
Etiology and Pattern of Ocular Trauma in Children and Their Management Consequences
- Dr.Afrina Khanam
- Jannatun Noor
- Dr. Nasimul Gani Chowdhury
- Sheikh Tamima Hasan
- Urmi Atika Islam
- Dr.Homayon Kabir
- Dr Naorin Jahan
- 1143-1149
- Mar 22, 2025
- Medicine
Etiology and Pattern of Ocular Trauma in Children and their Management Consequences
Dr. Afrina Khanam (MBBS)1*, Jannatun Noor (B.Optom)2, Dr. Nasimul Gani Chowdhury (MBBS, DCO, FCPS)3, Sheikh Tamima Hasan4, Urmi Atika Islam(B.Optom)5, Dr. Homayon Kabir (MBBS, DO)6, Dr Naorin Jahan7
1MS Resident, Institute of Community Ophthalmology (ICO), Chittagong Eye Infirmary & Training Complex Campus, Chittagong.
2Lecturer (Optometry), Institute of Community Ophthalmology (ICO), Chittagong Eye Infirmary & Training Complex Campus, Chittagong.
3Chief Consultant, Pediatric Ophthalmology Department, Chittagong Eye Infirmary & Training Complex (CEITC), Chittagong
4Assistant Professor (Optometry), Institute of Community Ophthalmology (ICO), Chittagong Eye Infirmary & Training Complex Campus, Chittagong.
5Teaching Assistant, Institute of Community Ophthalmology (ICO), Chittagong Eye Infirmary & Training Complex Campus, Chittagong.
6Fellow Pediatric Ophthalmology, Institute of Community Ophthalmology (ICO), Chittagong Eye Infirmary & Training Complex Campus, Chittagong.
7MS Resident, Institute of Community Ophthalmology (ICO), Chittagong Eye Infirmary & Training Complex Campus, Chittagong.
Corresponding Author*
DOI: https://doi.org/10.51244/IJRSI.2025.12020091
Received: 13 February 2025; Accepted: 17 February 2025; Published: 22 March 2025
ABSTRACT
Purpose: to determine the common causes of ocular trauma in the pediatric age group and their visual outcome after surgical intervention.
Methods: A retrospective study was conducted with the children underwent surgical intervention for ocular trauma between January 2021 to December 2023. Children reported at pediatric outpatient and emergency department with age range 0 to 16 years were enrolled. Various epidemiological parameters like age, sex distribution, duration of presentation, mode of injury, type of injury, and final visual outcome were analyzed.
Results: Out of 200 patients, 90% were below the age of 12 years; 35.5 % of children with ocular trauma belonged to age group 0 to 4years. The male to female ratio was 2:1. In this study, 149(74.5%) cases presented with corneal injury. Among ocular injuries, the major traumatic agents were wooden objects 70 (35%) and sharp object 38 (19%). Home was the most common place of injury152 (76%), followed by playground 27(13.5%), school 20 (10%) and workplace 1(0.5%). 27 (13.5%) cases were closed globe injuries and the rest 173 (86.5%) were open globe injuries. Most of the cases needed single surgery 128 (64%) and the rest 72 (36%) underwent multiple surgeries. Among them 41.5% needed repair of corneal injury with excision of prolapsed iris and 34% cases treated with IOL implantation with PPC & AVT later on. 48.5% of the patients got better visual acuity ranging from 6/6 to 6/18. In 12% cases central, steady, maintained were present, 39.5% patients were visually impaired and 4.5% developed phthisis bulbi.
Conclusion: Pediatric eye injuries occur most frequently in the home setting and mostly as the result of the use of wooden sticks and sharp objects like glass pieces, knife, and scissors, pen/pencil, and toy pistols. Corneal scars, astigmatism and amblyopia remain the most common causes of decreased vision after management of injuries in children.
