
Exploring the Experience of Academic Stress, Eating Behavior, and Food Choice among Black University Students
- Priscilla Oludara Jekayinfa
- Elisha Oluwatobi Olabisi
- 651-679
- May 16, 2024
- Social Welfare
Exploring the Experience of Academic Stress, Eating Behavior, and Food Choice among Black University Students
Priscilla Oludara Jekayinfa & Elisha Oluwatobi Olabisi
Ladoke Akintola University of Technology
DOI: https://doi.org/10.51244/IJRSI.2024.1104048
Received: 30 March 2024; Accepted: 12 April 2024; Published: 16 May 2024
ABSTRACT
Introduction: Academic stress is a common problem faced by university students in the UK, and it tends to affect dietary practices. The study explored the experience of academic stress, eating behaviour and food choice among black university students.
Methods: Descriptive cross-sectional design was adopted. A convenience sampling technique was utilised. Validated outcome measures were used for data collection. Data were analysed using descriptive statistics, Spearman correlation, and Wilcoxon signed rank test. Association between variables were considered significant at p< 0.050. IBM SPSS version 25 was used for data analysis.
Result: The response rate was meagre (n=42). The mean perceived stress scale score was 20.49±6.71, depicting moderate academic stress. The mean food group diversity score (FGDS) was 9.32±1.16 in Nigeria and lesser (6.38±2.090) in the UK. Rate of Food group adequacy (FGA) was 36(97.3%) in Nigeria as compared to the UK 19(51.4%). Consumption of non-communicable diseases (NCDs) – protective food groups (NCD protective) was higher (7.78±1.65) in Nigeria compared to the UK (4.35±2.41). However, consumption of food that predisposes to NCDs (NCD risk) was higher (7.73±1.84) in Nigeria, compared to the UK (5.16±3.59). Participants’ compliance with global dietary recommendations (GDR) was higher (9.054±2.449) in Nigeria compared to the UK (8.189±3.487). The differences between dietary indicators (FGDS, FGA, GDR, and NCD protective, NCD risk) scores in Nigeria and the UK were statistically significant as (p<0.01) in each case. Lastly, the academic stress level had a moderate negative significant correlation with their eating behaviour and food choices as measured by their GDR score (r=-.371, p=0.024).
Conclusion: Stress level was moderate, which negatively affected their dietary quality suggesting the need to implement supportive measures and educational programmes that can contribute to better stress management and improved nutritional practices. Further studies should ensure usage of a large and more diverse sample to aid usability and generalizability of findings.
Keywords: Academic stress, Black, Eating behavior, Experience, Food choice
INTRODUCTION
Background
Stress encompasses the demands put on a person’s physical and mental well-being by the environment, either physically or psychologically (Lin et al., 2020). Stress is a universal bodily reaction and capacity to maintain homeostasis. Due to its detrimental effects on human health, it is a worldwide issue (Soe et al., 2018). Stress is often unavoidable. When expectations are unreasonable or difficult to meet, a person may feel under pressure. A certain amount of stress might be energising and advantageous for leading a fruitful existence. On the other hand, persistently high amounts of stress can result in severe physical issues (Alsulami et al., 2018). College students experience academic and non-academic related stress, which can take many forms and be influenced by social, environmental, and psychological factors (Bedewy & Gabriel, 2015). An individual’s reaction to academic obligations is known as academic-related stress. It entails emotional anguish caused by the expected fear of scholastic failure. This can show up in several ways, such as overwhelming sentiments while adjusting to college life, academic obligations or commitments and an apparent barrier to reaching a goal (Anaman-Torgbor et al., 2021). Additionally, university undergraduate and graduate students must deal with additional school-related pressures such as a highly demanding course, extensive studying time, effective time optimisation, competition among fellow course mates in the classroom, financial obligations, domestic duties, and acclimating to a new lifestyle (Barbayannis et al., 2022).
The current cohort of students is significantly more worried and apprehensive than earlier generations since society has a general opinion that these students are more capable, particularly in terms of technological competency; yet, being esteemed to be more enlightened has placed huge expectations on their outcomes, and they are being pushed to meet ridiculous standards (Ramli et al., 2018). University life necessitates much individual effort, devotion, and commitment. It may also include living away from family, which causes social isolation and increases personal vulnerability. Students may be unprepared for this adjustment and feel academic stress (Rasheed et al., 2017). Most college students deal with academic stress, as revealed by Caso et al. (2020). Three out of every four undergraduate or graduate students in the United States of America reported feeling stressed, according to Barbayannis et al. (2022). A survey of university students in Australia found that 53% of them suffered from psychological distress (Asif et al., 2020). Academic accomplishment boosts students’ chances of getting a job in the labour market, consequently predicting their social and professional exploits (Santana et al., 2017). Furthermore, academic success is significant because of the family’s expectations and the desire to exceed one’s classmates. While stress generates excitement that might be called an academic incentive to a point, chronic stress may result in poor performance and cause health complications (Lin et al., 2020). Stress can result in the onset of psychological conditions, drug misuse, tension, sadness, low learner’s self-esteem, and suicidal ideation (Atta & Almilaibary, 2022). Experience of stress in its severe form can be detrimental to a student’s ability to concentrate and even function mentally. (Awadalla et al., 2022). Academic stress may lower enthusiasm, impair educational attainment, and raise university exit rates (Pascoe et al., 2020).
Furthermore, evidence suggests that stress alters food consumption, preference, and motivation (appetite and urge to eat) by activating affective brain connections and increasing glucocorticoid and insulin release. Affective cerebral connections and hormones impact several dietary behaviour elements (Debeuf et al., 2018). Accordingly, based on the root cause of the stress as well as its degree, stress may lead to inadequate or overeating (Debeuf et al., 2018). Individual variances exist as regards food intake; around 40% raise and reduce their calorie consumption when stressed, respectively, whereas nearly 20% do not modify feeding behaviour in stressful situations (Yau & Potenza, 2013). Hill et al. (2018) systematically reviewed primary literature on stress-related concepts. They found that stress was associated with eating less nutritious foods and detrimental consequences among persons aged 8 to 18. Furthermore, evidence suggests that college students are more likely to eat unhealthy foods and develop negative healthy behaviours throughout their time in school owing to academic stress, such as snacking and sweet foods consumption, junk food consumption, fast food consumption, and reduced vegetable and fruit intake (Almogbel et al., 2019; Caso et al., 2020). Failing to acclimate to an unfamiliar setting might also lead to unfavourable eating patterns, such as heavy alcohol usage (Choi, 2020).
Moreover, the majority of the developing world or low- and middle-income countries dominated by blacks are experiencing accelerated emigration due to several reasons, which include economic growth and efficiency of various sectors in the Countries, such as the health sector and educational sectors, among others (International Organization for Migration, 2023). Keeping the emigration factors in view alongside academic stress might make adjusting to a new dietary pattern regarding quality and diversity difficult, consequently impairing food choice and behaviour (Lee et al., 2022). Food adjustment in occidental countries may involve greater consumption of highly processed food items rich in saturated fats, sugars, and salt (Lee et al., 2022). Furthermore, evidence suggests that the rapid transition from conventional food regions to contemporary and industrialised diets that occurs as a result of migration to high-income countries predisposes one to experience adverse risks such as obesity, diabetes and cardiovascular diseases, among others (Berggreen-Clausen et al., 2022). According to research conducted in the USA, Blacks living in America have been reported to be eating poorly and not adhering to nutritional guidelines frequently (Brown et al., 2019).
However, eating behaviour is an essential component of daily life since it may impact long-term clinical outcomes as destructive dietary patterns like eating nutritionally deficient food, fasting, and not having to eat when necessary are known to result in a variety of medical conditions and dietary deficiencies (Kabir et al., 2018). Moreover, dietary practices in a population may be a predictor of overall health as well as the extent of their chances of developing lifestyle pathologies such as obesity, overweight, diabetes mellitus, hyperlipidaemia, substance abuse, lung diseases, high blood pressure, and cardiovascular disease, which are the leading causes of mortality across all nations (Al-Qahtani, 2016). Additionally, college is a crucial moment for increased weight since high school students who gain admission into college need to adjust to a new environment, making the prevention of overweight and obesity and its connected disorders a global concern (Deliens et al., 2014). Despite the available evidence on stress, eating habits and food choices among undergraduates, there is a dearth of research evidence in this resource setting. Moreover, there is a dearth of recent evidence as regards academic stress prevalence, eating habits and food choices among undergraduates generally and among a sample of the black population.
Findings of this study are of great benefit as they will influence policies and measures towards reducing academic stress and poor dietary habits and food choices. Hence, the need for conceptualising this study to explore the experience of academic stress, eating behaviour, and food choice among a sample of black university students in UK.
Thus, the research addressed the following research questions;
- What is the degree of academic stress among black university students?
- What are black university students’ eating habits and dietary preferences?
- Is there a significant difference between eating behaviour and food choice among black university students in Nigeria and the UK?
- Is there a significant relationship between the experience of academic stress and eating behaviour and food choice among black university students?
Operational Definition of Terms
Academic Stress refers to the demands that are put on black university students of South-Western Dosset, UK’s physical and mental well-being fromacademics, either physically or psychologically. The perceived stress scale measures it.
Black University Students: These are Nigerians who migrated to the United Kingdom and are presently undergoing formal educational training in tertiary institutions in South-Western Dosset, UK.
Eating Behaviour and Food Choice: These words are used jointly, and both depict the dietary habits and quality of black university students, respectively; it is measured by the Diet Quality Questionnaire developed by the Global Diet Quality Project
METHODS
Research Design
A quantitative cross-sectional study design was adopted to investigate the experience of academic stress, eating behaviour, and food choice among black university students in South-Western Dorset from April to June 2023.
Quantitative approaches generate numerical data from large, randomly selected populations, ensuring the generalizability of the study findings (Wright et al., 2016). Furthermore, the quantitative approach allowed mathematical examination of the relationship between academic-related stress and eating habits (Setia, 2016; Kosche et al., 2021). The cross-sectional design has the advantage of carrying out research over a short period as opposed to longitudinal studies (Kosche et al., 2021). Typically, they are affordable and straightforward to carry out. They prove valuable in establishing initial indications when preparing for a forthcoming, more robust investigation (Wang & Cheng, 2020).
