
Proportion, Precipitators and Prognostic Marker of 30-Day Heart Failure Readmission at Moi Teaching and Referral Hospital, Eldoret, Kenya
- Gamar Bajaber
- Constantine Akwanalo
- Shameem Ali
- 110-125
- Nov 30, 2023
- Health And Cybersecurity
Proportion, Precipitators and Prognostic Marker of 30-Day Heart Failure Readmission at MOI Teaching and Referral Hospital, Eldoret, Kenya
Gamar Bajaber, Constantine Akwanalo, Shameem Ali
MOI University, Kenya
DOI: https://doi.org/10.51244/IJRSI.2023.1011008
Received: 13 October 2023; Accepted: 01 November 2023; Published: 30 November 2023
ABSTRACT
Background: Heart failure (HF) affects 26 million people globally. It is associated with a high 30-day readmission rate due to multiple cardiovascular and non-cardiovascular precipitants. Readmissions are associated with high mortality, which may be predicted by pre-discharge N-terminal pro brain natriuretic peptide (NT-proBNP). There is no data on HF readmission rates, its precipitators and use of NT-proBNP as a prognostic marker at Moi Teaching and Referral Hospital (MTRH) in Western Kenya.
Objective: To determine the 30-day proportion of HF readmission, the precipitators of HF and the association between NT-proBNP and 30 days’ readmission.
Methods:This was a six-month prospective cohort study where we carried out a census and recruited adult participants admitted with HF at Moi Teaching and Referral Hospital. At discharge from hospital, an interviewer administered questionnaire was administered and blood samples for NT-proBNP drawn. Upon readmission, precipitators for HF were identified and compliance to therapy assessed using European heart failure Self Care Behavioral Scale. Continuous variables were summarized using median and IQR, categorical variables using frequencies and percentages. Associations were determined using Chi square, Fishers exact and Wilcoxon rank test. A p-value of <0.05 was considered statistically significant.
Results: From April to November 2018, 94 participants were recruited into the study; with median age 48 years (IQR 31,70), 58 (62%) were female, 35 (38%) consumed alcohol and 25(25%) smoked. Hypertension was the commonest comorbidity 20 (21%) while cardiomyopathy was the underlying etiology for HF in 58 (63%). HF with reduced Ejection Fraction (HFrEF) was present in 76% of the participants while 24% had HF with preserved Ejection Fraction (HFpEF). Sixty percent of the participants had NT-proBNP levels of >4137 pg/ml, which implied poor prognosis. Of 17 readmitted patients, 12 participants (12.8%) were readmitted within 30 days at MTRH. Six (6.4%) participants were lost to follow up. Median time to readmission was 14 days, (IQR 7, 26). Pneumonia (55%) was the commonest precipitator of HF readmissions, followed by arrhythmias (atrial fibrillation) in 5 (42%), anemia 4 (33%), noncompliance 4 (33%), acute kidney injury 2 (16.6%) and no identified precipitator 1 (8.3%). There was no association between NT-proBNP and readmission (p =0.584) or NT-pro BNP and survival (p=0.773). Readmission was associated with a high mortality (p=0.008) with 50% of readmitted participants dying during the readmission period. The total mortality of both readmitted and non-readmitted participants was 16% at the end of the 6 months’ study period.
Conclusions:In this cohort of participants with HF the proportion of 30 days readmission was high. Infections, mainly pneumonia was the commonest precipitator of readmission. Discharge NT-proBNP did not predict likelihood of 30 days’ readmission. Mortality was higher among participants readmitted within 30 days.
Recommendations: Measures like pneumoccal vaccinations should be implemented to prevent pneumonia. Early appointments to cardiac clinic (less than 2 weeks post discharge) should be given to screen for precipitators and reduce HF readmissions. A follow up study to assess % change in NT pro BNP in relation to 30 days readmission.
INTRODUCTION
1.1 Background information
The American Heart Association (Yancy et al., 2017) defines HF as a complex clinical syndrome that results from any structural or functional impairment of ventricular filling or ejection of blood. The cardinal manifestations of HF are dyspnea and fatigue, which may limit exercise tolerance; and fluid retention, which may lead to pulmonary and/or splanchnic congestion and/or peripheral edema. Decompensated heart failure refers to the onset of symptoms in heart failure that was previously controlled(Yancy et al., 2013)
Heart failure affects 26 million people worldwide and in the United States (US) and Europe ,it is associated with more than 1 million hospitalizations annually (Khan et al., 2015); however, eighty percent of the HF burden lies in low and middle income countries (LMIC) (Damasceno et al., 2012). In the developed world, the prevalence of heart failure is estimated to be 13% (Damasceno et al., 2012); whereas in sub Saharan Africa (SSA) the pooled prevalence is about 39.5% (Agbor et al., 2018). In Kenya, data from a hospital based study estimates prevalence at 7.5%(Kamau, 2009).
Deaths from cardiovascular diseases have risen by 14.5% between 2006-2016 (GBD 2017). In SSA, heart failure is one of the major contributors to the burden of cardiovascular diseases, with non-ischemic causes being the commonest (Carlson et al., 2017). The attributable inhospital mortality rate for decompensated heart failure in SSA is estimated to be 8.3%(Kraus et al., 2016). Cumulatively the economic burden is projected to amount to a total of 70 billion USD by 2030 (Hammond et al., 2016)
HF readmissions are highly associated with mortality.This is seen in the study from KNH which showed an association between re-hospitalization and increased mortality risk of 30% (Kamau, 2009) A study conducted in USA Alabama by Cherinne et al.,showed that in patients readmitted within 30 days,all-cause mortality was at 41% in the readmitted group and 27% in the non-readmitted group within a 2 to 12 month follow up period.(Hazards ratio 1.89 pvalue< 0.001)(Arundel et al., 2016).