INTRODUCTION
One of the main causes of non-congenital vision impairment in children is pediatric ocular trauma. Human misery, permanent disability, lost productivity, and financial difficulties are only a few of the numerous problems associated with these traumas 1. Ocular trauma can cause anything from minor to very serious conditions that can cause blindness 2. Although the annual incidence of ocular trauma is 15.2 per 100,000, it is significantly greater in developing nations and among those from poorer socioeconomic backgrounds3.
According to United States eye injury registry (USEIR), male to female ratio in pediatric population was 3:1. Pediatric eye injuries account for approximately 8%–14% of total injuries in children 4. And overall cases of ocular trauma, 52% cases are of pediatric group. Eye trauma is the most prevalent cause of unilateral blindness, with around 1.6 million people blind from eye injuries, 2.3 million with bilateral impaired vision, and 19 million with unilateral visual loss5.
Almost any environment can result in pediatric ocular injury, including homes, rural areas, sports-related activities, and auto accidents. It has been consistently shown that well-thought-out preventive strategies founded on reliable epidemiologic data are cost-effective 6.
The purpose of this study was to determine the pattern and common causes of ocular trauma in children presenting at the tertiary eye care center and evaluating various factors related to ocular trauma.
METHODS
This retrospective study was conducted in pediatric ophthalmology department of Chittagong eye infirmary and training complex in the period from January 2021 to December 2023. All patients with ocular trauma underwent surgical management aged between 0 and 16 years were included in this study. Patients with closed globe injuries that was not underwent surgical management was excluded from the study. Written informed consents were provided by all the parents and care givers of the study participants. Thorough history was obtained from the attending person regarding the socio demographics of the injured child and the circumstances of the injury. All patients were reviewed on the basis of age, gender, laterality, type of traumatic agents, mechanism of injury, place of injury, and number of surgeries. Distance between home and hospital, time interval between occurrence of injury and hospital admission were also recorded.
The initial clinical examination included visual assessment on presentation. These were followed by the biomicroscopic examination to assess the anterior segment damage (subconjunctival hemorrhage, corneal/scleral laceration, hyphaema, inflammation, irregular pupil, iris prolapse, lens subluxation, and cataract), and/or the posterior segment damage such as vitreous hemorrhage, retinal detachment, and choroidal hemorrhage. Conjunctival swabs were taken for microscopic examination and culture sensitivity (ME & C/S). X-ray chest and complete blood count were done before surgery. A thorough ophthalmic examination was performed in the pediatric or emergency department and was complemented by examination under anesthesia (EUA) if this was deemed necessary. When the surgical intervention was considered, EUA was conducted as the initial part of the surgical intervention. Ocular injuries were classified as per the World Health Organization (WHO) and Birmingham Eye Trauma Terminology System (BETTS). Managements given either in the form of medical or surgical intervention were noted. The subsequent follow-up findings were noted at 1 week, 1 month, 3 months and final best corrected visual acuity was taken at the end of 6 months.
Statistical Analysis
Data was analyzed using SPSS (version 16.0; IBM Inc., Chicago, IL, USA). Descriptive analysis was done, where categorical variables were presented as frequencies and percentages and continuous variables in the form of mean (±standard deviation) and range (minimum to maximum). A p-value below 0.05 was interpreted as an indicator of statistical significance.
RESULT
Out of 200 patients, 72.5% were male and 27.5% were female with the mean age of 6.9 3.8 years. The entire participant was grouped into four categories where majority of patients were in the age group of o to 4 years (39.5%). According to the clinical data 110 (55%) cases presented to the hospital within 24 hours of trauma, 70 cases (35%) presented after 24-48 hours of trauma, 13 (6.5%) cases presented after 48 hours but within 1week, 5(2.5%) cases reported after 1 week to 4 weeks and 2(1%) cases presented after 4 weeks of trauma. 39.5% (79) patients belonged to preschool and 60.5 % (121) belonged to school going groups. Among 200 patients 41.5% affected in right eye and 55% affected left eye. Only 3.5% of cases affected both eyes and all of which were injured by chemical products. All the demographic information is summarized in table 1.
