
Health Professionals’ Identification Levels of Risk Factors: In View of The Management of In-Patients Admitted with Upper Gastrointestinal Tract Swallowing Disorders in a Kenyan National Hospital
- Ndiema Dalphine C.
- Abuom T.
- Karia M.
- 740-751
- Apr 21, 2024
- Health
Health Professionals’ Identification Levels of Risk Factors: In View of The Management of In-Patients Admitted with Upper Gastrointestinal Tract Swallowing Disorders in a Kenyan National Hospital
Ndiema Dalphine C., Abuom T., Karia M.
Department of Early Childhood Studies and Special Needs Education (Speech-Language Pathology). Kenyatta University, Nairobi, Kenya
DOI: https://doi.org/10.51244/IJRSI.2024.1103052
Received: 05 March 2024; Accepted: 15 March 2024; Published: 20 April 2024
ABSTRACT
Adequate dysphagia awareness among health professionals is vital to facilitate collaborative dysphagia management. However, there are concerns that in many countries, many health professionals have low or moderate dysphagia awareness. In this descriptive, cross-sectional study, we assessed the identification levels on risk factors of oropharyngeal dysphagia among health professionals attending to adult inpatients in the acute-care facility of a level-six hospital in Kenya. The sample comprised 16 professionals from six specialties: neurologists, oncologists, nurses, nutritionists, physiotherapists, and speech-language therapists. We measured their risk factor identification levels using a previously validated nine-item questionnaire. Frequencies, percentages, and means were used to identify key patterns in participants’ risk factor identification levels, while the independent samples t-test and one-way ANOVA were used to establish cross-sectional differences in identification levels based on selected demographic and general characteristics. The mean risk factor identification score was 73.6% (SD = 17.14). There were significant differences in identification scores due to age (F = 4.67, p = .030), educational attainment (F = 5.94, p = .015), experience (F = 5.34, p = .020), and specialization (F = 5.06, p = .024). Mean comparisons showed that identification levels increased with educational attainment and were highest among participants in the category comprising oncologists, nutritionists, and speech therapists. From the findings, we concluded that health professionals in the facility have, on average, moderate OPD risk factor awareness and that increased educational attainment may enhance OPD awareness.
Keywords—awareness, interprofessional collaboration, oropharyngeal dysphagia, risk factor.
INTRODUCTION
A. Background Information
Oropharyngeal dysphagia (OPD) is a prevalent condition, especially among older adults. This disorder is characterized by abnormal swallowing physiology in the upper gastrointestinal tract, leading to a range of clinical complications, including malnutrition, dehydration, aspiration, suffocation, pneumonia, and, in extreme cases, death [1]. With over 40% of the world’s population having OPD, it remains a leading contributor to pressures on the global healthcare system [2]. Countries in Sub-Saharan Africa have the highest OPD rates [2]. Dysphagia in a population is associated with lengthy hospital stays, high readmission rates, and up to 40% additional healthcare costs [3,4]. The high health and economic burdens associated with OPD call for effective preventative and management interventions.
High-level cooperation between health professionals (HPs) from different specialties is vital for effective OPD management [5,6]. A multi-disciplinary approach to OPD management is consistent with the World Health Organization (WHO)’s Interprofessional Collaboration (IPC) model, which advocates for practitioners in different specialties to work together in open-team practices when dealing with complex issues [7]. Dysphagia is among the intricate problems in healthcare, given that this condition cuts across different clinical domains. Yet, dysphagia management in most healthcare settings is primarily the function of speech-language pathologists/therapists (SLTs) [8]. Their roles include identifying, assessing, treating swallowing difficulties and preventing secondary complications [8]. The IPC model shifts OPD management from SLTs alone to a team of collaborators from multiple disciplines. In addition to SLTs, the team may include nurses, medical officers, nutritionists, and physiotherapists. The model may facilitate effective OPD management and improved patient outcomes by promoting collaboration and cross-team communication among diverse HPs [9].
Early risk factor identification is vital for effective disease management. Past research has isolated various OPD predictive factors, including old age, malnutrition, dementia, stroke, and prolonged intubation [2;10]. According to [11], OPD is common across a range of neurological etiologies, such as spinal cord damage, head and neck cancer, traumatic brain injury, stroke, Parkinson’s disease, or as a result of respiratory illness or structural abnormalities such as COVID-19. Smithard et al. [12] point out that OPD affects 50% of patients with stroke across Australia and England, with about 60% of them within an acute facility (ACF). It is also known that OPD is a geriatric syndrome [13]. Age-related reduction in muscular mass and strength may exacerbate physiological changes in swallowing function in older, healthy persons, aggravating OPD from illnesses. Besides, OPD is a key risk for people with dementia [13].