Worldwide, HF readmission rates within 3 to 6 months of discharge range between 27-47% (Michalsen, König and Thimme, 1998). The THESUS-HF survey estimated a 15% sixty day readmission rate for patients with decompensated HF in sub-Saharan Africa (Damasceno et al., 2012). However, readmission rates as high as 50% have been reported for patients with heart failure in Africa, with most readmissions occurring within 30 days post discharge (Hernandez et al., 2013). In SSA the limited published data that is available describes a readmission rate ranging between 13 -25 % (Agbor et al., 2018); whereas in Kenya, a KNH study found that 29.5% of HF patients were re-hospitalized once,6.2% re-hospitalized twice and 2.3% were re-hospitalized thrice.
There are several factors that predispose a patient to decompensated heart failure. These include; Cardio-Vascular (CV) causes such as treatment noncompliance (to drugs or diet), cardiac ischemia, cardiac arrhythmia, uncontrolled hypertension or worsening disease. Non-CV causes include; infections especially pneumonia, anemia, acute renal failure, and sometimes no identified factors (Fonarow et al., 2008)(Platz et al., 2018)(Michalsen, König and Thimme, 1998). In a Berlin study, non-compliance to medication was the most common precipitator of readmission (Michalsen, König and Thimme, 1998). Similarly, in a study conducted at the Muhimbili National Hospital in Tanzania, the most common predictor was also noncompliance (Maro and Makule, 2009).
The 30-day temporal threshold for assessing readmission related outcomes has important clinical significance, it is during this time bracket when HF related mortalities and future readmissions can be prevented through optimal in-hospital care of admitted cases.Thirty-day readmission is the timing of special interest because it is when, if readmitted and managed well, mortalities and future readmissions are preventable(Hernandez et al., 2013) and the economic burden associated with readmissions can be minimized(Arundel et al., 2016) .
Use of NT pro BNP in guiding treatment and prognosis can help reduce HF readmissions.NT pro BNP,a biomarker released from the cardiac ventricles,has been used for diagnostic and prognostic purposes as well as guiding treatment in heart failure patients.As a diagnostic marker it has a 94.5% sensitivity and 90.6% specificity (Lee-Lewandrowski et al., 2007). High NT-pro BNP levels are associated with an increase in all-cause mortality and readmissions (Bettencourt et al., 2004). Using NT-pro BNP to guide treatment can aid in reducing the HF related hospital readmissions and mortality.
Bettencourt and colleagues showed that discharge NT-proBNP value of 4137 pg/mL was a much stronger predictor of hazard, with an 8% increase in the likelihood for death or readmission over 6 months per 1000 pg/mL of NT-proBNP over this threshold (P<.0001)(Januzzi et al., 2012).
Heart failure is a common diagnosis in our set up with observed high readmission rates, but no documentation to this effect. Readmission in heart failure is associated with increased morbidity and mortality, and increased cost of treatment. Additionally, there is limited data on the precipitators and frequency of readmission rates among patients with heart failure. Furthermore, use of discharge NT-pro BNP levels, a simple test that can be performed by the patient’s bedside, in predicting heart failure readmissions is unknown in our setting. This study will yield knowledge on proportion, precipitators and the association of discharge NT pro BNP as a prognostic marker of HF readmissions which may help during the development of strategies aimed at reducing HF associated readmissions, mortality and morbidity.
This study aimed at determining the precipitators of heart failure readmission, frequency of readmission and its association with mortality and utility of pre discharge NT-pro BNP in predicting the propensity for readmission during the care of heart failure patients in our setting.
METHODOLOGY
Study setting
This study was carried out at the medical inpatient wards (male and female) and Cardiac Care Unit (CCU) of Moi Teaching and Referral Hospital, Eldoret. MTRH is the second largest public referral hospital in Kenya with an 800-bed capacity. MTRH serves as a referral facility for western Kenya, some parts of Eastern Uganda, South Sudan and Tanzania. It has a catchment population of about 20.8 million.( (2019 Kenya Population and Housing Census Volume I: Population by County and Sub-County – Kenya National Bureau of Statistics, .). The hospital also serves as a teaching facility for medical undergraduate and post-graduate students. On average, the medical wards admit approximately 11 patients and CCU admits approximately 15 patients with heart failure in a month. This was based on recorded hospital data for the month July 2017.
Study population
All adult patients discharged after management for heart failure. These patients were followed up for readmission in MTRH medical wards and CCU within 30 days from the date of discharge.
Study design
This was a prospective cohort design.
Sampling technique
Census was implemented between April and November 2018.
Sample size
The aim of the study was to determine the proportion of participants readmitted due to heart failure within 30 days of discharge at MTRH. Data from the KNH study showed that among the patients treated and discharged due to heart failure, 29.5% were re-hospitalized once (Kamau, 2009).
To be 95% sure that we report the proportion of re-hospitalization within plus or minus 5% of the reported value at the KNH study, we determined the sample size using the following formula (Cochran, 1963).
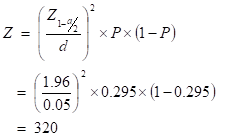
Where Zc is the quantile of the standard normal distribution corresponding to c x 100% percentile, c = (1-a/2), “a” is the type I error, d is the margin of error, and P is the proportion re-hospitalized due to heart failure.
Since this study had a 30 day follow up period, we anticipated that we will likely have loss to follow up participants. No study has reported this rate. Hence to protect our study from the possibility of ending up with a smaller sample size we inflate it by 10% as follows;
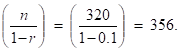
Data collection for this study was done over a period of 6 months. At MTRH, we anticipated up to 26 heart failure patients being discharged every month. This gave us approximately 156 HF patients over the period of data collection. The 156 patients included those with cor pulmonale as the hospital records pools them under heart failure diagnosis. 156 patients were less than the calculated sample size.