Table 1: Demographic data of patients
| Age distribution | ||||
| Age category | n | Percentage | ||
| 0-4 years | 71 | 35.5% | ||
| 5 – 8 years | 63 | 31.5% | ||
| 9 – 12 years | 45 | 22.5% | ||
| 13 – 16 years | 21 | 10.5% | ||
| Laterality of injured eye | ||||
| Right eye | 110 | 55% | ||
| Left eye | 83 | 41.5% | ||
| Both eye | 7 | 3.5% | ||
| Type of injuries | ||||
| Open globe | 173 | 86.5% | ||
| Closed globe | 27 | 13.5% | ||
The maximum number of injuries occurred at home was 152(76.0%) and playground 27(13.5%). (figure1).
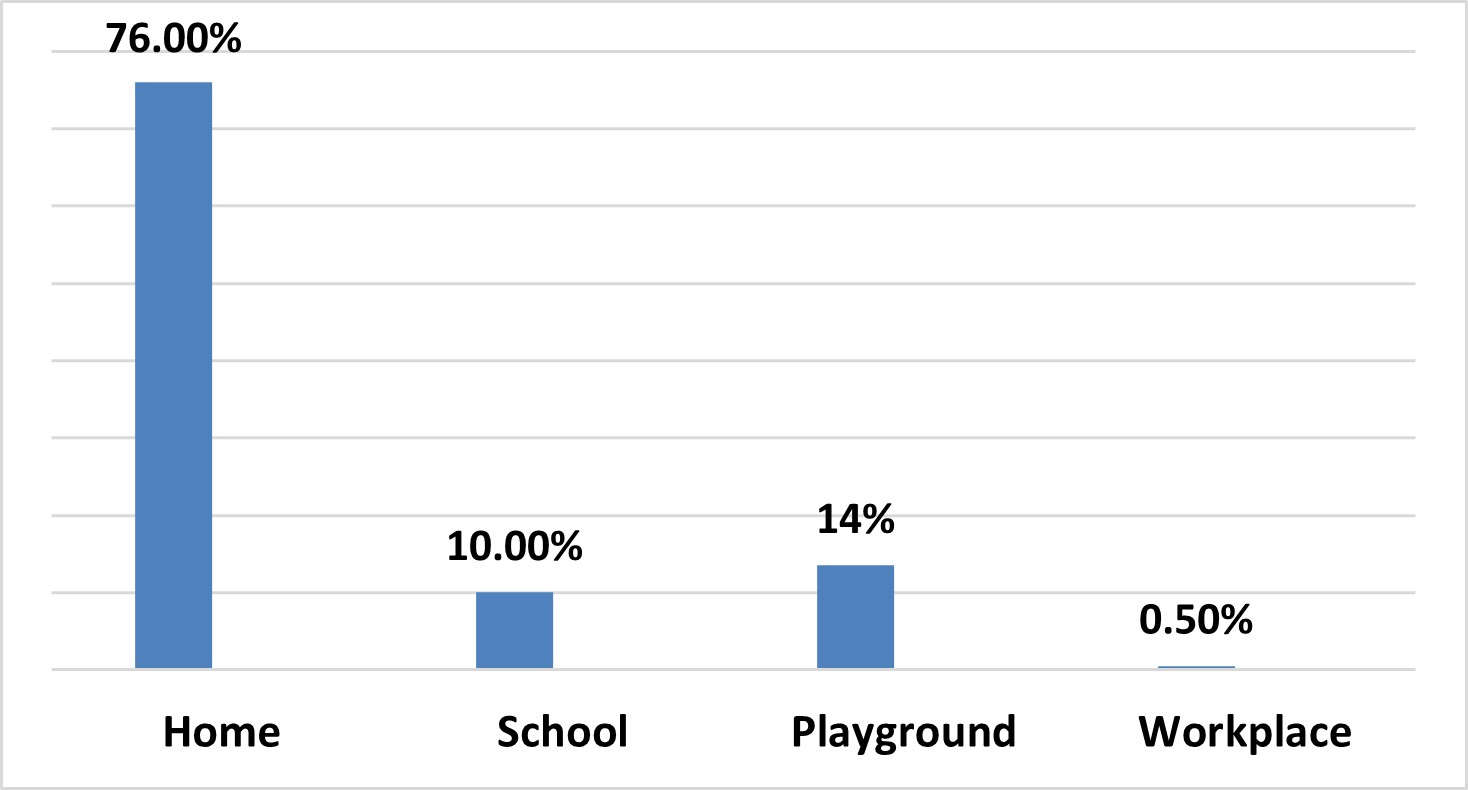
Figure 1: Percentage of places of injury
Injury with wooden stick was the most common 70(35.0%), second most common object was sharp object 38 (19%) such as glass piece, knife, scissors etc. Other common traumatic agents were flying stone 22(11%), tip of pencil or pen 18(9%), toy pistol 16(8%). 8 (4%) patients were injured by bird bites and 12(6%) patients by chemical injuries like lime burn, oil, super glue etc. The remaining 16 (8%) cases were injured by other means including RTA, fall from height, dog bite, fingernail injuries, key, iron rod, gas light burst etc.
