, “Maternal antenatal depression and infant disorganized attachment at 12 months,” Attach. Hum. Dev., 2013, doi: 10.1080/14616734.2013.743256.
[66] M. Galbally, S. J. Watson, M. H. van IJzendoorn, A. Tharner, M. Luijk, and A. J. Lewis, “Maternal trauma but not perinatal depression predicts infant-parent attachment,” Arch. Womens. Ment. Health, 2022, doi: 10.1007/s00737-021-01192-7.
[67] E. Lefkovics, I. Baji, and J. Rigó, “Impact of maternal depression on pregnancies and on early attachment,” Infant Ment. Health J., 2014, doi: 10.1002/imhj.21450.
[68] A. F. Dadi, E. R. Miller, and L. Mwanri, “Postnatal depression and its association with adverse infant health outcomes in low-and middle-income countries: A systematic review and meta-analysis,” BMC Pregnancy Childbirth, 2020, doi: 10.1186/s12884-020-03092-7.
[69] S. Zheng, K. LeWinn, T. Ceja, M. Hanna-Attisha, L. O’Connell, and S. Bishop, “Adaptive Behavior as an Alternative Outcome to Intelligence Quotient in Studies of Children at Risk: A Study of Preschool-Aged Children in Flint, MI, USA,” Front. Psychol., 2021, doi: 10.3389/fpsyg.2021.692330.
[70] J. Evans et al., “The timing of maternal depressive symptoms and child cognitive development: A longitudinal study,” J. Child Psychol. Psychiatry Allied Discip., 2012, doi: 10.1111/j.1469-7610.2011.02513.x.
[71] E. L. Prado et al., “Maternal depression is the predominant persistent risk for child cognitive and social-emotional problems from early childhood to pre-adolescence: A longitudinal cohort study,” Soc. Sci. Med., 2021, doi: 10.1016/j.socscimed.2021.114396.
[72] C. Hadley, A. Tegegn, F. Tessema, M. Asefa, and S. Galea, “Parental symptoms of common mental disorders and children’s social, motor, and language development in sub-Saharan Africa,” Ann. Hum. Biol., 2008, doi: 10.1080/03014460802043624.
[73] A. M. Hatcher, A. Gibbs, R. Jewkes, R. S. McBride, D. Peacock, and N. Christofides, “Effect of Childhood Poverty and Trauma on Adult Depressive Symptoms Among Young Men in Peri-Urban South African Settlements,” J. Adolesc. Heal., 2019, doi: 10.1016/j.jadohealth.2018.07.026.
[74] H. Mebrahtu et al., “The impact of common mental disorders among caregivers living with HIV on child cognitive development in Zimbabwe,” AIDS Care – Psychol. Socio-Medical Asp. AIDS/HIV, 2020, doi: 10.1080/09540121.2020.1739216.
[75] J. G. Uriyo, A. Abubakar, M. Swai, S. E. Msuya, and B. Stray-Pedersen, “Prevalence and Correlates of Common Mental Disorders among Mothers of Young Children in Kilimanjaro Region of Tanzania,” PLoS One, 2013, doi: 10.1371/journal.pone.0069088.
[76] N. L. Letourneau, L. Tramonte, and J. D. Willms, “Maternal depression, family functioning and children’s longitudinal development,” J. Pediatr. Nurs., 2013, doi: 10.1016/j.pedn.2012.07.014.
[77] I. Landi, M. Giannotti, P. Venuti, and S. de Falco, “Maternal and family predictors of infant psychological development in at-risk families: A multilevel longitudinal study,” Res. Nurs. Heal., 2020, doi: 10.1002/nur.21989.
[78] D. F. Hay, S. Pawlby, D. Sharp, P. Asten, A. Mills, and R. Kumar, “Intellectual problems shown by 11-year-old children whose mothers had postnatal depression,” J. Child Psychol. Psychiatry Allied Discip., 2001, doi: 10.1111/1469-7610.00784.
[79] C. Buss, E. P. Davis, C. J. Hobel, and C. A. Sandman, “Maternal pregnancy-specific anxiety is associated with child executive function at 69 years age,” Stress, 2011, doi: 10.3109/10253890.2011.623250.
[80] P. Ramchandani and L. Psychogiou, “Paternal psychiatric disorders and children’s psychosocial development,” The Lancet. 2009, doi: 10.1016/S0140-6736(09)60238-5.
[81] J. E. Buizer-Voskamp et al., “Paternal age and psychiatric disorders: Findings from a Dutch population registry,” Schizophr. Res., 2011, doi: 10.1016/j.schres.2011.03.021.
[82] P. Ip et al., “Associations of paternal postpartum depressive symptoms and infant development in a Chinese longitudinal study,” Infant Behav. Dev., 2018, doi: 10.1016/j.infbeh.2018.08.002.
[83] M. C. Finsaas et al., “Early Childhood Psychopathology Prospectively Predicts Social Functioning in Early Adolescence,” J. Clin. Child Adolesc. Psychol., 2020, doi: 10.1080/15374416.2018.1504298.