For the explorative association in objective 3, there were two independent variables, mortality and readmission. Using Peduzzis formula,
n = ![]() where k is the number of indendent variables, which is 2,p is the proportion of rehospitalisation from KNH ,29.5%. n for the associations objective was 67.7, with a 10% anticipated loss to follow up, n=74.
where k is the number of indendent variables, which is 2,p is the proportion of rehospitalisation from KNH ,29.5%. n for the associations objective was 67.7, with a 10% anticipated loss to follow up, n=74.
Since both calculated sample sizes were less than 356 as per fishers formula, a census was conducted within the six months’ period of April to November 2018.
Eligibility criteria
Inclusion Criteria
- All Patients discharged after management for heart failure
- All patients above 18 years of age who consented
Exclusion Criteria
- Pregnant women.
- End Stage Renal Disease
- Underlying active malignancy / on chemotherapy
- Immobility from stroke, fractures
- Participants with Chronic Obstructive Pulmonary Disease and asthma, pulmonary embolism and/or Cor Pulmonale
Recruitment procedure
From the 20th of April 2018 to 20th October 2018, participants were identified on a daily basis, i.e. heart failure patients in the medical wards and CCU of MTRH; among the identified cohort of patients, I consecutively approached those who fulfilled the eligibility criteria for consenting. These were patients who had been deemed clinically fit for discharge by the primary physician. All patients who consented to be part of the study were recruited into the study at the time of discharge and assigned a unique study identification number.Study was completed at the end of November 2018 as a follow up of participants discharged in October 2018.
Study procedure
Immediately after recruitment, all participants were interviewed by the primary investigator using an interviewer administered questionnaire. This initial questionnaire which was administered at the time of recruitment was used to obtain socio-demographic, clinical, medication history, laboratory parameters, Echo findings, etiology of heart failure, NT-Pro BNP levels, discharge medications and the date of discharge.
The date of discharge and dates corresponding to day 15 and day 30 post-discharge, were also recorded in a virtual ledger. Calendar reminders corresponding to these dates were then set so as to facilitate timely follow-up of participants when assessing for readmission and mortality.
At days 15 and 30 after discharge, participants were followed up by phone to check if they got readmitted to hospital due to heart failure. These time periods were purposefully selected so as to coincide with the 2-week and 1-month cardiac clinic follow up appointment schedules routinely given to patients at the time of discharge. In addition to follow up by phone, we also sought out for participants who were readmitted within 30 days of discharge from hospital during our daily ward and CCU surveillance.
For all the readmitted participants in decompensated HF, we administered a second questionnaire. This questionnaire assessed for presence/absence of precipitators which were not present at index discharge and led to decompensation. echocardiography, ECG, chest x-ray and laboratory findings were recorded in this questionnaire.
When seeking out for precipitators of heart failure, we only sought out for seven specific precipitators as advised by previous published research papers which included: 1) anemia, 2) acute kidney injury, 3) infections, 4) arrhythmia either new or worsening prior arrythmia if the rate is >100, 5) acute coronary syndrome and 6) adherence to self-care behavior 7) Uncontrolled hypertension
Participants who were readmitted in another facility were recorded as readmitted, but precipitators could not be obtained due to ethical limitations at other facilities which are not under MTRH/Moi University IREC catchment.
Data Analysis and Interpretation
Data analysis was done using STATA version 15. NT pro-BNP levels on initial discharge was treated as an independent variable, heart failure readmissions, and mortality was treated as dependent variable. Categorical variables i.e. gender, NT pro BNP, HFrEF, HFpEF, discharge medications, were summarized using frequencies and percentages. Continuous variables i.e, age, time to readmission, duration of hospitalization, were summarized using median and IQR.Associations among dependent variables (like readmission, mortality) and independent variables like NT pro BNP was done using chi square /fishers exact/ wilcoxon rank sum test.
Approval was sought from MTRH/Moi University Institutional Research Ethics Committee (IREC) before the study commenced. Permission to conduct the study was also obtained from the management of Moi Teaching and Referral Hospital.
All the participants were notified about the purpose of the study and politely asked without any coercion to give a signed written informed consent before participating.
RESULTS
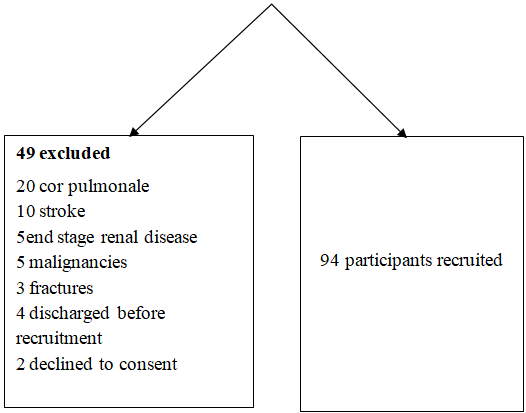
A total of 143 participants discharged with heart failure were screened between April and October 2018 and 49 were excluded.6 participants were lost to follow up.
4.1 Demographic Characteristics
Among the participants recruited, 36 (38.3%) were males with a median age of 48 (IQR 31,70). The participants level of education was mostly primary school level 44 (46.8%). Eleven (12%) were current smokers and 13 (13%) were current alcohol consumers.