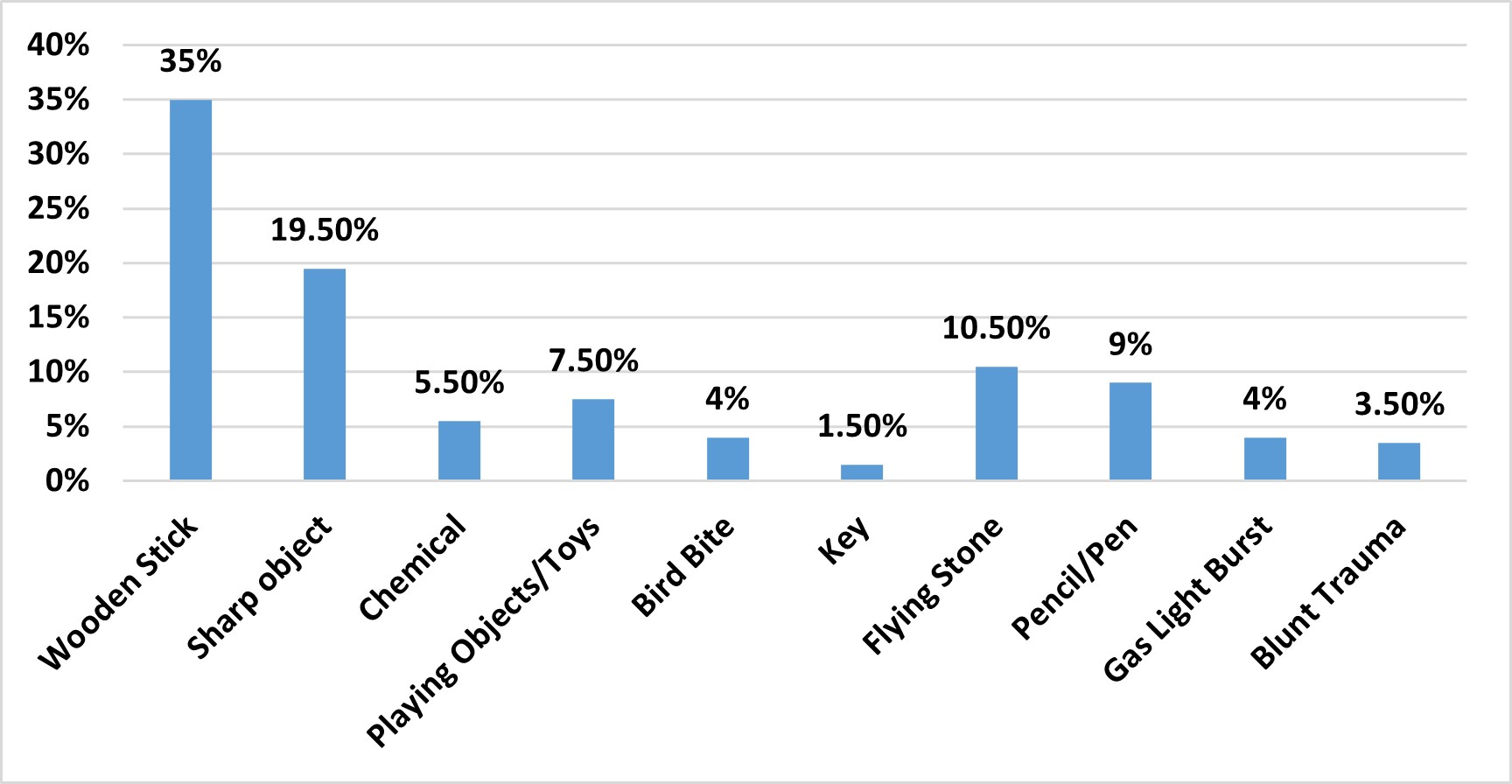
Figure 2: Types of objects causing ocular injury
Out of 200 cases, 149(74.5%) cases were of corneal injuries, 3(1.5%) cases of adnexal injuries (lid laceration), 10(5%) cases were of scleral tear and sclerocorneal involvement, and 72(36%) were traumatic cataract. 12(6%) were hyphaema at anterior chamber, 8(4%) cases were conjunctival laceration. 1(0.5%) case reported Endophthalmitis, 4(2%) cases of globe rupture. 6(3%) cases reported to vitreous and retinal involvement.
Table 3: Pattern of ocular injuries
| Anterior segment | Site of Injury | n | Percentage |
| Lid | 7 | 3.5% | |
| Conjunctiva | 8 | 4% | |
| Sclera | 10 | 5% | |
| Cornea | 149 | 74.5% | |
| Anterior chamber | 12 | 6% | |
| Lens | 72 | 36% | |
| Not affected | 6 | 3% | |
| Posterior segment | Vitreous | 5 | 2.5% |
| Retina | 2 | 1% | |
| Not affected | 121 | 60.5% | |
| Other | Uveitis | 3 | 1.5% |
| Endophthalmitis | 1 | 0.5% | |
| Globe rupture | 4 | 2% |
A total of 129(64.5%) patients underwent single surgery and 71(35.5%) patients needed multiple surgery. Among the 149(74.5%) patients of corneal injury, 83(41.5%) patients needed only corneal injury repair and 66 (33%) patients developed cataract that underwent IOL implantation with PPC & AVT later on. According to data 6(3%) patients with blunt trauma developed only cataract and underwent IOL implantation with PPC & AVT. 12(6%) cases treated with aspiration of hyphaema, 7(3.5%) patients required lid injury repair, and 5(2.5%) cases underwent repair of ruptured globe, 6(3%) cases needed with repair of conjunctival tear, 3(1.5%) cases required with foreign body removal and 7(3.5%) cases treated with EUA under general anaesthesia. Intra-vitra antibiotic injection (ceftazidime and vancomycin) were given under GA in 5 (2.5%) patients with corneal injury repair.
About 48.5% of the patients got normal visual acuity ranging from 6/6 to 6/18. In 12% cases, CSM were present. Out of 200 patient 28 % had visual acuity between less than 6/18 to counting figure one meter (CF 1 meter). 7 patients had Hand movement (HM), 7 patients had Perception of light positive (PL+ve) and 9 patients had No Perception of Light (NPL) vision after surgical treatment. According to the study 39.5% of patients were visually impaired and 4.5% of patients were phthisis.