Health professionals dealing with OPD patients should be aware of the associated risk factors. Their ability to identify OPD-related exposures is vital in early identification and intervention [14]. Besides, when HPs are aware of OPD risk factors, they are likely to participate actively in swallowing therapy, leading to improved clinical outcomes for patients with or at risk of having this condition. In contrast, minimal or lack of awareness of OPD risk factors among healthcare providers may impede their involvement in OPD management, leading to poor health outcomes for patients with swallowing disorders [15,16].
Given the role of awareness in OPD management, it raises concerns that in several countries globally, many HPs have low OPD awareness levels [17,18,19,20]. Limited dysphagia awareness among HPs is, in turn, associated with low readiness to administer treatment to OPD patients or actively engage in other swallowing disorder management aspects. In Kenya, over 70% of stroke patients are at risk of developing swallowing problems [16]. Although dysphagia screening has increased considerably during the past two decades, few nurses screen patients for this condition [16]. A key factor for nurses’ low involvement in OPD management in the country is that many assume that OPD screening is the role of physicians [15,16,21]. Such observations bring into question the level of dysphagia awareness among nurses and, by extension, other HPs in the country. However, there is limited research on swallowing disorder awareness among practitioners working in various clinical settings in the country. Additional research in this area may offer valuable information needed to develop effective OPD interventions.
Here, this study reports, for the first time, OPD risk factor awareness among HPs in the medical and surgical wards (acute-care facility) of a Kenyan level-six hospital. The study draws on the IPC model, which emphasizes a multi-disciplinary approach to OPD management. Improved OPD awareness levels are critical for successful collaboration.
B. Statement of the Problem
Given the complex nature of swallowing disorders, their effective management requires high-level collaboration between HPs in different specialties, including SLTs, medical officers, nurses, nutritionists, and other professionals. Such cooperation, in turn, calls on all HPs to have high awareness levels of various OPD aspects, specifically its risk factors. Some studies have reported low involvement of nurses and other HPs in swallowing disorder management in Kenya [15,16,21]. Their low involvement may be partly due to low dysphagia awareness levels [17,18,20]. However, there is limited research on dysphagia awareness among practitioners working in various clinical settings in Kenya. This gap may hinder the development of effective interventions to improve the clinical outcomes of persons with this condition.
C. Research Aim and Question
To address these gaps, we assessed OPD awareness levels among HPs attending to adult inpatients in the acute-care (ACF) facility of a level-six (national) hospital in Kenya. Specifically, we answered the following question: what is the current status of HPs’ identification levels of OPD risk factors among inpatients in the ACF of a Kenyan level-six national hospital? We use the term “identification level” to denote HPs’ ability to identify or recognize OPD risk factors from a set of possible risk factors, some of which may not apply to dysphagia. This ability is a critical component of OPD risk factor awareness. Our findings emphasize the need for increased training on OPD risk factors among the hospital’s HPs.
RESEARCH METHODS
This research is part of a larger study to establish HPs’ awareness and involvement in OPD management in Kenyan hospitals. We employed a descriptive, cross-sectional design to generate comprehensive data on the state of OPD awareness levels among individual HPs with varied characteristics. We used participants’ identification levels as a proxy for their awareness. Identification level was defined as the ability to recognize OPD risk factors from a set of possible risk factors, some of which may not apply to dysphagia.
The study’s setting was the medical and surgical wards of a leading level-six hospital in Nairobi City County, Kenya. Archival records obtained from the hospital and examined from July–December 2021 showed high inpatient SLT consultations and a relatively high OPD presence among inpatients in its medical and surgical wards [22]. Yet, prior to the current research, no study had assessed dysphagia awareness levels among HPs in the facility. We utilized a purposive technique to sample 19 individuals from a target population of 63 HPs (n = 30% of N) attending to adult inpatients in the hospital’s ACF [23]. Of the 19 HPs, 16 completed and returned the questionnaires, translating into an 84.2% return rate, which was considered adequate [23].
Participants were sampled proportionately from the six different specialties (work units) in the ACF: physiotherapists, nurses, nutritionists, SLTs, neurologists, and oncologists (Table I). The last four had one representative in each case and are indicate in the table under the “other” category. The sample had an equal number (n = 8) of male and female participants, while 62.5% (n = 10) were aged between 31-40 years. All had been in their profession for at least four (4) years, with 68.8% (n = 11) having been practicing for over six (6) years. The majority (75.0%, n = 12) had at least a bachelor’s degree.