Research Setting
The research was conducted at four universities and colleges in the United Kingdom’s southwestern region. These universities are Bournemouth University, Bournemouth and Poole College, Weymouth College, Arts University Bournemouth, and AECC University College (Complete University Guide, 2023). The United Kingdom is positioned off the northwestern coast of mainland Europe and consists of various regions, including England, Wales, Scotland, and the northern part of Ireland. As of 2023, the estimated population is 67,879,000 (Gilbert et al., 2023).
Target Population
The study population are Black university students in South-western Dorset, UK. The blacks originate in an African region with entirely different cultures and food choices. Hence, they are at risk of poor dietary habits because they have to adjust to a new feeding pattern and choices now that they have become part of the African diaspora. Moreover, it has been hypothesised that stress can alter their nutritional habits and quality, which have been established among studies in other populations, although not among blacks. Therefore, there is a need for such evidence among the Black population, who have now become a minority ethnic group in the UK. The Nigerian population was selected as a sample of the black population. This is because they are more easily accessible.
Inclusion and Exclusion Criteria
Defining criteria for including and excluding survey respondents is necessary for conducting high-quality scientific studies (Patino & Ferreira, 2018). The inclusion criteria establish the characteristics that qualify a person to participate in the research by reliably, consistently, and unbiasedly selecting the research population. The exclusion criteria specify the characteristics that exclude the selected group from participating in the research (Garg, 2016).
Inclusion Criteria: All blacks by race, age 19-64 years, who migrated into the United Kingdom from Nigeria who are attending Bournemouth University, Bournemouth and Poole College, Weymouth College, Arts University Bournemouth and AECC University College were included in the study. The age range was chosen as defined by Erik Erikson as being the young and middle-aged adulthood period (Mcleod, 2023). This ensures similarities among the study population to eliminate possible confounders from vast demographic differences. Furthermore, the younger age groups were excluded, considering the difficulties of gaining informed consent from their parents to participate in the study.
Exclusion Criteria: All who were ill, unavailable throughout the data collection period, and unwilling to participate in the study.
Instruments for Data Collection
A validated open- and closed-ended structured questionnaire was used, which is divided into three parts for adequate analysis. The first part focused on the sociodemographic characteristics.
The second and third parts focus on eating behaviour and food choice. This was measured by the Diet Quality Questionnaire (DQQ) developed by the Global Diet Quality Project (2021). The DQQ stands as a widely recognised tool for assessing dietary patterns on a societal scale. Its primary purpose is to collect data regarding the consumption of various food groups, which is crucial for calculating measures of nutritional quality across worldwide communities (Uyar et al., 2023).The questionnaire typically includes 29 questions about food groups and adherence to specific dietary guidelines or recommendations. It covered areas such as consuming fruits and vegetables, whole grains, lean proteins, unhealthy fats, sugary beverages, and processed foods.
The fourth part is the perceived stress scale (PSS), which has been used in other studies and focused on the experience of academic stress (Lin et al., 2020; Choi, 2020). The 10 question items are on Likert scales, which graduated from 0-4 for positive statements and reversed and coded for negative statements.
Scoring: PSS scores were obtained by reversing responses (e.g., 0 = 4, 1 = 3, 2 = 2, 3 = 1 & 4 = 0) to the four positively stated items (items 4, 5, 7, & 8) and then summing across all scale items. A short 4-item scale could be made from questions 2, 4, 5 and 10 of the PSS 10-item scale (Cohen et al., 1983).
Diet quality indicators used in this study are the Food Group Diversity Score (FGDS) and the Global Dietary Recommendation (GDR) score, which were obtained from the DQQ. These scores measure alignment with WHO global recommendations for healthy diets (WHO, 2020).
The Minimum Dietary Diversity for Women (MDD-W) consists of ten categories of food: 1) grains, white roots and tubers, and plantains; 2) pulses (beans, peas, and lentils); 3) nuts and seeds; 4) milk and milk products; 5) meat, poultry, and fish; 6) eggs; 7) dark green leafy vegetables; 8) other fruits and vegetables that are rich in vitamin A; 9) other vegetables; and 10) other fruits (Uyar et al., 2023). The Food Group Diversity Score (FGDS) is a continuous score ranging from 0 to 10, representing the ten food groups in the MDD-W, and applies to the entire population. A higher score indicates a greater probability of meeting nutritional adequacy (Uyar et al., 2023).
The non-communicable diseases (NCDs) – protective food groups (NCD protective), NCD risk food groups, and the overall GDR score were derived from the data on dietary consumption: (1) NCD protective score, which represents five global suggestions for health-promoting foods in a balanced diet (such as fruits and vegetables, legumes, nuts and seeds, whole grains, and dietary fibre); (2) NCD risk score, which reflects six global recommendations concerning dietary components that should be restricted (including total fat, saturated fat, dietary sodium, free sugars, processed meat, and unprocessed red meat); (3) overall GDR score, obtained by subtracting the NCD risk score from the NCD protective score encompassed all eleven recommendations in total (Wang et al., 2022).
Specifically, the overall GDR score is determined by subtracting the NCD risk score from the NCD protective score and then adding 9 to adjust the range of scores from 0 to 18. A higher score indicates a greater likelihood of meeting more recommendations, reflecting a more health-protective dietary pattern (i.e., higher scores correspond to increased adherence to health-promoting dietary guidelines).
The GDR score is presented as an average score within the population. Increased scores indicate diets of higher quality. Similarly, the GDR sub-metrics (GDR-Healthy and GDR-Limit) are average scores. The GDR score can also be represented as a binary indicator, indicating the percentage of the population that meets at least half of the global dietary guidelines. On the other hand, the FGDS is expressed as an average score within the population, where higher scores indicate better dietary quality. The FGDS can be presented as the percentage of the population that consumes a minimum of five out of the ten specified food groups.
It is important to note that no established threshold exists to define an absolute interpretation of “good” or “poor” diets about the GDR score, its subcomponents, or the overall DQ-Q score. There can be relative classifications into high, medium, and low scores depending on the tertile (Agriculture, Nutrition & Health Academy 2021).
Table 1: FGDS

(source: Agriculture, Nutrition & Health Academy 2021)
Table 2: Food Group Adequacy

(source: Global Diet Quality Project, 2021).
Table 3: GDR Healthy Component

(source: Agriculture, Nutrition & Health Academy 2021).
Table 4: GDR Limit Component

(source: Agriculture, Nutrition & Health Academy 2021).
Validity and Reliability
Validity describes how well an instrument assesses what it is intended to assess as required by the research questions and objectives (Ahmed & Ishtiaq, 2021). Although, there are “face”, “content”, “construct”, and “criterion” validity. However, face and content validity were ascertained as a matter of necessity. Face and content validity was done by the study supervisor and other experts in nutrition studies to ensure the instrument comprehensively measures the experience of academic stress, eating behaviour, and food choice in black university students. The capacity of a study tool to produce consistent findings across repeated assessments is implied by reliability, which is the measure of the tool’s internal consistency (Ahmed & Ishtiaq, 2021).
The instruments used are validated and standardised tools. The PSS-10 exhibited satisfactory internal coherence and reliability across multiple studies (Mozumder, 2022). The documented internal coherence of the questionnaire, as measured by Cronbach’s alpha, ranged from .71 to .91, while the test-retest reliability coefficient has consistently shown values above .70 in diverse populations (Mitchell et al., 2008; Chaaya et al., 2010; Lee, 2012). The dietary diversity measurement subscale reliability coefficient was 0.76 (Hussien et al., 2021). DQQ have used and validated several credible studies (WHO, 2021; Miller et al., 2022; Uyar et al., 2023). Reliability coefficients yielding a score above 0.75 depict high reliability and internal consistency (Koo & Li, 2016).
Sampling Technique
The study settings comprised five tertiary institutions. However, estimating the total black population considering the study time frame is not feasible, preventing the use of stratified or multistage random sampling techniques due to the accessibility of the students and the method of data collection. A convenience sampling method was utilised for the study. The convenience sampling technique is a non-probabilistic sampling approach based on the principle of accessibility and convenience. However, the drawback to this is the risk of bias because all the students do not have equal chances of being selected to participate in the study (Elfil & Negida, 2017). Thus, the instrument was administered to accessible students based on the inclusion and exclusion criteria.
Sample Size Determination
Calculating the sample size involves making a statistical estimate of all the people who should take part in the study. A sample size that is too large or too small is associated with inaccuracy in study findings (Kaur, 2017). Leslie Kish’s formula was utilised by Fishers (Kish, 1995).
n=z2 pq÷d2
Where;
n- desired sample size
q- The percentage not involved in the study
p- Percentage of the target population thought to possess a certain trait (prevalence of academic-related stress =46.4%) (Chukwuocha et al., 2021)
z- The critical value for a two-tail test at a 95% confidence level.
d- The absolute precision required on either side of a normal distribution curve at a confidence level of 95%; the degree of precision desired is usually set at 5%.
n= (1.96)2 x 0.464x (1-0.464)
(0.05)2
n=382
Considering a 10% attrition rate for the sake of non-response or poorly filled questionnaires
n= 420 participants
Method of Data Collection
Validated instruments structured in English into an online form using the Bournemouth University Online Survey Development Package were administered to the study participants. The questionnaire interface became accessible after indicating their consent to participate in the study. Additionally, three research assistants were recruited and underwent a three-day training program, lasting one hour per session, which covered research ethics and the data collection process. The participants were accessed through their social media platforms; thus, they received the survey link through their media platforms. Completing the study instrument took approximately 20 minutes. The entire data collection process spanned over one month.
Statistical Analysis
The quantitative data was assessed for completeness and underwent a cleaning process. The collected data was exported to IBM SPSS, version 25. Descriptive and inferential statistical methods were employed for analysis. Categorical variables were analysed using frequencies and percentages, while continuous data was described using mean and standard deviation (Guetterman, 2019).
To assess differences in diet quality between the retrospective data from Nigeria and the present diet quality, the Wilcoxon signed-rank test was used, and the Spearman rank correlation was used to assess relationship between academic-related stress and dietary habits due to non-normalcy of data determined after conducting the Kolmogorov Smirnov test and Shapiro Wilk test (Sundjaja et al., 2022). Statistical significance between variables was established at P<.050 (Tenny & Abdelgawad, 2022). The analysis results were presented in tables and charts to provide an overview of the findings.