4.2 Clinical characteristics
Table 1: Demographic characteristics of participants discharged from MTRH with heart failure
| Characteristic | Frequency n=94 |
| Median Age, (IQR) | 48 (31,70) |
| Female n (%) | 58 (61.7) |
| Level of Education n (%) | |
| None | 26 (28) |
| Primary | 44 (47) |
| Secondary | 20 (21) |
| Tertiary | 4 (4) |
| Social History n (%) | |
| Alcohol | 25 (38) |
| Smoking | 24(25) |
| Nonsmokers/nonAlcohol consumers | 45 (37) |
| Comorbidities n (%) | |
| Diabetes Mellitus | 8 (9) |
| Hypertension | 20 (21) |
| Dyslipidemia | 2 (2) |
| HIV positive | 5 (5) |
| No comorbidities | 64(63) |
| Diagnosis of heart failure in years’ n (%) newly diagnosed | 42(44.7) |
| 1-5 | 42(44.7) |
| 5-10 | 3(3.2) |
| 10 -15 | 5(5.3) |
| 15-20 | 2(2.1) |
Upon discharge (at recruitment), the mean duration of hospital stay for the participants was 11 days (IQR 6-13). The participants had a return visit to outpatient clinic scheduled within 2 weeks from date of discharge.
4.3 Etiology of Heart Failure
Among the participants, the most common documented causes of heart failure were cardiomyopathies, followed by rheumatic heart diseases as shown in graph 1 below.
*cardiomyopathies include restrictive cardiomyopathy 1, pacemaker induced cardiomyopathy 1, dilated cardiomyopathy 56 and HIV related cardiomyopathy 1. The classification of etiology of HF was based on that documented by the primary physician.
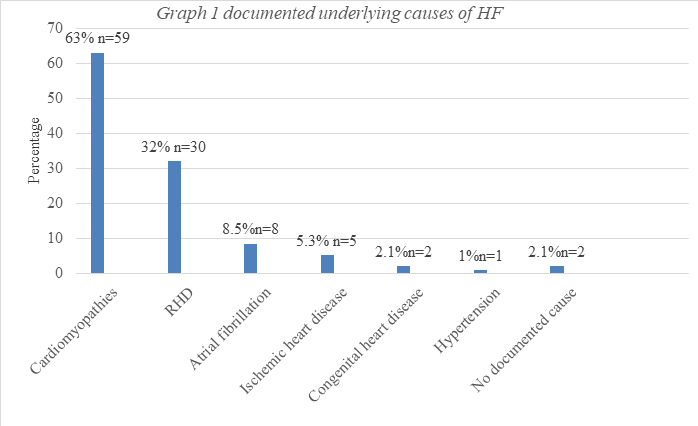
Figure 3: Graph showing documented underlying causes of HF
4.4 Laboratory Findings
Among the participants, the median creatinine level was 84 (IQR 64,103). All participants had a 2 dimensional echocardiography performed. Majority of the participants had heart failure with reduced ejection fraction (HFrEF) as shown in the table 2 below. The median pulmonary pressures were 62.5mmHg (IQR 50,76). Commonly prescribed medications at discharge were furosemide (lasix) and less frequently were beta blockers.
Table 2: Clinical characteristics of patients discharged with heart failure at MTRH
| Variable | Frequency/Median |
| Pulmonary pressure median (IQR) | 62.5 (50,76) |
| Ejection fraction n (%) | |
| HFpEF | 22 (23.4%) |
| HFrEF | 72 (76.6%) |
| NT pro BNP n (%) | |
| <20 | 10 (10.6%) |
| 20-15000 | 68 (72.3%) |
| >15000 | 16 (17%) |
| NT pro BNP (pg/ml) n (%) | |
| <4137 | 35(39.7) |
| >4137 | 53 (60.2) |
| Creatinine Median (IQR) | 84 (64,103) |
| Discharge Medication summary n (%) Diuretics: | |
| Lasix | 82 (87%) |
| Metolazone | 3 (0.03%) |
| spironolactone | 49 (52%) |
| Beta blockers | 35 (37.2%) |
| ACEI/ARB | 59 (62.8%) |
| Warfarin | 28 (29.8%) |
| Digoxin | 21 (22%) |
Table 3: Discharge clinical charachteristics of MTRH readmitted participants n=12
| Years since diagnosis | cut off NT pro BNP Pg/ml | Underlying etiology as per echo | Classification based on EF |
| 0-5 years 9 | >4137 5 | RHD 6 | HF r EF 9 |
| Newly diagnosed 3 | <4137 7 | DCM 5 | HF p EF 3 |
| Arrythmia 1 |
4.5 Proportion of 30 days’ readmission
Out of the 94 participants discharged with a diagnosis of heart failure, 17(18%) were readmitted within 30 days. Median time to readmission was 14 days IQR (7,26). Twelve (70.6%) of these 12 patients were readmitted at MTRH, a proportion of 12.8%,5 participants were readmitted in other facilities. We were unable to reach 6 participants on follow up.
Table 4: Clinical findings at readmission
| Variable | Median/ Freq | IQR |
| Systolic BP | 90.5 | 88.5, 108 |
| Diastolic BP | 60 | 55, 66.5 |
| Pulse | 101.5 | 91,123 |
| Spo2 | 93.5 | 91,95.5 |
| NYHA class | N | % |
| 2 | 1 | 8.33 |
| 3 | 2 | 16.67 |
| 4 | 9 | 75 |
| CVS risk score | N | % |
| 10 | 11 | 91.67 |
| 20 | 1 | 8.33 |
| Outcome after readmission | ||
| Died | 6 | 50 |
| Discharged Alive | 6 | 50 |
4.6. Common precipitators of readmission
The most common precipitator of readmission among participants readmitted to hospital was infections (92%), followed by arrythmias as shown in graph 2 below. Infections encompassed 55% (6) pneumonia, pulmonary TB 27% (3), urosepsis 8.3% (1), unknown source 8.3% (1). The type of arrhythmia observed was atrial fibrillation. ACS and uncontrolled hypertension 0 participants.