Participants were also asked to indicate if they had ever observed or had to use another a language other than Kiswahili or English with an inpatient to facilitate swallowing during feeding, whether an SLT was present in their unit, whether they had attended a swallowing disorder training program, whether they were satisfied with dysphagia training in their facility or wanted more training, and whether they had access to OPD educational resources.
TABLE I. Participant Characteristics
| Characteristic | Category | n | % |
| Gender | Male | 8 | 50.0 |
| Female | 8 | 50.0 | |
| Age group | 25-30 years | 6 | 37.5 |
| 31-35 years | 5 | 31.3 | |
| 36-40 years | 5 | 31.3 | |
| Educational attainment | Diploma | 4 | 25.0 |
| Bachelor | 8 | 50.0 | |
| Post-graduate | 4 | 25.0 | |
| Experience | 4-6 years | 5 | 31.3 |
| 7-9 years | 5 | 31.3 | |
| > 9 years | 6 | 37.5 | |
| Specialization | Physiotherapist | 7 | 43.8 |
| Nurse | 5 | 31.3 | |
| Other | 4 | 25.0 | |
| Used another language? | No | 1 | 6.3 |
| Yes | 15 | 93.8 | |
| Pathologist present | No | 1 | 6.3 |
| Yes | 15 | 93.8 | |
| Swallowing disorder training | No | 10 | 62.5 |
| Yes | 6 | 37.5 | |
| Want training | No | 1 | 6.3 |
| Yes | 15 | 93.8 | |
| Satisfied with training | No | 11 | 68.8 |
| Yes | 5 | 31.3 | |
| Access to resources | No | 11 | 68.8 |
| Yes | 5 | 31.3 |
We adopted a previously validated questionnaire to generate data on participants’ risk factor identification levels [24,25]. They were distributed to participants online through Google Forms following approvals and formal consent from the Kenya National Commission for Science Technology and Innovation (NACOSTI), and the Kenyatta University’s Ethics Review Committee (KU-ERC). The questionnaire had nine (9) risk factors. Participants were to isolate the ones that applied to OPD from the set. Identification levels were computed based on the number of correctly identified items. Raw frequencies, percentages, and means were used to summarize the identification levels, while the independent samples t-test and one-way ANOVA were used to assess cross-sectional differences in awareness levels based on participants’ characteristics. The study complied with the ethical guidelines outlined by Kenyatta University’s ethics review committee.
RESULTS
A. Results on Risk Factor Awareness Levels
We conducted three sets of statistical analyses. Firstly, we used descriptive summaries to establish key patterns in participants’ OPD risk factor identification levels. Respondents were first presented with nine (9) disorder risk factors. They were to identify the ones that applied to OPD from the list. Table II displays their responses to the nine items.
All participants identified cancer (head and neck) and trauma (intubation injury, inhalation burn) as OPD risk factors. The other most selected factors were neurological conditions, head/neck surgery, and TBI. In each case, 87.5% (n = 14) isolated the three as OPD risk factors.
We then isolated correct answers from the responses. On average, each participant answered correctly to 73.6% (SD = 17.14) of the nine items. We employed the following system to classify identification levels: 0–25% = very low, 26-50% = low, 51-75% = moderate, and > 75% = high awareness. Based on this scheme, the sample had, on average, moderate identification level of OPD risk factors. Fig. 1 further shows that 56.3% (n = 9) had low or moderate OPD risk factor identification scores. Only 43.8% (n = 7) had high identification levels, while none had very-low scores. Only 18.8% (n = 3) responded to all the items correctly, while the lowest score was only 44.4%.
We also computed aggregate scores in each risk factor item. The results are in Table III. Five (5) items (neurological conditions, head/neck surgery, traumatic brain injury, head/neck cancer, and trauma due to intubation injury/inhalation burn) were marked correctly by over 75% of the HPs. Hence, identification levels of these factors were considered high. Lowest scores were for COVID-19, Parkinson’s disease, and Alzheimer’s disease/dementia. Although these three are OPD risk factors, only 37.5% (n = 6), 43.8% (n = 7), and 50.0% (n = 8) considered COVID-19, Parkinson’s disease, and Alzheimer’s disease/dementia, respectively, as such.