Ethical Consideration
A letter of introduction addressed to the Ethical Review Committee” of Bournemouth University was obtained from the Faculty of Health and Social Sciences and submitted alongside the research proposal to the committee. The ethical approval was given on 7th April 2023 with Ref.no: 47961.
The study was conducted in accordance with the “Declaration of Helsinki” (World Medical Association, 2018). The study participants were required to provide written informed consent, including a clear explanation of the study objectives, benefits, absence of harm, the right to decide whether to participate (autonomy) and the right to anonymity and confidentiality of the information provided. The file was encrypted and stored in an SPSS format to prevent unauthorised access.
RESULTS
A total of 42 responses were retrieved, out of which 37 completed the study instrument and had adequate data for analysis. This translates to a response rate of 88.1%.
Table 5: Sociodemographic Characteristics
| Variables | Categories | n (%) |
| Gender | Female | 23(62.2) |
| Male | 14(37.8) | |
| Academic level | Postgraduate | 35(94.6) |
| Undergraduate | 2(5.4) | |
| Having undertaken a nutrition-related course | Yes | 9(24.3) |
| No | 28(75.7) |
Table 6: Degree of Academic Stress among Black University Students
| Variables | Responses (n=37) | Mean±SD | ||||
| Never f(%) | Almost never f(%) | Sometimes f(%) | Fairly often f(%) | Very often f(%) | ||
| Being upset because of something that happened unexpectedly | 2(5.4) | 3(8.1) | 19(51.4) | 7(18.9) | 6(16.2) | 2.32±1.03 |
| Feeling of nervousness and stress | 1(2.7) | 4(10.8) | 10(27) | 9(24.3) | 13(35.1) | 2.78±1.13 |
| Feeling of confidence about one’s ability to handle personal problems | 0(0) | 5(13.5) | 16(43.2) | 6(16.2) | 10(27) | 1.43±1.04 |
| Feeling of things going their way | 0(0) | 7(18.9) | 14(37.8) | 8(21.6) | 8(21.6) | 1.54±1.04 |
| Inability to control the important things in their lives | 2(5.4) | 6(16.2) | 13(35.1) | 7(18.9) | 9(24.3) | 2.41±1.19 |
| Not being able to cope with all the things that they had to do | 2(5.4) | 9(24.3) | 17(45.9) | 6(16.2) | 3(8.1) | 1.97±0.99 |
| Ability to control irritations in their life | 1(2.7) | 3(8.1) | 18(48.6) | 4(10.8) | 11(29.7) | 1.43±1.09 |
| Feeling of being on top of things | 1(2.7) | 6(16.2) | 19(51.4) | 6(16.2) | 5(13.5) | 1.78±0.98 |
| Being angered because of things that were outside of control | 2(5.4) | 2(5.4) | 14(37.8) | 10(27) | 9(24.3) | 2.59±1.09 |
| Difficulties were piling up so high that they could not overcome them | 3(8.1) | 6(16.2) | 14(37.8) | 8(21.6) | 6(16.2) | 2.22±1.16 |
| Overall Mean PSS score | 20.49±6.71 | |||||
Table 7: Food Group Diversity Score (FGDS) in Nigeria vs UK
| Food groups consumed | Responses (n=37) | |
| Nigeria f(%) | United Kingdom f(%) | |
| Grains, white roots and tubers, and plantains | 37(100) | 37(100) |
| Pulses (beans, peas and lentils) | 34(91.9) | 15(40.5) |
| Nuts and seeds | 32(86.5) | 17(45.9) |
| Diary | 35(94.6) | 27(73) |
| Meat, poultry and fish | 36(97.3) | 34(91.9) |
| Eggs | 30(81.1) | 11(29.7) |
| Dark green leafy vegetables | 33(89.2) | 14(37.8) |
| Other vitamin A-rich fruits and vegetables | 37(100) | 23(62.2) |
| Other vegetables | 34(91.9) | 29(78.4) |
| Other fruits | 37(100) | 29(78.4) |
| Overall mean food group diversity score | 9.32±1.16 | 6.38±2.09 |
Table 8: Food group adequacy in Nigeria vs UK
| Food groups | Responses (n=37) | |
| Nigeria f(%) | United Kingdom f(%) | |
| Starchy staples | 37(100) | 37(100) |
| Vegetables | 37(100) | 34(91.9) |
| Fruits | 37(100) | 30(81.1) |
| Pulses, nuts and seeds | 36(97.3) | 21(56.8) |
| Animal-source foods | 37(100) | 37(100) |
| Mean FGA score | 4.97±0.16 | 4.30±0.85 |
Table 9: NCD-Protect score
| NCD Protect Food Groups | Responses (n=37) | |
| Nigeria f(%) | United Kingdom f(%) | |
| Whole grain | 25(67.6) | 7(18.9) |
| Pulses | 34(91.9) | 15(40.5) |
| Vitamin A-rich orange vegetables | 27(73) | 23(62.2) |
| Other vegetables | 34(91.9) | 29(78.4) |
| Vitamin A-rich fruits | 36(97.3) | 7(18.9) |
| Citrus | 34(91.9) | 24(64.9) |
| Nuts and Seeds | 32(86.5) | 17(45.9) |
| Dark green leafy vegetables | 33(89.2) | 14(37.8) |
| Other fruits | 33(89.2) | 25(67.6) |
| NCD Protect overall mean score | 7.78±1.65 | 4.35±2.41 |
Table 10: NCD-Risk score
| NCD Risk Food Groups | Responses (n=37) | |
| Nigeria f(%) | United Kingdom f(%) | |
| Soft drinks | 33(89.2) | 20(54.1) |
| Baked / grain-based sweets | 35(94.6) | 26(70.3) |
| Other sweets | 30(81.1) | 24(64.9) |
| Processed meat | 25(67.6) | 17(45.9) |
| Packaged ultra-processed salty snacks | 31(83.8) | 22(59.5) |
| Deep fried food | 35(94.6) | 22(59.5) |
| Unprocessed red meat | 36(97.3) | 20(54.1) |
| Fast food and instant noodles | 36(97.3) | 23(62.2) |
| NCD Risk overall mean score | 7.73±1.84 | 5.16±3.59 |
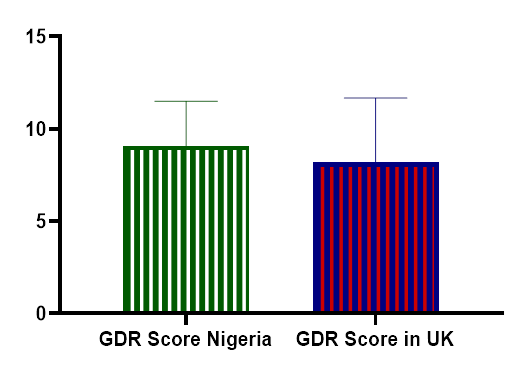
Fig 1: Global Dietary Recommendations (GDR) score
Table 11: Differences between eating behaviour and food choice among black university students in Nigeria and in the UK
| Dietary quality parameters | Wilcoxon Signed Ranks Test statistic (Z) | p |
| FGDS (UK) – FGDS (Nigeria) | -4.878 | 0.000* |
| FGA (UK) – FGA (Nigeria) | -3.866 | 0.000* |
| GDR (UK) – GDR (Nigeria) | -1.530 | 0.126 |
| NCD Protect (UK) – NCD Protect (Nigeria) | -4.810 | 0.000* |
| NCD Risk (UK) – NCD Risk (Nigeria) | -3.832 | 0.000* |
*- significant at p<.050, p-Probability value
Table 12: Relationship between the experience of academic stress, eating behaviour, and food choice in black university students
| Variables | FGDS | FGA | NCD Protect | NCD Risk | GDR | |
| Academic stress (PSS) | ρ | -0.278 | -0.290 | -0.292 | 0.151 | -.371 |
| p | 0.095 | 0.082 | 0.080 | 0.373 | 0.024* | |
ρ- spearman correlation coefficient,*- significant at p<.050, p-Probability value
Table 5 revealed about two-third 23(62.2%) were females, majority 28(75.7%) have undertaken nutrition related course while overwhelming majority 35(94.6%) were post-graduate students.
Table 6 showed that, out of 40, the average academic stress score was 20.49±6.71, depicting an overall moderate stress level. Feeling nervous and being angered because of things outside of control were fairly often experienced. The feeling of things not going their way, being upset because of something that happened unexpectedly, unable to control the essential things in their lives, not being able to cope with all the things that they have to do, not feeling of being on top of things and difficulties piling up were sometimes experienced.
Table 7 showed that, out of a total score of 10, the mean food group diversity score was 9.32±1.16 in Nigeria, while it was 6.38±2.09 in the UK. Most prevalent individual food groups consumed both in Nigeria and UK includes grains, white roots and tubers, and plantains, meat, poultry and fish, diary, fruits and vegetables.
Table 8 showed overall FGA score of 4.97±0.16 in Nigeria and 4.30±0.85 in UK out of a total score of 5. Food groups commonly eaten includes starchy staples, vegetables, fruits, pulses, nuts and seeds, and animal-source foods.
Table 9 showed NCD- protect overall mean score was 7.78±1.65 in Nigeria and 4.35±2.41 in UK out of a score of 9. The NCD-protective food groups include whole grain, pulses, vitamin A-rich orange vegetables, vegetables, vitamin A-rich fruits, citrus, nuts and seeds and dark green leafy vegetables.
Table 10 showed NCD-risk overall mean score was 7.73±1.84 in Nigeria and 5.16±3.59 in UK out of a score of 9. The NCD-risk food groups include soft drinks, sweets, processed meat, packaged ultra-processed salty snacks, deep fried food, unprocessed red meat and fast food & instant noodles.
Fig 1 showed the GDR score to be 9.054±2.449 in Nigeria and 8.189±3.487 in UK out of a score of 18.
Table 11 showed a significant increase in the quality of eating behaviour and food choices in Nigeria compared to the UK, thereby rejecting the null hypothesis. FGDS, FGA, and NCD protective and NCD-risk dietary scores were significantly higher in Nigeria as compared to the UK with (Z=-4.878, p=0.01), (Z=-3.866, p<0.01) and (Z=-4.810, p=0.01) respectively at p< .050. However, the NCD-risk dietary score was significantly higher in Nigeria compared to the UK with (Z=-3.832, p<0.01) at p< .050.