Graph 2. Precipitators of readmission in heart failure at MTRH
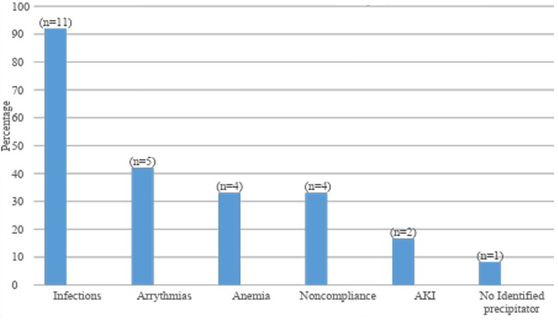
Figure 4: Precipitators of readmission in heart failure at MTRH
4.7 Association between NT-pro BNP levels and 30-day readmission at MTRH.
There was no statistically significant association between NT pro BNP and readmission (p-value 0.160) or mortality (p-value 0.728). From previous studies, a cut off NT pro BNP of 4137 has been associated with mortality and readmission. Therefore, to assess further whether there was an association, we used this NT pro BNP cut off in our analysis.
Among 55 (56%) participants with a discharge NT pro BNP of more than 4137 pg/ml, 4 (7.3%) were readmitted in MTRH. Out of the 39 participants who had NT pro BNP less than 4137, 8 (20.5%) got readmitted in MTRH within 30 days of discharge. Among the 12 patients readmitted at MTRH,4, (33.3%) had NT pro BNP more than 4137, and 8 (66.7%) had NT pro BNP less than 4137.There was also no association between NT pro BNP and duration of stay in the hospital prior to discharge (p-value 0.462), readmission or mortality as shown in Table 4 below.
Table 5: Association between discharge NT-pro BNP and readmission and mortality among patients with heart failure
| NT-Pro BNP (pg/ml) | Re-admission | P value | |
| Yes | No | 0.5841 | |
| <4137 | 8 (22.86) | 27 (77.14) | |
| >4137 | 9 (16.98) | 44 (83.02) | |
| Survival | |||
| Alive | Dead | 0.7731 | |
| <4137 | 30 (85.71) | 5 (14.29) | |
| >4137 | 43 (81.13) | 10 (18.87) | |
| Duration of stay in days | 9 (6,13) | 9 (6,21) | |
| Duration of stay and NT pro BNP | |||
| <4137 | >4137 |
0.104 2 |
|
| Duration of stay | 9 (6,16) | 5(8,13) | |
*1 Fishers’ exact 2 Wilcoxon rank sum test
We excluded 6 patients who were not reachable hence not possible to ascertain their readmission status.
4.8 Association between readmission and mortality
There was an association between readmission and mortality where mortality washigher among participants readmitted within 30 days (p 0.008) as shown in table 5 below.
Table 6. Association between readmission and mortality among patients readmitted with heart failure
| Readmission | Outcome | Fishers’ exact p-value | |
| Alive | Dead | ||
| No | 63 (88.73) | 8 (11.27) | 0.008 |
| Yes | 10 (58.82) | 7 (41.18) | |
4.9 Patients 30days Outcome
Out of the participants recruited, 73 (78%) were alive and 15 (16%) died by the end of30 days. Six (6%) participants were lost to follow up and thus their status was unknown. Out of the 12 participants readmitted within 30 days at MTRH, 6 (50%) died before discharge.
DISCUSSION
The mean age of the participants was 51 years and was almost similar to a study in KNH (Ogeng’o et al., 2014). These results are in agreement with Damasceno et al’s (Damasceno et al., 2012) findings, who reported that HF occurs 2 decades earlier in the black population than in Caucasians where it was found to occurr at a mean age of 72 years.. Similarly, Ponikowski et al also stated that in SSA, patients with heart failure are mostly below the age of 55 years (Ponikowski et al., 2014).This age disparity could be due to the varied regional causes of heart failure, where ischemic heart disease is the most common etiology in the developed countries, whereas cardiomyopathies (HIV associated and peripartum) and rheumatic heart diseases which have onset occur at much younger ages, are more prevalent in Africa.(Callender et al., 2014)
The education status of our participants was low with majority having primary school education at 47% and 28% had no previous education. This is almost similar to a study conducted in Muhimbili Hospital in Tanzania which reported that 53.6% participants had primary school education and 21% had no formal education (Maro and Makule, 2009). The level of education is important as it has been documented to contribute to noncompliance among HF patients increasing their likelihood for readmission (Kimani et al., 2016).This could be due to the fact that patients with higher literacy level have been found to have better health seeking behavior . A study conducted in Ethiopia however, found no association between level of education and HF behavior and treatment adherence ,but rather an association between HF knowledge and adherence.(Sewagegn and Fekadu, 2015)
The most common documented cause of heart failure in this study was cardiomyopathy at 58%. Similar findings have been previously reported from studies conducted in KNH and Muhimbili hospital in Tanzania (Ogeng’o et al., 2014)Maro & Makule, 2009). In 2016, Bloomfield et al, also found cardiomyopathy to be the most common etiologic entity underlying heart failure among patients admitted in MTRH (Bloomfield et al., 2016).
Our overall 30 days’ readmission rate was 18%. 12.8% of the participants were readmitted in MTRH, while others were readmitted in other hospitals. It was concluded to be a high readmission rate in comparison to THESUS-HF study(Damasceno et al., 2012) that had a 60-day readmission rate of 9.1%, vs 12.8% 30 days readmission in this study.
This was somewhat lower compared to proportions reported from other studies in the region. For instance; in a study done in KNH re-hospitalization rate was 49.2% but this was over a period of 12 weeks post-discharge as opposed to the 30 days which was assessed in this study. While the difference in proportions could be attributed to the time difference between these two studies, it could also be due to the fact that the study was conducted in 2009,currently there is improved management in terms of HF treatment (Kamau, 2009). Our readmission rate was similar to a study conducted by Michtalik et.al in John Hopkins Hospital, which was assessing changes in NT-pro BNP during hospitalization and risk of readmission and mortality in heart failure patients. The readmission rate was 13% after 30 days (Michtalik et al., 2011) . A post hoc analysis of the EVEREST Trial revealed a 30-day readmission rate of 5.7% (Khan et al., 2015). However, the EVEREST trial only looked at patients with HFrEF. OPTIMIZE HF study had a readmission rate of 29.6% in the 60-90 day follow up for outcomes (Fonarow et al., 2008) The difference in our rate vs OPTIMIZE-HF could be due to pooled data from multi-facilities in OPTIMIZE-HF, and the longer follow up period. We chose to assess 30 days’ readmission because several studies showed that most outcomes in heart failure occur within 30 days (Januzzi et al., 2012).