TABLE II. RESPONSES TO RISK FACTOR AWARENESS ITEMS
| Risk Factor | No, n (%) | Yes, n (%) |
| Neurological (stroke, cerebral palsy) | 2 (12.5) | 14 (87.5) |
| Surgical (head and neck surgery) | 2 (12.5) | 14 (87.5) |
| Traumatic brain injury | 2 (12.5) | 14 (87.5) |
| Alzheimer’s disease/dementia | 8 (50.0) | 8 (50.0) |
| Parkinson’s disease | 9 (56.3) | 7 (43.8) |
| Oncology (head and neck cancer) | 0 (0.0) | 16 (100) |
| Trauma (intubation injury, inhalation burn) | 0 (0.0) | 16 (100) |
| COVID-19 | 10 (62.5) | 6 (37.5) |
| Respiratory issues | 5 (31.3) | 11 (68.8) |
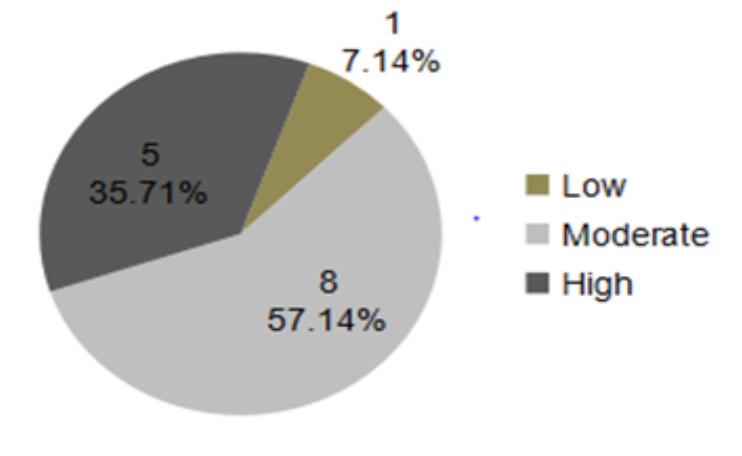
Fig 1. Awareness levels (low, moderate, or high)
B. Association between Risk Identification Levels and Selected Individual Characteristics
We also compared risk factor identification levels across participant categories. The Shapiro-Wilk test showed that the identification scores were normally distributed (SW = .911, p = .120), allowing us to use of parametric tests for the comparisons. Specifically, independent samples t-tests and one-way ANOVA were used as appropriate. The results were as shown in Table IV. Levene’s test indicated that all the models had significant homogeneity in their variances.
The differences in OPD risk factor identification levels due to gender and training were non-significant at the 95% confidence level (p > .050). There was a significant difference in risk factor awareness levels due to age (F = 4.67, p = .030). The mean scores indicated that, on average, the highest identification levels were among those aged 31-35, while the other two age groups had near-equal risk factor awareness levels. Post-hoc tests using Tukey’s HSD showed that the mean scores were significantly different between age groups 25-30 and 31-35 years (p = .030). The other differences were not statistically significant at the 95% confidence level. Thus, there was no definite pattern in differences in risk factor awareness levels due to age.
TABLE III. NUMBER (%) OF CORRECT RESPONSES
| Risk Factor | n | % |
| Neurological (stroke, cerebral palsy) | 14 | 87.5 |
| Surgical (head and neck surgery) | 14 | 87.5 |
| Traumatic brain injury | 14 | 87.5 |
| Alzheimer’s disease/dementia | 8 | 50.0 |
| Parkinson’s disease | 7 | 43.8 |
| Oncology (head and neck cancer) | 16 | 100 |
| Trauma (intubation injury, inhalation burn) | 16 | 100 |
| COVID-19 | 6 | 37.5 |
| Respiratory issues | 11 | 68.8 |
There was a significant difference in risk factor identification levels due to educational attainment (F = 5.94, p = .015). The mean scores suggested that, on average, identification levels increased with educational attainment. Participants with a post-graduate degree and a diploma certificate had the highest and lowest mean scores, respectively. Post-hoc comparisons revealed that only post-graduates and diploma certificate holders had a significant difference in their mean risk factor awareness scores (p = .014). The other differences were non-significant at the 95% confidence level.
There was a significant difference in risk factor awareness levels due to work experience (F = 5.34, p = .020). Mean score comparisons indicated that, on average, participants who had been in the healthcare professions for 7-9 years had the highest risk factor awareness levels, while those with a 4–6-year experience had the lowest scores (Table 4.7). Post-hoc tests indicated that HPs with a 7–9-year experience had, on average, significantly higher awareness levels than those who had worked for 4-6 years (p = .019). The other differences between the other experience pairs were non-significant (p > .050).