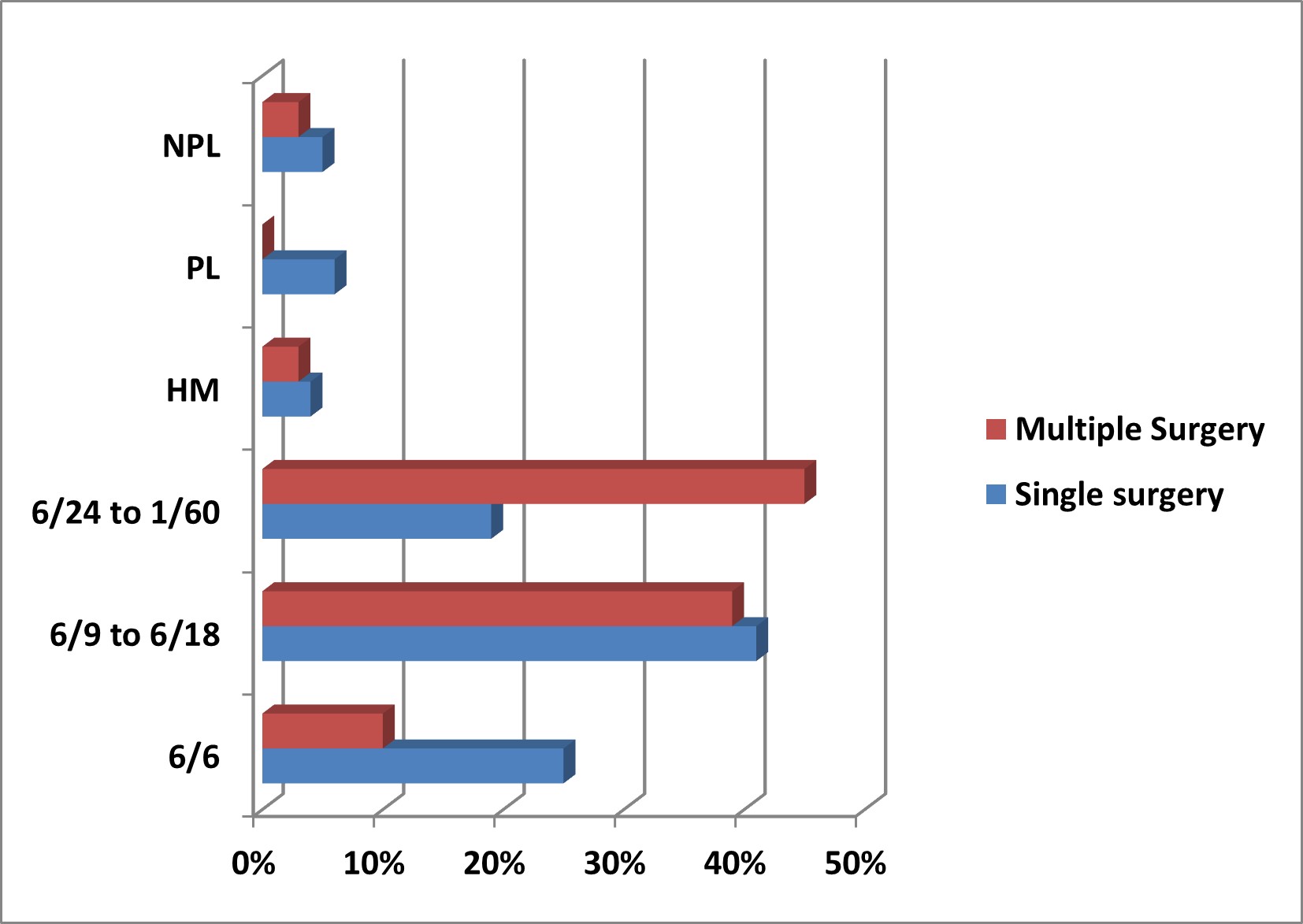
Figure 3: Final visual outcome
DISCUSSION
In this study, the children of the age group 5 to 12 years were more affected. It explains that children >10-year age are at higher risk for trauma, as they have more hours of outdoor activities and are not supervised by their parents. Also, the male was more affected than female children. An institutional study conducted at Helsinki’s University Eye Hospital; Finland 7 also showed that most likely age group presenting with ocular trauma was 13-16 years. In this study, 72.5% patients were male and 27.5% were female and male to female ratio was found 2:1. The explanation to this could be that greater risk-taking behavior and active participation in sports and recreational activities makes male patients more prone for ocular injuries. It is obvious that younger age groups are more vulnerable than older age groups. Younger people are more prone to irresponsible behavior and lack appreciation of potential hazards and areas of harm. This is in accordance with other published reports [8, 9, and 10].