Table 12 showed a moderate negative significant correlation between academic stress and GDR score with (r=-.371, p=0.024) at p< .050. However, a negative correlation was found between the overall academic stress level and the FGDS, FGA, and NCD Protect, while a positive correlation exists between the stress level and the NCD risk score. However, the correlations were not statistically significant, as p> .050 in each case.
DISCUSSION OF FINDINGS, CONCLUSION, RECOMMENDATIONS
Discussion of Findings
Stress can affect dietary practices in a population, which can predict overall health and the extent of their chances of developing lifestyle pathologies (Debeuf et al., 2018; Hill et al., 2018). This study explored the experience of academic stress, eating behaviour, and food choice in black university students, a larger proportion of whom were females, postgraduate students, and those who had undertaken nutrition-related courses.
Regarding the students’ eating behaviour and food choices, findings revealed that the majority had better dietary practices in Nigeria than in the UK. This was evident by various dietary quality-based indicators such as the food group diversity scores, food group adequacy, NCD-protective dietary score, NCD risk dietary score and global dietary recommendation score (Uyar et al., 2023; Global Diet Quality Project, 2023). Dietary Diversity refers to the number of food groups or foods consumed in a given period. They are a good source of macro and micronutrients and best ensure nutrient adequacy necessary to promote a healthy weight and reduce the risk for nutritional deficiencies and chronic diseases (Xu et al., 2022; Weerasekara et al., 2020). While the Black students were in Nigeria, the average food group diversity score was approximately 9 out of a score of 10 compared to the UK with 6 out of 10. The difference in the FGD in Nigeria and the UK was statistically significantly different. However, the recommended food diversity score is a minimum of five food groups, which the students in both countries met. Food groups still commonly consumed in both regions include grains, white roots and tubers, plantains, meat, poultry and fish, dairy, fruits and vegetables. However, it is arguable that diversities do not necessarily translate to healthy diets all the time. This is why the association between food diversities and NCDs is not constant; it is also affected by the type of food groups that are being consumed (Dolui et al., 2023). However, an ample body of evidence supports the fact that continuous consumption of a singular food group causes deficiency in crucial micronutrients and adds to the prevalence of micronutrient deficiencies (Abebe et al., 2023; Zeinalabedini et al., 2023).
This finding is inconsistent with a study by Omage and Omuemu (2018) among undergraduates in Southern Nigeria, who found that approximately half of the respondents had a high dietary diversity. However, the finding is somewhat close to the present-day reality in the UK, with the mean food group diversity score slightly above average. In contrast, a study among university students in South-western Nigeria by Sedodo et al. (2014) revealed the students had low dietary diversity scores. This difference might be because approximately all the participants in this present study are postgraduate students who, as in their last days in Nigeria, had completed their undergraduate studies and probably would have secured a job and earned a better living. To corroborate this opinion, Nzeagwu and Akagu (2011) revealed that economic factors have been the most significant determinant of food habits among a sample of Nigerian undergraduates. However, there is dearth of studies with focus only on postgraduate students or a mixture of undergraduates and postgraduates. Moreover, the studies were conducted in just a region of Nigeria, which is not representative of the whole nation.
Furthermore, this study showed that the overwhelming majority consumed all the five minimum food group requirements in Nigeria within the framework of food group adequacy; this is not consistent with what is observable in the UK, with approximately half meeting this requirement. The foods include starchy staples, vegetables, fruits, pulses, nuts and seeds and animal-source foods. This may be due to several factors, such as socioeconomic status. The broader body of evidence consistently indicates a favourable correlation between the socioeconomic profile and food quality within various demographic segments of the UK population (Northstone et al., 2014; Maguire & Monsivais, 2015). Although the economic state of the UK is better than that of Nigeria, the standard of living is higher (World Bank 2022). Furthermore, Black African students encounter substantial financial stress and challenges in comprehending and assimilating into the culture of universities in the United Kingdom (Hyams-Ssekasi et al., 2014). Moreover, it was revealed that in Nigeria, the students had good habits regarding food that protects against NCDs, such as whole grain, pulses, vitamin A-rich orange vegetables, vegetables, vitamin A-rich fruits, citrus, nuts and seeds and dark green leafy vegetables. The consumption of these foods has been reduced by half in the UK.However, the food consumption rate that predisposes to NCDs was significantly higher in Nigeria compared to the UK. These foods include soft drinks, sweets, processed meat, packaged ultra-processed salty snacks, deep-fried food, unprocessed red meat fast food and instant noodles.
Furthermore, the findings of this study revealed that consumption of NCD-risk and NCD-protective food was in similar proportions simultaneously in Nigeria and the UK. This is not a good practice as standard dietary guidelines recommend higher consumption of NCD-protective foods and decreased consumption of NCD-protective food (Afshin et al., 2017). These findings support Sprake et al. (2018), who found out a sample of university students in the UK adhered to four primary eating patterns: vegetarian, snacking, health-conscious, and convenience-oriented, involving red meat and alcohol. This reveals the need to discourage NCD-risk diets and encourage more of NCD protective diets.
Overall, the students’ GDR, which is a measure of the level of consumption of NCD-protective foods and NCD-risk diets, was higher in Nigeria compared to the UK. However, this difference was not statistically significant and the GDR was poorly met in both categories. Keeping in view this finding, a study revealed that individuals of Black ethnicity exhibited significantly lower scores on the healthy eating rating and reduced consumption of micronutrients (Li et al., 2017). This finding is somewhat close to Bennett et al. (2022), who found out that Black/African American communities were identified as having lower fruit and vegetable consumption rates. In contrast, Asian groups attained elevated diet quality ratings owing to increased fish consumption and reduced fat intake. The limitation of these studies is that they were not conducted strictly among university students.
However, in this present study, correlation analysis showed a moderate negative significant correlation between academic stress experienced and adherence to the GDR. Thus, as the stress level increased, there was a significant decrease in their dietary quality, evidenced by their eating behaviour and food choices. Furthermore, negative correlations exist between the stress level and other healthy dietary indicators. However, the correlations were not statistically significant. The level of stress among the population was moderate. Specifically, nervousness, anger, upset, and inability to control things and situations were fairly often experienced. This finding somewhat contrasts a multiracial study that reported high-stress levels in general. However, they found that Blacks had non-statistically significantly lower levels than Whites (Turner & Smith, 2015). The differences might be due to other factors associated with stress, as revealed in a previous UK systematic review, such as childhood trauma, parental factors and other changes that come with moving into higher education (Campbell et al., 2022). However, the lower level might be due to coping and adaptive skills built by the Blacks who have had a history of discrimination and stigma. However, the association between academic stress and eating behaviour is keeping in view with the findings of a study among Black, Asian and Minority Ethnic groups, which revealed a significant association between stress in university life and eating behaviour (Mensah et al., 2022). The consistency of these findings mandates collaborative interventions from nutritionists, policy makers and mental health experts.
Conclusion
Conclusively, the study revealed that Black University Students in the UK experienced an overall moderate level of academic stress, which negatively impacted their eating behaviour and food choices. The findings underscore the significance of recognising and addressing the relationship between academic stress and dietary practices among this group of university students.
Strengths and Limitations
A significant strength of this study is that major subjects, including stress and eating behaviour, were explored. Eating behaviour and stress have an impact on conditions such as cancers and CVDs, which are referred to as the leading causes of death. Another strength of the study is that validated tools were used in the assessment, and appropriate statistical measures were employed. The study used a non-parametric test for the inferential analysis, having observed the distribution’s non-normalcy and small sample size (Mishra et al., 2019). Another uniqueness is that the study is the first of its kind among Black people residing in the UK. Hence, the study serves as empirical support for further studies and can also contribute to the body of evidence for qualitative or quantitative synthesis in systematic reviews.
Furthermore, the study provided room for further research to explore the impact of the environment on dietary behaviours. However, this study was limited by its response rate, as many people were non-responsive to the research despite being assured that their responses would be confidential and that they had the right to withdraw at any time as they deemed fit. This might be because no financial gifts were attached to participation in the study. Therefore, we can say the study was limited by insufficient funding to cover a broader geographical scope and give participants a token. Furthermore, the study’s small sample size may affect the statistical power and increase the likelihood of type 2 errors (Shreffler & Huecker, 2023). Also, the study’s generalizability was limited on account of the small sample size (Faber and Fonseca 2014).
The convenience sampling method predisposes to a high risk of bias (Jager et al., 2017), and cross-sectional design is less effective in investigating causal relationships compared to longitudinal design (Savitz & Wellenius, 2023). Moreover, confounding variables were not controlled, as the analysis was done via correlation and Wilcoxon signed rank test (Pourhoseingholi et al., 2012). Recall bias has been established to influence the self-reporting method of collecting data (Althubaiti, 2016).
Recommendations for Practice
Dietary Approach to Relieve Stress- This study revealed that the academic stress level had a moderate negative significant correlation with their eating behaviour and food choices as measured by their GDR score. One of the implications of this is to provide an evidenced-based nutritional approach to managing stress as there are some dietary interventions to improve mood, such as the Mediterranean diet (Parletta et al., 2019), a 50:50 ratio of corn and soybean oils (Gabbay et al., 2018).
Collaboration and Support: Collaborative approaches and supports are essential to addressing food behaviours and academic stress among university students. This might require the universities to create and implement programs tailored to their student’s particular requirements by consulting a diversified team of health specialists, dietitians, nutritionists and mental health specialists. Psychologists and counsellors can offer counselling sessions, workshops, and resources focusing on stress management techniques, coping strategies, and resilience-building skills to Black university students. By doing this, the effect of stress on their dietary habit will be reduced significantly. Furthermore, nutritionists, on the other hand, have a crucial role here as they can provide valuable expertise in drawing evidence-based dietary educational programs. Nutritionists can emphasise the importance of a balanced diet and help students plan realistic meals that suit the cultural and environmental factors influencing food choices. They will help the students identify possible food alternatives to what they usually consume while in their country of origin.
Stress Management Interventions: This study revealed a moderate level of academic stress among university students. Therefore, it is crucial for educational institutions to implement stress management interventions. Counseling services, workshops, and support groups tailored to address students’ specific needs can be effective in helping them cope with academic stress.