In this study, the most common precipitator of readmission was infections at 92%, with pneumonia (55%) being most common. This is similar to what has been reported from Muhimbili teaching hospital in Tanzania (Maro and Makule, 2009) where out of 97 patients admitted over a 6 months period, 62.9% were readmitted due to infections (pneumonia, PTB, malaria, HIV). Similarly, the CHARM study showed that among non cv precipitants reported, respiratory infections were the commonest (Platz et al., 2018). Furthermore, pneumonia was also the most common precipitator of readmission in the OPTIMIZE-HF study, albeit at much lower rates (15.3%). OPTIMIZE-HF was conducted across 259 US hospitals between years 2003 and 2004 (Fonarow et al., 2008). The difference in the proportions of infection between our study and the two other studies, is that our study looked at precipitators of readmission within 30 days of discharge, while the CHARM and OPTIMIZE studies looked at precipitators retrospectively at the point of admission hence introducing the possibility of precipitator ascertainment bias. Although healthcare associated infections are defined as infections that occur 48 hours or more after hospital admission or within 30 days after discharge from hospital (Haque et al., 2018) from our study we cannot deduce whether the pneumonia patients presented with at readmission was hospital /health care associated or community acquired. A systematic review done by Calvillo et al showed that community acquired pneumonia that precipitated HF readmissions was associated with social factors like low income and low education level. (Calvillo–King et al., 2013). If clinicians are aware of this, they can have closer follow up for such patients whom they will have identified as having high-risk social factors. If it is healthcare associated, then appropriate measures by the hospital including infection prevention measures should be put in to practice to reduce the risk of hospital acquired infections.
The second precipitator for readmission was arrhythmias, mainly atrial fibrillation 5 (42%). This was similar to data yielded from the CHARM study by Elke et al, where among cardiovascular precipitants, arrhythmias were the most common precipitator of readmission. In the Muhimbili study, 15% of cases had arrhythmia as precipitating factors for readmission.(Maro and Makule, 2009). In contrast, a study conducted by Michalsen et al done in a Berlin teaching hospital in Germany had only 28.7% of cases with arrhythmias (Michalsen, König and Thimme, 1998). This difference could be explained by the fact that our percentage of atrial fibrillation was from a thirty day follow up cohort of readmitted patients, while the study by Maro and Michalsen focused on patients admitted with acute decompensated heart failure and they determined the precipitators for that admission. In the OPTIMIZE-HF study, arrhythmias were 3rd listed precipitator of heart failure readmissions at 13.5% (Fonarow et al., 2008). The difference could be due to that in the OPTIMIZE HF study, patients were followed up for 60 to 90 days. It might be that the arrhythmias were captured and managed earlier without causing readmission/decompensation within the 90 days follow up.
Non- compliance as a precipitator was documented in 4 (33%) patients and only 1 patient had no identified precipitator. In the study by Michalsen et al 23.5% were reported to be noncompliant to medication(Michalsen, König and Thimme, 1998) . The difference in results between this study and ours could be explained by the fact that the study was a cross-sectional one, while ours was a cohort which determined precipitators of readmission within 30 days of discharge for 12 readmitted patients. The Berlin study by Michalsen looked for precipitators of decompensated heart failure at the point of admission in heart failure, while our study was a follow up for readmission within 30 days,and when readmitted, precipitators are sought. OPTIMIZE HF study showed non adherence to diet at 5.2% and to medication at 8.9%, while we assessed non-adherence of both medication and diet using one tool, the European heart failure self-care behavior score (Fonarow et al., 2008).Jaarsma et al concluded that the EHFSc-9 which is what we used in our study, as a valid international tool that can be used in research to assess factors related to HF adherence (Jaarsma et al., 2009). Mitchalsen determined noncompliance if a patient took >2.5 l of fluid, took meds intermittently or didn’t take meds at all,or if the patient took excess sodium.There was no scoring system in that study.
NT-pro BNP was not found to have any statistically significant association to 30-day readmission (p value=0.160) or 30-day mortality (p value=0.728).This could be due to the fact that we had a small number of paticipants. Cut-off NT-pro BNP of 4137 pg/ml was used to determine an association between discharge NT pro BNP and mortality (p value <0.0001). (Bettencourt et al., 2004). Although we were unable to assess percentage change in NT-pro-BNP levels in this study, our study findings show that high NT-pro-BNP levels are common in our patients upon discharge from hospital. Bettencourt et al associated readmission over 6 months to discharge and percentage changes in NTpro BNP and found an association between it and outcome i.e. death and readmission (Bettencourt et al., 2004),while our study was assessing readmission within 30 days .In comparison , a study done in Leicester showed, in multivariate analysis, that pre‐discharge plasma level of NT‐pro BNP (odds ratio 15.30 [95% CI: 1.4–168.9], P=0.026) remained independently predictive of the composite primary endpoint of readmission and death within 350 days (O’Brien et al., 2003). This greatly differed from our study because the Leicester study had a sample size of 96, and only 34 patients had both admission and discharge NT-pro BNP, and they also followed up patients for 350 days, unlike our study that was assessing readmission within 30 days.