In this study 55% patients reported to hospital within 24hours and 35% patients within 48 hours. In a previous study by, they concluded that early reporting could save vision more which can support our study 11. In this study, most of the injuries took place at indoors (76%) followed by playground (13.5%) , school (10%) and workplace (0.5%). According to the United States Eye Injury Registry (41%) and Hungarian Eye Injury Registry (35%) the most frequent place of injury was Home 12. Five years of retrospective study on epidemiological characteristics and visual outcomes of pediatric ocular injuries, the study showed that the leading place of eye injury was home (60.4%),followed by outdoors (31.7%), School (5.2%) and the sporting area (2.2%).13 In 2017, another study conducted Helsinki eye trauma study, and concluded that 33% of ocular injuries occurred at home and 24% at schools or in Day Care faculties.14 In this study, it was found that Maximum injuries were accidental (84.5%) and 15.5% during playing. In 2012, Krystin N.Miller et al, conducted a retrospective study of accidental and recreation related eye injuries in children < 17 years age. It showed 26.9 cases of accidental and recreation related eye injuries per 100,000 children 15.
Lack of adequate parental supervision might have been an additional factor, which might have contributed. The household environment is equally hazardous as the outdoor play areas and schools. More attention must be paid to ensure a child-friendly home environment or at least a hazard-free home setting for children, especially for the younger age group. Being more active and more exposed to outdoor activities and sometimes even involved in childhood labor especially in developing countries and rural communities, it is not surprising that more than 70% of the injured children were males as already highlighted [8,16,17,18]. A striking finding in this study, like other reports [9,16] is the predominance of left eye (55%) injuries over right eyes (41.5%).
Most pediatric ocular injuries occur at home and are due to trauma by sharp objects. [15] In this study the most common object of injury was wooden stick (35%). The second most common object was sharp objects (19%) such as knife, scissors etc, followed by flying stone or brick (11%), pen & pencil (9%), toy pistol (8%), chemical (6%), and bird bite 4%. The remaining 8% cases were injured by other means including blunt trauma, metal objects, key, fall from height, dog bite, fingernail injuries etc. Another Indian study reported that most common cause of the injury was wooden objects (29.54%). 11
Most of the patients had corneal injuries in this study 149 (74.5%). This relatively high prevalence of corneal injuries has been emphasized by other reports 8. On the other hand, the remainder of the outer wall of the eye, namely the sclera, is less exposed (being relatively protected in the bony orbit), and is mechanically more robust than the cornea, hence less vulnerable to injury. Related to the outer wall of the eye and the occurrence of open injuries are the anterior chamber depth (6%). The delicate structure of the iris and the pupils renders it vulnerable to injury with the majority of ocular injuries. The natural crystalline lens is another very delicate intraocular structure that is very vulnerable in children’s eyes, as obvious in 36% of the eyes presenting with an abnormality in the lens. The lids, being the first anatomical structure and the first line of defense to the eyes, are commonly injured. Prognosis of the surgery was good 60.5% of patients had good visual acuity and 39.5% of the patient was visually impaired. In this study only 4.5% of patients were phthisis.
CONCLUSION
The most common causes of decreased vision after management of injuries in children are corneal scar, astigmatism and amblyopia. Maintaining a safe home environment is crucial to prevent blindness and eye injuries. Stopping the marketing of dangerous toys and disposing of household products safely is essential. Protection of children from hazardous event like dog bites, cricket ball, toy pistols, assault, fireworks and crackers are crucial. Mass awareness should be created in home, school and society to prevent this unwanted occurrence.