Finally, there was a significant difference in risk factor awareness levels due to specialization areas (F = 5.06, p = .024). From the mean scores (Table 4.8), HPs in the “other” category had, on average, higher risk factor awareness levels than those in the other groups. Nurses attained the lowest scores, although the nurse-physiotherapist awareness margin was narrow. Post-hoc comparisons confirmed that HPs in the “other” category had, on average, significantly higher risk factor awareness than both nurses (p = .025) and physiotherapists (p = .050). The risk factor awareness
TABLE IV. RISK FACTOR IDENTIFICATION LEVELS BY PARTICIPANTS’ CHARACTERISTICS
| Factor | Category | n | M | SD | t/F | p |
| Gender | Male | 8 | 73.61 | 13.196 | 0.00 | 1.000 |
| Female | 8 | 73.61 | 20.521 | |||
| Age group (years) | 25-30 | 6 | 64.82 | 10.927 | 4.67 | .030 |
| 31-35 | 5 | 88.89 | 11.110 | |||
| 36-40 | 5 | 68.89 | 18.256 | |||
| Education | Diploma | 4 | 61.11 | 11.115 | 5.94 | .015 |
| Bachelor | 8 | 70.84 | 11.784 | |||
| Post | 4 | 91.67 | 16.665 | |||
| Experience | 4-6 years | 5 | 62.22 | 9.942 | 5.34 | .020 |
| 7-9 years | 5 | 88.89 | 11.110 | |||
| > 9 years | 6 | 70.37 | 16.727 | |||
| Specialization | Nurse | 5 | 64.44 | 12.174 | 5.00 | .024 |
| Physio-therapist | 7 | 69.84 | 12.362 | |||
| Other | 4 | 91.67 | 16.665 | |||
| Training | No | 10 | 72.22 | 15.931 | -0.418 | .682 |
| Yes | 6 | 75.93 | 19.136 |
TABLE V. MIXED FACTOR MODEL FOR THE EFFECT OF PARTICIPANT CHARACTERISTICS
| Model | β | SE | t | p | LCL | UCL | PES |
| Intercept | 11.11 | 549.97 | 0.020 | 0.987 | -6976.95 | 6999.17 | < .001 |
| [Age=25-30 years] | -11.11 | 189.54 | -0.059 | 0.963 | -2419.46 | 2397.24 | < .001 |
| [Age=31-35 years] | -< .001 | 164.80 | 0.000 | 1.000 | -2094.04 | 2094.04 | < .001 |
| [Gender=Male] | 22.22 | 99.38 | 0.224 | 0.860 | -1240.53 | 1284.98 | 0.048 |
| [Specialization=Nurse] | -44.44 | 38.49 | -1.155 | 0.454 | -533.51 | 444.62 | 0.571 |
| [Specialization=Physio-therapist] | -22.22 | 49.69 | -0.447 | 0.732 | -653.60 | 609.15 | 0.167 |
| [Experience=4-6 years] | 22.22 | 111.11 | 0.200 | 0.874 | -1389.58 | 1434.02 | 0.038 |
| [Experience=7-9 years] | 33.33 | 108.87 | 0.306 | 0.811 | -1349.94 | 1416.61 | 0.086 |
| [Education=Diploma] | 22.22 | 110.55 | 0.201 | 0.874 | -1382.50 | 1426.95 | 0.039 |
| [Education=Bachelor] | -11.11 | 31.43 | -0.354 | 0.784 | -410.43 | 388.21 | 0.111 |
| [Training = No] | -< .001 | 49.69 | 0.000 | 1.000 | -631.38 | 631.38 | < .001 |
| [Resources=Yes] | -< .001 | 117.59 | 0.000 | 1.000 | -1494.11 | 1494.11 | < .001 |
difference between nurses and physiotherapists was non-significant (p = .775).
For further analyses, a mixed-factor univariate model was tested for the effect of each factor while controlling for the others. The results are in Table V. In addition to the factors assessed in Table IV, the model also accounts for the effects of access to OPD educational resources.
The table shows model coefficients (β), the corresponding t-values, confidence levels, p-values, and partial eta squared (PES) values. From the p-values, none of the coefficients was significant at the 95% confidence level. Hence, the effects of these variables were non-significant after controlling for other factors.
DISCUSSION
We analyzed responses from 16 HPs attending to adult inpatients in the ACF of a leading level-six hospital in Kenya to establish their identification levels of OPD risk factors. The majority of the participants were well-educated and experienced practitioners. Besides, all worked in professions that required them to interact regularly with OPD patients. Hence, they were expected to have high awareness and involvement in OPD management. However, their responses to the questionnaire items suggested that they had, on average, only moderate OPD risk factor identification levels. Only about a third (35.71%, n=5) had high identification levels (Fig. 1).