The mortality rate at the end of the study period was 16%, which was similar to Maro et al study in Muhimbili (Maro and Makule, 2009). Similarly, a meta-analysis of HF in SSA showed a mortality rate ranging from 14.7 to 35% within 30 days of discharge (Agbor et al., 2018). An association was noted in the patients who were readmitted and mortality (p-value was 0.008). In our study, out of those participants who were readmitted, 7 died (41.2%). The study in KNH by Kamau et al proved that readmission increased mortality by 30% (Kamau, 2009).This was also similar to a study in Alabama by Arundel et al, which showed that patients readmitted within 30 days post discharge had a higher mortality risk within a year post readmission ,all-cause mortality was at 41% in the readmitted group and 27% in the non readmitted group within a 2 to 12 month follow up period.( Hazards ratio 1.89 pvalue< 0.001).(Arundel et al., 2016)This indicates that readmission increases mortality rate especially one year following discharge. A study in Taiwan by Tung et al showed that post 30 day readmission mortality was at 26% in the readmitted group vs
20% in the nonreadmitted group within a 6 month follow up period.(Tung et al., 2016)
The mortality rate in this study was considered to be high.THESUS-HF study had a 180 day mortality rate of 17.8% (Damasceno et al., 2012) vs our 30day mortality rate of 16%.
This study draws strength from the fact that it was a cohort study which involved following up patients for 30 days from discharge, after which readmission rates was calculated, and precipitators of HF readmission determined. 30 days readmission is a time of interest since risk of readmissions and mortalities increases up to a year after this readmission. We also were able to assess mortality within the 30 days of discharge. In addition, we were also able to determine and evaluate Pre discharge NT pro BNP which is commonly unavailable in our settings.
Study Limitations
The study employed use of a census strategy rather than a probabilistic sampling approach; as a result, capacity to make inference on the population is limited.
CONCLUSION AND RECOMMENDATION
6.1 Conclusion
- The total 30-day readmission proportion in heart failure discharges was high.
- Infections, mainly pneumonia, was the commonest precipitator of readmission in patients with heart failure.
- There was no association between pre-discharge NT-Pro BNP and 30 days readmission. Readmission was associated with a high 30-day mortality.
6.2 Recommendations
- Since NT-pro BNP did not predict 30-day HF readmissions, a follow up study can be carried out to assess percentage change in NT pro BNP (difference between NT pro BNP at admission and discharge) in relation to 30 days readmission.
- Measures e.g. pneumococcal vaccine should be given to heart failure patients to prevent This will help in reducing readmissions in HF.
- Since most readmissions occurred within 2 weeks of discharge, early return clinic visits for early assessment and identification of any precipitators will help reduce readmissions and hence mortality associated with readmission.
REFERENCES
- 2019 Kenya Population and Housing Census Volume I: Population by County and Sub-County – Kenya National Bureau of Statistics. Available at: https://www.knbs.or.ke/?wpdmpro=2019-kenya-population-and-housing-census-volume-i-population-by-county-and-sub-county (Accessed: 30 August 2020).
- Agbor, V. N. et al. (2018) ‘Heart failure in sub-Saharan Africa: A contemporaneous systematic review and meta-analysis’, International Journal of Cardiology, 257, pp. 207–215. doi: 10.1016/J.IJCARD.2017.12.048.
- Arundel, C. et al. (2016) ‘Association of 30-Day All-Cause Readmission with Long-Term Outcomes in Hospitalized Older Medicare Beneficiaries with Heart Failure’, American Journal of Medicine, 129(11), pp. 1178–1184. doi: 10.1016/j.amjmed.2016.06.018.
- Bettencourt, P. et al. (2004) ‘N-Terminal–Pro-Brain Natriuretic Peptide Predicts Outcome After Hospital Discharge in Heart Failure Patients’, Circulation, 110(15), pp. 2168–2174. doi: 10.1161/01.CIR.0000144310.04433.BE.
- Bloomfield, G. S. et al. (2016) ‘Markers of Atherosclerosis, Clinical Characteristics, and Treatment Patterns in Heart Failure A Case-Control Study of Middle-Aged Adult Heart Failure Patients in Rural Kenya’, Global Heart, 11(1), pp. 97–107. doi: 10.1016/j.gheart.2015.12.014.
- Callender, T. et al. (2014) ‘Heart Failure Care in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis’, PLoS Medicine. Edited by P. Byass, 11(8), p. e1001699. doi: 10.1371/journal.pmed.1001699.
- Calvillo–King, L. et al. (2013) ‘Impact of Social Factors on Risk of Readmission or Mortality in Pneumonia and Heart Failure: Systematic Review’, Journal of General Internal Medicine, 28(2), pp. 269–282. doi: 10.1007/s11606-012-2235-x.
- Carlson, S. et al. (2017) ‘Capacity for diagnosis and treatment of heart failure in sub-Saharan Africa.’, Heart (British Cardiac Society), 103(23), pp. 1874–1879. doi: 10.1136/heartjnl-2016-310913.
- Damasceno, A. et al. (2012) ‘The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: Results of the sub-Saharan Africa survey of heart failure’, Archives of Internal Medicine, 172(18), pp. 1386–1394. doi: 10.1001/archinternmed.2012.3310.
- Fonarow, G. C. et al. (2008a) ‘Factors Identified as Precipitating Hospital Admissions for Heart Failure and Clinical Outcomes<subtitle>Findings From OPTIMIZE-HF</subtitle>’;, Archives of Internal Medicine, 168(8), p. 847. doi: 10.1001/archinte.168.8.847.
- Fonarow, G. C. et al. (2008b) ‘Factors Identified as Precipitating Hospital Admissions for Heart Failure and Clinical Outcomes<subtitle>Findings From OPTIMIZE-HF</subtitle>’;, Archives of Internal Medicine, 168(8), p. 847. doi: 10.1001/archinte.168.8.847.
- Hammond, D. A. et al. (2016) ‘Acute Decompensated Heart Failure’, Journal of Intensive Care Medicine. doi: 10.1177/0885066616669494.