Promotion of Healthy Eating Habits: This present study has identified significant differences in food group diversity and consumption patterns when they were in Nigeria and the UK. Educational programs are, therefore, recommended to focus on the importance of a balanced diet and NCD-protective diets rich in fruits, vegetables, whole grains, and lean proteins. Furthermore, targeted nutrition education is necessary, and the students should be educated about the health importance of the consumption of NCD-protective food groups and the potential risks associated with NCD-risk diets.
Funding: This study was limited by insufficient funds; further studies would require grant application and fundings. Woosong University Academic Research funded a similar study by Choi (2020).
Recommendations for Research
Further studies should be conducted using a larger sample size of the Black population in the UK via a mixed-method approach to promote generalizability and reduce underrepresentation. Also, studies should adopt a probabilistic approach to sample selection to reduce the chances of sampling bias.
However, the sampled Blacks in the UK had better dietary habits in Nigeria, evidenced by higher compliance with global dietary recommendations. Qualitative studies should be conducted to explore cultural determinants of dietary behaviour and food choices in depth. Studies should also use qualitative methods to explore the impact of relocation on dietary patterns. Furthermore, other determinants of stress should be investigated, and confounding variables should be adjusted for in the analysis.
REFERENCES
- Afshin, A., Micha, R., Webb, M., Capewell, S., Whitsel, L., Rubinstein, A., Prabhakaran, D., Suhrcke, M. & Mozaffarian, D. (2017). Effectiveness of dietary policies to reduce non-communicable diseases. In: Disease Control Priorities, 5(3): Cardiovascular, Respiratory, and Related Disorders. The World Bank, 101–115.
- Agriculture, Nutrition & Health Academy, (2021). Technical consultation on measuring healthy diets: Concepts, methods, and metrics . https://www.anh-academy.org/sites/default/files/2021-06/Global%20DQ%20Project%20Fact%20Sheet%20-%20Technical%20Consultation%20on%20Measuring%20Healthy%20Diets.pdf
- Ahmed, I. & Ishtiaq, S. (2021). Reliability and validity: Importance in medical research. The Journal of the Pakistan Medical Association, 71 (10), 2401–2406. https://pubmed.ncbi.nlm.nih.gov/34974579/
- Ajayi, J. F., Udo, R. K., Kirk-Greene, A. H. M.& Falola, T. O. (2023). Nigeria. Encyclopedia Britannica. https://www.britannica.com/place/Nigeria
- Almogbel, E., Aladhadh, A. M., Almotyri, B. H., Alhumaid, A. F. & Rasheed, N. (2019). Stress associated alterations in dietary behaviours of undergraduate students of Qassim University, Saudi Arabia. Open access Macedonian Journal of medical sciences, 7 (13), 2182–2188. http://dx.doi.org/10.3889/oamjms.2019.571
- Al-Qahtani, M. H. (2016). Dietary habits of Saudi medical students at university of Dammam. International journal of health sciences, 10 (3), 353–362.
- Alsulami, S., Al Omar, Z., Binnwejim, M. S., Alhamdan, F., Aldrees, A., Al-Bawardi, A., Alsohim, M. & Alhabeeb, M. (2018). Perception of academic stress among Health Science Preparatory Program students in two Saudi universities. Advances in medical education and practice, 9, 159–164. https://pubmed.ncbi.nlm.nih.gov/29559816/ .
- Anaman-Torgbor, J. A., Tarkang, E., Adedia, D., Attah, O. M., Evans, A. & Sabina, N. (2021). Academic-related stress among Ghanaian nursing students. Florence Nightingale Journal of Nursing, 29 (3), 263–270. http://dx.doi.org/10.5152/FNJN.2021.21030 .
- Asif, S., Mudassar, A., Shahzad, T. Z., Raouf, M. & Pervaiz, T. (2020). Frequency of depression, anxiety and stress among university students. Pakistan Journal of Medical Sciences Quarterly, 36 (5), 971–976. http://dx.doi.org/10.12669/pjms.36.5.1873 .
- Atta, I. S. & Almilaibary, A. (2022). The prevalence of stress among medical students studying an integrative curriculum during the COVID-19 pandemic. Advances in medical education and practice, 13, 35–45. http://dx.doi.org/10.2147/AMEP.S345330 .
- Awadalla, N. J., Alsabaani, A. A., Alsaleem, M. A., Alsaleem, S. A., Alshaikh, A. A., Al-Fifi, S. H. & Mahfouz, A. A. (2022). Increased mental stress among undergraduate medical students in south-western Saudi Arabia during the COVID-19 pandemic. PeerJ , 10 (e13900), e13900. http://dx.doi.org/10.7717/peerj.13900 .
- Barbayannis, G., B&ari, M., Zheng, X., Baquerizo, H., Pecor, K. W. & Ming, X. (2022). Academic stress and mental well-being in college students: Correlations, affected groups, and COVID-19. Frontiers in psychology, 13, 886344. http://dx.doi.org/10.3389/fpsyg.2022.886344 .
- Bedewy, D. & Gabriel, A. (2015). Examining perceptions of academic stress and its sources among university students: The Perception of Academic Stress Scale. Health psychology open, 2 (2), 2055102915596714. http://dx.doi.org/10.1177/2055102915596714 .
- Bekhet, A. K. & Zauszniewski, J. A. (2012). Methodological triangulation: an approach to understanding data. Nurse researcher, 20 (2), 40–43. https://pubmed.ncbi.nlm.nih.gov/23316537/ .
- Bennett, G., Bardon, L. A. & Gibney, E. R. (2022). A comparison of dietary patterns and factors influencing food choice among ethnic groups living in one locality: A systematic review. Nutrients, 14 (5), 941. http://dx.doi.org/10.3390/nu14050941
- Berggreen-Clausen, A., Hseing Pha, S., Mölsted Alvesson, H., &ersson, A. & Daivadanam, M. (2022). Food environment interactions after migration: a scoping review on low- and middle-income country immigrants in high-income countries. Public health nutrition, 25 (1), 136–158. http://dx.doi.org/10.1017/S1368980021003943 .
- Bolarinwa, O. A. (2015). Principles and methods of validity and reliability testing of questionnaires used in social and health science researches. Nigerian Postgraduate Medical Journal, 22 (4), 195.
- Braun, V. & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative research in psychology, 3 (2), 77–101. http://dx.doi.org/10.1191/1478088706qp063oa
- Brown, A. G. M., Houser, R. F., Mattei, J., Lichtenstein, A. H. & Folta, S. C. (2019). Qualitative exploration of cultural factors influencing diet among African-, Caribbean- and US-born Blacks living in the northeast USA. Journal of nutritional science, 8 (e23), e23. http://dx.doi.org/10.1017/jns.2019.19
- Campbell, F., Blank, L., Cantrell, A., Baxter, S., Blackmore, C., Dixon, J. & Goyder, E. (2022). Factors that influence mental health of university and college students in the UK: a systematic review. BMC Public Health, 22 (1). http://dx.doi.org/10.1186/s12889-022-13943-x
- Caso, D., Miriam, C., Rosa, F. & Mark, C. (2020). Unhealthy eating and academic stress: The moderating effect of eating style and BMI. Health psychology open , 7 (2), 2055102920975274. http://dx.doi.org/10.1177/2055102920975274
- Chaaya, M., Osman, H., Naassan, G. & Mahfoud, Z. (2010). Validation of the Arabic version of the Cohen Perceived Stress Scale (PSS-10) among pregnant and postpartum women. BMC Psychiatry, 10 (1), 111. https://pubmed.ncbi.nlm.nih.gov/21159169/
- Choi, J. (2020). Impact of stress levels on eating behaviors among college students. Nutrients, 12 (5), 1241. http://dx.doi.org/10.3390/nu12051241
- Cohen, S., Kamarck, T. & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24 (4), 385–396. http://dx.doi.org/10.2307/2136404
- Complete University Guide, (2023). University league tables. Thecompleteuniversityguide.co.uk. https://www.thecompleteuniversityguide.co.uk/league-tables/rankings/south-west-england
- Debeuf, T., Verbeken, S., Van Beveren, M.-L., Michels, N. & Braet, C. (2018). Stress and eating behaviour: A daily diary study in youngsters. Frontiers in psychology, 9, 2657. http://dx.doi.org/10.3389/fpsyg.2018.02657
- Deliens, T., Clarys, P., De Bourdeaudhuij, I. & Deforche, B. (2014). Determinants of eating behaviour in university students: a qualitative study using focus group discussions. BMC Public Health , 14 (1), 53. http://dx.doi.org/10.1186/1471-2458-14-53
- Dickerson Turner, F. & Smith, J. K. (2023). A Comparattive Sttudy on The Sttress Levels of Black, Whitte, Asian, and Lattino Undergraduatte Sttudentts. Core.ac.uk. https://core.ac.uk/download/pdf/56319249.pdf
- Elfil, M. & Negida, A. (2017). Sampling methods in Clinical Research; an Educational Review. Emergency (Tehran, Iran), 5 (1), e52
- Garg, R. (2016). Methodology for research I. Indian journal of anaesthesia, 60 (9), 640–645. http://dx.doi.org/10.4103/0019-5049.190619
- Gilbert, B. B., Spencer, U. M., Hastings, M., Whitelock, D., Morrill, J. S., Joyce, P., Frere, S. S., Kishlansky, M. A., Barr, N. A., Briggs, A., Josephson, P. R., Ravenhill, W., Kellner, P., Chaney, W. A., Colley, L. J., Smith, L. B., Atkins, R. C. & Prestwich, M. C. (2023). United Kingdom. Encyclopedia Britannica
- Guetterman, T. C. (2019). Basics of statistics for primary care research. Family medicine and community health, 7 (2), e000067. http://dx.doi.org/10.1136/fmch-2018-000067 .
- Hansen, M., O’Brien, K., Meckler, G., Chang, A. M. & Guise, J.-M. (2016). Understanding the value of mixed methods research: the Children’s Safety Initiative-Emergency Medical Services. Emergency medicine journal: EMJ, 33 (7), 489–494. http://dx.doi.org/10.1136/emermed-2015-205277 .