The IPC model’s emphasis on a multi-disciplinary approach to the management of complex health issues requires all HPs in clinical settings to have adequate OPD awareness levels. However, the present findings suggest that for the hospital in this study, many HPs in its medical and surgical wards have either low or moderate awareness of OPD, specifically its risk factors. These findings are comparable to those reported elsewhere [17,18,19,20]. These results highlight the need for increased awareness of OPD risk factors among HPs attending to patients in the ACF. Minimal identification levels of OPD risk factors may make it challenging for HPs at the facility to isolate and minimize patients’ exposures to OPD [15]. They may also lead to missed referrals, ineffective treatments, and increased complications [5]. There is a need for the management to create dysphagia risk factor awareness among the facility’s HPs.
The majority, and in some cases, the participants selected five of the nine questionnaire items as OPD risk factors.The least-selected items were COVID-19 and Parkinson’s disease. COVID-19 has been shown to be a leading risk factor for swallowing disorders [26]. From the records accessed by the researcher before the study, 7% of initial OPD diagnoses in the facility had COVID-19 [22]. Hence, we expected that participants would easily select COVID-19 as an OPD risk factor. However, only a small proportion of the respondents selected this item.
At least two factors could account for this unexpected finding. Firstly, it could be that due to the low presence of COVID-19 among OPD patients in the facility (7%), many HPs did not consider it a risk factor for swallowing complications. Another possibility is that many HPs in the sample were not actively involved in OPD management. In that case, it would be hard for them to know all OPD risk factors, especially those occurring in low proportions. This latter possibility is highly plausible considering the relatively low OPD awareness among the HPs in the sample. Irrespective of the reason, the present results show that HPs in the facility have varied views on what constitutes OPD risk factors.
Given the relatively low risk factor awareness levels observed in this study, it is not surprising that the analysis also revealed inadequate OPD training opportunities for HPs in the hospital’s medical and surgical wards (Table I). Only a slight majority (62.5%, n = 10) had attended a training course, workshop, or any education on swallowing disorders since joining the hospital. Less than a third, however, were satisfied with the training received, suggesting that even some who had been part of a training program were not content with the training they received. A possible reason could be that the training did not meet their needs. In that case, HPs may have low motivation to participate in such programs [27]. In either case, these results are consistent with findings from various parts of the world indicating that many HPs do not receive training or are inadequately trained on dysphagia management [8,28,29].
The IPC model emphasizes ongoing HP training (WHO, 2010). Regular training equips HPs with the knowledge and skills to manage OPD (Samuriwo, 2022). Besides, research shows regular training is a vital predictor of HP’s involvement and participation in OPD management [29,30]. Adequate training also prepares HPs to screen patients effectively for OPD and make appropriate referrals [29]. The inadequate training opportunities reported in this study may suggest that many HPs in the hospital’s ACF are inadequately prepared to handle OPD patients. Low OPD training may also indicate that many OPD inpatients admitted in the facility are at risk of going unidentified and missing timely referral or treatment opportunities.
On a positive note, the majority (93.8%, n = 15) stated that they would want additional training (Table I). This finding further confirms the low training opportunities at the facility. However, it also reveals a high willingness to participate in training programs. The hospital’s management could capitalize on this willingness and implement regular training programs. Notably, although training was expected to produce improved OPD risk factor awareness [31], the results indicated otherwise (Table IV). This unanticipated finding may be due to sample bias but may also imply that existing training programs were not as effective as expected.
When asked if they had ever observed or had to use another language with an inpatient other than Kiswahili or English when dealing with a patient with swallowing difficulties, the majority (93.8%, n = 14) were affirmative (Table 1). The implication is that working with OPD inpatients in the hospital’s medical and surgical wards requires HPs to have high cultural awareness and, if needed, have a translator to minimize misinformation or misinterpretations that may arise due to language or cultural differences [13].
The findings in Table IV suggested that, on average, OPD risk factor identification levels increased with educational attainment, and was highest among post-graduates. A post-graduate degree instills increased ability and confidence in HPs and enhances their understanding and application of specialty-related evidence [32]. This observation may explain the high awareness levels of OPD risk factors among post-graduates in this sample.
The findings on work experience were also against our expectations. Although past research suggests that increased work experience improves HPs’ knowledge and awareness [29,30], we could not verify this hypothesis. Instead, participants with 7–9 years of experience had, on average, better OPD risk factor awareness than those with longer experiences. It was beyond our scope to explore the reason for this inconsistency. In addition to sampling bias, factors not controlled, such as participants’ involvement with OPD patients, may explain the discrepancy.