- Haque, M. et al. (2018) ‘Health care-associated infections – An overview’, Infection and Drug Resistance. Dove Medical Press Ltd., pp. 2321–2333. doi: 10.2147/IDR.S177247.
- Hernandez, M. B. et al. (2013) ‘Predictors of 30-Day Readmission in Patients Hospitalized With Decompensated Heart Failure’, Clinical Cardiology, 36(9), pp. 542–547. doi: 10.1002/clc.22180.
- Jaarsma, T. et al. (2009) ‘The European Heart Failure Self-care Behaviour scale revised into a nine-item scale (EHFScB-9): a reliable and valid international instrument’, European Journal of Heart Failure, 11, pp. 99–105. doi: 10.1093/eurjhf/hfn007.
- Januzzi, J. L. et al. (2012) ‘Natriuretic Peptide Testing for Predicting Adverse Events Following Heart Failure Hospitalization’, Congestive Heart Failure, 18(s1), pp. S9–S13. doi: 10.1111/j.1751-7133.2012.00306.x.
- Kamau, D. K. (2009) ‘Post -discharge, short term morbidity and mortality of chronic heart failure at Kenyatta national hospital’. Available at: http://erepository.uonbi.ac.ke/handle/11295/25086 (Accessed: 30 March 2017).
- Khan, H. et al. (2015) ‘Length of hospital stay and 30-day readmission following heart failure hospitalization: insights from the EVEREST trial’, European Journal of Heart Failure, 17(10), pp. 1022–1031. doi: 10.1002/ejhf.282.
- Kimani, L. M. et al. (2016) ‘Treatment of chronic heart failure in adults at a referral hospital in Kenya: adverse drug reactions and determinants of adherence’, J. Pharmacol. Ther. African Journal of Pharmacology and Therapeutics Afr. J. Pharmacol. Ther, 5(51), pp. 35–41.
- Kraus, S. et al. (2016) ‘Heart failure in sub-Saharan Africa: A clinical approach.’, South African medical journal = Suid-Afrikaanse tydskrif vir geneeskunde, 106(1), pp. 23–31. Available at: http://www.ncbi.nlm.nih.gov/pubmed/26933706 (Accessed: 17 November 2017).
- Lee-Lewandrowski, E. et al. (2007) ‘Multi-center validation of the Response Biomedical Corporation RAMP® NT-proBNP assay with comparison to the Roche Diagnostics GmbH Elecsys® proBNP assay’, Clinica Chimica Acta, 386(1–2), pp. 20–24. doi: 10.1016/j.cca.2007.07.015.
- Maro, E. and Makule, C. (2009) ‘Causes of hospital readmission with heart failure at Muhimbili National hospital: Tanzanian experience’, Tanzania Medical Journal, 24(1). doi: 10.4314/tmj.v24i1.46416.
- Michalsen, A., König, G. and Thimme, W. (1998) ‘Preventable causative factors leading to hospital admission with decompensated heart failure.’, Heart (British Cardiac Society), 80(5), pp. 437–41. doi: 10.1136/HRT.80.5.437.
- Michtalik, H. J. et al. (2011) ‘Acute Changes in N-Terminal Pro-B-Type Natriuretic Peptide During Hospitalization and Risk of Readmission and Mortality in Patients With Heart Failure’, The American Journal of Cardiology, 107(8), pp. 1191–1195. doi: 10.1016/J.AMJCARD.2010.12.018.
- O’Brien, R. J. et al. (2003) ‘Pre-discharge, but not admission, levels of NT-proBNP predict adverse prognosis following acute LVF’, European Journal of Heart Failure, 5(4), pp. 499–506. doi: 10.1016/S1388-9842(03)00098-9.
- Ogeng’o, J. et al. (2014) ‘Pattern of Heart Failure in an Adult Kenyan Population’. doi: 10.4172/2324-8602.1000185.
- Platz, E. et al. (2018) ‘Prevalence and prognostic importance of precipitating factors leading to heart failure hospitalization: recurrent hospitalizations and mortality’, European Journal of Heart Failure, 20(2), pp. 295–303. doi: 10.1002/ejhf.901.
- Ponikowski, P. et al. (2014) ‘Heart failure: preventing disease and death worldwide’, ESC Heart Failure, 1(1), pp. 4–25. doi: 10.1002/ehf2.12005.
- Ponikowski, P. et al. (2016) ‘2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure’, European Heart Journal, 37(27), pp. 2129–2200. doi: 10.1093/eurheartj/ehw128.
- Sewagegn, N. and Fekadu, S. (2015) ‘Adherence to Self-Care Behaviours and Knowledge on Treatment among Heart Failure Patients in Ethiopia: The Case of a Tertiary Teaching Hospital’, Journal of Pharmaceutical Care & Health Systems, s4. doi: 10.4172/2376-0419.s4-001.
- Tung, Y.-C. et al. (2016) ‘Worse Prognosis in Heart Failure Patients with 30-Day Readmission.’, Acta Cardiologica Sinica, 32(6), pp. 698–707. doi: 10.6515/ACS20151113A.
- Yancy, C. W. et al. (2013) ‘2013 ACCF/AHA Guideline for the Management of Heart Failure’, Circulation, 128(16). Available at: http://circ.ahajournals.org/content/128/16/e240#sec-194 (Accessed: 31 March 2017).
- Yancy, C. W. et al. (2017) ‘2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America’, Journal of the American College of Cardiology, 70(6), pp. 776–803. doi: 10.1016/j.jacc.2017.04.025.
- Ziaeian, B. and Fonarow, G. C. (2016) ‘Epidemiology and aetiology of heart failure’, Nature Reviews Cardiology, 13(6), pp. 368–378. doi: 10.1038/nrcardio.2016.25.