- Hill, D. C., Moss, R. H., Sykes-Muskett, B., Conner, M. & O’Connor, D. B. (2018). Stress & eating behaviors in children and adolescents: Systematic review and meta-analysis. Appetite, 123, 14–22. https://pubmed.ncbi.nlm.nih.gov/29203444/ .
- Hussien, F. M., Mebratu, W., Ahmed, A. Y., Mekonnen, T. C., Hassen, A. M., Asfaw, Z. A., Hassen, H. Y. & Abate, K. H. (2021). Performance of individual dietary diversity score to identify malnutrition among patients living with HIV in Ethiopia. Scientific reports , 11 (1), 18681. http://dx.doi.org/10.1038/s41598-021-98202-6 .
- In, J. (2017). Introduction of a pilot study. Korean Journal of Anesthesiology, 70 (6), 601–605. http://dx.doi.org/10.4097/kjae.2017.70.6.601 .
- International Organization for Migration, (2023). World Migration Report 2022. https://worldmigrationreport.iom.int/wmr-2022-interactive/ .
- Kabir, A., Miah, S. & Islam, A. (2018). Factors influencing eating behavior and dietary intake among resident students in a public university in Bangladesh: A qualitative study. PloS one , 13 (6), e0198801. http://dx.doi.org/10.1371/journal.pone.0198801 .
- Kaur, S. (2017). Sample Size Determination (For Descriptive Studies). International Journal of Current Research, 9 (3), 48365–48367.
- Kish, L. (1995). Survey Sampling. Nashville, TN, USA: John Wiley & Sons.
- Koo, T. K. & Li, M. Y. (2016). A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of chiropractic medicine, 15 (2), 155–163. http://dx.doi.org/10.1016/j.jcm.2016.02.012 .
- Kosche, C., Rolader, R. & Yeung, H. (2021). Respect for human subjects: Ethics in research design. In: Dermatoethics. Cham: Springer International Publishing, 433–443.
- Lee, E.-H. (2012). Review of the psychometric evidence of the perceived stress scale. Asian nursing research, 6 (4), 121–127. https://pubmed.ncbi.nlm.nih.gov/25031113/ .
- Lee, S. D., Kellow, N. J., Huggins, C. E. & Choi, T. S. T. (2022). How and why diets change post-migration: A qualitative exploration of dietary acculturation among recent Chinese immigrants in Australia. Nutrients, 14 (17), 3573. http://dx.doi.org/10.3390/nu14173573 .
- Li, W., Youssef, G., Procter-Gray, E., Olendzki, B., Cornish, T., Hayes, R., Churchill, L., Kane, K., Brown, K. & Magee, M. F. (2017). Racial differences in eating patterns and food purchasing behaviors among urban older women. The journal of nutrition, health & aging, 21 (10), 1190–1199. http://dx.doi.org/10.1007/s12603-016-0834-7
- Lin, X.-J., Zhang, C.-Y., Yang, S., Hsu, M.-L., Cheng, H., Chen, J. & Yu, H. (2020). Stress and its association with academic performance among dental undergraduate students in Fujian, China: a cross-sectional online questionnaire survey. BMC medical education, 20 (1), 181. http://dx.doi.org/10.1186/s12909-020-02095-4 .
- Maguire, E. R. & Monsivais, P. (2015). Socio-economic dietary inequalities in UK adults: an updated picture of key food groups and nutrients from national surveillance data. The British journal of nutrition, 113 (1), 181–189. http://dx.doi.org/10.1017/S0007114514002621 .
- Mcleod, S. (2023). Erik erikson’s stages of psychosocial development. Simply Psychology. https://www.simplypsychology.org/Erik-Erikson.html .
- Mensah, F. Z., Lane, K. E. & Richardson, L. D. (2022). Determinants of eating behaviour in Black, Asian and Minority Ethnic (BAME) university students when living at and away from home: With a focus on the influence of food enculturation and food acculturation. Appetite, 171 (105932), 105932. https://www.sciencedirect.com/science/article/pii/S019566632200023X..
- Miller, V., Webb, P., Cudhea, F., Shi, P., Zhang, J., Reedy, J., Erndt-Marino, J., Coates, J., Mozaffarian, D. & Global Dietary Database, (2022). Global dietary quality in 185 countries from 1990 to 2018 show wide differences by nation, age, education, and urbanicity. Nature food, 3 (9), 694–702. https://www.nature.com/articles/s43016-022-00594-9 .
- Mitchell, A. M., Crane, P. A. & Kim, Y. (2008). Perceived stress in survivors of suicide: psychometric properties of the Perceived Stress Scale. Research in nursing & health, 31 (6), 576–585. https://pubmed.ncbi.nlm.nih.gov/18449942/ .
- Mozumder, M. K. (2022). Reliability and validity of the Perceived Stress Scale in Bangladesh. PloS one , 17 (10), e0276837. http://dx.doi.org/10.1371/journal.pone.0276837 .
- Northstone, K., Smith, A. D. A. C., Cribb, V. L. & Emmett, P. M. (2014). Dietary patterns in UK adolescents obtained from a dual-source FFQ and their associations with socio-economic position, nutrient intake and modes of eating. Public health nutrition , 17 (7), 1476–1485. https://www.cambridge.org/core/journals/public-health-nutrition/article/dietary-patterns-in-uk-adolescents-obtained-from-a-dualsource-ffq-and-their-associations-with-socioeconomic-position-nutrient-intake-and-modes-of-eating/2C5F1B30FAEDAB7945766AC116DC10F3 .
- Noyes, J., Booth, A., Moore, G., Flemming, K., Tunçalp, Ö. & Shakibazadeh, E. (2019). Synthesising quantitative and qualitative evidence to inform guidelines on complex interventions: clarifying the purposes, designs and outlining some methods. BMJ global health, 4 (Suppl 1), e000893. http://dx.doi.org/10.1136/bmjgh-2018-000893 .
- Pascoe, M. C., Hetrick, S. E. & Parker, A. G. (2020). The impact of stress on students in secondary school and higher education. International journal of adolescence and youth, 25 (1), 104–112. http://dx.doi.org/10.1080/02673843.2019.1596823
- Patino, C. M. & Ferreira, J. C. (2018). Inclusion and exclusion criteria in research studies: definitions and why they matter. Jornal brasileiro de pneumologia: publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia , 44 (2), 84–84. http://dx.doi.org/10.1590/s1806-37562018000000088
- Ramli, N. H., Alavi, M., Mehrinezhad, S. A. & Ahmadi, A. (2018). Academic stress and self-regulation among university students in Malaysia: Mediator role of mindfulness. Behavioral sciences, 8 (1). http://dx.doi.org/10.3390/bs8010012.
- Rasheed, F. A., Naqvi, A. A., Ahmad, R. & Ahmad, N. (2017). Academic stress and prevalence of stress-related self-medication among undergraduate female students of health and non-health cluster colleges of a public sector university in Dammam, Saudi Arabia. Journal of pharmacy & bioallied sciences, 9 (4), 251–258. http://dx.doi.org/10.4103/jpbs.JPBS_189_17 .
- Santana, C. C. A., Hill, J. O., Azevedo, L. B., Gunnarsdottir, T. & Prado, W. L. (2017). The association between obesity and academic performance in youth: a systematic review: Obesity and academic performance. Obesity reviews: an official journal of the International Association for the Study of Obesity, 18 (10), 1191–1199. https://pubmed.ncbi.nlm.nih.gov/28742946/ .
- Schoonenboom, J. & Johnson, R. B. (2017). How to construct a mixed methods research design. Kölner Zeitschrift für Soziologie und Sozialpsychologie , 69 (Suppl 2), 107–131. http://dx.doi.org/10.1007/s11577-017-0454-1 .
- Setia, M. S. (2016). Methodology series module 3: Cross-sectional studies. Indian journal of dermatology, 61 (3), 261–264. http://dx.doi.org/10.4103/0019-5154.182410.
- Soe, K. H., Than, N., Lwin, H., Htay, N. M., Phyu, K. & Abas, A. (2018). Knowledge, attitudes, and barriers toward research: The perspectives of undergraduate medical and dental students. Journal of education and health promotion, 7 (1), 23. http://dx.doi.org/10.4103/jehp.jehp_61_17 .
- Sprake, E. F., Russell, J. M., Cecil, J. E., Cooper, R. J., Grabowski, P., Pourshahidi, L. K. & Barker, M. E. (2018). Dietary patterns of university students in the UK: a cross-sectional study. Nutrition journal , 17 (1). http://dx.doi.org/10.1186/s12937-018-0398-y.
- Sundjaja, J. H., Shrestha, R. & Krishan, K. (2022). McNemar And Mann-Whitney U Tests. In: StatPearls. StatPearls Publishing.
- Tenny, S. & Abdelgawad, I. (2022). Statistical Significance. In: StatPearls. StatPearls Publishing.
- Uyar, B. T. M., Talsma, E. F., Herforth, A. W., Trijsburg, L. E., Vogliano, C., Pastori, G., Bekele, T. H., Huong, L. T. & Brouwer, I. D. (2023). The DQQ is a valid tool to collect population-level food group consumption data: A study among Women in Ethiopia, Vietnam, and Solomon Islands. The journal of nutrition, 153 (1), 340–351. https://www.sciencedirect.com/science/article/pii/S0022316622132591. .
- Wang, H., Herforth, A. W., Xi, B. & Zou, Z. (2022). Validation of the Diet Quality Questionnaire in Chinese children and adolescents and relationship with pediatric overweight and obesity. Nutrients , 14 (17), 3551. http://dx.doi.org/10.3390/nu14173551 .
- Wang, X. & Cheng, Z. (2020). Cross-sectional studies: Strengths, weaknesses, and recommendations. Chest, 158 (1S), S65–S71. http://dx.doi.org/10.1016/j.chest.2020.03.012. .
- World Bank, (2022). The world by income and region. Worldbank.org. https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html .
- World Health Organization, (2020). Healthy diet. https://www.who.int/news-room/fact-sheets/detail/healthy-diet .
- World Health Organization, (2021). Report of the technical consultation on measuring healthy diets: concepts, methods and metrics. https://apps.who.int/iris/rest/bitstreams/1405539/retrieve .
- World Medical Association, (2018). WMA declaration of Helsinki – ethical principles for medical research involving human subjects. https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ .
- Wright, S., O’Brien, B. C., Nimmon, L., Law, M. & Mylopoulos, M. (2016). Research design considerations. Journal of graduate medical education, 8 (1), 97–98. http://dx.doi.org/10.4300/JGME-D-15-00566.1 .
- Yau, Y. H. C. & Potenza, M. N. (2013). Stress and eating behaviors. Minerva endocrinologica, 38 (3), 255–267.
APPENDIX
APPENDIX 1: INFORMED CONSENT FORM
Participant Information Sheet
You are being invited to take part in a research project. Before you decide, it is important for you to understand why the research is being done and what it will involve. Please take time to read the following information carefully and discuss it with others if you wish. Ask us if there is anything that is not clear or if you would like more information. Take time to decide whether or not you wish to take part.
The title of the research project:
Exploring the experience of academic stress, eating behavior, and food choice in black university students.
What is the purpose of the research/questionnaire?
The aim of this project is to explore the experience of academic stress, eating behavior, and food choices in Nigerian postgraduate students studying in the United Kingdom. This simply means the project’s main objective is to discover the significant relationship between stress, eating behavior, food choices, and relocation.
Why have I been chosen?
The project is looking to have Nigerian participants who lived in Nigeria prior to their studies in the United Kingdom and are postgraduate students in the United Kingdom.
Do I have to take part?
It is up to you to decide whether or not to take part. If you do decide to take part, you will be given this information sheet to keep and be asked to sign a participant agreement form. We want you to understand what participation involves before you make a decision on whether to participate. If you or any family member have an ongoing relationship with BU or the research team, e.g., as a member of staff, as a student, or other service user, your decision on whether to take part (or continue to take part) will not affect this relationship in any way.
Can I change my mind about taking part?
Yes, you can stop participating in study activities at any time and without giving a reason. After you decide to withdraw from the study, we will not collect any further information from or about you. As regards to the information we have already collected before this point, your rights to access, change or move that information are limited. This is because we need to manage your information in specific ways in order for the research to be reliable and accurate.
What would taking part involve?
Taking part in this project requires you to fill a 4-sectioned close-ended survey with questions pertaining to the project title.
What are the advantages and possible disadvantages or risks of taking part?
Whilst there are no immediate benefits for those people participating in the project, it is hoped that this work will vastly contribute to the study gap this project is aimed at filling, indirectly adding to the bulk of knowledge required in Nutrition at large. Whilst we do not anticipate any risks to you in taking part in this study, you may be required to process some questions which might have an emotional impact on you.
What type of information will be sought from me and why is the collection of this information relevant for achieving the research project’s objectives?
Information concerning diet, stress, eating behavior, and food choices would be required. The responses to the survey are the information intended to be used to answer research questions which would bring a conclusion to this project.
How will my information be managed?
Bournemouth University (BU) is the organization with overall responsibility for this study and the Data Controller of your personal information, which means that we are responsible for looking after your information and using it appropriately. Research is a task that we perform in the public interest, as part of our core function as a university. Undertaking this research study involves collecting and/or generating information about you. We manage research data strictly in accordance with ethical requirements and current data protection laws. These control the use of information about identifiable individuals but do not apply to anonymous research data: “anonymous” means that we have either removed or not collected any pieces of data or links to other data which identify a specific person as the subject or source of a research result.
BU’s Research Participant Privacy Notice sets out more information about how we fulfill our responsibilities as a data controller and about your rights as an individual under the data protection legislation. We ask you to read this Notice so that you can fully understand the basis on which we will process your personal information. Research data will be used only for the purposes of the study or related uses identified in the Privacy Notice or this Information Sheet. To safeguard your rights in relation to your personal information, we will use the minimum personally-identifiable information possible and control access to that data as described below.
Publication:
You will not be able to be identified in any external reports or publications about the research without your specific consent. Otherwise, your information will only be included in these materials in an anonymous form, i.e., you will not be identifiable.
Security and access controls:
BU will hold the information we collect about you in hardcopy in a secure location and on a BU password-protected secure network where held electronically. Personal information which has not been anonymized will be accessed and used only by appropriate, authorized individuals and when this is necessary for the purposes of the research or another purpose identified in the Privacy Notice. This may include giving access to BU staff or others responsible for monitoring and/or audit of the study, who need to ensure that the research is complying with applicable regulations.
Further use of your information:
The information collected about you may be used in an anonymous form to support other research projects in the future, and access to it in this form will not be restricted. It will not be possible for you to be identified from this data.
Keeping your information if you withdraw from the study:
If you withdraw from active participation in the study, we will keep information which we have already collected from or about you if this has ongoing relevance or value to the study. This may include your personally identifiable information. As explained above, your legal rights to access, change, delete, or move this information are limited as we need to manage your information in specific ways in order for the research to be reliable and accurate. However, if you have concerns about how this will affect you personally, you can raise these with the research team when you withdraw from the study. You can find out more about your rights in relation to your data and how to raise queries or complaints in our Privacy Notice.
Retention of research data:
Project governance documentation, including copies of signed participant agreements: we keep this documentation for a long period after completion of the research so that we have records of how we conducted the research and who took part. The only personal information in this documentation will be your name and signature, and we will not be able to link this to any anonymized research results.
Research results:
This research is being carried out as part of the coursework for a degree awarded by BU. We will keep your personal information in identifiable form until after the assessment and award of the degree. You can find more specific information about retention periods for personal information in our Privacy Notice. We keep anonymized research data indefinitely so that it can be used for other research as described.
Contact for further information:
If you have any questions or would like Further Information, please contact; Supervisor: Chloe Casey [ccasey@bournemouth.ac.uk]
Research Team:
Priscilla Jekayinfa [S5515203@BOURNEMOUTH.AC.UK]
In case of complaints:
Any concerns about the study should be directed to s5515203@bournemouth.ac.uk.
If your concerns have not been answered by s5515203@bournemouth.ac.uk, you should contact Bournemouth University by email to researchgovernance@bournemouth.ac.uk. Thank you for considering taking part in this research project. Kindly respond if you have read the participant information sheet.
Please indicate that you have read and understood the participant information sheet for this research project and you consent to take part in the questionnaire before continuing.
I have read and understood the participant information sheet and I consent to take part in this questionnaire [ ]
I Do Not Consent To Take Part In This Questionnaire [ ]
I am a black university student currently studying the United Kingdom (a) Yes [ ] (b) No [ ]
APPENDIX II: QUESTIONNAIRE ON EXPLORING THE EXPERIENCE OF ACADEMIC STRESS, EATING BEHAVIOR, AND FOOD CHOICE IN BLACK UNIVERSITY STUDENTS
Part 1: SOCIODEMOGRAPHIC PROFILE
Age as at last birthday__________years
Gender (a) male (b) female (c) prefer not to say
Average Monthly Income/allowance (in pounds)_________________
Academic Level (a) undergraduate (b) postgraduate
Have you ever received nutrition-related education in any of your courses (a) Yes (b) No
SECTION 2: Dietary Quality while in NIGERIA. Now I’d like to ask you some yes-or-no questions about foods and drinks that you consumed the day before the last day in Nigeria during the day or night, whether you had it at home or somewhere else. Indicate yes or no as appropriate.
| Food items | (circle answer) | ||
| 1 | Rice, semo, couscous, bread, spaghetti, masa, pap, or tuwo/nri-eserese? | YES or NO | |
| 2 | Porridge, egbo/ dambu, corn, or Ofada rice? | YES or NO | |
| 3 | Sweet potato, fufu, gari, abacha, yam, lafun, blackamala, or plantain? | YES or NO | |
| 4 | Beans, awara from soy, moinmoin, Bambara groundnuts, pigeonpeas, African yambeans, or other local beans? | YES or NO | |
| Vegetables: | |||
| 5 | Carrots, pumpkin, squash that is orange inside, or sweet potatoes that are orange inside? | YES or NO | |
| 6.1 | Ewedu/ayoyo, pumpkin leaves, water leaves, bitter leaves, green, soko leaves, or baobab leaves? | YES or NO | |
| 6.2 | Zobo leaves, afang/okazi, karkashi, garden egg leaves, sweet potato leaves, or cowpea leaves? | YES or NO | |
| 7.1 | Tomatoes, garden eggs, okro, cucumber, green pepper, cabbage, or green beans? | YES or NO | |
| Fruits: | |||
| 8 | Mango, pawpaw, golden melon, locust bean fruit, or African cherry? | YES or NO | |
| 9 | Orange, tangerine, or grape fruit? | YES or NO | |
| 10.1 | Banana, guava, soursop, watermelon, cashewfruit, orapple? | YES or NO | |
| 10.2 | Pineapple, avocado pear, coconut flesh, dates, African bush pear,or African elemi? | YES or NO | |
| Sweets: | |||
| 11 | Cakes, cookies, sweet biscuits, wafers, chinchin, or puff puff? | YES or NO | |
| 12 | Sweets, chocolates, ice cream, or sesame brittle? | YES or NO | |
| Foods of animal origin: | |||
| 13 | Eggs or eggrolls? | YES or NO | |
| 14 | Wara from milk, or dairy cheese? | YES or NO | |
| 15 | Yogurt, nono, or furadenono? | YES or NO | |
| 16 | Sausages, hotdogs, corned beef, or kilishi? | YES or NO | |
| 17 | Cowmeat, rammeat, goatmeat, or any organs from these animals? | YES or NO | |
| 18 | Pigmeat, rabbit, dogmeat, or bushmeat? | YES or NO | |
| 19 | Chicken, turkey, guineafowl, quail, duck, or pigeon? | YES or NO | |
| 20 | Fish, canned fish, crab, prawn, or shrimp? | YES or NO | |
| Other foods: | |||
| 21 | Groundnuts, melonseeds, ogbono, bread fruit seeds, walnuts, or cashews? | YES or NO | |
| 22 | Packaged potato chips such as Pringles, or packaged plantain chips? | YES or NO | |
| 23 | Instant noodles such as Indomie or Chikki? | YES or NO | |
| 24 | Fried plantain, fried sweet potato, fried yam, akara, eggroll, samosa or springrolls, fried fish, or fried meat? | YES or NO | |
| Beverages: | |||
| 25 | Milk including powdered milk? | YES or NO | |
| 26 | Tea with sugar, coffee with sugar, 3-in-1, choco drink, Milo or Bournvita? | YES or NO | |
| 27 | Fruit juice, fruit flavoured drinks, zobo, or kunu? | YES or NO | |
| 28 | Soft drinks such as Coca-Cola, Fanta, Sprite, or chapman, malt drinks, or energy drinks such as Red Bull? | YES or NO | |
| Yesterday, did you get food from any place like… | |||
| 29 | Mr. Biggs, Big Treat, Domino’s, KFC, Tantalizer, or other places that serve meat pie, chicken pie, pizza or burgers? | YES or NO | |
SECTION 3: Dietary Quality now in UK. Now I’d like to ask you some yes-or-no questions about foods and drinks that you consumed YESTERDAY during the day or night, whether you had it at home or somewhere else.