Finally, individuals in the “other” specialization category had the highest OPD risk factor identification levels. The difference in awareness levels due to specialties may be explained by the degree of contact with OPD patients. Specifically, HPs who interact frequently with OPD patients are likely to have high awareness of this disorder [8]. The “other” category, included an SLT, who is expected to interact frequently with OPD patients. Hence, they were expected to have relatively high swallowing disorder awareness. In either case, the present findings may help the hospital’s management determine the areas to emphasize when designing interventions to improve OPD awareness among HPs.
CONCLUSIONS
HPs working in this facility had, on average, only moderate identification levels of OPD risk factors. Mean comparisons across different participant categories indicated that, on average, risk factor identification scores increased with educational attainment. The highest and lowest identification levels were among post-graduates and diploma certificate holders, respectively. Regarding their specialization, participants in the “other” category, which included neurologists, oncologists, nutritionists, and SLTs
on average, had higher risk factor awareness than nurses and physiotherapists. The differences in OPD risk factor identification levels due to gender, age, experience, and training were either inconsistent or non-significant.
Two (2) main conclusions can be drawn from the findings. Firstly, HPs attending to inpatients in the hospitals’ medical and surgical units have, on average, moderate identification levels of OPD risk factors. Secondly, high educational attainment is associated with increased identification levels of OPD risk factors.The management should consider developing strategies to increase OPD awareness among the hospital’s HPs.
A major limitation of this study was its relatively small sample size. Nevertheless, the sample was sufficiently representative of the target population. Additionally, the study was descriptive and did not control for other factors that could influence HPs’ knowledge or awareness of OPD risk factors. The limitations notwithstanding, the findings offer valuable insights into the state of OPD awareness among HPs in the hospital. Future studies could attempt to replicate the results using highly controlled designs.
ACKNOWLEDGMENT
The authors are humbled by the health professionals who provided valuable data in the study.
REFERENCES
- J. A. Cichero, S. Heaton, and L. Bassett, “Triaging dysphagia: Nurse screening for dysphagia in an acute hospital. J. Clin. Nurs., vol. 18, pp. 1649–1659, June 2009.
- F. Rajati, N. Ahmadi, Z. Naghibzadeh, and M. Kazeminia, “The global prevalence of oropharyngeal dysphagia in different populations: a systematic review and meta-analysis,” J. Transl. Med., vol. 20, pp. 175-187, April 2022.
- S. Attrill, S. White, J. Murray, et al., “Impact of oropharyngeal dysphagia on healthcare cost and length of stay in hospital: A systematic review,” BMC Health Serv. Res., vol. 8, pp.594-609, August 2018.
- D. A. Patel, S. Krishnaswami, E. Steger et al., “Economic and survival burden of dysphagia among inpatients in the United States,” Dis. Esophagus., vol. 31, pp. 1-17, January 2018.
- J. Bakhtiyari, R. Ghorbani, M. Salmani, et al., “Physicians’ perspective on a multidisciplinary approach to dysphagia management,” Iran. J. Otorhinolaryngol., vol. 31, pp. 141-146, May 2019.
- K. Dondorf, R. Fabus, and A.K. Ghassemi, “The interprofessional collaboration between nurses and speech-language pathologists working with patients diagnosed with dysphagia in skilled nursing facilities,” J. Nurs. Educ. Pract., vol. 6, pp. 17-20, Dec. 2015.
- World Health Organization. Framework for action on interprofessional education and collaborative practice. Available at: https://interprofessional.global/wp-content/uploads/2019/11/WHO-2010-Framework-for-Action-on-Interprofessional-Education-and-Collaborative-Practice.pdf
- A. F. Hady, H.M. Farag, and A.R. Sheikhany, “The awareness and knowledge of dysphagia among health care practitioners in Egypt,” Egypt. J. Otolaryngol., vol. 39, pp. 1-16, January 2023.
- S. Reeves, F. Pelone, R. Harrison et al., “Interprofessional collaboration to improve professional practice and healthcare outcomes,” The Cochrane Data. Syst. Rev., vol. 6, p. Cd000072.
- T. M. Almeida, L.M. Gomes, D. Afonso et al., “Risk factors for oropharyngeal dysphagia in cardiovascular diseases,” J. Appl. Oral Sci., vol. 28, e20190489, May 2020.
- M. C Rivelsrud, L. Hartelius, L. Bergström, M. Løvstad, and R. Speyer, “Prevalence of oropharyngeal dysphagia in adults in different healthcare settings: A systematic review and meta-analyses. Dysphagia, vol. 38, pp. 76-121, February 2023.
- D. Smithard, N. Smeeton, and C. Wolfe, “Long-term outcome after stroke: Does dysphagia matter?” Age Ageing, vol. 36, pp. 90-94, January 2007.