REFERENCE
- Yaxin Zhang, Kang Feng, Epidemiological Characteristics of Pediatric Ocular Trauma in China: A Multicenter Retrospective Hospital-Based Study ;J Ophthalmol. 2022,July ; doi: 10.1155/2022/4847027
- Vishal Wagh, Pravin Tidake, Clinical Study and Profile of Ocular Trauma: Findings from a Rural Hospital in Central India; Cureus. 2022 Jul; 14
- S Vats, G V S Murthy, M Chandra. Epidemiological study of ocular trauma in an urban slum population in Delhi, India; Indian J Ophthalmol.2008 Jul-Aug; 56(4): 313–316. doi: 4103/0301-4738.41413
- Brophy M, Sinclair SA, Hostetler SG, Xiang H. Pediatric eye injury related hospitalizations in the United States. Pediatrics 2006 Jun; 117(6):e1263-71.doi: 10.1542/peds.2005-1950.
- Shazia Qayum, Rashid Anjum, Shagufta Rather. Epidemiological profile of pediatric ocular trauma in a tertiary hospital of northern India. Chinese Journal of Traumatology 2018 Apr;21(2):100-103.doi: 10.1016/j.cjtee.2017.11.005.
- Ashok Hukumchand Madan, Rajesh Subhash Joshi, Preeti Dasharath Wadekar. Ocular Trauma in Pediatric Age Group at a Tertiary Eye Care Center in Central Maharashtra, India. Clin Ophthalmol. 2020 Apr. doi: 2147/OPTH.S244679
- Anna-Kaisa Haavisto, Ahmad Sahraravand. Paediatric eye injuries in Finland – Helsinki eye trauma study. Acta Ophthalmologica, Acta Ophthalmol. 2017 Jun;95(4):392-399. doi: 10.1111/aos.13327.
- Al Wadeai EAY, Osman AA, Macky TA Epidemiological features of pediatric ocular trauma in Egypt. J Ophthalmology 2016; October ;5.
- Sii F, Barry RJ, Abbott J. The UK paediatric ocular trauma study 2 (POTS2): demographics and mechanisms of injuries. Clin Ophthalmol. 2018; Dec :105–111.
- Qayum S, Anjum R, Rather S. Epidemiological profile of pediatric ocular trauma in a tertiary hospital of northern India. Chin J Traumatol. 2018 Apr; 21 (2):100–103.
- Singh S, Sharma B, Kumar K, Dubey A, Ahirwar K . Epidemiology , clinical profile and factora, predicting final visual outcome of pediatric ocular trauma in a tertiary care center of Central India. Indian J Ophthalmol. 2017 Nov; 65(11):1192-1197.doi: 10.4103/ijo.IJO_375_17.
- Kuhn F,Mester V,Berta A. Epidemiology of severe eye injuries USEIR and HEIR. 1998 May;95(5):332-43.doi: 10.1007/s003470050282.
- Puodzuviene E, Giedre Jokubauskiene ,Vieversyte M. Asselineau K. BMC Ophthalmol,2018; Jan 18. Doi; 10.1186/s12886-018-0676-
- Haavisto A.K, Sahraavand A,Holopainen JM, Leivo T. Paediatric eye injuries in Finland- Helsinkis eye trauma study, Acta Ophthalmol. 2017 Jun;95(4):392-399.doi: 10.1111/aos.13327.
- Miller KN,Collins CL, Chounthirath T. Pediatric Sports and Recreationa-Related Eye injuries Treated in US Emeregeancy Departments. Pediatrics.2018;141(2) :e20173083. 2018 Feb; 141(2) doi: 10.1542/peds.2017-3083.
- Wagle N, Usgaonkar U, Naik P. Pediatric ocular morbidity profile in the inpatient department of a tertiary health care hospital in Goa. IOSR-JDMS. 2018;March;Vol 17(3):7–9.
- Wang W, Zhou Y, Zeng J. Epidemiology and clinical characteristics of patients hospitalized for ocular trauma in South-Central China. Acta Ophthalmol. 2017 Sep; Vol:95 (6
- Cao H, Li L, Zhang M. Epidemiology of pediatric ocular trauma in the Chaoshan region, China, 2001–2010. PLoS ONE. 2013 April Vol:8(4) doi.org/10.1371/journal.pone.0060844