Please read the list of foods and drinks, and if you ate or drank ANY ONE OF THEM YESTERDAY, indicate yes.
| Food items | (circle answer) | |
| 1 | Rice, semo, couscous, bread, spaghetti, masa, pap, or tuwo / nri-eserese, pasta, tortilla? | YES or NO |
| 2 | Porridge, egbo / dambu, corn, Ofada rice, Fresh corn, popcorn, oats, granola, brown rice, or quinoa? | YESorNO |
| 3 | Sweet potato, fufu, gari, abacha, yam, lafun, black amala, or plantain? | YES or NO |
| 4 | Beans, refried beans, peas, lentils, hummus, chickpeas, tofu, lima beans, awara from soy, moin moin, bambara groundnuts, pigeon peas, African yam beans, or other local beans? | YES or NO |
| Vegetables: | ||
| 5 | Carrots, red tatase(red bell pepper), pumpkin, squash that is orange inside, or sweet potatoes that are orange inside? | YES or NO |
| 6.1 | Ewedu / ayoyo, pumpkin leaves, water leaves, bitter leaves, green, soko leaves, baobab leaves, broccoli, spinach, arugula, kale, collards, turnip greens, or mustard greens? | YES or NO |
| 7.1 | Zobo leaves, afang / okazi, karkashi, garden egg leaves, sweet potato leaves, cowpea leaves, Lettuce, tomatoes, green beans, celery, green peppers, cabbage, or cucumber? | YES or NO |
| 7.2 | Tomatoes, garden eggs, okro, cucumber, green pepper, cabbage, green beans, zucchini, mushrooms, eggplant, cauliflower, okra, asparagus, or radish? | YES or NO |
| Fruits: | ||
| 8 | Mango, ogbono fruit, pawpaw, golden melon, locust bean fruit, African cherry, canteloupe, mango, papaya, apricots, or dried apricots? | YES or NO |
| 9 | Orange, clementine, mandarin, tangerine, or grapefruit? | YES or NO |
| 10.1 | Banana, guava, soursop, watermelon, grapes, avocado, berries, cherries, cashew fruit, or apple? | YES or NO |
| 10.2 | Pineapple, avocado pear, kiwi, plums, prunes, peaches, nectarines, coconut flesh, dates, African bush pear, or African elemi? | YES or NO |
| Sweets: | ||
| 11 | Cakes, cookies, sweet biscuits, wafers, brownies, donuts, pastries, pie, chin chin, or puff puff? | YES or NO |
| 12 | Sweets, candy, candy bars, chocolates, ice cream, popsicles, milkshakes, pudding, ice cream, or sesame brittle? | YES or NO |
| Yesterday, did you eat any of the following foods of animal origin: | ||
| 13 | Eggs or egg rolls? | YES or NO |
| 14 | Wara from milk, or dairy cheese? | YES or NO |
| 15 | Yogurt, nono, or fura de nono? | YES or NO |
| 16 | Sausages, hot dogs, corned beef, kilishi, pepperoni, luncheon meat, ham, or bacon? | YES or NO |
| 17 | Hamburger, lamb, venison, cow meat, ram meat, goat meat, or any organs from these animals? | YES or NO |
| 18 | Pig meat, rabbit, dog meat, or bush meat? | YES or NO |
| 19 | Chicken, turkey, guinea fowl, quail, duck, or pigeon? | YES or NO |
| 20 | Fish, canned fish, crab, prawn, shrimp, tunafish, or seafood? | YES or NO |
| Other foods: | ||
| 21 | Groundnuts, melon seeds, ogbono, breadfruit seeds, walnuts, cashews, peanut butter, almond butter, peanuts, almonds, pecans, or pistachios? | YES or NO |
| 22 | Packaged potato chips such as Pringles, packaged plantain chips, cheetos, Doritos, Fritos, or Pringles? | YES or NO |
| 23 | Instant noodles such as Indomie or Chikki, ramen noodle soup or other instant soups? | YES or NO |
| 24 | Fried plantain, fried sweet potato, fried yam, akara, egg roll, samosa or spring rolls, fried fish, fried meat, french fries, onion rings, fried chicken, chicken nuggets, fish sticks, fish fry, or fried shrimp? | YES or NO |
| beverages: | ||
| 25 | Milk, including dairy milk on cereal or in lattes? | YES or NO |
| 26 | Fruit juice, fruit-flavored drinks, lemonade, sweet tea, tea with sugar, coffee with sugar, 3- in-1, choco drink, Milo or Bournvita? | YES or NO |
| 27 | Fruit juice, fruit flavoured drinks, zobo, or kunu? | YES or NO |
| 28 | Soft drinks such as Coca-Cola, Fanta, Sprite, or chapman, malt drinks, or energy drinks such as Red Bull, Pepsi, or Dr Pepper, sports drinks? | YES or NO |
| Yesterday, did you get food from any place like… | ||
| 29 | Yesterday, did you get food from places that serve meat pie, chicken pie, pizza or burgers, McDonald’s, Burger King, Subway or equivalents? | YES or NO |
SECTION 4: PERCEIVED STRESS SCALE
INSTRUCTIONS: The questions in this scale ask you about your feelings and thoughts during the last month. In each case, please indicate your response by placing an “X” over the circle representing HOW OFTEN you felt or thought a certain way.
| Items | Never Almost Never Sometimes Fairly Often Very Often |
| 1. In the last month, how often have you been upset because of something that happened unexpectedly? | |
| 2. In the last month, how often have you felt that you were unable to control the important things in your life? | |
| 3. In the last month, how often have you felt nervous and “stressed”? | |
| 4. In the last month, how often have you felt confident about your ability to handle your personal problems? | |
| 5. In the last month, how often have you felt that things were going your way? | |
| 6. In the last month, how often have you found that you could not cope with all the things that you had to do? | |
| 7. In the last month, how often have you been able to control irritations in your life? | |
| 8. In the last month, how often have you felt that you were on top of things? | |
| 9. In the last month, how often have you been angered because of things that were outside your control? | |
| 10. In the last month, how often have you felt difficulties were piling up so high that you could not overcome them? |
Thank you so much for participating. Your responses to this survey are invaluable and they would definitely contribute to the information gap in nutrition and behaviour at large.
APPENDIX III: ANALYSIS
| Tests of Normality | ||||||
| Kolmogorov-Smirnova | Shapiro-Wilk | |||||
| Statistic | df | Sig. | Statistic | df | Sig. | |
| FGDS total | .315 | 37 | .000 | .624 | 37 | .000 |
| Food adequacy total score | .538 | 37 | .000 | .155 | 37 | .000 |
| GDR | .194 | 37 | .001 | .886 | 37 | .001 |
| FGDS2 | .143 | 37 | .054 | .928 | 37 | .020 |
| Food Group Adequacy | .311 | 37 | .000 | .775 | 37 | .000 |
| Global Dietary Recommendations (GDR) score | .113 | 37 | .200* | .974 | 37 | .520 |
| NCD Protect | .256 | 37 | .000 | .756 | 37 | .000 |
| NCD Risk | .269 | 37 | .000 | .728 | 37 | .000 |
| NCD Protect | .159 | 37 | .019 | .950 | 37 | .099 |
| NCDRISK2 | .218 | 37 | .000 | .815 | 37 | .000 |
| Sum PSS | .093 | 37 | .200* | .972 | 37 | .454 |
| *. This is a lower bound of the true significance. | ||||||
| a. Lilliefors Significance Correction | ||||||
| Ranks | ||||
| N | Mean Rank | Sum of Ranks | ||
| FGDS2 – FGDS total | Negative Ranks | 31a | 16.90 | 524.00 |
| Positive Ranks | 1b | 4.00 | 4.00 | |
| Ties | 5c | |||
| Total | 37 | |||
| Food Group Adequacy – Food adequacy total score | Negative Ranks | 18d | 9.50 | 171.00 |
| Positive Ranks | 0e | .00 | .00 | |
| Ties | 19f | |||
| Total | 37 | |||
| Global Dietary Recommendations (GDR) score – GDR | Negative Ranks | 20g | 18.27 | 365.50 |
| Positive Ranks | 13h | 15.04 | 195.50 | |
| Ties | 4i | |||
| Total | 37 | |||
| NCD Protect – NCD Protect | Negative Ranks | 31j | 17.71 | 549.00 |
| Positive Ranks | 2k | 6.00 | 12.00 | |
| Ties | 4l | |||
| Total | 37 | |||
| NCDRISK2 – NCD Risk | Negative Ranks | 21m | 15.52 | 326.00 |
| Positive Ranks | 5n | 5.00 | 25.00 | |
| Ties | 11o | |||
| Total | 37 | |||
| a. FGDS2 < FGDS total | ||||
| b. FGDS2 > FGDS total | ||||
| c. FGDS2 = FGDS total | ||||
| d. Food Group Adequacy < Food adequacy total score | ||||
| e. Food Group Adequacy > Food adequacy total score | ||||
| f. Food Group Adequacy = Food adequacy total score | ||||
| g. Global Dietary Recommendations (GDR) score < GDR | ||||
| h. Global Dietary Recommendations (GDR) score > GDR | ||||
| i. Global Dietary Recommendations (GDR) score = GDR | ||||
| j. NCD Protect < NCD Protect | ||||
| k. NCD Protect > NCD Protect | ||||
| l. NCD Protect = NCD Protect | ||||
| m. NCDRISK2 < NCD Risk | ||||
| n. NCDRISK2 > NCD Risk | ||||
| o. NCDRISK2 = NCD Risk | ||||