- K. Alagiakrishnan, R.A. Bhanji, and M. Kurian, “Evaluation and management of oropharyngeal dysphagia in different types of dementia: A systematic review,” Arch. Gerontol. Geriatr., vol. 56, pp.1-9, May 2012.
- K. Yao, L. Wang, and L. Zhang, “Awareness of dysphagia-related complications and risks and the importance of early intervention in patients with Parkinson’s disease: A qualitative study,” Int. J. Clin. Pract.,vol., pp. 95-114, March 2023.
- C. O. Oduor, A. Keter, L.O. Diero et al. “Stroke types, risk factors, quality of care and outcomes at a referral hospital in western Kenya,” East Africa Med. J., vol. 92, pp. 324-332, October 2015.
- G. Omondi, A quality audit on the management of acute ischaemic stroke at Kenyatta National Hospital (unpublished Thesis). Nairobi: Kenyatta University, 2010.
- K. Knight, B. Pillay, J. van der Linde and E. Krüger, “Nurses’ knowledge of stroke-related oropharyngeal dysphagia in the eastern Cape, South Africa,” S. Afric. J. Comm. Dis., vol. 67, pp. 703-713, September 2020.
- E. Sánchez-Sánchez, Y. Avellaneda-López, E. García-Marín, et al., “Knowledge and practice of health professionals in the management of dysphagia,” Int. J. Environ. Res. Public Health, vol. 18, pp. 2139-49, February 2021.
- T. A. Obembe, A.M. Adebayo, O.T. Ojo, and I.A. Adebayo, “Awareness and utilization of outpatient services among residents of Odno West local government area, Ondo State, Nigeria,” Ann. Afr. Med., vol. 16, no. 1, pp. 10-16, January 2017.
- M. A. Khan, M. Moazzam, and A. Shehzad, “Assessment of awareness among speech and language pathology regarding dysphagia” J. Allied Health Sci., vol. 6, pp. 3-8, April 2021.
- R. Martino, N. Foley, and S. Bhogal, “Dysphagia after stoke: incidence, diagnosis, and pulmonary complications,” Stroke, vol. 36, pp. 2756-63, November 2005.
- D. C. Ndiema, T. Abuom, M. Karia, “A descriptive retrospective review on the epidemiology of oropharyngeal dysphagia in the acute-care facility of a Kenyan (level-six) national hospital, ”IOSR J. Nurs. Health Sci., vol. 12, pp. 20-28, November-December 2023.
- A. Mugenda and O. Mugenda, Research methods: Quantitative and qualitative approaches, Nairobi: ACTS Press.
- A. Rhoda and A. Pickel-Voight, “Knowledge of nurses regarding dysphagia in patients post stroke In Namibia,” Curat.,vol. 38, pp. 1564-1571, November 2015.
- X. Yong, A. Affizal, and V. Malarvini, “Medical officers’ awareness, involvement, and training in dysphagia management,” J. Sains Kes. Mal., vol. 16, pp. 7-16, January 2018.
- A. Holdiman, N. Rogus-Pulia, M.S. Pulia, L. Stalter, and S.L. Thibeault, “Risk factors for dysphagia in patients hospitalized with COVID-19. Dysphagia, vol. 38, pp. 933–942, January 2023.
- J. Grossmeier, P.H. Castle, J.S. Pitts, C. Saringer, et al., “Workplace well-being factors that predict employee participation, health and medical cost impact, and perceived support,” Am. J. Health Promot., vol. 34, pp. 349-358, January 2020.
- P. Anderle, R.S. Rech, V.M. Pasqualeto, and B.N. de Goulart, “Knowledge of the medical and nursing teams about the management of oral medications in hospitalized adult dysphagic patients,” Audiol. Comm. Res., vol. 23, p. e1933, January 2018.
- J. Sivertsen, B. Graverholt, and B. Espehaug, “Dysphagia screening after acute stroke: A quality improvement project using criteria-based clinical audit,” BMC Nurs., vol. 16, pp. 1-8, June 2017.
- P. Andrea, Knowledge of nurses regarding dysphagia in patients with stroke (master’s thesis). Namibia, University of the Western Cape.
- H. Hussain, K. Ahmad, Z. Yahaya, S.E. Wan, and I.H. Mohd, “Level of awareness, knowledge, and involvement of Malaysian medical and dental practitioners in dysphagia management of head and neck cancer patients,” Dysphagia, vol. 37, pp. 856-862, August 2022.
- S. Holloway, A. Taylor, and M. Tombs, “Impact of postgraduate study on healthcare professionals’ academic and clinical practice. Br. J. Health Care Manag., vol. 26, pp. 171-178, July 2020.