[84] D. Weijers, F. J. A. van Steensel, and S. M. Bögels, “Associations between Psychopathology in Mothers, Fathers and Their Children: A Structural Modeling Approach,” J. Child Fam. Stud., 2018, doi: 10.1007/s10826-018-1024-5.
[85] L. D. van der Pol et al., “Associations Between Fathers’ and Mothers’ Psychopathology Symptoms, Parental Emotion Socialization, and Preschoolers’ Social-Emotional Development,” J. Child Fam. Stud., 2016, doi: 10.1007/s10826-016-0490-x.
[86] H. B. Vidair et al., “Screening parents during child evaluations: Exploring parent and child psychopathology in the same clinic,” J. Am. Acad. Child Adolesc. Psychiatry, 2011, doi: 10.1016/j.jaac.2011.02.002.
[87] K. J. Hsu, K. C. Young-Wolff, K. S. Kendler, L. J. Halberstadt, and C. A. Prescott, “Neuropsychological deficits in major depression reflect genetic/familial risk more than clinical history: A monozygotic discordant twin-pair study,” Psychiatry Res., 2014, doi: 10.1016/j.psychres.2013.10.037.
[88] W. M. Weikum, L. C. Mayes, R. E. Grunau, U. Brain, and T. F. Oberlander, “The impact of prenatal serotonin reuptake inhibitor (SRI) antidepressant exposure and maternal mood on mother-infant interactions at 3 months of age,” Infant Behav. Dev., 2013, doi: 10.1016/j.infbeh.2013.04.001.
[89] R. Feldman, M. Monakhov, M. Pratt, and R. P. Ebstein, “Oxytocin Pathway Genes: Evolutionary Ancient System Impacting on Human Affiliation, Sociality, and Psychopathology,” Biological Psychiatry. 2016, doi: 10.1016/j.biopsych.2015.08.008.
[90] V. Mileva-Seitz et al., “Interaction between Oxytocin Genotypes and Early Experience Predicts Quality of Mothering and Postpartum Mood,” PLoS One, 2013, doi: 10.1371/journal.pone.0061443.
[91] E. C. Braithwaite, M. Kundakovic, P. G. Ramchandani, S. E. Murphy, and F. A. Champagne, “Maternal prenatal depressive symptoms predict infant NR3C1 1F and BDNF IV DNA methylation,” Epigenetics, 2015, doi: 10.1080/15592294.2015.1039221.
[92] H. Palma-Gudiel, A. Córdova-Palomera, E. Eixarch, M. Deuschle, and L. Fañanás, “Maternal psychosocial stress during pregnancy alters the epigenetic signature of the glucocorticoid receptor gene promoter in their offspring: A meta-analysis,” Epigenetics. 2015, doi: 10.1080/15592294.2015.1088630.
[93] M. Szyf, “DNA methylation, behavior and early life adversity,” Journal of Genetics and Genomics. 2013, doi: 10.1016/j.jgg.2013.06.004.
[94] M. Loi, J. C. L. Mossink, G. F. Meerhoff, J. L. Den Blaauwen, P. J. Lucassen, and M. Joëls, “Effects of early-life stress on cognitive function and hippocampal structure in female rodents,” Neuroscience, 2017, doi: 10.1016/j.neuroscience.2015.08.024.
[95] E. F. G. Naninck et al., “Chronic early life stress alters developmental and adult neurogenesis and impairs cognitive function in mice,” Hippocampus, 2015, doi: 10.1002/hipo.22374.
[96] S. J. H. van Rooij et al., “Increased activation of the fear neurocircuitry in children exposed to violence,” Depress. Anxiety, 2020, doi: 10.1002/da.22994.
[97] M. H. Teicher, J. A. Samson, C. M. Anderson, and K. Ohashi, “The effects of childhood maltreatment on brain structure, function and connectivity,” Nature Reviews Neuroscience. 2016, doi: 10.1038/nrn.2016.111.
[98] A. K. Smith, “Voxelwise mapping of neuronal structural connectivity in adolescents [thesis],” 2012.
[99] D. Glaser, “The effects of child maltreatment on the developing brain,” Med. Leg. J., 2014, doi: 10.1177/0025817214540395.
[100] N. D. Alves et al., “Chronic stress targets adult neurogenesis preferentially in the suprapyramidal blade of the rat dorsal dentate gyrus,” Brain Struct. Funct., 2018, doi: 10.1007/s00429-017-1490-3.
[101] M. Egeland, P. A. Zunszain, and C. M. Pariante, “Molecular mechanisms in the regulation of adult neurogenesis during stress,” Nature Reviews Neuroscience. 2015, doi: 10.1038/nrn3855.
[102] P. J. Lucassen et al., “Regulation of adult neurogenesis and plasticity by (Early) stress, glucocorticoids, and inflammation,” Cold Spring Harb. Perspect. Biol., 2015, doi: 10.1101/cshperspect.a021303.
[103] S. Chetty et al., “Stress and glucocorticoids promote oligodendrogenesis in the adult hippocampus,” Mol. Psychiatry, 2014, doi: 10.1038/mp.2013.190.